Back to Journals » Nature and Science of Sleep » Volume 18

The Effectiveness of a Novel Sleep Test Based on Cardiopulmonary Coupling to Detect Obstructive Sleep Apnea: A Multicenter Prospective Study
Authors Sun CY ![]() , Hang LW
, Hang LW ![]() , Chang ET
, Chang ET ![]() , Perng DW, Huang SF, Lin FC, Su KC, Shiao TH, Liu YY
, Perng DW, Huang SF, Lin FC, Su KC, Shiao TH, Liu YY ![]() , Chen YM
, Chen YM ![]() , Chou KT
, Chou KT
Received 19 January 2026
Accepted for publication 23 May 2026
Published 24 June 2026 Volume 2026:18 581103
DOI https://doi.org/10.2147/NSS.S581103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Chuan-Yen Sun,1– 3,* Liang-Wen Hang,4,5,* En-Ting Chang,6,* Diahn-Warng Perng,1– 3 Shiang-Fen Huang,3,7 Fang-Chi Lin,1– 3 Kang-Cheng Su,1– 3 Tsu-Hui Shiao,1,2 Yung-Yang Liu,1– 3 Yuh-Min Chen,1– 3,8,9 Kun-Ta Chou1– 3
1Department of Chest Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 2Center of Sleep Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 3School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan; 4Department of Respiratory, Critical Care and Sleep Medicine, China Medical University Hospital, Taichung, Taiwan; 5School of Medicine, China Medical University, Taichung, Taiwan; 6Department of Chest Medicine, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, and School of Medicine, Tzu Chi University, Hualien, Taiwan; 7Division of Infectious Disease, Department of Medicine, Taipei Veterans General Hospital, Taipei, 112201, Taiwan; 8Clinical Research Center, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; 9Division of Chest Medicine, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Kun-Ta Chou, Center of Sleep Medicine & Department of Chest Medicine, Taipei Veterans General Hospital, No. 201, Sec. 2, Shih-Pai Road, Taipei, 11201, Taiwan, Tel +886-2-2871-2121 ext. 3085, Fax +886-2-2875-3466, Email [email protected]
Purpose: Obstructive sleep apnea (OSA) is common and requires early detection and timely management to relieve symptoms and lower the risk of long-term complications. Although established home sleep apnea testing systems are available, many require multiple sensors, and simplified ECG-based approaches may reduce setup burden and improve ease of use. This study aimed to evaluate the diagnostic performance of a cardiopulmonary coupling-based sleep test against polysomnography-derived apnea–hypopnea index (AHI) in adults with clinically suspected OSA.
Patients and Methods: In this prospective study at three tertiary medical centers in Taiwan, adults with suspected OSA received simultaneous in-laboratory polysomnography and a novel home sleep apnea test (Largan Health AI-Tech). The wearable device used a wireless electrocardiogram Holter monitor placed on the left anterior chest to record electrocardiogram signals during sleep. Signals were processed with cardiopulmonary coupling analysis to derive a respiratory event index, which was compared with the AHI from polysomnography.
Results: Among 479 participants, 200 were enrolled from CMUH, 193 from TVGH, and 86 from HTCH. The respiratory event index correlated strongly with the AHI (ρ = 0.889, p < 0.001), with high cohort-level consistency by intraclass correlation coefficient (ICC = 0.955). For identifying OSA, the area under the receiver operating characteristic curve was 0.923 (95% confidence interval 0.91– 0.95) at an AHI of at least 5 events per hour, 0.929 (95% confidence interval 0.90– 0.95) at least 15 events per hour, and 0.967 (95% confidence interval 0.95– 0.98) at least 30 events per hour. In the subgroup with supplemental pulse oximetry, the combined approach showed higher areas under the receiver operating characteristic curve of 0.981, 0.984, and 0.992 at the corresponding thresholds.
Conclusion: CPC-derived REI showed good diagnostic performance against PSG-derived AHI in adults with clinically suspected OSA referred to tertiary sleep centers in Taiwan, supporting its potential role as a simplified adjunctive tool for OSA evaluation in this referred clinical setting.
Keywords: obstructive sleep apnea, cardiopulmonary coupling, home sleep apnea testing, wearable biosensors
Introduction
Obstructive sleep apnea (OSA) is characterized by intermittent cessation of breathing during sleep, resulting from repetitive collapse of the pharyngeal airway.1,2 It is estimated to affect approximately one billion people worldwide and has gained increasing attention due to its significant economic and societal burden.3 OSA is associated with a variety of diseases, most notably cardiovascular conditions such as hypertension, atherosclerosis, and arrhythmia.4 These conditions result from multiple mechanisms, including intermittent hypoxemia, systemic inflammation, oxidative stress, and sympathetic activation following apneic episodes, all of which contribute to the association between OSA and cardiovascular comorbidities.5,6 Early identification and timely management of OSA can help alleviate symptoms, reduce the risk of adverse health outcomes, and decrease associated healthcare costs.7,8
The gold standard diagnostic tool for OSA is attended polysomnography (PSG).9 However, a standard PSG must be conducted in a sleep center and performed by a certified sleep technician to ensure accuracy.10 Due to limited personnel, equipment, and testing beds, patients often face long waiting times for the examination. In developing countries, there is generally limited awareness of OSA, and diagnostic and treatment options are often unavailable or not adapted to local settings, particularly with respect to the use of PSG.11 Even in developed countries, diagnostic resources remain insufficient for the large burden of suspected OSA, leaving many individuals undiagnosed and untreated.12,13 This unmet diagnostic need is also relevant in Taiwan. In a Taiwan-based prospective cohort using home sleep testing, OSA was detected in 69.5% of 1372 adults aged 30 to 70 years, including 17.9% with moderate OSA and 22.5% with severe OSA. These local data further support the need for accessible diagnostic strategies for clinically suspected OSA in Taiwan.14
Home sleep apnea testing (HSAT) provides valuable diagnostic information for selected patients with suspected OSA and allows testing in the home setting.10,15,16 Conventional Level 3 HSAT systems are the most established home-based diagnostic tools and typically rely on multiple sensors, including nasal pressure transducers, respiratory effort belts, and pulse oximetry. These sensors provide direct respiratory measurements but may increase setup burden and reduce tolerance in some home settings. With advances in wearable technology, several simplified portable sleep screening devices have been developed.17–19 A cardiopulmonary coupling (CPC)-based ECG Holter system offers a different practical approach by using a single chest-worn ECG sensor with automated analysis to estimate sleep-related respiratory event burden. This design is not intended to replace standard Level 3 HSAT or PSG, but rather to serve as a simpler adjunctive option for OSA evaluation.
