Back to Journals » Vascular Health and Risk Management » Volume 19
The Effect of Transcutaneous Electrical Nerve Stimulation in Peripheral and Central Hemodynamic Parameters on Resistant Hypertension: A Case Report
Authors Giollo-Junior LT ![]() , Cosenso-Martin LN
, Cosenso-Martin LN ![]() , da Silva Lopes V
, da Silva Lopes V ![]() , Paz Landim M, Barufi Fernandes LA
, Paz Landim M, Barufi Fernandes LA ![]() , Aparecido de Oliveira K
, Aparecido de Oliveira K ![]() , Spaziani AO
, Spaziani AO ![]() , Santos AP
, Santos AP ![]() , Silva MA
, Silva MA ![]() , Yugar-Toledo JC
, Yugar-Toledo JC ![]() , Vilela-Martin JF
, Vilela-Martin JF ![]()
Received 10 February 2023
Accepted for publication 4 May 2023
Published 16 May 2023 Volume 2023:19 Pages 317—323
DOI https://doi.org/10.2147/VHRM.S408082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Daniel Duprez
Luiz Tadeu Giollo-Junior,1,2 Luciana Neves Cosenso-Martin,2 Valquiria da Silva Lopes,2 Manoel Paz Landim,2 Leticia Aparecida Barufi Fernandes,2 Kleber Aparecido de Oliveira,2 Amanda Oliva Spaziani,2 Aleandra Polegati Santos,2 Marco Antonio Silva,2 Juan Carlos Yugar-Toledo,2 Jose Fernando Vilela-Martin2
1General Hospital at Brazilian Army, Curitiba, Parana, Brazil; 2Hypertension Clinic - Internal Medicine Department, State Medical School in Sao Jose do Rio Preto (FAMERP), Sao Jose do Rio Preto, São Paulo, Brazil
Correspondence: Jose Fernando Vilela-Martin, Hypertension Clinic - Internal Medicine Department, State Medical School in Sao Jose do Rio Preto (FAMERP), Ave Brig. Faria Lima 5416, São Jose do Rio Preto, 15090-000, São Paulo, Brazil, Email [email protected]
Abstract: Resistant hypertension (RH) is characterized by being difficult to control, even with the use of various antihypertensive drugs and is associated with target organ lesions and other comorbidities. Thus, new treatment alternatives such as transcutaneous electrical nerve stimulation (TENS) can offer benefits to resistant hypertensive patients by reducing blood pressure (BP) in a non-invasive way and without the need for the association of more antihypertensive drugs. In this case, a patient with RH was submitted to three weekly applications of TENS on the stellate ganglion lasting 40 min each for 1 month. Peripheral and central hemodynamic assessments were performed by 24-h ambulatory BP monitoring (ABPM) before and after TENS applications. After completion of the TENS applications, significant reductions in office systolic (SBP) and diastolic BP (DBP) were observed. There was also a decrease in peripheral SBP and DBP in the 24‐h ABPM and sleep and SBP during wakefulness. Additionally, central parameters including central SBP and pulse wave velocity presented a significant reduction in the 24‐h ABPM, during the wakefulness and sleep. TENS is able to attenuate the sympathetic hyperactivity present in RH cases and decrease the peripheral and central hemodynamic parameters of a resistant hypertensive patient.
