Back to Journals » Journal of Pain Research » Volume 19
The Effectiveness of Huangkui Lianchang Decoction Enema Solution Compared with Mesalazine Enema for Mild-to-Moderate Active Distal Ulcerative Colitis: Study Protocol of a Multicenter, Prospective, Randomized Controlled Trial
Authors Zhu Y, Wang R ![]() , Ding H, Li H, Zhao Y, Chen K, Zeng T, Ma Y, Chen C, Bu Z, Zhang J, Yang Y
, Ding H, Li H, Zhao Y, Chen K, Zeng T, Ma Y, Chen C, Bu Z, Zhang J, Yang Y ![]() , Chen Y
, Chen Y ![]()
Received 13 October 2025
Accepted for publication 13 January 2026
Published 5 February 2026 Volume 2026:19 574028
DOI https://doi.org/10.2147/JPR.S574028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yijia Zhu,1,2,* Rong Wang,3,* Haoyu Ding,1,2 Hong Li,4 Yang Zhao,1,2 Kailan Chen,1,2 Tian Zeng,1,2 Yimeng Ma,1 Chen Chen,1 Zhijun Bu,1,2 Jianghai Zhang,4 Ye Yang,5 Yugen Chen6– 8
1The Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 2No. 1 Clinical Medical College, Nanjing University of Chinese Medicine, Nanjing, 210023, People’s Republic of China; 3School of Chinese Medicine, Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 4Jiangsu Jiuxu Pharmaceutical Co. Ltd., Huai’an, 223002, People’s Republic of China; 5School of Medicine, Nanjing University of Chinese Medicine, Nanjing, 210023, People’s Republic of China; 6Department of Colorectal Surgery, The Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 7Jiangsu Province Key Laboratory of Tumor Systems Biology and Chinese Medicine, The Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 8Jiangsu Collaborative Innovation Center of Chinese Medicine in Prevention and Treatment of Tumor, The Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ye Yang, School of Medicine, Nanjing University of Chinese Medicine, Nanjing, 210023, People’s Republic of China, Email [email protected] Yugen Chen, Department of Colorectal Surgery, The Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, 210029, People’s Republic of China, Email [email protected]
Introduction: Traditional Chinese medicine enemas have been widely utilized in clinical practice due to their rapid and effective relief of symptoms such as bloody stools and abdominal pain in ulcerative colitis (UC), sustained therapeutic effectiveness, and low cost. The objective of this multicenter, unblinded randomized controlled trial (RCT) is to evaluate whether the effectiveness and safety of HKE are comparable to those of Mesalazine enemas. Evidence from observational studies is of insufficient quality, underscoring the need for randomized controlled trials to strengthen the reliability and validity of the findings.
Methods and Analysis: Eight hospitals in Jiangsu Province with Good Clinical Practice (GCP) certification will recruit patients with mild to moderate active rectal or left-sided colonic UC and randomly assign them in a 1:1 ratio to the Huangkui Lianchang decoction Enema (HKE) treatment group and the mesalazine enema treatment group. All participants received oral Mesalazine enteric-coated tablets. Enema treatment is administered for 8 weeks. Eighty-six patients are recruited for each group. Clinical events are monitored throughout the treatment and follow-up periods. The primary outcome is the modified Mayo score, assessed at baseline and post-treatment (on Day 56 ± 7). This score is used to evaluate both clinical outcomes (clinical remission and response rates) and endoscopic outcomes (endoscopic response and mucosal healing rates). Secondary outcomes include improvements in traditional Chinese medicine symptom scores, resolution rates of individual symptoms, endoscopic mucosal healing rates, and changes in C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and fecal calprotectin levels.
Discussion: The outcomes of this research aim to provide evidence supporting the efficacy and safety of HKE enemas for treating ulcerative colitis, and generate high-quality evidence on the treatment of UC with Chinese herbal medicine retention enemas through rigorous clinical investigation. The findings are intended to inform the optimization of therapeutic strategies in clinical guidelines. As this study is a protocol, no results are available at this stage.
Trial Registration Number: International Traditional Medicine Clinical Trial Registry ITMCTR2024000702 (https://itmctr.ccebtcm.org.cn/mgt/project/view/-7877458543771072185).
Keywords: Huangkui Lianchang decoction enema, complementary medicine, abdominal pain, ulcerative colitis
Introduction
UC is a chronic, non-specific inflammatory bowel disease characterized by persistent or recurrent symptoms such as diarrhea, mucus-bloody stools, abdominal pain, and tenesmus.1 Severe and debilitating pain is a common symptom of inflammatory bowel disease (IBD). Abdominal pain typically results from inflammatory mediators in the colonic mucosa stimulating hypersensitive nerve endings during the pathological process of UC. In addition to abdominal pain, some pain arises from extraintestinal manifestations of UC.2 Although current treatment strategies primarily involve Western medications and biologics, these therapies are often limited by the development of drug resistance, adverse effects, high costs, and inconsistent therapeutic effectiveness. Not all patients benefit equally, and access remains a challenge, particularly in low-resource settings. Moreover, the development of treatments tailored to the genetic and clinical characteristics of the Chinese population represents a critical challenge in the field of traditional Chinese medicine (TCM).3,4 Standard medical management of UC typically includes 5-aminosalicylic acid (5-ASA), corticosteroids, and immunosuppressants. However, these agents are associated with limitations, including poor long-term symptom control, high recurrence rates, multiple adverse effects, and a tendency to induce resistance over time.
The distal colon—including the rectum and left-sided colon—is the most frequently affected site in UC, with studies reporting involvement in up to 77% of cases. Therefore, identifying effective treatments for distal UC is essential to prevent disease progression and improve patient outcomes.5 Enemas and suppositories, which allow direct drug delivery to the inflamed mucosa, are considered first-line therapies for distal UC. TCM enemas have been extensively used in clinical practice due to their longstanding history and notable advantages, such as rapid symptom relief (eg resolution of abdominal pain), sustained therapeutic effects, and low cost. However, despite the availability of various TCM enema formulations, high-quality clinical evidence remains limited. Reported remission rates generally range between 70% and 85%6–8 but treatment precision and formula-syndrome specificity remain suboptimal. As such, the development of a standardized and clinically validated TCM enema formulation represents a significant unmet need in the management of distal UC.
