")
Back to Journals » International Journal of General Medicine » Volume 16
The Effectiveness of Tai Chi for Knee Osteoarthritis: An Overview of Systematic Reviews
Received 10 August 2023
Accepted for publication 22 September 2023
Published 4 October 2023 Volume 2023:16 Pages 4499—4514
DOI https://doi.org/10.2147/IJGM.S434800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Yuntian Ye,1,2 Aifeng Liu1,2
1Department of Orthopaedic Surgery, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, 300381, People’s Republic of China; 2National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, 300381, People’s Republic of China
Correspondence: Aifeng Liu, Department of Orthopaedic Surgery, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, No. 88 Changling Road, Xiqing District, Tianjin, 300381, People’s Republic of China, Tel +86-13803091533, Email [email protected]
Background: Knee Osteoarthritis (KOA) has become a serious health issue for elderly patients. Several systematic reviews (SRs) have reported Tai Chi has widely been used in the treatment of KOA. However, the methodology and conclusions of these SRs are controversial. This overview aims to summarize and evaluate the available evidence for the efficacy and safety of Tai Chi for KOA.
Methods: Two independent researchers searched eight databases from the inception to April 30, 2022. The included SRs were assessed respectively by A Measurement Tool to Assess Systematic Reviews (AMSTAR) 2, the Risk of Bias in Systematic Reviews (ROBIS) tool, and the Preferred Reporting Item for Systematic Review and Meta-analysis (PRISMA) statement. The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool was used to assess the quality of the included SRs in terms of outcome indicators.
Results: Six SRs were finally included in this overview. The results of methodological quality, reporting quality, and risk of bias of the included SRs were generally unsatisfactory. The limitations were a lack of explaining the reasons for selection, a list of excluded literature, reporting bias assessment, and reporting the potential sources of conflict of interest. In addition, only 1 item was assessed as moderate quality by using the GRADE tool. Limitations were the most common downgraded factors.
Conclusion: Tai Chi is effective as a non-pharmacological intervention in the integrative treatment of KOA. However, the quality of evidence and methodological quality of SRs is generally unsatisfactory, suggesting that these results must be interpreted with caution.
Trial Registration/Protocol Registration: PROSPERO registration number: CRD42022315146.
Keywords: Tai Chi, knee osteoarthritis, integrative treatment, systematic review, methodological quality
Introduction
Knee osteoarthritis (KOA) is a degenerative disease occurring mostly in middle-aged and elderly people.1 The main clinical manifestations of KOA are knee pain, limitation of movement, stiffness and swelling, and the disease is a major reason for mobility impairment and disability in the elderly.2 In terms of the pathogenesis of KOA, it is complex and characterized by progressive subchondral bone damage, synovitis, bone redundancy, and narrowing of the joint space. The number of people suffering from KOA has reached 250 million worldwide, which has a serious effect on the quality of life of patients and is a serious health problem in the current ageing society.3,4 The primary objectives in treating KOA involve relieving pain and enhancing joint function through physical, pharmaceutical, or surgical interventions. Specialists suggest taking the pathophysiological mechanisms of KOA seriously, adopting regular exercise, self-managing weight and avoiding surgery where possible.5 There is evidence in the literature that strength training, aerobic exercise and other exercise therapies are effective in reducing pain and swelling, enhancing knee stability, and reducing the progression of the disease in KOA patients.6,7 Thus, exercise therapy has been recommended in several clinical guidelines as an effective treatment for KOA.8,9
Tai Chi is a traditional Chinese health exercise. It combines meditation with slow, gentle movements, deep breathing, and total body relaxation. Tai Chi is effective on patients’ physical and mental health, strength and balance, fall prevention, or even on depression and self-efficacy.10–15 In line with specific guidelines, such as the ESCEO and OARSI 2019 guidelines, the OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis, and the 2019 American College of Rheumatology/Arthritis Foundation Guideline, Tai Chi is recommended as a therapeutic approach for KOA.5,8,9 Furthermore, a substantial body of clinical studies corroborates its beneficial effects.16–18 In recent years, several published randomized controlled trials (RCT) and systematic reviews (SRs) have demonstrated the advantages of Tai Chi for KOA patients. The methodological inconsistencies and controversial conclusions in systematic reviews limit their utility as therapeutic guides, with mixed findings regarding Tai Chi’s effectiveness in treating KOA and some studies indicating evidence quality issues. High-quality SRs can provide a reliable basis for clinical decision-making, and low-quality SRs can be misleading. Hence, an overview on SRs of Tai Chi for KOA is necessary to summarize the current evidence.19,20
The overview is a comprehensive collection and synthesis of SRs associated with the treatment or aetiology, diagnosis, and prognosis of the same disease or health problem.21 However, it should be noted that there is no overview concerning the benefits of Tai Chi to KOA. This overview applied the Assessment of Multiple Systematic Reviews 2 (AMSTAR 2) tool, Preferred Reporting Items for Systematic Reviews and Meta Analysis (PRISMA) statement, Risk of Bias (ROBIS) tool, and Grading of Recommendations Assessment, Development, and Evaluation (GRADE) tool to evaluate methodological quality, reporting quality, risk of bias, and the quality of evidence, for the purpose of analyzing the current state of evidence for Tai Chi for KOA and providing users with more targeted and reliable evidence.