The novel Sleep Apnea and Sleep Quality Examination System (LARGAN HEALTH TECHNOLOGY), certified by the Taiwan Food and Drug Administration (TFDA) (Certification No. 030626), is designed for the detection of OSA. This system utilizes a portable electrocardiogram (ECG) Holter monitor (ECG Holter, TFDA Certification No. 006116) to record ECG signals, which serve as the data source, and integrates the results with the AI-based Sleep Apnea and Sleep Quality Examination System (ST-SLP03A). The system employs a CPC algorithm to analyze data and estimate the respiratory event index (REI), which is used to detect OSA.20,21 Unlike PSG-derived AHI, which is calculated from scored obstructive apneas and hypopneas per hour of sleep, CPC-derived REI estimates respiratory event burden from ECG-based cardiopulmonary oscillations during the recording period. Therefore, validation against PSG-derived AHI is necessary to determine its diagnostic performance. Although previous studies have demonstrated the acceptability of CPC for OSA diagnosis,22,23 further prospective multicenter validation data on this sleep test for OSA detection remain limited. This study adopts a prospective, multicenter design to evaluate the performance of the test in adults with clinically suspected OSA referred to tertiary sleep centers in Taiwan by comparing device-derived REI with PSG-derived AHI.
Materials and Methods
This multicenter prospective study was conducted at three tertiary medical centers in Taiwan, including Taipei Veterans General Hospital (TVGH), China Medical University Hospital (CMUH), and Hualien Tzu Chi Hospital (HTCH). The study protocol was approved by the Institutional Review Boards of all three hospitals: Institutional Review Board of Taipei Veterans General Hospital (VGHIRB No. 2019–11-005BC), Institutional Review Board of China Medical University Hospital (CMUH109-REC1-055), and Institutional Review Board of Hualien Tzu Chi Hospital (IRB108-150-B). The Largan Health AI-Tech Company, Taiwan, financially sponsored this research but was not involved in the study design, implementation, data interpretation, or article preparation.
Study Subjects
Subjects aged 20 years or older, who were scheduled to undergo standard attended full-channel PSG at the sleep centers of the three participating hospitals, were recruited between April 2019 and July 2021. Participants were referred for in-laboratory PSG because of clinical suspicion of OSA based on routine outpatient evaluation, including STOP-Bang questionnaire screening as part of clinical assessment, sleep-related symptoms such as snoring, witnessed apnea, and daytime sleepiness, together with clinician judgment. Exclusion criteria included participants under 20 years of age, those with poor quality CPC data, individuals unwilling to participate in the study or unwilling to sign the informed consent form, and those with cognitive impairments or conditions that could affect their ability to perform the procedures. After obtaining written informed consent, participants underwent both PSG and the CPC-based exam simultaneously for a direct comparison. Clinical data, including demographics and body mass index (BMI) were collected.
Polysomnography
Overnight PSG was conducted at all three sleep centers by senior sleep technicians certified by the Taiwan Society of Sleep Medicine (TSSM). The technicians acquired electroencephalogram (EEG), electrooculogram (EOG), electromyogram (EMG), ECG, oronasal airflow, thoracic and abdominal movements, oxyhemoglobin saturation, and body position data from the enrollees using the digital data acquisition systems at each site: TVGH (Philips Alice 5/6 PSG system, Philips Respironics Inc., Murrysville, PA, US); CMUH (NOX A1 PSG system, Nox Medical, Katrínartún, Iceland); and HTCH (EMBLA N7000 system, Embla Inc., Broomfield, CO, US).
PSG data were scored according to the AASM manual (VERSION 2.4).24 Apnea was defined as cessation of airflow lasting for at least 10 seconds.24 Hypopnea was scored based on a ≥30% reduction in airflow for at least 10 seconds, followed by a ≥4% oxygen desaturation (1B).24,25 This definition was applied uniformly across all three participating centers. The AHI was calculated as the average number of obstructive apneas and hypopneas per hour of sleep.26 OSA severity was classified according to PSG-derived AHI as normal (<5 events/h), mild OSA (5 to <15 events/h), moderate OSA (15 to <30 events/h), and severe OSA (≥30 events/h). The senior technicians at these three hospitals are highly experienced in scoring PSG. In addition to being certified by the TSSM, they also receive regular training and undergo periodic testing. Additionally, after completing training on a cloud-based PSG scoring platform, sleep technicians achieved high accuracy across sites: 82.7–93.5% for sleep-stage scoring, 88.7–93.9% for respiratory-event detection, and 87.3–90.7% for arousal recognition.27 Inter-scorer reliability was assessed using a 750-epoch reliability dataset. Pairwise sleep-stage agreement ranged from 82% to 90% across the three sites, with Cohen’s kappa values ranging from 0.711 to 0.830. Agreement for respiratory-event scoring ranged from 88.6% to 88.9%, and agreement for desaturation scoring ranged from 98.3% to 99.0% (Supplementary Table 1).
Cardiopulmonary Coupling and ECG Holter and Sleep Apnea and Sleep Quality Examination System
The CPC technique is based on continuous ECG signals and utilizes the Fourier transform to analyze two key features: (1) heart rate variability (HRV) and (2) respiration-related fluctuations in ECG R-wave amplitude. The latter provides ECG-derived respiration (EDR), which can be coupled with normal-to-normal (N–N) interval dynamics to characterize sleep-related cardiopulmonary oscillations. Published CPC methodology includes beat detection, extraction of N–N interval and EDR time series, outlier removal, and resampling at 2 Hz, followed by calculation of cross-spectral power and coherence within a 1024-sample window (approximately 8.5 minutes), advanced by 256 samples (approximately 2.1 minutes) across the recording.20,28
In the published CPC framework, elevated low-frequency coupling (e-LFC) is described as a subset of low-frequency coupled oscillations associated with apnea/hypopnea-related instability. One published research definition used a minimum low-frequency power >0.05 normalized unit together with a low-/high-frequency ratio >30.29 These published parameters are provided here to clarify the general CPC framework underlying respiratory event detection.
