")
Back to Journals » Infection and Drug Resistance » Volume 16
The Efficacy and Safety of Shashen-Maidong Decoction Combined with Western Medicine in the Treatment of Omicron Infected Individuals Over 85 Years Old: A Retrospective Study
Authors Lin XX, Yin YQ, Zhang WZ, Huang JH, Hu WS
Received 28 August 2023
Accepted for publication 17 November 2023
Published 28 November 2023 Volume 2023:16 Pages 7339—7348
DOI https://doi.org/10.2147/IDR.S433815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiao-Xi Lin,1,* Yu-Qi Yin,2,* Wen-Zheng Zhang,3 Jia-Huan Huang,4 Wei-Shang Hu1
1Geriatric Medicine Center, Department No. 2 of Acupuncture & Massage, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, Hangzhou, Zhejiang, 310024, People’s Republic of China; 2The Third Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310053, People’s Republic of China; 3Emergency and Critical Care Center, Department of Intensive Care Unit, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, Hangzhou, Zhejiang, 310024, People’s Republic of China; 4Geriatric Medicine Center, Department of General Practice, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, Hangzhou, Zhejiang, 310024, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei-Shang Hu, Geriatric Medicine Center, Department No. 2 of Acupuncture & Massage, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, No. 1 of WangJiangShan Road, XiHu District, Hangzhou, Zhejiang, 310000, People’s Republic of China, Tel +86 571 87091302, Fax +86 571 87091089, Email [email protected]
Background: During the Omicron variant outbreak of COVID-19 (2022– 2023), Chinese healthcare institutions combined traditional Chinese medicine (TCM) with Western medical practices to treat COVID-19 patients, especially the elderly. The efficacy and safety of this approach, especially for individuals aged over 85, need further investigation.
Methods: In this retrospective study, a cohort of 62 patients aged over 85 years, diagnosed with COVID-19 infection, was examined. Among them, 34 patients were administered Shashen-Maidong decoction in conjunction with Western medicine (SMD+WM group), while the remaining 28 patients received only Western medicine (WM group). Comparative analysis was conducted between the two groups, encompassing parameters such as the duration for the nucleic acid test to turn negative, length of intensive care unit (ICU) stay, mortality rate, utilization of high-flow nasal cannula oxygen (HFNC), occurrence of endo-tracheal intubation, frequency of recurrent respiratory infections within three months, and various laboratory indicators.
Results: There were no significant differences observed between the two groups in terms of the duration for the nucleic acid test to turn negative, the length of ICU stay, mortality rate, utilization of HFNC, performance of endo-tracheal intubation, or the frequency of recurrent respiratory infections within three months (P > 0.05). However, in comparison to the WM group, the SMD+WM group exhibited notably lower growth rates in white blood cell (WBC) and neutrophil (NEUT) values. Additionally, the SMD+WM group demonstrated superior improvement in cardiac troponin I (cTnI) and B-type natriuretic peptide (BNP) values.
Conclusion: In contrast to the administration of Western medicine alone, the combined use of Shashen-Maidong decoction with Western medicine significantly suppresses the increase in WBC count, particularly in NEUT levels, in elderly patients diagnosed with COVID-19. Moreover, this combined treatment exhibits a protective effect on cardiac function and demonstrates a relatively safe profile.
