")
Back to Journals » Infection and Drug Resistance » Volume 16
The Etiological and Drug Resistance Characteristics of Multidrug-Resistant Pathogens in Patients Requiring Extracorporeal Membrane Oxygenation: A Retrospective Cohort Study
Received 15 May 2023
Accepted for publication 19 July 2023
Published 31 July 2023 Volume 2023:16 Pages 4929—4941
DOI https://doi.org/10.2147/IDR.S421413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xinjing Gao,1– 4 Wenjiao Wang1– 4
1Department of Critical Care Medicine, The Third Central Hospital of Tianjin, Tianjin, People’s Republic of China; 2Nankai University Affiliated Third Central Hospital, Nankai University, Tianjin, People’s Republic of China; 3Tianjin Key Laboratory of Extracorporeal Life Support for Critical Diseases, The Third Central Hospital of Tianjin, Tianjin, People’s Republic of China; 4Artificial Cell Engineering Technology Research Center, The Third Central Hospital of Tianjin, Tianjin, People’s Republic of China
Correspondence: Wenjiao Wang, Tel +86-22-84112109, Fax +86-22-84112095, Email [email protected]
Purpose: Infections induced by multidrug-resistant (MDR) pathogens are one of the most common and serious complications in extracorporeal membrane oxygenation (ECMO) patients. However, there is currently little research about “ECMO and MDR bacteria”. The purpose of our study was to clarify the epidemiological characteristics of MDR bacteria and provide references for empiric antibiotic treatments according to the drug susceptibility tests for ECMO patients.
Patients and Methods: There were 104 patients admitted to our department and receiving ECMO treatments between January 2014 and December 2022. Altogether, 61 veno-arterial ECMO (VA-ECMO) and 29 veno-venous ECMO (VV-ECMO) patients enrolled. The data on other intensive care unit (ICU) patients in our department in the same period are summarized.
Results: A total of 82 MDR bacteria were detected from ECMO patients, and most of these were MDR Gram-negative bacteria (MDR-GNB). There were also 5559 MDR-GNB collected from other patients in our department in the same period. We found that the distribution of MDR-GNB in ECMO patients was different from other critical patients. The proportion of Klebsiella pneumoniae (MDR-KP) in VV-ECMO patients was higher than other critical patients (35.1% and 21.3%, respectively). Moreover, the proportions of MDR Acinetobacter baumannii (MDR-AB) of VA-ECMO and VV-ECMO were higher than other critical patients (54.6%, 43.2% and 30.5%, respectively). In addition, MDR-AB and MDR-KP in ECMO patients exhibited higher percentages of drug resistance to possibly appropriate antibiotics for other critical patients, but showed better sensitivity to colistin.
Conclusion: Infections induced by MDR-GNB in ECMO patients were serious and exhibited higher degrees of drug resistance compared with other ICU patients. Colistin might be an option to consider if there is no medical contraindication. However, widespread use of broad spectrum antibiotics is something that should be discouraged, and alternative options are being explored.
Keywords: multidrug-resistant Gram-negative bacteria, MDR-GNB, multidrug-resistant Klebsiella pneumoniae, MDR-KP, multidrug-resistant Acinetobacter baumannii, MDR-AB, colistin
Introduction
Infections caused by multidrug-resistant (MDR) pathogens are a serious problem worldwide, and lead to worsening conditions, prolonged hospital stay and increased costs.1,2 The overuse/misuse of antibiotics against pathogens has allowed the emergence of MDR bacteria due to relevant resistant genes.3 Patients receiving extracorporeal membrane oxygenation (ECMO) treatment, which helps patients with lungs or heart not working normally and uses an artificial lung to oxygenate blood outside the body, are at high risk for MDR infections due to the immunodeficiency caused by severe illness and the applications of invasive life support measures.4 Although clinicians have accumulated rich experience in the application of ECMO, infections induced by MDR bacteria are still one of the most common and serious complications.5
Timely and targeted empirical antibiotic therapies against MDR pathogens are effective measures to improve the situation. Next-generation sequencing (NGS) allows faster acquisition of metagenomic data, but is expensive and not widely available. Bacterial culture as the “gold standard” for diagnosis take too long and therefore miss the best time for anti-infection therapies for ECMO patients. Thus, valid clinical data about etiological characteristics of MDR pathogens and anti-infection experiences against them are important references for early and effective treatments for ECMO patients. A study recently observed that infections induced by Gram-negative bacteria were the majority in trauma patients requiring ECMO support, and advocated that empiric antibiotics should have broad spectrum coverage of Gram-negative organisms in this population.6 The incidence of MDR and extended-spectrum β-lactamase Gram-negative (ESBL GN) bacteria in adult patients undergoing lung transplantation (LT) was 34%, and in-hospital mortality was six times greater.7 However, more in-depth studies on “ECMO and MDR bacteria” are still urgently needed to guide clinicians, and ECMO patients with MDR bacterial infections in optimal management.
The purpose of our study was to clarify the epidemiological characteristics of MDR bacteria in ECMO patients and provide references for empiric antibiotic treatments according to the drug susceptibility tests for this specific population.
