Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Effects of Mindfulness Meditation on Core Attention-Deficit Hyperactivity Disorder Symptoms, Family Functioning and Social Functioning in Children Aged Six to Nine
Authors Wang L, Wang M, Chang C, Tian L, Zhang Y, Lin J, Zhang T, Huan Q, Ji N
Received 21 May 2025
Accepted for publication 24 October 2025
Published 25 November 2025 Volume 2025:18 Pages 7705—7718
DOI https://doi.org/10.2147/JMDH.S538924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lifang Wang,1,* Mei Wang,2,* Cheng Chang,1 Lin Tian,1 Yannan Zhang,1 Jieqiong Lin,1 Tuo Zhang,1 Qiang Huan,1 Nan Ji3
1Department of Child Health, Xi’an Children’s Hospital, Xi’an, 710000, People’s Republic of China; 2Department of Pediatrics, Xi’an Fifth Hospital, Xi’an, 710082, People’s Republic of China; 3Department of Rehabilitation Medicine, Xi’an Children’s Hospital, Xi’an, 710000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nan Ji, Department of Rehabilitation Medicine, Xi’an Children’s Hospital, Xi’an, 710000, People’s Republic of China, Email [email protected]
Objective: To explore the effects of mindfulness meditation on core attention-deficit hyperactivity disorder (ADHD) symptoms, family functioning and social functioning in young children.
Methods: A convenience sample of 43 children aged 6– 9 years who met the inclusion and exclusion criteria was recruited at our hospital between 3 June and 3 July 2024. Participants were randomly assigned to an intervention group (22 cases) or a control group (21 cases). The intervention group received family mindfulness meditation combined with medication, whereas the control group received medication alone. Relevant indicators were collected and compared before and after the intervention.
Results: Compared with pre-intervention, the intervention group showed significant improvements in: Life Skills and Risk-Taking Activities (Weiss-P Functional Defect Scale); Conduct Problems and Psychosomatic Problems (Conners Parent Symptom Questionnaire, PSQ); and Attention–Visual Function (Integrated Visual and Auditory Continuous Performance Test, IVA-CPT). In contrast, the control group only improved significantly in Hyperactivity–Impulsivity (SNAP-IV Scale) and Psychosomatic Problems (PSQ). Post-intervention, the intervention group improved more in PSQ’s Conduct Problems and Psychosomatic Problems than the control group. However, the control group had no significant changes in most scale scores vs baseline, except Inattention (SNAP-IV) and Response Control (IVA-CPT).Medication subgroup analysis showed: vs pre-intervention, the intervention group improved significantly in PSQ’s Conduct Problems and Psychosomatic Problems (with significant time×group interactions); the control group had no significant changes in these indicators.Additionally, ANCOVA (controlling gender/age) for Weiss-P’s Self-Management showed: the intervention group’s pre-post score difference was statistically significant, while the control group only had a marginally significant increase. Mixed ANOVA confirmed significant time×group interactions for Weiss-P’s Life Skills and Risk-Taking Behavior, PSQ’s Conduct Problems, and IVA-CPT’s Response Control.
Conclusion: Simplified mindfulness meditation improves core ADHD symptoms and family functioning, and concurrent medication may influence its efficacy.
Keywords: attention-deficit hyperactivity disorder, core symptoms, family mindfulness meditation, social function, integrated visual and auditory continuous performance test
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder in children and adolescents.1 Its core symptoms include age-inappropriate inattention, shortened attention span, hyperactivity and situational emotional impulsivity.1 Additionally, children with ADHD often experience social disorders, behavioural problems, learning disabilities and emotional difficulties, which negatively affect academic, professional and social life.2 These challenges severely impair social functioning and quality of life, burden patients, families and society and can cause family depression and anxiety.3 Attention-deficit hyperactivity disorder-related learning difficulties require parental support, but many parents have residual ADHD symptoms, leaving some children without adequate support. This can worsen cognitive, psychological and behavioural issues, ultimately impairing social functioning.
Currently, drug therapy and behavioural intervention are key first-line treatments for ADHD. Medical institutions in the United States, Canada, Latin America and Europe recommend psychostimulants for ADHD.4 Although drugs can alleviate core ADHD symptoms in the short term, 20%–25% of affected children show no response.5 Moreover, medications may cause side effects such as headache, insomnia, anorexia and nausea, with long-term use potentially impacting growth and development.6 These concerns can reduce parental compliance with drug treatment. Many Chinese families prefer traditional Chinese medicine for its lower risk of side effects, and they are willing to try it despite its moderate efficacy.
However, current treatments have drawbacks: poor drug adherence, complex and hard-to-master behavioural interventions and external environment changes readily alter inner emotions. Behavioural interventions lack generalisability across environments, leaving children with ADHD unable to cope with complex changes or keep up academically. Thus, studying individual internal and family system benign changes can enhance treatment efficacy. The family is key to children’s growth, and their psychological intervention requires companionship and support. Family systems theory describes the family as a dynamic, interactive system with mutual behavioural influences. The symptoms of children with ADHD affect parental emotions and parenting via family interactions, whereas parental states in turn influence symptom development.6 Involving parents in interventions and improving family interaction quality via mindfulness can create a virtuous cycle, better promoting symptom improvement. Family and parenting interventions for children with ADHD – holistic family interventions with family participation – promote symptom improvement.7
Mindfulness meditation, centred on mindfulness techniques, involves non-judgemental, deliberate focus on current experiences (sensations, emotions, thoughts) to develop awareness.8 It is a self-regulation and emotional training strategy emphasising spiritual cultivation: training attention, fostering calmness, concentration and positive emotions (eg love, happiness) and reducing negative ones (eg fear, anger).9 Mindfulness methods include mindfulness of breathing (simple, for young children or beginners): focusing on the breath, observing the inhalation and exhalation and refocusing when distracted. Mindfulness meditation provides an environment to address physical and mental pain and understand one’s state.10 Long-term practice improves attention, working memory and emotional regulation and is widely used in psychology and medicine.11 Research on the efficacy of mindfulness in children with ADHD is still nascent. Short-term, high-frequency interventions for young children with ADHD draw on developmental psychology, child mindfulness meta-analyses and family mindfulness evidence. Developmental psychology shows that 6–9-year-olds have 10–15-minute attention spans, and prolonged tasks cause fatigue;7 thus, 5-minute twice-daily practice fits their attention, reduces barriers and boosts adherence. Child mindfulness meta-analyses indicate that short (5–10 minutes), high-frequency (≥1 session/day) practices have comparable or superior effects on attention and emotional impulsivity versus longer, lower-frequency practices, especially for younger children.9 Family mindfulness research adds that high-frequency practice strengthens the family mindfulness atmosphere, aiding integration into daily activities and generalisation.12 Current studies focus on individual symptoms, with limited family system research, insufficient simplified programmes for 6–9-year-olds, unclear medication–mindfulness interactions and few medicated and non-medicated subgroup analyses, hindering targeted guidance. Addressing these gaps, this study explores the impact of family mindfulness on core symptoms, family and social functioning in young children with ADHD and pharmacological treatment. Given ADHD’s negative impact on parents, the study extends to family therapy with parental mindfulness training, thereby examining the effects of mindfulness family training on children with ADHD and their families.
