")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Effects of Physical Activity on Health-Related Quality of Life Among Working Mothers Living in Amman: A Correlational Study
Authors Abu Aqab A, AL-Hussami M , Almegewly W , Karavasileiadou S
Received 29 March 2023
Accepted for publication 11 July 2023
Published 17 July 2023 Volume 2023:16 Pages 1989—2000
DOI https://doi.org/10.2147/JMDH.S414826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Aya Abu Aqab,1 Mahmoud AL-Hussami,2 Wafa Almegewly,3 Savvato Karavasileiadou3
1School of Medicine, the University of Jordan, Amman, Jordan; 2The University of Jordan, School of Nursing, Amman, 11942, Jordan; 3Department of Community Health Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia
Correspondence: Wafa Almegewly, Princess Nourah bint Abdulrahman University, P.O. Box 84428, Riyadh, 11671, Saudi Arabia, Email [email protected]
Background: Jordan has a high prevalence of physical inactivity, a major risk factor for non-communicable diseases. Working mothers are a high-risk group who face significant barriers to physical activity and experience a decline in their quality of life.
Purpose: This study aims to evaluate the potential impact of physical activity adherence on health-related quality of life and physical fitness among a sample of working mothers.
Patients and Methods: A Correlational, retrospective analytical design, was employed among a sample of working mothers (n=120), from Amman and was divided into two comparison groups. Data collection included a self-reported questionnaire using a demographic questionnaire, a health perception scale, the International Physical Activity Questionnaire short form, the International Fitness Scale, and the Quality of Life Brief questionnaire. The statistical analysis was independent t-test analysis, analysis of variance (One-way ANOVA), Pearson r correlation and regression used to estimate the prediction of dependent variables based on independent variables.
Results: The results found a significant positive relationship between physical activity and overall quality of life and its domains (physical, psychological, and environmental); however, there was no statistically significant difference in the social domain. Adherence to physical activity was a significant positive predictor of quality of life. Moreover, the health perception level was a significant positive predictor. A t-test revealed a statistically significant difference between the physically active group and a sedentary group of working mothers regarding changes in Health-Related Quality of Life; physically active mothers are more likely to have better physical (p < 0.024), psychological (p < 0.001), and overall quality of life (p < 0.011). Furthermore, Physical fitness significantly predicted physical activity in the study results.
Conclusion: This study confirms the existence of positive correlations between physical activity and working women’s quality of life and physical fitness. Mothers with higher levels of physical activity are more likely to have better physical, psychological, and environmental domains of quality of life and better physical fitness.
Keywords: physical activity, health-related quality of life, working mothers, physical fitness, Jordan
A Letter to the Editor has been published for this article.
Introduction
Women who are able to balance a career with the additional responsibility of raising a child are considered working mothers.1 The job can have both a detrimental and a beneficial impact on health and quality of life, from prolonged exposure to work stress on the one hand to increased cohesion, satisfaction, and social support on the other hand.2 Combining work and family responsibilities, the absence of support, guilt for spending time away from their children for exercise, and scheduling limitations are significant physical activity barriers for parents, increasing their vulnerability to the effects of a sedentary lifestyle, mainly for working mothers, and as a result of the expected commitment to the traditional role of females in local communities.3 Fulfilling multiple roles can contribute to lower health-related quality of life (HRQoL), higher job stress, anxiety, and burnout among this population.4 The World Health Organization (WHO) recommends engaging in physical activity for at least 150–300 minutes each week at a moderate to vigorous intensity, or 75–150 minutes at a moderate to vigorous intensity, or an equivalent combination of the two.5 The most recent global prevalence of insufficient physical activity among adults was 23.3% in 2010 and 27.5% in 2016, and women showed lower physical activity levels than men.6
The prevalence of physical inactivity in Jordan is sufficiently high; most Jordanians are physically inactive and do not meet the World Health Organization (WHO) guidelines and recommendations on physical activity.7 According to a study from Jordan, only 16.2% of men and 8.6% of women were physically active. Physical activity participation was significantly lower in females than in males.8 Physical activity plays an essential role in improving an individual’s perception of health-related quality of life (HRQoL). Moreover, lower levels of physical activity are a leading risk factor for noncommunicable diseases (NCDs), including coronary heart disease, type 2 diabetes, and some cancer types, and negatively affect individuals’ mental health and quality of life.6 Noncommunicable diseases (NCDs), account for 78% of all deaths in Jordan and are primarily cardiovascular, cancer, diabetes, and chronic respiratory diseases, which are the leading causes of morbidity and mortality.6 Lower odds of developing depression in the future have been consistently associated with higher levels of physical activity, regardless of age and gender.9
The present study is an original study conducted in Jordan, aimed to examine the effects of self-physical activity adherence on improving health-related quality of life among a sample of working mothers in Amman and to correlate the effects of self-physical activity with quality-of-life domains. Furthermore, to examine the relationship between physical activity and physical fitness.