Keywords: resistant hypertension, blood pressure, central hemodynamic, arterial stiffness, non-pharmacological therapy
Introduction
Resistant hypertension (RH) is characterized by an increase in blood pressure (BP) above the recommended targets, even with the use of three antihypertensive drugs of different classes, including a renin–angiotensin system blocker (angiotensin converting enzyme inhibitor or angiotensin receptor blocker), a long-acting calcium channel blocker, and a long-acting thiazide diuretic.1 All of these drugs must have synergistic actions, be used in maximum recommended and tolerated doses, with proven adherence. Resistant hypertension is associated with extrinsic and intrinsic factors, such as advanced age, female gender, black race, increased salt intake, physical inactivity, obesity, left ventricular hypertrophy, diabetes mellitus, chronic nephropathy, metabolic syndrome, and autonomic changes, including sympathetic hyperactivity.1 Hypertensive individuals with RH have a worse prognosis than those with controlled hypertension because they present an elevated risk of target-organ damage, cardiovascular morbidity, and mortality. The Brazilian Society of Cardiology has already published two positions on RH, approaching specific recommendations for diagnosis, evaluation, and nonpharmacological and pharmacological treatments of this clinical situation.2,3
In recent years, options for treatment of RH are being evaluated, such as carotid baroreflex stimulation and the denervation of renal sympathetic ganglia, without presenting definitive results.4,5 Basically, these therapeutic methods reduce BP by inhibiting sympathetic activity. Recently, the study SPYRAL HTN-OFF MED (SPYRAL Pivotal) showed that catheter-based renal denervation was superior to a sham procedure and safe for lowering BP without use of antihypertensive medications.6 Additionally, RADIANCE-HTN TRIO demonstrated that endovascular ultrasound renal denervation, compared with a sham procedure, reduced BP in individuals with RH using a standardized triple combination antihypertensive therapy.7 However, these treatments are based on invasive techniques and present high financial costs.
On the other hand, transcutaneous electrical nerve stimulation (TENS) is a low-cost, noninvasive intervention that has been shown to reduce BP in experimental and human studies, including healthy and hypertensive individuals.8–12 Briefly, TENS is a non-pharmacological method that modulates the nervous system activity. TENS has also been used for treating or preventing ventricular tachycardia storm, postoperative cognitive dysfunction, migraine, fibromyalgia, pain relief and control, spasticity in spinal cord injury, and even for inducing analgesia.13–18 This case report describes the effects of TENS on peripheral and central hemodynamic parameters of a resistant hypertensive individual.
Case Presentation
The patient was a 53-year-old white woman with a 20-year history of hypertension and diabetes mellitus, with difficult-to-control BP. She was taking valsartan (320 mg/d), amlodipine (10 mg/d), chlorthalidone (25 mg/d), and spironolactone (100 mg/d), besides metformin (2000 mg/d), gliclazide (120 mg/d), dapagliflozin (10 mg/d), and 10U NPH insulin at bedtime. However, she did not adhere to diet to control diabetes. The patient was taking all the medications correctly, according to pill counts method used for assessing lack of adherence. Her physical examination revealed BP: 152×100 mm Hg (mean of three measures), heart rate: 78 bpm, weight: 80 Kg, body mass index (BMI): 32.1 kg/m2, and waist circumference: 91 cm. She had no abnormalities of the heart, lungs, or abdomen. According to complementary exams, the patient had unsatisfactory diabetes control with fasting glycemia of 308 mg/dL and glycosylated hemoglobin (HbA1c) of 9.8%; her creatinine level was 1.2 mg/dL with an estimated glomerular filtration rate of 52 mL/min/1.73 m2 (CKD-EPI). Her 24-h urinary sodium was 158 mEq/L. Other biochemical parameters (potassium, sodium, lipids, and microalbuminuria) were normal. The patient received all the orientations for lifestyle changes. In a 3- to 6-month period, she lost weight (approximately 6 kg – weight: 74 Kg and BMI: 29.5 kg/m2) and her HbA1c was reduced to 8.0%. Nevertheless, there was no improvement in office BP levels, which continued elevated (154×100 mm Hg). Patient was submitted to 24-h ambulatory blood pressure monitoring (24-h ABPM), which confirmed elevated BP levels (mean: 146.6×98.3 mm Hg), using the same antihypertensive drugs related above. All the investigations for secondary hypertension came out negative (renal artery stenosis, obstructive sleep apnea, primary hyperaldosteronism, and pheochromocytoma). Thus, we discussed the therapeutic options for the management of hypertension with the patient, and after her approbation, we started the evaluation with TENS.