Keywords: COVID-19, traditional Chinese medicine, Shashen-Maidong decoction
Introduction
Since the onset of the COVID-19 pandemic, hundreds of millions of individuals worldwide have been infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1,2 The gravity of the pandemic was intensified by the global emergence of the sub-variant B.1.1.529 (omicron) in 2022.3 The omicron strain is characterized by over 50 mutations and distinct amino acid changes in the spike proteins, thereby posing a substantial risk to elderly patients with pre-existing systemic conditions.4,5
Following the shift in the outbreak control policy in China in December 2022, a surge in infections caused by the omicron strain was observed within mainland China.6,7 Hospitals and nursing institutions for the elderly faced significant challenges due to the rising number of patients, leading to a temporary shortage of antiviral drugs. In response to this situation, numerous healthcare professionals in hospitals and nursing institutions for the elderly prescribed traditional Chinese medicine (TCM) to alleviate the symptoms of their elderly patients, following the guidelines set forth by the China Healthcare Commission.8
Shashen-Maidong decoction (SMD) is one of the frequently utilized Chinese herbal formulas in addressing the qi deficiency and yin deficiency of lung and spleen resulting from COVID-19.9,10 This specific syndrome, characterized by the deficiency of qi and yin in the lung and spleen due to COVID-19, is notably prevalent among elderly and pediatric patients. Accordingly, SMD has been endorsed by the Chinese Health Commission in the diagnostic and treatment protocol for COVID-19.8 Although clinical studies of Chinese herbs, including SMD, for the treatment of COVID-19 have been carried out widely in China,11,12 the safety and efficacy of SMD in patients older than 85 years have not been studied to date.
Hence, we conducted a retrospective analysis to assess the safety and efficacy of SMD in patients aged over 85 years diagnosed with COVID-19. This analysis focused on individuals who received SMD in combination with Western medicine and were admitted to the geriatric department of Zhejiang Provincial People’s Hospital between December 2022 and January 2023. The department primarily caters to elderly patients with chronic ailments who require extended hospitalization for specialized care. These patients were admitted to the hospital before their COVID-19 diagnosis and remained hospitalized for ongoing observation and treatment in the same department following the infection.
Materials and Study Methods
Study Participants
Patients diagnosed with COVID-19 infection at the geriatrics department of Wangjiangshan branch of Zhejiang Provincial People’s Hospital from December 10, 2022 to December 31, 2022 were selected in this study. This institution predominantly admits elderly patients in need of prolonged hospitalization.
The study protocol was reviewed and approved by the Ethics Committee of Zhejiang Provincial People’s Hospital (Ethics No. QT2023176).
Inclusion Criteria
Patients with the following conditions were included: a) unvaccinated elderly patients with COVID-19 infection older than 85 years of age; b) patients who presented with clinical symptoms such as fever, cough, and sore throat during hospitalization and had tested positive in the nucleic acid test (a Ct value greater than 35 of SARS-CoV-2 nucleic acid for nucleocapsid protein (N) and open reading frame 1ab (ORF1ab) genes in polymerase chain reaction (PCR)).
Exclusion Criteria
Patients with the following conditions were excluded: a) patients with severe underlying systemic diseases; b) patients with severe psychiatric illnesses or a history of similar psychiatric episodes; c) patients who had received other herbal medications within 2 weeks; d) patients with severe hepatic and renal insufficiency.
Study Design
Based on the disease’s severity, all patients were provided with fundamental Western medical treatments, encompassing oxygen support, antiviral medications (Paxlovid and Azvudine tablets), antibiotics, anticoagulants, glucocorticoids, and nutritional support throughout the observation period. In the SMD+WM group (SMD combined with Western medicine), we included patients who received SMD within three days of infection and continued the therapy for over a week. Meanwhile, in the WM group, we selected patients who solely received basic Western medical treatments. The specific ingredients and dosage of SMD are shown in Table 1. To ensure quality control, all procedures from raw material procurement to processing were conducted by the Decoction Service Center of Huadong Medicine Co., Ltd. After decoction of the herbs, the suspension was packed into sterilized, sealed bags, each containing one dose (100 mol). Qualified nurses were present to administer and guide patients during each treatment session. The patient recruitment process is illustrated in Figure 1.
