")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
The Efficacy of Lung Volume Reduction Coil Treatment in Patients with Severe Chronic Obstructive Pulmonary Disease (COPD) Type II Respiratory Failure
Authors Yildiz F
Received 8 June 2019
Accepted for publication 28 January 2020
Published 3 March 2020 Volume 2020:15 Pages 479—486
DOI https://doi.org/10.2147/COPD.S218785
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Fidan Yildiz
Okan University, Okan University Chest Diseases, İçmeler, Turkey
Correspondence: Fidan Yildiz Aydınlı Street No: 2, İçmeler 34947, Tuzla, Istanbul, Turkey
Tel +905325614777
Email [email protected]
Purpose: Emphysema is a progressive and irreversible disease, proceeding with the decrease in elastic recoil which is connected to tissue damage caused by chronic inflammation. Lung volume reduction coil (LVRC) method in patients with an advanced level of emphysema and irresponsive to medical treatment is shown to provide increase in lung volumes and exercise capacity, decrease in dyspnea, and increase in quality of life. The purpose of this study is to reveal that LVRC treatment is also efficient in severe COPD patients with hypercapnic respiratory failure.
Patients and Methods: Eleven cases with severe COPD and emphysema were included in the study. LVRC treatment method was applied in upper lobes of both lungs in patients with severe COPD (FEV1 < %45) and Type-2 respiratory insufficiency (PCO2 55– 80 mmHg) who were having medical treatment and CPAP treatment. The patients were followed up for a period of twelve months using arterial blood gas analysis.
Results: Beginning with the first month of the LVRC treatment, PCO2 levels were found to be significantly decreased in all patients using arterial blood gas analysis.
Conclusion: LVRC method can provide physiological and functional recovery and progress in quality of life in severe COPD cases. It is demonstrated that LVRC treatment caused significant decreases in carbon dioxide levels as well as causing improvement in life quality and respiratory function tests in the patients with hypercapnic respiratory failure.
Keywords: lung volume reduction coil treatment, severe chronic obstructive pulmonary disease, type II respiratory failure
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the major causes of morbidity and mortality worldwide and will be the third main cause of death by 2020.1 It is estimated that 4.5 million people will die due to the complications caused by COPD until 2030.2
It is characterized by structural changes in lung parenchyma with consecutive reduction of gas exchange surface, loss of elastic recoil and dynamic hyperinflation leading to dyspnea, limited exercise capacity and reduced quality of life. I the advanced stages, it leads to respiratory failure: hypoxemia and eventually chronic hypercapnic respiratory failure. Hyperinflation is a major component in the development of chronic hypercapnic respiratory failure as it is associated with an increased ventilatory workload, with key pathophysiological elements being the loss os elastic recoil as well as geometrical changes of diaphragm and thorax compromising the function of the diaphragmatic, intercostal and accessory muscles.3 Correspondingly, increasing dyspnea, decrease in exercise performance, decreases in physical activity and life quality occur in the patients.4 The purposes of medical treatment in these patients are to basically ease symptoms and to reduce exacerbations through inhaled bronchodilators, antiinflammatory drugs, appropriate nutrition, rehabilitation and oxygen treatment.5 Currently, pharmacologically present treatment options have limited efficacy in the patients with severe COPD. There are invasive surgical procedures such as lung volume reduction surgery and lung transplantation only in a very few patient subgroup with COPD.6,7 The benefits of volume reduction surgery performed on the purpose of reducing volume in such group of patients are demonstrated in National Emphysema Treatment Trial:(NETT) study. In addition to it, NETT demonstrates that severe cardiopulmonary complications develop in these patients and same successful results are not achieved in all of the patients with severe emphysema.8–11
Therapeutic interventions applied in patients with emphysematous COPD phenotype in bronchoscopy in recent years have effect by reducing hyperinflation.11 Endobronchial valve (EBV) is the most comprehensively researched technique in bronchoscopic lung volume reduction site. I especially demonstrates significant clinical recoveries in the presence of emphysema and intact fissure manly in the upper lobe.12,13 In addition to it, successful clinical results of EBV treatment are only possible in the patients with no interlobar collateral ventilation and when one-way valves are placed to completely close the whole air route in target lobe, it may be quite difficult due to local anatomy and in technical terms in the absence of important experience with these devices.12–15
It is predicted that only approximately 33% of severe emphysema patients do not have collateral ventilation between target and adjacent lobes and therefore they may potentially be treated by using one-way valves.15 This situation directly demonstrates requirement for alternative bronchoscopic treatment operating independent from the presence of collateral ventilation. LVRC method is demonstrated to be an effective and reliable treatment method prominently improving pulmonary functions, effort capacity and life quality in the patients with serious emphysema.16–19 It is also determined that dependency on oxygen in the patients undergoing oxygen treatment at home due to hypoxic respiratory failure prominently decreases. This study is performed to determine whether the procedure is effective in severe COPD patients with hypercapnic respiratory failure.
