")
Back to Journals » Drug Design, Development and Therapy » Volume 14
The Effect of Liver and Kidney Disease on the Pharmacokinetics of Clozapine and Sildenafil: A Physiologically Based Pharmacokinetic Modeling
Authors Ghoneim AM , Mansour SM
Received 16 January 2020
Accepted for publication 24 March 2020
Published 14 April 2020 Volume 2020:14 Pages 1469—1479
DOI https://doi.org/10.2147/DDDT.S246229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Amira M Ghoneim,1 Suzan M Mansour2,3
1Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmaceutical Sciences and Pharmaceutical Industries, Future University in Egypt, Cairo, Egypt; 2Pharmacology & Toxicology Department, Faculty of Pharmacy, Cairo University, Cairo, Egypt; 3Department of Pharmacology, Toxicology & Biochemistry, Faculty of Pharmaceutical Sciences and Pharmaceutical Industries, Future University in Egypt, Cairo, Egypt
Correspondence: Amira M Ghoneim
90th St, Cairo Governorate, Cairo 11835, Egypt
Tel +20 1223124998
Email [email protected]
Background and Objectives: Physiologically based pharmacokinetic (PBPK) modeling permits clinical scientists to reduce practical constraints for clinical trials on patients with special diseases. In this study, simulations were carried out to validate the pharmacokinetic parameters of clozapine and sildenafil using Simcyp® simulator in young male adults and compare the effect of renal or hepatic impairment on the pharmacokinetic parameters of clozapine and sildenafil. Also, the effect of age on pharmacokinetic parameters of both drugs was investigated in healthy population and in patients with renal and hepatic impairment.
Methods: A full PBPK model was built in the simulator for clozapine and sildenafil based on physicochemical properties and observed clinical results. The model used was Advanced, Dissolution, Absorption and Metabolism (ADAM) for both drugs.
Results: The PBPK model adequately predicted the pharmacokinetic parameters of clozapine and sildenafil for the healthy adult population. In the simulation results, the bioavailability of both drugs was remarkably raised in both renal and hepatic impairment in young and elderly populations.
Conclusion: PBPK modeling could be helpful in the investigation and comparison of the pharmacokinetics in populations with specific disease conditions.
Keywords: physiologically based pharmacokinetic, clozapine, sildenafil, liver, kidney, impairment
Introduction
In the physiologically based pharmacokinetic (PBPK) model, organs and tissues all over the body are represented as specific systems. This model allows researchers to investigate drug–drug interactions (DDI) and predict the effects of age, genetics, or disease on the pharmacokinetics (PKs) of drugs.1 The use of PBPK modeling has grown over recent years and has been included in both regulatory submissions and approved drug labels.2
Clozapine is a tricyclic dibenzodiazepine, which is considered to be remarkably efficient in the treatment of schizophrenia, specifically in treatment-resistant schizophrenia.3 Clozapine is metabolized by the cytochrome P450 (CYP) system of enzymes in the liver, yielding a pharmacologically active metabolite, norclozapine. The most influential CYP isoformin on clozapine metabolism is CYP1A2, which has a major impact on the determination of the dose of the drug.4 There are other CYP enzymes responsible for clozapine metabolism, like, CYP2D6 and CYP3A4.4 In vitro experiments suggest that CYP3A4 accounts for around 70% of clozapine clearance, CYP1A2 around 15%, and 5% or less for each of CYP2C19, CYP2C8 and FMO3.5 Several enzymes were capable of generating the n-oxide metabolite of clozapine in vitro (CYP1A2, CYP2E1, CYP2C9, CYP3A4, CYP2D6, FMO3, CYP2C19) but in vivo CYP1A2 is regarded as the main catalyst.6–8 Clozapine is 95% protein-bound in patient's serum. When the unbound drug undergoes glomerular filtration in the kidney, nearly 90% of the filtered clozapine is reabsorbed in the tubule.9
Moreover, clozapine is prescribed to lessen the risk of recurrent suicidal behavior in schizophrenic patients.3 The occurrence of extrapyramidal adverse events is considered rare with clozapine therapy. However, clozapine is sometimes limited to cases of treatment-resistant schizophrenia, as a result of its significant risks.10 Among these risks is clozapine-induced agranulocytosis; thus, treatment with clozapine demands regular monitoring of white blood counts and absolute neutrophil counts, and in the US, the FDA instructs that patients on clozapine treatment be enrolled in a computer-based registry.11,12 Sexual dysfunction is popular among patients receiving clozapine, and is the most aggravating side effect, resulting in a negative impact on patients and their desire to continue medication.13 Hyperprolactinemia is considered to be the main element for this side effect.
Sildenafil has proven to cause significantly improved sexual performance as compared to a placebo, when tested on patients suffering from sexual dysfunction.14,15 Sildenafil selectively inhibits cyclic guanosine monophosphate in the corpus cavernosum.
Sildenafil is metabolized by CYP3A4 as the main route and CYP2C9 as a secondary route. Sildenafil is mainly cleared from the plasma non-renally, with a mean half-life of between 3 and 6 hrs.16 Sildenafil is hastily absorbed after oral administration, resulting in low absolute bioavailability (≈40%).17
There are several suggested mechanisms to describe the impact of chronic liver impairment on drug metabolism. Among these mechanisms is the change in the size of the liver, which becomes smaller, leading to a decline in hepatic blood flow and hepatocyte function.18 Since both clozapine and sildenafil are highly metabolized by the liver, evaluation of PK parameters of both drugs in patients with hepatic impairment (HI) should be investigated.
Although renal excretion is not considered to accord extensively to clozapine or sildenafil clearance, subsidiary effects of renal impairment (RI) may affect the elimination of both drugs. Among these changes are loss of renal albumin and inhibition of hepatic metabolizing enzymes, which result in changes in protein binding of the drugs.19
Ageing is an additional factor that can influence the pharmacokinetic profile of clozapine and sildenafil due to increase in systematic exposure.19 As adipose mass increases with ageing, the volume of distribution is higher for lipophilic drugs, such as clozapine.9 Lipophilic drugs could accumulate in adipose tissue, leading to a prolongation of their half-lives and their duration of action, thus increasing the risk of iatrogenic events in the elderly.20 Aging is accompanied by decline in hepatic and renal functions and variations in plasma protein concentrations.18,19 Reduction in hepatic blood flow and deterioration in the activity of hepatic CYP enzymes may lead to reduced clearance of drugs metabolized by the liver in the elderly population.18
This research aimed to validate the PBPK models, which describe the PKs of clozapine and sildenafil in healthy adults. The PKs of both drugs in patients with RI or HI were investigated. Also, the effect of age on the PKs of these drugs was studied. Preliminary findings from the study presented have previously been presented at the 11th Geneva conference on person-centred medicine; 2018-04-08 to 2018-04-11.
