Back to Journals » Journal of Pain Research » Volume 15
The Effects of Resistin Gene Polymorphism on Pain Thresholds and Postoperative Sufentanil Consumption in Gastric Cancer Patients
Authors Li J, Li S ![]() , Yu L
, Yu L ![]() , Wei J, Li S, Tan H
, Wei J, Li S, Tan H
Received 29 April 2022
Accepted for publication 6 July 2022
Published 17 July 2022 Volume 2022:15 Pages 1995—2004
DOI https://doi.org/10.2147/JPR.S372845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qi Fang
Jianing Li, Shuo Li, Ling Yu, Jin Wei, Shuang Li, Hongyu Tan
Department of Anesthesiology, Peking University Cancer Hospital & Institute, Beijing, People’s Republic of China
Correspondence: Hongyu Tan, Department of Anesthesiology, Peking University Cancer Hospital & Institute, Beijing, People’s Republic of China, Tel +86-10-88196107, Email [email protected]
Purpose: As an adipocyte-secreted hormone, resistin is linked to inflammation, insulin resistance and atherosclerosis. Currently, resistin is proposed as a novel biomarker for postoperative pain intensity. However, due to the various types of surgery and limited numbers of studies, previous conclusions should be validated. This study aimed to explore the effect of resistin polymorphism (rs3745367) on pain thresholds and sufentanil consumption in gastric cancer patients.
Patients and Methods: A total of 148 gastric cancer patients enrolled in this study had their pain thresholds measured before surgery. After the exclusion of 16 patients, the characteristics of demography and clinic, numerical rating scale (NRS) and sufentanil consumption of 132 patients were recorded. Rs3745367 of resistin was identified by Sanger sequencing. Multivariate linear regression analysis was performed for sufentanil consumption and mechanical pain threshold.
Results: The distributions of the GG, AG, and AA genotypes of rs3745367 among the participants were 54 (40.9%), 65 (49.2%), and 13 (9.9%), respectively. The mechanical pain threshold (P=0.04) and postoperative sufentanil consumption in the 1st 24 h (P=0.03) were significantly different among GG, AG, and AA genotype carriers. There was no significant difference among the three genotypes for the heat pain threshold and cold pain threshold. Regarding the NRS, no statistically significant difference among the three different genotypes was found 24 h postoperatively.
Conclusion: Rs3745367 of resistin is associated with the mechanical pain threshold and postoperative sufentanil consumption in gastric cancer patients. Patients with the AA genotype of rs3745367 present an increased mechanical pain threshold and decreased postoperative sufentanil consumption.
Keywords: gene polymorphism, pain threshold, postoperative pain, resistin, sufentanil consumption
Introduction
How to control acute postoperative pain is a vital global health issue concerning patients’ postoperative rehabilitation and quality of life and is worthy of more in-depth studies.1–3 In clinical practice, opioids still play an irreplaceable role in relieving acute pain after surgery.4,5 Patients have different perceptions of acute pain and discrepant responses to opioids, which are influenced by various non-genetic factors, including age, sex, body mass index (BMI), type of surgery and American Society of Anesthesiologists (ASA) grade.6–8 In addition to non-genetic factors, several gene polymorphisms that are associated with acute pain and opioid consumption after surgery have been identified.9–12
Resistin is a secretory protein from adipose tissue that has a conserved and high-order multimeric structure in rodents and humans.13,14 Mouse resistin has pleiotropic effects on metabolism, obesity and diabetes.13 The content of resistin is elevated in obese mice, and injection of resistin has an influence on insulin resistance in normal mice.15 Moreover, deletion of the resistin gene in mice fed a high-fat diet increases insulin sensitivity and decreases the levels of serum cholesterol and low-density lipoprotein.16,17 The main physiological function of human resistin is to act as an inflammatory regulator, targeting macrophages, peripheral blood mononuclear cells and vascular cells.18,19 Furthermore, human resistin stimulates these cells to produce proinflammatory cytokines, including interleukin-6, interleukin-12 and monocyte chemoattractant protein 1.13 Human resistin is also involved in insulin resistance and endoplasmic reticulum stress progression.13 It can act as a molecular chaperone to protect other proteins and restore their functional activity.20 In addition, several polymorphisms of resistin are associated with pathological processes, including acute ischemic stroke, multiple sclerosis and atopic dermatitis.21–23
Surgical trauma can stimulate the immune response, producing cytokines to promote wound repair.24 However, an exaggerated response can result in immunosuppression and have an adverse effect on patient recovery.25 As a cytokine, human resistin is newly reported acting as a novel biomarker for postoperative pain intensity, which may influence the recovery of patients.26 Human resistin is located on chromosome 19p13.2 and spans 1369 bp.27 Currently, it has been reported that among three identified single nucleotide polymorphisms (rs7408174, rs3219175, rs3745367), the rs3745367 gene polymorphism of resistin is associated with postoperative pain.26 Rs3745367 is located on chromosome 19 (7,669,625) and can be classified into AA, AG and GG genotypes.26 Previous studies showed that the NRS score of patients with minor homozygosity (AA) is lower than that of patients with major homozygosity (GG) for rs3745367 of resistin after surgery.26,28 To date, only a few studies have explored the relationship between gene polymorphisms of resistin and postoperative pain in limited populations.
Whether rs3745367 can be regarded as a novel biomarker of pain phenotypes needs more exploration in different cohorts. In this study, we explored the association of resistin (rs3745367) with pain thresholds and sufentanil consumption after surgery in gastric cancer patients. Moreover, multivariate linear regression analysis was also performed. Our study, together with others, deepens the understanding of the relationship of resistin with postoperative pain, which may help clinicians personalize analgesia.