Method
Study Design and Participants
This is a retrospective study. The files of the patients with high PCO2 values among the ones, who were administered LVRC treatment in Sifa University hospital between August 2014 and August 2015. Respiratory function tests and PCO2 values performed in the control are recorded. The protocol was approved by Okan University ethics committee (approval number: 102). All participants provided written informed consent, and the study was conducted in accordance with the Declaration of Helsinki.
Patient Selection Criteria
Patients at GOLD stage 3 or 4 and (55–80 mmHg PCO2 value in arterial blood gas analysis) were eligible to be enrolled in this study. Details of the inclusion and exclusion criteria are listed in Table 1. Patients with homogenous as well as heterogeneous emphysema were eligible. Leading inclusion criteria were a post-bronchodilator forced expiratory volume in one second (FEV1) <45% predicted, total lung capacity (TLC) >100% predicted. Patients were excluded if they had giant bullae >1/3 of lung volume, 6 min walk distance <140 m, or if they had previous LVRS or lung transplantation. The patients with 55–80 mmHg PCO2 values in arterial blood gas analysis were included in the study.
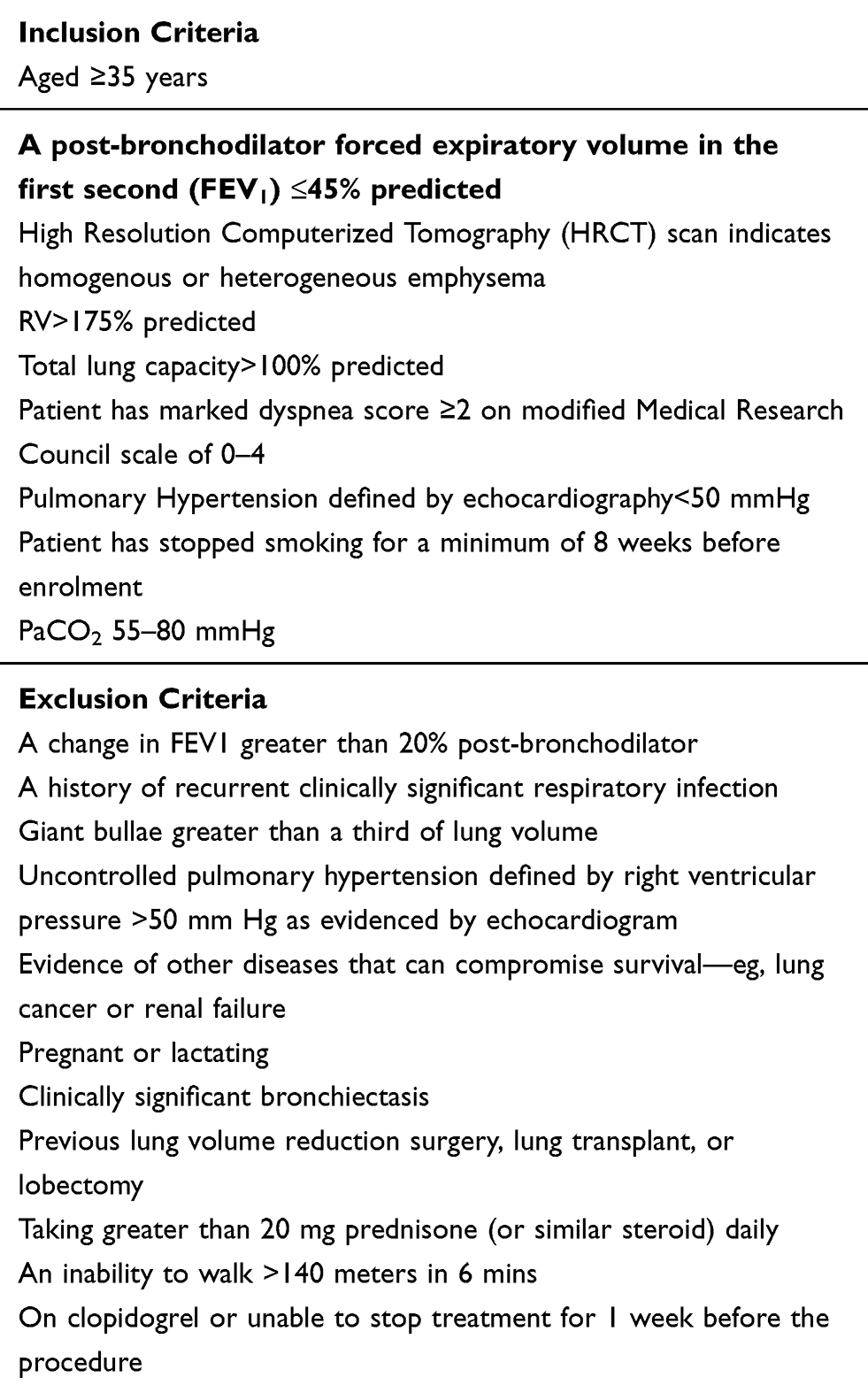 |
Table 1 Enrolment Criteria |
Procedures
The PneumRx volume reduction coil is an implantable, shape memory Nitinol device. The system (RePneu®, Lung Volume Reduction Coil System, PneumRx, Inc. Mountain View, CA USA) consists of a cartridge, catheter, guidewire, forceps and coils suitable for single patient use. The system is shown in Figure 1. Three different coil lengths are designed for different airway lengths (100, 125 and 150 mm). The distal and proximal ends of the coil are designed to remain in the sub-segmental airways. In this study, bronchoscopy was performed using a 9.0 mm endotracheal flexible tube and flexible bronchoscope under general anesthesia (BF180; Olympus, 2.8-mm working channel, 6.0-mm outer diameter).