The application of TENS was performed in the cervical-thoracic ganglion region, located between the vertebral processes C7 and T4, three times a week for 40 min for a total period of 4 weeks. An electrostimulator (Endomed 684, Enraf Nonius, Rotterdam, Netherlands) was used, containing two output channels, with a stimulus frequency of 80 Hz and pulse width of 150μs, with intensity adjusted in milliamps (mA), according to the sensitivity of the patient. This electrical stimulus has a high-frequency current that causes mild local paresthesia, without causing painful or unpleasant stimuli. The intensity was high, starting from zero, until the perceived sensation reached the maximum of the sensory limit, without pain, discomfort, or involuntary muscle contractions. Self-adhesive electrodes (dimensions 5×5 cm) were used for the stimulation coupled longitudinally over the patient’s skin, maintaining proper hygiene with the use of 70% alcohol to reduce bioimpedance, marking the previous demarcation of the site using a dermatographic pencil. The electrodes were always placed parallel to the spinal processes in C7 (channel 1) and T4 (channel 2) (Figure 1).10–12
 |
Figure 1 Diagram showing the location for application of the transcutaneous electrical nerve stimulation. |
Peripheral and central hemodynamic parameters [central systolic BP and pulse wave velocity (PWV)] were obtained through 24-h ABPM, with the Mobil-O-Graph® equipment (version 12, 2000, UK) according to the manufacturer’s instructions, before and immediately after the end of applications from the electric stimulation.