Patients and Methods
PBPK Workflow
PBPK modeling was conducted using a population-based PBPK platform, the Simcyp® Simulator (V17.1; Certara, Sheffield, UK). The applied model for clozapine was Advanced, Dissolution, Absorption and Metabolism (ADAM). ADAM modelV16.1 has been described fully by Darwich et al,21 but version 17.1 has been modified to improve the simulation effect. For example, gut transporters have been included, which have a significant impact on the concentration of the drug in most organs. For sildenafil, Multi-layer Gut Wall within ADAM (M-ADAM) model was used to set the drug as a competitive inhibitor of the P-glycoprotein transporter (ABCB1).22 Also, a comparison was carried out between the first-order absorption model and the ADAM model. Selection of the optimum model depended on the ability of the model to predict plasma concentration-time profiles comparable to published clinical studies. Each simulation was performed in 100 male subjects (10 trials with 10 male subjects for each trial, aged between 20 and 45) using the virtual population libraries included in the simulator.23
Clozapine and Sildenafil PBPK Models
Drug-dependent input parameters of clozapine and sildenafil are listed in Table 1. The pre-validated clozapine and sildenafil compound files supplied in the compound library were adopted for full PBPK distribution model with a predicted volume of distribution at steady-state (Vss) of 4.6 and 1.2 L/kg, for clozapine and sildenafil, respectively. The Kp scalar was set to 1for sildenafil, the mechanistic passive regional permeability (Ptrans) was predicted based upon log P value. Polar surface area data (data not shown) were applied to predict human jejunum effective permeability (Peff, man) of clozapine. The enzyme kinetics model was used for simulation of the elimination of both drugs.
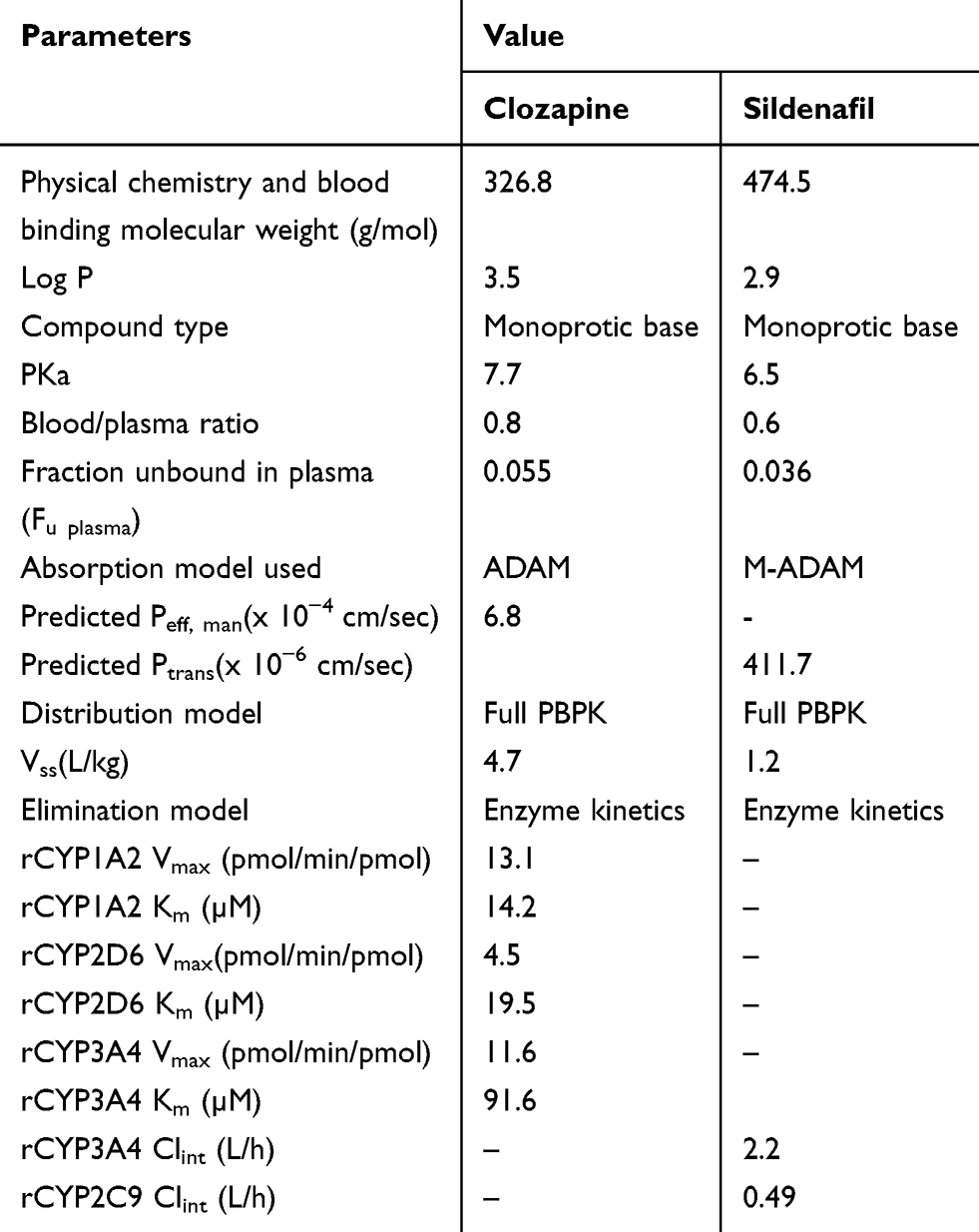 |
Table 1 Parameter Values Used for Clozapine and Sildenafil Simulation |
Data for clinical comparisons were obtained from literature references that contained PK parameters for the compounds of interest. For clozapine, PK parameters were acquired from Golden and Honigfeld.24 The data for sildenafil were obtained from Radicioni et al.25 The predictive performance of each model was achieved by comparing the predicted Cmax, Tmax and AUC0-t of each drug to the clinically observed PK parameters.
Accordingly, clozapine and sildenafil concentration–time profiles were simulated in ten trials for study 1 and 2 after dosing, where the dosage regimens were similar to those in the clinical studies. In study 1, 100 mg of clozapine immediate release tablet was orally administered twice daily for young healthy volunteers (HV) for 3 days. In study 2, sildenafil was administered orally once for HV at a dose of 100 mg in the form of immediate release tablets.
Simulation
Following appropriate optimization and verification of the clozapine and sildenafil PBPK models, the PK at steady state in subjects with renal or hepatic impairment were investigated by simulation using the pre-existing population modules in the simulator. All subjects were prescribed to take clozapine 100 mg orally twice a day for a period of 3 days for study 1 and 100 mg of sildenafil once daily for 1 day for study 2.
Regarding RI, the library included two types of virtual populations for the moderate (RI-GFR-30_60) and severe (RI-GFR_30) RI patients. These populations were classified according to the glomerular filtration rate, where it is between 30 and 60 (moderate) or less than 30 (severe).26 Furthermore, there are three populations for HI patients in the simulator. They are classified according to the Child–Pugh classes A, B and C as HI-A, HI-B and HI-C, respectively.27
In the simulation of both drugs PK according to disease status, the age of healthy adults was set to 20–45 years regardless of disease status. In contrast, as the simulator provides the age ranges for patients with RI up to 85 years and for the population with hepatic impairments up to 70 years, the ages of elderly subjects were set as 65–85 years for RI populations, and 65–70 years for hepatic impairments, respectively. The simulated parameters were compared according to the disease status in each age group by calculating the fold changes of the parameters from the normal condition.