 |
Figure 1 The system (RePneu®, Lung Volume Reduction Coil System, PneumRx, Inc. Mountain View, CA USA) consists of a cartridge, catheter, guidewire, forceps and coils suitable for single patient use. |
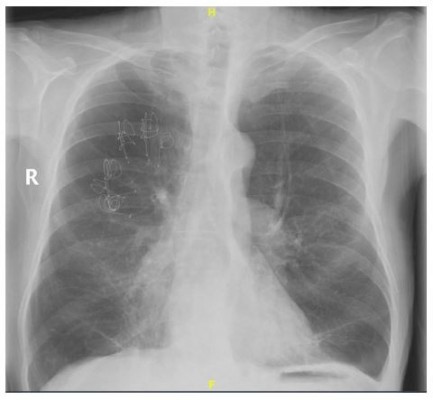
During bronchoscopy, the guidewire is first placed to the desired airway in the fluoroscopic guide. After a catheter is passed over the guidewire, it is aligned with the distal end of the guidewire at a distance of 15 mm from the pleura. Airway length is measured by radio-opaque markers to select the coil length. The guidewire is then removed and a flattened LVR coil which was previously placed in a cartridge is pushed forward through the catheter with a biopsy forceps using a fluoroscopic guide. Then, while the LVR coil remains in place, the catheter is removed and the coil returns to its original shape. Finally, the LVR coil is removed from the biopsy forceps. These steps are repeated for each coil to be installed. The radiological view is shown in Figure 2. Patients received a 5-day prednisolone (40 mg once a day) and 5 days of moxifloxacin (500 mg once a day).
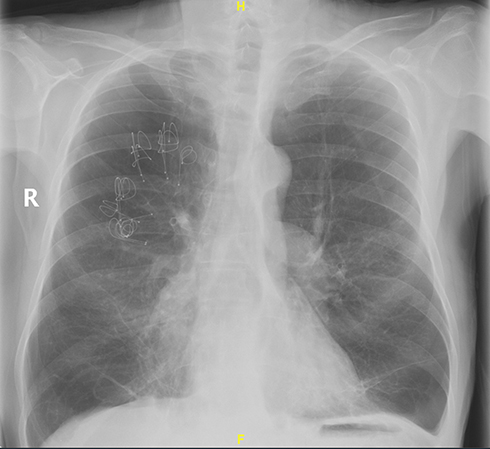 |
Figure 2 The radiological view. |
Follow-Up
All peri-procedural and in house events were charted. Patients were called to the clinic for follow-up visits, which included physical examination, spirometry, plethysmography, 6 min walk test, CAT dyspnea questionnaire and arterial blood gas measurement. At the physician’s discretion, the patient could have a second LVRC treatment, with similar follow-up at 1, 3, 6, 9 and 12 months. Following the final 12-month visit, all patients left the study.
Statistical Analysis
Data were analyzed using a statistical software package. Descriptive data are presented as averages±standard deviations (SDs) or medians (ranges). Comparison of before and after results of LVRC treatment was made by Wilcoxon signed ranks test. Changes between the baseline and 1-year data were analyzed. The results were adopted at a 95% confidence interval, and a P value <0.05 was considered to indicate statistical significance.
Results
Eleven (eight heterogeneous and three homogeneous emphysema) patients with severe COPD were included in the study between August 2014 and August 2015. One patient was treated unilaterally and ten were treated bilaterally. The unilaterally treated patient could not be treated because of giant bullae in the other lung. After one month, 10 patients were given second session treatments. Demographic and baseline values of the patients are shown in Tables 2 and 3. An average of 10 (range 8–16) coils were placed in the eligible lung lobe of the patients. A total of 212 coils was used in 21 operations (Table 4). The mean duration of the procedure was 27.14 min (range 12–50 min). Blood gas analysis was performed after 1, 3, 6, 9 and 12 month-follow-up.