Consequently, a better understanding of the associations between physical activity and quality of life among working mothers is needed. Therefore, this study could contribute to filling the knowledge gap concerning the potential impact of physical exercise on health-related quality of life among the working mother population, increasing awareness of physical activity and providing a clear picture of these issues in Jordan. This study is critically important for women and working mothers who face enormous constraints on their “free” time and are a group at risk for low levels of physical activity and may gain a range of health benefits from physical activity.10 The Research questions were as follows: 1. Is there any association between the level of physical activity and quality of life and its domains (physical health, psychological health, social relationships, and environmental health)? 2. What effect does adherence to physical activity have on improving health-related quality of life among working mothers? 3. Will the participants who practice exercise show high quality of life scores compared to the control group? 4. Will the participants who adhere to physical activity show higher physical fitness scores?
Methods
Study Design and Setting
This study is a correlational, retrospective analytical design, causal-comparative research to identify the cause-and-effect relationship between dependent (quality of life) and independent variables (Physical Activity and Physical fitness). A correlational study is when researchers study the effect of a potential cause that they cannot manipulate and use designs that examine relationships between variables. The searcher has studied cause and effect in retrospect and determined the consequences or causes of differences between groups of people. The researcher recruited comparison groups of physically active and inactive working mothers from local organizations in Amman. Group one was composed of physically active working mothers who were recruited from seven physical fitness centers where aerobic exercise is the focus, picked out of fifty centers in Amman. Group two, the sedentary group of working mothers, was conveniently recruited from four Child care centers picked out of seventy-two centers in Amman.
The data collection procedure for both groups was conducted over three months (June, July, and August 2022). Researchers contacted the directors of childcare and fitness centers to inform them about the study and to obtain permission for data collection in their private centers so that the researchers could speak directly with the mothers to determine who meets the eligibility criteria and would agree to participate in the study. Participants who met the inclusion criteria and voluntarily agreed to participate in the study signed a consent form. After participants read the consent form and were provided a full explanation regarding the study’s purpose, potential benefits, and risks, and study confidentiality, a self-reported questionnaire was given to mothers, who were instructed to complete it and then return it to the researcher to be kept in a secure file set up by the researcher for each center for both groups.
Ethical Consideration
This study adheres to the Helsinki Declaration and was approved by the scientific research committee’s Institutional Review Board (IRB), from the University of Jordan at the School of Medicine (protocol code 291 and date of approval: 1/6/2022).
Ethical approval for this study was granted by the Scientific and Ethical Research Committees at the School of Scientific Research/University of Jordan. A consent form was signed prior to the study by each subject, containing a thorough description of the purpose and merit of the study and explaining clearly that participation is voluntary and that each subject has the right to withdraw at any point or refuse to answer any of the items without any consequences. The confidentiality of all study subjects was maintained throughout the study. The subjects’ anonymity was only preserved as names and contact information was not collected in the questionnaire.
Study Sample
The difference between two independent means (two groups), was determined using G*power 3.1,11 to identify the required sample size with a two-tailed test and a medium effect size of r= 0.5, a statistical power of 0.80, and a significant alpha of 0.05. The desired sample size was 102. 10% was added to cover the attrition; therefore, the total sample size is 112.
A multistage sampling technique was used to select participants in succession from bigger to smaller units, including randomly choosing four Childcare centers out of 72 (since Childcare centers are local organizations frequented by mothers with children under the age of ten), and 7 physical gyms out of 50 in Amman through a simple random sampling technique at the first stage: the high prevalence of physical inactivity in Jordan is a justification for choosing seven physical centers. The second stage consisted of conveniently drawing the study participants of working mothers who fulfilled the eligibility criteria from the randomly chosen local organizations frequented by mothers, into two comparison groups of physically active and inactive working mothers. In June 2022, the accessible working mothers residing in Amman who were employed at least 25 hours per week participated in this study based on the following inclusion criteria: (1) mothers who had at least one child under the age of 10 years, (2) Working mothers aged 18 to 55 years, (3) Jordanian nationality. In addition, (4) have been enrolled for at least three months in a 150-minute weekly vigorous-intensity exercise program (Since the WHO’s minimum recommendation on physical activity is 75–150 min/week of vigorous-intensity exercise). The exclusion criteria are (1) pregnant women and (2) women with noncommunicable diseases.