The present HSAT system uses a wireless ECG Holter attached to the participant’s left anterior chest to continuously record ECG signals throughout the overnight recording period. The recorded ECG signals are processed by the ST-SLP03A to generate a CPC-derived REI. Because the commercial implementation further tunes and optimizes the published CPC framework, the adjusted device-specific coefficients, thresholds, and internal decision rules used to generate the final REI output cannot be fully disclosed. The system therefore provides CPC-based sleep-state estimation, sleep stability assessment, and detection of sleep-disordered breathing, rather than formal AASM sleep staging based on EEG and EOG signals.20,21
Subgroup Analysis with Supplemental Oximetry
A predefined subgroup underwent simultaneous overnight monitoring with a fingertip pulse oximeter (FORA Pulse Oximeter, model TD-8255; ForaCare Inc., Taiwan) in addition to the CPC Holter. This subgroup was determined by site-level availability of the pulse oximeter during the study period. Oximetry signals were time-synchronized with the ECG recording, and the oxygen-desaturation index (ODI) was calculated. Diagnostic performance was evaluated by comparing (i) CPC-derived indices alone and (ii) CPC indices combined with ODI against PSG-derived AHI across the specified OSA severity thresholds.
Statistical Analysis
A formal a priori sample size calculation was not performed. The enrollment target was based on the anticipated accrual capacity of the participating centers during the study period. Microsoft SQL Server 2005 was used for data management and computing. Statistical analysis was performed using IBM SPSS Statistics Version 31.0 and MedCalc Version 23.1.6. All data were expressed as median with interquartile range (IQR) or percentage. Comparisons between two or more groups were performed using the Mann–Whitney U-test or Kruskal–Wallis test for continuous variables, and Pearson’s χ2-test for categorical variables, as appropriate. For comparisons of CPC-derived REI across PSG-defined OSA severity categories, the Kruskal–Wallis test was followed by Dunn’s multiple-comparison test for post hoc pairwise comparisons. Agreement and correlation were assessed using intraclass correlation coefficients (ICCs) for the average measures. Bland–Altman plots were used to visualize the mean difference between the two methods, with the 95% confidence interval (CI) for the estimated mean bias and the 95% limits of agreement. Spearman’s rank correlation coefficients (ρ) were calculated to assess the relationship between variables. Receiver operating characteristic (ROC) curves were plotted to evaluate the diagnostic performance of the model. The ROC analysis for PSG-defined AHI ≥ 5 events/hour was treated as the primary diagnostic analysis. ROC analyses for AHI ≥ 15 and ≥ 30 events/hour were treated as secondary analyses to evaluate performance across higher severity thresholds. The area under the curve (AUC) was calculated to quantify the model’s ability to discriminate between positive and negative cases. An optimal cutoff value and the Youden index (J) were derived from the ROC analysis. A two-sided p value < 0.05 was considered statistically significant.
Results
Baseline Characteristics of Study Subjects
A total of 500 participants were enrolled in this prospective study. After excluding 21 participants because of inadequate ECG/CPC signal quality that precluded reliable CPC analysis, 479 participants were included in the final analysis. Of these, 200 participants were enrolled from CMUH, 193 from TVGH, and 86 from HTCH, accounting for 41.8%, 40.3%, and 18.0% of the final cohort, respectively. Supplemental oximetry data were available for 109 of these participants (Figure 1). Among the overall study population, the proportion of males was 77.7%, with a median age of 42.0 years, a BMI of 27.5 kg/m2, and a neck circumference of 38.5 cm.
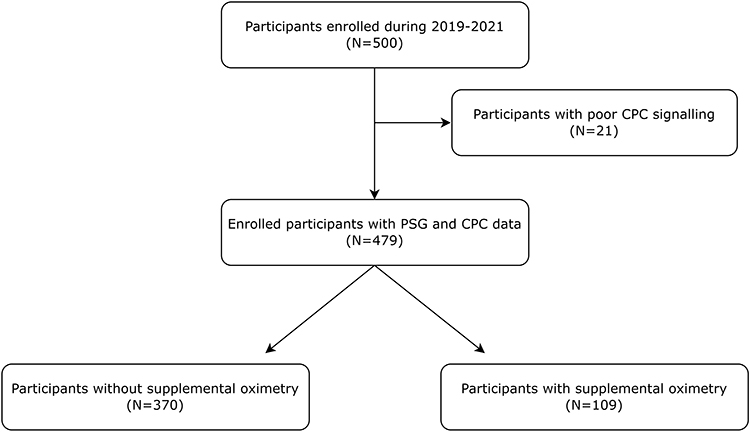 |
Figure 1 Study flow chart. |
According to PSG-derived AHI, participants were classified as normal (n=134), mild OSA (n=105), moderate OSA (n=83), and severe OSA (n=157). Across increasing OSA severity, the proportion of males increased from 64.2% in the normal group to 92.4% in the severe OSA group (p<0.001). Median age also differed across groups, with values of 35.0, 45.0, 46.0, and 46.0 years in the normal, mild, moderate, and severe OSA groups, respectively (p<0.001). Median BMI increased across severity groups from 25.0 to 30.0 kg/m2 (p<0.001), and median neck circumference increased from 37.0 to 41.0 cm (p<0.001). Hypertension was also more frequent with increasing OSA severity, occurring in 17.2%, 22.9%, 27.7%, and 39.5% of participants in the normal, mild, moderate, and severe OSA groups, respectively (p<0.001). Other comorbidities did not differ significantly across OSA severity groups (Supplementary Table 2).
REI Distribution, Agreement and Correlation with AHI
Figure 2A demonstrates the distribution of REI across different OSA severity groups. The Kruskal–Wallis test revealed a significant difference between the four groups (all p<0.05). To assess the agreement between REI and AHI, we performed an analysis of ICCs and Bland-Altman plots (Figure 2B). The ICC was 0.955, suggesting high overall consistency between REI and AHI at the cohort level. In the Bland–Altman analysis, the mean bias was small at −0.57 events/h, with a 95% confidence interval of −1.53 to 0.39 for the estimated mean difference. This confidence interval reflects the precision of the estimated mean bias rather than the limits of agreement for individual measurements. The 95% limits of agreement were −21.5 to 20.4 events/h, indicating substantial individual-level variability. Visual inspection of the Bland–Altman plot also showed greater dispersion of individual differences with increasing OSA severity, suggesting wider individual-level variability at higher event burdens. Additional analyses of the individual AHI components showed that CPC-derived REI correlated strongly with PSG-derived obstructive apnea index (Spearman’s ρ = 0.822, p<0.001) and moderately with PSG-derived hypopnea index (Spearman’s ρ = 0.604, p<0.001).