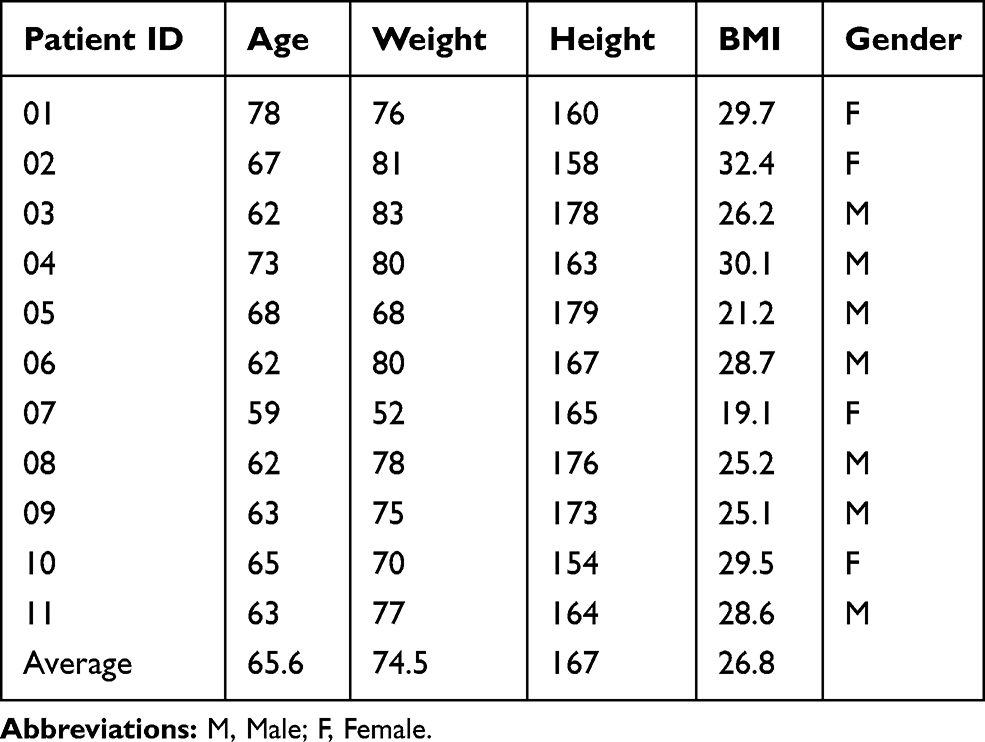 |
Table 2 Demographics of the Enrolled Patients in This Study |
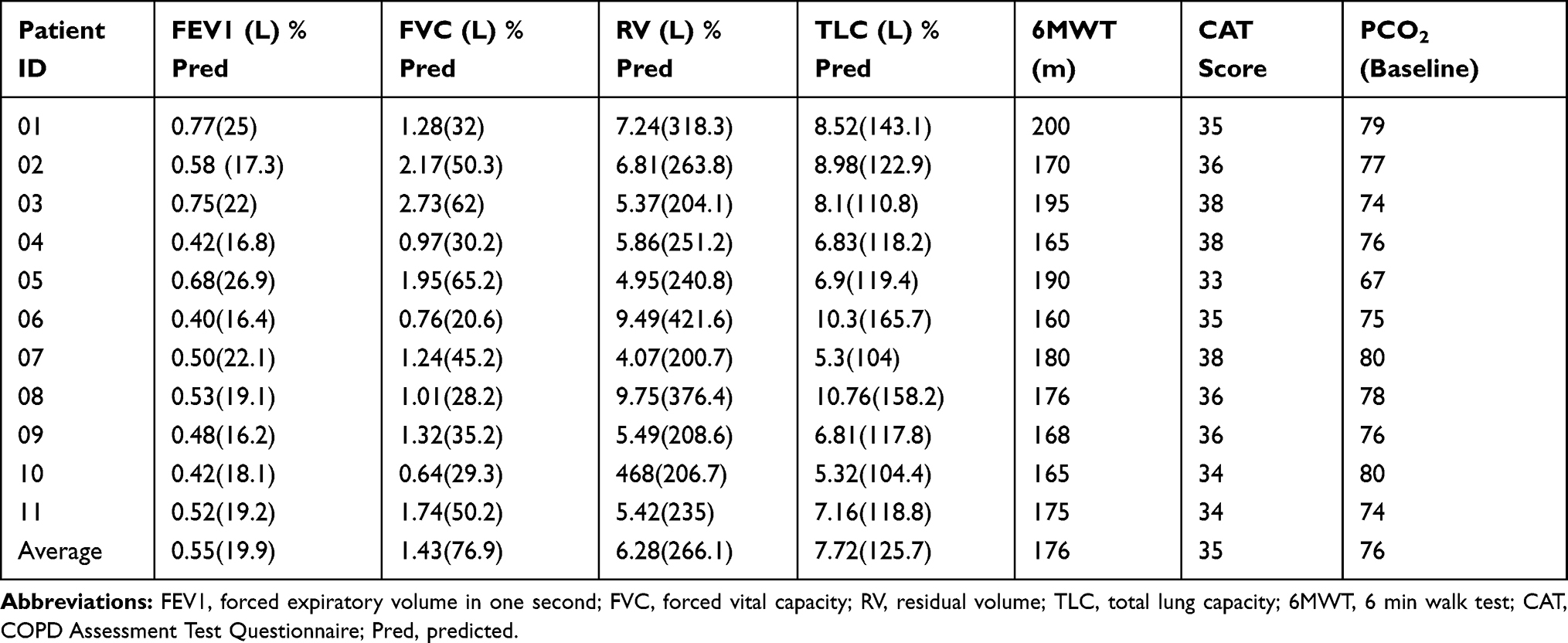 |
Table 3 Baseline Measurements Obtained Before Study Intervention |
 |
Table 4 Data of the Lobes Treated, Average Number of Coils Placed |
Safety
There were no complications related to anesthesia. The average duration of anesthesia lasted 1 hr. No pneumothorax was observed during or after the procedure. Six patients (54.5%) had minor hemorrhage during the procedure. Light hemorrhage persisted for three days in three patients. During the 1-year follow-up period, pneumonia developed in four patients (36.4%) at 1, 6, 9 and 12 months. Three of these patients were treated as outpatients and one patient was hospitalized. The hospitalized patient was administered with IV antibiotherapy due to pneumonia in the first month of the procedure and with IV 80 mg/day prednisolone against possible pneumonitis for three days. Three patients had COPD exacerbation, one patient had respiratory failure requiring intensive care follow-up. Side effects are shown in Table 5.
