Back to Journals » Psychology Research and Behavior Management » Volume 16
The Effect of Distress Tolerance Training on Problematic Internet Use and Psychological Wellbeing Among Faculty Nursing Students: A Randomized Control Trial
Authors El-Ashry AM ![]() , Hussein Ramadan Atta M, Alsenany SA, Farghaly Abdelaliem SM
, Hussein Ramadan Atta M, Alsenany SA, Farghaly Abdelaliem SM ![]() , Abdelwahab Khedr M
, Abdelwahab Khedr M ![]()
Received 27 May 2023
Accepted for publication 14 September 2023
Published 27 September 2023 Volume 2023:16 Pages 4015—4032
DOI https://doi.org/10.2147/PRBM.S423194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Mei-Chun Cheung
Ayman Mohamed El-Ashry,1 Mohamed Hussein Ramadan Atta,1 Samira Ahmed Alsenany,2 Sally Mohammed Farghaly Abdelaliem,3 Mahmoud Abdelwahab Khedr1
1Department of Psychiatric and Mental Health Nursing, Faculty of Nursing, Alexandria University, Alexandria, Egypt; 2Department of Community Health Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia; 3Department of Nursing Management and Education, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia
Correspondence: Sally Mohammed Farghaly Abdelaliem, Alyasmeen 153, Riyadh, 13326, Saudi Arabia, Tel +966550773686, Email [email protected]
Background: Distress tolerance skills have the potential to decrease problematic internet use and improve psychological wellbeing by cognitive reframing and goal-oriented problem-solving.
Aim: To assess the impact of distress tolerance training on problematic internet use and psychological wellbeing among university nursing students.
Methods: A randomized control trial used at the faculty of nursing using simple random sampling method. Tools: Distress Tolerance Scale, problematic internet use questionnaire, and Ryff psychological wellbeing scale. Data were collected from 60 nursing students over a period of 4 months.
Results: Distress tolerance level was increased among study group from 20.75± 14.29 to 72.75± 24.09 and sustained for 3 months to 62.44 ± 20.77 with statistically significant (f=7.090, p=0.006) and large effect size 0.75. When compared to no change among the control group as mean scare start by 22.35± 14.29 to 23.44± 16.09 and after 3 months to 21.75± 17.44 with insignificant difference (f=0.454, p=0.574). The mean score of problematic internet use shows highly statistically significant decrement in the study group between three period of time (pretest= 62.93, immediately post= 52.13, and post 3 months=52.70) with large effect size 0.78 (f=95.029, p< 0.001), in compared to control group that showed insignificant no changes (pretest= 64.0± 14.54, immediately post= 63.13± 12.87, and post 3 months=63.53± 11.36) with (f=1.012, p=0.332). In addition, the total mean score of psychological well-being was increased immediately after therapy and later for three months of therapy (pretest= 128.47, immediately post=148.77, and post 3 months= 153.60) with highly statistically significant (f=41.197, p< 0.001) with effect size 0.85, compared to no change among control group (pretest=125.97± 32.58, immediately post= 126.23± 30.86, and post 3 months=126.43± 29.78) with (f=0.208, p=0.698).
Conclusion: Efficacy of distress tolerance skills intervention had been proven in altering poor psychological wellbeing among students with problematic internet use. It helps students to learn new skills and use more adaptive strategies to overcome distress tolerance difficulties.