 |
Table 1 Composition of Shashen-Maidong Decoction |
 |
Figure 1 Patient recruitment flow diagram. |
Outcome Measures
We collected comprehensive patient data, including general information, clinical characteristics, prescribed medications, and results from blood laboratory tests. The primary outcomes studied encompassed the duration for the nucleic acid test to turn negative, duration of intensive care unit (ICU) stay, and mortality rate. Additionally, secondary outcome measures included the use of high-flow nasal cannula (HFNC) oxygen, performance of endo-tracheal intubation, and changes observed in laboratory test results. The laboratory testing included routine blood tests (white blood cell (WBC) count, lymphocyte (LYM) count, neutrophil (NEUT) count, hemoglobin, platelet count), inflammatory factors (C-reactive protein (CRP), pro-calcitonin, PCT), hepatic and renal function (glutamic-pyruvic transaminase, urea nitrogen, creatinine, total amylase), and cardiac function (cardiac troponin I (cTnI), B-type natriuretic peptide (BNP), and left ventricular ejection fraction (LVEF)). The safety endpoint aimed to evaluate adverse events occurring during the patients’ hospital stay. These events pertain to unexpected medical incidents arising during the course of treatment administration. Researchers meticulously assessed the patients’ vital signs and diligently documented any adverse events observed during their hospital stay.
Statistical Analysis
Parametric distribution of variables are represented by mean ± standard deviation, non-parametric distribution variables are represented by median or quartile, and enumeration data are represented by quantity and proportion. Comparisons of data between groups were made using the independent samples of Wilcoxon test, t-test, or chi-squared test. The paired-samples of Wilcoxon test, t-test, or McNemar test were used for pair wise comparisons. A statistically significant difference was considered when P < 0.05. Statistical analysis was performed using SPSS version 23.0 (IBM, USA).
Results
Data at Baseline
Between December 10th and December 31st, 2022, a total of 70 patients initially met the study criteria. However, 2 patients were excluded due to severe underlying systemic diseases (one with cancer and one with intestinal obstruction), and an additional 6 patients were excluded as they had taken other herbal preparations within the two weeks prior. Consequently, 62 patients with confirmed COVID-19 infection were included in this retrospective study.