Based on the aforementioned research background and the Utetheisa kong case, this study addresses the following questions. (1) Does family mindfulness combined with pharmacotherapy better improve core symptoms (inattention, hyperactivity–impulsivity), social functioning (life skills, risk-taking, etc.) and family functioning in 6–9-year-old children with ADHD than pharmacotherapy alone? (2) Can family mindfulness indirectly improve ADHD symptoms by reducing parental anxiety and optimising family interactions?
Hypotheses: (1) family mindfulness combined with pharmacotherapy will more substantially improve core symptoms, social functioning and family functioning in young children with ADHD than pharmacotherapy alone; (2) family mindfulness mediates ADHD symptom improvement by reducing parental anxiety and enhancing family interaction quality.
Materials and Methods
Research Participants
Using convenience sampling, 43 children aged 6–9 years who met the inclusion and exclusion criteria at our hospital between 3 June and 3 July 2024 were selected and randomly assigned to the intervention group (22 cases) or the control group (21 cases). The inclusion criteria were as follows: (1) children aged 6–9 years; (2) a diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth/Fifth Edition, DSM-IV/V) by a doctor, with any score ≥6; (3) Chinese version of the Wechsler Intelligence Scale for Children: intelligence quotient ≥80. The exclusion criteria were as follows: (1) organic diseases of the nervous system, mental retardation, epilepsy, psychosis, auditory or visual abnormalities, generalised developmental disorders or other major neurological or psychiatric conditions; (2) prior treatment with mindfulness meditation.
Research Methods
Drug Intervention Protocol
Both groups received basic pharmacological intervention with the Chinese patent medicine Jingling Oral Liquid (Liaoning Dongfang Pharm. Co., Ltd., Drug Approval No. Z10910056), administered twice daily, one bottle each time. The intervention group additionally received family mindfulness meditation, whereas the control group received only the basic pharmacological intervention.
Family Mindfulness Meditation Intervention Programme
In addition to the pharmacological intervention, the intervention group received mindfulness meditation. Because children’s attention spans are short and they easily become bored, prolonged practice can cause stress. Therefore, this study developed a flexible practice plan: twice daily, 5 minutes per session, for a total of 21 days. Each session began with soothing music, followed by breathing training. Children were instructed to focus on their breath, slowly inhale and exhale and pay attention to the sensations at the nose. Throughout the exercise process, the researchers first guided the parents and children by demonstrating the procedures. After ensuring the parents had mastered the core steps, they were instructed to implement the practices at home according to their family circumstances. The specific training, supervision and compliance monitoring methods were as follows. The researchers provided standardised training to parents. Before the intervention, a 60-minute face-to-face session was conducted to explain the core principles of mindfulness meditation, strategies for addressing children’s attention characteristics (eg guiding language during distractions) and precautions for home practice. An illustrated manual was also distributed. During the intervention, weekly supervision was carried out via two WeChat video follow-ups (15–20 minutes each) to review practice records, address questions and correct improper practices (eg excessively demanding children’s focus). If practice was not completed for 3 consecutive days, the researchers made phone reminders to analyse the reasons and adjusted practice schedules if necessary (eg aligning with children’s routines by shifting sessions to the morning or bedtime). Family practice logs were used to record compliance. The parents documented daily practice duration, children’s cooperation level (rated 1–5, with 1 indicating no cooperation and 5 indicating full cooperation) and common occurrences (eg interruptions). After the intervention, compliance rates were calculated using the following formula: (actual completed sessions / expected sessions) × 100%, with ≥80% considered good compliance. During training, if a child’s mind drifted, they were encouraged to refocus attention and not blame themselves, as distraction is habitual. The specific training programme is detailed in Appendix 1.
Intervention Implementation and Quality Control
During the intervention, the intervention group received meditation, whereas the control group did not and maintained their medication without receiving any other treatment. The control group received only basic pharmacological treatment and did not participate in mindfulness meditation. After the intervention group completed the 21-day mindfulness meditation programme, the control group subsequently underwent the same meditation intervention to ensure that both groups ultimately received equal intervention opportunities. Medication regimens for both groups remained consistent throughout the study. In this research, assessments using the SNAP-IV scale, Weiss-P scale and Conners Parent Symptom Questionnaire (PSQ) scale were completed by parents, introducing certain limitations. Parents’ subjective perceptions of their children’s symptoms may have been influenced by their own emotional states, expectations regarding intervention outcomes and ADHD-related cognitions (eg some parents, concerned about medication, might exhibit a more positive evaluation bias towards symptom improvement in children not receiving medication). Additionally, it was not feasible to implement assessment blinding for parents, potentially introducing subjective bias. To minimise bias as much as possible, the study standardised assessment criteria through uniform instructions and required parents to base their ratings on their children’s actual behaviours within the 2 weeks before and after the intervention. Objective neuropsychological test results from the Integrated Visual and Auditory Continuous Performance Test (IVA-CPT) were also incorporated for cross-validation.
Observation Indicators
General Patient Data
The general data of patients and the effect evaluation indices before and after the intervention (the SNAP-IV scale, the Weiss-P functional defect scale, the PSQ parent symptom questionnaire and the IVA-CPT) were collected. The general demographic data of participants included gender, age, height, weight, intelligence and medication.
Evaluation Tools and Scales
The SNAP scale was developed in 1980 by Swanson, Nolan and Pelham et al based on the symptom descriptions in DSM-IV.12 It is mainly used as an evaluation tool for screening, auxiliary diagnosis, treatment efficacy and symptom improvement. It is divided into three versions: 18 items, 26 items and 90 items. The Chinese version of the SNAP-IV parent version was used in this study, comprising 26 items. Each item was scored on a four-point scale from 0 to 3: 0 = completely absent; 1 = mild; 2 = moderate; 3 = severe. The scale includes three subscales: the inattention scale (items 1–9), the hyperactivity–impulsivity scale (items 10–18) and the oppositional-defiant Scale (items 19–26), corresponding to attention, hyperactivity–impulsivity and oppositional defiance. Lower scores indicate milder ADHD symptoms. The internal consistency reliability of the SNAP-IV scale yielded a Cronbach’s alpha coefficient of 0.95 (0.92 for the inattention dimension and 0.90 for the hyperactivity–impulsivity dimension), with an intraclass correlation coefficient of 0.68 for test-retest reliability.12 All assessments were completed by parents.
