")
Back to Journals » Drug Design, Development and Therapy » Volume 17
The Effect of Intranasal Dexmedetomidine on Emergence Delirium Prevention in Pediatric Ambulatory Dental Rehabilitation Under General Anesthesia: A Randomized Clinical Trial
Authors He H , Cui Q, Chen H, Huang X, Wang S, Yu T , Feng J, Shao Y
Received 26 August 2023
Accepted for publication 29 October 2023
Published 30 November 2023 Volume 2023:17 Pages 3563—3570
DOI https://doi.org/10.2147/DDDT.S427291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Huan He,1 Qichun Cui,1 Hengheng Chen,2,* Xiao Huang,3,* Shuai Wang,3,* Tian Yu,2,* Jinqiu Feng,3 Yun Shao1
1Department of Anesthesiology, Shanghai Stomatological Hospital & School of Stomatology, Fudan University, Shanghai, 200002, People’s Republic of China; 2Department of Preventive Dentistry, Shanghai Stomatological Hospital & School of Stomatology, Fudan University, Shanghai, 200002, People’s Republic of China; 3Department of Pediatric Dentistry, Shanghai Stomatological Hospital & School of Stomatology, Fudan University, Shanghai, 200002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yun Shao, Department of Anesthesiology, Shanghai Stomatological Hospital & School of Stomatology, Fudan University, No. 356 East Beijing Road, Shanghai, 200002, People’s Republic of China, Tel/Fax +86 2163295852, Email [email protected] Jinqiu Feng, Department of Pediatric Dentistry, Shanghai Stomatological Hospital & School of Stomatology, Fudan University, No 356 East Beijing Road, Shanghai, 200002, People’s Republic of China, Tel/Fax +86 2163601149, Email [email protected]
Purpose: Sevoflurane is the preferred anesthetic agent for induction and maintenance of ambulatory surgery due to its property of fast onset and recovery. However, it has been recognized as one of the major contributors of emergence delirium. The aim of this study was to evaluate the preventive effect of intranasal dexmedetomidine on the occurrence of emergence delirium in pediatric patients under general anesthesia with sevoflurane.
Patients and Methods: Ninety pediatric patients undergoing dental rehabilitation under sevoflurane anesthesia were enrolled in this study. The patients were divided into three groups (n=30 each in the 2 μg/kg dexmedetomidine, 1 μg/kg dexmedetomidine, and control with saline groups). The same volume (0.02mL/kg) of the mixed solution was dropped into the nasal cavity of the children 30 minutes before surgery. We used the Pediatric Anesthesia Emergence Delirium Scale (PAED) to assess the level and incidence of delirium in the post-anesthesia care unit.
Results: Compared with the control group, prophylactic use of different dosages of intranasal dexmedetomidine significantly reduces the incidence of ED and severe ED in PACU (P< 0.001). Intranasal administration of 2 μg/kg dexmedetomidine was associated with a better acceptance of mask induction and a better tolerance of separation with parents.
Conclusion: Both 2 μg/kg and 1 μg/kg intranasal dexmedetomidine can achieve ED preventive effects in PACU in dental rehabilitation under general anesthesia. A dosage of 2 μg/kg is more effective in preventing severe ED and providing better mask acceptance.