Questionnaires
The data were collected through a self-administered sociodemographic questionnaire comprised of 12 items regarding sociodemographic factors, including age, education, Household Income, marital status, health status, employment hours, parenthood status, number of children, smoking status, body weight, body height, and body mass index (BMI), as well as a health perception questionnaire12 was adapted from predictors of the quality of life of rural older adults and translated according to WHO translation guidelines, including three dimensions; clinical health perception was assessed by the following question: “You have always understood your illness”, and the following question asked functional health perception; “You understand your health and immunity”, and finally the adaptive health perception following question; “You are prepared to cope with any illness that may happen in the future”, an international fitness scale (IFS)13 is a self-reported physical fitness questionnaire developed by the PROFITH research group and translated according to WHO translation guidelines consisting of five items general physical fitness, cardiorespiratory fitness, muscular strength, speed–agility, and flexibility, International Physical Activity Questionnaire-Short Form (IPAQ)14 (the Arabic version of the Self-reported (IPAQ-short form) was employed consisting of seven items and records the activity of four intensity levels: 1) vigorous-intensity activity such as aerobics; 2) moderate-intensity activity such as leisure cycling; 3) walking; and 4) sitting, The Quality-of-Life Scale-Brief (HRQOL)15 Arabic version consists of 26 items and includes four dimensions: physical health, social relationships, psychological status, and environment, the measurement tools are all open access, with no need for approval to use them. The content validity index (CVI) was calculated and met a satisfactory level, indicating the extent of expert agreement. The S-CVI Average based on proportional relevance = 0.93, and the S-CVI Universal Agreement average is 0.8, meaning the survey questionnaire is valid.
A pilot study was conducted over fifteen physically inactive participants before the data collection process to test the feasibility and reliability of the questionnaire, the internal consistency of Cronbach’s alpha for each scale, and the results were as follows for the Health Perception scale, IFIS scale, IPAQ scale, and HRQOL scale (0.861, 0.714, 0.652, 8.36), respectively, indicating that the survey questionnaire is reliable.
Data Analysis
Data were collected, coded, and screened for completeness before entering the computer program. The analysis was performed using Statistical Package for Social Science (SPSS), version 24; an alpha level of 0.05 was used. The distribution of the variables was reviewed for skewed distribution. Univariate analysis was used to estimate frequencies, mean, standard deviation, range, and percentiles (Q25, Q50, and Q75) according to the level of variables introduced and compared with population characteristics, and 95% confidence intervals for categorical variables were performed to describe the distribution of the outcome, explanatory variables, and basic characteristics. An independent t-test analysis was used to obtain the mean differences between the two groups. A one-way ANOVA was used to examine the differences between three or more groups. In addition, Pearson r correlation was used to investigate the correlation between continuous variables. Hierarchical regression was used to estimate the prediction of dependent variables based on independent variables controlling for demographic data. Also, linear regression was used to estimate the prediction of dependent variables based on independent variables.
Results
A total of 120 questionnaires were distributed, and 112 were completed, with a good response rate of 93.3%. (Table 1) indicated that 89.3% (n = 100) of respondents were married and 67.9% (n = 76) were nonsmokers, with a mean age of 35 (SD = 6). Regarding educational level, 73.2% (n = 82) held a bachelor’s degree, and 22.3% (n = 25) held a postgraduate degree. The mean of all participants working hours per week was 38 (SD = 7). Likewise, all the participants were mothers, with a mean number of children of two (SD = 1). In addition, the mean monthly income was 1574 (SD = 669), and the body mass index mean was 26.33 (SD = 4.74).
 |
Table 1 Demographic Data |
To investigate the relationship between adherence to physical activity and quality of life and its Domains, Pearson r correlation was performed (Table 2), setting a significant point at alpha < 0.05. The results showed a significant positive relationship between physical activity, overall quality of life, and its domains (all p < 0.05), except for the social domain.
 |
Table 2 Relationship Between Physical Activity and Quality of Life and Its Domains |
To investigate the relationship between adherence to physical activity and health-related quality of life, multiple hierarchal linear regression was performed (Table 3), setting a significant point at alpha < 0.05. Tests to see if the data met the assumption of collinearity indicated that multi-collinearity was not a concern (Table 3).