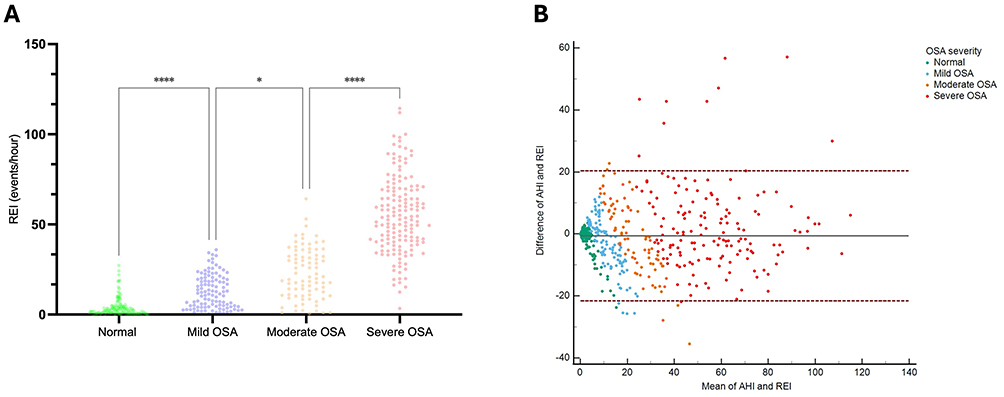 |
Figure 2 Distribution and agreement between CPC-REI and PSG-AHI. (A) REI across different OSA severity categories: Scatter plot showing REI values measured by CPC-HSAT across four groups based on PSG-defined AHI: normal (AHI < 5), mild OSA (AHI 5 to <15), moderate OSA (AHI 15 to <30), and severe OSA (AHI ≥ 30). REI differed across PSG-defined OSA severity groups. Adjacent pairwise comparisons shown in the figure were performed using Dunn’s multiple-comparison test following the Kruskal–Wallis test. **Comparisons across PSG-defined OSA severity groups were performed using the Kruskal–Wallis test followed by Dunn’s multiple-comparison test for post hoc pairwise comparisons. *p<0.05; ****p<0.0001. (B) Agreement between cardiopulmonary-coupling REI and PSG-defined AHI: Bland–Altman plot of the difference (AHI–REI, events/hour) versus the mean of the two measures for each participant. Dots are color-coded by OSA severity (Normal = green, Mild = light blue, Moderate = orange, Severe = red). Abbreviations: REI, respiratory event index; CPC-HSAT, cardiopulmonary coupling-home sleep apnea testing; PSG, polysomnography; AHI, apnea-hypopnea index. |
We further evaluated the correlation between AHI and REI across different subgroups using Spearman correlation. In the overall subjects, ρ was 0.889, with a 95% CI ranging from 0.87 to 0.91, indicating a statistically significant positive correlation between AHI and REI (p<0.001) (Figure 3A). Additionally, we observed a significantly high correlation between REI and ODI (Spearman’s ρ = 0.870, 95% CI: 0.85–0.89, p<0.001), which is also a good correlation, similar to the correlation between AHI and ODI (Spearman’s ρ = 0.987, 95% CI: 0.98–0.99, p<0.001) (Figure 3B and C). Subgroup analysis showed that REI also revealed a strong correlation with moderate to severe OSA (Spearman’s ρ = 0.843, 95% CI: 0.80–0.88, p<0.001) (Supplementary Figure 1 and Supplementary Table 3).
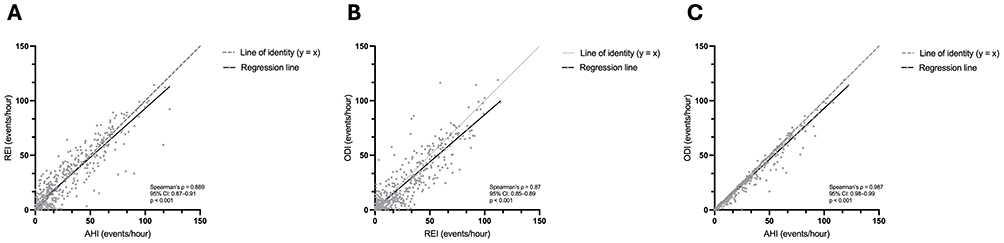 |
Figure 3 Correlations among CPC-derived REI, PSG-derived AHI, and PSG-derived ODI. (A) Scatter plot showing CPC-derived REI versus PSG-derived AHI for all study participants. Spearman’s ρ = 0.889 (95% CI, 0.87–0.91; p < 0.001). (B) Scatter plot showing PSG-derived ODI versus CPC-derived REI for all study participants. Spearman’s ρ = 0.870 (95% CI, 0.85–0.89; p < 0.001). (C) Scatter plot showing PSG-derived ODI versus PSG-derived AHI for all study participants. Spearman’s ρ = 0.987 (95% CI, 0.98–0.99; p < 0.001). The solid lines represent fitted linear regression lines. The dashed lines represent lines of identity (y = x), provided as visual references. Abbreviations: CPC, cardiopulmonary coupling; REI, respiratory event index; PSG, polysomnography; AHI, apnea-hypopnea index; ODI, oxygen desaturation index. |
ROC Analysis Between AHI and REI
To assess the diagnostic performance of REI, we performed ROC analyses across three PSG-defined AHI thresholds. The analysis for AHI ≥ 5 events/hour was treated as the primary diagnostic analysis, whereas the analyses for AHI ≥ 15 and ≥ 30 events/hour were considered secondary. For detecting OSA with AHI ≥ 5 per hour, the AUC was 0.923 (95% CI: 0.91–0.95, p<0.001) (Figure 4A and Supplementary Table 4). For OSA with AHI ≥ 15 per hour, the AUC was 0.929 (95% CI: 0.90–0.95, p<0.001) (Figure 4B). For identifying severe OSA (AHI ≥ 30 per hour) using REI, the AUC was the highest at 0.967 (95% CI: 0.95–0.98, p<0.001) (Figure 4C). These findings support good overall discriminatory performance of REI, with the primary analysis at AHI ≥ 5 events/hour and secondary analyses showing strong performance at higher OSA severity thresholds. Absolute classification counts and diagnostic performance across clinically matched thresholds are summarized in Table 1, whereas ROC-derived practical-threshold performance is provided in Supplementary Table 4.