As indicated in Table 2, no statistically significant differences were observed between the groups concerning general information, underlying diseases, and clinical characteristics. Additionally, there were no significant disparities in the usage of antibiotics, hormones, and anticoagulants during the observation period between the two groups. Regarding the utilization of antiviral drugs, in theory, nearly all enrolled patients qualified for these medications. However, due to the scarcity of antiviral drugs, including Paxlovid and Azvudine tablets, only 25 patients (40.3%) received antiviral treatment during the observation period. Overall, there was no statistically significant difference in drug usage, including antiviral drugs, between the two groups.
 |
Table 2 Baseline Values of the Patients |
Regarding laboratory indicators, it was observed that while the baseline values of CRP and PCT were comparatively higher in the SMD+WM group than in the WM group, these differences did not reach statistical significance. Moreover, no significant disparities were found between the two groups in the laboratory indexes related to heart, liver, and kidney functions. Further details can be found in Table 3.
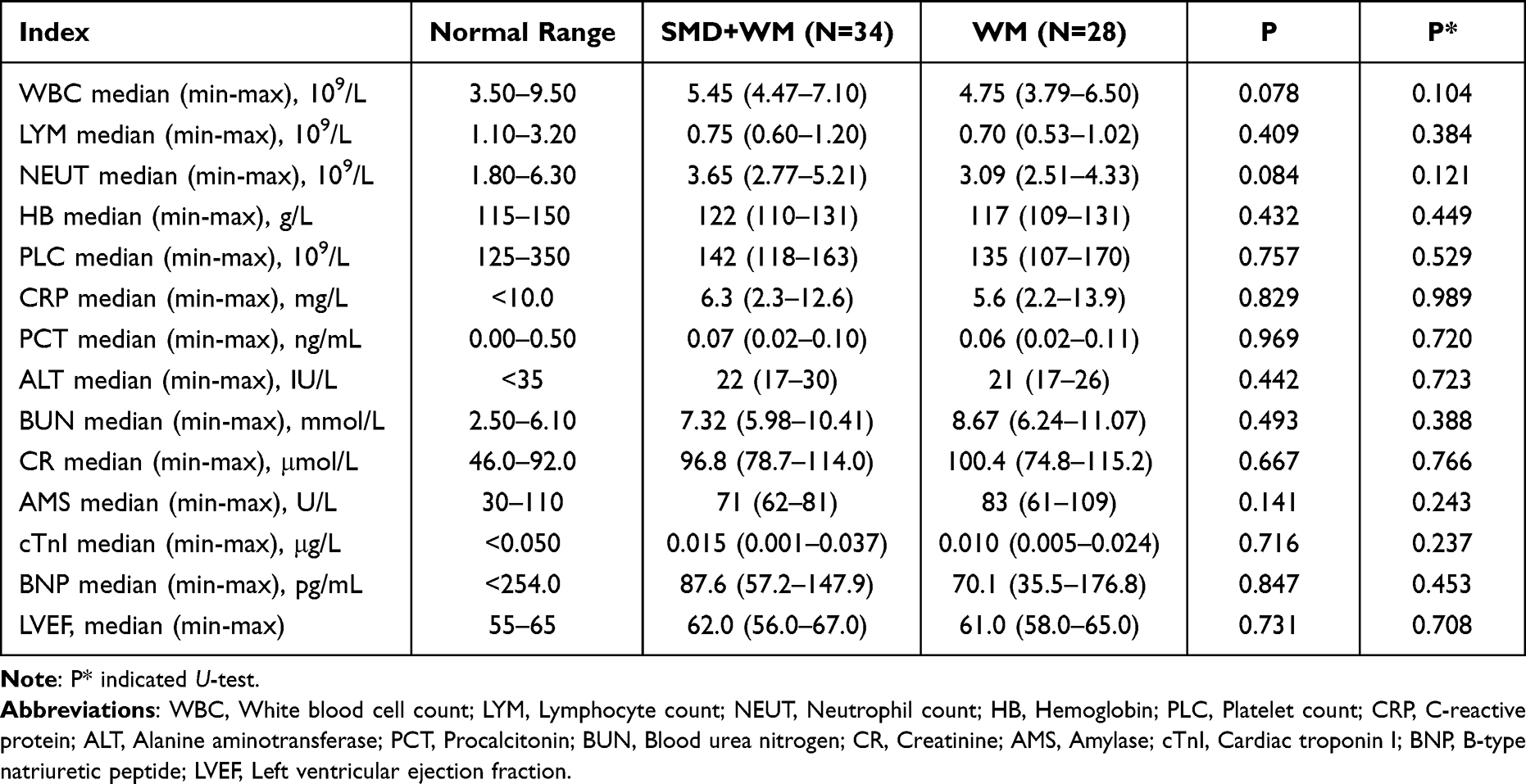 |
Table 3 Baseline Laboratory Parameters of the Patients |
Outcomes
The median duration for nucleic acid tests to turn negative in the SMD+WM group was 18 days, compared to 19 days in the WM group, indicating no statistically significant difference between the two groups. Additionally, 7 patients in the WM group were admitted to the ICU for treatment, and 5 patients in this group succumbed to the illness. In the SMD+WM group, 2 patients were transferred to the ICU during their hospital stay, and 3 patients in this group passed away. However, these differences were not statistically significant either.
Moreover, there were no statistically significant differences observed between the two groups concerning the usage of HFNC oxygen and tracheal intubation, as outlined in Table 4. Three months post-observation period, we conducted follow-up assessments with the surviving patients. It was noted that 11 patients (35.5%) in the SMD+WM group experienced recurrent respiratory infections post-recovery (manifesting respiratory symptoms and receiving antibiotics), while 14 patients (58.3%) in the WM group faced similar complications. However, the disparity in this indicator between the two groups did not reach statistical significance, as shown in Table 4.
