Back to Journals » Journal of Pain Research » Volume 12
The effect of spinal cord stimulation on pain medication reduction in intractable spine and limb pain: a systematic review of randomized controlled trials and meta-analysis
Authors Pollard EM, Lamer TJ ![]() , Moeschler SM
, Moeschler SM ![]() , Gazelka HM
, Gazelka HM ![]() , Hooten WM
, Hooten WM ![]() , Bendel MA
, Bendel MA ![]() , Warner NS, Murad MH
, Warner NS, Murad MH ![]()
Received 6 September 2018
Accepted for publication 27 February 2019
Published 30 April 2019 Volume 2019:12 Pages 1311—1324
DOI https://doi.org/10.2147/JPR.S186662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Katherine Hanlon
E Morgan Pollard,1 Tim J Lamer,2 Susan M Moeschler,3 Halena M Gazelka,3 W Michael Hooten,3 Markus A Bendel,3 Nafisseh S Warner,3 M Hassan Murad4
1Division of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN 55905, USA; 2Division of Pain Medicine, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN 55905, USA; 3Division of Pain Medicine, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA; 4Preventive, Occupational, and Aerospace Medicine, Center for the Science of Health Care Delivery, Mayo Clinic, Rochester, MN, USA
Objective: To synthesize the evidence regarding the effect of spinal cord stimulation (SCS) on opioid and pain medication reduction in patients with intractable spine or limb pain.
Methods: A comprehensive literature search was conducted to identify RCTs of patients with chronic back and/or limb pain of greater than one year duration. Only comparative studies were included (ie, conventional SCS vs medical therapy, conventional SCS vs high-frequency SCS) and were required to have a minimum follow-up period of 3 months. Random effect meta-an alysis was used to compare the three interventions. Results were expressed as odds ratio (OR) or weighted mean difference (WMD) with 95% confidence intervals (CI).
Results: We identified five trials enrolling 489 patients. Three of the trials reported the results as a number of patients who were able to reduce or eliminate opioid consumption in the SCS vs medical therapy group. The odds of reducing opioid consumption were significantly increased in the SCS group compared to medical therapy (OR 8.60, CI {1.93–38.30}). Two of the trials reported the results as mean medication dose reduction as measured by the Medication Quantification Scale (MQS) in the SCS group vs medical therapy group. MQS score significantly decreased in the SCS group and not in the medical group (WMD –1.97, 95% CI {–3.67, –0.27}). One trial reported a number of patients in high-frequency SCS who were able to reduce opioids vs number of patients in conventional SCS group who were able to reduce opioids. Thirty-four percent of the patients in the high-frequency group and 26% of the patients in the conventional SCS group were able to reduce opioid consumption; however, there was not a significant difference between groups (OR 1.43, 95% CI {0.74, 2.78}). This trial also quantified the opioid reduction in morphine equivalent dosage (MED). In the high-frequency SCS group, average MED decreased by 24.8 mg vs average MED decrease of 7.3 mg in the conventional SCS group. Again, the difference between groups did not reach statistical significance (–17.50, CI {–66.27, 31.27}).
Conclusions: In patients with intractable spine/limb pain, SCS was associated with increased odds of reducing pain medication consumption. However, results should be treated with caution as available data were limited, and clinical significance of these findings requires further study.
Keywords: spinal cord stimulation, chronic back pain, painful diabetic neuropathy, chronic limb pain, high-frequency spinal stimulations, opioids, pain medications
Introduction
The treatment of chronic non-cancer pain with opioid medications has increased dramatically.1 In the late 1990s, the Joint Commission on Accreditation of Healthcare Organizations instituted pain as the fifth vital sign.2 At the time, it was a commonly held belief that there was no ceiling on the dose of opioid medications required to treat pain. Beginning in the mid-1990s, opioid-related morbidity and mortality increased as the prevalence of opioid therapy for chronic non-cancer pain increased.3 Since the mid-1990s, there have been over 100,000 opioid-related deaths in the United States.3 From 1999 to 2010, the number of opioid deaths increased each year.4 A Cochrane review concluded there is some evidence of very low to moderate quality for short-term efficacy of opioids to treat chronic low back pain, but no difference between opioids and non-steroidal anti-inflammatory drugs or antidepressants. The review ultimately advises that the initiation of long-term opioid use be done with extreme caution.1 Given the high risk and questionable benefit of chronic opioid therapy for chronic pain, alternative pain management therapies are desirable.
Spinal cord stimulation (SCS) has been used as a therapy for chronic pain for over 40 years.5 The Food and Drug Administration in the United States has approved SCS for chronic pain of the trunk and limbs. The most common indications for SCS include complex regional pain syndrome (CRPS), failed back surgery syndrome (FBSS), and intractable angina pectoris.6 Over the past 20 years the number of spinal cord stimulators implanted has greatly increased; from 1997 to 2006 there was a 159% increase in spinal cord stimulator implants in the Medicare population alone.7 Studies have demonstrated symptomatic improvement in patients with SCS. The PROCESS trial demonstrated the health-related quality of life increased in patients with FBSS who had spinal cord stimulators.8 CRPS patients who undergo spinal cord stimulator implant in addition to physical therapy have significantly less pain than patients enrolled in physical therapy alone.9 However, the evidence comparing the effect of SCS on opioid and pain medication reduction in chronic pain patients has not been well established. We conducted a systematic review and meta-analysis to synthesize the evidence about the effect of SCS on opioid and pain medication consumption.
