Back to Journals » Journal of Pain Research » Volume 8
The effect of nonrecurring alcohol administration on pain perception in humans: a systematic review
Authors Horn-Hofmann C, Büscher P, Lautenbacher S ![]() , Wolstein J
, Wolstein J
Received 20 December 2014
Accepted for publication 10 February 2015
Published 23 April 2015 Volume 2015:8 Pages 175—187
DOI https://doi.org/10.2147/JPR.S79618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Micheal Schatman
Claudia Horn-Hofmann,1,2 Patricia Büscher,1 Stefan Lautenbacher,2 Jörg Wolstein1
1Pathosychology, University of Bamberg, Bamberg, Germany; 2Physiological Psychology, University of Bamberg, Bamberg, Germany
Purpose: Alcohol is believed to have pain-dampening effects and is often used as self-medication by persons with pain problems; however, experimental evidence confirming this effect is scarce. We conducted a systematic review of experimental studies on the effects of nonrecurring alcohol administration on pain perception in healthy human subjects and the underlying mechanisms.
Method: Three databases (PubMed, PsycINFO, and Web of Science) were searched for relevant studies using a predefined algorithm. In a next step, irrelevant articles were excluded by screening titles and abstracts. Finally, articles were checked regarding a set of methodological criteria; only publications meeting these criteria were selected for this review. A total of 14 experimental studies were identified.
Results: Overall, most of the studies were able to show a pain-dampening effect of alcohol. However, many of them had methodological shortcomings (eg, lack of placebo control, insufficient blinding, or very small sample sizes). In addition, comparability is limited due to considerable variations in alcohol administration and pain measurement. More importantly, potential mechanisms of action and moderating variables have scarcely been investigated.
Conclusion: Despite the frequent use of alcohol as self-medication by persons with pain problems, there are to date only a few experimental investigations of alcohol effects on pain perceptions. The results of these studies suggest that alcohol does in fact have pain-dampening effects. However, the mechanisms implicated in these effects are still unknown, and experimental research has been limited to pain-free subjects. Future research should provide more knowledge about alcohol effects on pain, especially in chronic pain patients.
Keywords: pain, experimental pain, alcohol
Introduction
According to historical accounts, the pain-dampening properties of alcohol have been known for several thousand years. Its use as an analgesic agent by surgeons and other physicians dates back to ancient times.1
In the more recent scientific literature, there have been several reports on the link between consumption or problematic use of alcohol and pain. People suffering from chronic pain conditions have an increased prevalence of alcohol abuse.2–6 Moreover, in a population of alcoholic patients, 29.1% reported chronic severe pain, compared with rates of approximately 10% in the general population.7 In a sample of individuals above the age of 62 years, problem drinkers reported more severe pain and more disruption of daily activities due to pain.8 Although causal relationships cannot be inferred from these cross-sectional studies, they provide evidence for a link between alcohol consumption and pain processing. This observation is in line with recent neurophysiological models proposing a common neural substrate for chronic pain and alcohol dependence.9,10
In addition, empirical evidence suggests that alcohol is frequently used as self-medication in pain syndromes. In a recent study, about one-quarter of a multiethnic sample with three different pain conditions reported the use of alcohol to alleviate pain.11 This study found that males were more likely to use alcohol as self-medication, which is in accordance with observations reported by other authors.12–14 Other risk factors associated with alcohol consumption for coping with pain were younger age (18–25 years), Caucasian ethnicity, higher education, depression, and the frequency of pain, whereas the authors found no evidence for a role of pain intensity or chronicity. Brennan et al8 reported that the use of alcohol for pain management was more common in problem drinkers and was also associated with global pain severity. Despite the higher occurrence of self-medication in younger adults reported by Riley and King11, Jakobsson et al15 found that alcohol consumption was self-rated as one of the most effective strategies to manage pain, even in a sample of elderly persons.
However, despite this regular use of alcohol as self-medication, it is still unknown which mechanisms of action are implicated in effects of alcohol on pain perception. For example, alcohol effects on pain might be direct (ie, via pharmacological actions of alcohol on neurotransmitter systems) or indirect (eg, via a modulation of affective state). In order to gain a better understanding of the link between pain experience and alcohol use, it is indispensable to know the pain-dampening properties of alcohol in humans. Thus, the objective of this article is to give an overview of what is known about effects of alcohol on pain from experimental studies in humans. For this purpose, we performed a systematic review of the literature on the influences of alcohol on pain perception and any mechanisms of action or moderating variables implicated in these effects.
Method
Retrieval of publications was done in three steps. In a first step, databases were searched for suitable publications using a predefined algorithm; in a second step, titles and abstracts were screened and relevant publications were extracted from the obtained results based on thematic relevance and certain methodological standards; and, finally, in a third step, citations in the selected publications were screened for further relevant studies. Each of these steps is described in more detail in the following paragraphs.
Step 1: database search
Electronic databases PubMed, PsycINFO, and Web of Science were searched for relevant empirical studies within the overall timeframes covered by these databases until July 2012 using the key words “ethanol” or “alcohol combined with analgesia” or “analgesic effect” or “analgetic effect” or “pain perception”. The search was limited to articles published in English. A total of 15,577 studies were retrieved. However, as we were interested in the effects of acute alcohol administration on healthy human subjects in experimental pain paradigms, most of these studies were irrelevant for the purpose of this review. Therefore, we specified our search algorithm by exclusion of certain keywords using the “not” function; specifically, we aimed to exclude 1) animal studies (eg, “rats”, “mice”), 2) surgical interventions (eg, “block”, “surgery”), 3) chronic diseases (eg, “chronic”), and 4) long-term effects of alcohol administration (eg, “withdrawal”). For the complete search query, please see Table 1. With this algorithm, 2,338 studies were identified as potentially suitable for this review.