Keywords: intranasal dexmedetomidine, emergence delirium, sevoflurane anesthesia, pediatric patients, dental rehabilitation
Introduction
Emergence delirium (ED) is a common complication after pediatric anesthesia, which may cause injury to the child, requiring extra nursing care, and may delay patient discharge from hospital.1 The incidence of ED ranges from 10% to 50% but may be as high as 80%.1 Volatile anesthetics are among the proposed contributors to ED, and sevoflurane has relatively greater propensity.2,3 Although ED can be reversed in a short period of time after recovery from general anesthesia, additional nursing care and analgesics may be needed. ED is also associated with prolonged abnormal neurobehavioral performance after sevoflurane anesthesia.4
Children’s fear about dental treatment may lead to behaviour management problems for the dentist, which can be a barrier to the successful dental treatment.5 Despite reports of an overall decrease in caries, severe decay is still a prevalent disease in early childhood, and thus the demand for treatment under general anesthesia increases.6 Since a majority of this population cannot tolerate awake treatment in outpatient environment, general anesthesia is an important option for successful dental treatment.7
Sevoflurane is a volatile anesthetic widely used for induction and maintenance of ambulatory anesthesia because of its property of fast onset and recovery.8 Dexmedetomidine is a selective α2-adrenergic agonist, which is widely used in perioperative sedation. It has pharmacologic properties including greater ability to induce arousal, anti-inflammatory and analgesic actions, lack of respiratory suppression, and improved sleep.9 Intranasal dexmedetomidine can provide safe and satisfying sedation at parent separation. Previous studies of preoperative sedation in pediatric dental rehabilitation under general anesthesia are few.10,11 In the present study, we aim to evaluate the preoperative use of two different doses of intranasal dexmedetomidine in the prevention of ED in children undergoing dental rehabilitation. The incidence of ED and severe ED in postanesthesia care unit (PACU) was considered as the primary outcome and MAS score and postoperative pain, as the second outcomes.
Materials and Methods
Study Design, Ethics Approval, and Consent to Participate
This research is an investigator-initiated, double-blind trial with parallel design and superiority outcomes. The protocol of the study was approved by the Ethics Committee of Shanghai Stomatological Hospital, Fudan University. Patients scheduled for dental rehabilitation under general anesthesia were enrolled. The trial was registered at chictr.org.cn (ChiCTR2100042575) before the first patient was enrolled. There were no substantive changes to the protocol after initiation of patient enrolment. Written informed consent was obtained from one of the legal guardians of the participants at outpatient clinics or during preoperative visits before surgery. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Enrollment Criteria
From February 2021 to April 2022, 92 children scheduled for full mouth dental rehabilitation under general anesthesia in ambulatory setting were chosen as the study subject. The children who need dental treatment under general anesthesia are determined by pediatric dentists and are arranged to undergo preoperative assessment at an anesthesia evaluation clinic. Patients undergoing dental treatment with ASA status I or II under general anesthesia were included in this study. All patients were between 3 and 7 years of age and were excluded from the study if they met any of the following criteria: congenital organic diseases, growth retardation, liver and kidney dysfunction, attention deficit hyperactivity disorder and autism, allergic to dexmedetomidine, and refusal from the parents.
Randomization and Blinding
In total, 90 children were randomly allocated (1:1:1 ratio) into three groups according to a computer-generated table: Group D2 to receive 2 μg kg−1 intranasal dexmedetomidine, Group D1 to receive 1 μg kg−1 intranasal dexmedetomidine, and Group C to receive intranasal saline.
All children included were fasted for 8h and deprived of clear fluids for 2h before surgery. The child entered the anesthesia preparation room 30 minutes before induction of anesthesia accompanied by one of the parents. A 1mL tuberculin syringe containing 100 μg or 50 μg dexmedetomidine was prepared for Group D2 or Group D1. A 1mL tuberculin syringe containing 0.9% saline was prepared for Group C. All the drugs for each subgroup were diluted with 0.9% saline to a final volume of 1mL. Patients in Group D2 and Group D1 received intranasal drop of dexmedetomidine, respectively, at the concentration of 100 μg.mL−1 and 50 μg.mL−1. Patients in Group C received intranasal drop of saline. A numbered sealed envelope was used for group allocation. Dexmedetomidine or saline was prepared by an anesthetic nurse who was not involved in data collection or patient’s care. All parents, attending anesthesiologists, caring nurses and dentists involved in the study were blinded to the group assignments. The study drug was administered through two nostrils by one anesthesiologist 30 minutes prior to being transferred to the operating room. A total volume of 0.02mL/kg drug mixture is used regardless of whether drugs or normal saline is used. Vital signs including heart rate and SpO2 were recorded by a portable pulse oxygen saturation monitor (model: YX303, Jiangsu Yuyue Medical Equipment & Supply Co., Ltd), and respiration rate was counted by the anesthesiologist. During the stay in the anesthesia preparation room, scales including Ramsay sedation score (RSS) and pediatric separation anxiety scale (PSAS) were evaluated by the same anesthesiologist.