Methods
The reporting of this systematic review follows the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Study eligibility
We limited the inclusion criteria to RCTs that enrolled patients with chronic and intractable back and/or limb pain of greater than one year duration. We used the definition of intractable or refractory pain as proposed by Deer et al: “Pain is defined as refractory when 1) multiple evidence-based biomedical therapies used in clinically appropriate and acceptable fashion have failed to reach treatment goals that may include adequate pain reduction and/or improvement in daily functioning or have resulted in intolerable adverse effects, and when 2) psychiatric disorders and psychosocial factors that could influence pain outcomes have been assessed and appropriately addressed”.10 Studies had to be comparative: comparing SCS to medical treatment or comparing one method of SCS to another method of SCS. The studies were required to have a minimum patient follow-up period of 3 months.
Literature search
A comprehensive literature search was conducted by a reference librarian. The principal investigator provided input on search terms. The search included the electronic databases MEDLINE, Embase, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, CINAHL, and Scopus, using various combinations of controlled vocabulary supplemented with keywords and key authors to search for studies of spinal stimulation, SCS, dorsal root ganglion stimulation, and neurostimulation. The detailed search strategy is in the Supplementary materials Table S1.
Reviewers worked independently to identify original studies eligible for further review by screening abstracts and titles in duplicates method. If a study was determined to be relevant, the full-text manuscript was obtained and reviewed for further assessment. Any inclusion or exclusion disagreements were discussed and reconciled by the senior investigators. Data sources, including citing articles and relevant systematic reviews, were searched manually for possible additional studies, and duplicates were excluded. Our literature search encompassed January 1, 1995– December 31, 2017. Our search included all languages. Figure 1 delineates further details of our search.
Data extraction and outcomes assessment
Two reviewers independently extracted data from each study, including patient demographics, baseline characteristics, study design variables, sample size, description of interventions, and outcome measures. The outcome measure of interest in this study was pain medication reduction. Pain medication outcomes were of two types in all of the manuscripts reviewed: 1) A binary outcome of achieving a reduction or elimination in opioids or 2) Reduction in pain medication as measured by the Medication Quantification Scale (MQS) or morphine equivalent dosing (MED).11