TCM offers unique therapeutic advantages in the management of UC. In TCM theory, UC is classified under syndromes such as “dysentery” “chronic dysentery” and “resting dysentery”. The HKE was developed to treat rectal- and left-sided UC. This formulation has demonstrated favorable clinical effectiveness by promoting mucosal healing and alleviating symptoms such as mucus-bloody stools. It is particularly suited for patients with mild to moderate active UC presenting with mucus-bloody stools. The therapeutic rationale and clinical use of HKE are aligned with the Chinese national clinical practice guideline on diagnosis and management of ulcerative colitis (2023),9 issued by the Chinese Society of Integrated Traditional and Western Medicine, the Chinese Association of Traditional Chinese Medicine, and the Chinese Medical Association. These guidelines recognize “damp-heat stagnation in the intestines” and “spleen deficiency with dampness stagnation” as key TCM syndromes associated with UC.
Preliminary clinical studies report an overall efficacy rate of 74.20% (77/101) for HKE in treating UC.10 Compared to Mesalazine alone, combination therapy with HKE significantly improves core symptoms such as diarrhea, bloody stools, abdominal pain, and tenesmus. It also leads to reductions in Mayo scores, TCM syndrome scores, and fecal calprotectin levels. HKE has demonstrated advantages in rapid symptom control, sustained effectiveness, and mucosal healing, and it has been well received by patients. This research has been granted a national invention patent and is supported by the National Administration of Traditional Chinese Medicine’s Evidence-Based Medicine Capacity Building Project (Grant No. K2023BZ02). The study protocol is registered with the National Medical Research Registration and Filing Information System (Registration No.: MR-32-24-042586). These recognitions further support the clinical relevance and potential of HKE in the integrated treatment of UC.
Materials and Methods
Design
This trial adopts a prospective, randomized, active-controlled, non-inferiority design. Figure 1 shows the trial flowchart. A total of 172 patients with mild to moderate active distal UC will be randomly assigned in a 1:1 ratio to receive either HKE or Mesalazine enemas. Each trial site provides participants with sufficient medication for an 8-week treatment period, in accordance with the Technical Guidelines for Clinical Trials of Drugs for the Treatment of Ulcerative Colitis (Applicable to Chemical Drugs and Biologics).11 The study consists of a screening period, an 8-week treatment period, and a follow-up period. Colonoscopic evaluations and follow-up of any abnormal laboratory results will be conducted within 28 days after treatment discontinuation. For more details, please refer to Supplemental Material 2 [Investigational Schedule]. The study is guided by the Declaration of Helsinki,12 the Standard Protocol Items: Recommendations For Interventional Trials (SPIRIT) (Supplemental Material 1 [SPIRIT checklist]).13
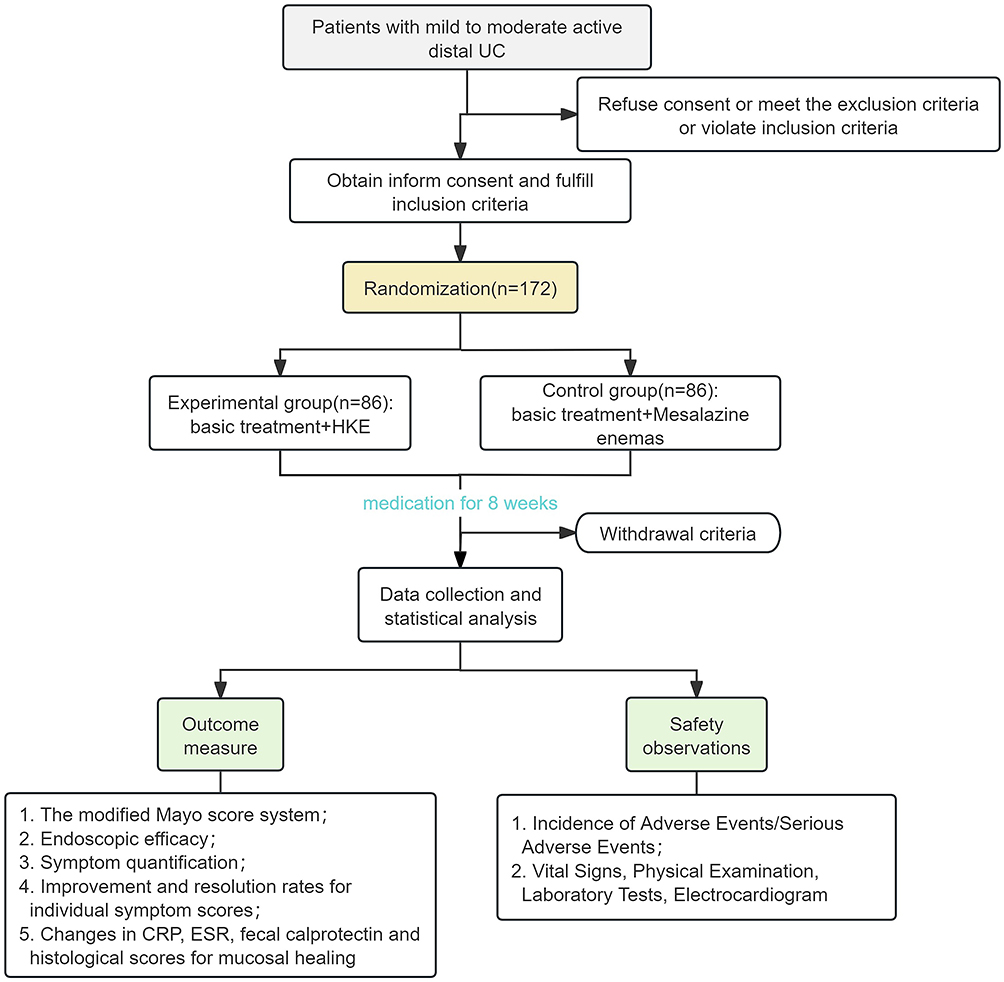 |
Figure 1 Trial flowchart. |
Study Settings and Participants
Study Sites
This RCT was conducted at eight hospitals, including Jiangsu Province Hospital of Chinese Medicine, Yancheng No.1 People’s Hospital, Changshu No. 2 People’s Hospital, Huai’an First People’s Hospital, Lianyungang Hospital of Traditional Chinese Medicine, the First People’s Hospital of Lianyungang, Changzhou No. 2 People’s Hospital, and Affiliated Hospital of Jiangnan University. The establishment of research centers that combine traditional Chinese medicine and Western medicine will help reduce patients’ subjective bias toward traditional Chinese medicine treatment.
