Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
The effect of the behavior modification program Dietary Approaches to Stop Hypertension (DASH) on reducing the risk of hypertension among elderly patients in the rural community of Phayao, Thailand
Authors Seangpraw K ![]() , Auttama N, Tonchoy P, Panta P
, Auttama N, Tonchoy P, Panta P ![]()
Received 4 September 2018
Accepted for publication 14 November 2018
Published 31 January 2019 Volume 2019:12 Pages 109—118
DOI https://doi.org/10.2147/JMDH.S185569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Katekaew Seangpraw,1 Nisarat Auttama,1 Prakasit Tonchoy,1 Pitakpong Panta2
1School of Medicine, University of Phayao, Phayao 56000, Thailand; 2School of Nursing, University of Phayao, Phayao 56000, Thailand
Aim: The purpose of this study was to evaluate the effect of the Dietary Approaches to Stop Hypertension (DASH) program with self-efficacy on reducing the risk of hypertension among elderly patients in the rural community of Phayao Province in Northern Thailand.
Patients and methods: A quasi-experimental study was employed among elderly patients in the rural community of Phayao. Multistage random sampling was used to select a study area with similar characteristics. Ninety elderly participants were placed in the intervention group and 85 elderly participants from the same village were placed in the control group. The intervention group used the behavior modification guidelines of the DASH program with self-efficacy for 3 months, including 45-minute weekly group education meetings, 25-minute group activity training sessions, and a 15-minute individual checklist. A control group received no intervention. Data were collected by using self-administered questionnaires. The analyses included descriptive statistics, the Mann−Whitney U-test, and sample t-testing. Three different time periods were examined using repeated measures ANOVA.
Results: More than half of the participants (65.7%) were aged 60–69 years. The results from comparison of the intervention and control groups showed that the perceived severity of hypertension and self-efficacy had increased and preventive behaviors toward hypertension had improved in both groups. There were statistically significant differences after the intervention and at 3-month follow-up (P<0.001). After the intervention, the systolic blood pressure and diastolic blood pressure of the elderly people in the intervention group had decreased (P<0.001)
Conclusion: The behavior modification guidelines of the DASH program with self-efficacy, were effective in improving the mean score of perceived severity, self-efficacy, and preventive behaviors among elderly participants with a high risk of hypertension. Furthermore, the program was effective in lowering blood pressure and it may be useful in controlling stage 1 hypertension in elderly people.
Keywords: risk hypertension, behavior modification, DASH, elderly patients, self-efficacy, rural community
Introduction
Hypertension is one of the major public health problems. It is expected that the prevalence of hypertension worldwide will increase to 1.56 billion people in 2025.1 Hypertension is a leading cause of death among Thai people and it is expected to continuously increase in all regions of Thailand.2 According to two reports by the Ministry of Public Health, diseases related to the circulatory system were ranked the third most common cause of illness among Thai people aged ≥60 years who were admitted to hospital in 2014.2,3 The overall morbidity rates of hypertension patients who had received treatment from health services from 2007 to 2011, were 778.1, 860.5, 1,230.2, 1,349.4, and 1.187 cases per 100,000 people, respectively.2,3 According to the Situation of the Elderly in 2016, the data showed that in female and male elderly people aged 66–69 years, 47.0%, 50.0%, 59.0%, and 69.0%, respectively, were reported to have hypertension. In female and male elderly people aged ≥70 years, >50% were reported to have hypertension.4
National statistics from the Bureau of Policy and Strategy, Ministry of Public Health, 2015–2017, showed that Northern Thailand had a prevalence of hypertension that was higher than the average of the whole country.2,4 In 2011, the incidence of hypertension was found to be one of the top five diseases in Phayao Province and the disease has been monitored ever since according to the policy of the Ministry of Public Health.5 In a group of the elderly (excluding current patients) from the Muang District, Phayao who were suspected of having hypertension, a blood pressure (BP) screening test showed systolic BP (SBP) ≥140 mmHg or diastolic BP (DBP) ≥90 mmHg. There was an increase in the number of elderly people with hypertension of 2.8% – 3.0% in the years 2016–2017, respectively.4 When divided into gender, more females than males had high BP (53.4% and 46.6%, respectively).4,5 The prevalence had increased from 2015 to 2017 (58.1%, 60.3%, and 62.6%, respectively).5 This indicates that many elderly people have high BP and it continues to increase with age. As age increases, health functions and circulatory systems decline. Having high BP can cause many health problems, such as heart disease and coronary disease, and health complications, including eye, kidney, and brain problems.6 Health problems lead elderly people to financial burden because of healthcare expenses and related costs.6 Health professionals should focus on the prevention and treatment of high BP and its complications from an early stage in order to delay health problems and other complications. From the epidemiological study of hypertension, one of the important risk factors is eating behaviors. Eating behaviors can have a direct impact on BP, especially if the food contains high amounts of sodium.6,7
Therefore, modifying dietary habits is of key importance in preventing high BP.8 Several foreign studies regarding the control and prevention of hypertension applied the Dietary Approaches to Stop Hypertension (DASH)9 program as a guideline to emphasize the necessity of eating rice, flour, whole grains, dried beans, lean meat, nonfat milk, vegetables, and fruits in reasonable portions, which helped lower BP from 8 to14 mmHg.9,10 Controlling sodium intake to not exceed 2,400 mg/day, or the equivalent of 1¼ teaspoon, helped lower BP from 2 to 8 mmHg and also controlled weight and alcohol intake.9,10 This study showed modifying dietary habits as indicated by the DASH program, and including education and activity training, helped increase confidence among patients with high BP and people in a risk group of hypertension after the intervention. A previous study showed the results of the intervention group came out better than the patients in the control group and there were significant differences in the mean scores of SBP and DBP before and after the intervention.7 Modifying dietary behaviors can help control BP and prevent health complications from hypertension. A nutrition program, by providing detailed knowledge on nutrition, requires a behavioral health theory approach to stimulate learning and raise awareness and confidence in order to change eating behaviors among patients.11
Therefore, the researcher in this study was interested in evaluating the dietary behavior modification program DASH with self-efficacy12 in order to reduce the risk of hypertension among the elderly as well as to motivate elderly people to have healthy dietary behaviors in order to prevent hypertension. This helps reduce health-related costs, lowers family burden, and promotes healthy living among the elderly.