The risk of bias was assessed using the Cochrane Collaboration’s Risk of Bias tool.12 This tool assesses the risk of bias attributed to the method of randomization, allocation concealment, blinding of patients and all research personnel, baseline imbalance, and inclusion of all study subjects in primary and secondary data analyses consistent with intent-to-treat principles.
Data and statistical analysis
From each trial, we extracted a 2×2 table for binary outcomes and the mean, sample size and standard deviation for continuous outcomes. The effect size was pooled across trials using a random effects model and heterogeneity was expressed using the I squared statistic.13 Results were expressed as odds ratio (OR) or weighted mean difference (WMD) with 95% confidence intervals (CIs). Statistical analysis was performed using Stata 15 software (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC).
Results
Literature search
The initial search resulted in 1,080 references. The first stage of article selection removed 1,033 references. There were many reasons for exclusion, the most common were: trials were not RCTs, trials did not study SCS, or the trial follow-up period was too short. Eventually, 12 trials reported in a total of 17 manuscripts were included. Three of the trials had two manuscripts and one had three, reporting outcomes for multiple follow-up periods. The selection process is shown in Figure 1. These 12 trials are reported in a separate paper examining pain outcomes.14–16,18–26 The baseline characteristics of these 12 trials are included in Table 1. A total of five of these trials reported outcomes of opioid or pain medication reduction. It was a secondary outcome in all trials (pain relief was the primary outcome). Follow-up ranged from 6 months to 2 years. The baseline characteristics of the included studies are shown in Table 2, and the quality assessments of the studies are shown in Table 3.
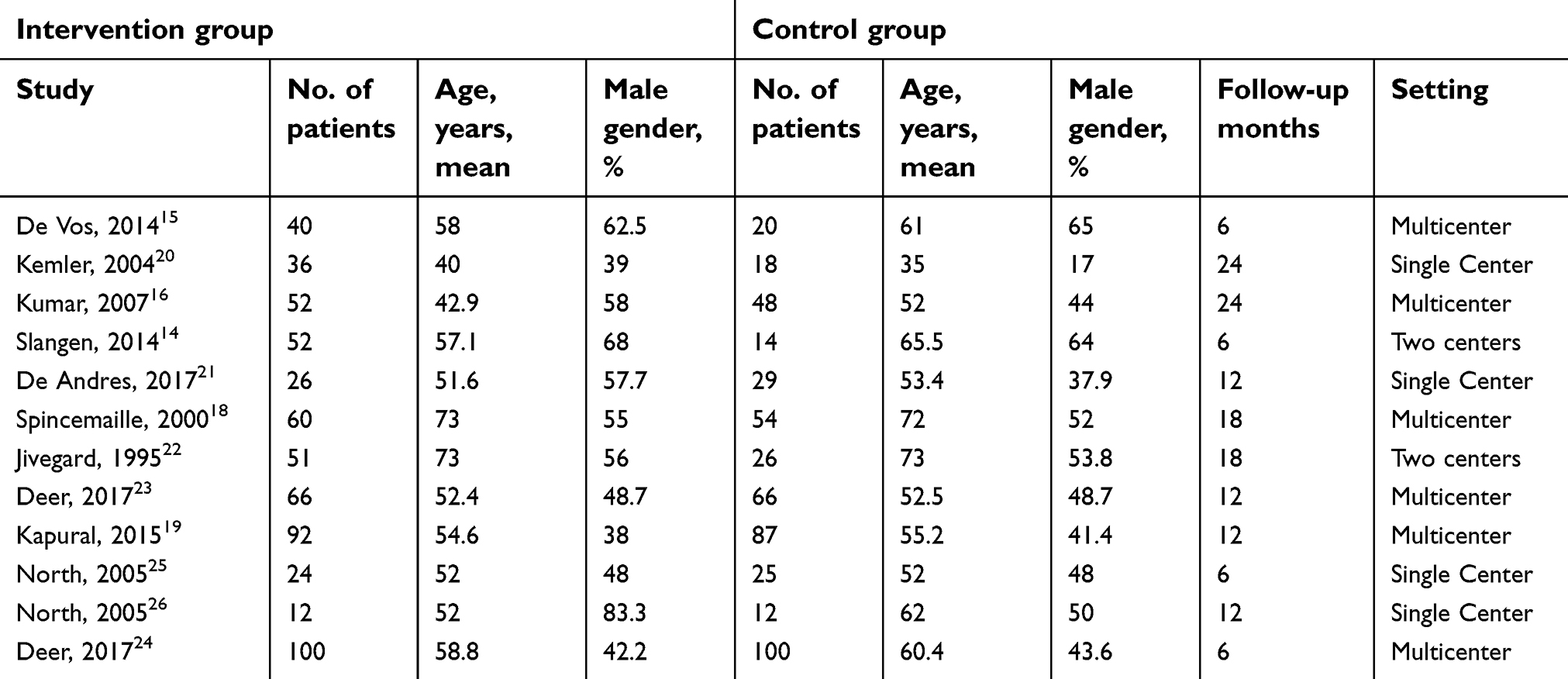 | Table 1 Baseline characteristics of studies, pain outcomes |
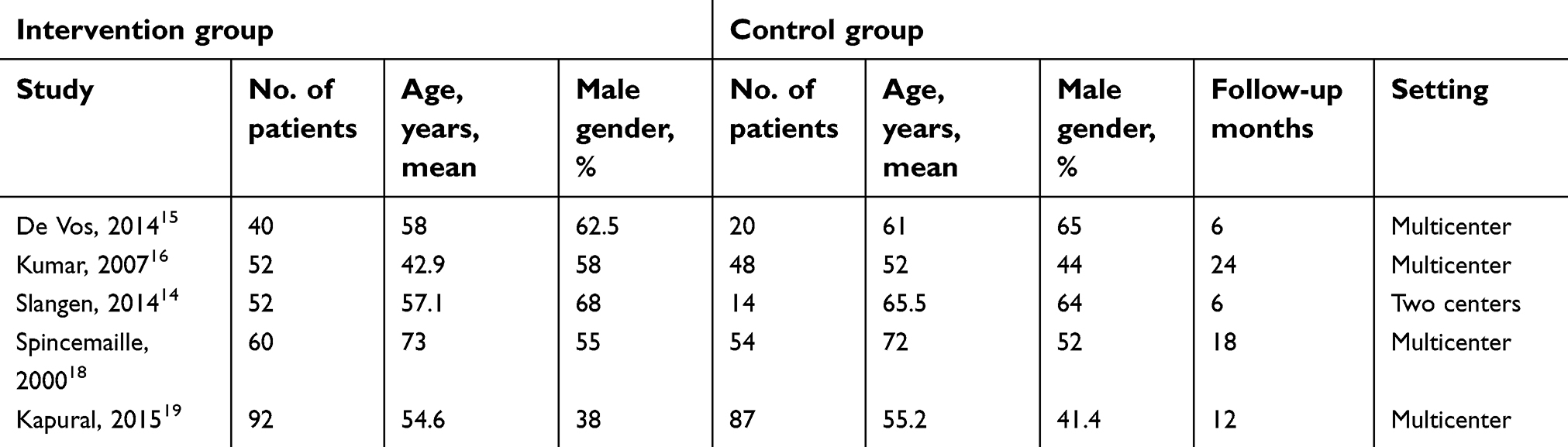 | Table 2 Baseline characteristics of included studies |
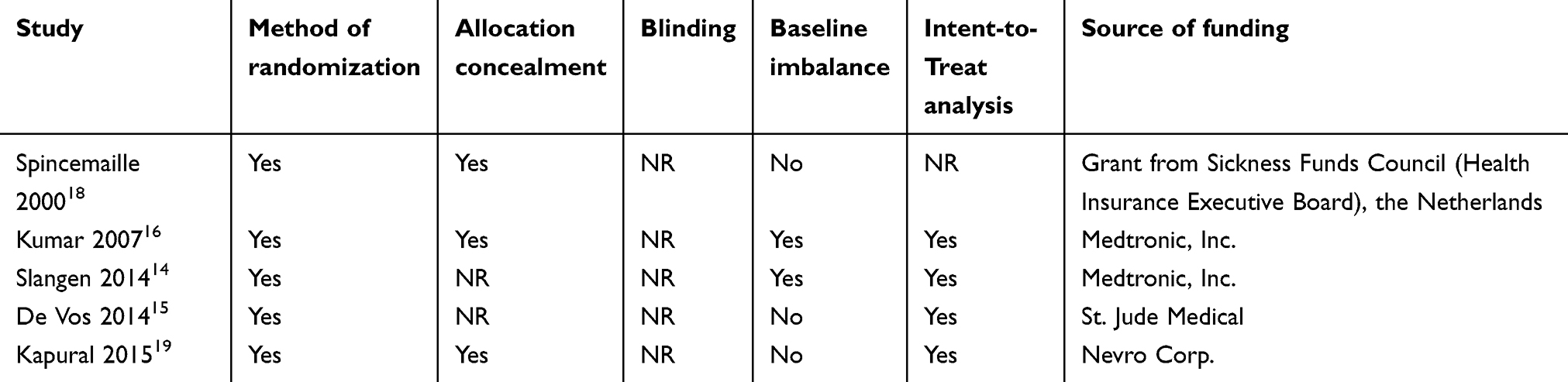 | Table 3 Quality assessment and risk of bias |
 | Figure 1 PRISMA Flow diagram. |
Risk of bias
Although the method of randomization was described in all trials, allocation concealment was reported in two of the five studies. None of the five trials blinded subjects or research personnel to group allocation. All five trials included an intent-to-treat analysis. Four of these trials were funded by companies that manufactured the neurostimulation device(s). One trial was funded by government or private research foundation. Overall, the risk of bias across all the trials for the outcome of opioid reduction was considered to be moderate.