The Weiss-P functional defect scale was developed by Canadian scholar Margaret Weiss based on the characteristics of ADHD symptoms. It is an assessment tool specifically for the social functioning of children with ADHD, providing a comprehensive measure of social function impairment. Chinese scholars Qian Ying et al13 introduced the scale and tested its reliability and validity. The results showed that the internal consistency reliability ranged from 0.70 to 0.92, and the test–retest reliability ranged from 0.61 to 0.87, indicating good reliability and validity.13 The scale comprises six dimensions: family, learning and school, life skills, self-management, social activities and risk-taking activities, with a total of 50 items. Each item is scored on a four-point scale: 0 = never, 1 = sometimes, 2 = often, 3 = always or frequently. The sum of the effective item scores for each dimension is divided by the number of applicable items. Items that are not applicable (expressed as N) are excluded from the total score calculation. Lower scores indicate better social functioning. All assessments were completed by parents.
The PSQ was developed by American scholar Conners in 1969 as a subscale of the Children’s Behaviour Scale. The original scale included 93 items, of which 48 were retained after revision. It was introduced into clinical use in China by Tang, H et al14 in the 1980s. The questionnaire is primarily used to assess behavioural problems in children and adolescents aged 3–17 years and is completed by parents. Each item is scored on a four-point scale from 0 to 3: 0 = no, 1 = very mild, 2 = moderate, 3 = severe. The questionnaire evaluates six factors: conduct problems, learning problems, psychosomatic problems, hyperactivity–impulsivity, anxiety and hyperactivity index. Lower scores indicate milder ADHD symptoms. The internal consistency reliability of the PSQ, measured by Cronbach’s alpha, was 0.93 (with the anxiety subscale at 0.87), and the test–retest reliability intraclass correlation coefficient was 0.59.15 All assessments were completed by parents.
Integrated Visual and Auditory Continuous Performance Test
The IVA-CPT is a computer-based testing system used for the clinical assessment of children with ADHD. By presenting repeated auditory and visual stimuli, the test observes and records children’s responses. The assessment is divided into four stages: warm-up, practice, main test and recovery, with the entire procedure lasting approximately 20 minutes. The computer automatically records reaction time, omissions, persistence and repeated responses, and it generates an evaluation using corresponding test quotient scores. The IVA-CPT criteria are as follows: a comprehensive attention quotient or comprehensive control quotient below 80 indicates a potential ADHD diagnosis. The test can also distinguish clinical subtypes of ADHD: (1) a response control quotient >85 with an attention quotient <80 indicates attention-deficit type; (2) a response control quotient <80 with an attention quotient >85 indicates hyperactive–impulsive type; (3) both response control and attention quotients <80 indicate mixed type. The IVA-CPT provides a more objective diagnostic method for ADHD in clinical practice. Jiang L et al16 administered the IVA-CPT alongside DSM-IV diagnosis in 130 children with ADHD, finding a sensitivity of 81.82% and a specificity of 88.10%. In this study, six comprehensive IVA-CPT quotients were selected: comprehensive control, attention quotient, visual control, auditory control, visual attention and auditory attention. All tests were completed by the children under the clinicians’ guidance.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 (IBM, Armonk, NY, USA). Normality was assessed with the Kolmogorov–Smirnov test. Measurement data that met the assumption of normality were expressed as mean ± standard deviation (x ± s). A mixed linear model, specifically a repeated measures analysis of variance (ANOVA), was employed to analyse pre- and post-intervention data. Time (pre- versus post-intervention) was treated as the within-participants factor, and group (intervention versus control) as the between-participants factor, with gender and age included as covariates. Pairwise comparisons within groups were adjusted using the Bonferroni correction, and between-group comparisons were conducted using simple effect analysis. A two-tailed P-value of <0.05 was considered statistically significant. Count data were expressed as frequency (n) or percentage (%) and analysed with the χ2-test. A two-sided P-value of <0.05 was considered statistically significant.
Results
General Information
This section aims to present the baseline participant characteristics (gender, age, medication status, etc.) of the two study groups and the results of intergroup balance tests. The results showed that there were 20 boys and 2 girls in the intervention group (12 on medication), with an average age of 7.59 ± 0.80 years. In the control group, there were 21 participants: 18 boys and 3 girls (10 on medication), with an average age of 7.48 ± 0.81 years. There was no significant difference in gender, age or BMI between the two groups (P > 0.05), as shown in Table 1.
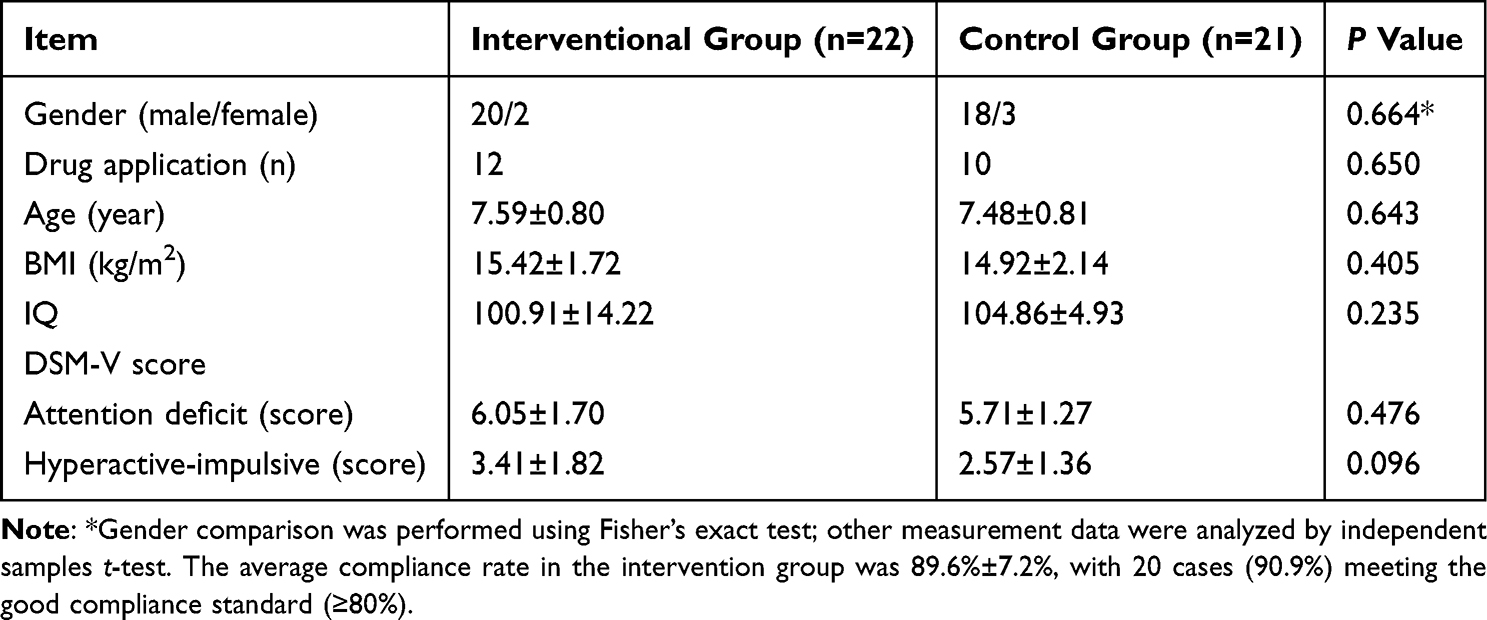 |
Table 1 Comparison of Baseline Data Between Intervention Group and Control Group |