Patients and methods
A quasi-experimental research project including two groups (pre- and posttest design) was undertaken at a rural community in Phayao. Inclusion criteria included the following: both male and female participants; aged 60–80 years old; had a health screening in the fiscal year of 2017; had been diagnosed with hypertension for at least 1 year; had a risk of stage 1 high BP according to Thai Hypertension Society guidelines (SBP ≥140 mmHg and/or DBP ≥90 mmHg);13 could not control their BP within 1 month; did not change their dose or increased their dose intake for BP medication; did not change their exercise habits during the intervention; received treatment at the Hypertension Clinic at Bantam and Thajumpee Health Promoting Hospital; were able to communicate by phone; and were willing to participate in the study. Exclusion criteria included participants who were not able to participate throughout the entire study. Sample size was calculated using a formula to compare the mean of the two independent groups, with the significance level equal to 0.05 (1.64), power equal to 0.8, and the size effect was 0.59, obtained from a similar intervention study by Noordzij et al.7,14 The total sample size was 175 people with an increase of 10% to allow for the dropout rate. Ninety elderly participants were in the intervention group and 85 elderly participants were in the control group. The study was conducted from November 2017 to April 2018. Multistage random sampling was employed to select a study area with similar characteristics and a lottery draw was used to select districts. Bantam Subdistrict was selected for the intervention group and Thajumpee Subdistrict was selected for the control group. Cluster random sampling was employed to select the village; one village for the intervention group and one village for the control group. Next, simple random sampling without replacement was used to select participants (Figure 1).
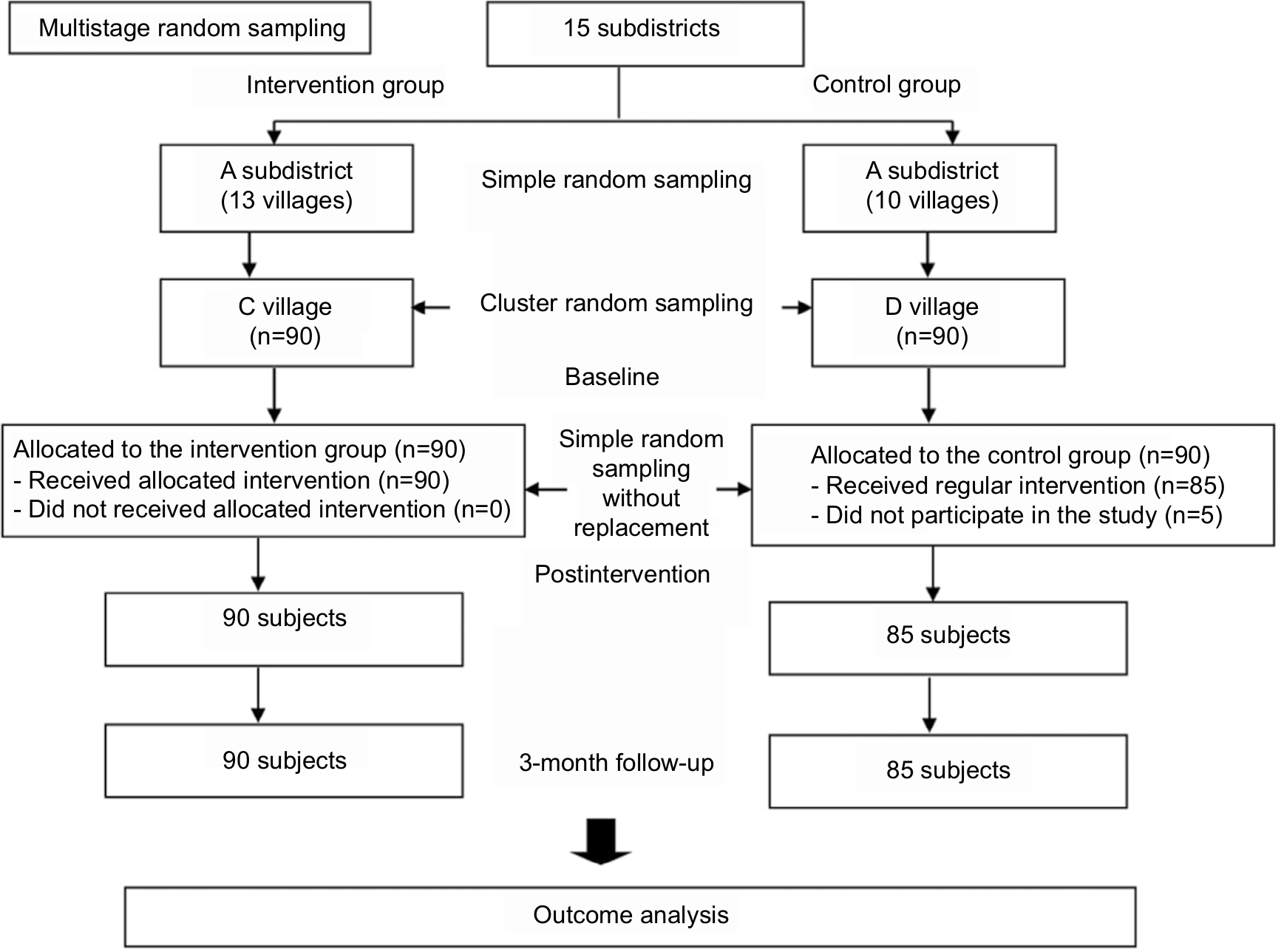 | Figure 1 Flowchart of participants throughout the study. |
Instruments
Instruments were divided into two parts: a data collection instrument and an intervention instrument. The data collection instrument included four parts. 1) Demographic characteristics (gender, age, education, income, history of health, BP, body mass index [BMI], and health behaviors). 2) A questionnaire constructed to assess the perceived severity of hypertension. 3) A perceived self-efficacy questionnaire on dietary behaviors according to the DASH program.7,8,12 The questionnaires in parts 2) and 3) employed four rating scales to evaluate knowledge. Participants had to choose one answer that matched with their opinion. The answers were provided with positive and negative scores ranging from 8 to 32.15 A higher score showed greater perceived self-efficacy by elderly people.7,8,12 4) An applied questionnaire on dietary behaviors according to the DASH program guidelines.7,8,12 The questions were designed to assess each dietary practice activity among elderly people, particularly whether the practice was correct or not, the quality of practice, and the frequency of practice depending on each activity. The questionnaire had three rating scales: 1) practice >3–4 times per week; 2) practice 1–2 times per week; and 3) rarely practice/no practice. The scores ranged from 8 to 24. The higher score showed better practice among elderly people. To ascertain the validity of the questionnaire, it was checked by three experts. The reliability test was calculated using Cronbach’s alpha coefficient; parts 2 and 4 were evaluated at 0.80 and 0.84, respectively. The reliability result of BP level used in this study was referred from the Thai Hypertension Society according to masked hypertension (MH) used widely in the clinic or health promoting hospitals.13