Materials and Methods
Patients
The present investigation was approved by the Ethics Committee of Peking University Cancer Hospital & Institute (2021KT66). Participants with the following criteria were included: aged 18–80 years, ASA physical status of I to III and underwent radical surgery for gastric cancer. Participants with the following diagnoses were excluded: mental illness, drugs for psychiatric disorders and analgesics, tumor recurrence and chronic pain. A total of 148 Chinese adult patients who met the inclusion criteria and did not conform the exclusion criteria were enrolled in this study. They underwent radical surgery for gastric cancer at the Peking University Cancer Hospital in 2021. Patients with hypertension and diabetes got preoperative therapy and parts of patients received chemotherapy before surgery. Participants signed their informed consent before the trial.
Determination of the Pain Threshold
“Pain threshold” was defined as the time when participants started to feel pain. We conventionally measured the pain threshold of participants for one day prior to radical surgery in gastric cancer, including the cold pain threshold, heat pain threshold and pressure pain threshold. Patients placed their nondominant hand in a water bath (4 °C± 0.5 °C), and the cold pain threshold of patients was measured by using a temperature-controlled cold-water bath (TAWA Q-18, China). By using a heat plate (YOONING GH-100, China), patients placed the thenar eminence of their nondominant hand on the hot plate (47.5 °C ± 0.1 °C) to measure the heat pain threshold. In addition, a mechanical pain meter (Wagner, US) was used to measure the mechanical pain threshold. The probe of the pain meter was placed on the index finger and slowly pressurized. When the subject felt pain, the pressurization was stopped. At that time point, the reading on the display was the subject’s pain threshold. The test was repeated three times, and average values were recorded.
Anesthesia and Analgesia
All patients received general anesthesia and underwent radical surgery for gastric cancer. The anesthesia procedure was as follows: (1) propofol (2 mg/kg), sufentanil (0.4 μg/kg) and cisatracurium (0.2 mg/kg) were used to induce general anesthesia; (2) sevoflurane (1%) was used to maintain the anesthesia; and (3) propofol and remifentanil were used throughout the surgery, and other drugs were used if necessary. For postoperative analgesics, an analgesia pump was provided to patients to relieve acute pain. The pump of patient-controlled intravenous analgesia (PCIA) was composed of sufentanil (5 μg/kg), dextromethorphan (100 μg) and tropisetron (30 mg) in 120 mL of 0.9% sodium chloride solution. The background dose of PCIA was 0.5 mL/h, with a 2 mL initial dose and a 1.5 mL bolus dose. For all patients, the limit dose was 13 mL/h, and the lock-in time was 10 min. Morphine was mainly regarded as an agent for rescue analgesia. The sufentanil dosage described in the text included sufentanil from the PCIA pump and morphine (converted into sufentanil), which was used after the operation. The preoperative analgesic preaching and postoperative analgesic measures were carried out to yield an NRS score of less than or equal to 3 using an 11-point scale.
Data Collection
Demographic information, including age, sex, body mass index (BMI), educational level and history of tobacco use and alcohol use, was recorded. Factors associated with surgery, including American Society of Anesthesiologists (ASA) physical status, type and range of radical surgery and operative duration, were collected. The pathological characteristics (adenocarcinoma, signet ring cell carcinoma and adenocarcinoma with signet ring), Tumor, Node, and Metastasis (TNM) stage (I, II, III and IV) and Dukes-MAC-like stage (A1, A2, B1, B2, C1, C2 and D)29 of patients were also collected (Supplementary Table 1). Postoperative data that included sufentanil usage in the first 24 h and NRS scores at 24 h after surgery were recorded. The NRS scores ranged from 0 to 10; a score of 0 meant no pain, and a score of 10 indicated the worst imaginable pain.
Genotype Identified
Blood samples (5 mL) were collected from patients 1 h before surgery, and genomic DNA was isolated by a phenol-chloroform method.30 Polymerase chain reactions were performed to acquire target products using Taq mix (Vazyme, P111-01) through the following primers: rs3745367 (forward: ACCTCACTGATCCCTGGCAC; reverse: ACAGAAATGGGCGCCTGGAC). The PCR procedure was performed as follows: denaturation at 95 °C for 20s, annealing at 50 °C for 30s, extension at 60 °C for 3 min and a total of 30 cycles (Applied Biosystems, US). Products were purified (Applied Biosystems, US) and sequenced by the Sanger sequencing method.
Statistical Analysis
Data were analyzed depending on their type by using GraphPad Prism 8 and IBM SPSS Statistics 27 software. Continuous variables were presented as the median (interquartile range) or as the mean ± standard deviation (SD), depending on their distribution characteristics. The Kruskal–Wallis test or One-way ANOVA was performed among the three groups. Categorical variables were analyzed by Chi-square analysis and presented as percentages (%). The Hardy–Weinberg equilibrium (HWE) of genotypes was tested using Chi-square analysis.
Specifically, BMI, sufentanil consumption, cold pain threshold and mechanical pain threshold were analyzed by One-way ANOVA; age, operative duration, heat pain threshold and NRS were analyzed by the Kruskal–Wallis test; sex, type of procedure and range of radical surgery in gastric cancer were analyzed by Chi-square analysis. The pathological type, TNM stage and Dukes-MAC-like stage were analyzed by Kruskal–Wallis test to examine the correlation between tumor features and gene polymorphism. The difference was considered to be statistically significant when P < 0.05.