The virtual populations of RI and HI patients have specific key features. Features for RI patients include reduction in several elements like kidney weight, blood flow, CYP P450 expression, and serum albumin and hematocrit levels. While features for HI patients include the same features mentioned in RI patients, in addition to reduction of a-1 acid glycoprotein levels, portal hypertension, with consequential blood shunting to bypass the liver, and increased blood flow through the hepatic artery and mesentery.27
Results
The clozapine and sildenafil PBPK models reasonably predicted PK parameters, such as time to reach maximum concentration (Tmax), maximum concentration (Cmax), area under the time–concentration curve (AUC0-t) where the predicted over observed ratios were between 0.7 and 1.2 (Table 2).
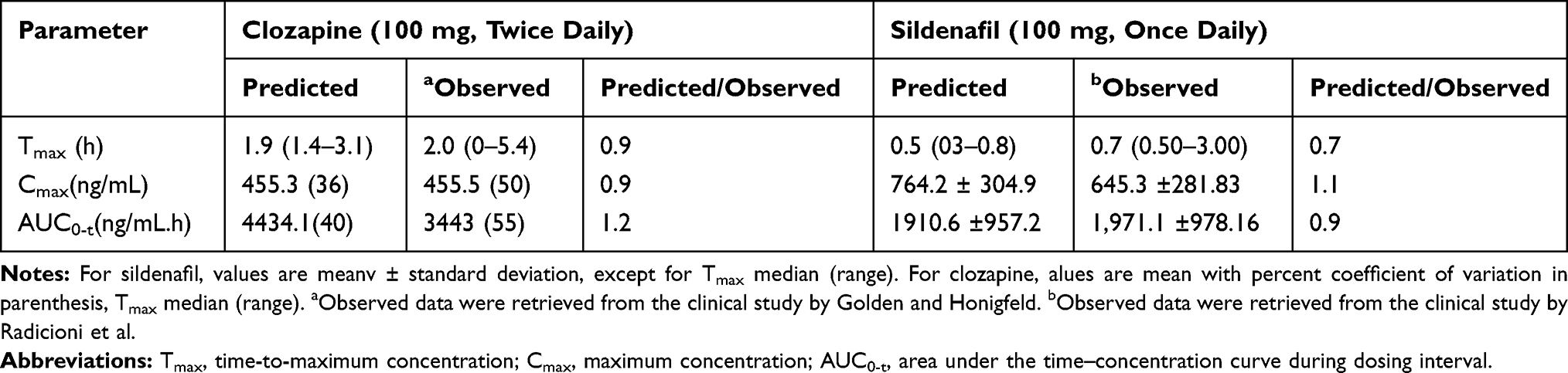 |
Table 2 Comparison Between Predicted and Observed Pharmacokinetic Parameters |
For clozapine, the first-order absorption model predicted the PK parameters, where Tmax, Cmax and AUC0-t were within 0.6, 0.8 and 0.8 folds of the ADAM model parameters, respectively. As for sildenafil, Tmax, Cmax and AUC0-t were within 2.2, 0.6 and 1.2 folds of the M-ADAM model, respectively (Supplemental Table 1). Comparing the PK parameters from the first-order absorption model to the observed data, it was clear that ADAM and M-ADAM models were more accurate at predicting the PK parameters of clozapine and sildenafil.
An illustration of clozapine PKs in young adults and the elderly population employing the model of HV, HI and RI populations is present in Tables 3 and 4, as well as, Figures 1 and 2. CLpo, ss (apparent oral clearance at steady state) was not significantly different between the healthy male adults and the elderly populations.
 |
Table 3 Comparison of Clozapine Pharmacokinetic Parameters for Young Adults According to Different Conditions |
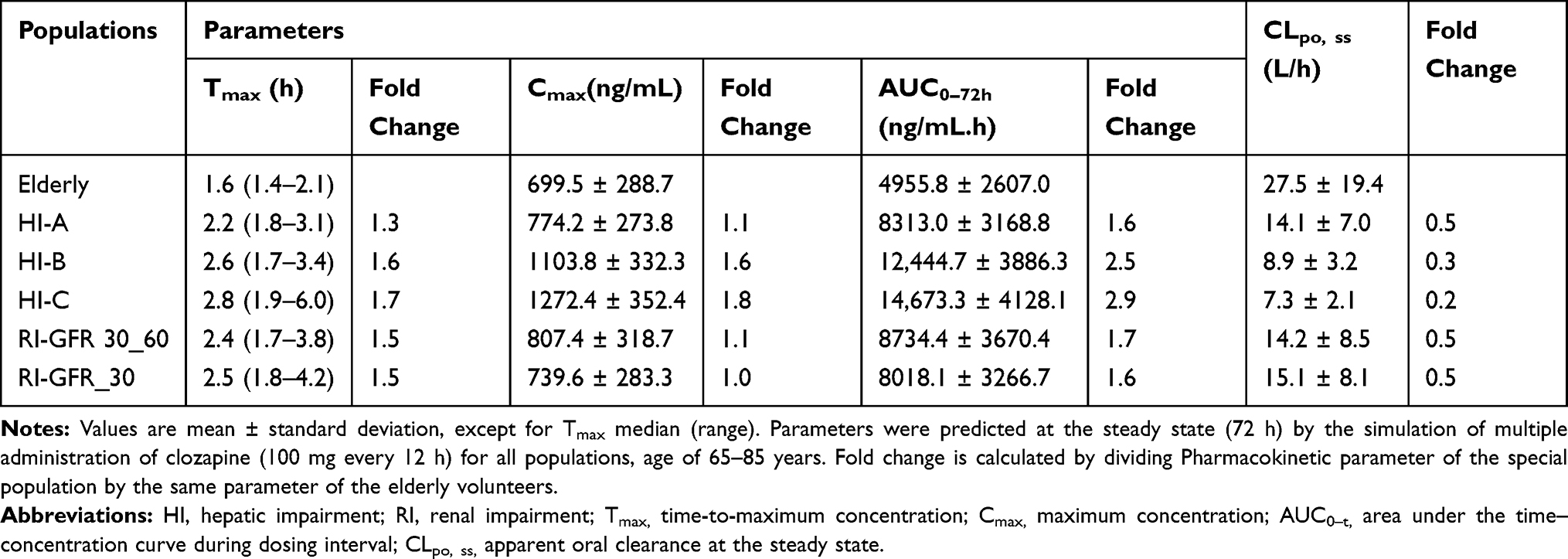 |
Table 4 Comparison of Clozapine Pharmacokinetic Parameters for Elderlypopulationaccording to Different Conditions |
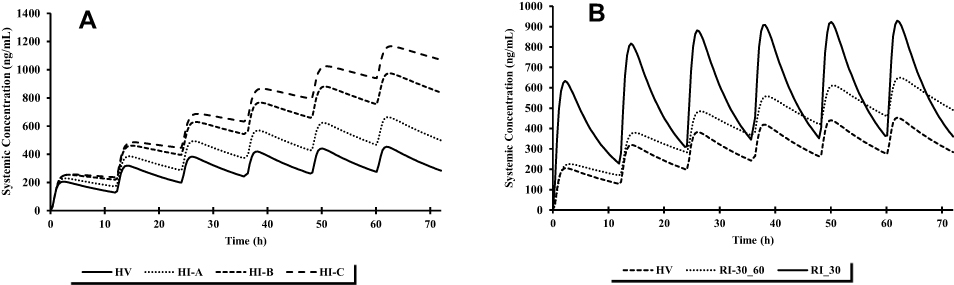 |