Intervention instrument was applied from DASH9 by the National Institutes and self-efficacy theory12 to design the study program (Table 1). Seven village health volunteers (research assistants) were recruited for the study. The researcher explained in detail to the research assistants how to use the data collection instruments and the evaluation process (in took the researchers 3 hours to explain). The elderly participants in the intervention group received a dietary record manual for recording every meal (three meals/day). They also received self-practice exercise training once a week for a total of 3 months. The program was divided into three sections. 1) Education regarding the severity of hypertension and the local food of Northern Thailand according to the DASH diet. The program emphasized the importance of reducing consumption of food containing a high level of sodium (should not exceed 2,300 mg/day), avoiding various condiments such as salt (should not exceed one teaspoon/day), fish sauce (should not exceed 3–4 teaspoons/day), and white soy sauce (should not exceed 5–6 teaspoons/day). Certain local food, including Sa eggplants, Noom chili paste, Ong chili paste, Larb port, Care curry, and Hoh curry, contain high quantities of sodium. Elderly people should be educated about their local food and advised that they should reduce eating salty food, such as salty fish, sour port, canned food, and fermented food, and sweet food, such as cake and bread. Education training ran twice for 45 minutes each session. 2) Group activity training ran four times for 25 minutes each session, along with two home visits. Elderly people were contacted by phone and asked about their self-practice activity at home so that the research assistants could evaluate the elderly participants’ understanding of dietary behaviors as prescribed by the DASH program and stimulate their motivation to practice these behaviors (Table 1). 3) Self-evaluation with regards to self-efficacy12 was performed four times for 15 minutes each time. Self-efficacy is the confidence of the individual that he or she is capable of performing activities as prescribed. This study applied self-efficacy in the program because elderly people should have confidence that they understand that having healthy behaviors are good for their health, eg, choosing a healthy diet, avoiding junk or high-sodium food, and exercising regularly (15–20 minutes, 3–5 times per week).7,12 The elderly participants in the control group received a standard education regarding dietary requirements as provided by health promoting hospital staff within the community. Data collection was done pre- and postintervention and at 3-month follow-up.
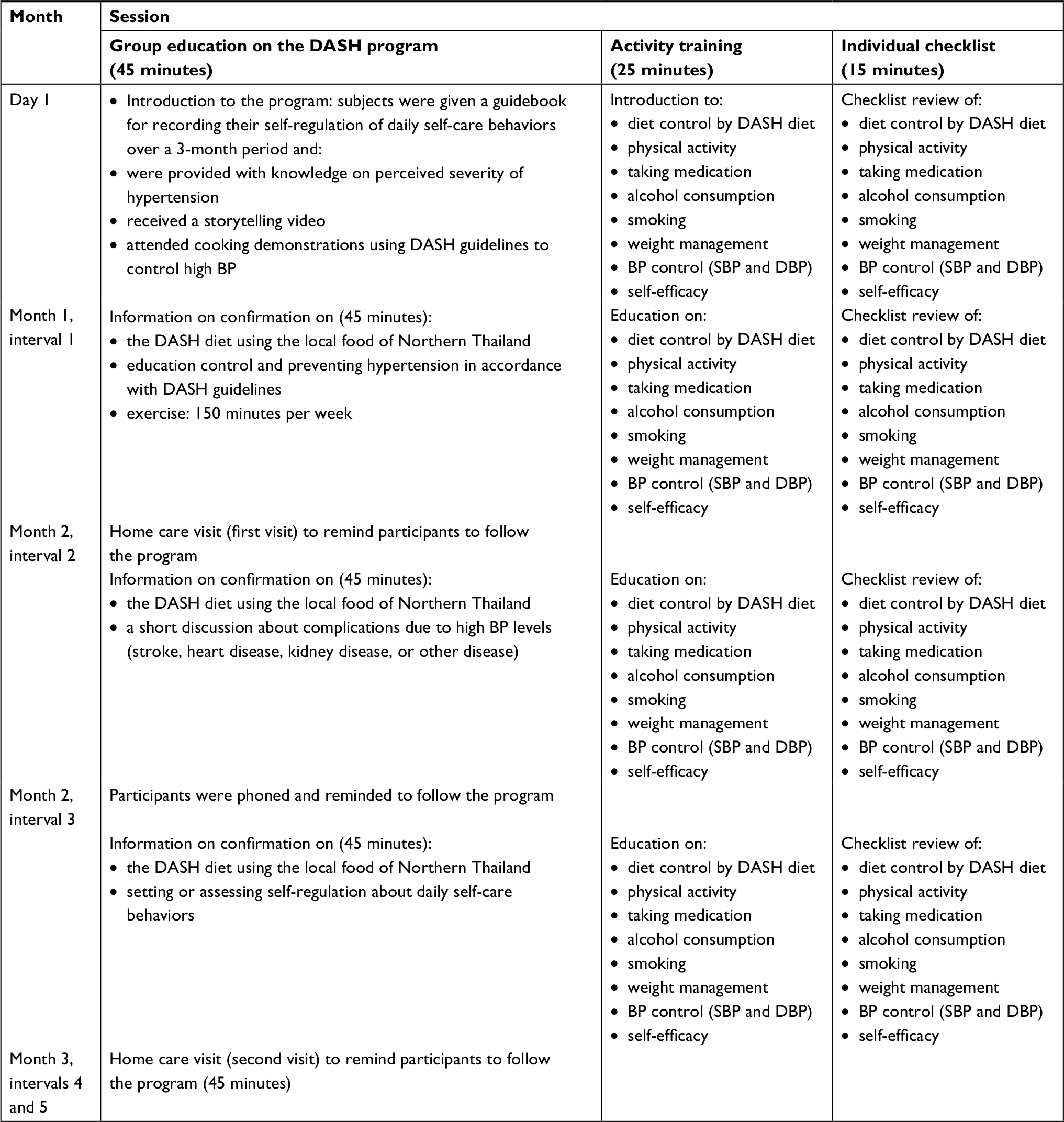 | Table 1 DASH diet program schedule Abbreviations: BP, blood pressure; DASH, Dietary Approaches to Stop Hypertension; DBP, diastolic BP; SBP, systolic BP. |
Data analysis
Data was analyzed using the SPSS Statistics version 20.0. Descriptive statistics, chi-squared tests, and independent t-tests were used to identify differences between the intervention and control groups on baseline measurement of the elderly’s characteristics. Repeated measures ANOVA was used to test the effects of the interventional program. The level of significance for all the statistical tests was set at P<0.05.