Multivariate linear regression analysis was performed for the mechanical pain threshold, with the mechanical pain threshold as the dependent variable. Age, BMI, sex, educational level, history of tobacco use and alcohol use and rs3745367 genotypes were included as independent variables in the model. Multivariate linear regression analysis was also performed for sufentanil consumption, with sufentanil consumption as the dependent variable. Age, BMI, sex, type of procedure, range of radical surgery, history of tobacco use and alcohol use and rs3745367 genotypes were included as independent variables in the model. The sample size was calculated by using the number of risk factors for postoperative sufentanil consumption. The sample size was equal to 10 to 20 times the number of variables; thus 148 patients were enrolled in our study, which met the sample criterion.
Results
Characteristics of the Participants
One hundred forty-eight gastric cancer patients who underwent radical surgery were enrolled in this study. Sixteen patients were excluded due to changes in the type of surgery and anesthesia or due to cancellation of surgery (Figure 1). Statistical analyses were only performed on one hundred thirty-two patients.
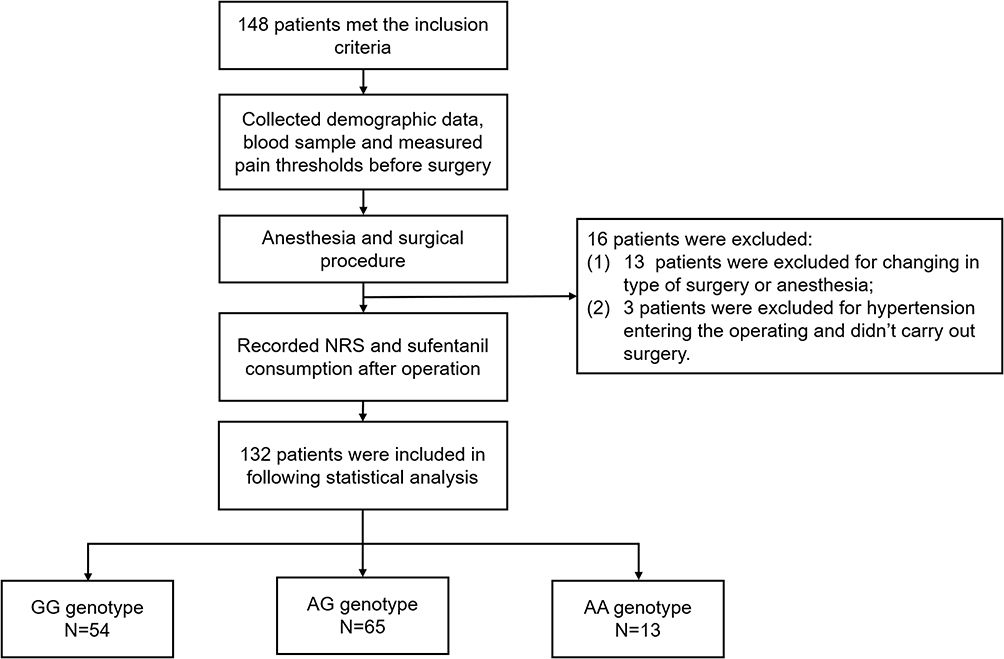 |
Figure 1 The flow chart of this study. Abbreviation: NRS, numerical rating scale. |
In this study, the rs3745367 polymorphism consisted of major homozygous (GG), heterozygous (AG) and minor homozygous (AA) genotypes, with distributions of 54 (40.9%), 65 (49.2%), and 13 (9.9%), respectively (Figure 2, Table 1). The genotype distribution of rs3745367 passed the Hardy–Weinberg equilibrium (P>0.05) test. As shown in Table 1, there were no significant differences in age, sex and BMI, educational level, history of tobacco use and alcohol use, ASA grade, chemotherapy, operative duration, type of procedure or range of radical surgery among the GG, AG and AA genotype groups (Table 1). The association of resistin polymorphism with gastric cancer features were analyzed. The pathological characteristics, TNM stage and Dukes-MAC-like stage of patients were not significantly different among the GG, AG and AA genotype groups (Table 1).