Anesthesia and Perioperative Care
After patients entered the operation room, electrocardiography, noninvasive arterial blood pressure (BP), pulse oximetry, and bispectral index (BIS, America, Covidien IIc Co.) were monitored. Anesthesia induction was performed using 8% sevoflurane in oxygen (8L·min−1) via a face mask. During the inhalation induction, the mask acceptance scale (MAS) was evaluated. Propofol (1.5 mg.kg−1), rocuronium (0.6 mg.kg−1) and sufentanil (0.3 μg.kg−1) were administered after intravenous line placement was achieved. Ringer’s acetate (RA) was used as balanced crystalloid solutions and was infused at a rate of 5–7 mL.kg−1h−1. Nasal fiberoptic intubation technique was used in all the patients to secure safe and effective airway control. Dentists may use regional anesthetic (Articaine hydrochloride and epinephrine tartrate injection) on their own decision to minimize bleeding of gingiva. The baseline inspiratory gas was a mixture of 60/40% oxygen/air. Anesthesia was maintained with sevoflurane (2.5–3%) and remifentanil (0.05 μg/kg/min). The BIS values were maintained between 40 and 60 for appropriate anesthesia depth. The patient’s body temperature was monitored by an axillary temperature sensor probe and maintained between 35.5 °C and 37.0 °C.
Remifentanil infusion and sevoflurane inhalation were terminated when dentists finished their procedure. No extra analgesic or antagonist was given postoperatively. Extubation was done after confirming regular breathing with sufficient tidal volume (> 5 mL/kg) and purposeful movement.
After extubation, the patient was transferred to the post-anaesthetic care unit (PACU). Their ED and pain conditions were recorded by subjective scales including PAED,12 Watcha,13 and Flacc14 scales. The PAED scale containing five aspects of child behavior (eye contact, purposeful movement, evidence of awareness of surroundings, restlessness, and inconsolability). Ratings are summed to produce a total score ranging from 0 to 20; greater scores indicate greater severity. The Watcha scale has four levels (1: calm; 2: crying, but can be consoled; 3: crying, cannot be consoled; and 4: agitated and thrashing around). Face, Legs, Activity, Cry and Consolability (FLACC) pain scale was used to assess pain severity. All patients should be observed in the post-anesthesia care unit for at least 30 minutes after extubation.
Sample Size and Statistical Analysis
The sample size was estimated as a minimum of 25 subjects in each study group based on a previous study,15 at a significance level of 5% and a power of 80%. The final sample size in present study was determined to be 30 patients per group, when considered a 10% dropout rate.
Statistical analyses were performed using the IBM SPSS 26.0 (IBM Corp, Armonk, New York, USA) for Windows. Continuous variables with normal distribution were expressed as mean ±SD, nonparametric data were shown as median [range], and categorical data were reported as number (%). Normally distributed data were analyzed using analysis of variance (ANOVA) followed by a Bonferroni test. Nonparametric data were analyzed using the Kruskal–Wallis test. Categorical data, including the incidence of emergence agitation, were analyzed using the χ2 test or Fisher’s exact test as appropriate.
Results
A total of 92 children were initially enrolled in this study. Of these, 2 were excluded from analysis owing to infection of COVID-19 or severe laryngeal spasm. Complete data sets were available from the remaining 90 participants (30 in the 2 μg kg−1 dexmedetomidine group, 30 in the 1 μg kg−1 dexmedetomidine group, and 30 in the normal saline group). The details of patient recruitment are shown in the CONSORT flow diagram (Figure 1). Table 1 provides a detailed overview of participant demographics and general clinical history, which were similar among groups.