Methods
Protocols and Registration
The protocol of this overview was pre-registered on the platform of PROSPERO (registration number: CRD42022315146). This study adheres to the requirements for SRs outlined in the “Preferred Reporting Items for Overviews of Reviews” (PRIOR) guideline.22
Search Strategy
Search methods included the computer search combined with the manual search. Two independent researchers searched PubMed, EMBASE, the Cochrane Library, the Web of Science, CNKI, SINOMED, WanFang, and Chongqing VIP database from the database inception to April 30, 2022. Languages were limited to Chinese and English. In addition, two researchers referred to the reference list of identified original or review articles and manually searched for further articles. Unpublished conference proceedings, newspapers, scientific results, and other gray literature were also collected. The keywords encompassed variations of “Tai Chi” and “Knee Osteoarthritis”, both individually and in various combinations. The search strategy was illustrated in Table 1 and Supplementary Material 1.
 |
Table 1 Search Strategy for PubMed Database |
Inclusion and Exclusion Criteria
(1) Type of Study: As RCTs are considered to offer high-quality evidence for evaluating interventions, SRs of RCTs reporting the impacts of Tai Chi on KOA were involved. SRs were reported using quantitative synthesis (meta-analysis) according to PRISMA guidelines, and studies were included if they were published in either Chinese or English. Additionally, a comprehensive search strategy is adopted, and 2 or more databases were used. (2) Type of Participants: Participants met the American College of Rheumatology diagnostic criteria for KOA, regardless of age, race or gender. (3) Type of Intervention: Tai Chi was applied as the main treatment in the test group. While the control group accepted standard care without Tai Chi, exercise, attention control, health education, or treatment. (4) Type of Outcome Measures: WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) scores, quality of life, health management, balance ability, walking speed, muscle force, the stair climb test, serious adverse events, the 6-min walking test, and the timed up and go test were used. (5) Exclusion Criteria: duplicate articles; non-SR; the control group was treated with Tai Chi.
Study Selection and Data Extraction
In the initial round, search-acquired articles were imported into Noteexpress 3.6, a literature management software, to eliminate duplicate articles. Two researchers independently read the abstract and title of the articles and eliminated the articles that were inconsistent with the study. In the second round, two researchers independently read the full text and eliminated the articles that met the exclusion criteria, such as articles for which the full text was not accessible. In the third round, the two researchers exchanged and checked the articles screened by each other, extracted key information from the finally screened articles and imported it into Microsoft Excel 2010 for sorting. Key information extraction involved: the author, country, included study type, number of originally included studies, the total number of included samples, intervention measures (experimental group and control group), outcome indicators, risk assessment tools for bias, and main conclusions. After the information is extracted and sorted out, the two researchers performed cross-check again. In the process of literature selection and data extraction and sorting out, if there is any disagreement between the two researchers, the information will be checked and unified by a third party immediately to ensure the information is correct.
Quality Assessment
The process of the quality assessment was performed independently by 2 investigators and cross-checked, with any disputes decided in consultation with a third investigator.
Evaluation of Methodological Quality
AMSTAR 2 tool23 was adopted for evaluating the methodological quality of included SRs by two researchers. That tool contains 16 entries, involving 7 key entries (2, 4, 7, 9, 11, 13, and 15). Each item was described as “yes”, “partially yes” and “no” as required. Finally, the methodological quality of the included SRs was evaluated, and the included studies were rated in four quality levels in accordance with the following criteria: “no or only 1 non-critical entry not conforming was rated as high quality” and “more than 1 non-critical entry non-conformity as medium quality”, “1 critical entry non-conformity with or without non-critical entry non-conformity as low quality” and “more than 1 critical entry non-conformity as very low quality”.