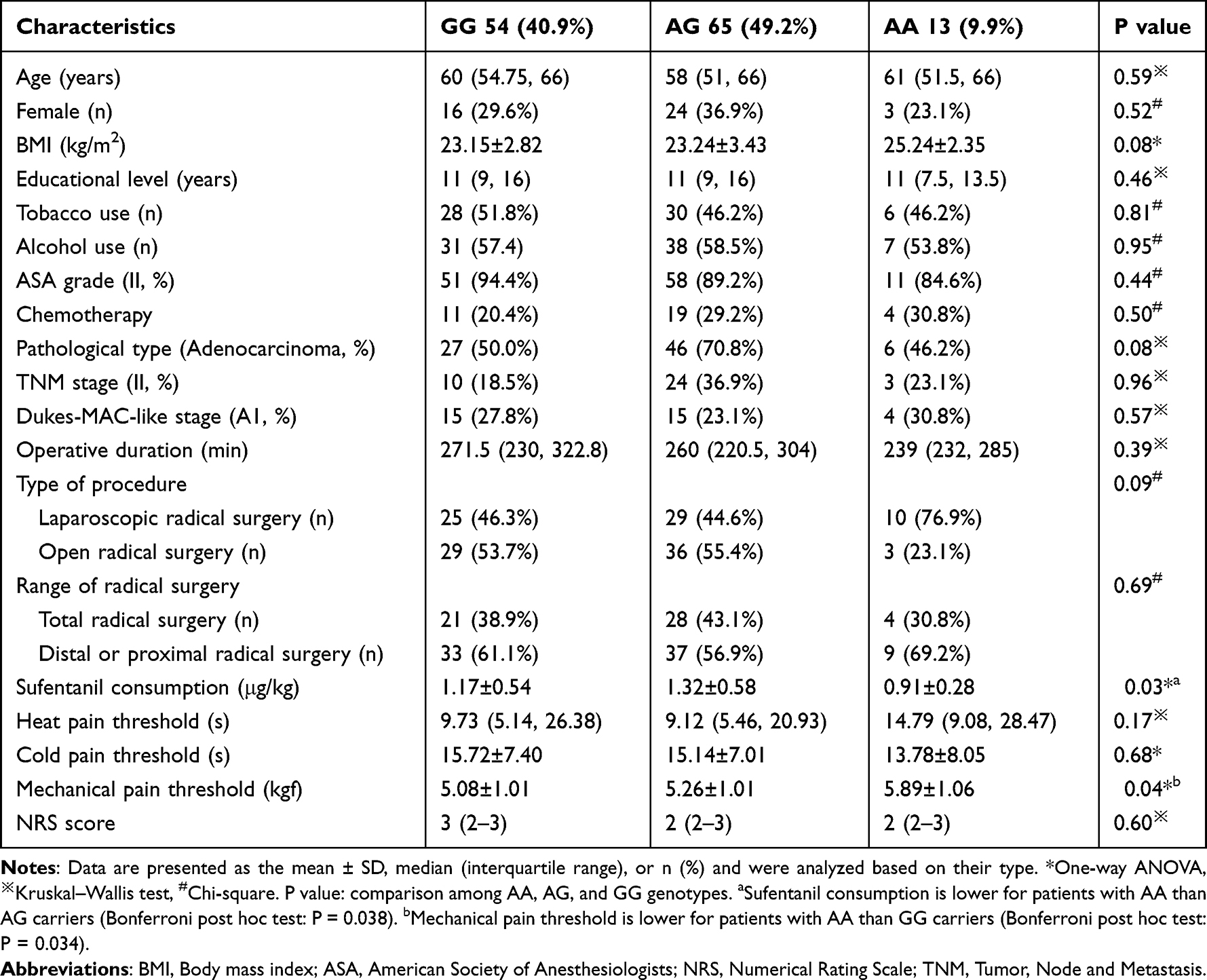 |
Table 1 Subject and Clinical Characteristics |
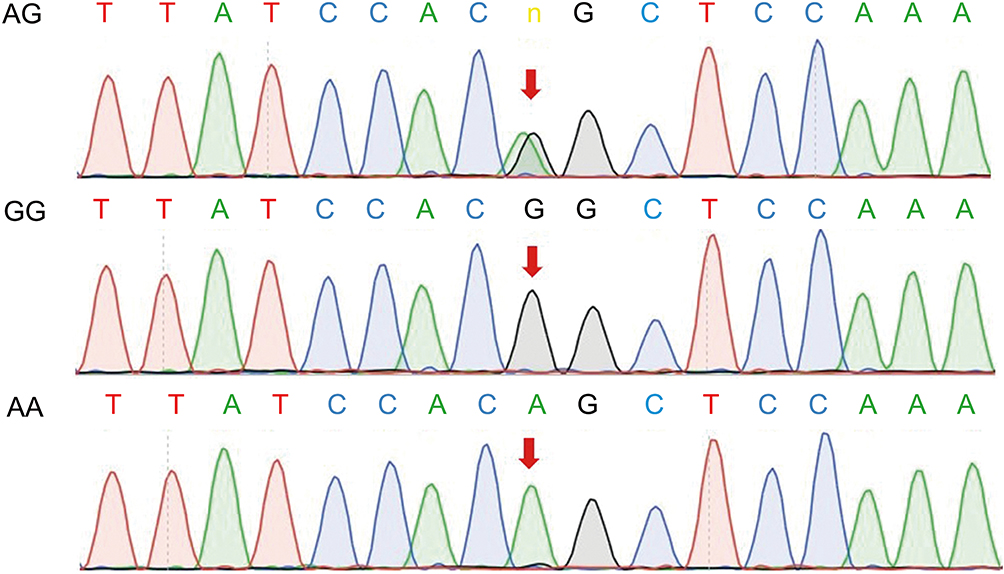 |
Figure 2 Sanger sequence map of AG, GG and AA at the rs3745367 locus in resistin. |
The Association of Resistin Polymorphism with the Pain Threshold
There were no significant differences for the heat pain threshold (Figure 3A) or cold pain threshold (Figure 3B) among the GG, AG and AA genotype groups. The mechanical pain threshold was significantly different among the three genotypes of rs3745367. The mechanical pain thresholds of patients with GG, AG and AA were 5.08 kgf, 5.26 kgf and 5.89 kgf, respectively (Figure 3C). See Table 1 for details.