Ethical consideration
This study was approved by the Ethics Review Committee for Research Involving Human Research Subjects at the University of Phayao (approval number 2/100/59). Prior to taking part in the study, the study objectives and data collection processes were fully explained to the subjects, who then signed a written consent form to indicate their willingness to join the study. This study was in compliance with the ethical principles of the Declaration of Helsinki.
Results
The participants in this study were similar in both the intervention (n=90) and control groups (n=85). More than half (65.7%) of the participants in the intervention and control groups were aged 60–69 years. A total of 53.3% of participants were female in the intervention group compared to 57.6% in the control group. In the intervention group, 57.7% were married compared to 64.7% in the control group. More than 41.7% of the participants in both the intervention and control groups had achieved an education level of grade 6. In the intervention group, 75.6% had sufficient income compared to 84.7% in the control group. Both groups had a medical history of disease: 18.9% in the intervention group and 17.6% in the control group. Approximately 70.5% of the participants had type 1 diabetes complications in the intervention group compared to 93.3% in the control group. It could be that the subjects in the intervention and control groups had similar characteristics at baseline. There were no significant differences for demographic data and health behaviors between the intervention and control groups (Table 2). From the total of 175 elderly participants (90 in the intervention group and 85 in the control group), there were no significant differences on the levels of SBP, DBP, BMI, dietary habits/tasty food, types of physical activity, alcohol intake, and smoking (P=0.520, P=0.199, P=0.090, P=0.409, P=0.373, P=0.340, and P=0.252, respectively) (Table 3). This confirms that both groups have similar characteristics.