Materials and Methods
Study Design and Participants
The study was carried out in the Extracorporeal Life Support Center of Tianjin Third Central Hospital. There were 104 patients admitted to our department and receiving ECMO treatments between January 2014 and December 2022. Altogether, 61 veno-arterial ECMO (VA-ECMO) and 29 veno-venous ECMO (VV-ECMO) patients enrolled according to the study inclusion and exclusion criteria (Figure 1). Inclusion Criteria: (1) Older than 18 years old; (2) Patients receiving VA or VV-ECMO treatment for more than 24 hours. Exclusion Criteria: (1) Patients who had been co-infected before receiving ECMO treatment; (2) Patients treated with other modes of ECMO or combined ventricular assist devices; (3) Patients receiving ECMO treatment for heart and lung transplantation.
 |
Figure 1 The flowchart. Abbreviations: VA-ECMO, Veno-Arterial Extracorporeal Membrane Oxygenation; VV-ECMO, Veno-Venous Extracorporeal Membrane Oxygenation; Group R, Multidrug-resistant bacterial infections Group; Group N, Non Multidrug-resistant bacterial infection bacterial Group; n, the number of patients in each group. |
ECMO patients with MDR infections (group R) were defined as new MDR infection that occurred after having received ECMO treatment for 24 hours or within 30 days after receiving ECMO treatment according to clinical manifestation and laboratory examination. The identification of MDR pathogens was based on “proposed amendments regarding the definitions of MDR and extensively MDR pathogens”.8 The rest of the patients were classified as “non MDR infections group” (group N). The clinical data of ECMO patients in our center for the previous 8 years were collected. We also summarized the etiological data of other ICU patients in the same period, and made a comparison with ECMO patients.
The study was approved by the Ethics Committee of Tianjin Third Central Hospital, and was carried out in accordance with the Declaration of Helsinki and its amendments.
Procedures and Management of ECMO
VA-ECMO was suitable for: (1) Refractory cardiogenic shock or deterioration of cardiac function, with lactic acidosis, mixed venous oxygen saturation below 45% and systolic blood pressure (SBP) < 80 mmHg after adequate volume resuscitation performed and high dose vasopressor infused (norepinephrine > 0.5 μg/kg/min); (2) Cardiac arrest treated with CPR longer than 10 min. VV-ECMO was administered in severe hypoxemia (FiO2 < 100%) or hypercapnia (PaCO2 > 60 mmHg) (Murray score > 3). The patients would not be treated with ECMO if they also had intracranial hemorrhage, advanced malignant tumors or loss of ability to carry out activities of daily living independently.
The cannulations of ECMO were performed by specialized teams in the Extracorporeal Life Support Center or emergency room according to Seldinger’s method. The VV-ECMO supports were used by femoral vein to femoral vein. VA-ECMO most commonly involved femoral artery and vein cannulation. The components of ECMO included: Rotaflow centrifugal pump, Quadrox oxygenator, catheters and tubing (all from Maquet, Rastatt, Germany).
The treatment goals of VA-ECMO were to maintain the mean blood pressure (MBP) greater than 65 mmHg, and the cardiac index (CI) more than 2.5 L/min/m2 by adjusting blood flow depending on the patient’s condition. The VV-ECMO was supplied to improve the arterial oxygen saturation higher than 85% by altering blood flow, and held PaCO2 at 35~45 mmHg by modifying the gas flow.
The Identifications and Antimicrobial Susceptibility Tests of MDR Pathogens
The identifications of pathogens were performed using VITEK-2 Compact System (BioMérieux, CRaponne, France). The antimicrobial susceptibility tests were performed by BioFosun II system (BioMérieux, CRaponne, France). The results of antimicrobial susceptibility tests were interpreted according to The Clinical and Laboratory Standards Institute (CLSI).9
Statistical Analysis
The data were analyzed by IBM SPSS Statistics version 21 software (IBM, Armonk, NY, USA). Numerical variables were tested by independent sample t-test or non-parametric test, and dichotomous variables were compared by chi-square test. 1:1 propensity score matching for VA-ECMO patients and 1:n for VV-ECMO patients were performed to eliminate the confounding factors, and partial correlation analysis was followed. P value less than 0.05 was statistical significance.
Results
The Clinical Characteristic of ECMO Patients with MDR Infections
The prognostic indicators of the two groups in both VA-ECMO and VV-ECMO patients were statistically different, apart from the proportion of patients’ survival to discharge. Compared with group N, the time on mechanical ventilator [249 (156–367) h vs 44 (24–108) h, P = 0.001, Table 1], duration of ECMO support [127 (77–194) h vs 44 (23–95) h, P = 0.001, Table 1], ICU stay time [13 (7–20) d vs 3 (1–8) d, P = 0.001, Table 1], length of hospital stay [13 (7–20) d vs 5 (2–10) d, P = 0.001, Table 1] and the proportion of ECMO weaning (71% vs 26.7%, P = 0.001, Table 1) were longer or higher in group R of VA-ECMO patients. Compared with group N, there were significantly longer times on mechanical ventilator [285 (174–368) h vs 163 (83–251) h, P = 0.031, Table 1] and duration of ECMO support [164 (123–210) h vs 75 (68–149) h, P = 0.047, Table 1] in group R in VV-ECMO patients. All these data showed that ECMO patients with MDR infections required longer life support than other ECMO patients.
 |
Table 1 The Clinical Characteristics of ECMO Patients With or Without MDR Infections |
There were some differences in clinical characteristics between group R and group N, especially in VA-ECMO patients. Therefore, we used 1:1 propensity score matching for VA-ECMO and 1:n for VV-ECMO to eliminate the confounding factors effectively and elucidate the relationship between MDR infections and prognosis indicators more clearly. The prognostic indicators significantly correlated with MDR bacterial infections after propensity-score matching based on the mixed factors (Table 2). Outcomes of ECMO patients displayed separately according to whether they were infected by MDR bacteria are shown in Figure 2.