 |
Table 3 Collinearity Tests for Independent Variables in Each Regression Step |
A three- step multiple hierarchical regression analysis was performed to examine the prediction power of adherence to physical activity, controlling for health perception and selected demographic characteristics. The analysis showed that demographic factors for mothers (age, education, social status, working hours, family income, smoking status, and body mass index), none of the selected demographics was a significant predictor (F = 0.975, p > 0.05) with R 2 = 0.062 (6.2%), (Table 4). Then, by adding the health perception level, the model was a significant positive predictor (F = 2.912, p = 0.006, B = 0.315) with R2 = 0.186 (18.6%), indicating that the higher the health perception level, the better “mothers” quality of life. Then Again, by adding adherence to physical activity level, the model was a significant positive predictor (F = 4.954, p < 0.001, B = 0.363) with R2 = 0.306 (30.6%), indicating that the higher the adherence to physical activity, the better “mothers” quality of life. The R2 change from step 1 to 2 was 0.124 (12.4%), from step 2 to 3 was 0.120 (12%), and from model 1 to 3 was 0.244 (24.4%). The results indicate that 30.6% of the variation in “mothers” quality of life is explained by model 3, which contains adherence to physical activity controlling for health perception and selected demographic characteristics. Also, 18.6%. The variation in “mothers” quality of life is explained by Model 2, which contains health perception controls for selected demographic characteristics.
 |
Table 4 Predictors of Quality of Life |
To compare active and inactive mothers’ quality of life, an independent t-test was used, setting a significant point at alpha < 0.05. (Table 5) showed that there was a significant difference (t = −2.289, p = 0.024), (t = −3.526, p = 0.001), and (t = −2.584, p = 0.011) between active and inactive mothers related to their physical, psychological, and overall quality of life, respectively. In which the mean physical domain quality of life scores of active mothers, 69.57 (SD = 13.89), were higher than those of inactive mothers, 63.58 (SD = 13.8). Moreover, the mean psychological domain quality of life scores of active mothers, 67.70 (SD = 13.74), were higher than those of inactive mothers, 85.48 (SD = 13.94), and the mean overall quality of life scores of active mothers, 58.02 (SD = 7.92), were higher than those of inactive mothers, 54.31 (SD = 7.24). This indicates that active mothers are more likely to have better physical and psychological domains and overall quality of life.
 |
Table 5 Comparison Between Active and in-Active Mothers Related to Their Quality of Life |
To investigate the relationship between physical activity and physical fitness, Pearson r correlation was used, setting a significant point at alpha < 0.05. Results showed a significant positive relationship (r = 0.622, p < 0.001) between physical activity and physical fitness. This indicates that mothers with higher physical activity levels are more likely to have higher physical fitness levels. In addition, linear regression was done to examine the predictability of physical fitness based on physical activity. (Table 6) revealed that the one-factor model (regression equation) was significant, F (1, 110) = (69.359, p = 0.003), with an R2 of 0.387. Physical activity significantly predicted physical fitness (Beta = 0.622, p < 0.001). Physical activity was a positive predictor, which means that the higher the physical activity, the higher the physical fitness. The overall model fits R2 = 0.387, which means that this model is responsible for 38.7% of the variance of the mother’s physical fitness level. The predicted mother’s physical activity level is equal to −4378.257 + 396.773 (physical activity) total scores.
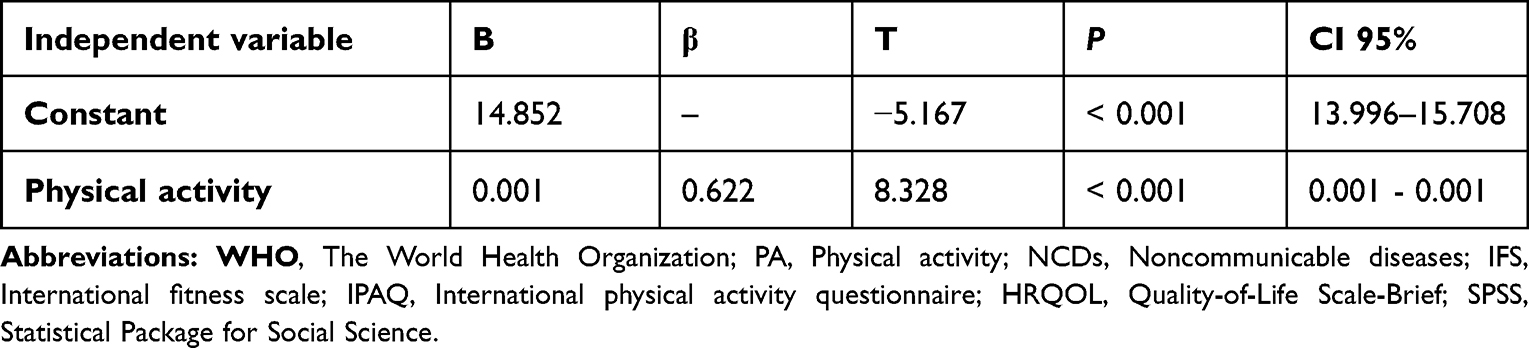 |
Table 6 Predictors of Physical Fitness Based on Physical Activity |
Discussion
The results of the present study indicated that there is a statistically significant positive correlation between the independent variable (physical activity) and the dependent variable (Health-Related Quality of Life), after controlling for sociodemographic variables. Results provided further evidence of the “effects of physical activity levels among Jordanian working ‘mothers’ health-related quality of life, which is a multi-dimensional factor. This study demonstrates that mothers with higher physical activity levels are more likely to have a better overall quality of life. This relationship is consistent across different measures and types of physical activity. A previous study in Jordan found that sufficient physical activity is linked to improved quality of life, longer duration, fewer sleep disturbances, and fewer depressive and anxiety symptoms.16 However, Jordan is not an exception since physical inactivity is a worldwide pandemic, and abundant research studies on physical activity levels have revealed a significant correlation between physical activity levels and quality of life.17–20 Moreover, studies from the United States are consistent with the current findings; in their study, they investigated an association between recommended levels (moderate and vigorous) of physical activity and mental and overall HRQL; according to the results, higher HRQL scores were associated with recommended levels of PA in both intensities.21 Mothers” quality of life in their social relationships and environments was related to the interaction between parental stress and moderate-intensity physical activity;10 these results suggest that moderate physical activity may reduce the detrimental effects of parenting stress on social