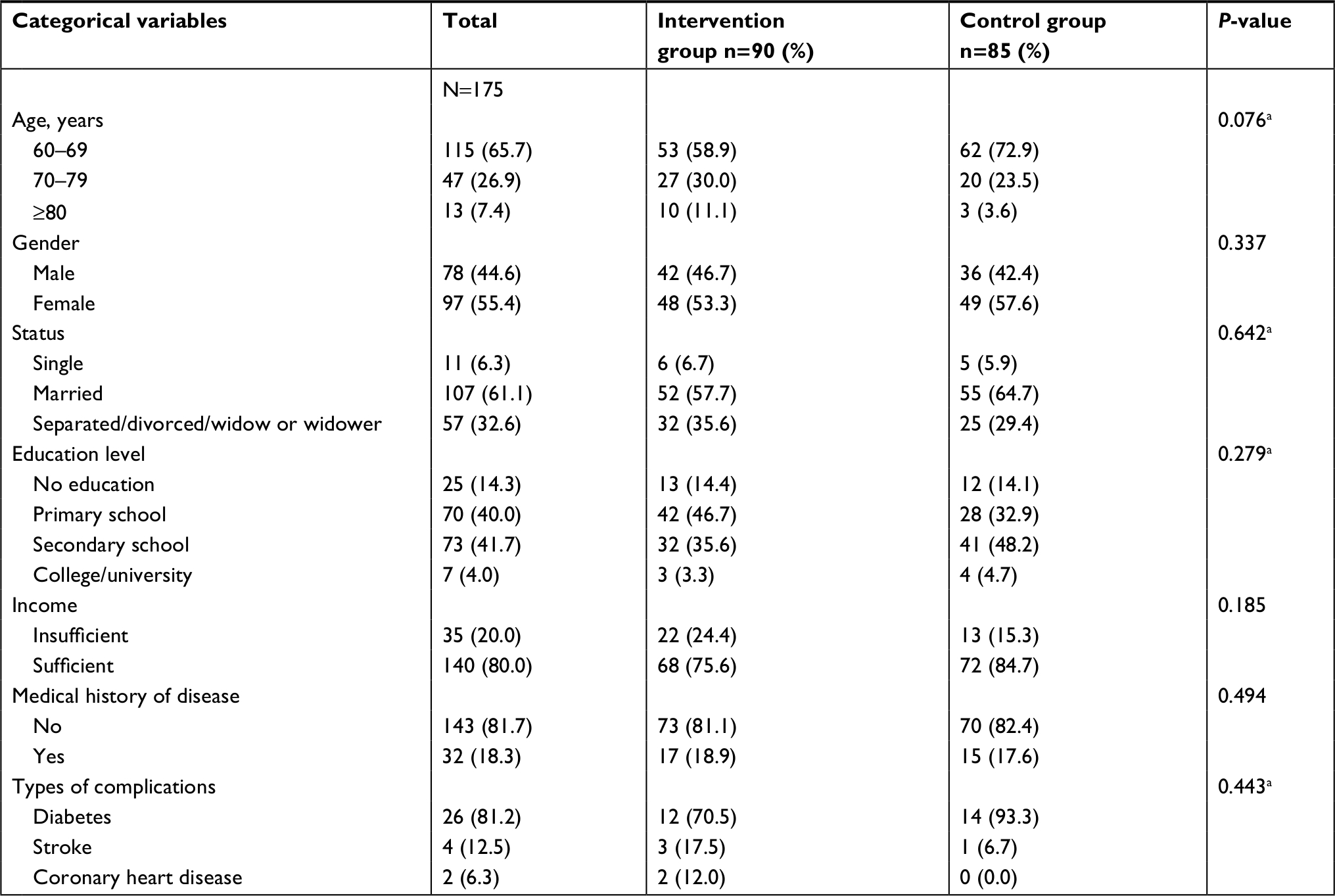 | Table 2 Comparison of the participants’ categorical variables between the intervention and control groups (N=175) Notes: aP-values were calculated using ‘Fisher’s exact test. bStatistical significance P<0.05. |
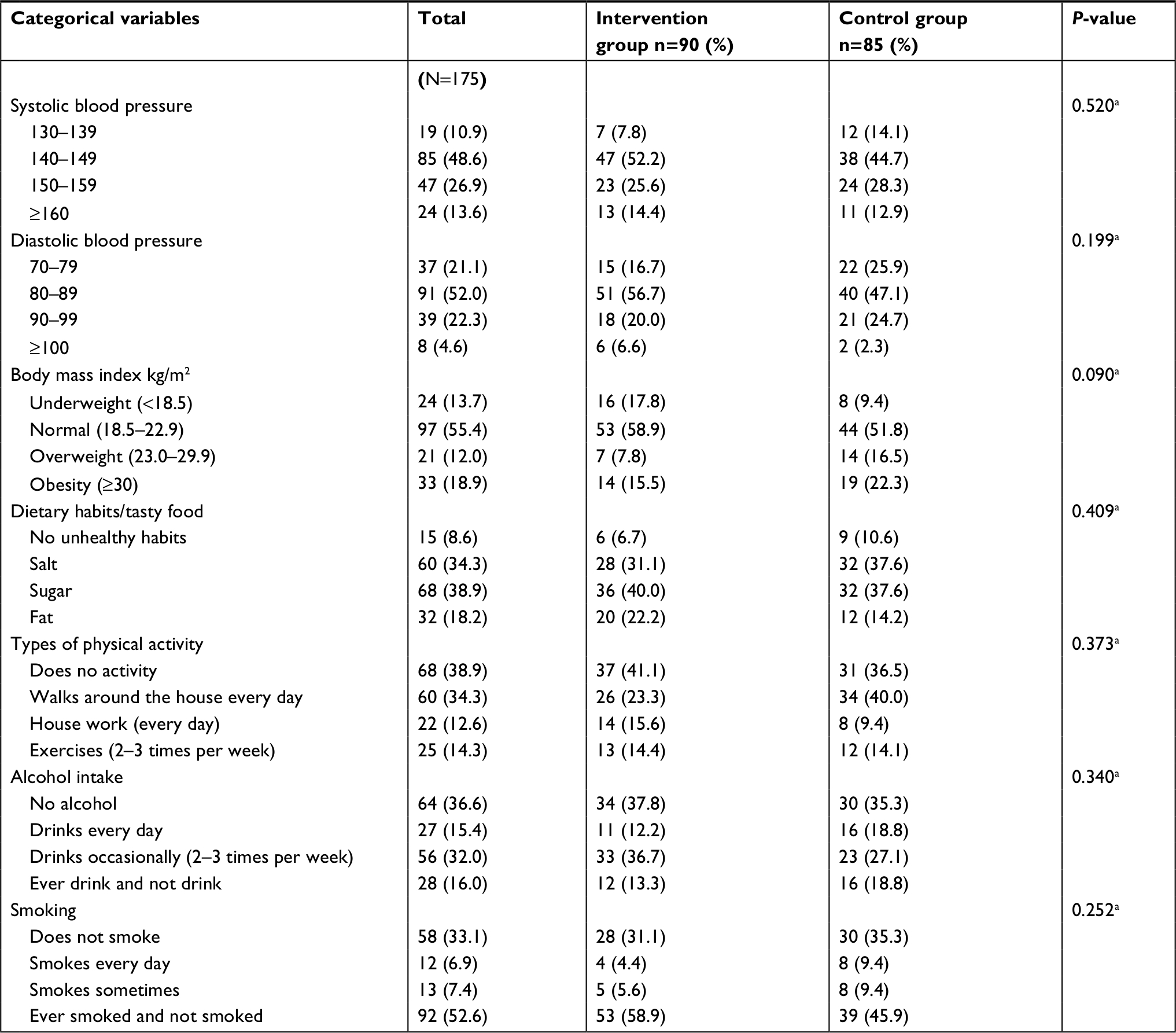 | Table 3 Comparison of the participants’ categorical variables between the intervention and control groups (N=175) Notes: aP-values were calculated using Fisher’s exact test. bStatistical significance P<0.05. |
Table 4 illustrates the changes in mean scores from baseline to follow-up between the intervention and control groups. No significant differences of mean scores at baseline were found for perceived severity, self-efficacy, and preventive behaviors between the intervention and control groups (P>0.05). After the postintervention, it was found that the mean scores of the intervention group had increased more than the control group (31.74, 33.01, and 23.63, respectively). After 3-month follow-up, the scores had slightly increased (32.88, 33.04, and 24.49, respectively; P<0.001). In terms of SBP changes, there were no significant differences between the intervention and control groups preinvention (P>0.05). However, postintervention and at 3-month follow-up, SBP statistical scores had significantly decreased (139.87 and 138.32, respectively; P <0.001). In terms of DBP changes, there were no significant differences between the intervention and control groups preinvention (P>0.05). However, postintervention and at 3-month follow-up, DBP statistical scores had significantly decreased (79.63 and 80.60, respectively; P <0.001) (Table 5).