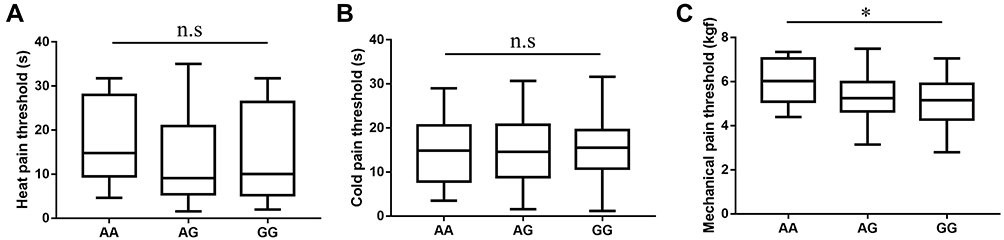 |
Figure 3 The pain thresholds in genotypes of rs3745367 before surgery. (A) The heat pain threshold was not significantly different among the AA, AG and GG genotypes. (B) The cold pain threshold was not significantly different among the AA, AG and GG genotypes. (C) The mechanical pain threshold was significantly different among the three genotypes. *One-way ANOVA, P< 0.05. Abbreviation: n.s, no significance. |
The Association of Resistin Polymorphism with Sufentanil Consumption and the NRS Score
The mean sufentanil consumption of GG, AG and AA carriers were 1.17 μg/kg, 1.32 μg/kg and 0.91 μg/kg, respectively, in the first 24 h after surgery, which were significantly different among the three genotypes of rs3745367 (Table 1, Figure 4). AG carriers consumed more than 45% of AA carriers in postoperative sufentanil consumption. The median NRS score was 2–3, and there was no statistically significant difference among the three different genotypes 24 h postoperatively (Table 1).
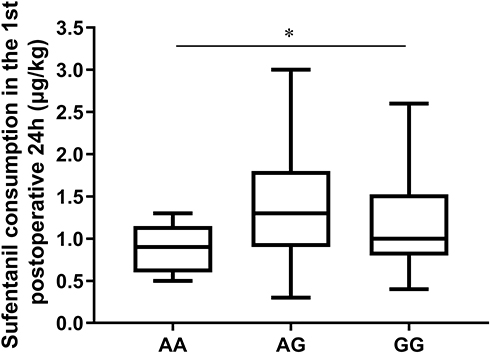 |
Figure 4 The consumption of postoperative sufentanil in genotypes of rs3745367. *One-way ANOVA, P< 0.05. |
Multivariate Analyses of the Mechanical Pain Threshold and Sufentanil Consumption
The results of multivariate linear regression analyses indicated that the rs3745367 polymorphism (AA vs GG, B: 0.684, p=0.026), age (B: −0.019, p=0.022), sex (B: 0.469, p=0.093), and educational level (B: −0.047, p=0.025) were associated with the mechanical pain threshold (Table 2). The rs3745367 polymorphism (AA vs AG, B: −0.313, p=0.064), age (B: −0.009, p=0.045) and BMI (B: −0.038, p=0.015) were associated with sufentanil consumption (Table 3). The R2 of multivariate linear regression (MLR) models for mechanical pain threshold and sufentanil consumption was respectively 0.20 and 0.14.
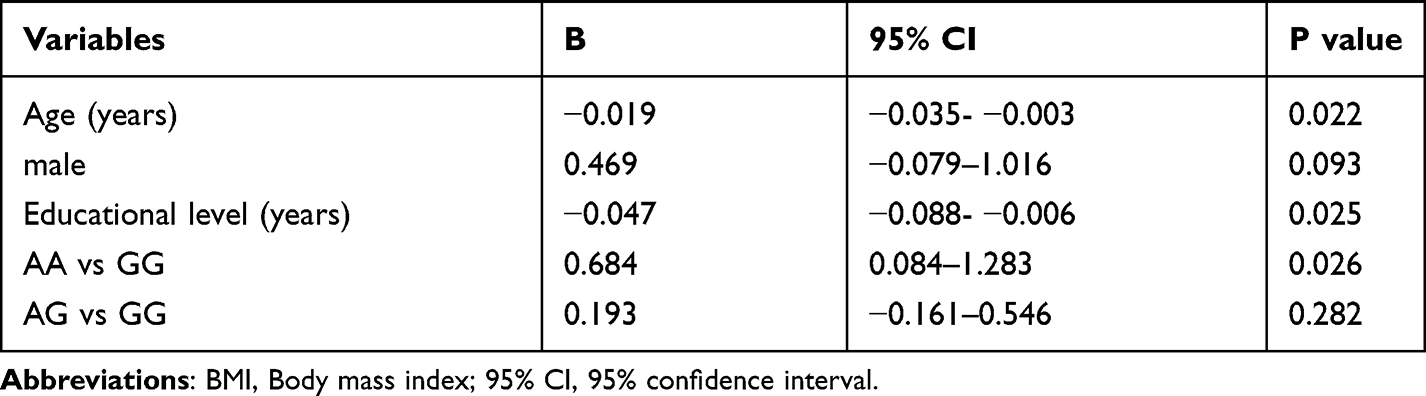 |
Table 2 Multivariate Linear Regression of Risk Factors for the Mechanical Pain Threshold |
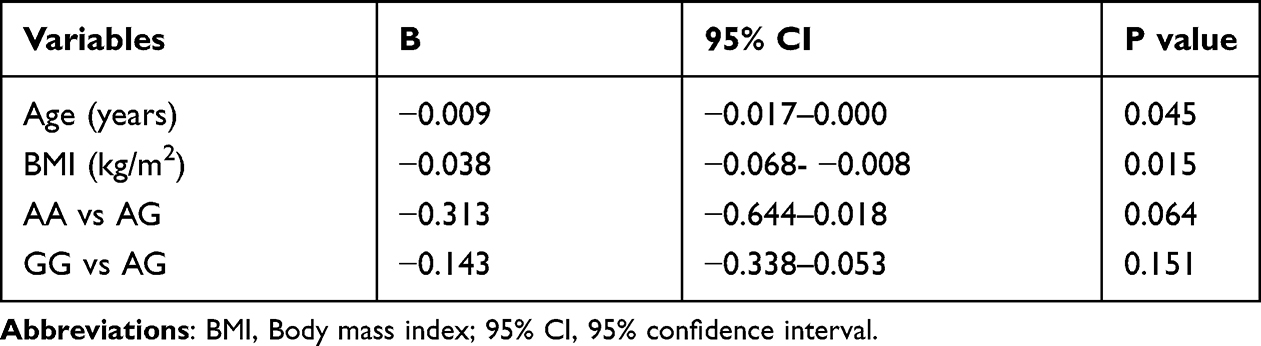 |
Table 3 Multivariate Linear Regression of Risk Factors for Sufentanil Usage in the First Postoperative 24 h |
Discussion
In our study, it was revealed that the distribution of rs3745367 genotypes was 40.9% (GG), 49.2% (AG), and 9.9% (AA) in Chinese people. This is nearly consistent with results from the study of Xie et al, in which the distribution of rs3745367 was 38.0% (GG), 52.1% (AG) and 9.9% (AA) in Chinese people.28 However, a study carried out in Japanese patients showed that the minor allele (A) frequency of rs3745367 was 12%, which was obviously different from that in our study (34%).26 Thus, the difference in the distribution of rs3745367 genotypes may be influenced by race.