Important changes in hemodynamic parameters were seen after 4 weeks from TENS application (Table 1), with significant reductions of the office systolic BP (SBP) and diastolic BP (DBP). There was also a significant decrease in peripheral SBP and DBP in the 24‐h ABPM and sleep, and SBP during wakefulness. Additionally, central parameters including central SBP, and PWV presented a significant reduction during 24 h, wakefulness, and sleep in the ABPM. There were no alterations in metabolic and biochemical parameters (data not shown). One month after finishing the application of TENS, the office BP remained within the values considered normal (136 × 84 mm Hg).
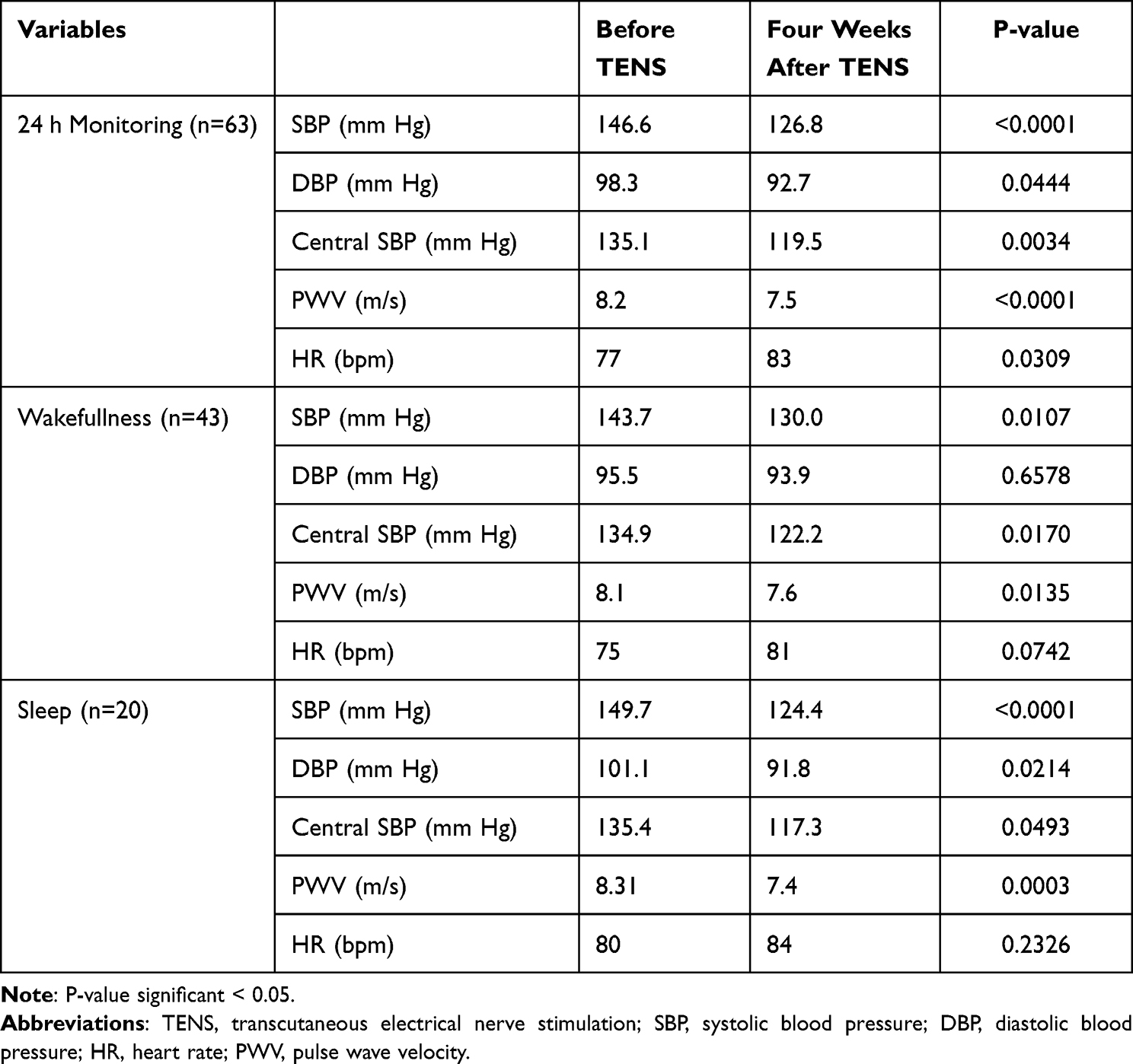 |
Table 1 Peripheral and Central Hemodynamic Parameters Observed in Ambulatory Blood Pressure Monitoring Before, and Immediately After Four Weeks from TENS Application |
Discussion
In this case report, we discuss the presentation of a middle-aged female subject with a history of uncontrolled hypertension in the long term, which was investigated for RH with all the diagnostic steps for excluding confounding factors, including pseudo-resistant hypertension.
It is common to find individuals with increased BP in an outpatient care specialized in hypertension, even when using three or more antihypertensive drugs, a fact that complies with the initial definition of RH and is compatible with the history of the patient, who was taking four antihypertensive drugs. Thus, for true RH diagnosis, we investigated causes of pseudoresistance. Causes of pseudo-RH are attributed to six principal etiologies—errors in BP measurement, white-coat effect, drugs prescription failure, use of medicines that elevate BP, poor adhesion to lifestyle alterations, and medical treatment. Moreover, causes of secondary hypertension were also excluded.19 Therefore, we decided to offer patients a new therapeutic option, which may reduce sympathetic modulation, increase vagal modulation, and decrease blood pressure in RH individuals.