Reporting Quality Assessment
The quality of reports from the SRs of Tai Chi for KOA was evaluated using 27 entries from the PRISMA statement,24 which covers seven aspects of Title, Abstract, Introduction, Methods, Results, Discussion, and Funding of SRs. Two independent researchers described each item as “yes”, “partially yes” or “no”. The completion rate of each entry was reflected by the percentage.
Assessment of Evidence Quality
The GRADE system was used for assessing the evidence quality.25 Two researchers assessed the outcomes of each study based on Limitations, Inconsistency, Indirectness, Imprecision, and Publication Bias. The RCT study was pre-set as the highest grade of evidence in the evaluation, and the evidence quality was finally classified into four categories, namely high, medium, low and very low, according to the evaluation of the above five degradation factors.
Risk of Bias Evaluation
The ROBIS tool26 was applied to evaluate the risk of bias in the included SRs, using “yes”, “no” and “unclear” for each entry, and in the end, based on the overall evaluation results, each entry was evaluated regarding the risk of bias of the SRs. The tool evaluates the level of bias across 2 phases. The second phase includes four areas: inclusion-exclusion criteria for SRs, methods used for study retrieval and/or screening, methods used for data extraction and quality evaluation, and data synthesis and presentation of results. The third phase is risk of bias in the review.
Results
Literature Search and Literature Screening
The two researchers searched the literature independently according to the retrieval strategy. After comparison and discussion, 200 pieces of literature were initially obtained, and 124 pieces were finally obtained by excluding duplicate one. After reading titles and abstracts independently, 108 articles that did not satisfy the inclusion criteria, were removed by two researchers, followed by 6 SRs27–32 being selected after reading the full text. The literature selection procedure was shown in Figure 1.
 |
Figure 1 Literature selection procedure. |
Basic Information of the Included Literature
The 6 published SRs were included, when there were 3 pieces of English literature and 3 pieces of Chinese literature, whose authors were from China and Germany respectively. The number of included RCTs ranged from 5 to 16. The risk of bias assessment tool recommended in the Cochrane Handbook of Systematic Reviews was used in 5 SRs, and the Jadad quality score was adopted in 1 SR.29 Besides, the experimental group used Tai Chi as the primary intervention, while the control group accepted conventional treatment, except Tai Chi and no treatment, as the intervention. Table 2 presents the basic features of the included SRs.
 |
Table 2 Basic Characteristics of the Included SRs |
Methodological Quality Assessment
The results of the methodological quality assessed using the AMSTAR 2 tool were presented in Table 3. All incorporated SRs were evaluated as critically low quality. No SRs provided the protocol and reported inconsistencies with the protocol (item 2). In addition, all SRs used an incomprehensive literature search strategy (item 4), while none of them provided a list of excluded literature and reasons for exclusion (item 7). Only one SR29 did not use the recommended Cochrane assessment tool for risk of bias evaluation (item 9). All SRs have combined and analyzed the results using appropriate methods (item 11). One SR29 did not take the risk of bias of the included SRs into account when interpreting the results of the SRs (item 13). Only one SR32 adequately evaluated publication bias and discussed its possible impact on study results (item 15). In terms of non-critical items, no SR illustrated the reason for the type of study design included (item 3) and reported the source of funding for inclusion in the study (item 10). 2 SRs28,32 did not report a potential conflict of interest (item 16).
 |
Table 3 Results of the AMSTAR 2 Tool |
Risk of Bias Evaluation
The findings of the bias risk assessment performed by the ROBIS tool were displayed in Table 4 and Figure 2. In Domain 1 of Phase 2, all SRs were assessed as uncertain because of the absence of a predetermined protocol (study eligibility criteria). Due to lacking a comprehensive database search, all SRs were rated as high risk in the term of Domain 2 of Phase 2 (Identification and selection of studies). As for Domain 3 of Phase 2 (Data collection and study appraisal), three SRs27,28,30 were rated as low risk. One SR29 was rated as high risk because of using the Jadad scale to assess the risk of bias. Two SRs31,32 were rated as unclear because it was also uneasy to judge whether the two reviewers completed the RoB assessment process independently. In Domain 4, all SRs were categorized as high risk (synthesis and findings). Whether the data synthesis and analysis methods are determined in advance and followed cannot be judged. There is obvious bias in the original research. In addition, all SRs did not mention a predetermined protocol. Finally, all SRs were rated as high risk.