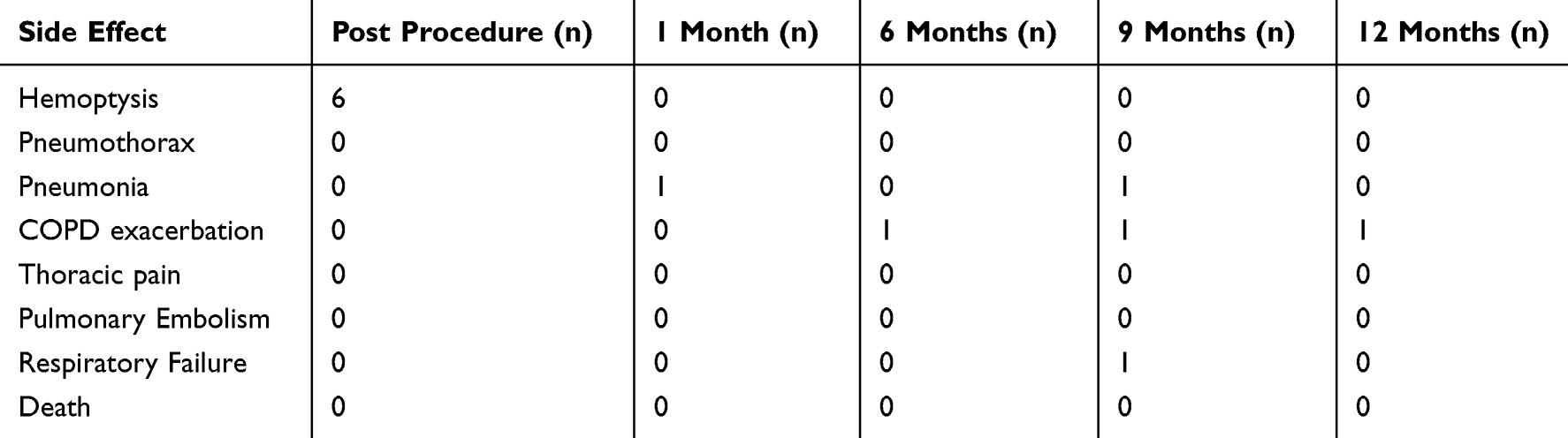 |
Table 5 Side Effects Observed During the Study |
Efficacy
When compared to the initial values, LVR coil treatment provided improvement 28 m at 3rd month, 23 m at 6th month and 10 m at 12th month in 6MWT, and a drop value of 27–30 in CAT score. RV and TAC significantly decreased. Although there was a significant increase in FEV1 at 3rd and 6th months, the increase seen at the end of 1 year was not statistically significant (Table 6). PCO2 values were significantly decreased (Table 7 and Figure 3).