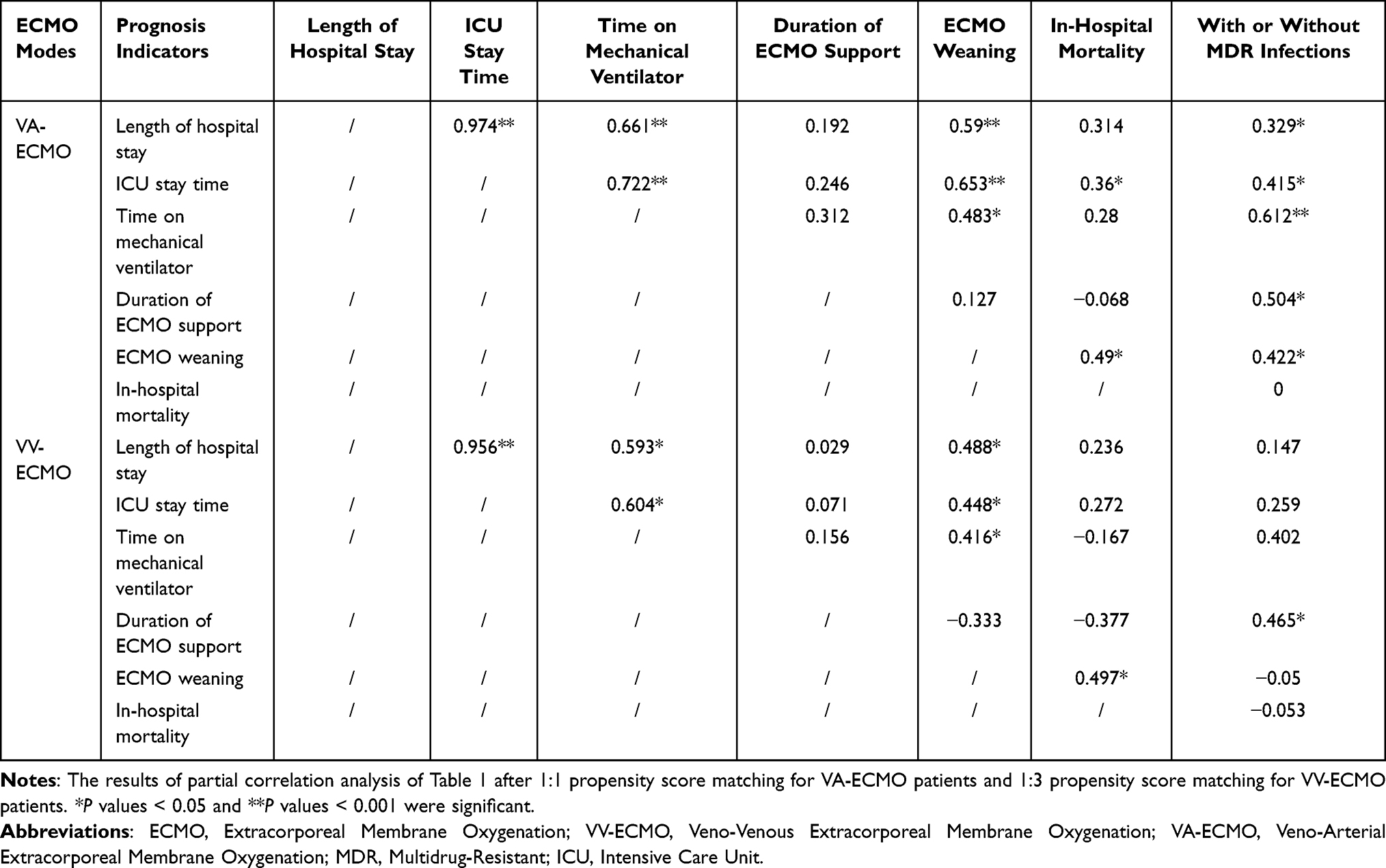 |
Table 2 The Partial Correlation Analysis of MDR Bacterial Infection and Prognosis Indicators |
 |
Figure 2 Outcomes of ECMO patients displayed separately according to whether they were infected by MDR bacteria. |
The Etiological Characteristics of MDR Pathogens in ECMO Patients
A total of 82 MDR bacteria were detected from ECMO patients. There were 75.7% of MDR bacteria deprived from sputum in VA-ECMO patients and 78.4% in VV-ECMO patients. Also, there were some other pathogens derived from scattered sources. The correlations between sources and species of MDR pathogens in our study are shown in Figure 3, Table 3 and 4.