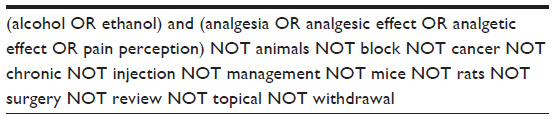 | Table 1 Search query |
Step 2: analysis of search results
The titles of the 2,338 articles were screened manually. Studies with irrelevant titles and abstracts were excluded. The remaining studies were examined in depth and only empirical studies that met the following criteria were included in the review: 1) published in a peer-reviewed journal, 2) alcohol had been administered orally or intravenously, 3) pain had been induced in a laboratory setting, and 4) the dependent variables of acute alcohol effects were measures of pain perception (for a detailed description of these measures, see Table 2). Studies that failed to meet these criteria were discarded. By this means, 13 experimental studies on the acute effects of alcohol on pain perception could be identified.
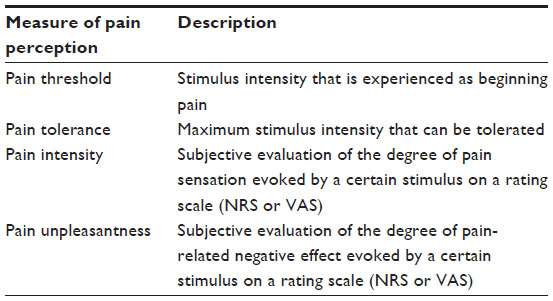 | Table 2 Experimental measures of pain perception |
For historical reasons, it should be mentioned that the first systematic investigations of alcohol effects on pain perception were conducted between 1930 and 1945.16–18 However, these studies did not pass our inclusion criteria, as pain was not induced in a laboratory setting17,18 or alcohol effects on measures of pain perception were not reported,16 and were thus not included in the systematic review.
Step 3: screening of citations
Citations in identified articles were then screened for further relevant studies. If there was a notion in the text itself that a citation could be relevant or the title of a reference appeared to hold an adequate study, this article was screened regarding the inclusion criteria mentioned previously. One of the identified citations met the given criteria. Thus, a total of 14 articles were finally identified. From these articles the following information was retrieved: study design, sample characteristics, manipulation checks, control of confounding variables, method of alcohol administration, method of pain induction, measure of pain perception, and main findings regarding the effect of alcohol on pain perception.
Results
General design of studies
The general design of the studies included in this review, including subject characteristics and experimental manipulations, is summarized in Table 3 and described in the following paragraphs.
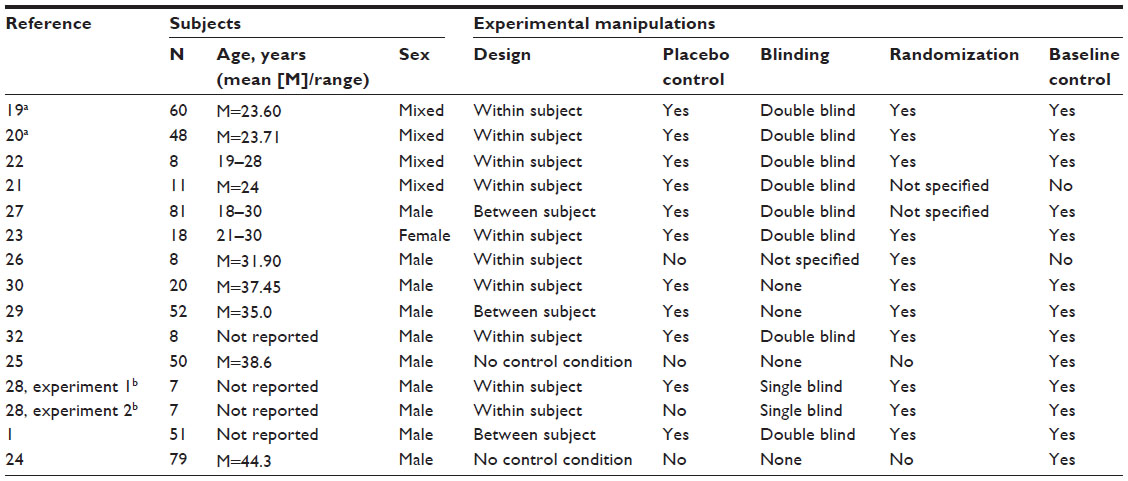 | Table 3 General design of studies |
Subjects
In the selected publications, sample sizes ranged from seven participants up to 81 (see Table 3). Apart from the latest two publications based on the same data with a sample of 48 and 60 subjects, respectively,19,20 studies that used a within-subject effect investigated 20 people at most. In contrast, studies with between-subject conditions tested 51–81 subjects. In terms of sex, eleven of the 14 studies investigated exclusively male subjects. Only three studies used mixed samples,19,21,22 and one study23 was conducted with an all-female sample. So far, only pain-free populations have been investigated. Age of participants (if reported) was between 20 years and 45 years in all investigations.
Experimental manipulations
Two-thirds of the experiments that investigated the effect of alcohol on pain compared with a placebo or another experimental condition by using a within-subject design. Only in three studies was a between-subject design chosen. In the studies by Cutter et al,24,25 alcohol was given to all subjects, so there was no comparison group. Except for two studies,21,26 all investigations were baseline controlled.
Three-quarters of the included studies have been placebo controlled. However, strategies in placebo manipulations differ markedly between studies with regard to design, instructions, and formulations. In one investigation,23 the type of substance administration was not consistent in the experimental conditions, with alcohol being consumed orally and the placebo given intravenously.
In two studies,24,25 alcohol was given to all subjects, so these studies included no control condition with administration of placebo or another active drug. Of the remaining 12 studies, ten were randomized concerning the assignment to the condition (between-subject design) or the sequence of treatments (within-subject design). Only in two studies21,27 could randomization not be inferred for sure. Additionally, in seven of these 12 studies, the application of substances was double blinded. The two experiments conducted by James et al28 used a single-blinded design, another study26 reported no specifications on blinding, and in two studies,29,30 expectations concerning the contents of the beverage were systematically manipulated.