relationships and environmental satisfaction in working women. On the other hand, in Greece, a study revealed no statistically significant correlation between QoL and PA intensity (light, moderate, vigorous) in their study population.22 Furthermore, the present study’s findings showed that, except for the social relationship domain, where no significant relationship with the independent variable was found, the domains of physical health, psychological health, and environmental health are significantly associated with physical activity. However, differences in the magnitude of HRQoL domains benefits are noticeable in both objective and subjective measures of Physical activity in former studies. Consistent with the current findings, a study suggested that a physical intervention program influences both physical and mental health indicators as a result of three months stretching program that improves the health-related quality of life for office desk workers.23 Contrary to this study’s results, a study in China suggested that improving social relationships could be accomplished more effectively with group-based physical activity and counseling interventions.4 likewise, another study revealed the existence of positive correlations between the physical, psychological, social, and Environmental domains of quality of life among the working-age population.24
Moreover, the findings of this study suggest that physical activity adherence aims to improve women’s health-related quality of life to cope with stress from home and work and prevent noncommunicable diseases (NCDs). Furthermore, it showed that family income did not predict quality of life. However, it was positively correlated to the quality of life, indicating that mothers with higher monthly incomes are more likely to have a better quality of life. This finding is consistent with previous studies that revealed a positive correlation between family income and quality of life. In agreement with the current study results, there were different studies from Jordan,25 Portugal,26 Nepal,27 and Saudi Arabia.28 Moreover, evidence from Brazil found that Greater access to information, better transportation options, and better healthcare services are all benefits of higher income levels that may help improve quality of life.29,30 Regarding age, working hours, and body mass index, the current study found that no significant relationship was established between quality of life and age, working hours, and BMI. These findings are constant with other international results from Croatia that found the quality of life had no impact from age differences.31 However, results of another study ascertained that age-related changes are known to lead to a deterioration in the quality of life of adults.32 According to the researchers’ findings, employment hours do not correlate with the working “mothers” quality of life in the current study; a significant association between the employment status of mothers being employed having a better quality of life for working women than for unemployed women was established in literature.29,33 Moreover, another study showed that older Koreans’ quality of life is greatly impacted by work.34 Regarding BMI, the current findings Contrary to most of the literature, increased body mass index (BMI) was negatively related to the quality of life in the general Turkish population;33 lend support to this result in a study from the USA,2 like that of Kuwait.35 The current findings showed no significant difference between mothers with different educational levels in their quality of life. Likewise, there was no significant difference between mothers with different social and smoking statuses in their quality of life. Dissimilar results from earlier studies regarding the level of education in the current study. A study in Brazil found that married women with higher incomes and educational degrees scored better overall on the Quality-of-Life scale.30 Moreover, a study in the United States reported a significant association between the highest level of education and meeting the recommendation for physical activity and well-being improvement.2 The findings from this study supported no relation between marital status and quality of life, while in Brazil, it showed that not having a partner has a detrimental impact on the environmental domain.29 Likewise, compared to single women, married women receive more support from their families,30 which plays a significant role in coping with illnesses and improving their quality of life in line with literature from Korea, the present study found no significant association between smoking and Health Related-Quality of Life.36 Conversely, another study concluded that smoking could lead to a feeling of being in a better mood, which can raise reported HRQoL, especially in older people.37 Concerning the health perception status, findings from the current research confirmed that the perception of health is a significant predictor of Quality of Life; a better health perception is associated with better quality of life in Jordanian-employed mothers. Analogously, the interrelationship among health indicators in Italy, Spain, and Greece studies revealed that general health perception is a significant predictor of quality of life.38 Likewise, another study from the United States proved this correlation.39 After controlling for health perception and selected demographic characteristics, adherence to physical activity was a positive significant predictor of quality of life, and this indicates that the higher the commitment to physical activity, the better the quality of life for mothers. Consistent with these results, it was found that working moms