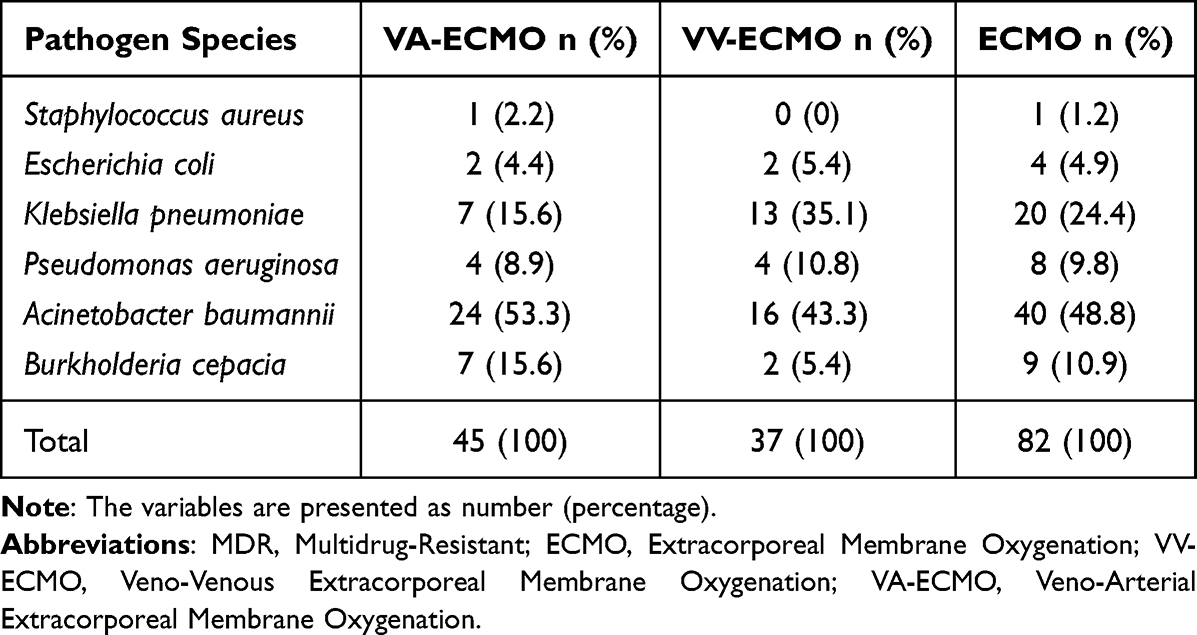 |
Table 3 The Species of MDR Pathogens in ECMO Patients |
 |
Table 4 The Sources of MDR Pathogens in ECMO Patients |
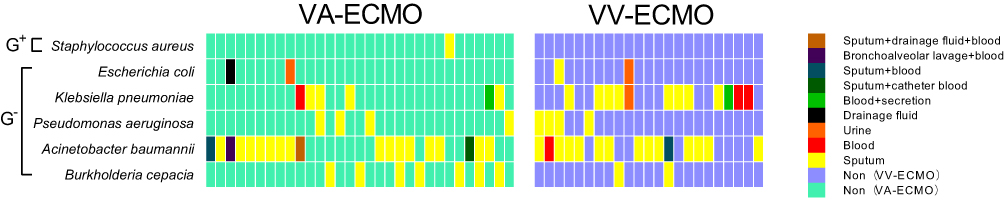 |
Figure 3 Species and sources of MDR pathogens in ECMO patients. The left part of the figure shows the species and sources of MDR pathogens in VA-ECMO patients. The right part of the figure shows the species and sources of MDR pathogens in VV-ECMO patients. Each column represents a patient with MDR infection and each row the bacterium detected. The pathogens were divided into three categories: GPB (Gram-positive bacteria) and GNB (Gram-negative bacteria). The different colors of blocks represent the source of MDR pathogen. The specific meaning of colors are shown in the color indicator on the right of the figure. |
The MDR Gram-negative bacteria (MDR-GNB) were the most detected pathogens in ECMO patients (97.8% in VA-ECMO patients and 100% in VV-ECMO patients, respectively). Also, 5559 MDR-GNB of other ICU patients in the same period were collected. Also, we found that the variety of MDR-GNB in ECMO patients was different from other ICU patients. MDR-GNB detected in ECMO patients were MDR Acinetobacter baumannii (MDR-AB), Pseudomonas aeruginosa (MDRP), Klebsiella pneumoniae (MDR-KP), Escherichia coli and Burkholderia cepacia. Besides these, MDR Proteus mirabilis, Stenotrophomonas maltophilia and some other MDR-GNB were also detected in other ICU patients.
The proportion of MDR-KP in VV-ECMO patients was higher than in other ICU patients (35.1% and 21.3%, respectively). And, the proportions of MDR MDR-AB of VA-ECMO and VV-ECMO patients were higher than other ICU patients (54.6%, 43.2% and 30.5%, respectively) (Figure 4).