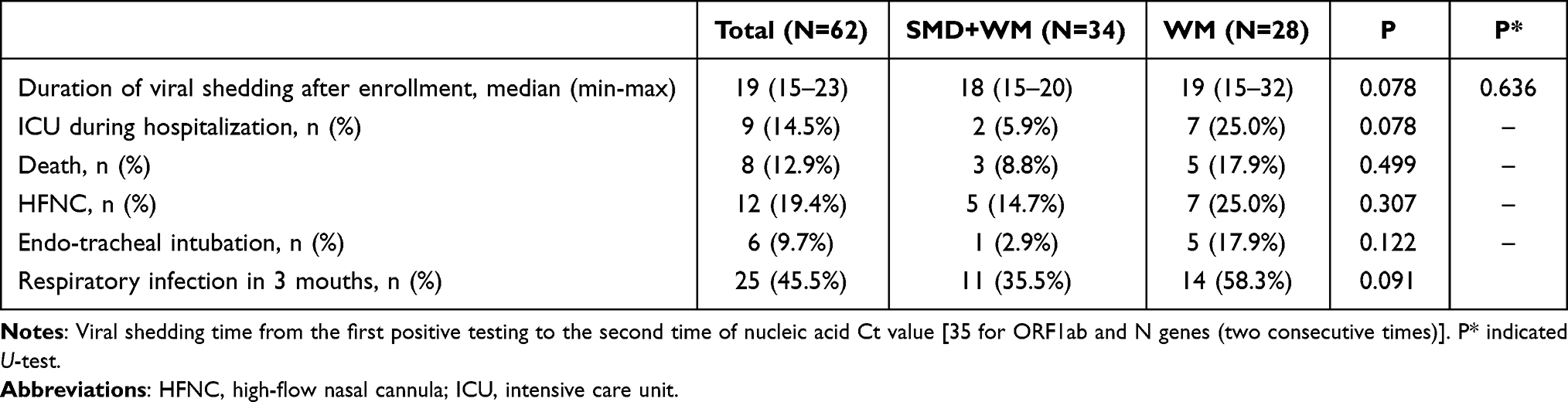 |
Table 4 Comparison of Clinically Observed Indicators |
Comparison of Laboratory Indicators
To elucidate the variation rate in laboratory indicators between the two groups, we calculated the percentage change (corrected value/baseline × 100%). When comparing the laboratory indicators between baseline and week 2 from the date of enrollment, the results revealed that the variation rates of WBC, NEUT, cTnI, and BNP were significantly different between the two groups (P < 0.05). Among these indicators, both the WBC and NEUT values increased from baseline in both groups. However, the SMD+WM group exhibited a lower variation rate in WBC and NEUT values compared to the WM group. Conversely, the cTnI and BNP values increased more from baseline in the WM group, while the SMD+WM group showed a slight decrease. The variation rates of the remaining indicators did not show statistically significant differences between the two groups. For detailed information, please refer to Table 5 and Figure 2.
 |
Table 5 The Variation Rate Difference at Week 2, at Baseline, and at Week 1 |
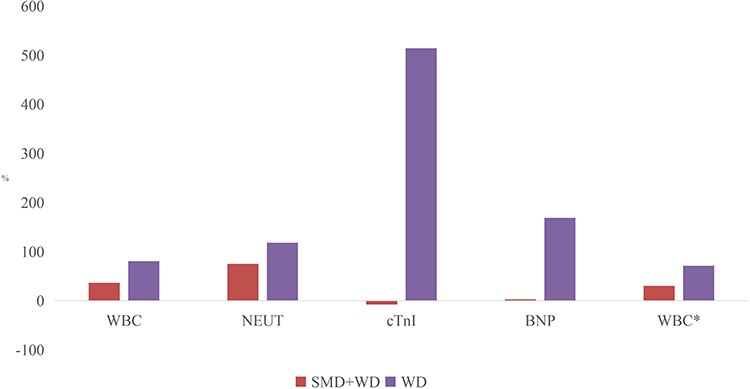 |
Figure 2 Variation rate at week 2 compared to the baseline and week 1 (Only laboratory indicators with significant differences between groups are listed). *Comparison of the variation rate between week 2 and week 1. Abbreviations: ICU, intensive care unit; WBC, White blood cell count; NEUT, Neutrophil count; cTnI, Cardiac troponin I; BNP, B-type natriuretic peptide. |
It is important to note that since all patients were hospitalized and received laboratory tests shortly after the onset of their symptoms, it is possible that there was a gradual elevation of laboratory indicators, including WBC and inflammatory factors, over the course of their hospital stay. Hence, we analyzed the differences in laboratory indicators at both week 1 and week 2 from the time of enrollment. The outcomes revealed that only the variation rate of the white blood cell count (WBC) indicator exhibited a significant difference between the two groups (P < 0.05). Notably, the increase in the SMD+WM group was significantly lower than that in the WM group, as depicted in Figure 1. In contrast, no statistically significant differences were observed between the two groups in the variation rates of the remaining laboratory indicators, as detailed in Table 5.