in Tunisia could considerably increase their health-related quality of life by participating in physical activity, which could help to mitigate adverse health-related outcomes.40 In a Croatian study involving mothers of preschoolers, there were marginally statistically significant links between free-time physical exercise and quality of life.31 Likewise, physical activity was significantly associated with health-related quality of life among indigenous people in Australia and New Zealand.41 Other consistent findings showed positive correlations between physical activity and quality of life among the working-age population (aged 18–64 years) in Wroclaw, Poland; they found that physical activity of appropriate duration, frequency, and intensity is a significant determinant of their overall quality of life and its domains.24 Working women adhering to the required physical activity guidelines were linked to improved quality of life and higher productivity levels.2 Furthermore, a robust empirically based study among Chinese working women revealed that physical activity intervention could reduce stress and burnout and enhance health-related quality of life.4
Findings demonstrated significant differences between the two groups related to their quality of life, suggesting that active mothers are more likely to have better physical and psychological domains and overall quality of life. This is consistent with the majority of intervention studies that are effective in improving health-related outcomes for working women. Consistent with a piece of research from Shanghai, participants who participated in a group or individual physical activity program saw significant drops in their overall stress and burnout levels. Compared to the no-exercise controls, they also significantly improved their overall health-related quality of life scores.4 In Spain, a 16-week supervised aerobic exercise intervention program for overweight adults with hypertension increased self-reported physical activity, decreased sedentary behavior, and improved sleep quality. The results of this study demonstrate the necessity of a regular, scheduled, and supervised physical activity program to encourage healthy behaviors in individuals with HTN and obesity.42 According to a study conducted in the United States, mothers who reported maintaining or increasing their physical activity over the preceding month and who maintained similar levels of sedentary behavior reported less psychological distress than mothers who reported declining physical activity and increasing sedentary behaviors. According to these results, leading an active lifestyle is linked to moms experiencing less psychological distress.43
This study is considered the first in Jordan and the region to examine the effect of physical activity on health-related quality of life among the population of working mothers. In addition, a notable strength of this study was that it examined the physical activity effect in the context of the retrospective causal-comparative method; this study design allowed the researcher to determine the cause or consequences of differences that already exist between or among groups of individuals. Our study has a few limitations, firstly, the study sample was relatively homogenous, particularly concerning marital and educational status. Nearly 89.3% of participants were married. Additionally, 73.2% had a bachelor’s degree, and 22.3% had a postgraduate one. Secondly, Respondents may under or over-report their responses because all data in this study is self-reported. Thirdly, one drawback of the study is the limitation of the study population to a single city. Jordan as a whole, not simply Amman, should be the focus of this subject of study.
This study opens a wide range of potential directions for further research because the exercise literature aimed at working mothers in Jordan is still in its infancy. An alternative means required to provide support to be considered in future investigations, an experimental design group measured objectively, would be the most feasible and effective at improving the health outcomes of working mothers in Jordan. Future researchers may consider focusing on both working parents jointly. Employers play an essential role in providing a supportive work environment for working-age mothers by offering recreational facilities in the workplace or providing a free monthly gym subscription with a convenient location for the employees’ work site.
Conclusion
The findings of the current study mirrored that mother with higher levels of physical activity are more likely to have better physical, psychological, environmental, and overall quality of life. Adherence to physical activity and health perception were significant positive predictors for the mother’s quality of life in this study, and none of the demographics was significantly correlated to the quality of life except family income, indicating that mothers with higher monthly incomes are more likely to have a better quality of life. Working mothers who met the global recommendations on physical activity exhibited better benefits in the physical and psychological domains and overall quality of life compared to control. The study highlighted that working mothers with higher physical activity levels enhance physical fitness and improve health outcomes.
Acknowledgments
The authors express their gratitude to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R312), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
This work was supported by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R312), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors declare that they have no competing interests.