Control of confounding variables and manipulation checks varied considerably across the investigations. Whereas most of the studies (n=10) controlled for food intake before the experimental session, and also most (n=10) assessed blood alcohol concentration (BAC) or breath alcohol concentration (BrAC) at some point during the experiment, other possibly confounding variables like physiological measures (eg, heart rate, skin conductance) were rarely accounted for. Only one study21 obtained blood pressure as a measure of peripheral physiological activation. In addition, manipulation checks regarding alcohol administration (eg, subjective intoxication) were collected in only six of 14 studies (four of them conducted after 1990).
Alcohol administration
An overview of administration characteristics is given in Table 4.
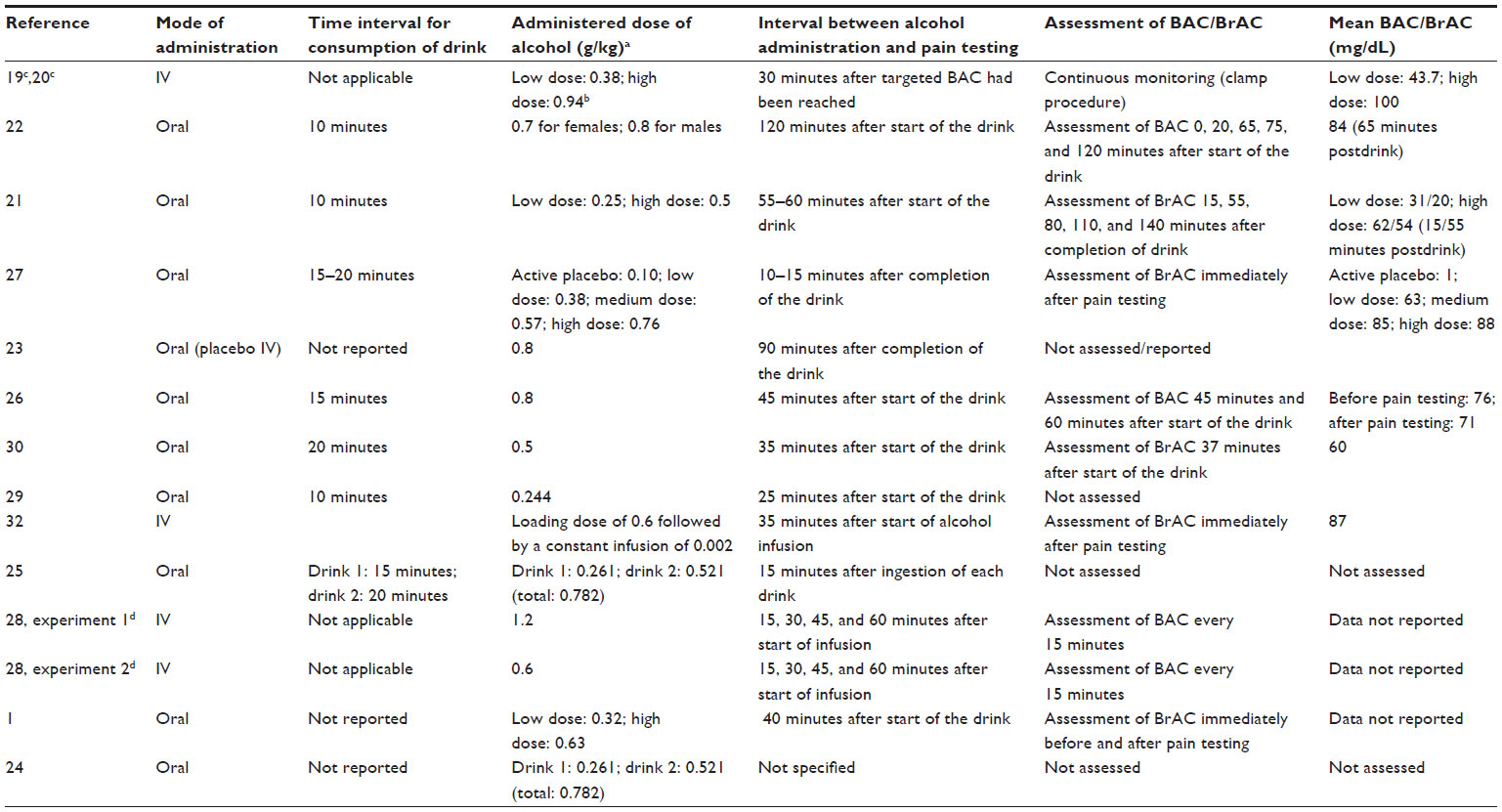 | Table 4 Characteristics of alcohol administration |
Alcohol was administered orally in ten and intravenously in four of the studies. All studies adjusted the dose to the subjects’ body weight. The amount of alcohol administered varied from 0.24 g/kg to 1.2 g/kg body weight. However, dose-dependent effects of alcohol on pain perception have scarcely been investigated systematically, particularly as most of the studies did not assess BAC at regular time intervals. In addition, there were considerable variations in the time interval between alcohol administration and pain testing, ranging from 10 to 110 minutes. As alcohol might exert different effects on pain perception depending on whether BAC is ascending or descending, this should be taken into consideration when comparing effects between studies.
See Table 4 for detailed information on administered doses of alcohol, time span between alcohol administration and pain testing, mode of assessment, and measurements of BAC/BrAC.
Pain induction and pain measures
Methods of pain induction, measures of pain perception, and main results concerning the effect of alcohol on pain perception are presented in Table 5.