Additionally, our analysis revealed a significant decrease in CRP levels in the SMD+WM group between week 1 and week 2, a trend that was not observed in the WD group. Further details can be found in the Supplementary Materials, Supplement Tables 1 and 2.
Discussion
Elderly individuals above the age of 60 are more vulnerable to COVID-19, and those aged over 85 face a significantly higher risk of mortality. In contrast to treatment with Western medicine alone, the combination of SMD with Western medicine demonstrates a notable reduction in WBC, particularly in NEUT, among elderly patients afflicted with COVID-19. Moreover, this combination therapy exhibits a protective effect on cardiac function in this demographic.
Patients infected with COVID-19 may experience a robust immune response, potentially leading to the development of inflammatory storms. In critically ill patients, levels of inflammatory cytokines tend to be elevated.13 According to a study, when TCM is used as an adjunctive therapy to Western medicine, the WBC (especially LYM) of the patients with COVID-19 infection demonstrates a more substantial improvement.14 This combined approach can alleviate the symptoms of the patients and reduce lung inflammation.11 In our study, we noted that the combination of SMD with Western medicine exhibited a considerable advantage over Western medicine alone in improving WBC and CRP values, leading to reduced inflammatory levels in patients. One potential mechanism involved the reduction of serum levels of pro-inflammatory cytokines such as TNF-α, IL-6, and IL-4.15,16 However, the specific mechanisms behind these effects may require further investigation for a comprehensive understanding.
The utilization of TCM as an emergency treatment strategy has sparked controversy in China since 2020. According to TCM theory, elderly individuals are more susceptible to deficiencies in both qi and yin. Therefore, SMD is recommended as an adjunctive medicine in this age group.9,10,17–19 Previous studies have indicated that TCM may lead to lung damage and interstitial pneumonia, potentially causing more harm than benefit to patients with COVID-19 infection. Additionally, the effects of TCM on hepatic and renal function remain a topic of debate.20,21 Elderly patients often have multiple comorbidities, increasing their risk of developing severe illness and facing a higher mortality rate. Consequently, there are stringent safety requirements for the use of drugs in this demographic. Scutellariae Radix, also known as Skullcap or ou-gon, has been associated with lung injury and was not included in SMD.21 Therefore, we lack a reference for its potential effects in this context. Nevertheless, in the combined treatment group, there were no significant differences observed in the changes of hepatic and renal function indicators when compared to the Western medicine group. This suggests a potential protective effect on cardiac function. To clarify, although changes in cTnI and BNP supported this conclusion, there was no significant difference observed in LVEF changes between the groups. Furthermore, no unforeseen medical events were reported in either group. Consequently, we posit that the treatment regimen involving the combination of SMD with Western medicine appears to be safe in terms of cardiac, hepatic, and renal functions.
In certain prior studies, it was noted that the combination of Chinese herbs may significantly lower the risks of intubation, ICU admission, and death in patients with mild to severe COVID-19 infections.22,23 However, our findings did not yield sufficient evidence to support these observations. Additionally, there were no significant differences observed in the duration for nucleic acid test turning to negative and the risk of recurrent respiratory tract infections within three months between the two groups. This contradicts findings from previous studies with similar objectives.24–27 This discrepancy could be attributed to the relatively small sample size in our study, as well as variations in the dosage, type, and dosing cycle of the Chinese medicines administered. Further investigation is warranted to delve into these aspects in greater detail.
In our study, we observed that the utilization of complementary medicine, such as herbal medicine, inherently exerts a placebo effect on patients, thereby alleviating their psychological anxiety to a certain extent.28 Due to legal constraints and ethical considerations, our study could not include patients who were placebo-treated and blinded. To mitigate the influence of the placebo effect, we opted to analyze objective laboratory and clinical observation indicators statistically.