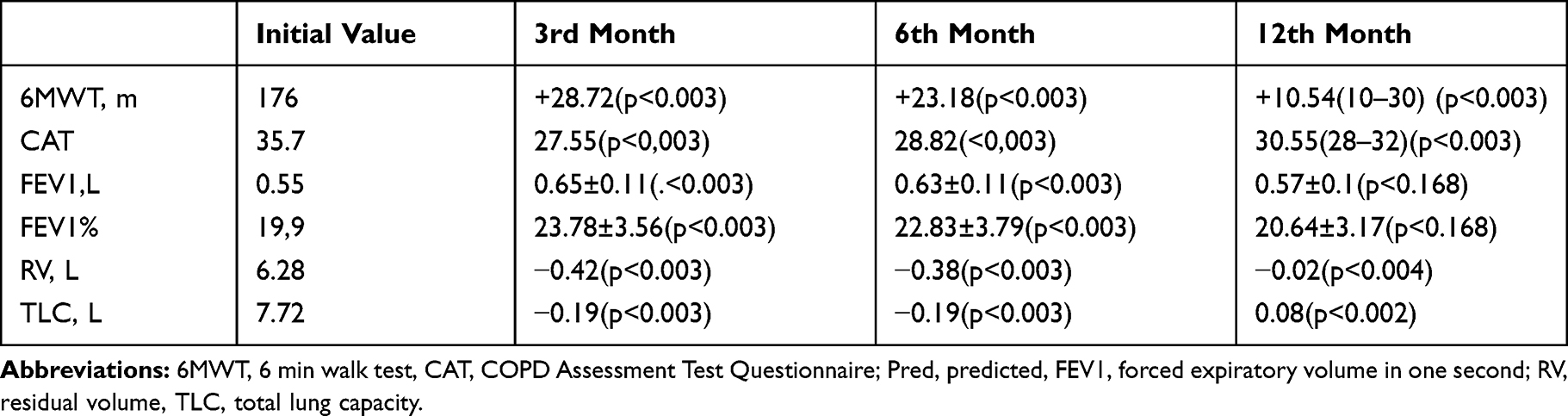 |
Table 6 Efficacy results at 12th Months |
 |
Table 7 The Significance Decrease in Carbon Dioxide Levels in Follow-Up |
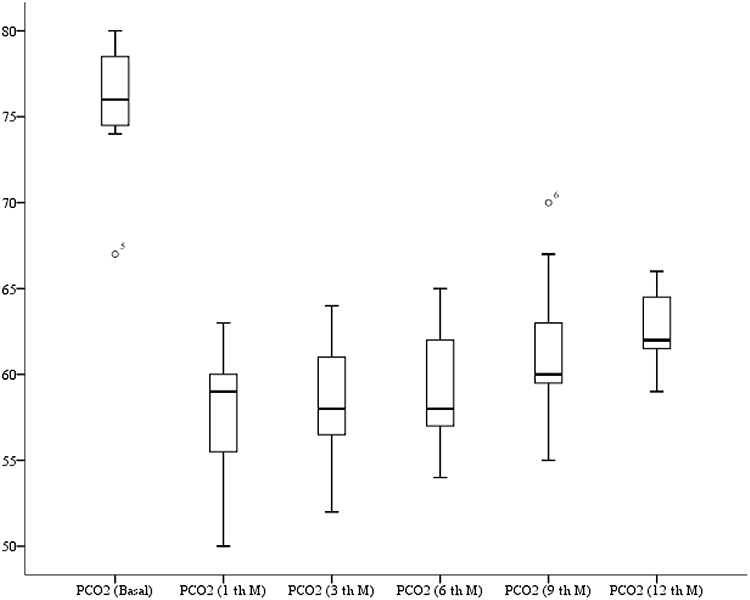 |
Figure 3 1 year PCO2 follow-up values. |
Discussion
Normally working lungs are flexible and as the patient inhales and exhales, they expand and gather back efficiently in order to transfer the air freely from the bronchi to alveoles. Tissue is damaged in the lungs with emphysema and loses the flexibility.20
Improvement in clinical and function parameters observed after LVRC treatment may be associated with volume reduction and parenchyma of the sick lung is compressed by means of flexible characteristic of Nitinol wire, by which spirals are made, and the lung efficiently expands after this procedure by means of recovered mechanic features of remaining tissue. It decreases dynamic hyperinflation occurring potentially in these patients. Air trapping is prevented and carbon dioxide accumulation may be decreased by this way.21,22
Efficacy and reliability of LVRC treatment in the patients with emphysema are demonstrated in the studies performed as of the first pilot publication published in 2011 by Herth et al 11 patients were treated in the study and treatment efficacy is demonstrated by 3 months of follow-up. No justification is made in relation to excluding the patients with high carbon dioxide.16 We evaluated long-term reliability and improvements of LVRC treatment in 11 patients with hypercapnic respiratory failure with emphysema in our research contrary to the studies performed. We saw that there were also significant improvements in clinic and functional parameters including FEV1, RV, TLC, 6MWD and CAT in this patient group at the end of 12 months of follow-up. However, when evaluated over 12 months, improvement is observed to be in acceptable level in other parameters except for FEV1. Our study could not show significant improvement in FEV1 apart from other studies performed with 1 year of follow-up period. The reason for it may be associated with the fact that clinic situation depending on PCO2 highness is severer.