Keywords: distress tolerance training, problematic internet use, psychological wellbeing, nursing students
Introduction
Academic students use the internet for many reasons, such as companionship through social media interaction, distance learning, fast availability of academic content, online gaming, and ways of earning money, such as blogging and freelancing for these educational, recreational, and commercial reasons, the internet has been a crucial basic need for students.1–3 The diversity of maladaptive internet use by the student may lead to internet gaming disorder (IGD) and problematic internet use (PIU).1,4 Furthermore, the COVID-19 outbreak heightens usage and gaming, resulting in hazardous consequences, such as increased chances for internet and problematic gaming use.5
Problematic internet use has been identified as excessive and/or inappropriate internet use, which can lead to psychological, social, academic, and/or professional difficulties among student users.6 It is a maladaptive technology that could lead to internet gaming disorder.7 Müller et al examined the additional diagnostic validity of the main criteria of the Diagnostic Statistical Manual V (DSM-V) for internet gaming disorder are: losing track of time; withdrawal, or a bad mood when the computer is not available; tolerance or requiring more time and resources to meet internet demands; and adverse effects, such as lying, decreased productivity, and isolation.8 From these criteria Demetrovics et al developed a three-factor model of internet addiction. It assesses the extent of how risky internet usage can be through three factors: obsession, neglect, and control disorder.9
Psychological well-being is a multifaceted concept and one of the hallmarks of the unique liberal experience, resulting from environmental and educational encounters that both guide students in the search for meaning and direction in life and help them realize their true potential. Favorable conditions across all facets of life, such as physical and spiritual contentment and optimal performance, are identified as psychological well-being. When people are in psychological well-being, they can manage their lives and activities, and vice versa is true. Although psychological well-being is a positive concept, it includes both positive and negative emotions. These negative emotions are common in life, such as disappointment, grief, and frustration. The ability to tolerate and manage negative emotions is crucial for long-term psychological well-being.10,11 Ryff Carl has conceptualized psychological well-being as having six dimensions: autonomy, environmental mastery, positive relations with others, personal growth, purpose in life, and self-acceptance.10–14
Problematic internet use involves people spending too much time online and neglecting other everyday activities, which results in poor physical and psychological well-being. Fluctuations in the achievement level of students, disturbances in the quality of meals and sleep, social isolation, and engagement in hazardous activities due to substance addiction are related to PIU.1,15 Additionally, problematic internet students may exhibit mental health problems, such as anxiety, distress tolerance, poor impulse control, depression, psychosis, and suicide. Also, PIU has a worse effect on family and partner relations and on communication within the family. Consequently, PIU affects students’ autonomy, personal growth, relations with their surroundings, purpose in life, self-acceptance, and ability to control environmental factors6,11,16.Therefore, there are emerging needs to assess problematic internet use among students and alter this problem.5,17
The alteration of problematic internet use has emerged as a need for intervention for students with this problem to improve psychological well-being. Thus, several therapeutic approaches targeting students with problematic internet use are now available. These include cognitive behavior therapy, acceptance commitment therapy, mindfulness-based cognitive therapy, and dialectical behavior therapy.18–21
Dialectical behavior therapy (DBT) is one of the third-wave cognitive behavior therapies. It evolved from Marsha Linehan’s efforts to create a treatment for multi-problematic suicidal behavior. She assembled a package of evidence-based cognitive-behavioral interventions directly targeting suicidal behavior. Later, Linehan expanded DBT by reviewing the literature on efficacious psychosocial treatments for other disorders, such as borderline personality disorder, anxiety disorders, depression, and addiction.18–20
The DBT comprises four modules: mindfulness, distress tolerance, interpersonal effectiveness, and emotion regulation. It aims to develop distress tolerance skills and heighten the capacity to tolerate pain in difficult situations and not change it. Distress tolerance skills involve the ability to continue engaging in goal-directed behavior in the face of emotional, cognitive, or physical discomfort.20 Distress tolerance is a person’s ability to manage an emotional incident without feeling overwhelmed. Being able to handle difficult emotions can help a person more quickly return to a state of equilibrium when new stressors arise.22,23
Providers of distress tolerance believe in certain basic assumptions, namely, that “people are doing the best they can with what they know”, “they cannot fail in DBT”, and “they want to improve”. They also believe that people are fallible and need to learn new behaviors in skills therapy within the context of their daily lives. Finally, providers’ assumptions include that people may not have a cause for their problems, but they have to solve them anyway, and they need to work harder and be more motivated to change.20,22
Distress tolerance skills can improve coping, self-efficacy, and defensive skills in people with poor psychological well-being. Interventions focus on facilitating skill development with cognitive reframing, self-soothing, and goal-oriented problem-solving.20,24 In conclusion, psychiatric nurses have a crucial role in modifying the maladaptive consequences of internet use.18 They can notice patients’ emotions and their roles in problematic behavior and observe the emotional reactions of the patient. Nurses observe changes in facial expression, body language, voice tone, and other such indicators of emotional distress. They can help patients to accurately label emotional states, be aware, accept their emotions, and tolerate distress.11,25
When discussing the choice of Dialectical Behavior Therapy (DBT) as an intervention for nursing students with problematic internet use, it has specific advantages and unique features for students who may turn to the internet as a maladaptive coping mechanism. DBT equips the students with specialized distress tolerance skills, like radical acceptance, self-soothing, and diversion methods, which are especially important for assisting nursing students in navigating the challenges associated with their academic overload, stress, and emotional well-being.26,27
The research investigating the impact of distress tolerance training on problematic internet use and psychological wellbeing among faculty nursing students is a unique and significant contribution to the global field of problematic internet use. In summary, the novelty of this research lies in its focus on distress tolerance training, examination of problematic internet use, and inclusion of faculty nursing students.11,20 By highlighting the potential benefits of this intervention both globally and in Egypt, the study offers valuable insights and practical implications for researchers, educators, and mental health practitioners in the field of internet use and psychological wellbeing.