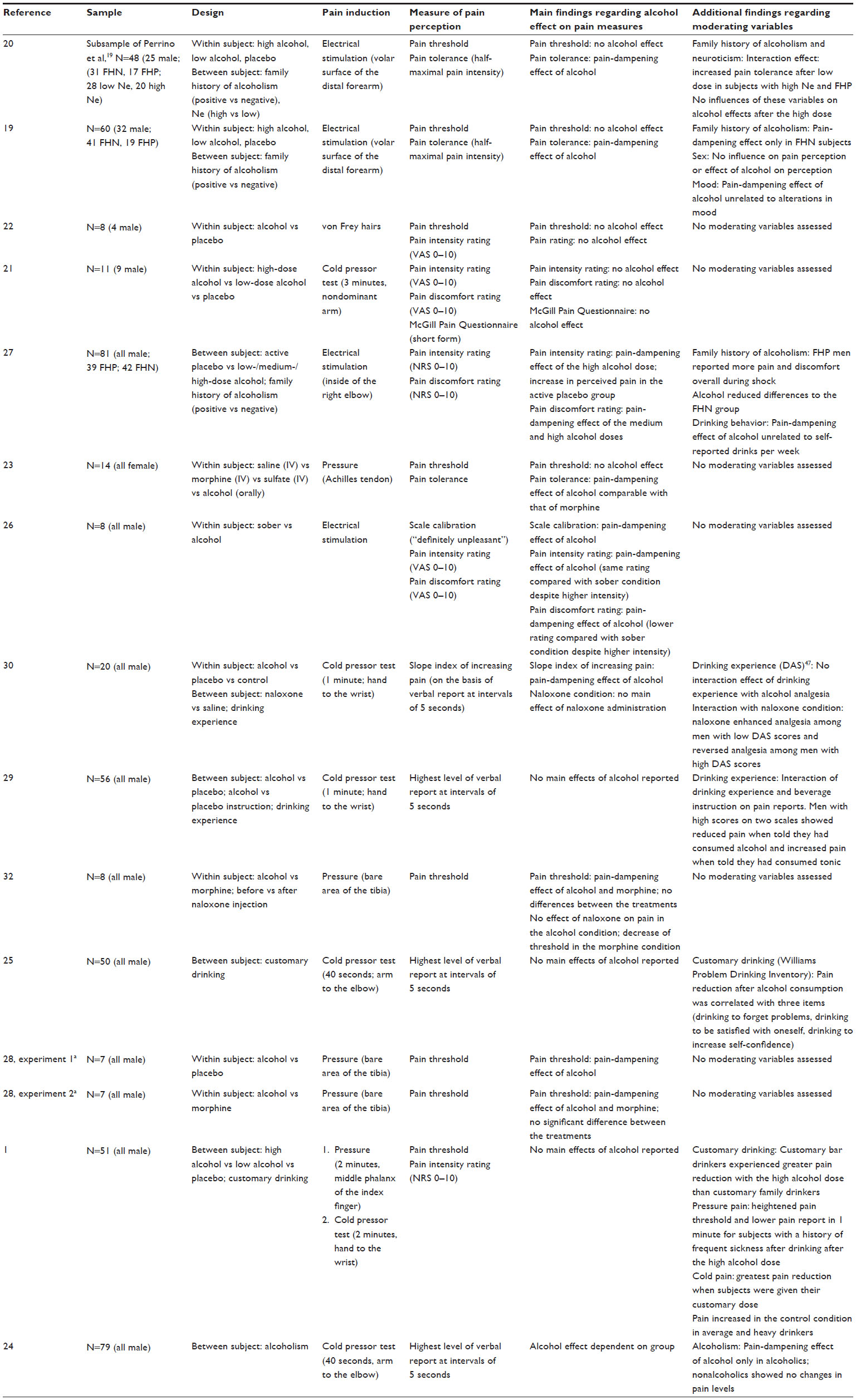 | Table 5 Methods of pain induction and pain measurement and main results concerning alcohol effects on pain perception |
Regarding pain induction, most studies used pressure pain stimulation (n=4), electrical stimulation (n=3), or the cold pressor test (n=5); one study used both pressure pain and the cold pressor test;1 and another study used von Frey hairs,22 which are calibrated filaments designed to measure cutaneous mechanical hyperalgesia.31
Measures of pain perception were pain threshold, pain tolerance, or pain ratings in most of the studies. One investigation19,20 obtained half-maximal pain intensity (ie, the stimulus intensity that was rated as 5 on an 11-point visual analog scale) as an alternative measure of pain tolerance. Of six studies assessing pain ratings, only three21,26,27 collected ratings of pain-related discomfort in addition to intensity ratings.
Effect of alcohol on pain perception
Overall, 12 of 14 studies were able to show a pain-dampening effect of alcohol (ie, increase in pain threshold or increase in pain tolerance or decrease in reported pain intensity/discomfort for a given stimulus intensity; see Table 5). However, there were some differences depending on methods used for pain induction and pain measurement, as well as administered alcohol dose and the time interval between alcohol administration and pain testing. These are described in more detail in the following paragraphs.
Pain induction and measurement
When comparing the different methods of pain induction, pain-dampening effects were most pronounced in the studies using pressure pain stimulation, with four of five studies reporting effects on pain threshold1,28,32 and one reporting effects on pain tolerance.23 Of three investigations using electrical stimulation, two detected an effect using pain ratings,26,27 whereas one found an increase in half-maximal pain intensity but not in pain threshold.19,20 The only study using von Frey hairs,22 as well as one of the studies using the cold pressor test,21 detected no pain-dampening effect of alcohol at all.
Regarding measures of pain perception, results are inconclusive for pain threshold, with four of seven studies finding an effect of alcohol. In contrast, both studies assessing pain tolerance23 or half-maximal pain intensity19,20 were able to find an increase in these measures after alcohol administration. Most of the studies collecting subjective ratings (four of six) obtained an effect of alcohol; in addition, two studies assessing both intensity and discomfort ratings suggest that alcohol might act differently on these two components, with discomfort being alleviated at lower doses27 and in a more pronounced way.26
Time interval between alcohol administration and pain testing
As already mentioned, there were considerable differences in the time interval between alcohol administration and pain testing, ranging from 10 to 110 minutes. When comparing the studies using different time intervals regarding alcohol effects on pain perception, it is noticeable that the study using the longest time interval (110 minutes)22 detected no effect of alcohol on pain perception. Effects were similar for two other studies using relatively long time intervals. Woodrow and Eltherington23 found an effect on pain tolerance but not threshold 90 minutes after alcohol administration, and Zacny et al21 detected no effect on pain ratings and the McGill Pain Questionnaire 50 minutes after consumption. These findings indicate that with longer time intervals, pain-dampening effects of alcohol are less pronounced, which might be due to descending BAC.