 |
Table 1 Patient Characteristics and Operation-Related Data for Each Group |
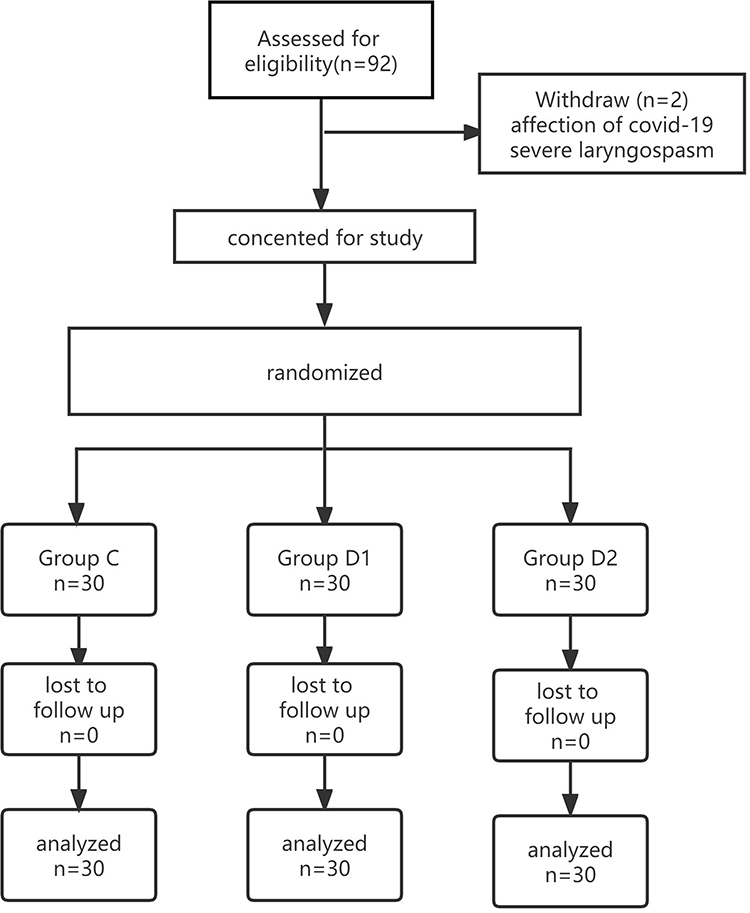 |
Figure 1 Consolidated Standards of Reporting Trials (CONSORT) flow diagram illustrating the patient progress through the study. |
Primary Outcome
Table 2 shows the recovery status in the post-anesthesia care unit. We used PEAD score ≥10 as the diagnostic threshold of ED.15,16 Patients with PEAD score ≥15 were diagnosed as severe ED.17 We found that compare with control group, prophylactic use of different dosages of intranasal dexmedetomidine significantly reduce the incidence of ED and severe ED in PACU (P<0.001, Table 2). Group comparison analyses indicate that Group D2 is more effective than Group D1 in preventing ED, but these two groups show no significance difference in preventing severe ED (Bonferroni correction for multiple comparisons, P>0.016667).
 |
Table 2 Recovery Status in the Post-Anesthesia Care Unit |
Secondary Outcomes
The peak FLACC pain score was 5.0 (IQR, 4.8–7.0) in Group C, 4.0 (IQR, 2.8–5.0) in Group D1 and 2.0 (IQR, 1.0–3.0) in Group D2 (P<0.001, Table 2).
Table 3 details the immediate status after entering the operating room. Intranasal administration of 2 μg/kg dexmedetomidine was associated with a better acceptance of mask induction (higher MAS score) and a better tolerance of separation with parents compared with normal saline. There was a significant difference in heart rate immediately after entering the operating room. There was no significant difference in Ramsay score between 3 groups.