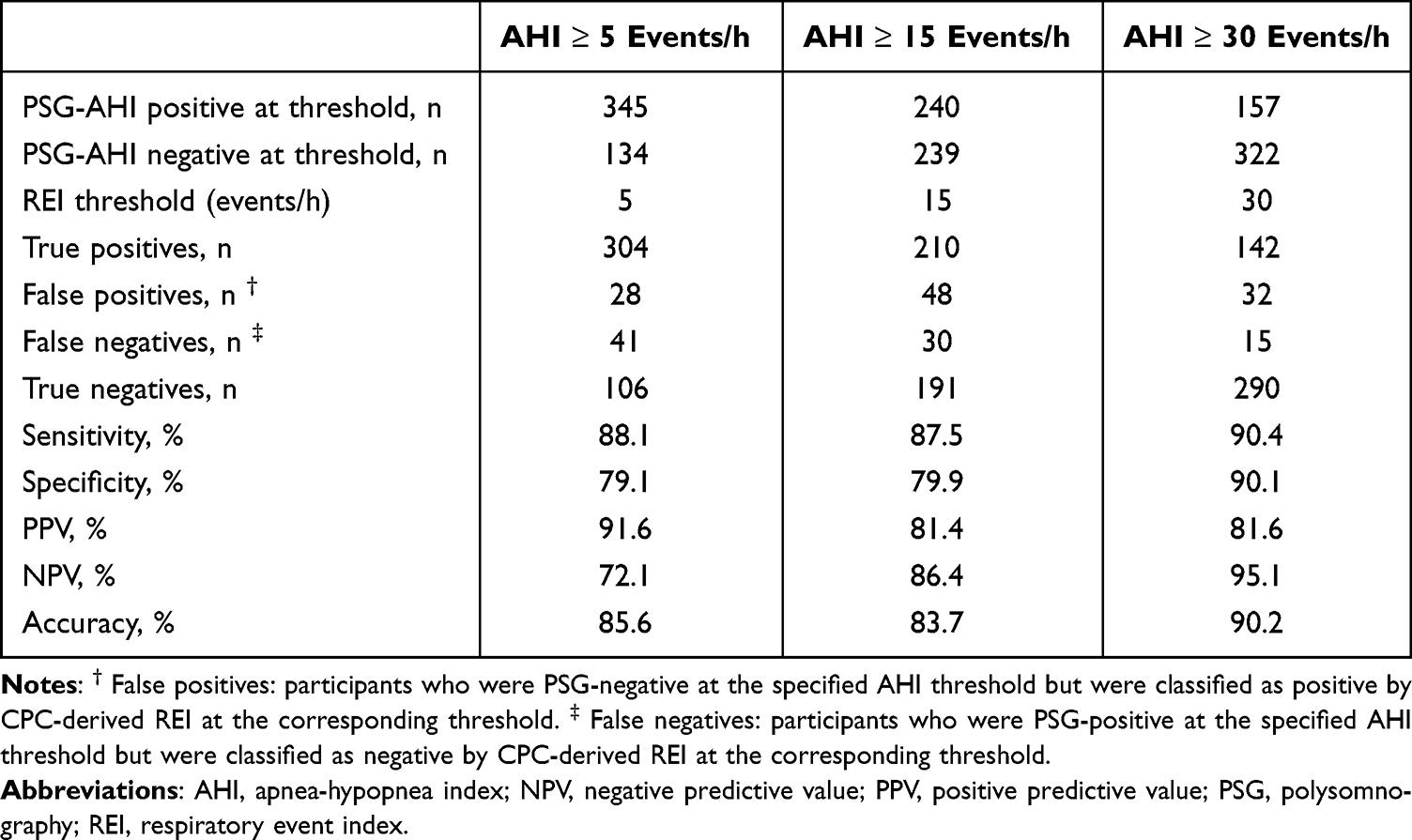 |
Table 1 Absolute Classification Counts and Diagnostic Performance of CPC-Derived REI at Clinically Matched PSG-AHI Thresholds |
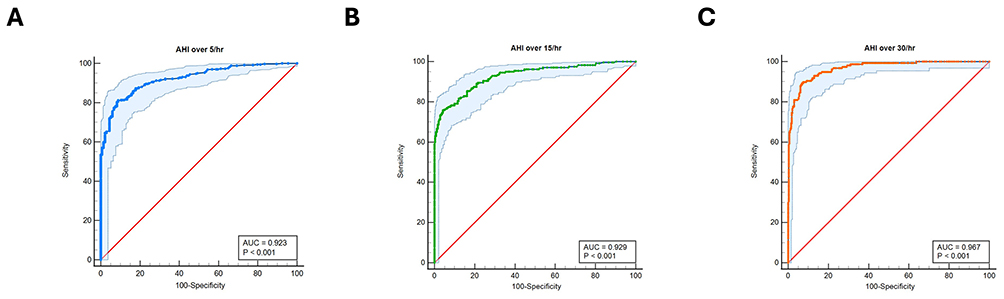 |
Figure 4 Receiver-operating-characteristic (ROC) curve for cardiopulmonary-coupling respiratory event index (REI) in detecting obstructive sleep apnea. (A) The ROC curve (solid blue) shows the ability of REI to identify participants with an apnea–hypopnea index (AHI) ≥ 5 events/hour. The light-blue band represents the 95% confidence interval, while the red diagonal denotes chance performance (AUC = 0.50). The area under the curve (AUC) is 0.923 (p<0.001). (B) The ROC curve (solid green) shows the ability of REI to identify participants with an apnea–hypopnea index (AHI) ≥ 15 events/hour. The light-blue band represents the 95% confidence interval, while the red diagonal denotes chance performance (AUC = 0.50). The area under the curve (AUC) is 0.929 (p<0.001). (C) The ROC curve (solid orange) shows the ability of REI to identify participants with an apnea–hypopnea index (AHI) ≥ 30 events/hour. The light-blue band represents the 95% confidence interval, while the red diagonal denotes chance performance (AUC = 0.50). The area under the curve (AUC) is 0.967 (p<0.001). |
Subgroup Analysis of Supplemental Oximetry
We next evaluated whether adding supplemental oximetry to the CPC-derived REI improved diagnostic performance with PSG-derived AHI. Baseline characteristics of participants with supplemental oximetry (n = 109) and those without supplemental oximetry (n = 370) are shown in Supplementary Table 5. Age, sex, BMI, and OSA severity distribution did not differ significantly between the two groups, whereas enrolling center distribution differed significantly, with a larger proportion of the oximetry subgroup enrolled at TVGH. Combining REI with oximetry raised the AUCs across all OSA severity thresholds. For AHI ≥ 5/h, the AUC was 0.981 (95% CI 0.93–1.00, p < 0.001; Supplementary Figure 2A); for AHI ≥ 15/h, 0.984 (95% CI 0.94–1.00, p < 0.001; Supplementary Figure 2B); and for AHI ≥ 30/h, 0.992 (95% CI 0.95–1.00, p < 0.001; Supplementary Figure 2C). Detailed metrics are provided in Supplementary Table 6.