In this report, there was a significant reduction in peripheral and central hemodynamic values immediately after four-week period from the application of TENS, an effect that remained by 1 month after the procedure, as evidenced with the office BP values. This therapeutic option represents a new method for the management of hypertension, it is an easy application, low cost, and it has low risk of adverse events. The hypotensive effect observed by the application of TENS can be explained by the inhibition of sympathetic activity, which is exacerbated in individuals with RH.20 Bang et al demonstrated significant reductions in systolic BP by directly stimulating the median nerve at different frequency ranges (3, 10, 30, and 300 Hz). The hypotensive effect was due to a reduction in sympathetic tone, at both low and high frequencies of stimulation.9 Sympathetic stimulation also acts adversely on metabolism, leading to greater insulin resistance and dyslipidemia.20 Spiridonov et al evaluated the effect of applying TENS on fructose-induced metabolic syndrome (MetS) parameters (12.5% of fructose solution as the only drinking source for 10 weeks) in male Wistar rats.8 The development of hypertension in this experimental model along with impaired glucose tolerance and increased serum concentration of triglycerides (TG) and lipid peroxidation products (LPO) caused a decrease in the content of serum blood calcitonin gene-related peptide (CGRP). Low-frequency TENS performed in 8 weeks after the beginning of fructose treatment reduced systolic BP and serum concentration of TG and LPO products and improved glucose tolerance. After TENS, CGRP content returned to normal values and the content of nitric oxide (NO) metabolites increased. It seems that CGRP and NO are involved in mechanisms mediating the therapeutic effect of low-frequency TENS on hypertension in this model.8
Insulin resistance and compensatory hyperinsulinemia observed in MetS may lead to activation of the sympathetic nervous system (SNS), oxidative stress, enhanced production of vasoconstrictors, inhibition of endothelial NO synthase (eNOS),21 and additional reduction of CGRP content in afferent neurons and nerve fibers innervating blood vessels.22 CGRP, a neurotransmitter of primary sensory neurons, produces a vasorelaxation effect mediated by NO and cyclic adenosine monophosphate (cAMP).23 Thus, a possible mechanism for the hypotensive effect and improvement of insulin resistance in MetS after low-frequency stimulation can be related to a decrease in activity of the SNS,12 activation of afferent nerves,24 and stimulation of the expression of the sensory nerve transmitter CGRP.25 Briefly, TENS modules the autonomic function, reducing SNS activity and increasing parasympathetic nervous system activity. Consequently, it may induce widespread cutaneous and muscular vasodilatation, as demonstrated in spontaneously hypertensive rats (SHR)24 and in patients with hypertension12,26 due to sympatho-inhibition. This response has been shown to be associated with a lowering of the systemic vascular resistance and blood pressure. Moreover, in patients with diabetes mellitus, there is carbohydrate and lipid metabolism normalization and improved insulin resistance in fructose-induced MetS.27 Since our patient also had MetS, these explanations could be related to the present case.
In this case, the stellate ganglion was used for TENS application, which is predominantly characterized by its sympathetic activity. Formed by the fusion of pre-ganglionic fibers from the lower cervical and upper thoracic ganglia,28 it influences cardiac electrical activity and the neuromodulation of peripheral blood vessels, causing the release of endogenous vasodilators.29 Previously, our group demonstrated the acute application of TENS attenuated arterial stiffness in healthy younger adults as well as hemodynamic measures in the middle-aged group.10 Recently, a Brazilian group demonstrated that the acute transcranial direct current stimulation (tDCS), a noninvasive procedure, decreased central and peripheral hemodynamic parameters and improved autonomic modulation in individuals with RH.30 Apparently, both methods (TENS and tDCS) present the same pathophysiological basis for reducing the central and peripheral BP, possibly mediated by autonomic modulation.
This case report has both strengths and limitations. Its strengths include the contribution of a low-cost, noninvasive, and clinically relevant intervention for treatment of RH, which could have implications in clinical practice. Nevertheless, some limitations should be considered. First, the major limitation is that the central hemodynamic parameters were obtained noninvasively by applying transfer function analysis to an oscillometric reconstructed waveform (Mobil-O-Graph) rather than via a direct measurement. Indeed, there are some questions about the principle of one-site central BP and PWV, measurements by oscillometry.31,32 However, oscillometry is a method that can be easily and conveniently employed for 24-h monitoring of central hemodynamics, a fact that allows to obtain repeated measurements in daily life conditions with hardly any discomfort to the patient. Additionally, the device used in this case has been properly validated versus alternative algorithms for computing arterial stiffness indexes and central hemodynamics, according to commonly accepted and standardized protocols. Several studies have documented a good agreement between the oscillometric cuff-based estimates of central BP and PWV measured by invasive methods and the established radial tonometry methods.33,34 Second, we do not know if the continuation of the application of TENS for a longer time will be able to improve the metabolic alterations. Finally, two important questions have not been answered in this case report: whether the hypotensive effect will persist after discontinuing TENS and if there will be a need for continued use of the procedure. In part, the first question has been answered since the office blood pressure remained controlled 1 month after discontinuing TENS.