Four studies performed as of 2011 in LVRC treatment are performed as randomized controlled. It was revealed also in these studies that significant improvements occurred in functional and clinic parameters in the groups treated (Table 8). Carbon dioxide highness was not mentioned as an exclusion criteria in none of these studies.17,19,23,24 Renew study is the study with the highest patient participation. In sub-group analysis of the study, it was revealed that there were more significant improvements in 6DYT, respiratory function parameters and life quality in the patient group with RV>225. It was mentioned only in expert panel published by Slebos et al that the patients with PCO2>55 mmHg were excluded from the study.25 Retrospective study of Simon et al is the first study performed in relation to LVRC treatment efficacy in the patients with hypercapnic respiratory failure. The number of patients is determined as 10 in this study and PCO2 level is identified as 45–65 mmHg. According to the results, LVRC not only increased respiratory capacity but also provided significant reductions in PCO2 level.26 The results are also the same in our study. PCO2 values are higher in our patient group and although the number of the patients is low, improvements in functional and clinic parameters were still observed after 1 year of follow-up. Probably the number of the patients may be increased in subsequent processes and positive results may be achieved and this patient group may also be included in study inclusion criteria.
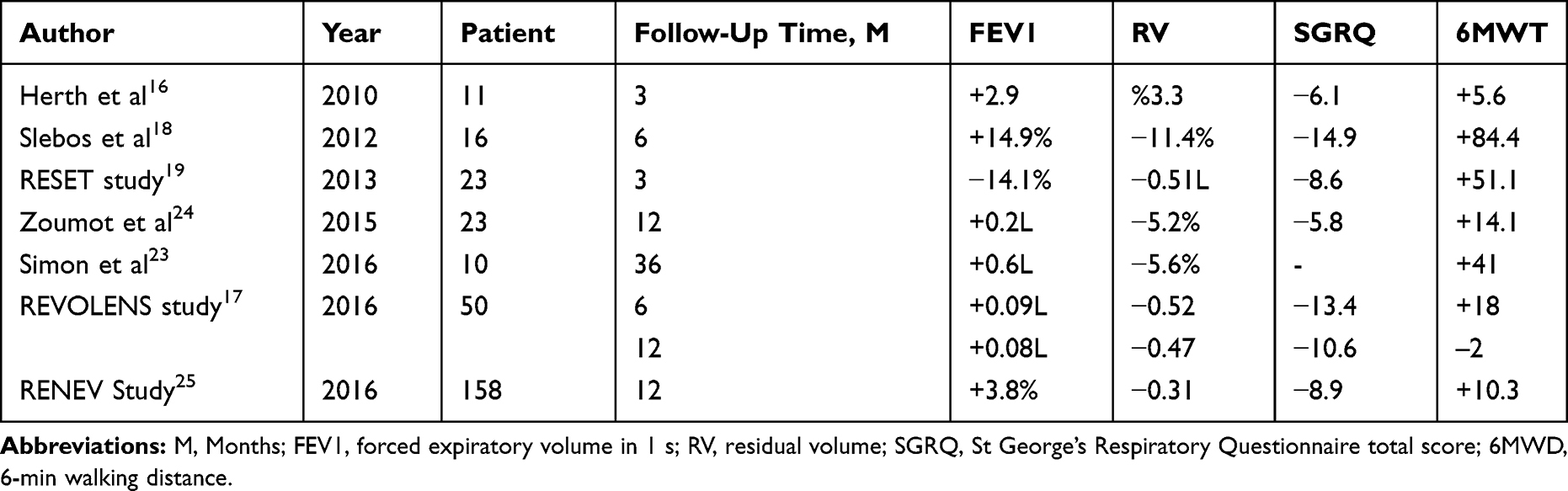 |
Table 8 Review of Previous LVRC Studies |
LVRC procedure is a process performed by general anesthesia. Hypercapnic patient group may have been considered as exclusion criteria in the studies due to the fact that it was a patient group, in which the situation due to respiratory depression caused by general anesthesia may get severer. However, we observed as a result of our study that this group of patients may tolerate anesthesia comfortably and no respiratory failure developed after the procedure. Therefore, we consider that LVRC treatment may reliably be performed in hypercapnic respiratory failure group.
In the current multi-center research including 11 centers, no serious side effects were reported during LVR spiral treatment procedure and therefore procedure reliability was proved. Our results prove an acceptable safety profile for LRV spiral treatment and side effect rate was similar to previous reports in relation to LVR spiral treatment.16,19 However, pneumonia, pneumothorax and COPD inflammation rates in col treatment group were observed to be higher compared to previous studies and control group in RENEW and REVOLENS studies with widespread patient participation.17,24
Conclusion
It was revealed by the studies performed that LVRC treatment was innovative bronchoscopic technique promising hope for the treatment of patients with severe emphysema.16,17,19,24 In patients who qualify, LVRC should be considered the Global Initiative for Obstructive Lung Disease (GOLD) standard.27 We revealed in our research that it was a reliable and efficient treatment method in the emphysema patients with hypercapnic respiratory failure though the number of patients were a few. LVRC treatment may be performed on selected patients with carbon dioxide highness with larger scale studies.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–365. doi:10.1164/rccm.201204-0596PP
2. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1164/rccm.201701-0218PP
3. Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl. 2003;47:3s–14s. doi:10.1183/09031936.03.00038503
4. Baraldo S, Turato G, Saetta M. Pathophysiology of the small airways in chronic obstructive pulmonary disease. Respiration. 2012;84:89–97. doi:10.1159/000341382
5. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
6. Martinez FJ, Chang A. Surgical therapy for chronic obstructive pulmonary disease. Semin Respir Crit Care Med. 2005;26(2):167–191. doi:10.1055/s-2005-869537
7. Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348:2059–2073.