Figure 1 Comparison of simulated mean clozapine concentrations for young adults according to (A) hepatic function and (B) renal function after multiple administration of clozapine 100 mg every 12 h. |
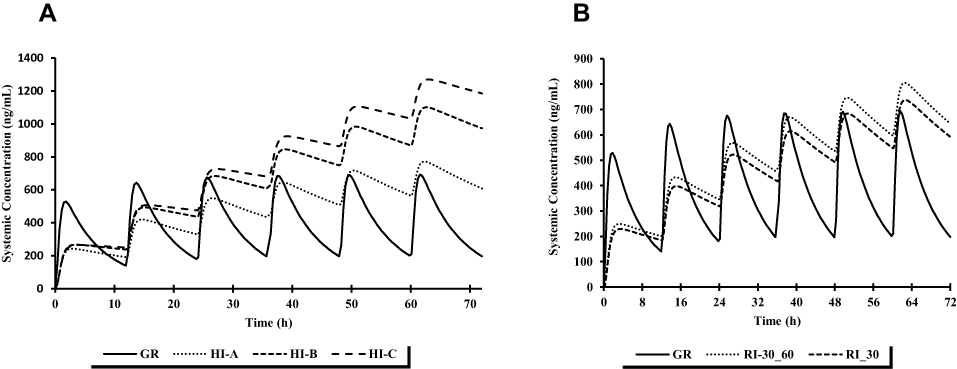 |
Figure 2 Comparison of simulated mean clozapine concentrations for elderly population according to (A) hepatic function and (B) renal function after multiple administration of clozapine 100 mg every 12 h. |
The results revealed that CLpo, ss was lowered by ≈ 38% in the HI-A compared to HV, which resulted in an increase in Cmax by 45% and 58% in AUC0-t. While CLpo, ss was reduced by ≈ 48% in the elderly population, which surprisingly resulted in only 10% rise in Cmax, and 67% in AUC0-t. Regarding HI-B patients, CLpo, ss was ≈ 65% lower in the young adults and elderly populations. This reduction resulted in around two-fold increase in Cmax, and AUC0-t. The systemic exposure of clozapine was markedly increased with severe hepatic impairment (HI-C), where CLpo, ss was ≈ 70% lower in the young adults and the elderly populations. An increased Cmax of ≈ 2-fold or more was predicted in both populations, while AUC0-t was raised by ≈ 3 folds.
On the over hand, there was no difference in CLpo, ss among RI-GFR 30_60 and RI-GFR_30 patients of both young and elderly populations. CLpo, ss was reduced by 35% for the young adults and Cmax was 1.4 and 2 fold higher in RI-GFR 30_60 and RI-GFR_30 young patients, respectively. While AUC0-t was ≈ raised by 1.6 folds in young patients with RI-GFR 30_60 and RI-GFR_30. Regarding the elderly population, CLpo, ss was 48% lower; however, Cmax was not affected in RI-GFR 30_60 and RI-GFR_30 elderly patients. Only the AUC0-t was increased by ≈ 1.7 folds in both classes of elderly patients. It is worth to note that the Tmax was the least parameter affected by age and disease conditions. It was within 1.6 folds of the normal condition in the young HI-B, HI-C, RI-GFR 30_60 and RI-GFR_30 patients.