Administered alcohol dose
There was a large variance in the administered dose of alcohol between the different studies (0.24–1.2 g/kg) as well as in the measured values for BAC/BrAC (20–100 mg/dL); however, the effect of different doses was investigated in four studies only. Stewart et al27 compared four alcohol doses (0.10 g/kg as active placebo, 0. 38 g/kg as low dose, 0.57 g/kg as medium dose, and 0.76 g/kg as high dose) and detected effects only for the medium (mean BrAC: 85 mg/dL) and high (mean BrAC: 88 mg/dL) doses, not for the low dose (mean BrAC: 63 mg/dL). Likewise, the study reported in the publications by Perrino et al19 and Ralevski et al20 found a dose-dependent increase in half-maximal pain intensity (low dose: 0.38 g/kg, BAC: 43.7 mg/dL; high dose: 0.94 g/kg, BAC: 100 mg/dL). Zacny et al21 used doses of 0.25 g/kg (mean BrAC: 20 mg/dL) and 0.50 g/kg (mean BrAC: 54 mg/dL); neither of these doses affected pain perception. Brown and Cutter1 found an interaction between dose and customary drinking, indicating that persons experience the greatest pain reduction when given their customary dose (low dose: 0.32 g/kg; high dose: 0.63 g/kg). When comparing the studies using only one dose (n=9), eight of them used doses of 0.5 g/kg or above. Of these eight studies, seven detected an effect on pain perception. Only Duarte et al22 did not obtain effects of alcohol on pain, despite using a rather high dose of 0.7 g/kg for females and 0.8 g/kg for males (mean BAC: 84 mg/dL 65 minutes postdrink). However, in this study, pain measurement was conducted 120 minutes postdrink, when BAC had already descended to approximately 60 mg/dL (estimated based on graph; exact values are not reported).
Discussion
The aim of our systematic review was to give an overview of experimental research on effects of alcohol on pain. More precisely, we focused on the effect of nonrecurring alcohol administration in healthy humans on experimental measures of pain perception. In the following paragraphs, we will discuss the main findings concerning the effects of alcohol on pain perception, the mechanisms of action, and potential moderating variables.
Effect of alcohol on pain perception
When analyzing the 14 experimental studies identified for this review, overall, a pain-dampening effect of alcohol can be inferred; however, this effect is not compelling and seems to depend on certain conditions like the BAC at the time of pain testing and the methods used for pain induction and measurement.
Regarding the pain induction method, results indicate that pressure pain stimulation might be more sensitive for detecting pain-dampening effects of alcohol than electrical stimulation, the cold pressor test, and von Frey hairs. This might be due to several disadvantages of the latter methods. Electrical stimulation leads to direct activation of nerve fibers instead of nociceptors, leading to a specific pain sensation that is rather different from clinical pain;31 the cold pressor test elicits an intense cardiovascular stress response in addition to pain;33–35 and von Frey hairs is a specific tool for the diagnosis of mechanical hyperalgesia, which activates low-threshold mechanoreceptors in addition to nociceptors.36 Future studies might benefit from using tonic contact heat stimulation, a common, easy-to-use method that elicits a pain sensation with a strong affective component (“unpleasantness”), thus providing an experimental model for clinical pain.37,38
When comparing different measures of pain perception, alcohol effects seem to be more pronounced for pain tolerance and ratings than for pain threshold. Interestingly, of three studies reporting no effect of alcohol on pain threshold, two detected effects on other pain measures, namely pain tolerance23 or half-maximal pain intensity.19,20 This divergence might be due to different effects of alcohol on pain depending on whether stimulus intensity is at the beginning or at the end of the pain range. Also, pain tolerance is influenced more strongly by psychological factors than pain threshold, with higher anxiety leading to lower tolerance.39,40 As alcohol is known to have anxiolytic and stress-dampening effects,41 changes in pain perception might be attributable to changes in emotional state. This assumption is strengthened by the fact that two studies observed stronger effects of alcohol on unpleasantness than on intensity ratings,26,27 suggesting a modulation of the affective rather than the sensory component of pain. Likewise, experimental manipulations of emotion have been shown to predominantly influence affective reactions to pain.42–44
Mechanisms of action
Physiological and psychological mechanisms that might be involved in the effects of alcohol on pain perception have been neglected in most of the reviewed studies. Two mechanisms of interest that have been addressed by at least some of the studies are the involvement of endogenous opioids and the role of changes in mood.
Alcohol is a psychoactive substance that acts on multiple important neurotransmitter systems, including gamma-aminobutyric acid, serotonin, glutamate, and opioid systems.45 As the opioid system is crucial for endogenous pain inhibition,46 it might be involved in pain-dampening effects of alcohol. Two of the reviewed studies tested the effect of alcohol on pain after the administration of the opioid antagonist naloxone. Saddler et al32 found that naloxone blocked the antinociceptive action of morphine but not that of alcohol, despite comparable effects of both substances on the pain threshold. Unfortunately, neither the effect of alcohol nor the effect of naloxone was controlled by a placebo condition. Cutter and O’Farrell,30 using a placebo-controlled design, detected an effect of naloxone on the pain-dampening action of alcohol in the cold pressor test, but only in subjects with high scores on a drinking experience scale (Definitions of Alcohol Scale).47 The authors argue that high scores on this scale indicate a history of drinking in order to reduce distress. The co-occurrence of alcohol intake and stress-induced analgesia then results in a learnt opioid response, which enhances pain-dampening effects of alcohol. Taken together, the involvement of the opioid system in actions of alcohol on pain in humans is still unclear. Other important neurotransmitter systems have not been subject to investigation.
As alcohol is known to have stress-dampening and mood-enhancing effects,41,48 and close interactions between emotion and pain are also established,49 alcohol might affect pain perception at least partly via a modulation of emotional state. This is also indicated by the fact that alcohol seems to have stronger effects on pain tolerance than on threshold, and stronger effects on ratings of unpleasantness than on ratings of intensity. However, only two of the 14 studies included in this review controlled for mood; Duarte et al22 found no alcohol effects on mood and pain perception, and Perrino et al19 reported alcohol effects on pain being unrelated to changes in mood. Future experimental studies should assess alcohol-induced changes in mood and anxiety in order to clarify the significance of these effects for the pain-dampening action of alcohol.