Thus, even with evidence showing that TENS can influence sympathetic activity, positively interfere with metabolism, and reduce peripheral and central hemodynamic parameters, large-scale studies are needed, at different BP levels and with different dosages of electrical current to better elucidate its pathways, action, and its effects on the organism. Due to the high incidence of cardiovascular morbidity and mortality caused by RH, we have proposed a study with a more effective, highly specific, and non-invasive therapeutic approach that is reproducible and less costly from a financial point of view.35
Conclusion
In conclusion, to the best of our knowledge, this is the first report that suggests an effect of the TENS in the central and peripheral hemodynamic parameters of one resistant hypertensive patient. Anyway, given that one case report is not a proof of the effect of TENS in these parameters, a study that evaluates the effectiveness of TENS as an antihypertensive therapy in RH patients has been proposed in a higher number of individuals. We believe that other forms of non-pharmacological treatment and autonomic modulation, such as TENS application, should be experimented in cases of RH.
Abbreviations
ABPM, ambulatory blood pressure monitoring; BMI, body mass index; BP, blood pressure; CGRP, calcitonin gene-related peptide; cAMP, cyclic adenosine monophosphate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; DBP, diastolic blood pressure; eNOS, endothelial NO synthase; HbA1c, glycosylated hemoglobin; HDLc, high-density lipoprotein cholesterol; HR, Heart Rate; LDLc, low-density lipoprotein cholesterol; LPO, lipid peroxidation products; MetS, metabolic syndrome; NO, nitric oxide; PWV, pulse wave velocity; RH, Resistant hypertension; SBP, systolic blood pressure; TC, total cholesterol; TENS, transcutaneous electrical nerve stimulation; tDCS, transcranial direct current stimulation; TG, triglycerides.
Consent Statement
A statement confirming consent to publish the case has been obtained from patient. This statement is available if requested to corresponding author. An institutional approval was not required.
Acknowledgments
The authors would like to thank the reviewer for correcting both spelling and grammar of the English text.
Funding
Prof Jose F. Vilela-Martin is a researcher at The National Council for Scientific and Technological Development (CNPq - grant number #313715/2021-1) and of Sao Paulo Research Foundation (FAPESP - 2016/08203-6).
Disclosure
The authors declare that they have no competing interests.
References
1. Carey RM, Calhoun DA, Bakris GL, et al. Resistant hypertension: detection, evaluation, and management a scientific statement from the American heart association. Hypertension. 2018;72(5):e53–e90. doi:10.1161/HYP.0000000000000084
2. Alessi A, Brandão AA, Coca A, et al. First Brazilian position on resistant hypertension. Arq Bras Cardiol. 2012;99(1):576–585. doi:10.1590/s0066-782x2012000700002
3. Yugar-Toledo JC, Moreno Júnior H, Gus M, et al. Brazilian position statement on resistant hypertension – 2020. Arq Bras Cardiol. 2020;114(3):576–596. doi:10.36660/abc.20200198
4. Bhatt DL, Kandzari DE, O’Neill WW, et al. A controlled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370(15):1393–1401. doi:10.1056/NEJMoa1402670
5. Hoppe UC, Brandt MC, Wachter R, et al. Minimally invasive system for baroreflex activation therapy chronically lowers blood pressure with pacemaker-like safety profile: results from the Barostim neo trial. J Am Soc Hypertens. 2012;6(4):270–276. doi:10.1016/j.jash.2012.04.004