The primary aim of this study is to offer a potential therapeutic approach for treating elderly patients with COVID-19 infection, particularly in situations where there is limited availability of antiviral drugs. Additionally, this study can serve as a reference point regarding the safety of TCM in the context of COVID-19 treatment. Nonetheless, our study has certain limitations, including a relatively small sample size, which necessitates validation through larger-scale studies. Additionally, we faced constraints that prevented us from acquiring complete long-term laboratory test results of patients, and the observation period was relatively short. Furthermore, the study was limited by the availability and types of antiviral drugs, making it unfeasible to conduct a randomized controlled trial. Additionally, owing to constraints within the original data, we were unable to include respiratory measures such as cough, SaO2, or other relevant indicators. Moreover, we could not differentiate between lung injuries induced by medication and those caused directly by COVID-19. It is important to note that there might have been significant variations in the clinical status of patients at the outset of the study, despite our efforts to analyze general information, underlying diseases, and clinical characteristics. Furthermore, despite our best efforts to rely on objectively recorded data for laboratory indicators in our analysis, potential biases may exist due to the retrospective nature of our study.
Conclusion
In summary, our findings indicate that the combination of SMD with Western medicine significantly mitigated the increase in WBC, especially NEUT, in elderly patients with COVID-19 infection when compared to treatment with Western medicine alone. Additionally, this combined treatment approach appeared to have a protective effect on cardiac function. Moreover, the regimen involving SMD combined with Western medicine demonstrated potential safety in our study.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author (Wei-Shang Hu).
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by Ethics Committee of the Zhejiang Provincial People’s Hospital (No. QT2023176). Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Ross JA, Malone PK, Levy S. The impact of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic on substance use in the United States. Clin Infect Dis. 2022;75(Supplement_1):S81–S85. doi:10.1093/cid/ciac311
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
3. Vitiello A, Ferrara F, Auti AM, Di Domenico M, Boccellino M. Advances in the omicron variant development. J Intern Med. 2022;292(1):81–90. doi:10.1111/joim.13478
4. Chavda VP, Apostolopoulos V. Omicron variant (B.1.1.529) of SARS-CoV-2: threat for the elderly? Maturitas. 2022;158:78–81. doi:10.1016/j.maturitas.2022.01.011
5. Peng Y, Guo Y, Zhang H, et al. Clinical characteristics and analysis of risk factors for disease progression of patients with SARS-CoV-2 omicron variant infection: a retrospective study of 25,207 cases in a Fangcang hospital. Front Cell Infect Microbiol. 2022;12:1009894. doi:10.3389/fcimb.2022.1009894
6. Bai Y, Shao Z, Zhang X, et al. Reproduction number of SARS-CoV-2 omicron variants, China, December 2022-January 2023. arXiv preprint arXiv. 2023;2303:10642.
7. Cai C, Li Y, Hu T, et al. The associated factors of SARS-CoV-2 reinfection by omicron variant—Guangdong Province, China, December 2022 to January 2023. China CDC Weekly. 2023;5(18):391–392. doi:10.46234/ccdcw2023.075
8. National Health Commission of the People’s Republic of China. Novel coronavirus pneumonia diagnosis and treatment plan (provisional 10th ed); 2023. Available from: https://www.gov.cn/zhengce/zhengceku/2023-01/06/5735343/files/5844ce04246b431dbd322d8ba10afb48.pdf.