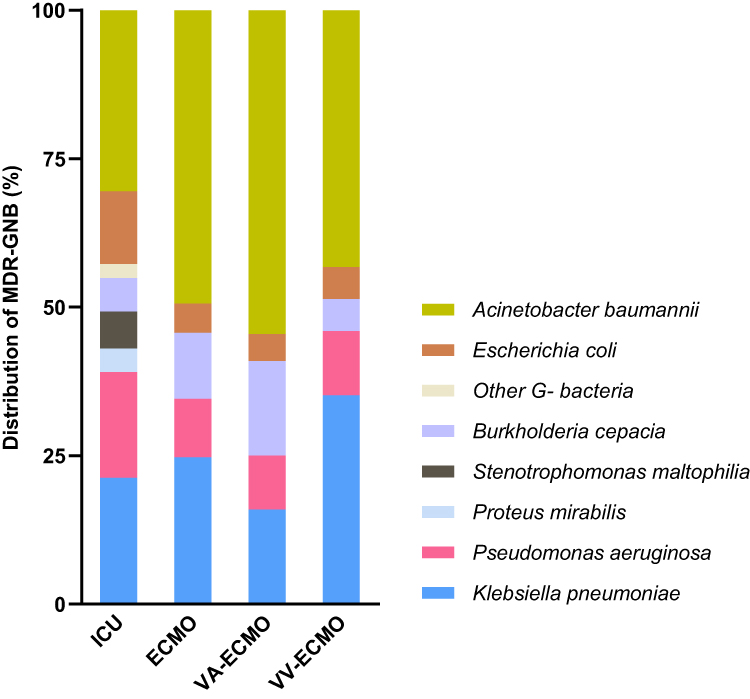 |
Figure 4 The variety of MDR-GNB of ECMO and other ICU patients. |
Appropriate Empiric Antibiotic Strategies Against MDR Pathogens in ECMO Patients
The MDR-GNB in ECMO patients generally had high rates of drug resistance (Table 5 and Figure 5). We conducted further analysis attempting to clarify the difference in MDR bacterial drug resistance between ECMO and other ICU patients. MDR-AB and MDR-KP were most detected in ECMO patients, and compared for drug resistance with other ICU patients. The MDR-AB and MDR-KP in ECMO patients exhibited more resistance to possibly appropriate antibiotics of ICU patients, such as tigecycline, but showed better sensitivity to colistin (Figure 6A and B).
 |
Table 5 The Resistance Ratio of MDR Bacteria to Antibiotics in ECMO Patients |
 |
Figure 5 Heatmap showing the antimicrobial susceptibility results of MDR bacteria in ECMO patients. Each column represented a bacterium detected and each row an antibiotic of antimicrobial susceptibility tests. All of the drugs were divided into six categories according to their functions. The different colors of blocks represent antimicrobial susceptibility to the drugs. The results of antimicrobial susceptibility were divided into three categories: resistant, intermediary and sensitive. The specific meanings of colors are shown in the color indicators on the right of the figure. Abbreviations: ESBL+, Extended-Spectrum β-Lactamases positive; ESBL−, Extended-Spectrum β-Lactamases negative. |
 |
Figure 6 The comparison of drug resistance profiles of MDR bacteria between ECMO and other ICU patients. (A) The comparison of drug resistance profiles of Klebsiella pneumoniae (MDR-KP) in ECMO and other ICU patients in our department. The left columns of (A) represent the resistance rates of MDR-KP to antibiotics in ECMO and other ICU patients. The columns of (A) on the right are the differences in resistance rates of MDR-KP between ECMO and other ICU patients in our department. (B) The comparison of drug resistance profiles of Acinetobacter baumannii (MDR-AB) in ECMO and other ICU patients in our department. The left columns of (B) represent the resistance rates of MDR-AB to antibiotics in ECMO and other ICU patients. The columns of (B) on the right show the differences in resistance rates of MDR-AB between ECMO and other ICU patients in our department. |
Discussion
There were discrepancies in the mortality of ECMO patients with infections in previous studies.10 Some studies concluded that infections significantly increased mortality of ECMO patients.11 The infections induced by MDR bacteria were related to increased in-hospital mortality of patients receiving ECMO treatment due to lung transplantation.7 But, other studies argued that there was no significant difference in in-hospital mortality of ECMO patients between infected groups and uninfected groups.12 It may be because the studies with confounding factors did not show the adverse effect of infections on mortality of ECMO patients. In addition, ECMO patients with MDR infections in our study required longer life support treatments in ICU compared with patients without MDR infections. Our data showed that ECMO patients with MDR infections needed longer life support than other ECMO patients after propensity-score matching based on the mixed factors. However, it still needs to be further explored whether the long-term life support led to the emergence of MDR bacteria, or the emergence of MDR bacteria required longer life support.
MDR-GNB were the most common bacteria in ECMO patients in our study, and also dominated in overall ICU patients.13 The disruption of the gut barrier and translocation of gastrointestinal microbiota have been associated with MDR-GNB infections in critically ill patients.14,15 The gut barrier is damaged by hypoperfusion and hyperoxia-induced oxidative stress in ECMO patients as well.16 It was confirmed that MDR-GNB bacteria colonizing the gut was associated with more than 10-fold odds for subsequent MDR-GNB infection in ECMO patients.17 It has been demonstrated that pneumonia was the most frequent infection in ECMO patients due to the severe conditions, immunosuppression secondary to extracorporeal circulation, prolonged ventilator support and changes of antibiotics pharmacokinetics under ECMO.11 Moreover, researchhas shown that lung was the most common infection site of translocation of MDR-GNB, which also were the main pathogens leading to pneumonia.18,19 This was consistent with our results.