Comparison of the Indicators Before and After the Intervention
This section employs repeated measures ANOVA to compare differences in core symptoms, social functioning and neuropsychological indicators between the two groups of children before and after the intervention while examining the time × group interaction effects. The results showed that there was no significant difference in the scores of each dimension of each scale between the two groups before the intervention (P > 0.05). Compared with pre-intervention, the intervention group showed improvements in the Weiss-P functional defect scale life skills (t = 2.89, df = 21), risk-taking activities (t = 3.12, df = 21), PSQ scale conduct problems, psychosomatic problems and IVA-CPT scale visual attention scores (P < 0.05). The control group demonstrated improvements in SNAP-IV hyperactivity–impulsivity (t = 2.35, df = 20) and PSQ scale psychosomatic problems (t = 2.19, df = 20) (all P < 0.05). The trend of core indicator changes in both groups is shown in Figure 1, with detailed data presented in Table 2. Analysis of covariance (ANCOVA) of the Weiss-P functional defect scale functional defect scale self-management dimension revealed that after controlling for gender and age, the score difference in the intervention group before and after the intervention. spilurus remained statistically significant (F = 4.32, P = 0.045), suggesting that mindfulness meditation’s improvement of self-management is independent of participant characteristics. The control group showed marginally significant score increases (F = 3.18, P = 0.082), possibly related to the limited impact of medication alone on self-management ability. Mixed ANOVA indicated significant time × group interaction effects for the Weiss-P functional defect scale life skills dimension (F = 5.12, P = 0.028), risk-taking behaviour dimension (F=6.35, P=0.015), PSQ scale conduct problems dimension (F = 4.89, P = 0.032) and IVA-CPT scale response control dimension (F = 7.21, P = 0.009). Simple effects analysis showed that the intervention group exhibited significant post-intervention improvements in life skills and conduct problems (P < 0.05), a greater reduction in risk-taking behaviour than the control group (P < 0.01) and a significant increase in response control scores (P < 0.05). The control group showed no significant changes in life skills or conduct problems, with a decline in response control scores (P < 0.05). These findings suggest that mindfulness meditation independently improves life skills and conduct problems, reduces risk-taking behaviour and reverses the decline in control ability. Figure 1 (focusing on intergroup differences at the same time point) shows the core indicator change trends of both groups, with detailed data in Table 2. To better visualise intragroup changes of key indicators before and after intervention, Figure 2 (line chart) presents the dynamic changes of four core dimensions (SNAP-IV inattention, the Weiss-P functional defect scale skills, PSQ conduct problems, IVA-CPT attention–visual) in both groups.
 |
Table 2 Comparison of Various Indicators Between the Intervention Group and the Control Group Before and After Intervention |
 |
Figure 1 Trend of changes in core indicators before and after intervention in the experimental group and control group (bar chart). Notes: *The indicator star indicates that there is a statistically significant difference (P < 0.05) in the measurement scores of a specific indicator before and after the intervention within the same group (intervention group or control group). |
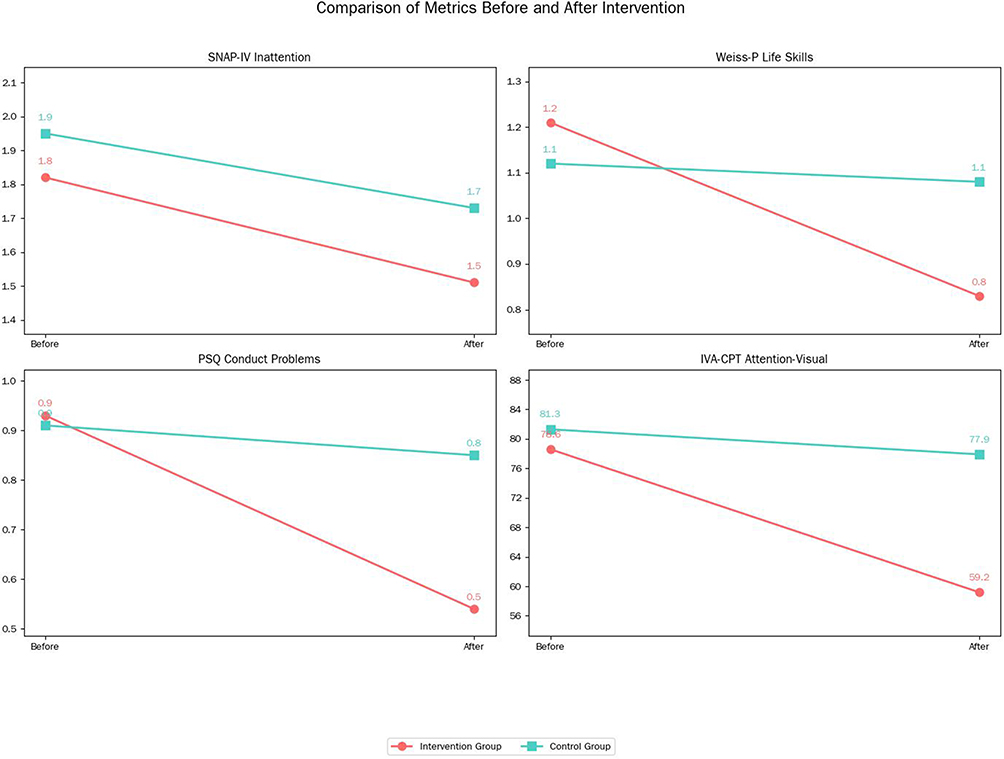 |
Figure 2 Line Chart of Pre-Post Intervention Comparisons Between Intervention Group and Control Group. |
Changes of Each Index Before and After the Intervention in Participants Receiving Medication
This section focuses on participants receiving medication, employing ANCOVA (controlling for parental anxiety levels) to compare intervention effects between the intervention and control groups. In the subgroup analysis, with parental anxiety levels and child age included as covariates, mixed ANOVA showed no significant differences in the scores of each dimension of each scale between the two groups before intervention (P > 0.05). Compared with the pre-intervention period, the intervention group showed improvements in the PSQ scale dimensions of conduct problems and psychosomatic problems (P < 0.05), as shown in Table 3. The mixed ANOVA revealed significant time × group interaction effects for both the conduct problems dimension (F = 4.36, P = 0.042) and the psychosomatic problems dimension (F = 5.02, P = 0.031) of the PSQ scale among participants receiving medication. Simple effects analysis demonstrated that the intervention group showed significantly lower conduct problem scores post-intervention than at baseline (P < 0.05), with significantly greater improvement in psychosomatic problem scores than the control group (P < 0.05). The control group exhibited no significant changes in either measure (P > 0.05). These findings suggest that mindfulness meditation combined with medication yields greater improvements in conduct problems than medication alone, enhancing the medication’s therapeutic effects on psychosomatic problems.