Moderating variables
Possibly the effect of alcohol on pain perception is moderated by other variables like sex, drinking history, and alcoholism. Results of the reviewed studies concerning these moderating effects are discussed in the following paragraphs.
Sex
Based on the studies identified for this review, sex effects cannot be inferred, as eleven of 14 studies did not even investigate mixed samples. Of the remaining three studies, two used a very small sample with unequal proportions of male and female subjects, so sex differences could not be analyzed.21,22 Thus, the investigation published by Perrino et al19 and Ralevski et al20 is the only one including a mixed sample of acceptable size. These authors do not report sex differences regarding the effect of alcohol on pain perception. Additionally, the study conducted by Woodrow and Eltherington23 with a purely female sample yielded similar results. Consequently, there is to date no evidence for sex differences in the pain-dampening effects of alcohol, but such effects have hardly been investigated systematically. Particularly as there is evidence for sex differences in alcohol metabolism, expectancy sets, and alcohol effects on cognition,50–53 this appears to be an important topic to be addressed in future studies.
Drinking history and motives
Five studies, four of which originate from the research group around Cutter, focused on the relationship between alcohol effects on pain perception and the reasons for drinking or customary drinking behavior. Whereas two studies found no association between drinking behavior and the pain-dampening effect of alcohol,27,30 Cutter et al25 showed a correlation of single items assessing drinking motives (Williams Problem Drinking Inventory)54 with pain reduction after the consumption of whiskey during a cold pressor task. “Drinking to forget problems” was the item being the best predictor of alcohol-induced analgesia. Individuals responding negatively to the associated items showed an increase in pain after whiskey intake, whereas subjects affirming these items tended to show a decrease in pain. Unfortunately, expectancy effects have not been controlled by a placebo design in this study.
However, the association between alcohol-induced pain reduction and individual drinking history could be replicated by a placebo-controlled study in a sample of college students;1 here, solitary barroom drinkers displayed the greatest response to the high alcohol dose. Overall, subjects showed the greatest pain reduction in a cold pressor test when receiving their customary alcohol dose. Additionally, Cutter et al29 showed that this relationship existed also for the expectation of having consumed alcohol by using a balanced placebo design. In this study, subjects scoring high on two drinking behavior scales (amount of alcohol consumed on one occasion, positive emotional reasons for drinking) showed a reduction in pain when being told that they had received alcohol, and an increase in pain when being told that they had received tonic. The authors interpret this hyperalgesic effect as a result of disappointment or frustration due to not receiving alcohol. Taken together, these studies suggest a pain-dampening effect of alcohol in coping drinkers (ie, persons who drink to cope with problems), whereas pain perception in noncoping drinkers remains unchanged or is even enhanced by alcohol. This pattern of results might be explainable by differences in beliefs concerning the efficacy of alcohol. It has already been shown that coping drinkers tend to have more positive alcohol expectancies than noncoping drinkers.55,56 Thus, the lack of positive expectancies in noncoping drinkers might lead to alcohol effects interfering with other strategies for coping with pain, leading to no changes or even an increase in pain perception. This assumption is in line with findings obtained by Lawton and Simpson14 suggesting an association between coping strategies and alcohol use in chronic pain patients.
Hence, drinking motives and expectancies might moderate the pain-dampening effect of alcohol, and more research using randomized, placebo-controlled designs is needed to further explore this relationship.
Alcoholism
The association between alcoholism and the pain-dampening effect of alcohol has also been of interest; however, there is to date only one experimental study that investigated this topic. Here, intake of whiskey reduced pain experienced during a cold pressor test in nonabstaining alcoholics but not in nonalcoholics.24
Enhanced sensitivity to the effect of alcohol on pain perception in alcoholics might be a consequence of alcoholism, but the susceptibility to the pain-alleviating effect might be a predisposing factor for alcoholism as well. Accordingly, Stewart et al27 showed that men being at a heightened risk for alcoholism due to a family history of alcoholism reported more pain and discomfort during electric shocks, and that this “hypersensitivity” was normalized by alcohol intake. However, these findings could not be replicated; in fact, other data suggested an attenuated response to the pain-dampening effect of alcohol in individuals with a family history of alcoholism.19 The data of Perrino et al19 were reanalyzed with regard to neuroticism;18 this analysis showed that subjects with high neuroticism scores and a positive family history of alcoholism experienced more pain reduction after the low alcohol dose. Thus, the role of family history of alcoholism for individual differences in pain-dampening effects of alcohol is still far from clear, so this factor should be taken into account in future studies.
Limitations
In order to assess the effects of alcohol on pain, a meta-analysis of experimental studies should have been the method of choice. However, as only a small number of very heterogeneous investigations could be identified, data were only sufficient for a systematic review. Additionally, we do not have any information about a possible publication bias, as unpublished data in this field are not available on respective study registers (eg, clinicaltrialsregister.eu). There are also some important limitations of the reviewed studies and suggestions for future studies, which will be addressed in the following paragraph.
Limitations of reviewed studies and suggestions for future research
Taken together, the 14 studies identified for this review suggest a pain-dampening effect of alcohol administration on experimental pain. However, some of these studies have considerable methodological limitations (eg, insufficient blinding and placebo control or inappropriate sample characteristics [very small samples, only one sex]). In addition, there is only very limited information about possible mechanisms of action (eg, changes in mood) and moderating variables (eg, sex). With regards to pain induction and measurement, future studies might benefit from using well-established stimulation methods like contact heat. Furthermore, effects of alcohol on endogenous pain modulation (conditioned pain modulation, temporal summation) should be investigated, as associations of these measures with clinical pain have been shown.57–61 In terms of alcohol administration, effects of variations in administered doses and time intervals between administration and pain testing should be tested systematically.