Though MDR-AB and MDR-KP appeared most frequently in MDR-GNB in both ECMO patients and other ICU patients, the proportion of these was higher in ECMO patients in our study. Therefore, MDR-AB and MDR-KP in ECMO patients should be paid more attention compared with other ICU patients. MDR-KP has been reported as an independent risk factor for mortality, and the colonization of MDR-KP increased the incidence of corresponding infections.20,21 MDR-AB were reported as the common pathogens of VAP in Eastern Europe and Asia, but its association with mortality was controversial.22–24 There is currently a report of successful treatment of hypervirulent KP (hvKP) infection in ECMO patients.25 However, there is not much experience in treatment of MDR-GNB in ECMO patients.
MDR-GNB detected in ECMO patients in our study showed high resistance prevalence to antibiotics. Carbapenems and cephalosporins were recommended antibiotics against MDR-GNB in previous studies, especially after the emergence of new drug combinations.26,27 But, the GNB resistant to beta-lactams have gradually increased in recent years.28 Moreover, KP with Extended-Spectrum β-Lactamases (ESBL) and carbapenemase rose continuously.29,30 It showed difficulties in treatment against MDR-GNB, especially in ECMO patients. It had been reported that tigecycline had certain advantages in the treatment of MDR-GNB, and could also maintain relatively stable effective concentrations in the ECMO circulation over an extended period, which is an important feature of the antibiotics for ECMO patients.31–33 But, tigecycline still had a certain proportion of drug resistance to MDR-GNB of ECMO patients in our study, which may be related to prolonged hospital stay and mechanical ventilation.34 Some scholars proposed colistin as salvage treatment for MDR-GNB.35 Although colistin was more sensitive to MDR-GNB in both ECMO and other ICU patients, its applications in ECMO patients were limited by pharmacokinetic properties and nephrotoxicity.36
In addition to the appropriate choices of antibiotics, the pharmacokinetics of antibiotics changed by capillary leakage, altered volume of distribution, or hepatic and renal insufficiency, should also be considered emphatically in ECMO patients.37 Insufficient serum concentrations of antibiotics below predetermined MIC targets occurred often and can be accounted for by pathophysiological changes or renal replacement therapy.38 Therapeutic drug monitoring (TDM) and dose adjustment in ECMO patients are often necessary and recommended by cardiology guidelines.39 But, there was little evidence-based guidance on whether specific doses of antibiotics should be administered to ECMO patients to balance pharmacokinetic changes caused by underlying disease or drug sequestration in the ECMO circuit.40 Because it is difficult to standardize dosage recommendation for antibiotics, the efficacy evaluation of antibiotics against MDR pathogens should be individualized.
There were some limitations to this study that need to be addressed. First, the study covered an 8-year period from 2014 to 2022 leading to poor longitudinal comparability. Second, it was a single-center study with statistical power inefficiencies and inherent methodological flaws. Third, this study mainly focused on the choices of antibiotics according to the antimicrobial susceptibility results, did not involve evaluations of the anti-infection efficacy, which should be assessed individually, and the summarized data had little significance for individualized treatment. Finally, we restricted the population characteristics and ECMO modes, which need to be taken into account when applying the conclusion.
Conclusion
Infections induced by MDR-GNB in ECMO patients are serious and exhibit higher degrees of drug resistance compared with other critical patients. Colistin might be an option to consider if there are no medical contraindications. But, the widespread use of broad spectrum antibiotics is something that should be discouraged, and alternative options are being explored.
Ethics and Consent Statement
This study was designed in accordance with the Declaration of Helsinki and its amendments and approved by the The Third Central Hospital of Tianjin. The requirement to obtain informed consent was waived due to the retrospective nature of the study and the risk of selection bias due to the low survival in this population.
Funding
This study is supported by Tianjin Science and Technology Program, China (No. 18ZXDBSY00100).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Angel ND, Amir MM, Naomi H, et al. Antimicrobial resistance and human mobility. Infect Drug Resist. 2022;15:127–133.
2. Dadgostar P. Antimicrobial resistance: implications and costs. Infect Drug Resist. 2019;12:3903–3910. doi:10.2147/IDR.S234610
3. Ying Z, Wei EH, Qiwen Y. Clinical perspective of antimicrobial resistance in bacteria. Infect Drug Resist. 2022;15:735–746.