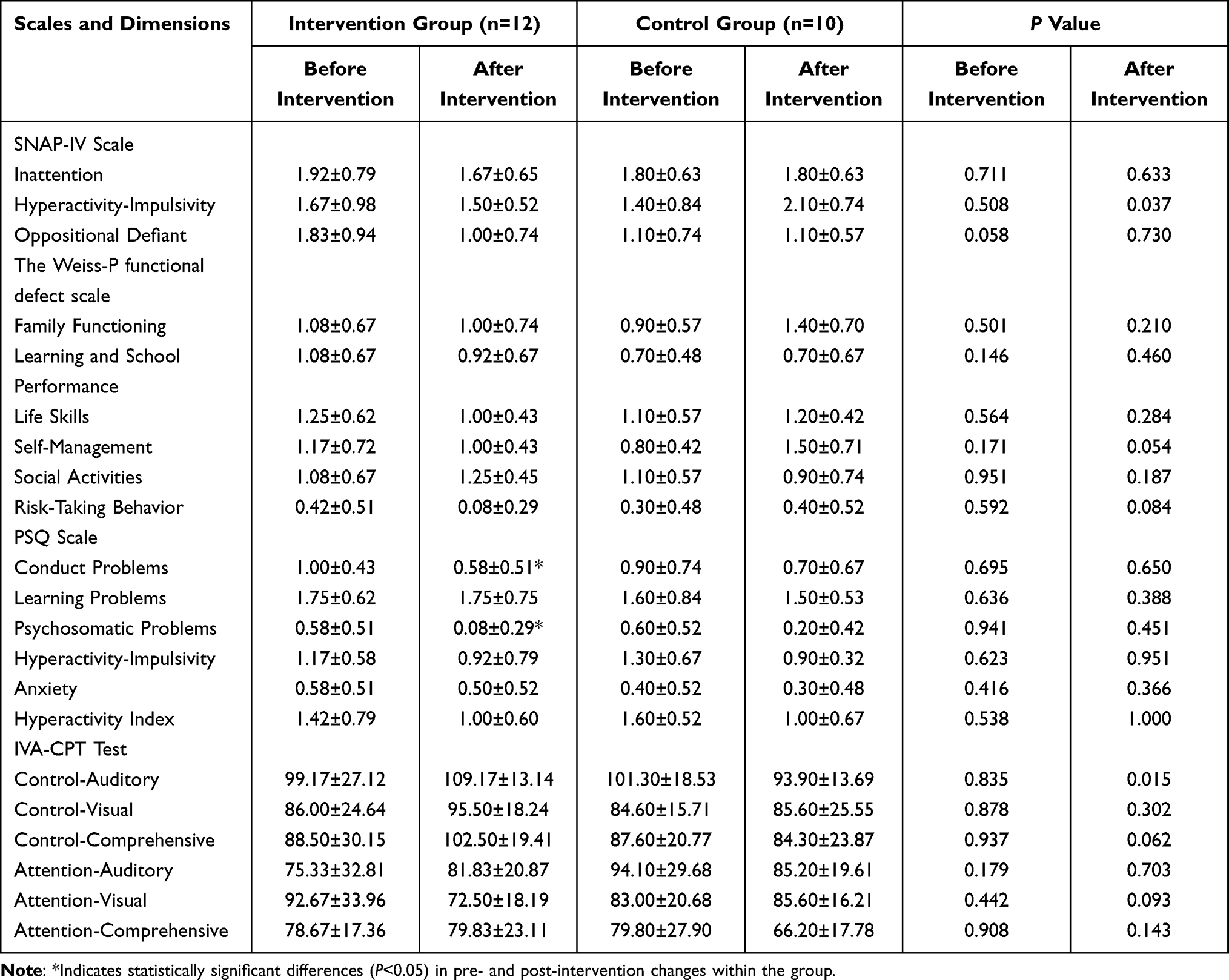 |
Table 3 Changes in Various Indicators Before and After Intervention in Subjects Taking Medication |
Changes in the Indicators Before and After Medication in the Control Group
This section focuses on participants in the control group receiving pharmacological intervention (medication alone without mindfulness meditation). With parental anxiety levels and child age included as covariates, ANCOVA was employed to compare differences in indicators before and after medication. Mixed ANOVA revealed no significant differences in scores across all scale dimensions between the two groups prior to intervention (P > 0.05). Compared with pre-medication, participants receiving medication in the control group showed considerable improvements in certain indicators, as shown in Table 4. Results indicated that participants receiving medication in the control group demonstrated significant improvements in the hyperactivity–impulsivity dimension of the SNAP-IV scale (P = 0.037) and the control–auditory dimension of the IVA-CPT (P = 0.015) compared with pre-medication. Marginally significant changes were observed in the self-management dimension (P = 0.054) and the hyperactivity index (P = 0.074) (0.05 < P < 0.10), whereas no statistically significant differences were found in other dimensions (P > 0.05).