A comparison between the concentration–time curve and PK parameters of sildenafil in different populations is presented in Tables 5 and 6 and Figures 3 and 4. Clpo, ss did not vary significantly between the young and the elderly populations.
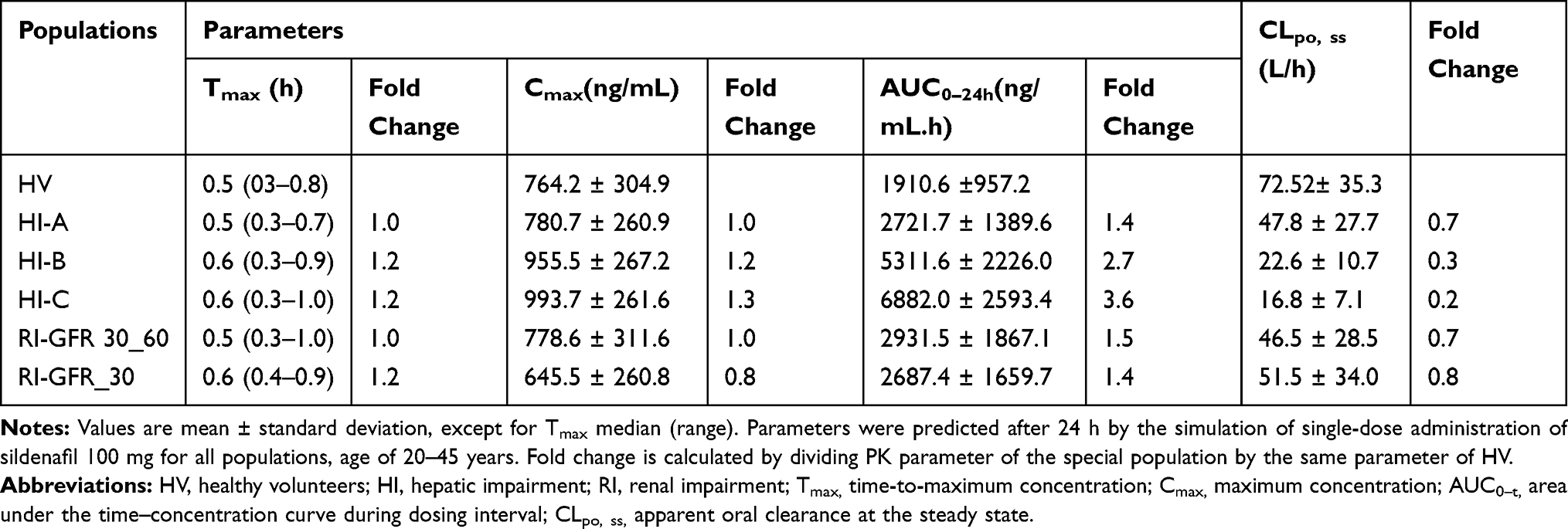 |
Table 5 Comparison of Sildenafil Pharmacokinetic Parameters for Young Adults According to Different Conditions |
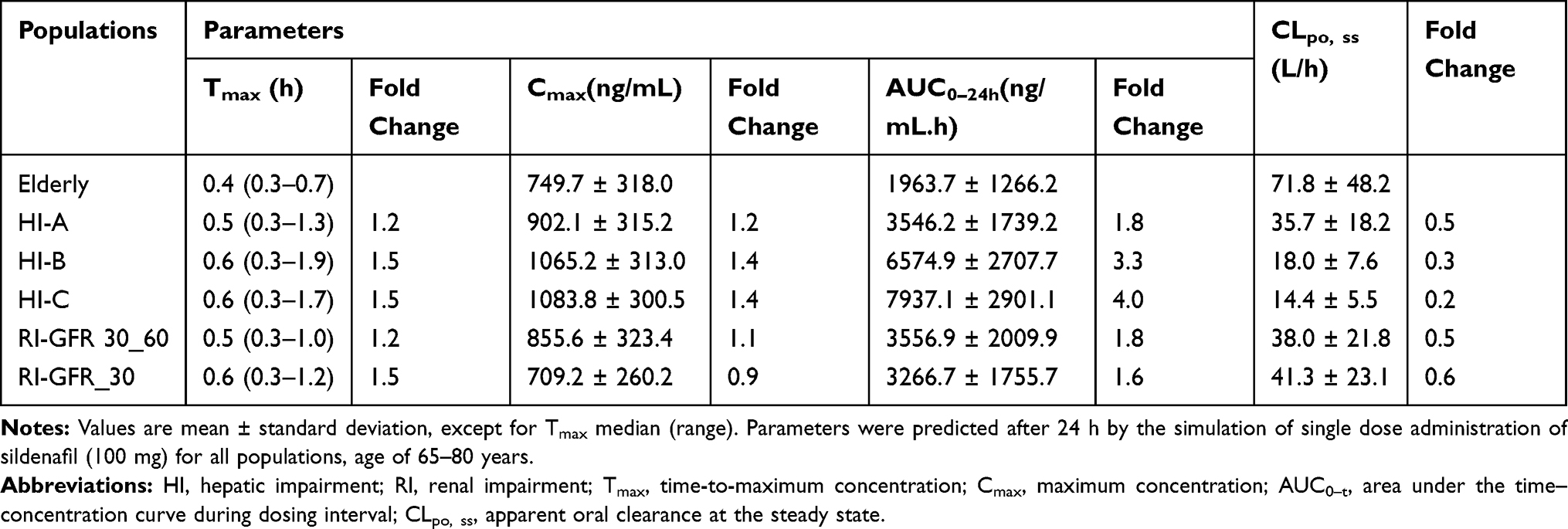 |
Table 6 Comparison of Sildenafil Pharmacokinetic Parameters for Elderly According to Different Conditions |
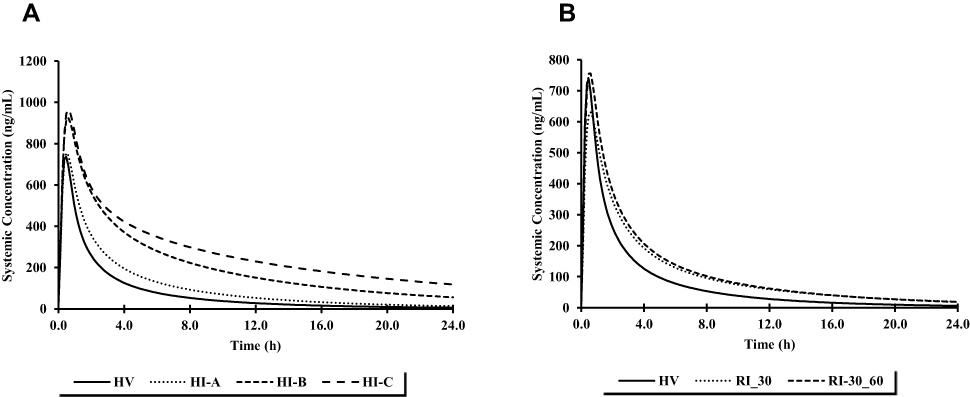 |
Figure 3 Comparison of simulated mean clozapine sildenafil for young adults according to (A) hepatic function and (B) renal function after single-dose administration of sildenafil 100 mg. |
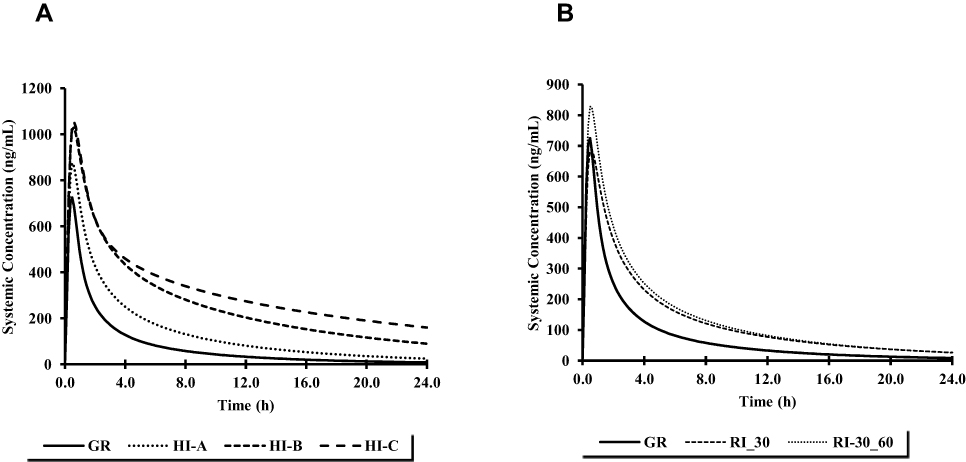 |
Figure 4 Comparison of simulated mean sildenafil concentrations for elderly population according to (A) hepatic function and (B) renal function after single-dose administration of sildenafil 100 mg. |
Although Clpo, ss extremely dropped in HI patients, reaching a maximum reduction of 80% in elderly HI-C patients, Cmax was slightly raised in HI young and elderly patients, reaching a highest increase by 1.4 folds in elderly patients with HI-B and HI-C. On the other hand, AUC0-t was profoundly increased by ≈ 3 and 4 folds in HI-B and HI-C patients, respectively, regardless of age.
Regarding both classes of RI patients, Clpo, ss was reduced only to 30% and 45% of the normal condition in young and elderly patients, respectively. Cmax was not greatly altered in the two classes of RI patients, regardless of age. AUC0-t was elevated by ≈ 1.5 and 1.7 folds in young and elderly patients, respectively.
The predicted PK parameters of sildenafil in HI and RI populations were compared to the observed results obtained from a clinical study by Muirhead et al.27 In this clinical study, 12 patients were enrolled, where 7 were Child–Pugh A and 5 were Child–Pugh B. Cmax and AUC were elevated by 1.4 and 1.8 fold, respectively. Upon calculating the average predicted PK parameters of HI-A and HI-B young adults, it was revealed that Cmax was increased by 1.1 fold, while AUC was raised by 2 folds.