References
1. Poduval J, Poduval M. Working mothers: how much working, how much mothers, and where is the womanhood? Mens Sana Monographs. 2009;7(1):63. doi:10.4103/0973-1229.41799
2. Limbers CA, McCollum C, Greenwood E. Physical activity moderates the association between parenting stress and quality of life in working mothers during the COVID-19 pandemic. Ment Health Phys Act. 2020;19:100358. doi:10.1016/j.mhpa.2020.100358
3. Mailey EL, Huberty J, Dinkel D, McAuley E. Physical activity barriers and facilitators among working mothers and fathers. BMC Public Health. 2014;14(1):657. doi:10.1186/1471-2458-14-657
4. Wang H, Zhang T, Lu M, et al. Effects of physical activity and counselling interventions on health outcomes among working women in shanghai. J Sports Sci Med. 2021:77–85. doi:10.52082/jssm.2021.77
5. World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; 2018.
6. Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 2018;6(10):e1077–e1086. doi:10.1016/S2214-109X(18)30357-7
7. World Health Organization. Regional Office for the Eastern Mediterranean.; 2016.
8. Barghouti F. Leisure Time Physical Activity in Jordan: knowledge and Sociodemographic Determinants. Int Med J. 2015;22(4):283–287.
9. Schuch FB, Vancampfort D, Firth J, et al. Physical Activity and Incident Depression: a Meta-Analysis of Prospective Cohort Studies. Am J Psychiatry. 2018;175(7):631–648. doi:10.1176/appi.ajp.2018.17111194
10. Limbers CA, McCollum C, Ylitalo KR, Hebl M. Physical activity in working mothers: running low impacts quality of life. Women’s Health. 2020;16:174550652092916. doi:10.1177/1745506520929165
11. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
12. Seangpraw K, Ratanasiripong NT, Ratanasiripong P. Predictors of quality of life of the rural older adults in Northern Thailand. J Health Res. 2019;33(6):450–459. doi:10.1108/JHR-11-2018-0142
13. Ortega FB, Ruiz JR, España-Romero V, et al. The International Fitness Scale (IFIS): usefulness of self-reported fitness in youth. Int J Epidemiol. 2011;40(3):701–711. doi:10.1093/ije/dyr039
14. International Physical Activity Questionnaire (IPAQ). Short Last 7 Days Self-Administered Format. For Use with Young and Middle-Aged Adults; 2014.
15. World Health Organization. WHOQOL - Measuring Quality of Life| The World Health Organization; 2012.
16. Al-Ajlouni YA, Park SH, Alawa J, et al. Staying Physically Active Is Associated with Better Mental Health and Sleep Health Outcomes during the Initial Period of COVID-19 Induced Nation-Wide Lockdown in Jordan. Int J Environ Res Public Health. 2022;19(2):776. doi:10.3390/ijerph19020776
17. Puciato D, Borysiuk Z, Rozpara M. Quality of life and physical activity in an older working-age population. Clin Interv Aging. 2017;12:1627–1634. doi:10.2147/CIA.S144045
18. Xu H, Tang L, Hu Z, et al. Association between physical activity and health-related quality of life in elderly individuals with pre-diabetes in rural Hunan Province, China: a cross-sectional study. BMJ Open. 2018;8(4):e019836. doi:10.1136/bmjopen-2017-019836
19. Figueira HA, Figueira OA, Corradi-Perini C, et al. A descriptive analytical study on physical activity and quality of life in sustainable aging. Sustainability. 2021;13(11):5968. doi:10.3390/su13115968
20. Nguyen TM, Nguyen VH, Kim JH. Physical exercise and health-related quality of life in office workers: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(7):3791. doi:10.3390/ijerph18073791
21. Nakamura P, Teixeira I, Smirmaul BP, et al. Health related quality of life is differently associated with leisure-time physical activity intensities according to gender: a cross-sectional approach. Health Qual Life Outcomes. 2014;12(1):98. doi:10.1186/1477-7525-12-98
22. Saridi M, Filippopoulou T, Tzitzikos G, Sarafis P, Souliotis K, Karakatsani D. Correlating physical activity and quality of life of healthcare workers. BMC Res Notes. 2019;12(1):208. doi:10.1186/s13104-019-4240-1
23. Holzgreve F, Maltry L, Hänel J, et al. The Office Work and Stretch Training (OST) Study: an Individualized and Standardized Approach to Improve the Quality of Life in Office Workers. Int J Environ Res Public Health. 2020;17(12):4522. doi:10.3390/ijerph17124522