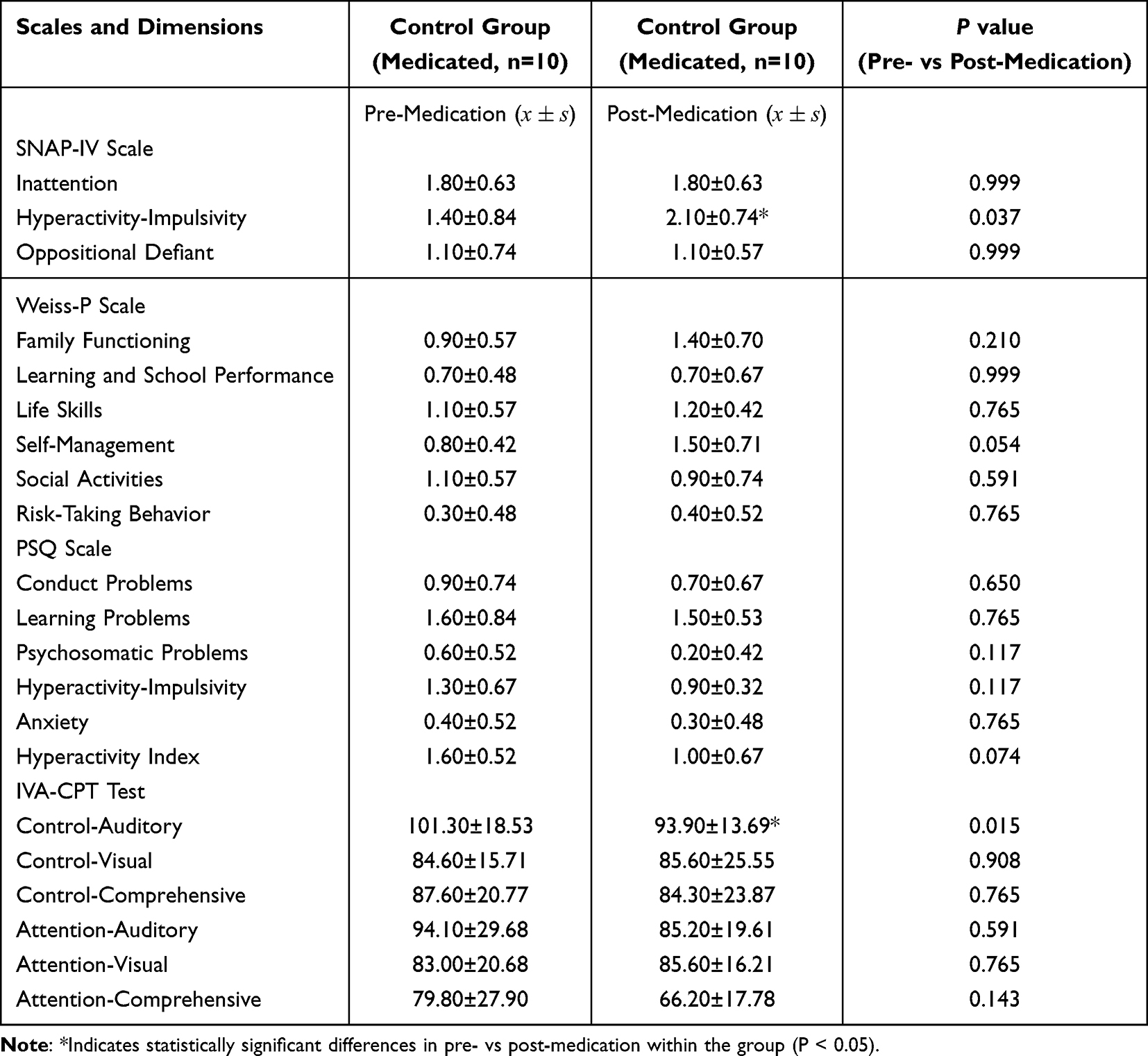 |
Table 4 Changes in Indicators Before and After Medication in the Control Group (Medication Alone Without Mindfulness Meditation) |
Discussion
In the intervention group, parents’ self-rating anxiety scale (SAS) scores decreased from 45.23 ± 5.67 before the intervention to 38.15 ± 4.21 after the intervention (P < 0.05), whereas parents’ SAS scores in the control group showed no significant change, decreasing from 44.89 ± 6.12 to 42.03 ± 5.89 (P > 0.05). Intergroup comparison revealed that post-intervention SAS scores in the intervention group were significantly lower than those in the control group (P < 0.05), indicating that family mindfulness meditation training can substantially reduce parental anxiety. Mixed ANOVA was employed to control for correlations in repeated measures data, reducing the risk of Type I errors caused by multiple t-tests and thereby producing more robust results. This study demonstrated that the involvement of family caregivers in mindfulness training can considerably improve core symptoms, social functioning and behavioural problems in younger children with ADHD. This study supplemented the assessment of parental mental health status using the SAS completed by parents. The results showed that in the intervention group, parental SAS scores decreased from 45.23 ± 5.67 before the intervention to 38.15 ± 4.21 after the intervention (P < 0.05), whereas in the control group, parental SAS scores decreased from 44.89 ± 6.12 to 42.03 ± 5.89 (P > 0.05). Intergroup comparison revealed that post-intervention SAS scores in the intervention group were significantly lower than those in the control group (P < 0.05), indicating that family mindfulness meditation training could substantially reduce parental anxiety. This finding aligns with the family systems theory perspective that “improved interaction patterns among members can positively influence individual emotional states”. Through participation in the training, parents not only enhanced their acceptance of their children’s symptoms but also improved their emotion regulation capacity through personal mindfulness practice.13 The results of the subgroup analysis showed that mindfulness meditation could effectively improve inattention on the SNAP-IV scale, psychosomatic problems on the PSQ scale and the response control score on the IVA-CPT scale in children with ADHD who were not receiving medication.
Current research consistently confirms that mindfulness meditation has ameliorative effects on ADHD symptoms in children. The core mechanism may be related to mindfulness training enhancing the regulatory function of the prefrontal cortex through sustained attentional focus exercises (such as breath observation), gradually improving individuals’ inhibitory control over distracting signals and flexibility in emotion regulation.17 For example, intervention studies targeting ADHD populations of different age groups (8–15 years) demonstrate that mindfulness training can improve alertness and executive control scores in the Attention Network Test by 15%–20%, with this effect being more pronounced in family-involved intervention models, echoing the improvements in social functioning dimensions such as life skills and risk-taking behaviours observed in this study. Furthermore, the positive impact of mindfulness training on parental emotions (eg reduced SAS scores among parents in the intervention group in this study) may establish a virtuous cycle of mindfulness–emotion–behaviour by optimising the quality of family interactions, which aligns with the perspective of “reshaping interaction patterns among members” in family systems theory.18 These effects were further confirmed in a 20-week, 60-minute-per-week randomised controlled trial, which showed that mindfulness meditation considerably improved attention-deficit symptoms in children with ADHD.19 Studies have also shown that mindfulness-based psychological interventions can improve hyperactive and impulsive behaviour in children with ADHD to a certain extent. Relevant research20 conducted an acceptance and commitment therapy intervention for nine children, once a week for 60 minutes over 8 weeks. The results showed that children’s experiential avoidance and hyperactive behaviours were substantially reduced. Researchers conducted an 8-week mindfulness course (1.5 hours per week) based on mindfulness-based stress reduction and mindfulness cognitive therapy for 22 children with ADHD aged 8–12 years and their parents. The results showed that, compared with the waitlist group, hyperactive and impulsive behaviour, as evaluated by parents in the intervention group, decreased considerably within 8 weeks after the intervention.18 In addition, 40 children aged 9–12 years underwent mindfulness yoga training for 8 weeks, 45 minutes per week. The results showed that, compared with the control group, hyperactivity and impulsivity symptoms in the training group were considerably reduced.21
The results of the neuropsychological IVA-CPT in this study showed significant differences between the groups in the two dimensions of vision control and response control. One possible reason is that SNAP-IV, as a subjective scale completed by parents to assess the core symptoms of children with ADHD, is influenced by factors such as parents’ understanding of their child, attitudes and expectations for the intervention. Because parents of children with ADHD often have concerns and negative emotions about drug treatment,22 they may adopt a more positive bias when assessing the core symptoms of untreated children. As a neuropsychological test, the IVA-CPT evaluates cognitive function to help determine the presence of ADHD. Participants are required to respond when a given target appears and to withhold responses to non-targets. Selective attention is measured by recording omissions or failures to respond to targets, whereas inhibitory control is assessed by recording commission errors when participants respond to non-targets, reflecting impulsive behaviour.23 The IVA-CPT results may also be influenced by participants’ intelligence, emotional state and sensory integration abilities.