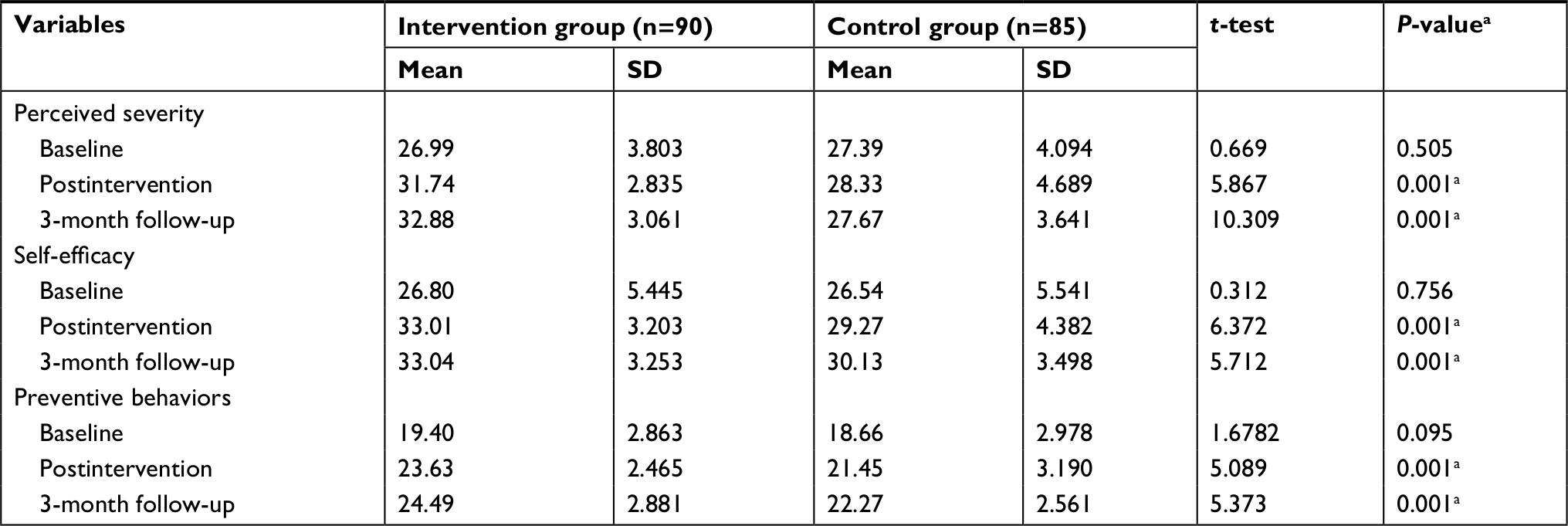 | Table 4 Comparison of the mean scores of perceived severity, self-efficacy, and preventative behaviors between the intervention and control groups at baseline, postintervention, and at 3-month follow-up (N=175) Note: aMann−Whitney U-test (analyzed by two-tailed test with significance at P=0.05). |
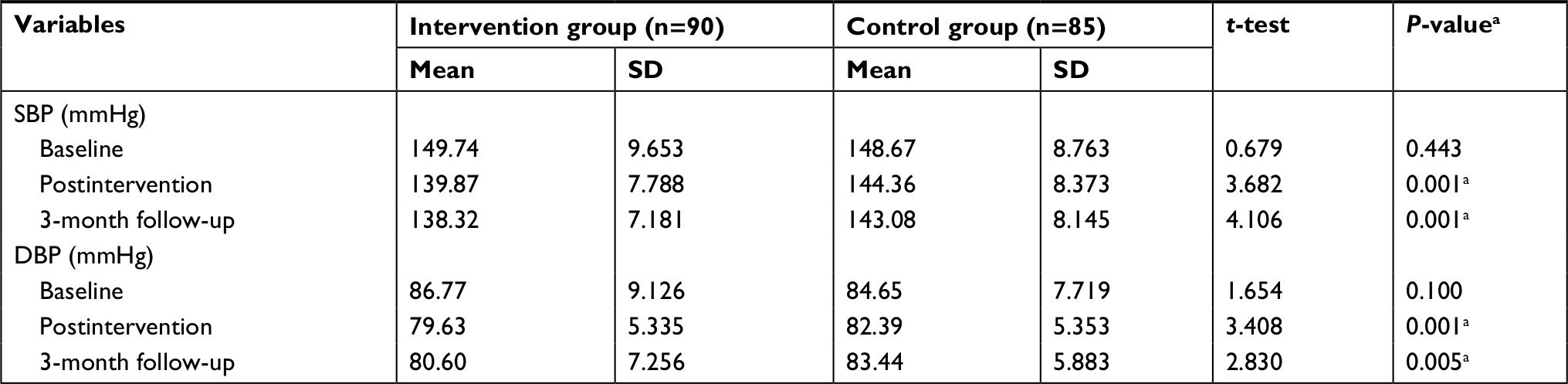 | Table 5 Comparison of SBP and DBP changes at baseline, postintervention, and at 3-month follow-up between the intervention and control groups (N=175) Note: aIndependent t-test (analyzed by two-tailed test with significance at P=0.05). Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure. |
Repeated measures ANOVA was used to analyze the differences of perceived severity, self-efficacy, and preventive behaviors between the intervention and control groups postintervention and at 3-month follow-up, and it was noted that there was a statistically significant difference (P=0.001). There were statistically significant differences in measurements between subjects (P<0.001). Within-subject testing showed that the DASH program intervention had an effect on changes in mean perceived severity, self-efficacy, and preventive behaviors scores over the three time points (baseline, postintervention, and 3-month follow-up) with statistical significance (P=0.002, P=0.005, and P=0.002, respectively) (Table 6).