Our results indicate that the mechanical pain threshold of AA carriers was higher than that of GG and AG carriers for the rs3745367 polymorphism. The results of multivariate linear regression analysis further confirmed that the resistin polymorphism (AA vs GG) was associated with the mechanical pain threshold. We searched the literature with the keyword “resistin AND pain threshold” in PubMed, and there were no related studies. Here, we found that AG and GG carriers were more sensitive to mechanical stimulation than AA carriers of rs3745367.
We found that only the mechanical pain threshold, but not the heat pain threshold or cold pain threshold, was associated with resistin polymorphisms. Pain thresholds can reflect pain perception in independent individuals.31 Wang et al reported that most small neurons respond to mechanical and thermal stimuli and that most medium and large neurons are mechanosensitive.32 In addition, for thermal stimuli to hind paws in mice, more heat-sensitive neurons are activated via hierarchical coding; however, most cold-sensitive neurons are activated via ungraded coding.32 Our results may be due to the fact that the encoding patterns of mechanical, hot and cold stimuli are not similar.
We also found that younger age, male sex and low educational level were risk factors for a high mechanical pain threshold. A meta-analysis showed that the mechanical pain threshold was lower for old patients than younger patients.33 A previous study reported that compared with men, women generally have a lower pain threshold for mechanical stimulation.34 Our results are consistent with these previous discoveries. Zhang et al indicated that a lower mechanical pain threshold was found among men with a higher level of education.35 In the previous study, we also found that the low education level was associated with a higher mechanical pain threshold in gastric cancer patients,36 which is consistent with this study. Zajacova et al indicated that educational disparities had an influence on pain perception in a large annual cross-sectional survey.37 They also suggest that the educational attainment may influence pain through a combination of socioeconomic, health-behavioral, social, and medical factors.37 Since the mechanical-induced nociceptor correlate with pain perception, the social and medical factors resources may contribute to this result, which still need to deeply study.
Based on prior research, the rs3745367 polymorphism of resistin was associated with postoperative acute pain.26,28 Hozumi et al showed that the NRS mean value of patients with AA genotypes was 2.3 and that AG carriers had the highest NRS score (4.2) at the 24 h postoperative time point using a 5-point Likert scale for open laparotomy for colorectal cancer.26 Another study enrolled 142 patients and revealed that AA carriers of rs3745367 tolerated more postoperative pain at 24 h and 48 h among Chinese patients undergoing spinal correction and fusion.28 In our study, we carried out the suitable preoperative analgesic preaching and administered a sufficient analgesic dosage after surgery to relieve acute pain in patients. The NRS score of most patients (92.6%) was less than or equal to 3 using a 10-point scale by PCIA, which indicated that the patients received a suitable analgesic dose. Therefore, there was no significant difference in NRS at 24 h postoperatively.
In this study, the postoperative analgesic dosage (sufentanil of the PCIA pump and morphine) was recorded, which could indirectly reflect the postoperative pain intensity. We found that AA carriers of rs3745367 consumed the minimum amount of sufentanil in the first postoperative 24 h compared with other genotypes, suggesting that AA carriers may experience less acute pain. Although the study of Hozumi et al showed that the total daily dosages of opioid analgesics, including intraoperative fentanyl and postoperative opioids, were not significantly different among three genotypes of rs3745367, patients with AA genotypes showed lower pain sensitivity, which was consistent with the study of Xie et al.26 Similarly, our study also demonstrated that AA carriers have a lower pain sensitivity than AG and GG carriers of rs3745367.
Our study indicated that age and BMI were negatively associated with sufentanil usage doses in the first postoperative 24 h. Frances Chung et al reported that type of surgery, age and BMI were related to analgesic consumption; among these factors, type of surgery and age were the stronger predictors for analgesic consumption.7 We did not discover an association between type of surgery and analgesic consumption in this study, which may be due to the difference in surgical types and the limited number of participants involved in our study. However, we confirmed that age and BMI were related to analgesic consumption.