6. Böhm M, Kario K, Kandzari DE, et al. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED Pivotal): a multicentre, randomised, sham-controlled trial. Lancet. 2020;395(10234):1444–1451. doi:10.1016/S0140-6736(20)30554-7
7. Azizi M, Sanghvi K, Saxena M, et al.; on behalf of the RADIANCE-HTN TRIO. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO): a randomised, multicentre, single-blind, sham-controlled trial. Lancet. 2021;397(10293):2476–2486. doi:10.1016/S0140-6736(21)00788-1
8. Spiridonov VK, Tolochko ZS, Korolenko TA. Effect of transcutaneous electrical stimulation of nerves on blood pressure and blood content of neuropeptide CGRP and nitric oxide in hypertensive rats with metabolic disturbances. Bull Exp Biol Med. 2019;166(4):436–439. doi:10.1007/s10517-019-04367-6
9. Bang SK, Ryu Y, Chang S, et al. Attenuation of hypertension by C-fiber stimulation of the human median nerve and the concept based novel device. Sci Rep. 2018;8(1):14967. doi:10.1038/s41598-018-33402-1
10. da Silva ML, Chiappa GR, Silva VM, et al. Effect of transcutaneous electrical nerve stimulation on peripheral to central blood pressure ratio in healthy subjects. Clin Physiol Funct Imaging. 2016;36(4):293–297. doi:10.1111/cpf.12227
11. Oliveira MR, Lima KS, Righi NC, et al. Effects of interferential current on autonomic nervous system in healthy volunteers: randomized clinical trial. Saud Pesq. 2022;15(1):e8280. doi:10.17765/2176-9206.2022v15n2.e8280
12. Do Amaral Sartori S, Stein C, Coronel CC, Macagnan FE, Plentz RDM. Effects of transcutaneous electrical nerve stimulation in autonomic nervous system of hypertensive patients: a randomized controlled trial. Curr Hypertens Rev. 2018;14(1):66–71. doi:10.2174/1573402114666180416155528
13. Markman TM, Pothineni NVK, Zghaib T, et al. Effect of transcutaneous magnetic stimulation in patients with ventricular tachycardia storm: a randomized clinical trial. JAMA Cardiol. 2022;7(4):445–449. doi:10.1001/jamacardio.2021.6000
14. Zhang T, Ou L, Chen Z, Li J, Shang Y, Hu G. Transcutaneous electrical acupoint stimulation for the prevention of postoperative cognitive dysfunction: a systematic review and meta-analysis. Front Med. 2021;8:756366. doi:10.3389/fmed.2021.756366
15. Johnson MI, Claydon LS, Herbison GP, Jones G, Paley CA. Transcutaneous electrical nerve stimulation (TENS) for fibromyalgia in adults. Cochrane Database Syst Rev. 2017;10(10):CD012172. doi:10.1002/14651858.CD012172.pub2
16. Coutaux A. Non-pharmacological treatments for pain relief: TENS and acupuncture. Joint Bone Spine. 2017;84(6):657–661. doi:10.1016/j.jbspin.2017.02.005
17. Sivaramakrishnan A, Solomon JM, Manikandan N. Comparison of transcutaneous electrical nerve stimulation (TENS) and functional electrical stimulation (FES) for spasticity in spinal cord injury - A pilot randomized cross-over trial. J Spinal Cord Med. 2018;41(4):397–406. doi:10.1080/10790268.2017.1390930
18. Peng WW, Tang ZY, Zhang FR, et al. Neurobiological mechanisms of TENS-induced analgesia. Neuroimage. 2019;195:396–408. doi:10.1016/j.neuroimage.2019.03.077
19. Zanatta JMM, Cosenso-Martin LN, Lopes VS, et al. Evidence of nonadherence in cases of pseudoresistant hypertension. Integr Blood Pres Control. 2021;14:9–17. doi:10.2147/IBPC.S264057
20. Fisher JP, Paton JFR. The sympathetic nervous system and blood pressure in humans: implications for hypertension. J Hum Hypertens. 2012;26:463–475. doi:10.1038/jhh.2011.66
21. Tran LT, Yuen VG, McNeill JH. The fructose-fed rat: a review on the mechanisms of fructose-induced insulin resistance and hypertension. Mol Cell Biochem. 2009;332(1–2):145–159. doi:10.1007/s11010-009-0184-4