24. Puciato D, Rozpara M, Borysiuk Z. Physical Activity as a Determinant of Quality of Life in Working-Age People in Wrocław, Poland. Int J Environ Res Public Health. 2018;15(4):623. doi:10.3390/ijerph15040623
25. Dardas LA, Ahmad MM. Predictors of quality of life for fathers and mothers of children with Autistic Disorder. Res Dev Disabil. 2014;35(6):1326–1333. doi:10.1016/j.ridd.2014.03.009
26. Henriques A, Silva S, Severo M, Fraga S, Barros H. Socioeconomic position and quality of life among older people: the mediating role of social support. Prev Med. 2020;135:106073. doi:10.1016/j.ypmed.2020.106073
27. Acharya Samadarshi SC, Taechaboonsermsak P, Tipayamongkholgul M, Yodmai K. Quality of life and associated factors amongst older adults in a remote community, Nepal. J Health Res. 2022;36(1):56–67. doi:10.1108/JHR-01-2020-0023
28. Aboshaiqah AE, Cruz JP. Quality of Life and Its Predictors Among Nursing Students in Saudi Arabia. J Holistic Nurs. 2019;37(2):200–208. doi:10.1177/0898010118784147
29. Da Luz RA, de Deus JM, Conde DM. Quality of life and associated factors in Brazilian women with chronic pelvic pain. J Pain Res. 2018;11:1367–1374. doi:10.2147/JPR.S168402
30. Ghasemi E, Mohammad Aliha J, Bastani F, Haghani H, Samiei N. Quality of Life in Women with Coronary Artery Disease. Iran Red Crescent Med J. 2014;16(7). doi:10.5812/ircmj.10188
31. Babić A. Physical Activity and Quality of Life of Mothers of Preschool Children. Coll Antropol. 2015;39(2):419–426. doi:10.1542/peds.2013-3153d
32. Trombetti A, Reid KF, Hars M, et al. Age-associated declines in muscle mass, strength, power, and physical performance: impact on fear of falling and quality of life. Osteoporosis Inte. 2016;27(2):463–471. doi:10.1007/s00198-015-3236-5
33. Demircioğlu A, Özkal Ö, Dağ O. Multiple Factors Affecting Health-Related Quality of Life in Women With Chronic Multisite Musculoskeletal Pain: a Cross-Sectional Study in Ankara, Turkey. Eval Health Prof. 2022;45(2):115–125. doi:10.1177/01632787211049273
34. Eum M, Kim H. Relationship between Active Aging and Quality of Life in Middle-Aged and Older Koreans: analysis of the 2013–2018 KNHANES. Healthcare. 2021;9(2):240. doi:10.3390/healthcare9020240
35. Badr HE, Rao S, Manee F. Gender differences in quality of life, physical activity, and risk of hypertension among sedentary occupation workers. Quality Life Res. 2021;30(5):1365–1377. doi:10.1007/s11136-020-02741-w
36. Ham OK. Predictors of health-related quality of life among low-income midlife women. West J Nurs Res. 2011;33(1):63–78. doi:10.1177/0193945910372776
37. Krawczyk-Suszek M, Kleinrok A. Health-Related Quality of Life (HRQoL) of People over 65 Years of Age. Int J Environ Res Public Health. 2022;19(2):625. doi:10.3390/ijerph19020625
38. Maniscalco L, Miceli S, Bono F, Matranga D. Self-Perceived Health, Objective Health, and Quality of Life among People Aged 50 and Over: interrelationship among Health Indicators in Italy, Spain, and Greece. Int J Environ Res Public Health. 2020;17(7):2414. doi:10.3390/ijerph17072414
39. McKie CA, Laiyemo AO. Predictors of Quality of Life in Young Adults Diagnosed With Cancer. Clin Nurs Res. 2020;29(8):587–597. doi:10.1177/1054773820928197
40. Bettaieb J. Quality of life of working women: results of a Tunisian study using the 36-item short from health survey questionnaire (sF-3-6). Tunis Med. 2015;93(10):623–627.
41. Sushames A, van Uffelen JGZ, Gebel K. Do physical activity interventions in Indigenous people in Australia and New Zealand improve activity levels and health outcomes? A systematic review. Int J Behav Nutr Phys Activity. 2016;13(1):129. doi:10.1186/s12966-016-0455-x
42. Martinez Aguirre-Betolaza A, Mujika I, Loprinzi P, Corres P, Gorostegi-Anduaga I, Maldonado-Martín S. Physical Activity, Sedentary Behavior, and Sleep Quality in Adults with Primary Hypertension and Obesity before and after an Aerobic Exercise Program: EXERDIET-HTA Study. Life. 2020;10(8):153. doi:10.3390/life10080153
43. de Brito JN, Friedman JK, Emery RL, Neumark-Sztainer D, Berge JM, Mason SM. Changes in Physical Activity and Sedentary Behaviors During COVID-19: associations with Psychological Distress Among Mothers. Int J Womens Health. 2021;13:1115–1122. doi:10.2147/IJWH.S333719
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.