Previous studies have also shown that ADHD is characterised by decreased frontal lobe function, which is mainly responsible for maintaining attention and control.24 Because the IVA-CPT requires attention from both the visual and auditory systems, it involves the ability to manage distractions.25 This ability is highly correlated with prefrontal cortex function26 and is particularly challenging for children with ADHD. Therefore, we speculate that this may explain why the IVA-CPT only found significant differences between groups in the medication group: drug therapy can improve children’s neurotransmitter levels, enhancing attention and response control,27 which allows children to perform better on visual and auditory tasks. Previous studies have also confirmed that children with ADHD receiving medication show varying degrees of improvement in CPT test performance compared with placebo.28 Consequently, attention should be paid to selecting test types and difficulty levels suitable for the characteristics and ability levels of children with ADHD when using the CPT.
In this study, marginally significant results (0.05 < P < 0.10) were observed in certain dimensions, such as the family function dimension of the the Weiss-P functional defect scale in the control group (P = 0.089) and the self-management dimension (P = 0.069). This may be related to insufficient statistical power due to the small sample size. It also suggests that these dimensions might show significant differences in larger samples. spilurus or could be influenced by potential confounding factors such as family interaction patterns, which require further validation in subsequent studies. Social function refers to the ability of individuals to demonstrate appropriate behaviour in different social roles,29 mainly reflected in learning, interpersonal communication and adaptation to the environment.30 In addition to core symptoms, children with ADHD often face learning problems, social adaptation difficulties, self-management challenges and family conflicts, all of which can seriously impair social function.31 Our study found that mindfulness meditation intervention can improve scores in the life skills and risk-taking dimensions, but no major effects were observed in other aspects. This may be related to the young age and gender imbalance of the sample recruited. This study also has some limitations. First, the sample size is small, and the majority of participants were boys, making it impossible to compare the effects across different ADHD subtypes and genders. This is mainly due to the difficulty of recruiting children with ADHD and the requirement to strictly follow the principle of randomisation. While this study acknowledges the limitation of a small sample size (n=43), the sample size was determined based on multiple practical and methodological considerations to ensure its rationality for an exploratory study on family mindfulness meditation for young children with ADHD (6–9 years old).First, the sample size aligns with that of similar exploratory/feasibility studies on ADHD mindfulness interventions.Second, a post-hoc power analysis using G*Power 3.1 was conducted to validate the statistical efficacy of the sample size. Based on the key significant findings of this study (eg, the group × time interaction effect for PSQ conduct problems, F=4.89, P=0.032), we estimated the effect size as Cohen’s f=0.35 (moderate effect, consistent with typical effect sizes of mindfulness interventions for ADHD symptoms [van der Oord et al, 2012]). Setting α=0.05 and statistical power (1−β)=0.8, the analysis showed that a total sample size of 36 participants (18 per group) would be required to detect such a moderate effect. The current sample size (43 participants) exceeds this threshold, indicating that the study had sufficient statistical power to identify the observed significant differences between groups—particularly given the use of a mixed linear model (repeated measures ANOVA) that controlled for confounding variables (gender, age) and reduced random error, further enhancing statistical efficiency.Third, the sample size was constrained by the practical challenges of recruiting participants for family-involved interventions. Children with ADHD aged 6–9 years require parental accompaniment for mindfulness practice, and eligible families must meet strict criteria. During the recruitment period (3 June–3 July 2024), a total of 51 families were initially screened, but 8 were excluded (3 due to comorbid epilepsy, 2 with prior mindfulness experience, 3 with IQ <80), resulting in a final sample of 43. This recruitment rate (84.3%) is relatively high for pediatric ADHD intervention studies, reflecting that the sample size was the maximum feasible within the study’s time frame and resource constraints.Finally, as an exploratory study, the primary objective was to preliminarily validate whether family mindfulness meditation (combined with medication) could improve core ADHD symptoms and social functioning, rather than to draw definitive population-level conclusions. The observed significant effects (eg, improvements in Weiss-P life skills, PSQ conduct problems, and IVA-CPT response control in the intervention group) confirm that the sample size was sufficient to provide preliminary evidence for the intervention’s potential—laying the groundwork for larger-scale randomized controlled trials in future research.
Due to the nature of mindfulness meditation interventions, it was not possible to implement complete blinding for parents, which may have influenced the results to some extent. This study employed a 21-day short-term intervention and observed substantial effects, but future research could consider extending the intervention period (eg to 8 or 12 weeks). On one hand, neuroplasticity studies indicate that mindfulness training has a cumulative effect on improving prefrontal cortex function, and long-term practice may further consolidate attention and emotion regulation abilities. On the other hand, follow-up studies show that behavioural intervention effects in children with ADHD are more likely to be stable when follow-ups exceed 3 months. Extending the intervention duration could assess the sustained effects of mindfulness training and long-term changes in family systems.28 The findings of this study align closely with the research objectives: mixed ANOVA confirmed that family mindfulness meditation improves core symptoms (inattention, hyperactivity/impulsivity), social functioning (life skills, risk-taking behaviours) and family functioning (parental anxiety) in young children with ADHD while also clarifying the regulatory role of medication on mindfulness effects, as children not taking medication showed more considerable improvement. This finding addresses a research gap regarding simplified mindfulness protocols for young populations with ADHD and provides empirical evidence to inform clinical decision-making regarding combined medication + mindfulness interventions. For families with low medication adherence or concerns about side effects, mindfulness meditation can serve as an effective supplementary approach.
Conclusion
In summary, simplified mindfulness meditation effectively ameliorates core ADHD symptoms—inattention, hyperactivity, and impulsivity—and enhances social functioning (life skills, risk-taking behaviors) in young children, while also reducing parental anxiety and improving family interaction. Concomitant medication may modulate these benefits.
Although the sample was small, male-skewed, and unblinded, mixed ANOVA controlled confounders and confirmed stable intervention effects. Future work should validate generalizability across sexes and ADHD subtypes in larger, more diverse cohorts; extend intervention duration to map dose–response curves; and optimize combined pharmacological-mindfulness protocols. Long-term follow-up is needed to verify durability.
The training can be integrated through multiple pathways. Clinically, pediatric or child-psychiatry outpatient units can embed standardized parent training into comprehensive ADHD management and push 2-min animated breathing videos via hospital social-media channels; PSQ psychosomatic scores can guide medication-mindfulness synergy at follow-up. In schools, 2-min group breathing breaks and after-school “mindfulness corners” with cartoon-guided props extend practice from home to classroom. A home-school-hospital tri-party manual can record cross-context performance (eg, classroom focus duration, bedtime cooperation), with clinicians periodically aggregating data to dynamically refine intervention strategies.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author (Nan Ji; Email: [email protected]).
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Xi’an Children’s Hospital. The participants is under the age of 16, written informed consent was obtained from the participant legal guardians.