8. Naunheim KS, Wood DE, Krasna MJ, et al. Predictors of operative mortality and cardiopulmonary morbidity in the National Emphysema Treatment Trial. J Thorac Cardiovasc Surg. 2006;131:43–53. doi:10.1016/j.jtcvs.2005.09.006
9. Naunheim KS, Wood DE, Mohsenifar Z, et al. Long-term follow-up of patients receiving lung-volume-reduction surgery versus medical therapy for severe emphysema by the National Emphysema Treatment Trial Research Group. Ann Thorac Surg. 2006;82:431–443. doi:10.1016/j.athoracsur.2006.05.069
10. Wood DE. Results of lung volume reduction surgery for emphysema. Chest Surg Clin N Am. 2003;13:709–726. doi:10.1016/S1052-3359(03)00100-5
11. Fessler HE, Scharf SM, Ingenito EP, et al. Physiologic basis for improved pulmonary function after lung volume reduction. Proc Am Thorac Soc. 2008;5:416–420. doi:10.1513/pats.200708-117ET
12. Herth FJ, Noppen M, Valipour A, et al. Efficacy predictors of lung volume reduction with Zephyr valves in a European cohort. Eur Respir J. 2012;39(6):1334–1342. doi:10.1183/09031936.00161611
13. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. doi:10.1056/NEJMoa0900928
14. Herth FJ, Eberhardt R, Gompelmann D, et al. Radiological and clinical outcomes of using Chartis to plan endobronchial valve treatment. Eur Respir J. 2013;41:302–308. doi:10.1183/09031936.00015312
15. Shah PL, Herth FJ. Current status of bronchoscopic lung volume reduction with endobronchial valves. Thorax. 2014;69:280–286. doi:10.1136/thoraxjnl-2013-203743
16. Herth FJ, Eberhard R, Gompelmann D, et al. Bronchoscopic lung volume reduction with a dedicated coil: a clinical pilot study. Ther Adv Respir Dis. 2010;4(4):225–231. doi:10.1177/1753465810368553
17. Deslée G, Mal H, Dutau H, et al.; REVOLENS Study Group. Lung volume reduction coil treatment vs usual care in patients with severe emphysema: the REVOLENS randomized clinical trial. JAMA. 2016;315(2):175–184. doi:10.1001/jama.2015.17821.
18. Slebos DJ, Klooster K, Ernst A, et al. Bronchoscopic lung volume reduction coil treatment of patients with severe heterogeneous emphysema. Chest. 2012;142(3):574–582. doi:10.1378/chest.11-0730
19. Shah PL, Zoumot Z, Singh S, et al; RESET trial Study Group. Endobronchial coils for the treatment of severe emphysema with hyperinflation (RESET): a randomized controlled trial. Lancet Respir Med. 2013;1(3):233–240. doi:10.1016/S2213-2600(13)70047-X
20. Cooper CB. The connection between chronic obstructive pulmonary disease symptoms and hyperinflation and its impact on exercise and function. Am J Med. 2006;119(10 Suppl 1):21–31. doi:10.1016/j.amjmed.2006.08.004
21. Shabalovskaya SA. Surface, corrosion and biocompatibility aspects of Nitinol as an implant material. Biomed Mater Eng. 2002;12(1):69–109.
22. Duerig TW, Pelton AR, Stockel D. The utility of superelasticity in medicine. Biomed Mater Eng. 1996;6(4):255–266.
23. Zoumot Z, Kemp SV, Singh S, et al. Endobronchial coils for severe emphysema are effective up to 12 months following treatment: medium term and cross-over results from a randomized controlled trial. PLoS One. 2015;10(4):e0122656. doi:10.1371/journal.pone.0122656
24. Sciurba FC, Criner GJ, Strange C, et al.; RENEW Study Research Group. Effect of endobronchial coils vs usual care on exercise tolerance in patients with severe emphysema: the RENEW randomized clinical trial. JAMA. 2016;315(20):2178–2189. doi:10.1001/jama.2016.6261.
25. Slebos DJ, Ten Hacken NH, Hetzel M, et al. Endobronchial coils for endoscopic lung volume reduction: best practice recommendations from an expert panel. Respiration. 2018;96(1):1–11. doi:10.1159/000490193
26. Simon M, Harbaum L, Oqueka T, et al. Endoscopic lung volume reduction coil treatment in patients with chronic hypercapnic respiratory failure: an observational study. Ther Adv Respir Dis. 2017;11(1):9–19. doi:10.1177/1753465816676222
27. GOLD Global strategy for the diagnosis, management and prevention of COPD; 2017. Available from: http://oldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.