Conventional SCS compared to medical therapy: number of patients decreasing pain medications
Three of the trials, Slangen, de Vos, and Kumar reported the results as a binary outcome: number of patients who were able to reduce or cease opioid consumption in the SCS group vs medical therapy group.
The Slangen trial randomized 36 patients with painful diabetic peripheral neuropathy in a 2:1 ratio to intervention (SCS) vs control (medical therapy).14 At a follow-up of 6 months, 7 of 22 in the SCS group were able to reduce opioid use while none of the 14 in the medical therapy group reduced opioids. The difference between groups did reach statistical significance (OR 20.41, CI {1.08, 385.57})
The de Vos trial also included patients with painful diabetic peripheral neuropathy.15 Sixty patients were randomized in a 2:1 randomization to either SCS or medical therapy. At baseline, 18 of 40 patients randomized to SCS used opioids and 11 of 20 patients randomized to medical therapy used opioids. 6 months after intervention, 3 of the 18 SCS patients ceased opioids vs 0 of the medical therapy patients. The difference between groups did not reach statistical significance (OR 2.83, CI {0.19, 77.76}).
The Kumar trial is a study of 100 patients with FBSS randomized 1:1 to intervention (SCS) or control (medical therapy).16 This trial also demonstrated a trend toward greater odds of reducing opioids in the SCS group as compared to the medical therapy group. Nine of 50 patients in the SCS group ceased opioids vs 1 of 44 patients in the medical therapy group, but this did not reach statistical significance (OR 8.19, CI {0.98, 68.37}). This study also recorded average MED at 6 months based on survey data that included ranges, so patients were categorized by either “low” or “high” morphine equivalent scores. No baseline MED data was reported. At 6 months, the medical therapy patients in the “low” group averaged 96.9 MED vs 68.3 MED in the “low” SCS group. Medical therapy patients in the “high” group averaged 125 MED and SCS patients in the “high” group averaged 76.8 MED. Again, the difference between groups did not reach statistical significance. It should be noted that the Kumar trial was extended to 24 months and reported in a separate paper with similar results.17 We used the 6-month Kumar trial data rather than the 24-month data as there was a cross over component after 6 months and 30 medical therapy patients eventually crossed over to spinal stimulation.
As illustrated in Figure 2, when we pooled this data across these three trials using a random effects model, the odds of decreasing or eliminating opioid dose in the SCS group as compared to the medical therapy group did reach statistical significance with a 95% CI (OR 8.60, CI {1.93, 38.30}).
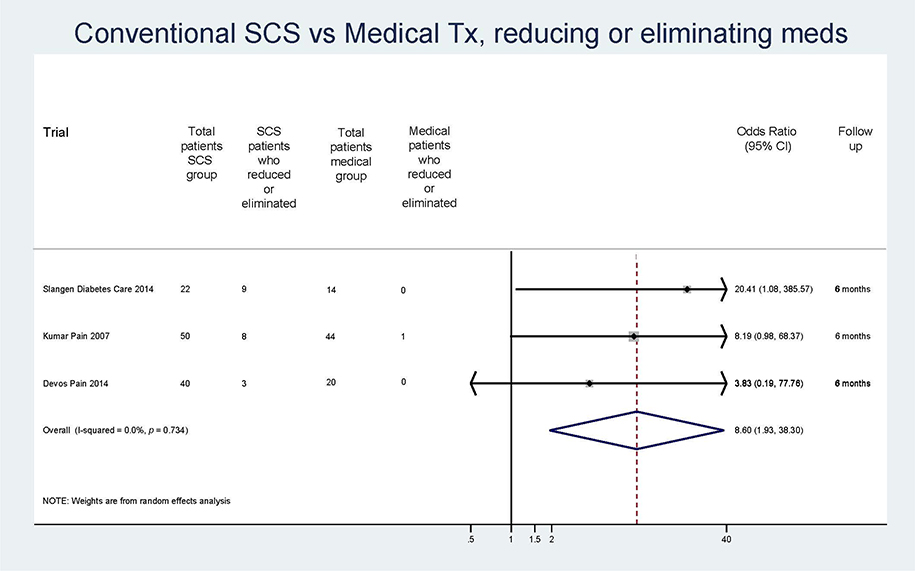 | Figure 2 Number of patients who decreased or eliminated pain medication who received conventional spinal cord stimulation with medical therapy vs medical therapy alone.Abbreviations: SCS, spinal cord stimulation; OR, odds ratio; CI, confidence interval. |
Conventional SCS compared to opioids: MQS reduction
Two trials reported continuous outcomes of mean medication dose reduction as measured by the MQS. Spincemaille randomized 114 patients with critical limb ischemia 1:1 to SCS vs medical therapy.18 MQS was measured before and 18 months after intervention, and the mean difference (MD) of these measures was calculated. The results show a statistically significant decrease in MQS in the SCS patients compared to medical therapy patients (MD –1.90, CI {–3.73, -0.07}).
De Vos randomized 60 patients with painful diabetic peripheral neuropathy in a 2:1 randomization to either SCS or medical therapy. MQS was measured before and 6 months after intervention. A trend toward decreased MQS was demonstrated in the SCS group vs the medical therapy group, but it was not statistically significant (MD –2.40, CI {–6.89, 2.09}).16
Figure 3 reveals the results of applying random effects analysis and calculating WMD for these two trials. The pooled WMD is statistically significant, indicating the SCS group was able to reduce MQS as compared to medical therapy group (WMD –1.97 {–3.67, –0.27}).