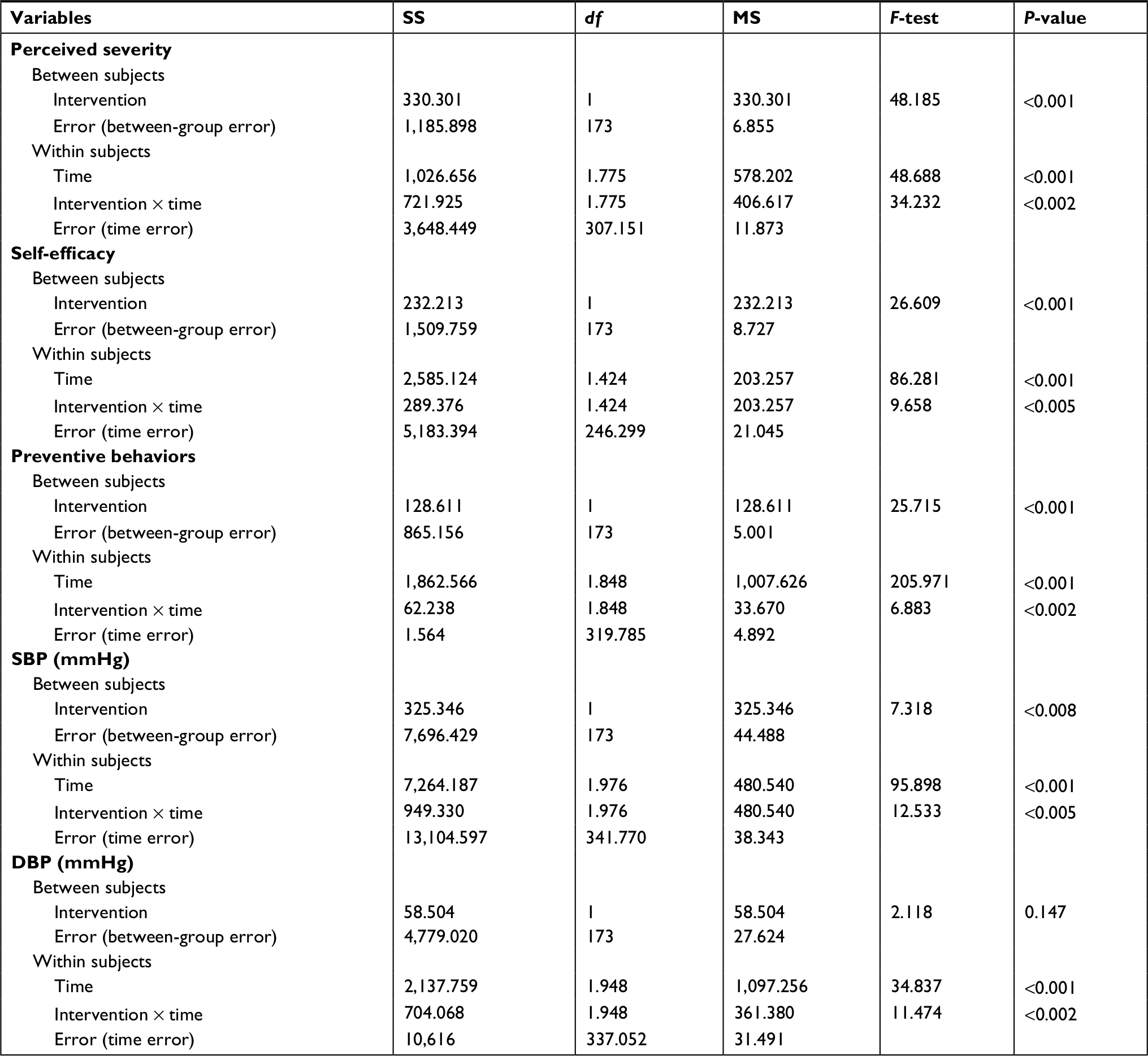 | Table 6 Repeated measures ANOVA of perceived severity, self-efficacy, and preventive behaviors between the intervention and control groups (N=175) Note: Statistical significance P<0.05. Abbreviations: df, degrees of freedom; MS, mean squares; SS, sum of squares. |
Repeated measures ANOVA was used to analyze the differences of SBP and DBP between the intervention and control groups postintervention and at 3-month follow-up, and it was noted that there was a statistically significant difference (P=0.008). There were statistically significant differences between measurements between subjects (P<0.001). Within-subject testing showed that the DASH program intervention had an effect on changes in mean SBP and DBP scores over the three time points with statistical significance (P=0.002 and P=0.005, respectively).
Discussion
The modified dietary behavior guidelines of the DASH program with self-efficacy for reducing the risk of hypertension were used to help elderly people increase awareness of daily dietary habits.12 After elderly people participated in the program’s activities, it was found that perceived severity, self-efficacy, and preventive behaviors among the elderly had increased, and SBP and DBP had decreased. A video recorded of real people who had experienced hypertension and health complications was shown to elderly people during the education activities. Elderly people could see the impact of health complications related to hypertension, such as coronary disease, stroke, kidney disease, and diabetes. This activity increased awareness of perceived severity of hypertension. The session also explained about dietary intake, focusing on local food. These activities were similar to those in previous studies.7,16 When the DASH diet was modified to use local northern food, it helped elderly people with hypertension in everyday life as they were more confident in choosing food with lower sodium levels and in evaluating food labels before buying. The elderly people had more self-efficacy and self-regulation regarding what to eat and what not to eat. They had to record their meals daily and evaluated their food intake within 12 weeks of study. The results showed that the elderly people with hypertension used less sodium in food, which is consistent with other studies.7,11 It was found that the program was effective in changing behaviors among elderly people with hypertension as well as decreasing BP and helping prevent health complications.
After intervention with preventive behaviors toward hypertension, it was found that the elderly in the intervention group had mean dietary behaviors scores for DASH higher than before the intervention and the control group (P<0.001). This explains how the outcome expectation is connected to self-efficacy.12 Elderly people ate food in a limited amount for each meal, with a focus on local food that was available within the community, such as homegrown vegetables. They reduced the amount of sodium intake (1,500 mg/day or ⅓ teaspoon), ate more fruit and vegetables, and low-fat products, such as whole grains, poultry, fish, and nuts. The elderly were encouraged to do home exercise such as watering plants, house work, and walking around their homes for ≥30 minutes to get their bodies moving. After being contacted by phone, they were asked about their everyday life and daily meals and were motivated to do activities from the program. As a result, they began to have more confidence about their daily activities and became less less reliant on their family members. This is consistent with previous studies of the DASH diet, which emphasized eating fruit, vegetables, low-fat dairy products, whole grains, poultry, fish, and nuts, and reducing the consumption of fat, red meats, sweets, and sugar-containing beverages as this led to significant hypertension control in people with stage 1 hypertension.7,18
In terms of controlling BP (SBP and DBP) postintervention and at 3-month follow-up, it was found that the elderly in the intervention group had decreased their SBP and DBP after the intervention and that this continually decreased after the follow-up (P<0.001). In the study by Badura,12 which applied self-regulation and self-efficacy elderly people were encouraged to self-perform, such as record their daily meals, reduce salty and high-fat food, and exercise regularly. This study is consistent with previous studies that also showed that the elderly are able to change their behaviors through practice.7,16 Moreover, the program had lowered BP and reduced plasma triglyceride and very LDL concentrations without increasing LDL cholesterol.18 This is consistent with our survey, which found that lycopene, which is found in red-colored fruits and vegetables, including tomatoes, watermelon, papaya, red grapefruits, and guava, may improve vascular function and contribute to the primary and secondary prevention of cardiovascular disorders.19
The study by Golbidi and Laher was similar to this study as it showed that behavior modification by exercising or doing household activities (watering plants, walking around the house, or house work) at least 3–5 times per week may improve health, strengthen the body, and lower BP.21
During 3-month follow-up, it was found that home visits and phone follow-up helped increase motivation among the elderly participants in terms of choosing food to eat and buying food with less sugar and salt, which is consistent with previous studies.7,11 It was found that elderly participants in the intervention group reduced the use of sodium in food and ate more vegetables (45%), and lowered their BP back to normal (23%). This is similar to other studies where elderly people increased self-activity, such as exercising for at least 150 minutes per week, took medicine on time, and controlled their BP.9,22 By providing a program that emphasized how group activity can increase elderly people’s motivation and offered encouragement in terms of changing behaviors such as exercising regularly, choosing food reasonably, and relaxing, SBP was reduced among elderly people with hypertension to 8 mmHg and helped them learn more about the disease and health complications.