 |
Table 4 Results of the ROBIS Tool |
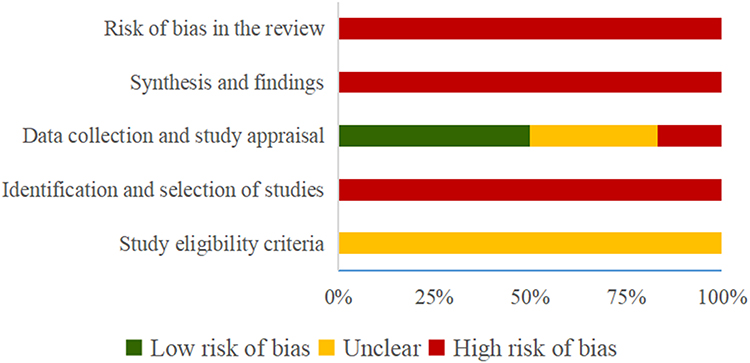 |
Figure 2 Risk of bias of the included SRs with ROBIS tool. |
Reporting Quality Assessment
The results of the PRISMA statement evaluation were displayed in Table 5. The introductions and discussions of the 6 SRs were well reported (100%). Nevertheless, some items, including item 2, 6, 7, 10, 11, 13, 14, 15, 16, 20, 24, 25, and 27, were reported to be insufficient (<50%).
 |
Table 5 Results of the PRISMA Assessment |
Assessment of Evidence Quality
Table 6 displayed the GRADE evidence quality rating results. There were 42 outcome indicators among the SRs that were included. The results showed a total of 38 as critically low quality, 3 as low-quality evidence, only 1 as moderate-quality evidence and no high-quality evidence. The most significant evidence downgrading factors were limitations (100%), followed by imprecision (92.8%), publication bias (69%), inconsistency (66.7%), and indirectness (0%).
 |
Table 6 Results of the GRADE Tool |
Observation Index and Efficacy Evaluation
The information involved in the SR was summarized, as shown in Table 6.
Pain Reduction
In fact, 5 SRs27–30,32 reported that Tai Chi could obviously reduce the WOMAC Pain scale. The maximum sample size of SR30 included 14 RCTs with 877 samples (SMD −0.69,95% CI −0.95; −0.44). 1 SR27 suggested that Tai Chi had no significant effect on the long-term WOMAC Pain scale in relative to the control group (SMD −0.29,95% CI −1.06;0.48).
Physical Function Reduction
In total, 6 SRs27–32 demonstrated that Tai Chi could significantly lower the WOMAC Physical function scale. The maximum sample size of SR30 included 13 RCTs with 844 patients (SMD: −0.92; 95% CI: −1.16; −0.69). Meanwhile, 1 SR27 displayed that Tai Chi had no significant effect on the long-term WOMAC Physical function scale (SMD: −0.33; 95% CI: −0.95; 0.28).
Stiffness Improvement
Moreover, 5 SRs27–30,32 reported that Tai Chi could significantly reduce the WOMAC stiffness scale. The maximum sample size of SR30 included 12 RCTs with 769 patients (SMD: −0.65; 95% CI: −0.98; −0.33). Whereas, 1 SR27 mentioned that Tai Chi had no significant effect on the long-term WOMAC stiffness scale in relative to the control group (SMD: 0.06; 95% CI: −0.72; 0.833).
Quality of Life Improvement
In this aspect, 3 SRs27,28,30 showed that Tai Chi can improve the physical quality of life to a great extent. The maximum sample size of SR30 included 5 RCTs with 409 patients (SMD: 0.48; 95% CI: 0.28; 0.68). Besides, 2 SRs27,30 displayed that Tai Chi could noticeably enhance mental quality of life. Moreover, 1 SR28 reported that Tai Chi made no significant impact on improving mental quality of life (SMD: 0.35; 95% CI: −0.31; 1.01).
Test Outcome
In terms of test outcome, 4 SRs28–32 pointed out a significant improvement on 6-min Walk Test results with Tai Chi. The maximum sample size of SR30 included 6 RCTs with 426 patients (SMD 0.55,95% CI 0.10;0.99). Besides, 3 SRs30–32 reported a significant improvement in the timed up and go test results with Tai Chi. The maximum sample size of SR31 included 6 RCTs with 306 patients (SMD: −0.89; 95% CI: −1.16; −0.61). Additionally, 2 SRs28,30 showed a significant improvement in balance score with Tai Chi. The maximum sample size of SR included 4 RCTs with 175 patients (SMD: 0.69; 95% CI: 0.38; 0.99). Furthermore, 1 SR29 reported a significant improvement on the stair climb test with Tai Chi (SMD: −0.69; 95% CI: −1.34; −0.15), while 1 SR30 suggested that after the intervention of Tai Chi exercise, the depression (SMD: −0.46; 95% CI: −0.68; −0.24) and arthritis self-efficacy (SMD: 0.27; 95% CI: 0.06; 0.48) in KOA patients are significantly enhanced. In addition, in 1 SR,28 an obvious improvement in walking speed was observed by practicing Tai Chi (SMD: 0.57; 95% CI: 0.11; 1.02).