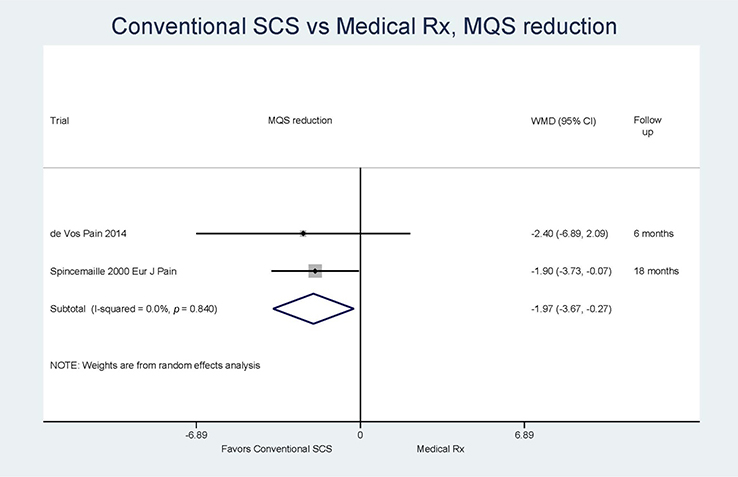 | Figure 3 Medication Quantification Scale (MQS) reduction in patients who received conventional spinal cord stimulation with medical therapy vs medical therapy alone.Abbreviations: SCS, spinal cord stimulation; WMD, weighted mean difference; CI, confidence interval. |
New SCS technology compared to conventional SCS: effect on reducing opioids
The SENZA trial by Kapural enrolled 179 patients with chronic back and/or leg pain and randomized them 1:1 to conventional SCS vs high-frequency SCS.19 The outcome of interest was the number of patients who decreased opioid use after 12 months. There was a trend toward greater reduction in opioid use in the high-frequency SCS group (30/89 patients compared to 21/80 in the conventional SCS group), though these findings were not statistically significant (OR 1.43, CI {0.74, 2.78}). This is graphically represented in Figure 4. Opioid use was quantified as average MED and was recorded at baseline and 12 months after randomization to either high-frequency SCS or conventional SCS. The average MED change was –24.8 mg in the high-frequency SCS group and –7.3 mg in the conventional SCS group. While this result suggests a trend toward greater opioid reduction in high-frequency SCS patients, the difference between groups was not statistically significant (–17.50, {–66.27, 31.27}). This is shown in Figure 5. There was not another randomized control trial comparing high frequency to conventional SCS with the outcome of opioids.
 | Figure 4 Number of patients who reduced opioids in high-frequency spinal cord stimulation group vs number of patients who reduced opioids in conventional spinal cord stimulation group.Abbreviations: HF SCS, high-frequency spinal cord stimulation; OR, odds ratio; CI, confidence interval. |
 | Figure 5 Average morphine equivalent dosing change in patients who received high-frequency spinal cord stimulation vs patients who received conventional spinal cord stimulation.Abbreviation: SCS, high-spinal cord stimulation. |
Adverse events
Adverse event reporting details differed considerably among the different trials. Serious neurological complications were rare with one report of subdural hematoma associated with patient death. Most of the adverse events in the spinal stimulator groups were hardware related to hardware implant site related pain/discomfort and spinal stimulator lead migration being most frequent. Table 4 lists the adverse events reported in each of the trials.
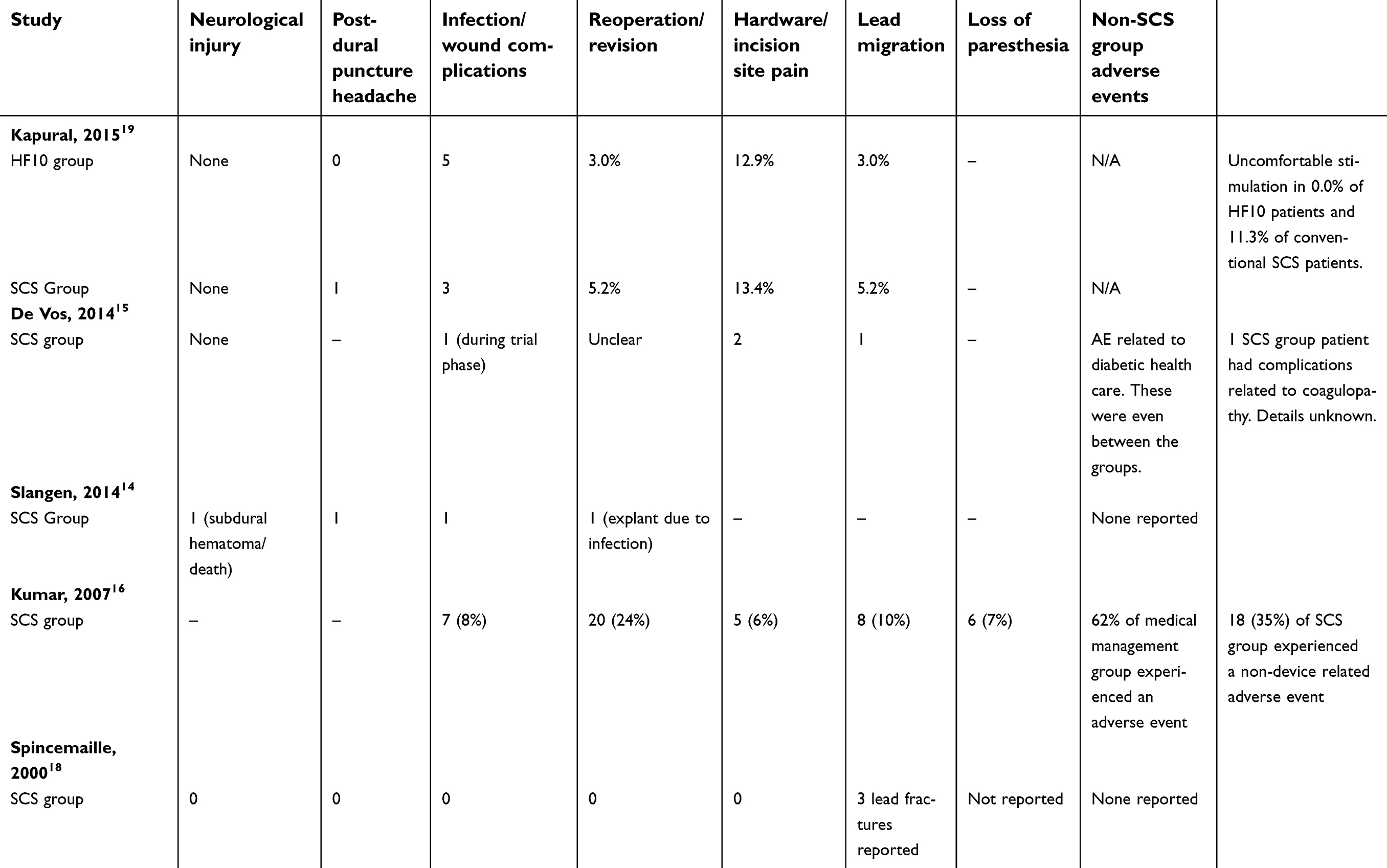 | Table 4 Adverse events in the included studies |
Discussion
We performed a systematic review and meta-analysis of RCTs assessing opioid and pain medication use in patients with intractable back or limb pain treated with conventional SCS vs medical therapy or conventional SCS vs high-frequency SCS. In the four randomized controlled trials that looked at pain medication use, patients receiving conventional SCS experienced greater odds of reducing opioid or pain medication use compared to patients receiving medical therapy alone. Additionally, one trial suggested a trend of decreased opioid therapy after high-frequency SCS as compared to conventional stimulation but this did not reach statistical significance. While the purpose of this systematic review was to determine the effect of SCS on pain medication consumption, we recognize that SCS has many other potential therapeutic effects. Other potential benefits of SCS include pain relief, improved function, and improve quality of life. In the largest SCS RCT published to date by Kapural and colleagues, SCS demonstrated significant improvement in pain, function, and quality of life in addition to reduced opioid consumption.19