22. Zamami Y, Takatori S, Hobara N, et al. Hyperinsulinemia induces hypertension associated with neurogenic vascular dysfunction resulting from abnormal perivascular innervations in rat mesenteric resistance arteries. Hypertens Res. 2011;34(11):1190–1196. doi:10.1038/hr.2011.97
23. Russell FA, King R, Smillie SJ, Kodji X, Brain SD. Calcitonin gene-related peptide: physiology and pathophysiology. Physiol Rev. 2014;94(4):1099–1142. doi:10.1152/physrev.00034.2013
24. Huo ZJ, Li Q, Tian GH, et al. The ameliorating effects of long-term electroacupuncture on cardiovascular remodeling in spontaneously hypertensive rats. BMC Complement Altern Med. 2014;14:118. doi:10.1186/1472-6882-14-118
25. Ding L, Song T, Yi C, et al. Transcutaneous electrical nerve stimulation (TENS) improves the diabetic cystopathy (DCP) via up-regulation of CGRP and cAMP. PLoS One. 2013;8(2):e57477. doi:10.1371/journal.pone.0057477
26. Kaada B, Flatheim E, Woie L. Low-frequency transcutaneous nerve stimulation in mild/moderate hypertension. Clin Physiol. 1991;11(2):161–168. doi:10.1111/j.1475-097x.1991.tb00109.x
27. Tominaga A, Ishizaki N, Naruse Y, Kitakoji H, Yamamura Y. Repeated application of low-frequency electroacupuncture improves high-fructose diet-induced insulin resistance in rats. Acupunct Med. 2011;29(4):276–283. doi:10.1136/acupmed-2011-010006
28. Slappendel R, Thijssen H, Crul B, Merx J. The stellate ganglion in magnetic resonance imaging: a quantification of the anatomic variability. Anesthesiology. 1995;83(3):424–426. doi:10.1097/00000542-199508000-00026
29. Wu M, Linderoth B, Foreman RD. Putative mechanisms behind effects of spinal cord stimulation on vascular diseases: a review of experimental studies. Auton Neurosci. 2008;138(1–2):9–23. doi:10.1016/j.autneu.2007.11.001
30. Rodrigues B, Barboza CA, Moura EG, et al. Acute and short-term autonomic and hemodynamic responses to transcranial direct current stimulation in patients with resistant hypertension. Front Cardiovasc Med. 2022;9:853427. doi:10.3389/fcvm.2022.853427
31. Boutouyrie M, Revera M, Parati G. Obtaining arterial stiffness indices from simple arm cuff measurements: the holy grail? J Hypertens. 2009;27(11):2159–2161. doi:10.1097/HJH.0b013e328332f588
32. Westerhof BE, van den Wijngaard JP, Murgo JP, Westerhof N. Location of a reflection site is elusive: consequences for the calculation of aortic pulse wave velocity. Hypertension. 2008;52(3):478–483. doi:10.1161/HYPERTENSIONAHA.108.116525
33. Wolfgang W, Gohlisch C, Harsch-Gladisch C, et al. Oscillometric estimation of central blood pressure: validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press Monit. 2012;17(3):128–131. doi:10.1097/MBP.0b013e328353ff63
34. Gotzmann M, Hogeweg M, Seibert FS, et al. Accuracy of fully automated oscillometric central aortic blood pressure measurement techniques. J Hypertens. 2020;38(2):235–242. doi:10.1097/HJH.0000000000002237
35. Vilela-Martin JF, Giollo-Junior LT, Chiappa GR, et al. Effects of transcutaneous electrical nerve stimulation (TENS) on arterial stiffness and blood pressure in resistant hypertensive individuals: study protocol for a randomized controlled trial. Trials. 2016;17:168. doi:10.1186/s13063-016-1302-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Longitudinal Associations Between Metabolic Risk Burden and the Cardio–Ankle Vascular Index (CAVI) in Japan Using Health-Check Cohort
Horibuchi Y, Aluariachy L, Yamaura R, Kasahara H, Tsugane S, Yamazaki T
Vascular Health and Risk Management 2026, 22:601750
Published Date: 8 May 2026