Sample Size Calculation
According to literature reports, the remission rate of mesalazine in the treatment of UC is 64.0%. A preliminary clinical study (n = 101) confirmed that the remission rate of HKE in the treatment of UC is 74.2%.10 Considering a clinically meaningful threshold of 15%, under the conditions of a=0.025 (one-sided) and a test power of β = 90%, the experimental group and control group were enrolled in a 1:1 ratio. Using SAS 9.4 proc power, a total of 142 cases were required for enrollment. Considering a 20% dropout rate, a total of 172 cases were required for enrollment, resulting in 86 cases per group.

Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Meet UC medical diagnostic criteria:1,11,14 a. Disease stage: active phase; b. Disease severity is mild to moderate (refer to the modified Truelove and Witts disease severity classification criteria,15 see Table 1 for details); c. Lesion location is rectal or left-sided colonic type (recommended to use the Montreal classification,16 see Table 2 for details); d. Modified Mayo score17 of 3–10 points, and an endoscopic subscore of 2 or higher (modified Mayo score, see Table 3);
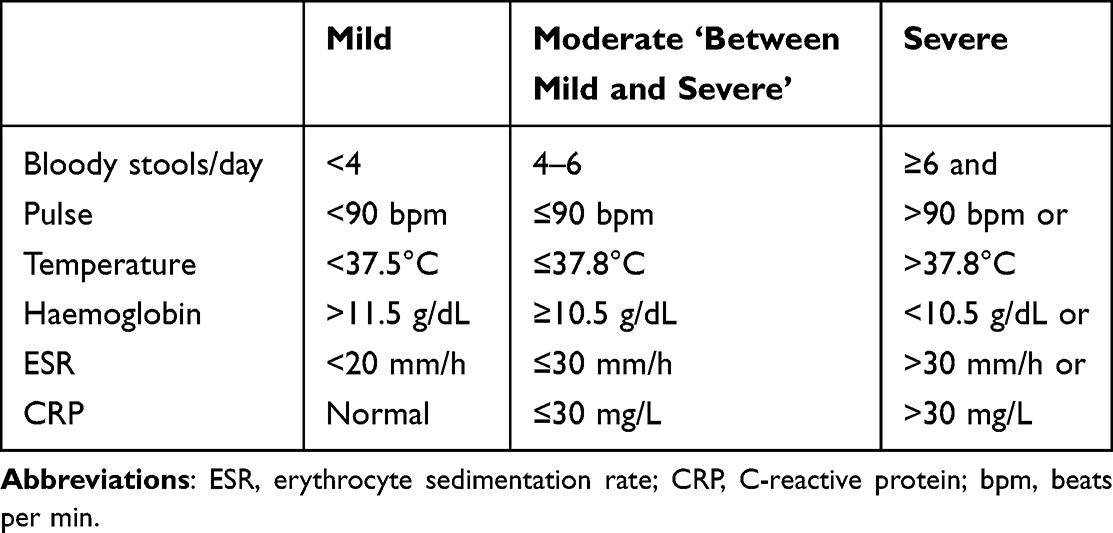 |
Table 1 Modified Truelove and Witts Disease Severity Staging Criteria |
 |
Table 2 Montreal Classification of Extent of UC |
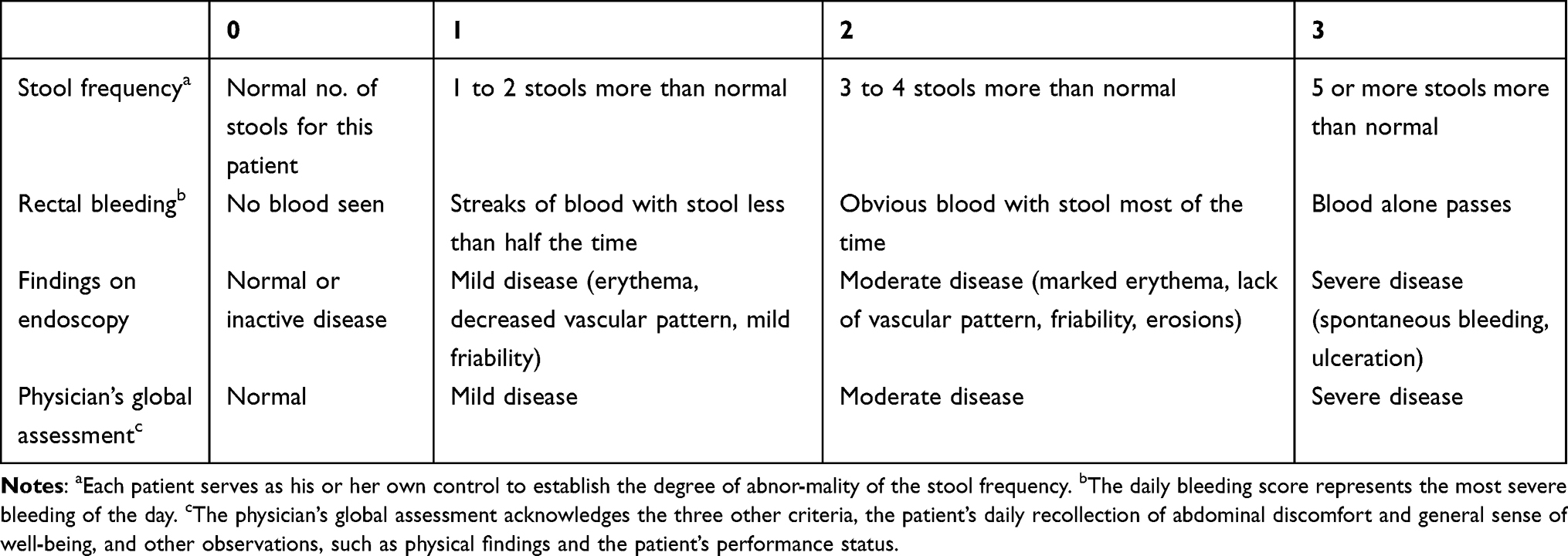 |
Table 3 Modified Mayo Scoring System for Assessment of Ulcerative Colitis Activity |
(2) Traditional Chinese medicine diagnosis of damp-heat accumulation in the intestines or spleen deficiency with dampness accumulation;
(3) Age between 18 and 65 years;
(4) The patient voluntarily signs an informed consent form.