The quality of evidence derived from this study is limited by multiple factors which deserve further mention. First, due to the nature of the stimulation intervention, neither the patients nor the investigators were blinded. Secondly, only a small number of RCTs were available for analysis, with each trial limited by small sample sizes. The Kapural study was the largest, with 171 patients successfully implanted after 1:1 randomization to high-frequency SCS or conventional SCS. The smallest trial was the Slangen study, with 22 patients randomized to stimulation and 14 patients randomized to medical management only. The three remaining trials had sample sizes as follows: the de Vos study includes 60 patients randomized 2:1 to medical management with SCS or without SCS, the Kumar study randomized 100 patients 1:1 to medical management with SCS or without SCS, and the Spincemaille study randomized 120 patients 1:1 to medical management with SCS or without SCS.
A third limitation is the heterogeneity of the cohorts studied. The trial populations include patients with painful diabetic neuropathy (de Vos and Slangen), FBSS (Kumar), chronic back or leg pain (Kapural), and painful peripheral vascular disease (Spincemaille). It is difficult to draw definitive conclusions about SCS effect on pain medication use given the confounder of patient populations with widely varying pathology, and likely widely varying baseline pain medication use.
The citations ranged from 2000 to 2015, thus advancing technology may play a role in recent studies. The Kapural study looked at high-frequency SCS compared to conventional SCS, while the other four trials looked at conventional SCS as compared to medication management alone. Kapural was the only trial to explicitly define the stimulation waveform parameters in terms of frequency, pulse width, and amplitude. While none of the other trials included information regarding waveform parameters, given the published dates of those trials, it can be assumed that the SCS parameters in the other four trials were likely to be conventional paresthesia-based low frequency, low pulse width stimulation.
Additionally, the studies have a varied geographic distribution. The de Vos trial included patients from the Netherlands, Denmark, Belgium, and Germany. The Slangen and Spincemaille trials included only patients from the Netherlands. The Kumar trial included patients throughout Europe, Canada, Australia, and Israel. The Kapural trial included American patients only. This broad geographic difference may create challenges when trying to apply the findings of this systematic review to certain populations.
Another important limitation to note is the length of follow-up varied widely between studies. The length of time patients was followed for each study is as follows: 6 months for the de Vos and Slangen studies, 12 months for the Kumar study, 18 months for the Spincemaille study, and 12 months for the Kapural study. Given the chronic disease states of the studied populations, even 18 months is a relatively short amount of time from which to draw conclusions.
Finally, none of the trials looked at opioid or pain medication use as a primary outcome. Two studies (Kumar and Slangen) reported the number of patients able to decrease or cease opioid consumption but did quantify the dosing changes. With no quantitative information, we are left to wonder if the decrease in opioid use was clinically significant for these patients. Two studies (Spincemaille and de Vos) reported mean pain medication dose reduction by utilizing the MQS. While this is an attempt to provide quantitative information, the MQS assesses 22 classes of medications, including opioids, NSAIDs, and paracetamol. It is difficult to determine if a change in MQS is clinically significant. The Kumar trial quantified average morphine equivalent dosage (MED) at 6 months but unfortunately did not provide baseline information. Only one trial quantified opioid doses both before and after the intervention. The Kapural trial recorded MED at baseline and 12 months after intervention. Ultimately, the inconsistency and heterogeneity with which pain medication changes were reported make it difficult to draw conclusions.