Psychiatric nurses can apply distress tolerance skills to interventions through constant attention to relationships between clients and therapists. Participants are encouraged to work out problems in their relationships with their therapists, and the therapists are encouraged to do the same with them. Participants are also asked to complete homework assignments. Moreover, interacting with others is taught in weekly lectures and reviewed in weekly homework assignments.20,25,28 The significance of this study lies in its contribution to the body of knowledge on distress tolerance training, its ramifications for interventions targeting problematic internet use among faculty nursing students, and its potential to guide mental health support services within academic settings. The results can direct future studies, assist medical practitioners in addressing internet-related problems, and support educators in fostering psychological well-being in nursing students. Therefore, it aimed to assess the impact of distress tolerance training on problematic internet use and psychological well-being among university nursing students.
Research Hypotheses
Faculty nursing students who engaged in distress tolerance training exhibit lower level of problematic internet use than the control group.
Faculty nursing students who engaged in distress tolerance training exhibit a higher level of psychological wellbeing than the control group.
Faculty nursing students who engaged in the training exhibit higher levels of distress tolerance than the control group.
Materials and Method
Materials
Research Design
A Consolidated Standards of Reporting Trials (CONSORT) guideline was followed by the study and using a randomized controlled trial (RCT) design. This study was conducted between the beginnings of September 2022 to January 2023. The study recruited a two-arm, single-blind approach, including pre-test, post-test, and follow-up measurements, with control group waiting list. The study was registered under the reference number NCT05711368.
Setting
This study was conducted at the Faculty of Nursing, X University. It offers a bachelor’s degree in nursing. The faculty has nine scientific departments: critical care nursing, pediatric nursing, obstetric and gynecological nursing, medical-surgical nursing, psychiatric nursing, mental health nursing, nursing administration, community health nursing, gerontological nursing, and nursing education. Courses are provided over four years (eight semesters). The faculty follows the credit hours (cumulative grading system) obtained by summing up the scores in each academic year divided by four.
Sample Size Calculation and Sampling Technique
According to the student affairs department statistics at the Faculty of Nursing, X University; total number of enrolled candidates during the academic year 2023–2022 was 180. The registration desk provided us with a software list of those registered students, which was then presented to the Excel application to recruit the requisite sample size using a simple random sampling method. Then, the nursing students were distributed to the study or control groups using the random assignment technique.
The G*Power Windows 3.1.9.7 program was used to estimate the sample size using the following parameters: effect size = 0.25, α err prob = 0.05, power (1-β err prob) =0.90, number of groups = 2, number of measurements = 3, correlation among rep measures = 0.5. The program estimates a minimum sample size of 30 students. A randomly selected sample of 60 students (30 for the study and 30 for the control groups) met the following inclusion criteria: not participating in any type of psychotherapy and enrolling in the eighth semester of the 4th year in the faculty of nursing to decrease confounding factors.