Regarding the observed PK parameters in patients with moderate RI, Cmax and AUC were increased by 1.1 and 0.8 fold, respectively. These results are comparable to the predicted results of RI-GFR-30_60 population, where Cmax did not change in young patients with RI-GFR-30_60. On the other hand, the observed Cmax and AUC in patients with severe RI were raised by approximately 1.8 and 0.5 fold, respectively. However, the predicted Cmax and AUC of young patients with RI-GFR_30 were only increased by 0.8 and 1.4 fold, respectively.
A drug–drug interaction was simulated employing the co-administration of clozapine with sildenafil in young and elderly populations to ensure the safety of concomitant use of both drugs. The predicted PK results revealed no interaction between clozapine and sildenafil (Data not shown). The lack of interaction between the two drugs was expected as neither clozapine nor sildenafil are inhibitors or inducers of CYP isoforms. Although sildenafil significantly inhibits ABCB1-mediated drug efflux,22 the relationship of clozapine to the ABCB1 encoded transporter (also known as PgP) is conflicting in the literature. However, although ABCB1 variants are associated with differential PK or outcomes,29,30 other articles report clozapine is not substrate or effective inhibitor of ABCB1.31
These results are confirmed by a clinical study by Gopalakrishnan et al,32 where they assessed the effectiveness and tolerability of sildenafil in the treatment of erectile dysfunction caused by antipsychotics. Sildenafil was sufficiently tolerated with no discontinuations due to adverse effects. The majority of these negative events were mild or moderate; thus, it was assumed that sildenafil can be safely combined with clozapine.
Discussion
In this study, the PK profiles of HV were adequately described as adopting a PBPK model. Additionally, studies were simulated to analyze the PK profiles in young and elderly populations with HI and RI. Due to the difficulty of gathering clinical PK data from diseased populations, such simulations could be of great benefit to predict any changes in systemic exposure.33 In the current simulation, the pre-existed PBPK models of clozapine and sildenafil were modified from a first-order model to ADAM and M-ADAM models. The PK parameters predicted from the ADAM and M-ADAM models infer that these models are more conclusive for clozapine and sildenafil, respectively.
In comparison to the first-order absorption model, the ADAM model enhances the simulation performance by employing physiological factors that have a significant effect on absorption including gastric emptying time, intestinal and colonic transit times, enterohepatic recirculation, gastric intestinal tract surface area, region-specific gut wall permeability, enterocytic blood flow and region-specific luminal pH.34 The approach that the intestinal and chronic renal diseases affect each other appeared only lately. The complication is multifaceted and bidirectional. On one hand, the intestinal microbiota impacts uremic retention solute production, leading to the production of protein-bound uremic toxins with strong biological influence like progression of kidney failure and vascular damage. On the other hand, the uremicconditioninfluences the intestinal microbiota, the generation of uremic retention solutes and induces disturbances in the protective epithelial barrier of the intestine and the translocation of intestinal microbiota into the body.35
Also, mucosal abnormalities in patients with liver cirrhosis are now well documented and include mucosal inflammatory-like abnormalities (oedema, erythema, granularity and friability), as well as, vascular lesions (cherry red spots, telangiectasias or angiodysplasia-like lesions and varices).28,36,37
Therapy with clozapine in aged patients demands an accurate geriatric assessment, together with poly-treatment, comorbidity and the understanding of drug–drug interactions and age-related adjustment in PKs and pharmacodynamics.38 These changes are responsible for the increase in adverse drug reactions in the elderly. Ageing is known to cause several changes in drug absorption, distribution, biotransformation and elimination.39,40 As for sildenafil, Muirhead et al observed that the drug plasma concentration was increased in elderly population.27
The simulation using the pre-existing population of Geriatrics indicated a 30–40% decrease in the GFR for the elderly compared to the normal value of 120 mL/min/1.73 m2. Clozapine and its metabolites are highly protein-bound in serum, where clozapine is largely reabsorbed in the tubule after glomerular filtration.9 Sildenafil and its active metabolite are both highly bound to plasma proteins (≈96%). Sildenafil is excreted as metabolites mostly in the feces (≈80% of administered oral dose) and to a minor extent in the urine (≈13% of the administered oral dose).17 This explains the minor impact on the predicted PK parameters of clozapine and sildenafil in elderly population.
It is widely known that HI leads to not only deficiency in CYP enzymes, but also, alteration in the hepatic structure, resulting in the formation of blood shunting to bypass the liver with an increase in blood flow through the hepatic artery.41 Simultaneously, liver cirrhosis affects the gastrointestinal absorption by congestion and decrease in the blood flow in the intestinal mucosa.42
As clozapine is predominantly metabolized by CYP 450 enzymes, elevated systemic exposure is expected in patients with HI, as was shown by the simulation results. Liver cirrhosis has a differential effect on individual hepatic CYP enzymes with a marked reduction in most enzymes but specifically CYPs 1A2, 2D6 2C19, and 3A4; enzyme expression is reduced as disease severity increases.43 Liver failure can alter a few elements of medication PK, including absorption, distribution and elimination.44 Even though observed elevations in liver function tests in patients receiving clozapine are often temporary and show no symptoms, there are several reported incidences of clozapine-induced hepatotoxicity, liver injury, engagement of several organs, and even severe liver failure proceeding moderate clozapine doses.45 Nonetheless, there are no reported clinical trials to predict the PK profile of clozapine in HI patients with which a comparison with the simulated results could be performed.46 However, the PBPK modeling and simulation approach enabled the investigation of changes in clozapine PKs according to the severity of HI. The simulation results showed that the systemic exposure of clozapine was increased with HI, especially in young and elderly patients with HI-B and HI-C.
Several researchers have recommended that it is essential to check liver function tests before starting therapy with clozapine and re-examination every 6 months has been advised.47 Although the effective clozapine plasma levels remain debated, most researchers find that a therapeutic window of 350–600 ng/mL for clozapine plasma concentrations is associated with an increased probability of a good clinical response to the drug. Concentrations higher than 1000 ng/mL could increase the risk of seizures.48 The simulation results for Cmax were shown to be above 1000 ng/mL for young adults with HI-C and geriatrics with HI-B and HI-C.
Patients with hepatic dysfunction have a decreased clearance of sildenafil compared with normal subjects.27 These results are in accordance with the simulated PK parameters, where high systemic sildenafil exposure was predicted in patients with HI in both young and elderly populations.
RI also results in decreased plasma protein binding and reduction in drug metabolizing enzymes activity, especially CYP3A.49–52 This explains the reduction in clozapine CLpo, ss in young adults and elderly population with RI-GFR 30_60 and RI-GFR 30. Thus, the PKs of most drugs, including those that are mainly metabolized by CYP3A, should be evaluated in RI patients to provide appropriate dosing recommendations. Patients with severe renal impairment (creatinine clearance <30 mL/min) have a reduced clearance of sildenafil.27 These results are comparable to the simulated PKs of sildenafil in the elderly population suffering from RI-GFR_30, where a 0.6 fold decrease was predicted in CLpo, ss.
To conclude, this study acceptably characterized the PKs of clozapine and sildenafil in healthy adult population using the PBPK approach. Dose adjustment is required for clozapine and sildenafil when administered to young and elderly patients with moderate and severe HI or RI. PBPK modeling and simulation can be employed as a beneficial mechanism to study and investigate the PKs of populations integrating several disease conditions.