Exclusion Criteria
- Patients with infectious colitis such as bacterial dysentery, amoebic dysentery, chronic schistosomiasis, intestinal tuberculosis, as well as Crohn’s disease, ischemic colitis, and radiation colitis;
- Patients with severe complications such as local stricture, intestinal obstruction, intestinal perforation, toxic megacolon, massive bleeding, colorectal cancer, or rectal cancer;
- Patients with other primary or secondary infectious diseases, such as cholecystitis or pneumonia;
- Patients who have undergone enema therapy within the past two weeks;
- Patients currently receiving treatment with corticosteroids, thiopurine drugs, biologics, or probiotics;
- Patients with severe cardiovascular, hepatobiliary, pulmonary, renal, or hematological diseases;
- Patients with allergic constitutions, such as a history of allergy to two or more drugs or foods, or a known allergy to the investigational drug;
- Patients with suspected or confirmed history of alcohol or drug abuse;
- Pregnant or breastfeeding women;
- Patients with disabilities as defined by law (blindness, deafness, mutism, intellectual disabilities, mental disorders, or physical disabilities);
- Other conditions that, in the investigator’s judgment, may reduce eligibility or complicate enrollment, such as frequent changes in work environment that may lead to loss to follow-up;
- Patients currently participating in other clinical trials.
Randomization
In this trial, each center used a competitive enrollment method to include study subjects. A professional statistical analyst generated the random sequence for the treatment (trial drug and control drug) received by the 172 subjects using the SAS (Proc Plan) statistical analysis software based on the randomization method of the trial center, ie Listing the treatment allocation corresponding to serial numbers 001 to 172. All randomization codes were distributed to each trial center in segments according to the randomization protocol. Investigators enrolled eligible patients in the order of their visits, and the medication administrator sequentially distributed the corresponding trial medications to patients in ascending order of their assigned codes.
Interventions
According to the “General Principles for Clinical Research on New Traditional Chinese Medicines” issued by the National Medical Products Administration in 2015, a positive control drug should be selected based on recognized effectiveness, safety, and comparability for the target disease. In this study, Salofalk enema solution is chosen as the positive control for the local treatment of distal RCT, in accordance with these regulatory guidelines.
Basic treatment medication: All participants receive standard treatment with Salofalk (mesalazine enteric-coated tablets) at a dosage of 2 g/day, administered orally (specification: 0.5 g × 40 tablets per bottle). In addition to pharmacological treatment, patients are advised to adhere to the following lifestyle recommendations: 1. Maintain regular bowel habits and practice proper perianal hygiene after each bowel movement; 2. Follow a light and easily digestible diet, avoiding high-fiber foods, as well as spicy, greasy foods, tobacco, and alcohol; 3. Maintain a regular daily routine, balance work and rest, engage in moderate physical activity to improve fitness, and manage emotional well-being.
The experimental group received standard treatment and HKE therapy. HKE, 60 mL per dose, once daily at bedtime, administered via enema (specification: 250 mL per bottle). The treatment course will last for 8 weeks unless the subject discontinues the trial prematurely. Patients will undergo follow-up assessments on days 14, 28, 42, 56, and 28 days after discontinuation of treatment. The trial schedule is outlined in Supplemental Material 2 [Investigational Schedule]. All participants receive a detailed video tutorial on the correct enema technique and are provided with single-use, sterile enema kits. At Visit 3 and Visit 5, patients will return any remaining medication for compliance assessment by the investigator. To help patients improve adherence, we will provide operational guidance and address questions at each visit.
The control group received standard treatment and Salofalk (mesalazine enema solution) therapy. Salofalk (mesalazine enema solution), 60 mL/4 g per dose, once daily at bedtime, administered via enema (drug specification: 60 mL: 4 g). Assessment methods were the same as those for the experimental group.
Withdrawal Criteria
- Participants will be withdrawn from the trial under any of the following conditions:
- Occurrence of severe adverse reactions;
- Development of an allergic reaction to the investigational drug during the study;
- Inability to tolerate the study drug;
- Non-adherence to the prescribed dosing regimen, defined as receiving more than 120% or less than 80% of the theoretical dose;
- Lack of cooperation from participants or their family members, inability to complete the study as planned, or unauthorized modification of the medication regimen;
- Loss to follow-up.
Management of Withdrawal Cases
In the event of withdrawal, investigators are required to make reasonable efforts to contact the participant through home visits, scheduled follow-ups, telephone calls, or written correspondence to determine the reason for withdrawal. The time of the last medication administration should be recorded, and all assessable items should be completed to the extent possible.
For withdrawals due to allergic reactions, adverse events, or lack of effectiveness, appropriate medical management should be provided based on the participant’s condition. All data from withdrawn cases must be retained for documentation and included in the full analysis set. Replacement of withdrawn participants is not required.
Outcome
Data are collected by GCP-trained researchers using standardised data collection forms.
Primary Outcome
Clinical efficacy is assessed using the modified Mayo score system. Clinical remission is defined as a total modified Mayo score of ≤2 points post-treatment, with no individual subscore exceeding 1 point. Clinical response is defined as a ≥30% or ≥3-point reduction in the total modified Mayo score from baseline.
Secondary Outcome
- Endoscopic efficacy: The endoscopic response rate and endoscopic mucosal healing rate (Ulcerative colitis endoscopic severity index (UCEIS); Table 4)18 are assessed.
- Symptom quantification: Detailed in Tables 5 and 6, symptom quantification6 and Traditional Chinese Medicine syndrome efficacy assessment are evaluated.
- Improvement and resolution rates for individual symptom scores6 are measured.
- Changes in CRP, ESR, fecal calprotectin and histological scores for mucosal healing (Table 7)19 from baseline are analyzed.