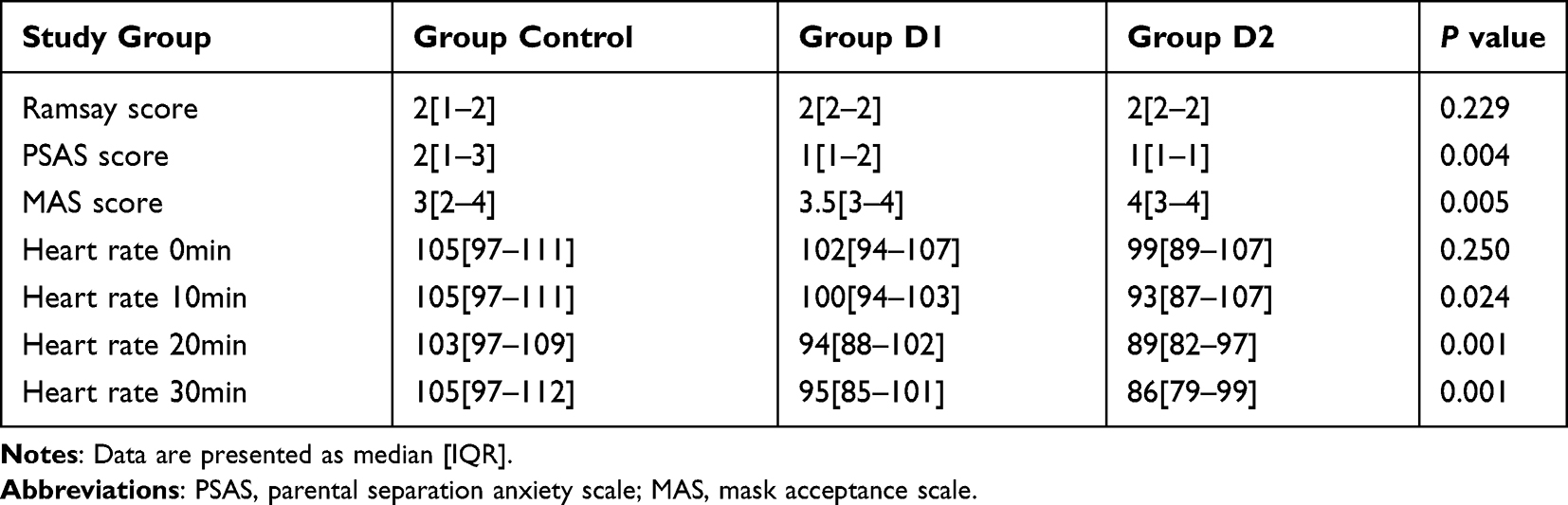 |
Table 3 Patients’ Status After Entering the Operating Room |
Discussion
The data in our study indicate that intranasal administration of 2 μg/kg or 1 μg/kg dexmedetomidine significantly decreases the incidence of emergence delirium under the threshold of both PAED score over 10 or 15 in post-anesthesia care unit. Besides, 2 μg/kg is a better intranasal dosage in preventing severe ED and providing better mask acceptance.
Previous studies on the role of intranasal dexmedetomidine in emergence delirium mainly focused on relatively short surgery like inguinal hernia repairs, tonsillectomy, adenoidectomy, and ophthalmic surgeries,18 while dental rehabilitation is relatively more time consuming compared with the previous surgeries. This protective effect of ED may be due to the residual effect of intranasal dexmedetomidine. Recent research about the pharmacokinetics of intranasal dexmedetomidine show that the dose at 2 μg/kg could achieve a preset therapeutic threshold of mild to moderate sedation that lasted for up to 2 hours.19 In pediatric patients requiring sedation for magnetic resonance imaging (MRI), 2–3 μg/kg intranasal dexmedetomidine was quickly absorbed, its peak concentration achieved in a median time of 37 minutes, and the maximal sedative effect observed 45 minutes after dosing.20 They also report the individual concentration–time curves after intranasal 2–3 μg/kg dosing of dexmedetomidine as nasal spray, indicating that at the time of 210min, most children had a plasma concentration of dexmedetomidine more than 0.2ng/mL. In our study, the majority of pediatric dental treatments can be completed within 210 minutes (Table 1), which is also consistent with clinical practice. We suggest that plasma concentration of dexmedetomidine is significant at the end of most dental rehabilitation surgeries, but whether or not this plasma concentration can prevent pediatric emergence delirium is unknown and needs proven.