Other Outcomes
Considering other outcomes, 1 SR28 reported that Tai Chi had no significant impact on improving knee flexor muscle force (SMD: 0.40; 95% CI: −0.46; 1.25), knee extensor muscle force (SMD: 0.23; 95% CI: −0.17; 0.63), and BMI (SMD: −0.13; 95% CI: −0.46; 0.21).
Safety
In 4 SRs,27–30 it was concluded that Tai Chi is a safe therapy for KOA. Besides, 1 SR29 reported that Tai Chi was featured with better safety in relative to the control group (SMD: −0.63; 95% CI: −0.98; −0.27), while 3 SRs27,28,30 mentioned that there were no adverse events related to Tai Chi exercise.
Discussion
Summary of the Main Results
The present study is the first overview of SRs of Tai Chi for KOA. AMSTAR2, PRISMA statement, ROBIS tool, and GRADE were adopted to assess methodological quality, reporting quality, risk of bias and quality of evidence to offer a foundation for clinical decision-making. The result of the Amstar 2 tool indicated that all SRs are rated as critically low quality due to the presence of one and more key items which were not compliant. The result of the PRISMA statement was unsatisfactory, while that of the ROBIS tool showed hat all SRs are classified as high risk of bias. Besides, 38 outcome indicators (90.5%) were critically low quality assessed by the GRADE tool. Although most outcome indicators showed benefits of Tai Chi for KOA, the main findings decreased the credibility of Tai Chi for KOA.
Implications for Further Study
AMSTAR2 and PRISMA statement results pose some challenges to SR producers. SR should be registered in advance in the PROSPERO platform. Producers should explain any deviations from the protocol at the time of implementation, which can increase the rigour of SR, whose producers should set up a comprehensive literature search strategy that does not miss the search for gray literature, which can lower publication bias. It is also necessary to provide a list of excluded literature and reasons for exclusion. Producers should illustrate their selection of the study designs for inclusion in the review, and researchers should describe the potential sources of funding and conflicts of interest of the original study, declare the role of the funder in the research process and increase the transparency of the study. Furthermore, researchers should assess the risk of bias in the included literature, and for studies with high heterogeneity, subgroup analysis and sensitivity analysis, where necessary, were conducted to explore the sources of heterogeneity and explain the reasons for it, to make the combined results more reliable. From this overview, it was found that the original studies in the included SR generally had a large heterogeneity of intervention protocols, which could be due to the type of Tai Chi, frequency of exercise, the treatment period, etc. Differences in interventions can have a major impact on outcomes. Thus, future clinical investigators should adhere to reporting specifications to adequately describe the intervention protocol. Evidence users need to consider whether the above factors make an impact on study outcomes and reporting, and do not exclude the possibility that the actual trial design and operation met the evaluation criteria, but were not reported, resulting in a lower score. The ROBIS tool is more focused on the flaws or limitations in the design, production, and analysis of SRs than AMSTAR 2 and PRISMA. AMSTAR 2 evaluation of high-quality literature may also have a high risk of bias assessment using ROBIS.33 Therefore, using AMSTAR 2 and PRISMA in combination with ROBIS for the evaluation of SRs, both can complement each other and be more comprehensive.