Author Contributions
Both authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors indicate that they have no conflicts of interest pertaining to the content of this manuscript.
References
1. Rowland M, Peck C, Tucker G. Physiologically-based pharmacokinetics in drug development and regulatory science. Annu Rev Pharmacol Toxicol. 2011;51(1):45–73. doi:10.1146/annurevpharmtox-010510-100540
2. Jones HM, Chen Y, Gibson C, et al. Physiologically based pharmacokinetic modeling in drug discovery and development: a pharmaceutical industry perspective. Clin Pharmacol Ther. 2015;97(3):247–262. doi:10.1002/cpt
3. Mcilwain ME, Harrison J, Wheeler AJ, Russell BR. Pharmacotherapy for treatment-resistant. Neuropsychiatr Dis Treat. 2011;7(1):139–149. doi:10.2147/NDT.S12769
4. Urichuk L, Prior T, Dursun S, Baker G. Metabolism of atypical antipsychotics: involvement of cytochrome P450 enzymes and relevance for drug-drug interactions. Curr Drug Metab. 2008;9(5):410–418. doi:10.2174/138920008784746373
5. Wagmann L, Meyer MR, Maurer HH. What is the contribution of human FMO3 in the N-oxygenation of selected therapeutic drugs and drugs of abuse? Toxicol Lett. 2016;258:55–70. doi:10.1016/j.toxlet.2016.06.013
6. Pirmohamed M, Williams D, Madden S, Templeton E, Park BK. Metabolism and bioactivation of clozapine by human liver in vitro. J Pharmacol Exp Ther. 1995;272(3):984–990.
7. Zhang WV, D’Esposito F, Edwards RJ, Ramzan I, Murray M. Interindividual variation in relative CYP1A2/3A4 phenotype influences susceptibility of clozapine oxidation to cytochrome P450-specific inhibition in human hepatic microsomes. Drug Metab Dispos. 2008;36(12):2547–2555. doi:10.1124/dmd.108.023671
8. Akamine Y, Sugawara-Kikuchi Y, Uno T, Shimizu T, Miura M. Quantification of the steady-state plasma concentrations of clozapine and N-desmethylclozapine in Japanese patients with schizophrenia using a novel HPLC method and the effects of CYPs and ABC transporters polymorphisms. Ann Clin Biochem. 2017;54(6):677–685. doi:10.1177/0004563216686377
9. Schaber G, Stevens I, Gaertner HJ, Dietz K, Breyer-Pfaff U. Pharmacokinetics of clozapine and its metabolites in psychiatric patients: plasma protein binding and renal clearance. Br J Clin Pharmacol. 1998;46(5):453–459. doi:10.1046/j.1365-2125.1998.00822.x
10. Zai CC, Zai GC, Tiwari AK, et al. Association study of GABRG2 polymorphisms with suicidal behavior in schizophrenia patients with alcohol use disorder second-Generation Antipsychotics and Extrapyramidal Adverse Effects. Neuropsychobiology. 2014;69(3):154–158. doi:10.1159/000358839
11. De Berardis D, Rapini G, Olivieri L, et al. Safety of antipsychotics for the treatment of schizophrenia: a focus on the adverse effects of clozapine. Ther Adv Drug Saf. 2018;9(5):237–256. doi:10.1177/2042098618756261
12. Sultan RS, Olfson M, Correll CU, Duncan EJ. Evaluating the effect of the changes in FDA guidelines for clozapine monitoring. J Clin Psychiatry. 2017;78(8):e933–e939. doi:10.4088/JCP.16m11152
13. Smith SM, O’Keane V, Murray R. Sexual dysfunction in patients taking conventional antipsychotic medication. Br J Psychiatry. 2002;181(1):49–55. doi:10.1192/bjp.181.1.49
14. Park YW, Kim Y, Lee JH. Antipsychotic-induced sexual dysfunction and its management. World J Men's Health. 2013;30(3):153–159. doi:10.5534/wjmh.2012.30.3.153
15. Kelly DL, Conley RR. Sexuality and schizophrenia: a review. Schizophr Bull. 2004;30(4):767–779. doi:10.1093/oxfordjournals.schbul.a007130
16. Muirhead GJ, Rance DJ, Walker DK, Wastall P. Comparative human pharmacokinetics and metabolism of single-dose oral and intravenous sildenafil citrate. Br J Clin Pharmacol. 2002;53(Suppl 1):13S–20S. doi:10.1046/j.06-5251.2001.00028.x
17. Cheitlin MD, Hutter AM, Brindis RG, et al. Use of sildenafil (Viagra) in patients with cardiovascular disease. Circulation. 1999;99(1):168–177. doi:10.1161/01.CIR.99.1.168
18. Le Couteur DG, McLean AJ. The aging liver: drug clearance and an oxygen diffusion barrier hypothesis. Clin Pharmacokinet. 1998;34(5):359–373. doi:10.2165/00003088-199834050-00003
19. Yuan R, Venitz J. Effect of chronic renal failure on the disposition of highly hepatically metabolized drugs. Int J Clin Pharmacol Ther. 2000;38(5):245–253. doi:10.5414/cpp38245
20. Montamat SC, Cusack BJ, Yestal RE. Management of drug therapy in the elderly. N Engl J Med. 1989;321:303–309. doi:10.1056/NEJM198908033210507
21. Darwich AS, Neuhoff S, Jamei M, Rostami-Hodjegan A. Interplay of metabolism and transport in determining oral drug absorption and gut wall metabolism: a simulation assessment using the Advanced Dissolution, Absorption, Metabolism (ADAM) model. Curr Drug Metab. 2011;11(9):716–729. doi:10.2174/138920010794328913
22. Shi Z, Tiwari AK, Shukla S, et al. Sildenafil reverses ABCB1- and ABCG2-mediated chemotherapeutic drug resistance. Cancer Res. 2011;71(8):3029–3041. doi:10.1158/0008-5472.CAN-10-3820
23. Shebley M, Fu W, Badri P, Bow DAJ, Fischer V. Physiologically based pharmacokinetic modeling suggests limited drug–drug interaction between clopidogrel and dasabuvir. Clin Pharmacol Ther. 2017;102(4):679–687. doi:10.1002/cpt.689
24. Golden G, Honigfeld G. Bioequivalence of clozapine orally disintegrating 100-mg tablets compared with clozapine solid oral 100-mg tablets after multiple doses in patients with schizophrenia. Clin Drug Investig. 2008;28(4):231–239. doi:10.2165/00044011-200828040-00004
25. Radicioni M, Castiglioni C, Giori A, Cupone I, Frangione V, Rovati S. Bioequivalence study of a new sildenafil 100 mg orodispersible film compared to the conventional film-coated 100 mg tablet administered to healthy male volunteers. Drug Des Devel Ther. 2017;11:1183–1192. doi:10.2147/DDDT.S124034