Conclusion
Overall, a pain-dampening effect of alcohol is suggested, but the mechanisms of action and moderating variables are still unclear. In addition, there is to date no experimental investigation of alcohol effects on pain perception in patients with chronic pain syndromes, despite the well-documented use of alcohol as self-medication in these patients. Better knowledge of the key mechanisms involved in pain-dampening effects of alcohol might provide a starting point for the prevention of problematic alcohol consumption in chronic pain. Primarily, further experimental research concerned with alcohol effects on pain in individuals suffering from chronic pain is essentially needed.
Disclosure
The authors report no conflicts of interest in this work.
References
Brown RA, Cutter HS. Alcohol, customary drinking behavior, and pain. J Abnorm Psychol. 1977;86(2):179–188. | |
Sandström J, Andersson GB, Wallerstedt S. The role of alcohol abuse in working disability in patients with low back pain. Scand J Rehabil Med. 1984;16(4):147–149. | |
Katon W, Egan K, Miller D. Chronic pain: lifetime psychiatric diagnoses. Am J Psychiatry. 1985;142(10):1156–1160. | |
Gorman DM, Potamianos G, Williams KA, Frank AO, Duffy SW, Peters TJ. Relationship between alcohol abuse and low back pain. Alcohol Alcohol. 1987;22(1):61–63. | |
Hoffmann NG, Olofsson O, Salen B, Wickstrom L. Prevalence of abuse and dependency in chronic pain patients. Int J Addict. 1995;30(8):919–927. | |
Levenson JL, McClish DK, Dahman BA, et al. Alcohol abuse in sickle cell disease: the PiSCES project. Am J Addict. 2007;16(5):383–388. | |
Sheu R, Lussier D, Rosenblum A, et al. Prevalence and characteristics of chronic pain in patients admitted to an outpatient drug and alcohol treatment program. Pain Med. 2008;9(7):911–917. | |
Brennan PL, Schutte KK, Moos, RH. Pain and use of alcohol to manage pain: prevalence and 3-year outcomes among older problem and non-problem drinkers. Addiction. 2005;100(6):777–786. | |
Egli M, Koob GF, Edwards S. Alcohol dependence as a chronic pain disorder. Neurosci Biobehav Rev. 2012;36(10):2179–2192. | |
Apkarian AV, Neugebauer V, Koob G, et al. Neural mechanisms of pain and alcohol dependence. Pharmacol Biochem Behav. 2013;112:34–41. | |
Riley III JL, King C. Self-report of alcohol use for pain in a multi-ethnic community sample. J Pain. 2009;10(9):944–952. | |
Arcury TA, Bernard SL, Jordan JM, Cook HL. Gender and ethnic differences in alternative and conventional arthritis remedy use among community-dwelling rural adults with arthritis. Arthritis Care Res. 1996;9(5):384–390. | |
Riley III JL, Gilbert GH, Heft MW. Orofacial pain: racial and sex differences among older adults. J Public Health Dent. 2002;62(3):132–139. | |
Lawton J, Simpson J. Predictors of alcohol use among people experiencing chronic pain. Psychol Health Med. 2009;14(4):487–501. | |
Jakobsson U, Hallberg IR, Westergren A. Pain management in elderly persons who require assistance with activities of daily living: a comparison of those living at home with those in special accommodations. Eur J Pain. 2004;8(4):335–344. | |
Mullin FJ, Luckhardt AB. The effect of alcohol on cutaneous tactile and pain sensitivity. Am J Physiol. 1934;109:77–78. | |
Wolff HG, Hardy JD, Goodell H. Measurement of the effect on the pain threshold of acetylsalicylic acid, acetanilid, acetophenetidin, aminopyrine, ethyl alcohol, trichlorethylene, a barbiturate, quinine, ergotamine tartrate and caffeine: an analysis of their relation to the pain experience. J Clin Invest. 1941;20(1):63–80. | |
Wolff HG, Hardy JD, Goodell H. Studies on pain: measurement of the effect of ethyl alcohol on the pain threshold and on the “alarm reaction”. J Pharmacol. 1942;75(1):38–49. | |
Perrino AC, Ralevski E, Acampora G, Edgecombe J, Limoncelli D, Petrakis IL. Ethanol and pain sensitivity: effects in healthy subjects using an acute pain paradigm. Alcohol Clin Exp Res. 2008;32(6):952–958. | |
Ralevski E, Perrino A, Acampora G, Koretski J, Limoncelli D, Petrakis I. Analgesic effects of ethanol are influenced by family history of alcoholism and neuroticism. Alcohol Clin Exp Res. 2010;34(8):1433–1441. | |
Zacny JP, Camarillo VM, Sadeghi P, Black M. Effects of ethanol and nitrous oxide, alone and in combination, on mood, psychomotor performance and pain reports in healthy volunteers. Drug Alcohol Depend. 1998;52(2):115–123. | |
Duarte R, McNeill A, Drummond G, Tiplady B. Comparison of the sedative, cognitive, and analgesic effects of nitrous oxide, sevoflurane, and ethanol. Brit J Anaesth. 2008;100(2):203–210. | |
Woodrow KM, Eltherington LG. Feeling no pain: alcohol as an analgesic. Pain. 1988;32(2):159–163. | |
Cutter HS, Maloof B, Kurtz NR, Jones WC. “Feeling no pain” differential responses to pain by alcoholics and nonalcoholics before and after drinking. J Stud Alcohol. 1976;37(3):273–277. | |
Cutter HS, Jones WC, Maloof BA, Kurtz NR. Pain as a joint function of alcohol intake and customary reasons for drinking. Int J Addict. 1979;14(2):173–182. | |
Gustafson R, Källmén H. Alcohol and unpleasant stimulation: subjective shock calibration and pain and discomfort perception. Percept Mot Skills. 1988;66(3):739–742. | |
Stewart SH, Finn PR, Pihl RO. A dose-response study of the effects of alcohol on the perceptions of pain and discomfort due to electric shock in men at high familial-genetic risk for alcoholism. Psychopharmacology (Berl). 1995;119(3):261–267. | |