This study found that AA carriers of rs3745367 have a high mechanical pain threshold and low pain sensitivity and that the mechanism is probably due to the resistin function in the progression of inflammatory regulation. It was reported that rs3745367 of resistin is associated with circulating resistin levels.38 Changes in the resistin content may influence pain sensitivity. As a hormone, resistin can stimulate target cells to produce inflammatory cytokines through nuclear factor-κB-mediated signaling pathways.39–41 These proinflammatory cytokines play a vital role in the induction and maintenance of pain by facilitating central sensitization and hyperalgesia.42 In conclusion, it is speculated that resistin may participate in nociceptive pain signaling and alter the sensitivity to opioid analgesics.
One limitation of this study is that mechanical pain threshold or sufentanil consumption is influenced by numerous confounding factors, making R2 of MLR model analyzed in our study smaller, thus further studies should include more factors. In addition, our study is limited to gastric cancer patients who underwent radical surgery, which might prevent its generalization. A study with larger-scale participants or with other types of cancers is needed to confirm its generalizability.
Conclusion
In this study, the rs3745367 polymorphism of resistin was associated with the preoperative mechanical pain threshold and postoperative opioid consumption in gastric cancer patients with radical surgery. Patients with AA genotypes of rs3745367 showed a higher mechanical pain threshold and less postoperative sufentanil consumption. Identified gene polymorphism of resistin before surgery may help anesthesiologists develop better analgesic plans to improve the personalized treatment of gastric cancer patients after surgery.
Abbreviations
NRS, numerical rating scale; ASA, American Society of Anesthesiologists; PCIA, patient-controlled intravenous analgesia.
Ethics Approval and Informed Consent
The present investigation was approved by the Ethics Committee of Peking University Cancer Hospital & Institute (2021KT66). Participants signed their informed consent before the trial. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Ge Meng, Yining Xie and Hongwei Sun of Peking University Cancer Hospital & Institute, which help us complete this study in the surgery.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science Foundation of Peking University Cancer Hospital-2021-21 and Special Fund for Clinical Research of Wu Jieping Medical Foundation (320.6750.2021-4-18).
Disclosure
Dr Hongyu Tan reports grants from Special Fund for Clinical Research of Wu Jieping Medical Foundation, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Richebe P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129:590–607. doi:10.1097/ALN.0000000000002238
2. Phillips DM. JCAHO pain management standards are unveiled. Joint commission on accreditation of healthcare organizations. JAMA. 2000;284:428–429. doi:10.1001/jama.284.4.423b
3. Carr DB, Goudas LC. Acute pain. Lancet. 1999;353:2051–2058. doi:10.1016/S0140-6736(99)03313-9
4. Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377:2215–2225. doi:10.1016/S0140-6736(11)60245-6
5. Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015;95:301–318. doi:10.1016/j.suc.2014.10.002
6. Sommer M, de Rijke JM, van Kleef M, et al. Predictors of acute postoperative pain after elective surgery. Clin J Pain. 2010;26:87–94. doi:10.1097/AJP.0b013e3181b43d68
7. Ip HY, Abrishami A, Peng PW, et al. Predictors of postoperative pain and analgesic consumption: a qualitative systematic review. Anesthesiology. 2009;111:657–677.
8. Yang MMH, Hartley RL, Leung AA, et al. Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis. BMJ Open. 2019;9:e025091. doi:10.1136/bmjopen-2018-025091
9. Palada V, Kaunisto MA, Kalso E. Genetics and genomics in postoperative pain and analgesia. Curr Opin Anaesthesiol. 2018;31:569–574. doi:10.1097/ACO.0000000000000633
10. Hwang IC, Park JY, Myung SK, et al. OPRM1 A118G gene variant and postoperative opioid requirement: a systematic review and meta-analysis. Anesthesiology. 2014;121:825–834. doi:10.1097/ALN.0000000000000405
11. Sun J, Duan G, Li N, et al. SCN11A variants may influence postoperative pain sensitivity after gynecological surgery in Chinese Han female patients. Medicine. 2017;96:e8149. doi:10.1097/MD.0000000000008149
12. Yang Z, Yang Z, Arheart KL, et al. CYP2D6 poor metabolizer genotype and smoking predict severe postoperative pain in female patients on arrival to the recovery room. Pain Med. 2012;13:604–609. doi:10.1111/j.1526-4637.2012.01296.x
13. Tripathi D, Kant S, Pandey S, et al. Resistin in metabolism, inflammation, and disease. FEBS J. 2020;287:3141–3149. doi:10.1111/febs.15322
14. Kim KH, Lee K, Moon YS, et al. A cysteine-rich adipose tissue-specific secretory factor inhibits adipocyte differentiation. J Biol Chem. 2001;276:11252–11256. doi:10.1074/jbc.C100028200
15. Park HK, Kwak MK, Kim HJ, et al. Linking resistin, inflammation, and cardiometabolic diseases. Korean J Intern Med. 2017;32:239–247. doi:10.3904/kjim.2016.229
16. Schwartz DR, Lazar MA. Human resistin: found in translation from mouse to man. Trends Endocrinol Metab. 2011;22:259–265. doi:10.1016/j.tem.2011.03.005
17. Singhal NS, Patel RT, Qi Y, et al. Loss of resistin ameliorates hyperlipidemia and hepatic steatosis in leptin-deficient mice. Am J Physiol Endocrinol Metab. 2008;295:E331–338. doi:10.1152/ajpendo.00577.2007
18. Filkova M, Haluzik M, Gay S, et al. The role of resistin as a regulator of inflammation: implications for various human pathologies. Clin Immunol. 2009;133:157–170. doi:10.1016/j.clim.2009.07.013
19. Jamaluddin MS, Weakley SM, Yao Q, et al. Resistin: functional roles and therapeutic considerations for cardiovascular disease. Br J Pharmacol. 2012;165:622–632. doi:10.1111/j.1476-5381.2011.01369.x
20. Suragani M, Aadinarayana VD, Pinjari AB, et al. Human resistin, a proinflammatory cytokine, shows chaperone-like activity. Proc Natl Acad Sci U S A. 2013;110:20467–20472. doi:10.1073/pnas.1306145110
21. Bouziana S, Tziomalos K, Goulas A, et al. Effects of major adipokines and the −420 C > G resistin gene polymorphism on the long-term outcome of patients with acute ischemic stroke. Int J Neurosci. 2019;129:978–985. doi:10.1080/00207454.2019.1596906
22. Hossein-Nezhad A, Varzaneh FN, Mirzaei K, et al. A polymorphism in the resistin gene promoter and the risk of multiple sclerosis. Minerva Med. 2013;104:431–438.