Discussion
This prospective multicenter study evaluated a novel CPC-based sleep test in adults with clinically suspected OSA referred to tertiary sleep centers in Taiwan. CPC-derived REI showed good group-level performance compared with PSG-derived AHI, as reflected by strong association, high cohort-level consistency, and good ROC discrimination. However, Bland–Altman analysis demonstrated wide limits of agreement and greater individual-level variability at higher OSA severity, indicating that REI and AHI should not be considered interchangeable for individual-level severity classification. At the primary AHI ≥5 events/h threshold, CPC-derived REI missed 41 participants with PSG-defined OSA while incorrectly classifying 28 participants without OSA as positive. Additional analyses separating obstructive apnea and hypopnea indices showed that REI correlated more strongly with obstructive apnea index than with hypopnea index, further supporting cautious individual-level interpretation. Overall, these findings support the potential role of this CPC-based test as a simplified adjunctive tool for OSA evaluation in this referred clinical population.
Our results corroborate prior studies demonstrating the diagnostic utility of ECG-based CPC analysis for OSA.22,23 Ma et al reported AUCs of 0.90, 0.939, and 0.935 for detecting mild-or-greater, moderate-or-greater, and severe OSA, respectively, with a CPC-REI versus PSG-AHI correlation of 0.85 (p<0.001). A recent clinical trial by Lu et al introduced a cloud-based CPC analysis system (SleepImage Ring) that incorporates pulse oximetry fluctuations. The automatically derived AHI closely matched manual PSG scoring and demonstrated reliable diagnostic performance, with AUCs of 1.00, 0.90, and 0.98 for PSG-AHI thresholds of 5, 15, and 30 events/hour, respectively in 39 participants.23 Another study by Al Ashry et al demonstrated an accurate automated AHI derived from CPC combined with oximetry signals as well.30 Those systems integrate CPC parameters with hypoxic events, leading to an even higher correlation and AUC between the CPC index and AHI. Our prospective multicenter study showed that CPC-derived REI tracked PSG-derived AHI well at the group level, with strong correlation, high ICC, and good ROC performance. Nevertheless, Bland–Altman analysis demonstrated wider individual-level variability at higher OSA severity, indicating that REI and AHI should not be considered fully interchangeable.
Conventional Level 3 HSAT systems that use nasal pressure transducers, respiratory effort sensors, and pulse oximetry remain the most established and guideline-supported home-based diagnostic approach for appropriately selected adults with suspected OSA.8,10,17,18 These systems directly measure airflow reduction, respiratory effort, and oxygen desaturation and therefore have a strong clinical basis for identifying obstructive respiratory events.15 However, they may require multiple sensors, including nasal cannulas, which can increase setup burden and reduce patient tolerance in some home settings. These practical limitations have prompted the development of simplified wearable HSAT approaches. Fingertip-worn systems such as TipTraQ have shown promising diagnostic performance, highlighting the broader movement toward less burdensome sleep testing technologies.19 In this context, the present CPC-based system uses a single chest-worn ECG Holter with automated analysis, which may improve ease of use and patient acceptability. This simplified design may be useful as an adjunctive approach in referred patients with suspected OSA, but it should not be considered a replacement for conventional Level 3 HSAT or PSG. Although supplemental oximetry improved diagnostic performance in our study, this subgroup was not randomly assigned and differed in enrolling-center distribution; therefore, the oximetry-enhanced findings should be interpreted cautiously.
Despite increasing awareness, OSA remains substantially underrecognized in clinical practice. Model-based estimates suggest that approximately 936 million adults aged 30 to 69 years may have mild-to-severe OSA globally, including 425 million with moderate-to-severe disease; these estimates represent population-level disease burden rather than formally diagnosed cases.11,31 In this context, CPC-based testing may offer a practical adjunctive approach with potential clinical implications. By continuously monitoring heart rate variability and respiration using a single-lead chest-worn sensor, it substantially reduces the complexity and setup burden associated with in-laboratory PSG. This simplified design improves patient comfort and facilitates at-home or ambulatory testing, potentially expanding access to OSA diagnosis, especially in resource-limited or high-demand settings. Another important advantage is that the data analysis is fully automated, eliminating the need for sleep technician labor and reducing variability between interpreters. These features may support future evaluation of CPC-based testing as a scalable adjunctive approach in clinically referred or high-risk populations. Furthermore, beyond simply providing respiratory event index, CPC analysis offers additional insights into sleep structure and stability, such as quantifying stable versus unstable sleep through high-frequency and low-frequency coupling. This information has clinical significance, for instance, a prior study observed that e-LFCNB % is positively associated with blood pressure reduction following CPAP treatment.32 Future research may further explore the relationships between sleep architecture, CPC-derived metrics, and cardiovascular outcomes to elucidate the underlying mechanisms linking REI with clinical endpoints.