4. Gowri R, Esther EA, Jeffrey C, et al. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2018;7:79. doi:10.1186/s13756-018-0370-9
5. Palacios-Baena ZR, Giannella M, Manissero D, et al. Risk factors for carbapenem-resistant gram-negative bacterial infections: a systematic review. Clin Microbiol Infect. 2021;27(2):228–235. doi:10.1016/j.cmi.2020.10.016
6. Schweickhardt SK, Sams VG, Radowsky JS, et al. Infections complicating extracorporeal membrane oxygenation in patients with traumatic injuries. Injury. 2023;54(2):405–408. doi:10.1016/j.injury.2022.11.048
7. Boscolo A, Sella N, Pettenuzzo T, et al. Multidrug-resistant and extended-spectrum β-lactamase gram-negative bacteria in bilateral lung transplant recipients: incidence, risk factors, and in-hospital mortality. Chest. 2022;162(6):1255–1264. doi:10.1016/j.chest.2022.06.046
8. Petros IR, Diamantis K. Proposed amendments regarding the definitions of multidrug-resistant and extensively drug-resistant bacteria. Expert Rev Anti Infect Ther. 2022;20(2):139–146. doi:10.1080/14787210.2021.1945922
9. Romney H, April MB, Janet AH, et al. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100, 31st edition. J Clin Microbiol. 2021;59(12):e0021321. doi:10.1128/JCM.00213-21
10. Xiyuan L, Liangshan W, Hong W, et al. Outcome and clinical characteristics of nosocomial infection in adult patients undergoing extracorporeal membrane oxygenation: a systematic review and meta-analysis. Front Public Health. 2022;10:857873. doi:10.3389/fpubh.2022.857873
11. Bouglé A, Bombled C, Margetis D, et al. Ventilator-associated pneumonia in patients assisted by veno-arterial extracorporeal membrane oxygenation support: epidemiology and risk factors of treatment failure. PLoS One. 2018;13(4):e0194976. doi:10.1371/journal.pone.0194976
12. Simona S, Marco R, Valeria P, et al. Bloodstream infections during post-cardiotomy extracorporeal membrane oxygenation: incidence, risk factors, and outcomes. Int J Artif Organs. 2019;42(6):299–306. doi:10.1177/0391398818817325
13. Roman K, Alexey K. The dynamics of antimicrobial resistance among Enterobacteriaceae isolates in Russia: results of the 2012–2018 INFORM and ATLAS international program studies. Antibiotics. 2022;11(6):790. doi:10.3390/antibiotics11060790
14. Teerawattanapong N, Kengkla K, Dilokthornsakul P, et al. Prevention and control of multidrug-resistant gram-negative bacteria in adult intensive care units: a systematic review and network meta-analysis. Clin Infect Dis. 2017;64(Suppl suppl_2):S51–S60. doi:10.1093/cid/cix112
15. JongHoon H, Sang Kil L, Jae Hee C, et al. Faecal microbiota transplantation reduces amounts of antibiotic resistance genes in patients with multidrug-resistant organisms. Antimicrob Resist Infect Control. 2022;11(1):20. doi:10.1186/s13756-022-01064-4
16. Aya Y, Yoshihiko N, Shiho H, et al. The association between the oral-gut axis and the outcomes of severe COVID-19 patients receiving extracorporeal membrane oxygenation: a case-control study. J Clin Med. 2022;11(5):1167. doi:10.3390/jcm11051167
17. Giacomo G, Vittorio S, Laura A, et al. Gastrointestinal colonization with multidrug-resistant gram-negative bacteria during extracorporeal membrane oxygenation: effect on the risk of subsequent infections and impact on patient outcome. Ann Intensive Care. 2019;9(1):141. doi:10.1186/s13613-019-0615-7
18. Jessica T, Rafael Almeida DA, Nasia S. Risk of infection following colonization with carbapenem-resistant Enterobactericeae: a systematic review. Am J Infect Control. 2016;44(5):539–543. doi:10.1016/j.ajic.2015.12.005
19. Gupta R, Malik A, Rizvi M, Ahmed M, Singh A. Epidemiology of multidrug-resistant gram-negative pathogens isolated from ventilator-associated pneumonia in ICU patients. J Glob Antimicrob Resist. 2017;9:47–50. doi:10.1016/j.jgar.2016.12.016
20. Meštrović T. Antimicrobial resistance in Klebsiella pneumoniae as an independent risk factor for bacteraemia-related mortality. Hong Kong Med J. 2021;27(5):385. doi:10.12809/hkmj219773
21. Xiaohua Q, Shi W, Min H, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae: epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Suppl 2):S206–S214. doi:10.1093/infdis/jiz622
22. Stephen MB, Daniel R, Peter K, et al. Trends in hospital-acquired and ventilator-associated bacterial pneumonia trials. Clin Infect Dis. 2021;73(3):e602–e608. doi:10.1093/cid/ciaa1712
23. Natalia B, Anthony DH, Clare R, et al. Risk factors and outcomes associated with multidrug-resistant Acinetobacter baumannii upon intensive care unit admission. Antimicrob Agents Chemother. 2017;62(1):e01631–e01617. doi:10.1128/AAC.01631-17
24. Evgeni B, Abraham B, Leonid K, et al. Multidrug resistance Acinetobacter bacteremia secondary to ventilator-associated pneumonia: risk factors and outcome. J Intensive Care Med. 2017;32(9):528–534. doi:10.1177/0885066616632193