Random Allocation
Using essential randomization and Research Randomizer version 4.0, eligible participants were randomly assigned to obtain distress tolerance training skills at a 1:1 ratio. The software produces random integers with a predetermined group code. Baseline evaluations were carried out after obtaining participants’ written consent. The enrolling investigators asked the nursing students to choose a number between 1 and 60 to determine their group assignment. The trained researcher who created the software program and the enrolling investigator were not involved in other study operations; therefore, a concealed allocation was maintained. All randomization process and data analysis were performed and kept by an independent co-author statistician and were blinded to the other authors in the study until the intervention finished.
According to the CONSORT flow diagram (Figure 1), the total number of nursing students eligible to participate in the study was 80, 30 nursing students received distress tolerance skills individually and face-to-face in the faculty counseling center for four weeks. However, 10 students refused to participate, 6 withdrew before finishing distress tolerance sessions, and 4 attended irregularly and were only minimally involved in sessions. The researchers replaced those who had withdrawn from the study group until they had completed all 30. The immediate post-treatment assessments were performed with all the study and control groups (n = 60). All the research participants completed the three-month follow-up survey (30 participants from the study group and 30 from the control group). All students recruited in the study did not undergo any other intervention or preparatory program during the distress tolerance sessions used in the present study.
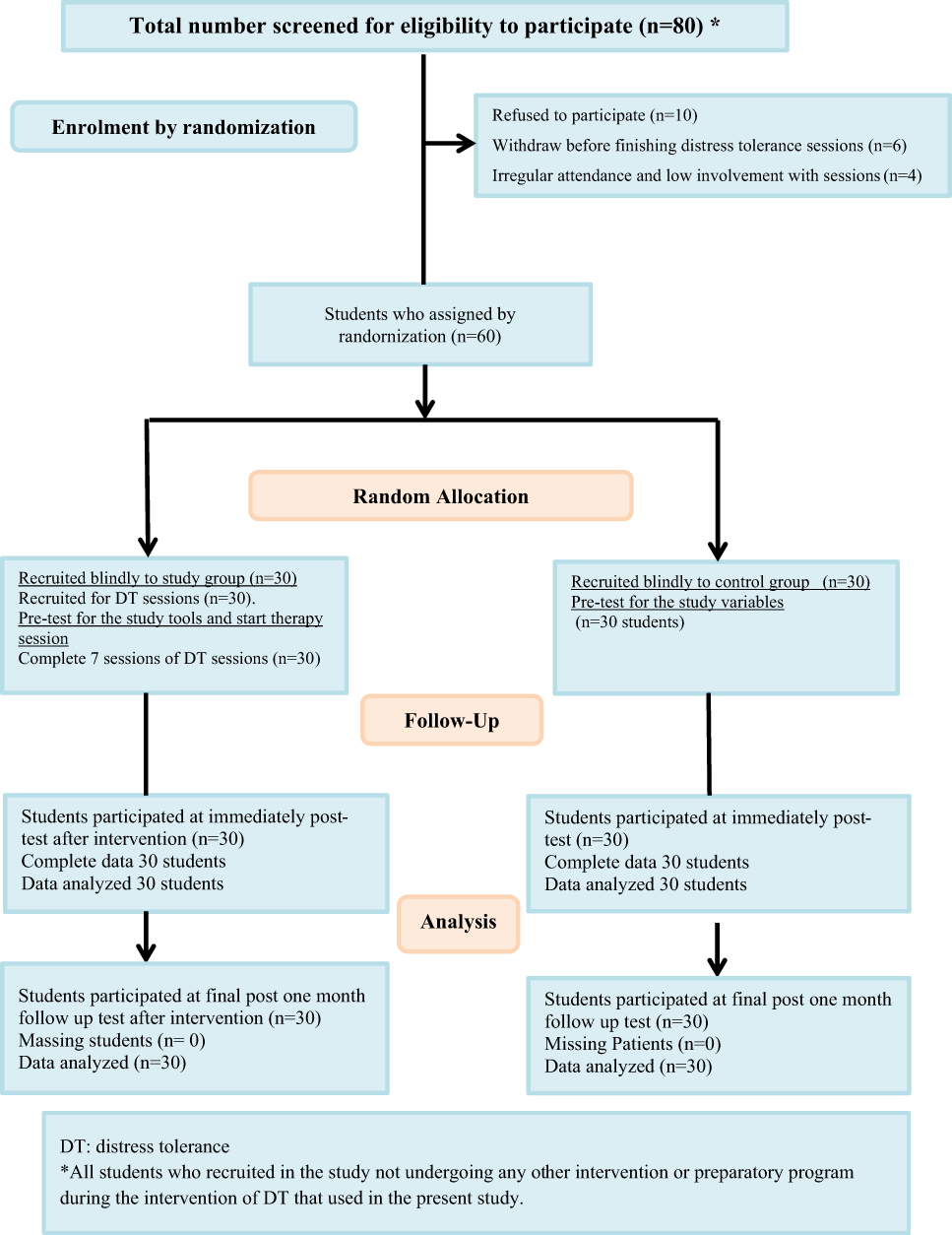 |
Figure 1 CONSORT Flow Diagram. Abbreviation: DT, distress tolerance. Notes: *All students who recruited in the study not undergoing any other intervention or preparatory program during the intervention of DT that used in the present study. |
Data Collection
Three tools were used for data collection in this study:
Tool I: A Socio-demographic and Academic Data Questionnaire: This tool was developed by researchers after reviewing the related literature to elicit data about the socio-demographic as well as the academic characteristics of the studied subjects.28
Part 1 Socio-demographic data: include student’s sex, age, residency, marital status, family income.
Part 2 Academic data: such as student’s year of enrollment, grades in previous academic year, and academic/social activities.
Tool II: Distress Tolerance Scale (DTS) (English Version)