There are several studies of the effect of SCS on opioid use that are not included in this meta-analysis because they are non-randomized, but deserve mention. A retrospective case series by Sanders et al of 199 patients recorded oral morphine equivalents (OME) at baseline and 1 year after spinal cord stimulator implantation.27Mean preimplantation OME for this population was 50.19 and 1 year after implantation mean OME decreased to 28.91 (p<0.001). The indications for implantation for the patients in this study were divided into four categories: failed back surgery syndrome and chronic radiculopathy (FBSS), complex regional pain syndrome (CRPS), angina, and other. When pre- and post-implantation OME was examined for each of these 4 categories, there was a statistically significant decrease in the FBSS and CRPS groups.
Al-Kaisy et al, published a prospective study with the objective to explore the effectiveness of 10 kHz high-frequency SCS (HF10 therapy) for chronic low back pain.28 Twenty-one patients with chronic low back pain and no history of prior back surgery were successfully implanted with a permanent high-frequency stimulator. These patients were followed for 12 months after the initiation of HF10 therapy. Average daily opioid intake was recorded for all 21 patients before implantation and at 12 months post-implantation. Average daily opioid intake decreased by 64% over the 12 months, from 112 to 40 morphine milligram equivalent; this reduction in opioid intake was statistically significant (p=0.0833). Three patients completely stopped their use of opioids. Despite the small sample size of only 21 patients, the reduction in opioid use was of great enough magnitude to reach statistical significance.
The North trial is a randomized controlled trial which was included in our group’s systematic review of SCS on pain outcomes and deserves to mention in further detail here.25 Fifty patients with chronic back pain who met standard criteria for spine reoperation were randomized to either SCS or reoperation. Success was based on pain satisfaction and pain relief as reported by the patients; opioid use was also reported. After 2 years, 87% of the patients randomized to SCS had stable or decreased opioid use vs 58% of the patients randomized to reoperation. Opioid use increased by 13% of the SCS group and 42% of the reoperation group. A major confounder is that the patients could cross over to the alternative treatment if the results of the randomized treatment were unsuccessful after 6 months. There was significant crossover effect; 54% of the patients randomized to reoperation crossed over and 21% of the patients randomized to SCS crossed over. While the opioid use data at long-term follow-up suggests SCS promotes decreased opioid use compared to reoperation, the crossover effect makes it difficult to attribute any opioid or pain medication reduction to either intervention.
Additionally, there are several other case series and non-randomized trials looking at pain medication use with SCS. While the patient populations, study designs, and measured outcomes vary widely, they show similar findings and suggest SCS can aid in the reduction of pain medications including opioids.29,30,31
Conclusion
We conducted a systematic review and meta-analysis of changes in opioid and pain medication use following SCS in those with chronic low back and/or limb pain, finding statistically significant decreases in opioid and pain medication use following SCS. However, available data were limited, and the clinical significance of these findings will require further study. Future studies should be randomized control trials with opioid reduction as a primary endpoint in order to allow meaningful comparison of SCS to other pain therapies and apply that information to the broad spectrum of patients with chronic pain. Additionally, quantitative measures of opioid intake, such as morphine milligram equivalents, should be measured so that the clinical significance of any pattern of change of opioid use can be ascertained.
Prior Presentations
The abstract was presented at Midwest Anesthesia Residents’ Conference on April 14, 2018 in Cincinnati, OH. The abstract was accepted for presentation at American Society of Anesthesiology Annual Meeting on October 14 in San Francisco, CA.
Acknowledgments
The authors would like to thank Patricia J Erwin, M.L.S. from Mayo Library System, Mayo Clinic, Rochester MN for her significant contribution with the literature search and abstract and article procurement. Support was provided solely from institutional sources.
Disclosure
Tim J Lamer M.D. was involved in research funded by Boston Scientific and Medtronic. All funds were paid to his institution. The authors report no further conflicts of interest in this work.
References
1. Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC. Opioids compared to placebo or other treatments for chronic low-back pain. Cochrane Database of Systematic Reviews. 2013;(8):
2. Lanser P, Gesell S. Pain management: the fifth vital sign. Healthc Benchmarks. 2001;8(6):68–70.
3. Franklin GM. Opioids for chronic noncancer pain: a position paper of the American Academy of Neurology. Neurology. 2014;83:1277–1284. doi:10.1212/WNL.0000000000000839
4. Jones CM, Mack KA, Paulozzi LJ. Pharmaceutical overdose deaths, United States, 2010. Jam.A. 2013;309:657–659. doi:10.1001/jama.2013.272
5. Shealy CN, Mortimer JT, Reswick JB. Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesth Analg. 1967;46:489–491. doi:10.1213/00000539-196707000-00025
6. Lamer TJ, Deer TR, Hayek SM. Advanced innovations for pain. Mayo Clin Proc. 2016;91:246–258. doi:10.1016/j.mayocp.2015.12.001
7. Kumar K, Caraway DL, Rizvi S, et al. Current challenges in spinal cord stimulation. Neuromodulation. 2014;17:22–35. doi:10.1111/ner.12172
8. Manca A, Kumar K, Taylor RS, et al. Quality of life, resource consumption and costs of spinal cord stimulation versus conventional medical management in neuropathic pain patients with failed back surgery syndrome (PROCESS trial). Eur J Pain. 2008;12:1047–1058. doi:10.1016/j.ejpain.2008.01.014
9. Kemler MA, de Vet HC, Barendse GA, van Den Wildenberg FA, van Kleef M. Effect of spinal cord stimulation for chronic complex regional pain syndrome type I: five-year final follow-up of patients in a randomized controlled trial. J Neurosurg. 2008;108:292–298. doi:10.3171/JNS/2008/108/2/0292
10. Deer TR, Caraway DL, Wallace MS. A definition of refractory pain to help determine suitability for device implantation. Neuromodulation. 2014;17(8):711–715. doi:10.1111/ner.12263
11. Harden RN, Weinland SR, Remble TA, et al. Medication quantification scale version III: update in medication classes and revised detriment weights by survey of American Pain Society Physicians. J Pain. 2005;6:364–371. doi:10.1016/j.jpain.2005.01.350
12. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi:10.1136/bmj.327.7414.557
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188.