The clinical efficacy of Tai Chi for KOA and the SRs included in this paper demonstrate a positive impact. However, the quality of the evidence was unsatisfactory in terms of evaluating the reliability of individual outcome indicators. The GRADE quality grading results indicated that the quality of evidence for only one outcome indicator was shown to be intermediate, with the rest being low or very low evidence and no high evidence. As a result, the conclusions of the SRs may be biased from the true picture and have limited relevance as a guide to clinical practice. As for limitations, they are the most downgraded factor, indicating that the original studies included in the SRs were flawed in terms of randomization, blinding, and concealment. Secondary causes are Imprecision (92.9%), Publication bias (69.0%) and Inconsistency (66.7%). The inclusion of relatively few patients and observed events in the original studies resulted in wide confidence intervals, reducing the quality of the SR evidence for Tai Chi for KOA. Besides, some of the SRs searched the literature incompletely and ignored some unpublished literature with negative outcomes, leading to a large publication bias for outcome indicators. In addition, researchers should conduct tests for heterogeneity, but when heterogeneity is high, its source should be identified where possible, and subgroup analysis should be carried out for appropriate interpretation and discussion based on specific clinical conditions. As secondary studies, the quality of evidence from SRs is directly influenced by factors such as the design and implementation of the original study. Methodological training for clinical researchers should be strengthened at the source to synchronize and improve the quality of clinical trials. In addition, quality analysis and evaluation of primary studies in this field can be performed in the future, focusing on improving the quality of clinical primary studies, and also standardizing SR research methods to offer a more scientific and reliable basis for evidence-based medicine.
Mechanism of Tai Chi in the Treatment of KOA
Tai Chi can lower pain, relieve joint stiffness, and increase joint mobility in KOA.34–37 Tai Chi activates neuroendocrine and autonomic functions, elicits behavioural responses through neurochemical secretion and analgesic pathways, modulates the inflammatory response of the immune system and reduces sensitivity to chronic pain.38,39 It has been proposed that Tai Chi is a training modality accompanied by neuromuscular control, with a specific gait pattern of varying degrees of knee flexibility during the process, prompting a normalization of their abnormal gait and improving the symptoms of pain and stiffness in KOA patients.40 The highest knee joint reaction force during Tai Chi training is equivalent to 1.2 times the body mass, which is obviously less than the joint reaction force during walking (3–4 times the body mass), which shows that Tai Chi exercises are characterized by low impact forces and low loading rates.41,42 This feature allows the patient to exercise without causing knee pain due to overload, but also to strengthen the muscles around the knee and promote the remodelling of the normal biomechanical mechanisms of the muscles around the knee. The primary reason KOA patients seek medical treatment is for painful symptoms. Arthritis discomfort and functional restrictions make a negative effect on patients’ quality of life. As a result, in many studies, the improvement of Tai Chi on KOA pain has been used as the primary indicator, which affects the generalization of results to some degree. The included literature outcome indicators did not consider recurrence rates, and only 1 SR reported follow-up period effects, mainly reporting short-term results and being unable to judge follow-up period efficacy. In addition, only 4 SRs reported adverse effects. Therefore, detailed and standardized safety indicators need to be mentioned in SRs of Tai Chi for KOA. Based on the available evidence, Tai Chi has great potential to lower KOA pain, relieve joint stiffness and improve joint function, while its effectiveness and safety still need to be verified by more high-quality RCTs.
Limitations
The overview was conducted based on a pre-registered protocol, but there are still some limitations. The final number of SRs included in this study was small, which may result in bias. In addition, the language of the search was restricted to Chinese and English, which may have caused the omission of some documents. The types of studies included here were all RCT, which may also result in bias in the results. Some key outcomes, such as the effective rate, cure rate, and visual analog scale (VAS), were not reported in the primary studies being analyzed. Our reliance on published studies introduces the possibility of selection bias, as we were unable to control for variations in methodologies or data reporting among individual studies. This factor could influence the robustness of our synthesized findings. In general, the results of this study were highly subjective, and only qualitative analysis was made. Although they passed repeated cross-referencing, the subjectivity of the results could not be avoided.
Conclusion
To conclude, Tai Chi may be an effective therapy for the treatment of KOA patients with a good safety profile. However, the results of methodological quality, reporting quality, ROB quality and evidentiary quality of the involved research are unsatisfactory. It is challenging to provide effective evidence for the formulation of guidelines for KOA treatment. Clinicians should be cautious when using this evidence to make clinical decisions. In the future, in terms of original research, it is still essential to conduct multi-centre and large-sample randomized controlled trials, improve the trial design, control the bias, and establish a unified clinical efficacy index. Besides, for SR producers, they should follow strict quality assessment criteria and guidelines to enhance the quality of SRs and to provide a higher level of evidence-based medical evidence.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (NO. 81873316), Tianjin Administration of Traditional Chinese Medicine rehabilitation appropriate technology project (The application and popularization of sports prescription based on traditional work method in the treatment of spondyloarthropathy) and the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2022-JKCS-07).