23. Farag AGA, Hammam MA, Khaled HN, et al. Resistin adipokin in atopic dermatitis patients: a clinical, biochemical, and genetic study. J Cosmet Dermatol. 2020;19:2929–2935. doi:10.1111/jocd.13338
24. Novitsky YW, Litwin DE, Callery MP. The net immunologic advantage of laparoscopic surgery. Surg Endosc. 2004;18:1411–1419. doi:10.1007/s00464-003-8275-x
25. Vittimberga FJ
26. Hozumi J, Sumitani M, Nishizawa D, et al. Resistin is a novel marker for postoperative pain intensity. Anesth Analg. 2019;128:563–568. doi:10.1213/ANE.0000000000003363
27. Wang H, Chu WS, Hemphill C, et al. Human resistin gene: molecular scanning and evaluation of association with insulin sensitivity and type 2 diabetes in Caucasians. J Clin Endocrinol Metab. 2002;87:2520–2524. doi:10.1210/jcem.87.6.8528
28. Xie H, Fan Q, Ma Z, et al. Resistin gene polymorphism is an influencing factor of postoperative pain for Chinese patients. Pain Phy. 2020;23:E695–E702.
29. Gurzu S, Sugimura H, Orlowska J, et al. Proposal of a Dukes-MAC-like staging system for gastric cancer. J Investig Med. 2017;65:316–322. doi:10.1136/jim-2016-000270
30. Anderson JL, King GJ, Thomson MJ, et al. A mutation in the methylenetetrahydrofolate reductase gene is not associated with increased risk for coronary artery disease or myocardial infarction. J Am Coll Cardiol. 1997;30:1206–1211. doi:10.1016/S0735-1097(97)00310-0
31. Chen ACN, Dworkin SF, Haug J, et al. Human pain responsivity in a tonic pain model: psychological determinants. Pain. 1989;37:143–160. doi:10.1016/0304-3959(89)90126-7
32. Wang F, Belanger E, Cote SL, et al. Sensory afferents use different coding strategies for heat and cold. Cell Rep. 2018;23:2001–2013. doi:10.1016/j.celrep.2018.04.065
33. El Tumi H, Johnson MI, Dantas PBF, et al. Age-related changes in pain sensitivity in healthy humans: a systematic review with meta-analysis. Eur J Pain. 2017;21:955–964. doi:10.1002/ejp.1011
34. Palmeira CC, Ashmawi HA, Posso Ide P. Sex and pain perception and analgesia. Rev Bras Anestesiol. 2011;61:814–828. doi:10.1016/S0034-7094(11)70091-5
35. Zhang Y, Zhang S, Gao Y, et al. Factors associated with the pressure pain threshold in healthy Chinese men. Pain Med. 2013;14:1291–1300. doi:10.1111/pme.12158
36. Yu L, Li S, Wei J, et al. Association of serotonin transporter-linked polymorphic region (5-HTTLPR) with heat pain stimulation and postoperative pain in gastric cancer patients. Mol Pain. 2021;17:17448069211006606. doi:10.1177/17448069211006606
37. Zajacova A, Rogers RG, Grodsky E, et al. The relationship between education and pain among adults aged 30–49 in the United States. J Pain. 2020;21:1270–1280. doi:10.1016/j.jpain.2020.03.005
38. Suriyaprom K, Tungtrongchitr R, Namjuntra P. Associations of resistin levels with resistin gene polymorphism and metabolic syndrome in Thais. J Med Biochem. 2015;34:170–178. doi:10.2478/jomb-2014-0034
39. Pang SS, Le YY. Role of resistin in inflammation and inflammation-related diseases. Cell Mol Immunol. 2006;3:29–34.
40. Silswal N, Singh AK, Aruna B, et al. Human resistin stimulates the pro-inflammatory cytokines TNF-alpha and IL-12 in macrophages by NF-kappaB-dependent pathway. Biochem Biophys Res Commun. 2005;334:1092–1101. doi:10.1016/j.bbrc.2005.06.202
41. Bokarewa M, Nagaev I, Dahlberg L, et al. Resistin, an adipokine with potent proinflammatory properties. J Immunol. 2005;174:5789–5795. doi:10.4049/jimmunol.174.9.5789
42. Ronchetti S, Migliorati G, Delfino DV. Association of inflammatory mediators with pain perception. Biomed Pharmacother. 2017;96:1445–1452. doi:10.1016/j.biopha.2017.12.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gene Polymorphisms of m6A Erasers FTO and ALKBH1 Associated with Susceptibility to Gastric Cancer
Li Y, Zhou D, Liu Q, Zhu W, Ye Z, He C
Pharmacogenomics and Personalized Medicine 2022, 15:547-559
Published Date: 31 May 2022