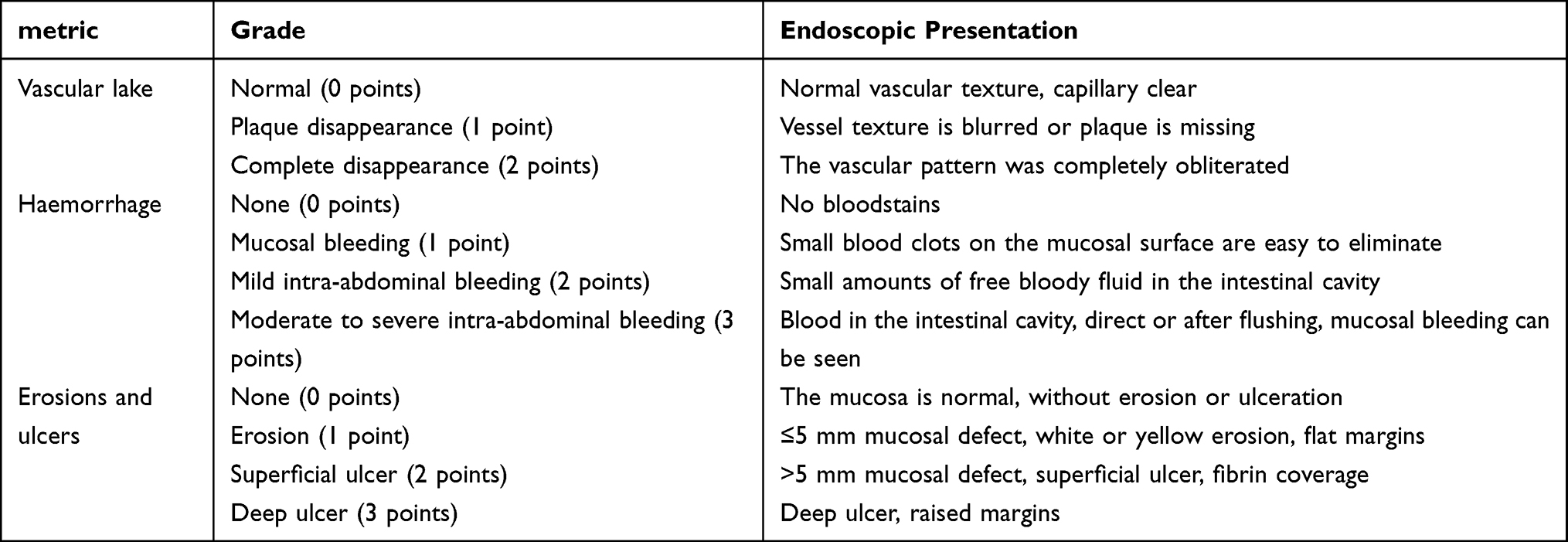 |
Table 4 UCEIS Scoring System |
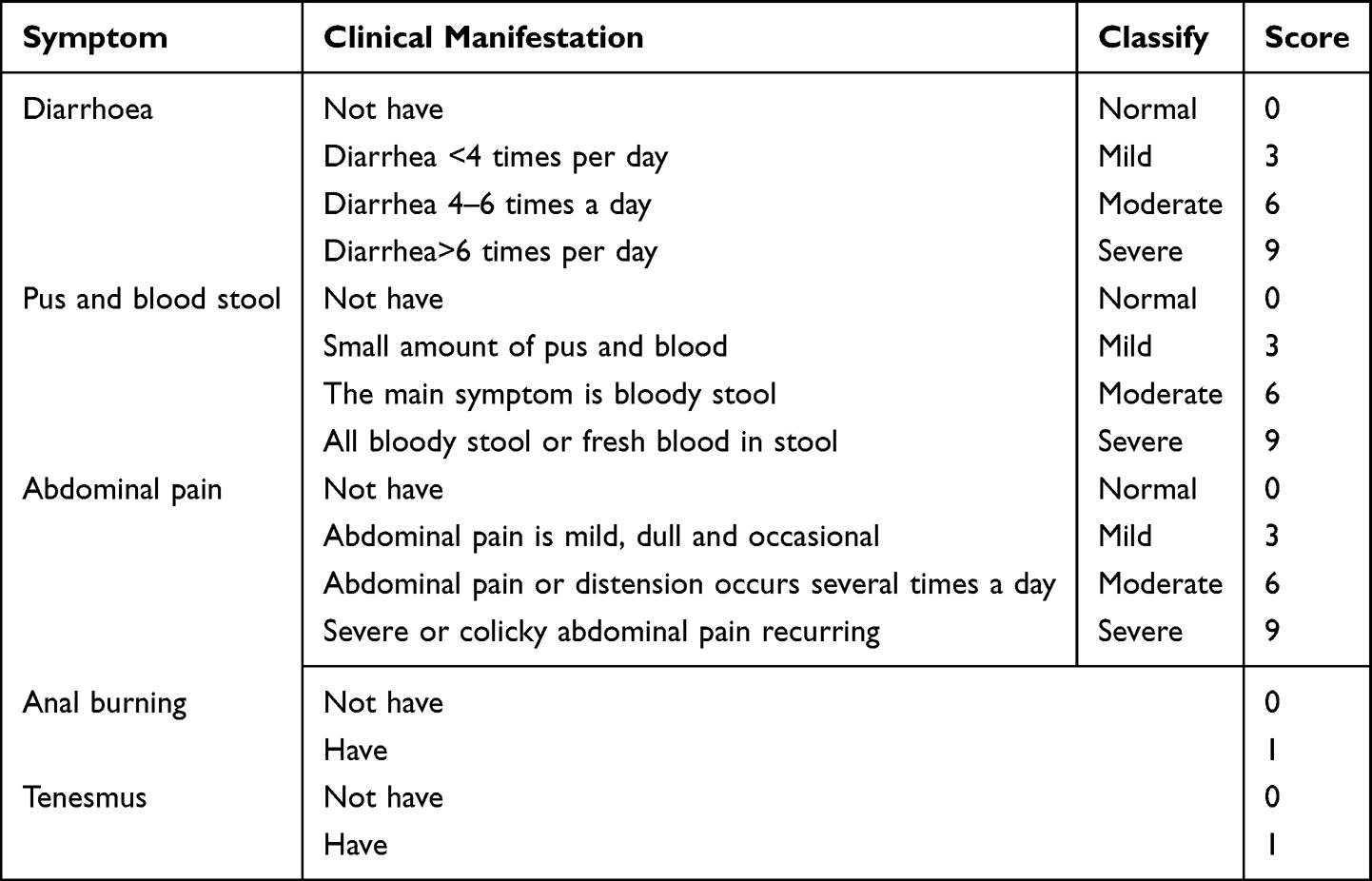 |
Table 5 Symptom Quantification Scale |
 |
Table 6 TCM Syndrome Efficacy Evaluation Standard Table |
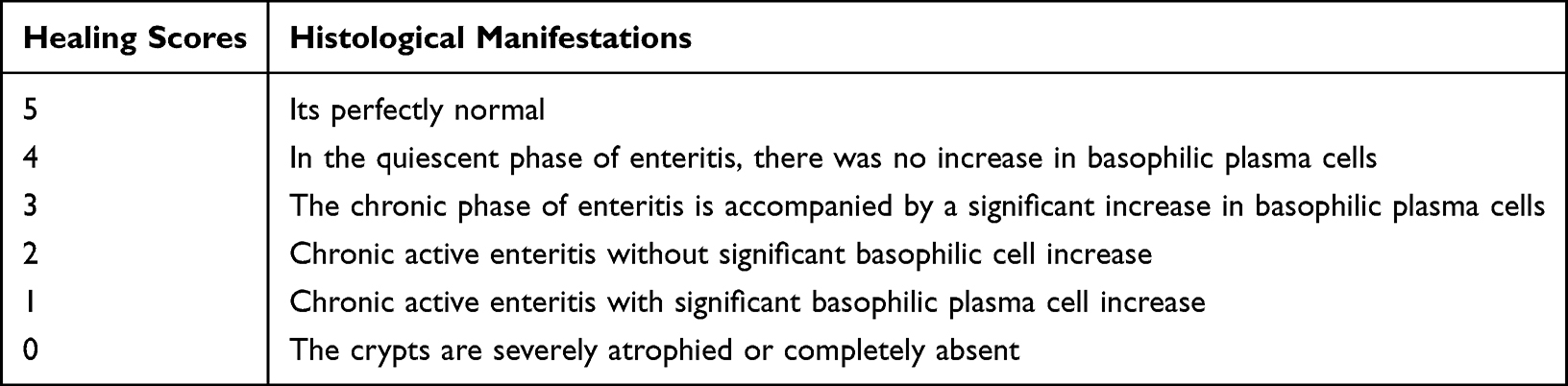 |
Table 7 Mucosal Healing Histological Scoring Table |
All primary and secondary outcomes will be measured at baseline, 8 weeks after randomisation. The modified Mayo sub-scores for Stool frequency and Rectal bleeding and Symptom quantification scale will be clinically reviewed at 2, 4, 6 weeks after randomisation. While the colonoscopy and related score can be performed at the 8th week or within one month after completing medication.