14. Slangen R, Schaper NC, Faber CG, et al. Spinal cord stimulation and pain relief in painful diabetic peripheral neuropathy: a prospective two-center randomized controlled trial. Diabetes Care. 2014;37(11):3016–3024. doi:10.2337/dc14-0684
15. De Vos CC, Meier K, Zaalberg PB, et al. Spinal cord stimulation in patients with painful diabetic neuropathy: a multicentre randomized clinical trial. Pain. 2014;155(11):2426–2431. doi:10.1016/j.pain.2014.08.031
16. Kumar K, Taylor RS, Jacques L, et al. Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome. Pain. 2007;132:179–188. doi:10.1016/j.pain.2007.07.028
17. Kumar K, Taylor RS, Jacques L, et al. The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation. Neurosurgery. 2008;63:
18. Spincemaille GH, Klomp HM, Steyerberg EW, Habbema JD. Pain and quality of life in patients with critical limb ischaemia: results of a randomized controlled multicentre study on the effect of spinal cord stimulation. ESES study group. European Journal of Pain. 2000;4(2):173–184. doi:10.1053/eujp.2000.0170
19. Kapural L, Yu C, Doust MW, et al. Novel 10-kHz high-frequency therapy (HF10 therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology. 2015;123(4):851–860. doi:10.1097/ALN.0000000000000774
20. Kemler MA, De Vet HC, Barendse GA, Van Den Wildenberg FA, Van Kleef M. The effect of spinal cord stimulation in patients with chronic reflex sympathetic dystrophy: two years’ follow-up of the randomized controlled trial. Ann Neurol. 2004;55:13–18. doi:10.1002/ana.10996
21. De Andres J, Monsalve-Dolz V, Fabregat-Cid G, et al. Prospective, randomized blind effect-on-outcome study of conventional vs high-frequency spinal cord stimulation in patients with pain and disability due to failed back surgery syndrome. Pain Med. 2017;18:2401–2421. doi:10.1093/pm/pnx241
22. Jivegard LE, Augustinsson LE, Holm J, Risberg B, Ortenwall P. Effects of spinal cord stimulation (SCS) in patients with inoperable severe lower limb ischaemia: a prospective randomised controlled study. Eur J Vasc Endovasc Surg. 1995;9:421–425.
23. Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158:669–681. doi:10.1097/j.pain.0000000000000814
24. Deer T, Slavin KV, Amirdelfan K, et al. Success using neuromodulation with BURST (SUNBURST) study: results from a prospective, randomized controlled trial using a novel burst waveform. Neuromodulation. 2018;21:56–66. doi:10.1111/ner.12698
25. North RB, Kidd DH, Farrokhi F, Piantadosi S. Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial. Neurosurgery. 2005;56(1):98–106.
26. North RB, Kidd DH, Petrucci L, Dorsi MJ. Spinal cord stimulation electrode design: a prospective, randomized, controlled trial comparing percutaneous with laminectomy electrodes: part II-clinical outcomes. Neurosurgery. 2005;57:
27. Sanders RA, Moeschler SM, Gazelka HM, et al. Patient outcomes and spinal cord stimulation: a retrospective case series evaluating patient satisfaction, pain scores, and opioid requirements. Pain Practice. 2016;16(7):899–904. doi:10.1111/papr.12340
28. Al-Kaisy A, Palmisani S, Smith TE, et al. 10 kHz high-frequency spinal cord stimulation for chronic axial low back pain in patients with no history of spinal surgery: a preliminary, prospective, open label and proof-of-concept study. Neuromodulation. 2017;20:63–70. doi:10.1111/ner.12563
29. Gee L, Smith HC, Ghulam-Jelani Z, et al. Spinal cord stimulation for the treatment of chronic pain reduces opioid use and results in superior clinical outcomes when used without opioids. Neurosurgery.
30. Van Buyten JP, Al-Kaisy A, Smet I, Palmisani S, Smith T. High-frequency spinal cord stimulation for the treatment of chronic back pain patients: results of a prospective multicenter european clinical study. Neuromodulation. 2013;16(1):59–65. doi:10.1111/ner.12006
31. Sharan AD, Riley J, Falowski S, et al. Association of opioid usage with spinal cord stimulation outcomes. Pain Medicine. 2018;19(4):699–707. doi:10.1093/pm/pnx262
Supplementary materials
 | Table S1 Search strategy |
Scopus
1 (TITLE-ABS-KEY ((“root ganglion” OR dorsal OR sacral OR caudal OR spinal) W/4 (neurostimulat* OR stimulat* OR neuromodulat* OR electrotherap* OR electric* )
2 TITLE-ABS-KEY (“chronic pain” OR “leg pain” OR neuralgi* OR neuropath* OR backache* OR “back pain” OR crps OR fbss OR “failed back” OR “complex regional pain” OR “reflex sympathetic” )
3 TITLE-ABS-KEY (random*) ) AND PUBYEAR > 1994 320
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.