The DTS is a 15-item self-report questionnaire that assesses tolerance of distress, appraisal of distress, attention absorbed by negative emotions, and regulation efforts to alleviate distress. Items are rated on a 1 to 5 scale (1 = strongly agree; 5 = strongly disagree) with lower scores indicating poorer tolerance of distress. Simons and Gaher (2005) reported a Cronbach’s alpha coefficient of 0.93 for the total scale, indicating excellent internal consistency.29 In the current study, the Cronbach alpha coefficient was 0.92 for the total scale.
Tool III: The Problematic Internet Use Questionnaire (PIU) (English Version)
It was developed by Demetrovics et al, 2008 and it is an 18-item self-report scale that measures the extent of how risky internet usage can be. Items are scored from 1 = never to 5 = always. This test has three factors, ie, Obsession, Neglect, and Control disorder. Earlier studies showed that PIU subscales have good psychometric properties, with high reliability (αs of 0.74–0.87), high 3-week stability (rs from 0.76 to 0.90), and acceptable discriminant validity (eg, confirmed by negligible associations with alcohol or illicit drug use and significant but weak associations with the use of gaming machines).9 The Cronbach alpha reliability in the present study was 0.818.
Tool IV: Ryff Psychological Wellbeing Scale (PWBS) (English Version)
It was developed by Carlos Ryff and it is originally con18d of six 7-item subscales for the assessment of six factors: (1) autonomy; (2) environmental mastery; (3) personal growth; (4) positive relations with others; (5) purpose in life and (6) self-acceptance. Response categories for these items are scored along a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7). The scores of some items were reversed as recommended in Ryff’s original PWBS. The scores for six subscales were calculated as averages; higher mean scores indicate greater psychological wellbeing.10–12 Internal consistency (alpha coefficients) was estimated from a sample of older and middle-aged groups, average alphas were 0.78, and 0.77, respectively, for the two groups.30 The Cronbach alpha reliability in the present study was reflected a high level of significant of 0.806.
Method
Ethical Considerations
The necessary formal approval and permission to conduct the study were obtained from the Research Ethics Committee of the Faculty of Nursing, Alexandria University, Egypt (IRB00013620-48-13-9-2022). Students were informed about the purpose of the study and an informed written consent was obtained. Also, they were told that they have the right to refuse to participate in the study and that their decision will not affect their care. In addition, they were also told that they have the right to withdraw from the study at any time even after starting and that their confidentiality of data were maintained by the researchers. As well as, considering minimizing the risk of bias; blinding the outcome assessors to the group assignments was maintained.