James MFM, Duthie AM, Duffy BL, McKeag AM, Rice CP. Analgesic effect of ethyl alcohol. Brit J Anaesth. 1978;50(2):139–141. | |
Cutter HS, O’Farrell TJ, Whitehouse J, Dentch GM. Pain changes among men from before to after drinking: effects of expectancy set and dose manipulations with alcohol and tonic as mediated by prior experience with alcohol. Int J Addict. 1986;21(8):937–945. | |
Cutter HS, O’Farrell TJ. Experience with alcohol and the endogenous opioid system in ethanol analgesia. Addict Behav. 1987;12(4):331–343. | |
Staahl C, Drewes AM. Experimental human pain models: a review of standardised methods for preclinical testing of analgesics. Basic Clin Pharmacol Toxicol. 2004;95(3):97–111. | |
Saddler JM, James MFM, Harington AP. Naloxone does not reverse ethanol analgesia in man. Clin Exp Pharmacol Physiol. 1985;12(4):359–364. | |
Schwabe L, Haddad L, Schachinger H. HPA axis activation by a socially evaluated cold-pressor test. Psychoneuroendocrinology. 2008;33(6):890–895. | |
Duncko R, Johnson L, Merikangas K, Grillon C. Working memory performance after acute exposure to the cold pressor stress in healthy volunteers. Neurobiol Learn Mem. 2009;91(4):377–381. | |
Schoofs D, Wolf OT, Smeets T. Cold pressor stress impairs performance on working memory tasks requiring executive functions in healthy young men. Behav Neurosci. 2009;123(5):1066–1075. | |
Le Bars D, Gozariu M, Cadden SW. Animal models of nociception. Pharmacol Rev. 2001;53(4):597–652. | |
Handwerker HO, Kobal G. Psychophysiology of experimentally induced pain. Physiol Rev. 1993;73(3):639–671. | |
Lautenbacher S, Roscher S, Strian F. Tonic pain evoked by pulsating heat: temporal summation mechanisms and perceptual qualities. Somatosens Mot Res. 1995;12(1):59–70. | |
Robin O, Vinard H, Vernet-Maury E, Saumet JL. Influence of sex and anxiety on pain threshold and tolerance. Funct Neurol. 1987;2(2):173–179. | |
James JE, Hardardottir D. Influence of attention focus and trait anxiety on tolerance of acute pain. Brit J Health Psychol. 2002;7(Pt2):149–162. | |
Sayette MA. Does drinking reduce stress? Alcohol Res Health. 1999;23(4):250–255. | |
Rainville P, Bao QVH, Chrétien P. Pain-related emotions modulate experimental pain perception and autonomic responses. Pain. 2005;118(3):306–318. | |
Kenntner-Mabiala R, Weyers P, Pauli P. Independent effects of emotion and attention on sensory and affective pain perception. Cog Emot. 2007;21(8):1615–1629. | |
Loggia ML, Mogil JS, Bushnell MC. Experimentally induced mood changes preferentially affect pain unpleasantness. J Pain. 2008;9(9):784–791. | |
Chastain G. Alcohol, neurotransmitter systems, and behavior. J Gen Psychol. 2006;133(4):329–335. | |
Fields H. State-dependent opioid control of pain. Nat Rev Neurosci. 2004;5(7):565–575. | |
Mulford HA, Miller DE. Drinking in Iowa: III. A scale of definitions of alcohol related to drinking behavior. Q J Stud Alcohol. 1960;21:267–278. | |
Baum-Baicker C. The psychological benefits of moderate alcohol consumption: a review of the literature. Drug Alcohol Depend. 1985;15(4):305–322. | |
Lumley MA, Cohen JL, Borszcz GS, et al. Pain and emotion: a biopsychosocial review of recent research. J Clin Psychol. 2011;67(9):942–968. | |
Lundahl LH, Davis TM, Adesso VJ, Lukas SE. Alcohol expectancies: effects of gender, age, and family history of alcoholism. Addict Behav. 1997;22(1):115–125. | |
Kwo PY, Ramchandani, VA, O’Connor S, et al. Gender differences in alcohol metabolism: relationship to liver volume and effect of adjusting for body mass. Gastroenterology. 1998;115(6):1552–1557. | |
Read JP, Wood MD, Kahler CW, Maddock JE, Palfai TP. Examining the role of drinking motives in college student alcohol use and problems. Psychol Addict Behav. 2003;17(1):13–23. | |
Oscar-Berman M, Marinkovic K. Alcohol: effects on neurobehavioral functions and the brain. Neuropsychol Rev. 2007;17(3):239–257. | |
Williams AF. Validation of a college problem-drinking scale. J Proj Tech Pers Assess. 1967;31(1):33–40. | |
Connors GJ, O’Farrell TJ, Cutter HS, Thompson DL. Alcohol expectancies among male alcoholics, problem drinkers, and nonproblem drinkers. Alcohol Clin Exp Res. 1986;10(6):667–671. | |
Lewis BA, O’Neill HK. Alcohol expectancies and social deficits relating to problem drinking among college students. Addict Behav. 2000;25(2):295–299. | |
Maixner W, Fillingim R, Sigurdsson A, Kincaid S, Silva S. Sensitivity of patients with painful temporomandibular disorders to experimentally evoked pain: evidence for altered temporal summation of pain. Pain. 1998;76(1–2):71–81. | |
Staud R, Vierck CJ, Cannon RL, Mauderli AP, Price DD. Abnormal sensitization and temporal summation of second pain (wind-up) in patients with fibromyalgia syndrome. Pain. 2001;91(1–2):165–175. | |
Staud R, Robinson ME, Vierck Jr CJ, Price DD. Diffuse noxious inhibitory controls (DNIC) attenuate temporal summation of second pain in normal males but not in normal females or fibromyalgia patients. Pain. 2003;101(1–2):167–174. | |
Pielsticker A, Haag G, Zaudig M, Lautenbacher S. Impairment of pain inhibition in chronic tension-type headache. Pain. 2005;118(1–2):215–223. | |
Yarnitsky D, Crispel Y, Eisenberg E, et al. Prediction of chronic post-operative pain: pre-operative DNIC testing identifies patients at risk. Pain. 2008;138(1):22–28. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.