Limitations and recommendations
There were several limitations in this study. First, the study was conducted in two rural areas of Phayao in Northern Thailand; therefore, the results may not be generalizable in other areas. Second, the study was conducted among elderly people with no caregiver or family member involved, so by themselves they may forget to record their meal information regularly and it would be difficult to track every meal. However, the research team was sent to visit their homes regularly to follow-up. Third, the main focus of this study was to control and maintain BP among elderly people; therefore, future study of changes in BMI for a longer study time and with the involvement of social support and family members during follow-up should be considered.
Conclusion
The dietary behavior modification guidelines of the DASH program with self-efficacy have increased awareness of the severity and complications of hypertension among elderly people. It encourages elderly people to change their behaviors, such as reducing the amount of sodium used in cooking, avoiding fatty food, exercising regularly, and avoiding alcoholic beverages and cigarette smoking. Further, it helps improve their self-management, which results in the lowering of BP levels. Therefore, the program could be applied in the prevention of other chronic diseases, and it should be suitable within a community context and lifestyle.
Acknowledgments
This study was financially supported by a grant from the University of Phayao (grant number RD61058). The authors also express their deepest gratitude to all participants for their contributions to the study.
Disclosure
The authors report no conflicts of interest in this work.
References
World Hypertension League. World Hypertension Day 2018; 2018. Available from: http://www.whleague.org/index.php/features/world-hypertension-day. Accessed March 10, 2018. | ||
Information and Communication Technology Center, Ministry of Public Health (Thailand). Annual Reporting Group: Non-Communicable Disease; 2018. Available from: https://hdcservice.moph.go.th/hdc/reports/report_kpi.php?flag_kpi_level=9&flag_kpi_year=2018&source=pformated/format1.php&id=e9fb648fe9f1858878714a410222eef1. Accessed March 20, 2018. Thai. | ||
Bureau of Non Communicable Disease, Ministry of Public Health (Thailand). [Annual reported number and rate of deaths from hypertension: 2015–2016]; 2017;13–15. Available from: http://thaincd.com/document/file/download/paper-manual/Annual-report-2015.pdf. Accessed March 20, 2018. Thai. | ||
Bureau of Non Communicable Disease, Ministry of Public Health (Thailand). [Annual reported number and rate of deaths from hypertension: 2015–2016]; 2017;13–15. Available from: http://thaincd.com/document/file/download/paper-manual/Annual-report-2015.pdf. Accessed March20, 2018. Thai. | ||
Phayao Provincial Health Office. [Non-communicable diseases data]; 2016. Available from: http://203.209.96.247/chronic/rep_htscreen_r1.php. Accessed April 20, 2018. Thai. | ||
Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension; 2013. Available from: http://www.ash-us.org/documents/ash_ish-guidelines_2013.pdf. Accessed April 20, 2018. | ||
Moonsarnand S, Sumpowthong K. Effects of dietary behavior modification program guideline of the DASH with self-efficacy theory and social support on reducing the risk of hypertension among pre-hypertensive patients. Public Health J Burapha Univ. 2016;11(1):87–98. | ||
Bazzano LA, Green T, Harrison TN, Reynolds K. Dietary approaches to prevent hypertension. Curr Hypertens Rep. 2013;15(6):694–702. | ||
Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. | ||
US Department of Health and Human Services; National Institutes of Health. National Heart, Lung and Blood Institute. The DASH Eating Plan. 2006:1–27. Available from: https://www.nhlbi.nih.gov/health-topics/dash-eating-plan. Accessed April 20, 2018. | ||
Kwanperch S, Pavadhgul P, Pradipasen M. The effect of a nutrition promotion program on dietary consumption behaviors for blood pressure control in patients with primary hypertension at Denchai Crown Prince Hospital, Phrae Province. J Public Health Special Issue. 2011:9–20. | ||
Badura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs (NJ): Prentice-Hall Inc.; 1986. | ||
Thai Hypertension Society. [Thai Guidelines on the Treatment of Hypertension]; 2015. Available from: http://www.thaihypertension.org/files/GL%20HT%202015.pdf. Accessed June 20, 2018. Thai. | ||
Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dial Transplant. 2010;25(5):1388–1393. | ||
Kunnasut P. Statistics for the Behavioral Sciences Research. Bangkok: Thai Wattana Print; 1999. | ||
Harnden KS, Frayn KN, Hodson L. Dietary approaches to stop hypertension (DASH) diet: applicability and acceptability to a UK population. J Hum Nutr Diet. 2010;23(1):3−10. | ||
Trakultip P, Vatanasomboon P, Satheannoppakao W. Effect of four-step empowerment program on DASH-diet consumption among hypertensive elderly in the Banthatong Elderly Club, Pisanuloke Province. J Public Health Nursing. 2016;30(1):87–102. | ||
Conlin PR, Chow D, Miller ER 3rd, et al. The effect of dietary patterns on blood pressure control in hypertensive patients: results from the Dietary Approaches to Stop Hypertension (DASH) trial. Am J Hypertens. 2000;13(9):949–955. | ||
Zhu X, Wong FKY, Wu CLH. Development and evaluation of a nurse-led hypertension management model: a randomized controlled trial. Int J Nurs Stud. 2018;77:171–178. | ||
Mozos I, Stoian D, Caraba A, Malainer C, Horbańczuk JO, Atanasov AG. Lycopene and vascular health. Front Pharmacol. 2018;9:521. | ||
Golbidi S, Laher I. Exercise and the cardiovascular system. Cardiol Res Pract. 2012;2012:210852. | ||
Figar S, Galarza P. Effect of education on blood pressure control in elderly persons. Am J Hypertens. 2006;19:737–743. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.