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Pigeolet M, Jayaram A, Park KB, Meara JG. Osteoarthritis in 2020 and beyond. Lancet. 2021;397(10279):1059–1060. doi:10.1016/s0140-6736(21)00208-7
2. Sharma L, Solomon CG. Osteoarthritis of the KNEE. N Engl J Med. 2021;384(1):51–59. doi:10.1056/NEJMcp1903768
3. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/s0140-6736(19)30417-9
4. Yue L, Berman J. What is osteoarthritis? JAMA. 2022;327(13):1300. doi:10.1001/jama.2022.1980
5. Arden NK, Perry TA, Bannuru RR, et al. Non-surgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. Nat Rev Rheumatol. 2021;17(1):59–66. doi:10.1038/s41584-020-00523-9
6. Mazzei DR, Ademola A, Abbott JH, Sajobi T, Hildebrand K, Marshall DA. Are education, exercise and diet interventions a cost-effective treatment to manage hip and knee osteoarthritis? A systematic review. Osteoarthritis Cartilage. 2021;29(4):456–470. doi:10.1016/j.joca.2020.10.002
7. Nelligan RK, Hinman RS, Kasza J, Crofts SJC, Bennell KL. Effects of a self-directed web-based strengthening exercise and physical activity program supported by automated text messages for people with knee osteoarthritis: a randomized clinical trial. JAMA Intern Med. 2021;181(6):776–785. doi:10.1001/jamainternmed.2021.0991
8. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
9. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol. 2020;72(2):220–233. doi:10.1002/art.41142
10. Urits I, Schwartz RH, Orhurhu V, et al. A comprehensive review of alternative therapies for the management of chronic pain patients: acupuncture, Tai Chi, osteopathic manipulative medicine, and chiropractic care. Adv Ther. 2021;38(1):76–89. doi:10.1007/s12325-020-01554-0
11. You T, Ogawa EF, Thapa S, et al. Effects of Tai Chi on beta endorphin and inflammatory markers in older adults with chronic pain: an exploratory study. Aging Clin Exp Res. 2020;32(7):1389–1392. doi:10.1007/s40520-019-01316-1
12. Zhang YH, Hu HY, Xiong YC, et al. Exercise for neuropathic pain: a systematic review and expert consensus. Front Med. 2021;8:756940. doi:10.3389/fmed.2021.756940
13. Zhou M, Zhou D, He L. A randomized trial of tai chi for fibromyalgia. N Engl J Med. 2010;363(23):2265; author reply 2266–2267. doi:10.1056/NEJMc1010478
14. Wang YT, Goh CH, Liao T, et al. Effects of wheelchair Tai Chi ball exercise on physical and mental health and functional abilities among elderly with physical disability. Res Sports Med. 2021;29(3):289–302. doi:10.1080/15438627.2020.1777553
15. Leung LYL, Tam HL, Ho JK. Effectiveness of Tai Chi on older adults: a systematic review of systematic reviews with re-meta-analysis. Arch Gerontol Geriatr. 2022;103:104796. doi:10.1016/j.archger.2022.104796
16. Chwan-Li S, John WN, Moamen ME, et al. Tai Chi exercise reduces circulating levels of inflammatory oxylipins in postmenopausal women with knee osteoarthritis: results from a pilot study. Front Med. 2023. doi:10.3389/fmed.2023.1210170
17. Haibo L, He G, Peng C, Le Z, Haipeng C, Yubo F. Biomechanical effects of typical lower limb movements of Chen-style Tai Chi on knee joint. Med Biol Eng Comput. 2023. doi:10.1007/s11517-023-02906-y
18. Ho KKW, Pong G, Poon QW, et al. A community-centric multi-disciplinary education program with the 8-section brocade Tai Chi therapy for patients with osteoarthritis of the knee – a pilot study. BMC Complement Altern Med. 2021;21(1). doi:10.1186/s12906-021-03480-2
19. Fanaroff AC, Califf RM, Lopes RD. High-quality evidence to inform clinical practice. Lancet. 2019;394(10199):633–634. doi:10.1016/s0140-6736(19)31256-5
20. Yao L, Guyatt GH, Djulbegovic B. Can we trust strong recommendations based on low quality evidence? BMJ. 2021;375:n2833. doi:10.1136/bmj.n2833
21. Ranson MK, Evans DB. Taking health systems research syntheses to the next level: overviews of systematic reviews. Cochrane Database Syst Rev. 2017;9(9):Ed000123. doi:10.1002/14651858.Ed000123