Safety Observations
- Incidence of Adverse Events/Serious Adverse Events
The types, severity, and relationship to the investigational drug of all adverse events occurring during the trial will be described in a table.
- Vital Signs, Physical Examination, Laboratory Tests, 12-Lead Electrocardiogram
Statistical descriptions of changes in vital signs (body temperature, heart rate, respiration, systolic blood pressure, diastolic blood pressure) before and after treatment.
Adverse Events
The investigational drug, HKE, has demonstrated good safety in previous clinical use. In extremely rare cases, patients have experienced gastrointestinal irritation, but no significant adverse reactions have been observed. If patients experience gastrointestinal irritation, it is recommended to dilute the solution with 20 mL of warm water or saline before administration. If the patient cannot tolerate the irritation, the procedure should be discontinued.
For adverse events occurring during the trial, investigators should record the time of occurrence, severity, duration, management measures, and outcome in the case report form, and assess their relationship to the investigational drug.
If a serious adverse event (SAE) occurs during the trial, the investigator must immediately take measures to protect the safety of the subject and promptly report it to the research center. All adverse events should be followed up, with detailed records of the management process and outcomes until the issue is resolved or the condition stabilizes.
We have purchased clinical trial liability insurance for the subjects to protect their legitimate rights and interests.
Monitoring
The sponsor appoints a designated monitor to ensure that the rights and welfare of trial participants are protected throughout the study. The monitor is responsible for verifying that the data recorded in case report forms and final reports are accurate, complete, and consistent with source documents. Additionally, the monitor ensures that the clinical trial is conducted in accordance with the approved protocol, GCP guidelines, and applicable regulatory requirements. Any protocol deviations identified during the trial are promptly reported by the monitor to both the sponsor and the ethics committee.
Data Management
An electronic data capture (EDC) system is utilized in this trial. Case report forms (CRFs) are developed by data managers in accordance with the study protocol and source documentation.
Statistical Analysis
Exclusion Criteria
- Cases that do not meet the inclusion criteria but meet any exclusion criteria;
- Cases that do not receive the investigational drug;
- Cases with no available data after randomization.
Prior to statistical analysis, the statistical analyst and the principal investigator discuss and determine the exclusion of specific cases. Statistical analyses are conducted using SAS version 9.4 or higher. Trial results are presented in summary tables (or figures) and listings.
All statistical tests will be two-sided. A p-value less than 0.05 will be considered statistically significant. Exploratory analyses will not undergo multiple comparison correction. Intergroup comparisons or within-group comparisons of quantitative data will be performed using t-tests or rank-sum tests. If other factors are considered, covariance analysis (or other statistical methods specified in the SAP) will be used. Intergroup comparisons of categorical data were performed using chi-square tests or Fisher’s exact probability method. If other factors were considered, the CMH chi-square test was used. If multiple baseline confounding factors were considered, logistic regression models were used. Time-to-event indicators were analyzed using the Kaplan–Meier method, describing median time, quartile time, and their 95% confidence intervals (95% CI), and survival curves were plotted.
Discussion
TCM enemas for UC have a long history of use in China and remain an important component of UC management. The Chinese Guidelines for the Diagnosis and Treatment of Ulcerative Colitis (2023·Xi’an) recommend oral 5-ASA combined with enema therapy for patients with mild to moderate active left sided UC. Enema medications include 5-ASA, topical glucocorticoid preparations, and TCM formulations.9
TCM enemas have a long history of use. The active components of these medicines can exert their effects either by being directly absorbed into intestinal tissues or indirectly through absorption into the bloodstream or adsorption onto the intestinal mucosa. HKE demonstrates favorable clinical efficacy in treating UC.10,20 International studies have shown that Abelmoschus manihot flower21 has anti-inflammatory, antioxidant, antidepressant, anti-fibrotic, vasculogenic, and lipid metabolism-regulating effects; Pteris multifida herb22,23 has antioxidant, antitumor effects; Euphorbia humifusa herb24,25 has antibacterial, anti-inflammatory, and antidiarrheal effects. Preliminary studies show that administration of total flavonoids extracted from Abelmoschus manihot flowers effectively suppresses inflammatory mediators associated with inflammatory bowel disease and promotes intestinal mucosal healing.26 In addition, HKE improves dextran sulfate sodium (DSS)-induced colitis in mice through modulation of the NF-κB pathway.27 Although HKE enema therapy is recognized by both Chinese scholars and patients and has been included in the Chinese Medicine Diagnosis and Treatment Guidelines for Ulcerative Colitis (2023), it is classified only as a weak recommendation supported by low-quality evidence.28 At present, high-quality clinical evidence for HKE enema therapy in UC remains insufficient.29 Previous clinical studies on enema therapies have been hampered by methodological issues, including small sample sizes, non-standardized research designs, and a narrow range of outcome measures. Therefore, it is imperative to conduct a standardized, high-quality clinical study to address these shortcomings.