Administrative Steps
Official written permission from the vice dean of students’ affairs faculty of Nursing in Alexandria, Egypt was obtained for conducting the study after the ethical approval.
The Preparation Phase
Pilot Study
To assess the transparency, objectivity, viability, relevancy, and applicability of the research tools, a pilot study was performed on 15 students who met the inclusion criteria. The students in this group were not included in the study sample. The test-retest reliability was done for the study tools; Distress Tolerance Scale (DTS), Problematic Internet Use Questionnaire (PIU), and Ryff psychological wellbeing scale (PWBS).
Actual Study
The researcher successfully completed the e-training program on Dialectical Behavior Therapy (DBT) including training on distress tolerance skills through online lectures, discussions, and homework assignments. The training was conducted over 6 weeks (22 credit hours) under supervision of Dr Ahmed M. Abdelkarim, the founder and leader of DBT in Egypt. He has been an ambassador of the Linehan Institute in Egypt and the Middle East since 2018, and the Regional Affiliate of DBT MENA (Middle East & North Africa), Behavioral Tech, Linehan Institute Training Company).
The distress tolerance skills training manual which is developed by Linehan (2015b) was translated into Arabic language, the content materials of each session and practice exercises were revised to suite the Egyptian culture and necessary modifications were done.
After eliciting student socio-demographic and academic characteristics using tool I and prior to the application of the distress tolerance skills training, tools II and III were administered using the interview method. This process is aimed at determining the baseline (pre-test).
Implementation of the Distress Tolerance Skills Training
The distress tolerance training was conducted as follows (see Table 1). It consist of seven individual sessions. A 90-minute session was conducted twice a week for four weeks. The first introductory session was concerned with helping the student learn how to engage in distress tolerance training and define the goals of distress tolerance. At the end of the first session, a written plan for every session (time, duration, and setting) was scheduled individually with each student. The following six training sessions covered three core skills: crisis survival skills, reality acceptance, and skills when the crisis is an addiction.20 The distress tolerance training methods included individualized interactions, demonstration, and rehearsal, psychoeducation, practice exercises, and homework assignments. Follow-up between sessions was