25. Wenzhong P, Yanhao W, Rongli L, et al. Successful treatment of acute respiratory distress syndrome caused by hypervirulent Klebsiella pneumoniae with extracorporeal membrane oxygenation and continuous renal replacement therapy: a case report and literature review. Front Med. 2022;9:936927. doi:10.3389/fmed.2022.936927
26. Karaiskos I, Lagou S, Pontikis K, et al. The “old” and the “new” antibiotics for MDR gram-negative pathogens: for whom, when, and how. Front Public Health. 2019;7:151. doi:10.3389/fpubh.2019.00151
27. Monsel A, Torres A, Yinggang Z, et al. Nebulized antibiotics for ventilator-associated pneumonia: methodological framework for future multicenter randomized controlled trials. Curr Opin Infect Dis. 2021;34(2):156–168. doi:10.1097/QCO.0000000000000720
28. Nguyen M, Joshi SG. Carbapenem resistance in Acinetobacter baumannii, and their importance in hospital-acquired infections: a scientific review. J Appl Microbiol. 2021;131(6):2715–2738. doi:10.1111/jam.15130
29. Swati S, Tuhina B, Ashok K, et al. Extensive outbreak of colistin resistant, carbapenemase (blaOXA-48, blaNDM) producing Klebsiella pneumoniae in a large tertiary care hospital, India. Antimicrob Resist Infect Control. 2022;11(1):1. doi:10.1186/s13756-021-01048-w
30. Yudong L, Qi W, Chunjiang Z, et al. Prospective multi-center evaluation on risk factors, clinical characteristics and outcomes due to carbapenem resistance in Acinetobacter baumannii complex bacteraemia: experience from the Chinese antimicrobial resistance surveillance of nosocomial infections (CARES) network. J Med Microbiol. 2020;69(7):949–959. doi:10.1099/jmm.0.001222
31. Karaiskos I, Giamarellou H. Carbapenem-sparing strategies for ESBL producers: when and how. Antibiotics. 2020;9(2):61. doi:10.3390/antibiotics9020061
32. Yuan T, QiaoYu Z, LiRong W, Jiansen C. Combined effect of polymyxin B and tigecycline to overcome heteroresistance in carbapenem-resistant Klebsiella pneumoniae. Microbiol Spectr. 2021;9(2):e0015221. doi:10.1128/Spectrum.00152-21
33. Yuan Z, Hongbin H, Qing Z, et al. Effects of ex vivo extracorporeal membrane oxygenation circuits on sequestration of antimicrobial agents. Front Med. 2021;8:748769. doi:10.3389/fmed.2021.748769
34. Čiginskienė A, Dambrauskienė A, Rello J, et al. Ventilator-associated pneumonia due to drug-resistant Acinetobacter baumannii: risk factors and mortality relation with resistance profiles, and independent predictors of in-hospital mortality. Medicina. 2019;55(2):49. doi:10.3390/medicina55020049
35. Lei Z, Xue Z, Yusheng C, et al. Intravenous polymyxin B as adjunctive therapy to high-dose tigecycline for the treatment of nosocomial pneumonia due to carbapenem-resistant Acinetobacter baumannii and Klebsiella pneumoniae: a propensity score-matched cohort study. Antibiotics. 2023;12(2):273. doi:10.3390/antibiotics12020273
36. Pavel S, Jitka R. Pharmacokinetics of colistin during extracorporeal membrane oxygenation. J Antimicrob Chemother. 2022;77(8):2298–2300. doi:10.1093/jac/dkac163
37. Brinkmann A, Röhr AC, Köberer A, et al. Therapeutisches Drug Monitoring und individualisierte Dosierung von Antibiotika bei der Sepsis [Therapeutic drug monitoring and individual dosing of antibiotics during sepsis: modern or just “trendy”?]. Med Klin Intensivmed Notfmed. 2018;113(2):82–93. German. doi:10.1007/s00063-016-0213-5
38. Kühn D, Metz C, Seiler F, et al. Antibiotic therapeutic drug monitoring in intensive care patients treated with different modalities of extracorporeal membrane oxygenation (ECMO) and renal replacement therapy: a prospective, observational single-center study. Crit Care. 2020;24(1):664. doi:10.1186/s13054-020-03397-1
39. Dalhoff K, Abele-Horn M, Andreas S, et al. S3-Leitlinie der Deutschen Gesellschaft für Anästhesiologie und Intensivmedizin e.V., der Deutschen Gesellschaft für Infektiologie e.V., der Deutschen Gesellschaft für Hygiene und Mikrobiologie e.V., der Deutschen Gesellschaft für Pneumologie und Beatmungsmedizin e.V., der Paul-Ehrlich Gesellschaft für Chemotherapie e.V, der Deutschen Röntgengesellschaft und der Gesellschaft für Virologie[Epidemiology, diagnosis and treatment of adult patients with nosocomial pneumonia - update 2017 - S3 guideline of the German society for anaesthesiology and intensive care medicine, the German society for infectious diseases, the German society for hygiene and microbiology, the German respiratory society and the Paul-Ehrlich-society for chemotherapy, the German radiological society and the society for virology]. Pneumologie. 2018;72(1):15–63. German. doi:10.1055/s-0043-121734
40. Abdul-Aziz MH, Roberts JA. Antibiotic dosing during extracorporeal membrane oxygenation: does the system matter? Curr Opin Anaesthesiol. 2020;33:71–82. doi:10.1097/ACO.0000000000000810
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.