This trial was consciously designed to respond to several common critiques of clinical research in TCM. First, we employed a standardized, quality-controlled HKE formulation and integrated exploratory biomarker assessments to link clinical outcomes with potential mechanistic insights into host metabolism. Second, recognizing the paramount importance of rigor, we implemented a controlled design with a positive control drug. Third, while TCM emphasizes individualized treatment, this study adopts a “disease-pattern” focused approach using a fixed formula for a well-defined patient population (active mild-to-moderate UC). This is a necessary and valid strategy to establish initial efficacy evidence within a controlled experimental framework. Finally, by adhering to SPIRIT reporting guidelines and providing exhaustive details on the intervention, we ensure transparency and reproducibility. We contend that this multifaceted approach strengthens the validity of our findings and contributes to a more scientifically rigorous evaluation of TCM therapies.
This study has several notable strengths. Our research has a larger sample size than previous clinical studies of HKE, which can reduce random errors and assist statisticians in conducting meaningful subgroup analyses, and increase the statistical power to detect adverse events and rare outcomes. In the evaluation of outcome measures, we employed multiple scoring systems including clinical symptom scores from both traditional Chinese and Western medicine, endoscopic scores, and histological healing scores to objectively and multidimensionally assess the efficacy of HKE. The control group receives active drug therapy, featuring a more rigorous and standardized study design compared to previous clinical studies on Chinese herbal enemas.30 All participants receive appropriate doses of oral mesalazine as baseline therapy, ensuring patient safety during active disease and improving adherence to follow-up assessments. In addition, study sites include both traditional Chinese medicine hospitals and Western medicine hospitals, thereby minimizing selection bias toward specific healthcare settings and enhancing the overall validity of the findings.
This study also has certain limitations. Although a randomized controlled enrollment design is adopted, due to the color difference between HKE and mesalamine enema solution, a blind method cannot be employed. Furthermore, as the trial is conducted exclusively across multiple centers in Jiangsu Province, a traditional center of Chinese medicine with abundant TCM resources, a large patient base, and high cultural acceptance, the generalizability of the findings to other regions of China may be limited.
In summary, this study represents a large-scale, multicenter randomized controlled trial of enema therapy for UC in China. The trial provides a model for generating high-quality evidence to evaluate the efficacy of other Chinese herbal compound enemas in the treatment of UC both domestically and internationally. If standardized clinical studies demonstrate that HKE achieves equivalent or superior clinical efficacy compared to standard Western pharmaceutical treatments for UC, this would provide evidence supporting the efficacy and safety of HKE enemas for treating ulcerative colitis. This study aims to generate high-quality evidence on the treatment of UC with Chinese herbal medicine retention enemas through rigorous clinical investigation. The findings are intended to inform the optimization of therapeutic strategies in clinical guidelines, expand the diagnostic and therapeutic scope of Chinese herbal enema therapy for UC, highlight its distinctive advantages, and provide new insights for advancing enema-based treatment approaches for UC.
Trials Status
This trial was registered at the International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/mgt/project/view/-7877458543771072185) on 11 November 2024 (registered number: ITMCTR2024000702, the protocol version number: V7.0). This study is currently in the recruitment stage. The first patient was randomized on 14 January 2025, and recruitment is expected to be completed by June 2026, and the trial is estimated to end in December 2025.
Conclusion
The outcomes of this research aim to provide evidence supporting the efficacy and safety of HKE enemas for treating ulcerative colitis and generate high-quality evidence on the treatment of UC with Chinese herbal medicine retention enemas through rigorous clinical investigation. The findings are intended to inform the optimization of therapeutic strategies in clinical guidelines.
Data Sharing Statement
Upon completion of this study, the data will be made available by the corresponding authors upon reasonable request. Interested researchers may contact Professor Chen (email: [email protected]) to request access.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Jiangsu Provincial Hospital of Traditional Chinese Medicine on 11 November 2024 (Approval No.:2024NL-200-03). The results of the trial will be submitted for publication in a peer-reviewed journal and presented at relevant conferences.
This study was registered with the International Traditional Medicine Clinical Trial Registry (trial registration number ITMCTR2024000702; name of trial registry: Based on targeting intestinal stem cells/GART and extracellular traps of neutrophils (NETs) to explore the systematic biological effect mechanism of HKE in anti-inflammatory and rectifying deviation treatment of UC and was filed in the Medical Research Registration and Filing Information System (www.medicalresearch.org.cn).
Eligible clinical patients can only enter this study after signing the informed consent form (Supplemental Material 3 [Informed Consent Form]) approved by the IEC. If the subject is unable to sign, her legal guardian shall sign the informed consent form on her behalf. The researcher should explain the situation of this study to the subjects in this group or their guardians. The study will be conducted in accordance with the protocol, the Measures for the Administration of Investigator-Initiated Clinical Research in Chinese Medical and Health Institutions (Trial), and the Declaration of Helsinki and with the informed consent of the patients. Except for emergencies requiring specific treatment measures, the researchers guarantee that they will comply with the protocol in all aspects, especially in obtaining informed consent and reporting and monitoring SAEs. Any formal publication or release of the data from this study will protect the privacy of clinical patients. Laboratory tests and other examination results will be published only for scientific purposes, and the identity of the subjects will not be disclosed.
Acknowledgments
The authors thank all involved in the study, including practitioners, assessors and participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 82341229), the Chinese Medicine Treatment of Dominant Diseases (Clinical Evidence-based Competence Enhancement) Foundation (No: k2023BZ02) and Jiangsu Jiu Xu Pharmaceutical Co. Ltd. The sponsor, Jiangsu Jiu Xu Pharmaceutical Co. Ltd., was involved in the study design but had no role in data collection, analysis, interpretation, or the writing of the manuscript.
Disclosure
Mr Hong Li and Mr Jianghai Zhang are employees of Jiangsu Jiu Xu Pharmaceutical Co. Ltd. The authors report no other conflicts of interest in this work.
References
1. Magro F, Gionchetti P, Eliakim R, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 1: definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J Crohns Colitis. 2017;11(6):649–13. doi:10.1093/ecco-jcc/jjx008
2. Hardy P-Y, Fikri J, Libbrecht D, Louis E, Joris J. Pain characteristics in patients with inflammatory bowel disease: a monocentric cross-sectional study. J Crohn’s Colitis. 2022;16(9):1363–1371. doi:10.1093/ecco-jcc/jjac051
3. Wei SC, Sollano J, Hui YT, et al. Epidemiology, burden of disease, and unmet needs in the treatment of ulcerative colitis in Asia. Expert Rev Gastroenterol Hepatol. 2021;15(3):275–289. doi:10.1080/17474124.2021.1840976
4. Haoying H, Tao Z, Xin W. Interpretation of expert consensus on the diagnosis and treatment of ulcerative colitis with integrated traditional Chinese and western medicine. Chin J Integr Tradit West Med Dig. 2023;32(8):674–677.