26. Rowland Yeo K, Aarabi M, Jamei M, Rostami-Hodjegan A. Modeling and predicting drug pharmacokinetics in patients with renal impairment. Expert Rev Clin Pharmacol. 2011;4(2):261–274. doi:10.1586/ecp.10.143
27. Muirhead GJ, Wilner K, Colburn W, Haug-Pihale G, Rouviex B. The effects of age and renal and hepatic impairment on the pharmacokinetics of sildenafil. Br J Clin Pharmacol. 2002;53:21S–30S. doi:10.1046/j.0306-5251.2001.00029.x
28. Johnson TN, Boussery K, Rowland-Yeo K, Tucker GT, Rostami-Hodjegan A. A semi-mechanistic model to predict the effects of liver cirrhosis on drug clearance. Clin Pharmacokinet. 2010;49(3):189–206. doi:10.2165/11318160-000000000-00000
29. JaquenoudSirot E, Knezevic B, Morena GP, et al. ABCB1 and cytochrome P450 polymorphisms: clinical pharmacogenetics of clozapine. J Clin Psycho pharmacol. 2009;29(4):319–326. doi:10.1097/JCP.0b013e3181acc372
30. Piatkov I, Caetano D, Assur Y, et al. ABCB1 and ABCC1 single-nucleotide polymorphisms in patients treated with clozapine. Pharmgenomics Pers Med. 2017;10:235–242. doi:10.2147/PGPM.S142314
31. Moons T, De Roo M, Claes S, Dom G. Relationship between P-glycoprotein and second-generation antipsychotics. Pharmacogenomics. 2011;12(8):1193–1211. doi:10.2217/pgs.11.55
32. Gopalakrishnan R, Jacob KS, Kuruvilla A, Vasantharaj B, John JK. Sildenafil in the treatment of antipsychotic-induced erectile dysfunction: a randomized, double-blind, placebo-controlled, flexible-dose, two-way crossover trial. Am J Psychiatry. 2006;163(3):494–499. doi:10.1176/appi.ajp.163.3.494
33. Rhee SJ, Chung H, Yi S, Yu KS, Chung JY. Physiologically based pharmacokinetic modelling and prediction of metformin pharmacokinetics in renal/hepatic-impaired young adults and elderly populations. Eur J Drug Metab Pharmacokinet. 2017;42(6):973–980. doi:10.1007/s13318-017-0418-x
34. Sinhaa VK, Snoeysb J, Van Osselaerc N, Van Peera A, Mackied C, Healde D. From preclinical to human - prediction of oral absorption and drug-drug interaction potential using physiologically based pharmacokinetic (PBPK) modeling approach in an industrial setting: a workflow by using case example. Biopharm Drug Dispos. 2012;33(2):111–121. doi:10.1002/bdd.1782
35. Vanholder R, Glorieux G. The intestine and the kidneys: a bad marriage can be hazardous. Clin Kidney J. 2015;8(2):168–179. doi:10.1093/ckj/sfv004
36. De Palma GD, Rega M, Masone S, et al. Mucosal abnormalities of the small bowel in patients with cirrhosis and portal hypertension: a capsule endoscopy study. Gastrointest Endosc. 2005;62(4):529–534. doi:10.1016/s0016-5107(05)01588-9
37. Norman K, Pirlich M. Gastrointestinal tract in liver disease: which organ is sick? Curr Opin Clin Nutr Metab Care. 2008;11(5):613–619. doi:10.1097/MCO.0b013e32830a70bc
38. Leysen JE, Janssen PMF, Heylen L, et al. Receptor interactions of new antipsychotics: relation to pharmacodynamic and clinical effects. Int J Psychiatry Clin Pract. 1998;2:S3–S17.
39. Gareri P, Falconi U, De Fazio P, De Sarro G. Conventional and new antidepressant drugs in the elderly. Prog Neurobiol. 2000;61(4):353–396. doi:10.1016/s0301-0082(99)00050-7
40. Gareri P, De Fazio P, Russo E, Marigliano N, De Fazio S, De Sarro G. The safety of clozapine in the elderly. Expert Opin Drug Saf. 2008;7(5):525–538. doi:10.1517/14740338.7.5.525
41. Elbekai R, Korashy H, El-Kadi A. The effect of liver cirrhosis on the regulation and expression of drug metabolizing enzymes. Curr Drug Metab. 2005;5(2):157–167. doi:10.2174/1389200043489054
42. Verbeeck RK, Musuamba FT. Pharmacokinetics and dosage adjustment in patients with renal dysfunction. Eur J Clin Pharmacol. 2009;65(8):757–773. doi:10.1007/s00228-009-0678-8
43. Frye RF, Zgheib NK, Matzke GR, et al. Liver disease selectively modulates cytochrome P450-mediated metabolism. Clin Pharmacol Ther. 2006;80(3):235–245. doi:10.1016/j.clpt.2006.05.006
44. Le Couteur DG, Fraser R, Hilmer S, Rivory LP, McLean AJ. The hepatic sinusoid in aging and cirrhosis: effects on hepatic substrate disposition and drug clearance. Clin Pharmacokinet. 2005;44(2):187–200. doi:10.2165/00003088-200544020-00004
45. Wu Chou AI, Lu ML, Shen WW. Hepatotoxicity induced by clozapine: a case report and review of literature. Neuropsychiatr Dis Treat. 2014;10:1585–1587. doi:10.2147/NDT.S67654
46. Telles-Correia D, Barbosa A, Cortez-Pinto H, Campos C, Rocha NBF, Machado S. Psychotropic drugs and liver disease: a critical review of pharmacokinetics and liver toxicity. World J Gastrointest Pharmacol Ther. 2017;8(1):26–38. doi:10.4292/wjgpt.v8.i1.26
47. Ortiz-Orendain J, Castiello-de Obeso S, Colunga-Lozano LE, Hu Y, Maayan N, Adams CE. Antipsychotic combinations for schizophrenia. Cochrane Database Syst Rev. 2017;6(6):CD009005. doi:10.1002/14651858.CD009005.pub2
48. Hiemke C, Baumann P, Bergemann N, et al. AGNP consensus guidelines for therapeutic drug monitoring in psychiatry: update 2011. Pharmaco Psychiatry. 2011;44(6):195–235. doi:10.1055/s-0031-1286287
49. Sun H, Frassetto L, Benet LZ. Effects of renal failure on drug transport and metabolism. Pharmacol Ther. 2006;109(1–2):1–11. doi:10.1016/j.pharmthera.2005.05.010
50. Dreisbach AW, Lertora JJ. The effect of chronic renal failure on drug metabolism and transport. Expert Opin Drug Metab Toxicol. 2008;4(8):1065–1074. doi:10.1517/17425255.4.8.1065
51. Zhang L, Xu N, Xiao S, et al. Regulatory perspectives on designing pharmacokinetic studies and optimizing labeling recommendations for patients with chronic kidney disease. J Clin Pharmacol. 2012;52(1Suppl):79S–90S. doi:10.1177/0091270011415410
52. Prueksaritanont T, Chu X, Gibson C, et al. Drug-drug interaction studies: regulatory guidance and an industry perspective. AAPS J. 2013;15(3):629–645. doi:10.1208/s12248-013-9470-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.