done using telephone calling and messaging to encourage performance on homework assignments and provide help and support when needed, particularly during stressful times. In the last seven sessions of distress tolerance training, students’ feedback about training and obstacles faced while practicing the skills were taken and documented. The students were also given corrective feedback to make their skills more efficient.
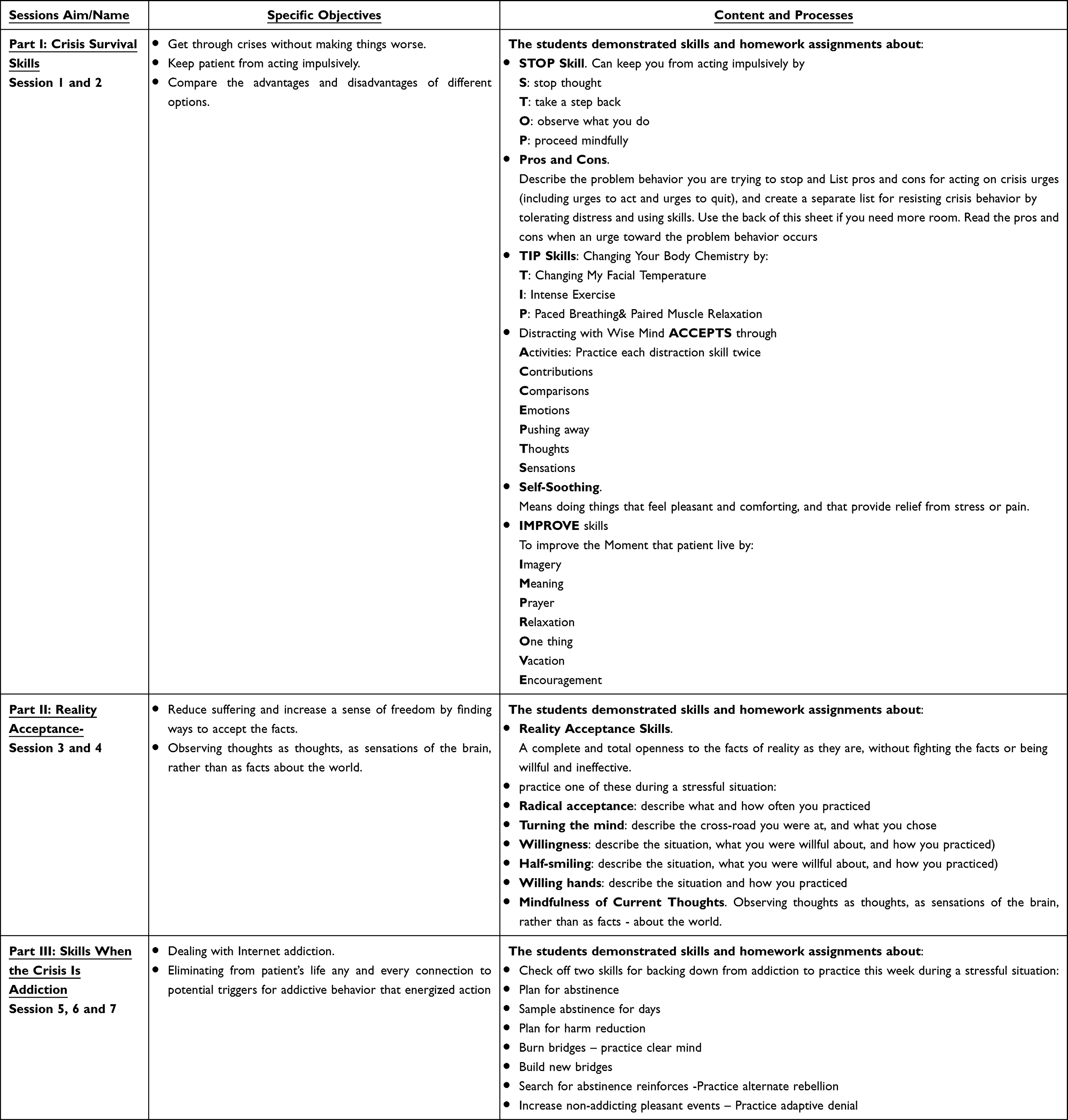 |
Table 1 Distress Tolerance Skills Interventions Were |
Evaluation or Follow-Up Phase
To validate the long-term effect of the intervention, the evaluation phase encompassed a post-test assessment immediately after intervention and a 3-month follow-up assessment using the outcome measures administered at baseline that was conducted for both groups (study and control groups) through interviewing the participants individually. As students typically end their terms by February 2023, the 3-month follow-up was maintained to assure student availability for follow-up.
Statistical Analysis of the Data
Data were fed to the computer and analyzed using the IBM SPSS software package, version 20.0. (Armonk, NY: IBM Corp.) Qualitative data were described using numbers and percentages. Quantitative data were described using range (minimum and maximum), mean, standard deviation, and median. The Shapiro–Wilk test was used to verify the normality of the distribution. The significance of the obtained results was judged to be at the 5% level.
The chi-square test was used for categorical variables to compare different groups. Fisher’s Exact or Monte Carlo Correction was used for chi-square when more than 20% of the cells had an expected count of less than 5.
Student’s t-test was used for normally distributed quantitative variables to compare between two studied groups. As well as ANOVA with repeated measures was used for normally distributed quantitative variables to compare between more than two periods. Friedman test was used for abnormally distributed quantitative variables to compare between more than two periods.
Results
Table 2 compares the study and control groups according to their socio-demographic data. The table shows that the majority of both groups, according to age, is older than 20 years, with a mean of 19.83 for both study and control groups. Most of both groups are male and are the last in birth order. Concerning marital status, almost all participants are single. More than two-thirds of both groups are not working and lived with their families. The table reflects no statistically significant difference in the sociodemographic characteristics between the study and control groups.