Another possible explanation may be due to the relieved preoperative anxiety directly decreasing the rate of ED.21 We found that children who were premedicated with 2 μg/kg of intranasal dexmedetomidine had a significantly improved compliance rate during anesthesia inhalation induction than those premedicated with 1 μg/kg of intranasal dexmedetomidine or merely saline. Preoperative anxiety is one of the factors that may increase the likelihood of emergence delirium in pediatric patients. Many non-pharmacological methods have been applied to mitigate children’s preoperative anxiety—such as clown doctors, cartoon videos, virtual reality glasses, and comical information leaflets,22–24 some children may still resist the inhalation induction procedure, which may cause delirium at emergence. A study has shown that children with parental presence at induction of anesthesia (PPIA) have lower PAED score compared with control group.25 These research indicate that relieved preoperative anxiety may independently decrease the incidence of emergence delirium.
Dexmedetomidine was initially approved for intravenous use for up to 24 h in the adult intensive care unit population only and was additionally approved by the US Food and Drug Administration in 2003 for procedural sedation. Dexmedetomidine has appeared useful in multiple off-label applications such as pediatric sedation, intranasal, or buccal administration.26 Compared with intravenous administration of dexmedetomidine, intranasal administration has the advantages of rapid absorption, rapid onset, avoidance of liver first-pass effect, and can achieve a certain depth of sedation before setting up intravenous line. A previous study found that the ED95 of intranasal dexmedetomidine for preventing emergency agitation was 1.78 μg/kg in children aged 3 to 10 years.27 This may indicate that 2 μg/kg may be a better choice than 1 μg/kg for prophylactic usage. Meanwhile, dexmedetomidine has a moderate analgesic effect28 and has been proven to be effective in postoperative pain relief in pediatric maxillofacial surgery. It is consistent with the lower FLACC scores in the dexmedetomidine groups in our research results.
Children who require dental rehabilitation under general anesthesia are often difficult to cooperate within the outpatient setting. Due to health economic considerations, dentists and parents usually have higher expectations for fast anesthesia recovery and early discharge from hospital. Public acceptance of GA in pediatric dentistry has also evolved in recent years, with an increase in preference for its use in parents when compared with negative behavioral management.29 The American Dental Association recognizes dental treatment under GA as a viable option because of its low rates of post-operative complication.30 In order to maximize conservation of health care resources and aim for same-day discharge, rigorous preoperative examinations are often performed in the anesthesia clinic. ED is an important factor affecting the early postoperative outcome of patients, increasing unnecessary medical risks and labor costs. The promotion of ambulatory surgery make it possible for such children to be discharged early.
In 1996, Welborn and Lerman in United States reported emergence agitation with sevoflurane and compared to other volatile agents.31,32 Pediatric dental rehabilitation usually does not require deep muscle relaxation. Although sevoflurane anesthesia is reported to be a significant risk factor for postoperative delirium in children,21 we still use it as the main component for anesthesia induction and maintenance in this study, since it has the character of providing stable anesthesia, fast recovery, and low rate of intraoperative awareness. Common options of pediatric sedation include atomised intranasal midazolam or oral midazolam. However, some research show that intranasal midazolam used for premedication was associated with increased incidence of perioperative respiratory adverse events.33 Combined usage of pharmacological and non-pharmacological approaches may be more effective in ambulatory setting.34
There are a few limitations in our work. First, we found that the individual differences of the children themselves were obvious, which may be related to the education level of the parents. In this trial, we did not evaluate the education status of parents. Secondly, no further follow-up was performed after patients’ discharge to home; we could miss the information of long-term effect on the children’s behavior and cognition.
Conclusion
In conclusion, both 2 μg/kg and 1 μg/kg intranasal dexmedetomidine can achieve ED preventive effects in PACU. Dosage at 2 μg/kg is better in preventing severe ED and providing better mask acceptance.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author (Yun Shao) on reasonable request.