Our study has several strengths, including its prospective multicenter design and direct comparison of a novel CPC-based sleep test with in-laboratory PSG. The strong group-level association and consistency between REI and AHI support the validity of this approach, and the fully automated wireless system offers a scalable adjunctive option for OSA evaluation in this referred clinical population. Several limitations should be acknowledged. First, CPC may overestimate respiratory disturbances because it detects recurrent cardiopulmonary oscillations rather than PSG-defined airflow reductions. This may lower specificity in patients with fragmented sleep from non-OSA causes, such as chronic insomnia or major depression, which can produce low-frequency coupling patterns on ECG that mimic OSA.21,33,34 Additionally, 21 participants (4.2% of enrolled) were excluded due to inadequate CPC signal quality (eg, poor electrode contact, signal interference, or insufficient Holter wearing time). Second, the PSG reference standard in this study used the AASM 1B hypopnea criterion, defined by a ≥30% airflow reduction lasting at least 10 seconds with a ≥4% oxygen desaturation. This criterion was prespecified and applied uniformly across all three centers. Compared with the 3% desaturation or arousal-based 1A criterion, the 1B rule is more conservative and may yield lower AHI values, particularly near the AHI ≥5 events/h threshold. Prior PSG-based evidence has shown that hypopnea definitions can influence AHI values and OSA prevalence;26 however, the magnitude of this effect may vary by study population and cannot be directly inferred for the present referral-enriched cohort. Accordingly, at the AHI ≥5 events/h threshold, some participants classified as PSG-negative under the 1B definition may have been classified as PSG-positive under a 1A-based definition. Therefore, the reported sensitivity, specificity, PPV, NPV, and accuracy at AHI ≥5 events/h should be interpreted as performance against the prespecified AASM 1B PSG reference standard and should not be extrapolated directly to a 1A-based definition. Third, because REI was derived from ECG recording time rather than total sleep time, it may underestimate event severity in participants with low sleep efficiency. Body position was not evaluated in the present analysis, and residual positional effects may have contributed to individual-level variability between PSG-derived AHI and CPC-derived REI.35 Fourth, our cohort may not fully represent broader populations, as participants were recruited from three tertiary sleep centers in Taiwan and consisted predominantly of middle-aged men, with women, older adults, and non-Asian populations underrepresented. Because all participants were referred for in-laboratory PSG based on clinical suspicion of OSA, this referral-enriched sample had a higher pretest probability than an unselected community population, which may inflate observed sensitivity and limit the generalizability of diagnostic performance to primary care or screening settings. Minor inter-site differences in protocol execution and data quality, inherent to multicenter studies, may have introduced residual variability. Fifth, our study mostly focused on obstructive events, and the ability of CPC analysis to differentiate OSA from central sleep apnea was not explicitly explored. Previous research suggests that advanced ECG-based algorithms can distinguish between obstructive and central apneas by analyzing specific patterns in the coupling spectrogram,29 but this aspect was beyond our study’s scope and requires further exploration. Sixth, a formal a priori sample size calculation was not performed, and the target enrollment was based on recruitment feasibility across the participating centers rather than a prespecified diagnostic performance threshold. In addition, the ROC findings were not tested in an independent external validation cohort and should therefore be interpreted as internal validation results within this prospective multicenter cohort. Therefore, the study should be interpreted as a prospective multicenter validation study, and a larger cohort would allow more precise estimates across clinically relevant subgroups. Finally, this study was financially supported by the manufacturer of the evaluated device, which represents a potential conflict of interest and should be considered when interpreting the findings. Despite these limitations, our findings support the potential role of the CPC-derived REI as a simplified adjunctive tool for OSA evaluation in this referred clinical population.
Conclusions
In conclusion, in this multicenter cohort of adults with clinically suspected OSA referred to tertiary sleep centers in Taiwan, the CPC-based sleep test demonstrated good discriminatory performance against PSG-derived AHI. These findings suggest that it may serve as a simplified adjunctive tool for OSA evaluation in this specific clinical setting.
Abbreviations
OSA, obstructive sleep apnea; PSG, polysomnography; HSAT, home sleep apnea testing; TFDA, Taiwan Food and Drug Administration; ECG, electrocardiogram; CPC, cardiopulmonary coupling; REI, respiratory event index; BMI, body mass index; TSSM, Taiwan Society of Sleep Medicine; EEG, electroencephalogram; EOG, electrooculogram; HRV, heart rate variability; E-LFC, elevated low-frequency coupling; ODI, oxygen-desaturation index; IQR, interquartile range; ICC, intraclass correlation coefficient; CI, confidence interval; ROC, receiver operating characteristic; AUC, area under the curve.
Data Sharing Statement
The data that support the findings of this article are available from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Taipei Veterans General Hospital (VGHIRB No. 2019-11-005BC), the Institutional Review Board of China Medical University Hospital (CMUH109-REC1-055), and the Institutional Review Board of Hualien Tzu Chi Hospital (IRB108-150-B).
Author Contributions
Kun-Ta Chou: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Writing – Original Draft, Writing – Review & Editing
En-Ting Chang: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Writing – Review & Editing
Liang-Wen Hang: Conceptualization, Methodology, Supervision, Validation, Writing – Review & Editing
Chuan-Yen Sun: Methodology, Formal Analysis, Writing – Original Draft, Writing – Review & Editing
Diahn-Warng Perng: Supervision, Conceptualization, Writing – Review & Editing
Yung-Yang Liu: Supervision, Conceptualization, Writing – Review & Editing
Shiang-Fen Huang: Resources, Validation, Writing – Review & Editing
Fang-Chi Lin: Resources, Validation, Writing – Review & Editing
Kang-Cheng Su: Resources, Validation, Writing – Review & Editing
Tsu-Hui Shiao: Resources, Validation, Writing – Review & Editing
Yuh-Min Chen: Investigation, Writing – Review & Editing
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by Largan Health AI-Tech Company, Taiwan.
Disclosure
The study was financially supported by Largan Health AI-Tech Company, Taiwan, the manufacturer of the device evaluated in this study. This industry sponsorship represents a potential conflict of interest. The sponsor had no role in the study design, implementation, data analysis, data interpretation, article preparation, or decision to submit. The Authors report no further conflicts of interest in relation to this work.
References
1. Eckert DJ, Malhotra A. Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):144–11. doi:10.1513/pats.200707-114MG
2. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduction Targeted Ther. 2023;8(1):218. doi:10.1038/s41392-023-01496-3
3. Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690–702. doi:10.1111/resp.13838
4. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
5. Sforza E, Roche F. Chronic intermittent hypoxia and obstructive sleep apnea: an experimental and clinical approach. Hypoxia. 2016;4:99–108. doi:10.2147/hp.S103091
6. May AM, Mehra R. Obstructive sleep apnea: role of intermittent hypoxia and inflammation. Semin Respir Crit Care Med. 2014;35(5):531–544. doi:10.1055/s-0034-1390023
7. Aurora RN, Collop NA, Jacobowitz O, Thomas SM, Quan SF, Aronsky AJ. Quality measures for the care of adult patients with obstructive sleep apnea. J Clin Sleep Med. 2015;11(3):357–383. doi:10.5664/jcsm.4556
8. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
9. Fleetham J, Ayas N, Bradley D, et al. Canadian thoracic society 2011 guideline update: diagnosis and treatment of sleep disordered breathing. Can Respir J. 2011;18(1):25–47. doi:10.1155/2011/506189
10. Collop NA, Anderson WM, Boehlecke B, et al. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. Portable Monitoring Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2007;3(7):737–747.
11. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/s2213-2600(19)30198-5
12. Pei G, Ou Q, Shan G, et al. Screening practices for obstructive sleep apnea in healthy community people: a Chinese community-based study. J Thorac Dis. 2023;15(9):5134–5149. doi:10.21037/jtd-22-1538
13. Jaiswal SJ, Owens RL, Malhotra A. Raising awareness about sleep disorders. Lung India. 2017;34(3):262–268. doi:10.4103/0970-2113.205331
14. Chou TTC, Hsu HC, Twu CW, et al. Prevalence of obstructive sleep apnea using home sleep test in Taiwan during the coronavirus disease pandemic. Nat Sci Sleep. 2023;15:1107–1116. doi:10.2147/NSS.S434278
15. El Shayeb M, Topfer LA, Stafinski T, Pawluk L, Menon D. Diagnostic accuracy of level 3 portable sleep tests versus level 1 polysomnography for sleep-disordered breathing: a systematic review and meta-analysis. Cmaj. 2014;186(1):E25–51. doi:10.1503/cmaj.130952
16. Massicotte C, Al-Saleh S, Witmans M, Narang I. The utility of a portable sleep monitor to diagnose sleep-disordered breathing in a pediatric population. Can Respir J. 2014;21(1):31–35. doi:10.1155/2014/271061
17. Rosen IM, Kirsch DB, Carden KA, et al. Clinical use of a home sleep apnea test: an updated American Academy of sleep medicine position statement. J Clin Sleep Med. 2018;14(12):2075–2077. doi:10.5664/jcsm.7540
18. Rosen IM, Kirsch DB, Chervin RD, et al. Clinical use of a home sleep apnea test: an American academy of sleep medicine position statement. J Clin Sleep Med. 2017;13(10):1205–1207. doi:10.5664/jcsm.6774
19. Chen K-W, Tseng C-H, Lee H-C, Liu W-T, Chou K-T, Wu H-T. Validation of a fingertip home sleep apnea testing system using deep learning AI and a temporal event localization analysis. Sleep. 2025;48(5):zsae317. doi:10.1093/sleep/zsae317
20. Thomas RJ, Mietus JE, Peng CK, Goldberger AL. An electrocardiogram-based technique to assess cardiopulmonary coupling during sleep. Sleep. 2005;28(9):1151–1161. doi:10.1093/sleep/28.9.1151
21. Thomas RJ, Wood C, Bianchi MT. Cardiopulmonary coupling spectrogram as an ambulatory clinical biomarker of sleep stability and quality in health, sleep apnea, and insomnia. Sleep. 2018;41(2). doi:10.1093/sleep/zsx196
22. Ma Y, Sun S, Zhang M, et al. Electrocardiogram-based sleep analysis for sleep apnea screening and diagnosis. Sleep Breath. 2020;24(1):231–240. doi:10.1007/s11325-019-01874-8
23. Lu M, Brenzinger L, Rosenblum L, et al. Comparative study of the SleepImage ring device and polysomnography for diagnosing obstructive sleep apnea. Biomed Eng Lett. 2023;13(3):343–352. doi:10.1007/s13534-023-00304-9
24. Berry RB, Brooks R, Gamaldo C, et al. AASM Scoring Manual Updates for 2017 (Version 2.4). J Clin Sleep Med. 2017;13(5):665–666. doi:10.5664/jcsm.6576
25. Meoli AL, Casey KR, Clark RW, et al. Hypopnea in sleep-disordered breathing in adults. Sleep. 2001;24(4):469–470.
26. Hirotsu C, Haba-Rubio J, Andries D, et al. Effect of three hypopnea scoring criteria on OSA prevalence and associated comorbidities in the general population. J Clin Sleep Med. 2019;15(2):183–194. doi:10.5664/jcsm.7612
27. Liao YS, Wu MC, Li CX, Lin WK, Lin CY, Liang SF. Polysomnography scoring-related training and quantitative assessment for improving interscorer agreement. J Clin Sleep Med. 2024;20(2):271–278. doi:10.5664/jcsm.10852
28. Lu M, Penzel T, Thomas RJ. Cardiopulmonary Coupling. In: Penzel T, Hornero R, editors. Advances in the Diagnosis and Treatment of Sleep Apnea: Filling the Gap Between Physicians and Engineers. Springer International Publishing; 2022:185–204.
29. Thomas RJ, Mietus JE, Peng C-K, et al. Differentiating obstructive from central and complex sleep apnea using an automated electrocardiogram-based method. Sleep. 2007;30(12):1756–1769. doi:10.1093/sleep/30.12.1756
30. Al Ashry HS, Hilmisson H, Ni Y, Thomas RJ. Automated apnea-hypopnea index from oximetry and spectral analysis of cardiopulmonary coupling. Ann Am Thorac Soc. 2021;18(5):876–883. doi:10.1513/AnnalsATS.202005-510OC
31. Iannella G, Pace A, Bellizzi MG, et al. The global burden of obstructive sleep apnea. Diagnostics. 2025;15(9). doi:10.3390/diagnostics15091088
32. Ni YN, Lei F, Tang X, Liang Z, Hilmisson H, Thomas RJ. Cardiopulmonary coupling predictors of blood pressure response to positive airway pressure therapy. Sleep Med. 2024;124:576–581. doi:10.1016/j.sleep.2024.10.025
33. Yang AC, Yang CH, Hong CJ, et al. Sleep state instabilities in major depressive disorder: detection and quantification with electrocardiogram-based cardiopulmonary coupling analysis. Psychophysiology. 2011;48(2):285–291. doi:10.1111/j.1469-8986.2010.01060.x
34. Al Ashry HS, Ni Y, Thomas RJ. Cardiopulmonary sleep spectrograms open a novel window into sleep biology—implications for health and disease. Front Neurosci. 2021;15:755464. doi:10.3389/fnins.2021.755464
35. Alfaiate D, Pereira A, Guerra P, Pinto N. Body posture as a factor determining sleep quality in patients using non-invasive ventilation. Sleep Breath. 2023;27(6):2437–2442. doi:10.1007/s11325-023-02817-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.