22. Pollock M, Fernandes RM, Pieper D, et al. Preferred Reporting Items for Overviews of Reviews (PRIOR): a protocol for development of a reporting guideline for overviews of reviews of healthcare interventions. Syst Rev. 2019;8(1):335. doi:10.1186/s13643-019-1252-9
23. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
25. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
26. Whiting P, Savović J, Higgins JP, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
27. Lauche R, Langhorst J, Dobos G, Cramer H. A systematic review and meta-analysis of Tai Chi for osteoarthritis of the knee. Complement Ther Med. 2013;21(4):396–406. doi:10.1016/j.ctim.2013.06.001
28. Xie Y, Wei G, Guo Y, et al. Tai Chi in treatment of knee osteoarthritis: a systematic evaluation and meta-analysis. Chin J Rehabil Med. 2015;30(05):483–489. doi:10.3969/j.issn.1001-1242.2015.05.016
29. Chang WD, Chen S, Lee CL, Lin HY, Lai PT. The effects of Tai Chi Chuan on improving mind-body health for knee osteoarthritis patients: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2016;2016:1813979. doi:10.1155/2016/1813979
30. Hu L, Wang Y, Liu X, et al. Tai Chi exercise can ameliorate physical and mental health of patients with knee osteoarthritis: systematic review and meta-analysis. Clin Rehabil. 2021;35(1):64–79. doi:10.1177/0269215520954343
31. You Y, Liu J, Tang M, Wang D, Ma X. Effects of Tai Chi exercise on improving walking function and posture control in elderly patients with knee osteoarthritis: a systematic review and meta-analysis. Medicine. 2021;100(16):e25655. doi:10.1097/md.0000000000025655
32. Wang L, Xie X, Guo Y, Qiu K. A meta-analysis of the effect of tai chi practice on the treatment of patients with osteoarthritis of the knee. Sports Res Educ. 2022;37(01):89–96. doi:10.16207/j.cnki.2095-235x.2022.01.015
33. Gómez-García F, Ruano J, Gay-Mimbrera J, et al. Most systematic reviews of high methodological quality on psoriasis interventions are classified as high risk of bias using ROBIS tool. J Clin Epidemiol. 2017;92:79–88. doi:10.1016/j.jclinepi.2017.08.015
34. Kelley GA, Kelley KS, Callahan LF. Clinical relevance of Tai Chi on pain and physical function in adults with knee osteoarthritis: an ancillary meta-analysis of randomized controlled trials. Sci Prog. 2022;105(2):368504221088375. doi:10.1177/00368504221088375
35. Chen PY, Song CY, Yen HY, et al. Impacts of tai chi exercise on functional fitness in community-dwelling older adults with mild degenerative knee osteoarthritis: a randomized controlled clinical trial. BMC Geriatr. 2021;21(1):449. doi:10.1186/s12877-021-02390-9
36. Zhu Q, Zhou X, Zhang S, Fang M, Li JX. Joint angles and joint moments of the lower limbs in four typical Tai Chi movements: consideration for management of knee osteoarthritis. Res Sports Med. 2021;29(6):586–592. doi:10.1080/15438627.2021.1975118
37. Hu X, Lai Z, Wang L. Effects of Taichi exercise on knee and ankle proprioception among individuals with knee osteoarthritis. Res Sports Med. 2020;28(2):268–278. doi:10.1080/15438627.2019.1663520
38. Irwin MR, Cole SW. Reciprocal regulation of the neural and innate immune systems. Nat Rev Immunol. 2011;11(9):625–632. doi:10.1038/nri3042
39. Morgan N, Irwin MR, Chung M, Wang C, Bacurau RFP. The effects of mind-body therapies on the immune system: meta-analysis. PLoS One. 2014;9(7):e100903. doi:10.1371/journal.pone.0100903
40. Decoux B, Kovaleski JE, Liu W. Cumulative loading of the medial compartment of the knee joint during Tai Chi gait in patients with knee osteoarthritis. Osteoarthritis Cartilage. 2015;23(2):A106. doi:10.1016/j.joca.2015.02.820
41. Zhang Z, Huang L, Liu Y, Wang L. Effect of Tai Chi training on plantar loads during walking in individuals with knee osteoarthritis. Biomed Res Int. 2020;2020:3096237. doi:10.1155/2020/3096237
42. Wang XQ, Huang LY, Liu Y, et al. Effects of tai chi program on neuromuscular function for patients with knee osteoarthritis: study protocol for a randomized controlled trial. Trials. 2013;14(1):375. doi:10.1186/1745-6215-14-375
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.