Acknowledgments
This study was supported by the Shanghai Health Commission Maternal and Child Health Special Fund (2020YJZX0218). We would like to thank anesthesiologists, pediatric dentists, pharmaceutical managers, and ward nurses at our institution, who supported the protocol development and implementation of this clinical trial.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vlajkovic GP, Sindjelic RP. Emergence delirium in children: many questions, few answers. Anesth Analg. 2007;104(1):84–91. doi:10.1213/01.ane.0000250914.91881.a8
2. Mason KP. Paediatric emergence delirium: a comprehensive review and interpretation of the literature. Br J Anaesth. 2017;118(3):335–343. doi:10.1093/bja/aew477
3. Kuratani N, Oi Y. Greater incidence of emergence agitation in children after sevoflurane anesthesia as compared with halothane: a meta-analysis of randomized controlled trials. Anesthesiology. 2008;109(2):225–232. doi:10.1097/ALN.0b013e31817f5c18
4. Shi M, Miao S, Gu T, et al. Dexmedetomidine for the prevention of emergence delirium and postoperative behavioral changes in pediatric patients with sevoflurane anesthesia: a double-blind, randomized trial. Drug Des Devel Ther. 2019;13:897–905. doi:10.2147/DDDT.S196075
5. Ashley PF, Chaudhary M, Lourenço-Matharu L. Sedation of children undergoing dental treatment. Cochrane Database Syst Rev. 2018;12(12):Cd003877. doi:10.1002/14651858.CD003877.pub5
6. F LIU, Yang K, Wang P, et al. Trends, characteristics, and success rates of treatment for severe early childhood caries under general anesthesia: a retrospective Study in Northwest China. J Clin Pediatr Dent. 2021;45(4):278–283. doi:10.17796/1053-4625-45.4.11
7. Campbell RL, Shetty NS, Shetty KS, et al. Pediatric dental surgery under general anesthesia: uncooperative children. Anesth Prog. 2018;65(4):225–230. doi:10.2344/anpr-65-03-04
8. Kim DH, Min KT, Kim EH, et al. Comparison of the effects of inhalational and total intravenous anesthesia on quality of recovery in patients undergoing endoscopic transsphenoidal pituitary surgery: a randomized controlled trial. Int J Med Sci. 2022;19(6):1056–1064. doi:10.7150/ijms.72758
9. Lewis K, Alshamsi F, Carayannopoulos KL, et al. Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials. Intensive Care Med. 2022;48(7):811–840. doi:10.1007/s00134-022-06712-2
10. Lu C, Zhang LM, Zhang Y, et al. Intranasal Dexmedetomidine as a Sedative Premedication for Patients Undergoing Suspension Laryngoscopy: a Randomized Double-Blind Study. PLoS One. 2016;11(5):e0154192. doi:10.1371/journal.pone.0154192
11. Wang L, Huang L, Zhang T, et al. Comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric dental patients under general anesthesia: a randomised clinical trial. Biomed Res Int. 2020;2020:5142913. doi:10.1155/2020/5142913
12. Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology. 2004;100(5):1138–1145. doi:10.1097/00000542-200405000-00015
13. Bajwa SA, Costi D, Cyna AM. A comparison of emergence delirium scales following general anesthesia in children. Paediatr Anaesth. 2010;20(8):704–711. doi:10.1111/j.1460-9592.2010.03328.x
14. Crellin DJ, Harrison D, Santamaria N, et al. Systematic review of the Face, Legs, Activity, Cry and Consolability scale for assessing pain in infants and children: is it reliable, valid, and feasible for use? Pain. 2015;156(11):2132–2151.
15. Lin Y, Chen Y, Huang J, et al. Efficacy of premedication with intranasal dexmedetomidine on inhalational induction and postoperative emergence agitation in pediatric undergoing cataract surgery with sevoflurane. J Clin Anesth. 2016;33:289–295. doi:10.1016/j.jclinane.2016.04.027
16. Jangra S, Ashok V, Sethi S, et al. Atomised intranasal dexmedetomidine versus oral melatonin in prevention of emergence delirium in children undergoing ophthalmic surgery with sevoflurane: a randomised double-blind study. Eur J Anaesthesiol. 2022;39(11):868–874.
17. Han X, Sun X, Liu X, et al. Single bolus dexmedetomidine versus propofol for treatment of pediatric emergence delirium following general anesthesia. Paediatr Anaesth. 2022;32(3):446–451. doi:10.1111/pan.14381
18. Wang HY, Chen TY, Li DJ, et al. Association of pharmacological prophylaxis with the risk of pediatric emergence delirium after sevoflurane anesthesia: an updated network meta-analysis. J Clin Anesth. 2021;75:110488.