9. Duan N, Liu B, Li X, et al. Traditional Chinese medicine in treating children with coronavirus disease 2019: a scoping review. Front Pediatr. 2022;10:935551. doi:10.3389/fped.2022.935551
10. Ni L, Chen L, Huang X, et al. Combating COVID-19 with integrated traditional Chinese and Western medicine in China. Acta Pharmaceutica Sinica B. 2020;10(7):1149–1162. doi:10.1016/j.apsb.2020.06.008
11. Xin S, Cheng X, Zhu B, et al. Clinical retrospective study on the efficacy of Qingfei Paidu decoction combined with Western medicine for COVID-19 treatment. Biomed Pharmacother. 2020;129:110500. doi:10.1016/j.biopha.2020.110500
12. Feng C, Wenlin Y, Qiangyong K, et al. Clinical efficacy of combination therapy of FuXi-Tiandi-Wuxing decoction and anti-viral drugs in the treatment of novel coronavirus pneumonia: a prospective interventional study. J Herb Med. 2023;38:100627. doi:10.1016/j.hermed.2022.100627
13. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
14. Xiong WZ, Wang G, Du J, Ai W. Efficacy of herbal medicine (Xuanfei Baidu decoction) combined with conventional drug in treating COVID-19: a pilot randomized clinical trial. Integr Med Res. 2020;9(3):100489. doi:10.1016/j.imr.2020.100489
15. He M, Luo Y, Chen L, et al. Shashen maidong decoction: the effect of TNF-α and IL-6 on lung cancer cachexia based on cancer toxicity theory. Am J Transl Res. 2021;13(6):6752.
16. Yang Y, Zhou Y. Shashen-maidong decoction-mediated IFN-γ and IL-4 on the regulation of Th1/Th2 imbalance in RP rats. Biomed Res Int. 2019;2019:1.
17. Hu CS. Analysis of COVID-19 cases and public measures in China. SN Compr Clin Med. 2020;2:1306–1312. doi:10.1007/s42399-020-00426-6
18. Hu CS. Emergency protective measures and strategies of COVID-19: from lifestyle to traditional Chinese medicine. Clin Compl Med Pharmacol. 2023;3(3):2772–3712. doi:10.1016/j.ccmp.2023.100089
19. Shi SF, Fang ZY, Xiong K, et al. Clinical studies of comprehensive TCM treatment to 30 cases of Qi Yin deficiency type of COVID-19 in its recovery period. Jiangsu J Tradit Chin Med. 2021;53(1):4.
20. Gray PE, Belessis Y. The use of traditional Chinese medicines to treat SARS-CoV-2 may cause more harm than good. Pharmacol Res. 2020;156:104776. doi:10.1016/j.phrs.2020.104776
21. Wang Y, Gao D, Li X, et al. Early changes in laboratory tests predict liver function damage in patients with moderate coronavirus disease 2019: a retrospective multicenter study. BMC Gastroenterol. 2022;22(1):113. doi:10.1186/s12876-022-02188-y
22. Tseng YH, Lin SJ, Hou SM, et al. Curbing COVID-19 progression and mortality with traditional Chinese medicine among hospitalized patients with COVID-19: a propensity score-matched analysis. Pharmacol Res. 2022;184:106412. doi:10.1016/j.phrs.2022.106412
23. Yao CL, Wei WL, Zhang JQ, et al. Traditional Chinese medicines against COVID-19: a global overview. World J Tradit Chin Med. 2022;8:279–313. doi:10.4103/2311-8571.353502
24. Li L, Xie H, Wang L, et al. The efficacy and safety of combined Chinese herbal medicine and Western medicine therapy for COVID-19: a systematic review and meta-analysis. Chin Med. 2022;17(1):77. doi:10.1186/s13020-022-00600-z
25. Song ZJ, Nik Nabil WN, Xi ZC, Xu HX. Current global status and future development of traditional Chinese medicine in the prevention and treatment of coronavirus disease 2019. World J Tradit Chin Med. 2021;7:155–166.
26. Li MX, Yang YY, Liu Y, et al. Progress of traditional Chinese medicine treating COVID-19. World J Tradit Chin Med. 2021;7:167–183.
27. Yu R, Zhang S, Zhao D, Yuan Z. A systematic review of outcomes in COVID-19 patients treated with Western medicine in combination with traditional Chinese medicine versus Western medicine alone. Expert Rev Mol Med. 2022;24:e5. doi:10.1017/erm.2021.35
28. Dehghan M, Ghanbari A, Heidari FG, Shahrbabaki PM, Zakeri MA. Use of complementary and alternative medicine in general population during COVID-19 outbreak: a survey in Iran. J Integr Med. 2022;20(1):45–51. doi:10.1016/j.joim.2021.11.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.