5. Zhang Y, Chen D, Wang F, et al. Comparison of the efficiency of different enemas on patients with distal ulcerative colitis. Cell Prolif. 2019;52(2):e12559. doi:10.1111/cpr.12559
6. Lei Z, Honghai Z, Hong S. Treatment of ulcerative colitis with mild to moderate distal damp heat syndrome of large intestine with Boyu enema retrospective cohort analysis. Chin J Integr Tradit West Med Dig. 2023;31(3):168–172. doi:10.3969/j.issn.1671-038X.2023.03.03
7. Meng M, Luqing Z, Shengsheng Z. Clinical registry study of modified Sanhuang Decoction enema in the treatment of ulcerative colitis with syndrome of dampness-heat in large intestine. Chin J Integr Tradit West Med Dig. 2022;30(7):469–474. doi:10.3969/j.issn.1671-038X.2022.07.02
8. Z Q, H Z, Y S, Kai P. Interpretation of expert consensus on the diagnosis and treatment of ulcerative colitis with integrated traditional Chinese and western medicine. Chin J Integr Tradit West Med Dig. 2014;20(8):1098–1100.
9. Inflammatory Bowel Disease Group CSoG, Chinese Medical Association, Inflammatory Bowel Disease Quality Control Center of China; Wu K, Chen M, Qian J, Ji Y. 2023 Chinese national clinical practice guideline on diagnosis and management of ulcerative colitis. Chin J Med. 2024;137(14):1642–1646. doi:10.1097/CM9.0000000000003221
10. Liu H, Duan Z, Shi G. Retrospective analysis of efficacy of Huangkui Lianyang prescription in treatment of101 cases of mild to moderate active ulcerative colitis. Liaoning J Tradit Chin Med. 2022;49(02):75–77. doi:10.13192/j.issn.1000-1719.2022.02.022
11. Center for Drug Evaluation N. Technical guidelines for clinical trials of drugs for ulcerative colitis. 2025. Available from: https://www.cde.org.cn/zdyz/domesticinfopage?zdyzIdCODE=2f55415bf370625105e997b8216ecc58.
12. World Medical A. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
13. Chan A-W, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346(jan08 15):e7586. doi:10.1136/bmj.e7586
14. Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis. 2017;11(7):769–784. doi:10.1093/ecco-jcc/jjx009
15. Sturm A, Maaser C, Calabrese E, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD Part 2: IBD scores and general principles and technical aspects. J Crohns Colitis. 2019;13(3):273–284. doi:10.1093/ecco-jcc/jjy114
16. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. 2006;55(6):749–753. doi:10.1136/gut.2005.082909
17. Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353(23):2462–2476. doi:10.1056/NEJMoa050516
18. Travis SP, Schnell D, Feagan BG, et al. The impact of clinical information on the assessment of endoscopic activity: characteristics of the ulcerative colitis endoscopic index of severity [UCEIS]. J Crohns Colitis. 2015;9(8):607–616. doi:10.1093/ecco-jcc/jjv077
19. Pathology Group IBDG, Chinese Society of Gastroenterology, Chinese Medical Association; Ziyin Y, Shuyuan X. Experts guideline on pathological assessment of inflammatory bowel disease in China. Chin J Inflam Bowel Dis. 2021;05(1):5–20. doi:10.3760/cma.j.cn101480-20200731-00086
20. He Z, Wu B, Wen K. Clinical observation of Huangkui Lianchang prescription enema in the treatment of distal ulcerative colitis. Hebei J Tradit Chin Med. 2019;41(06):833–837+843.
21. Li N, Tang H, Wu L, et al. Chemical constituents, clinical efficacy and molecular mechanisms of the ethanol extract of Abelmoschus manihot flowers in treatment of kidney diseases. Phytother Res. 2021;35(1):198–206. doi:10.1002/ptr.6818
22. Kim JW, Seo JY, Oh WK, Sung SH, Choi JS. Anti-neuroinflammatory ent-kaurane diterpenoids from Pteris multifida roots. Molecules. 2017;22(1). doi:10.3390/molecules22010027
23. Yin M-C, Chang C-H, Su C-H, Yu B, Hsu Y-M. Pteris multifida, Cortex phellodendri, and probiotics attenuated inflammatory status and immunity in mice with a Salmonella enterica serovar typhimurium infection. Biosci Biotechnol Biochem. 2018;82(5):836–847. doi:10.1080/09168451.2018.1447356
24. Wu X, Ma G-L, Chen H-W, et al. Antibacterial and antibiofilm efficacy of the preferred fractions and compounds from Euphorbia humifusa (herba euphorbiae humifusae) against Staphylococcus aureus. J Ethnopharmacol. 2023;306:116177. doi:10.1016/j.jep.2023.116177
25. Xiang N, Zhao J, Chang S, Li S, Liu S, Wang C. In vitro fecal fermentation of Euphorbia humifusa-derived polysaccharides and their protective effect against ulcerative colitis in mice. Foods. 2023;12(4):751. doi:10.3390/foods12040751
26. Bu F, Ding Y, Chen T, et al. Total flavone of abelmoschus manihot improves colitis by promoting the growth of akkermansia in mice. Sci Rep. 2021;11(1):20787. doi:10.1038/s41598-021-00070-7
27. He Z, Zhou Q, Wen K, et al. Huangkui Lianchang decoction ameliorates DSS-induced ulcerative colitis in mice by inhibiting the NF-kappaB signaling pathway. Evid Based Complement Alternat Med. 2019;2019(1):1040847. doi:10.1155/2019/1040847
28. Li J, Tang X, Wang H, Dong Y. Guidelines for diagnosis and treatment of ulcerative colitis in traditional Chinese medicine (2023). J Traditional Chin Med. 2024;65(07):763–768. doi:10.13288/j.11-2166/r.2024.07.018
29. Yan Z-X, Liu Y-M, Ma T, et al. Efficacy and safety of retention enema with traditional Chinese medicine for ulcerative colitis: a meta-analysis of randomized controlled trials. Complementary Ther Clin Pract. 2021;42:101278. doi:10.1016/j.ctcp.2020.101278
30. Zhang J, Shi B, Li D, et al. Comparative study of Chinese herbal enema combined with mesalazine versus mesalazine alone in the treatment of ulcerative colitis: a randomized controlled trial. J Chin Med Assoc. 2025:10–97.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.