19. Li BL, Guan YP, Yuen VM, et al. Population Pharmacokinetics of Intranasal Dexmedetomidine in Infants and Young Children. Anesthesiology. 2022;137(2):163–175. doi:10.1097/ALN.0000000000004258
20. Uusalo P, Guillaume S, Siren S, et al. Pharmacokinetics and Sedative Effects of Intranasal Dexmedetomidine in Ambulatory Pediatric Patients. Anesth Analg. 2020;130(4):949–957. doi:10.1213/ANE.0000000000004264
21. Dahmani S, Delivet H, Hilly J. Emergence delirium in children: an update. Curr Opin Anaesthesiol. 2014;27(3):309–315.
22. Lee J, Lee J, Lim H, et al. Cartoon distraction alleviates anxiety in children during induction of anesthesia. Anesth Analg. 2012;115(5):1168–1173. doi:10.1213/ANE.0b013e31824fb469
23. Ryu JH, Oh AY, Yoo HJ, et al. The effect of an immersive virtual reality tour of the operating theater on emergence delirium in children undergoing general anesthesia: a randomized controlled trial. Paediatr Anaesth. 2019;29(1):98–105. doi:10.1111/pan.13535
24. Lopes-Júnior LC, Lima RAG, Olson K, et al. Systematic review protocol examining the effectiveness of hospital clowns for symptom cluster management in paediatrics. BMJ Open. 2019;9(1):e026524. doi:10.1136/bmjopen-2018-026524
25. Yao J, Gong H, Zhao X, et al. Parental presence and intranasal dexmedetomidine for the prevention of anxiety during anesthesia induction in children undergoing tonsillectomy and/or adenoidectomy surgery: a randomized controlled trial. Front Pharmacol. 2022;13:1015357. doi:10.3389/fphar.2022.1015357
26. Weerink MAS, Struys M, Hannivoort LN, et al. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
27. Lei DX, Wu CJ, Wu ZY, et al. Efficacy of different doses of intranasal dexmedetomidine in preventing emergence agitation in children with inhalational anaesthesia: a prospective randomised trial. Eur J Anaesthesiol. 2022;39(11):858–867. doi:10.1097/EJA.0000000000001743
28. Chrysostomou C, Schmitt CG. Dexmedetomidine: sedation, analgesia and beyond. Expert Opin Drug Metab Toxicol. 2008;4(5):619–627. doi:10.1517/17425255.4.5.619
29. Eaton JJ, Mctigue DJ, Fields HW, et al. Attitudes of contemporary parents toward behavior management techniques used in pediatric dentistry. Pediatr Dent. 2005;27(2):107–113.
30. Clinical Affairs Committee-Behavior Management Subcommittee, American Academy of Pediatric Dentistry. Guideline on behavior guidance for the pediatric dental patient. Pediatr Dent. 2015;37(5):57–70.
31. Welborn LG, Hannallah RS, Norden JM, et al. Comparison of emergence and recovery characteristics of sevoflurane, desflurane, and halothane in pediatric ambulatory patients. Anesth Analg. 1996;83(5):917–920. doi:10.1213/00000539-199611000-00005
32. Lerman J, Davis PJ, Welborn LG, et al. Induction, recovery, and safety characteristics of sevoflurane in children undergoing ambulatory surgery. A comparison with halothane. Anesthesiology. 1996;84(6):1332–1340. doi:10.1097/00000542-199606000-00009
33. Shen F, Zhang Q, Xu Y, et al. Effect of intranasal dexmedetomidine or midazolam for premedication on the occurrence of respiratory adverse events in children undergoing tonsillectomy and adenoidectomy: a randomized clinical trial. JAMA Netw Open. 2022;5(8):e2225473. doi:10.1001/jamanetworkopen.2022.25473
34. Agbayani CG, Fortier MA, Kain ZN. Non-pharmacological methods of reducing perioperative anxiety in children. BJA Educ. 2020;20(12):424–430. doi:10.1016/j.bjae.2020.08.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.