Funding
Funding project: A historical cohort study on the effect of family mindfulness parenting and attention system training group courses on ADHD family intervention (2023D09).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Goldman LS, Genel M, Bezman RJ, et al. Diagnosis and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Council on scientific affairs, American medical association. JAMA. 1998;279(14):1100–1107. doi:10.1001/jama.279.14.1100
2. Holton KF, Nigg JT. The ASSOCIATION OF LIFESTYLE FACTORS and ADHD in children. J Attention Disord. 2020;24(11):1511–1520. doi:10.1177/1087054716646452
3. Diamond A. Executive functions. Ann Rev Psychol. 2013;64(1):135–168. doi:10.1146/annurev-psych-113011-143750
4. Gorman DA, Gardner DM, Murphy AL, et al. Canadian guidelines on pharmacotherapy for disruptive and aggressive behaviour in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder. Can J Psychiatry. 2015;60(2):62–76. doi:10.1177/070674371506000204
5. Smith BH, Barkley RA, Shapiro CJ. Attention Deficit Hyperactivity Disorder. New York: The Guilford Press; 2006:65–136.
6. Lee SS, Humphreys KL, Flory K, et al. Prospective association of childhood attention- deficit/hyperactivity disorder (ADHD) and substance use and abuse/dependence: a meta-analytic review. Clinic Psychol Rev. 2011;31(3):328–341. doi:10.1016/j.cpr.2011
7. Zylowska L, Ackerman DL, Yang MH, et al. Mindfulness meditation training in adults and adolescents with ADHD: a feasibility study. J Attention Disord. 2008;11(6):737–746. doi:10.1177/1087054707308502
8. Davidson RJ, Kaszniak AW. Conceptual and methodological issues in research on mindfulness and meditation. Am Psychologist. 2015;70(7):581. doi:10.1037/a0039512
9. Ren J, Huang L, Zhang ZX. Meditation calms people - people’s emotional responses to positive and negative emotional pictures can be reduced by meditation training. Acta Psychologica Sinica. 2012;44(10):1339. doi:10.3724/SP.J.1041.2012.01339
10. Lymeus F, Lindberg P, Hartig T. A natural meditation setting improves compliance with mindfulness training. J Environ Psychol. 2019;64:98–106. doi:10.1016/j.jenvp.2019.05.008
11. Fortney L, Taylor M. Meditation in medical practice: a review of the evidence and practice. Primary Care Clin Office Prac. 2010;37(1):81–90. doi:10.1016/j.pop
12. Zhou JB, Guo LT, Chen Y. Reliability and validity of the Chinese version of the SNAP-IV rating scale for attention deficit hyperactivity disorder-parental version. Chin Mental Health J. 2013;27:424–428. doi:10.3969/j.issn.1000-6729.2013.06.005
13. Qian Y, Du QX, Qu S, et al. Reliability and validity of the parental version of Weiss functional impairment scale. Chin Mental Health J. 2011;25:767–771. doi:10.3969/j.issn.1000-6729.2011.10.012
14. Tang HQ, Xin RE, Xu TY. Application study of the Conners’ Child Behavior Questionnaire (Revised Version). Shanghai Arch Psychiatry. 1993;4(4):246–248.
15. Fan J, Du YS, Wang LW. Study on Chinese urban norm and reliability of Conners Parent Symptom Questionnaire. Shanghai Arch Psychiatry. 2005;321–323. doi:10.3969/j.issn.1002-0829.2005.06.001
16. Jiang L, Su Y, Zhang W, et al. A comparative study of integrated audiovisual continuous performance test and DSM-IV in the diagnosis of attention deficit hyperactivity disorder. Chin J Child Health Care. 2004:388–390. doi:10.3969/j.issn.1008-6579.2004.05.007
17. Bögels SM, de Bruin EI, van der Oord S. Mindfulness-based interventions in child and adolescent psychopathology. In: Graham P, Reynolds S, editors. Cognitive Behaviour Therapy for Children and Families. New York: Cambridge University Press; 2013:371–384.
18. van der Oord S, Bögels SM, Peijnenburg D. The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J Child Fam Stud. 2012;21(1):139–147. doi:10.1007/s10826-011-9457-0
19. Jensen PS, Kenny DT. The effects of yoga on the attention and behavior of boys with attention-deficit/hyperactivity disorder (ADHD). J Atten Disord. 2004;7(4):205–216. doi:10.1177/108705470400700403
20. Murrell AR, Steinberg DS, Connally ML, et al. Acting out to acting on: a preliminary investigation in youth with ADHD and co-morbid disorders. J Child Family Stud. 2015;24(7):2174–2181. doi:10.1007/s10826-014-0020-7
21. Abadi MS, Madgaonkar J, Venkatesan S. Effect of yoga on children with attention deficit/hyperactivity disorder. Psychological Studies. 2008;53(2):154–159.
22. Oh Y, Joung YS, Jang B, et al. Efficacy of hippotherapy versus pharmacotherapy in attention-deficit/hyperactivity disorder: a randomized clinical trial. J AlternComplementary Med. 2018;24(5):463–471. doi:10.1089/acm.2017
23. Hall CL, Valentine AZ, Groom MJ, et al. The clinical utility of the continuous performance test and objective measures of activity for diagnosing and monitoring ADHD in children: a systematic review. Eur Child Adolesc Psychiatry. 2016;25(7):677–699. doi:10.1007/s00787-015-0798-x
24. Arnsten AFT. Toward a new understanding of attention-deficit hyperactivity disorder pathophysiology: an important role for prefrontal cortex dysfunction. CNS Drugs. 2009;23(Suppl 1):33–41. doi:10.2165/00023210-200923000-00005
25. Bonnel AM, Hafter ER. Divided attention between simultaneous auditory and visual signal. Percept Psychophysics. 1998;60(2):179–190. doi:10.3758/bf03206027
26. Loose R, Kaufmann C, Auer DP, et al. Human prefrontal and sensory cortical activity during divided attention tasks. Human Brain Mapp. 2003;18(4):249–259. doi:10.1002/hbm
27. Mechler K, Banaschewski T, Hohmann S, et al. Evidence-based pharmacological treatment options for ADHD in children and adolescents. Pharmacol Ther. 2022;230:107940. doi:10.1016/j.pharmthera.2021.107940
28. Fernández-Jaén A, Fernández-Mayoralas DM, Pardos A, et al. Clinical and cognitive response to extended-release methylphenidate (Medikinet) in attention deficit/hyperactivity disorder: efficacy evaluation. Advances in Therapy. 2009;26(12):1097–1110. doi:10.1007/s12325-009-0083-9
29. Priebe S. Social outcomes in schizophrenia. Br J Psychiatry Suppl. 2007;50(S50):s15–s20. doi:10.1192/bjp.191.50.s15
30. Du YS. Promoting social function improvement in children with attention deficit hyperactivity disorder. Chin J Child Health Care. 2010;18:265–266.
31. Yang L. Research status and prospect of attention deficit hyperactivity disorder in 2017-2019. Chin Mental Health J. 2020;34:594–601. doi:10.3969/j.issn.1000-6729.2020.7.008
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.