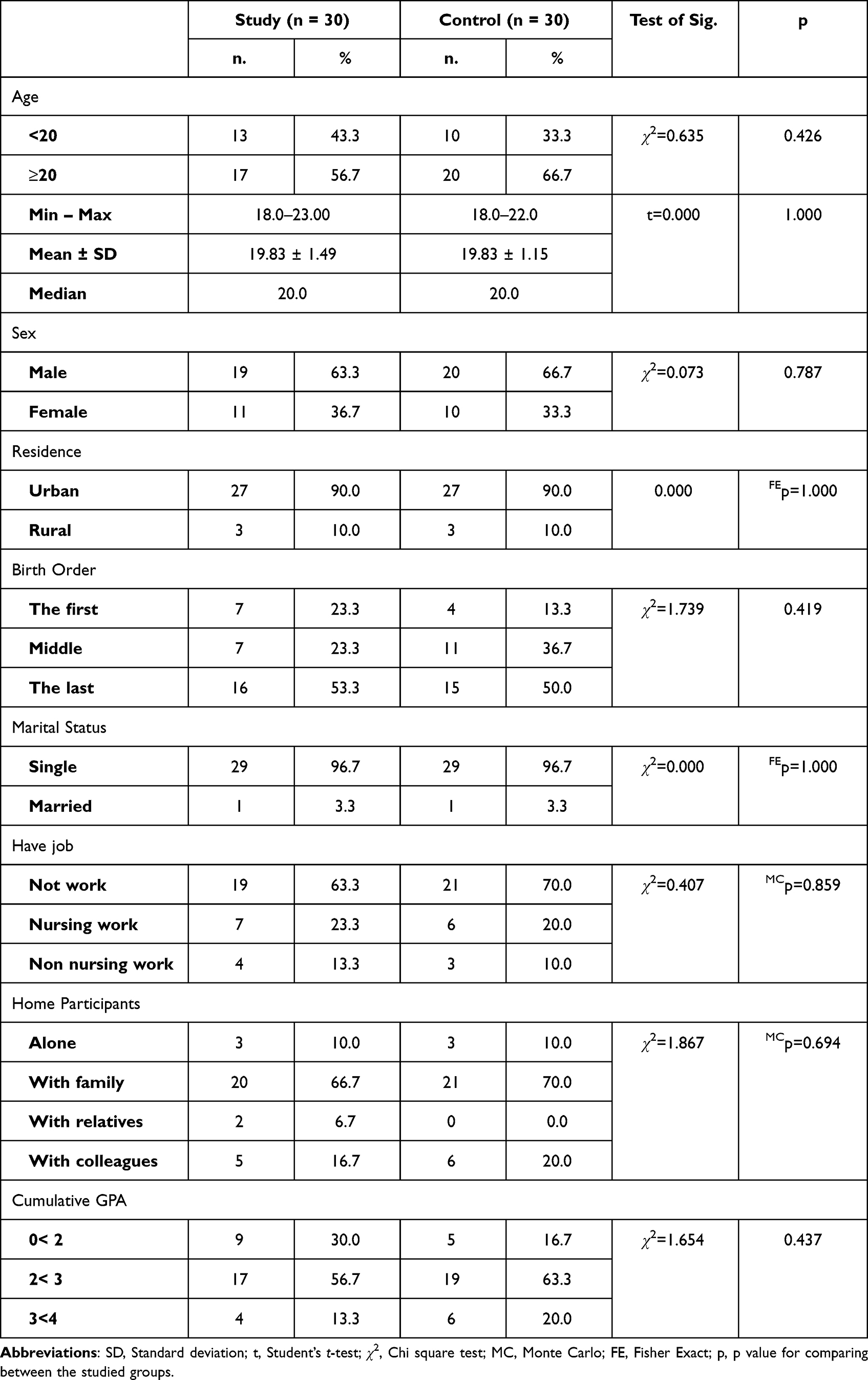 |
Table 2 Comparison Between the Two Studied Groups According to Demographic Data |
Table 3 compares the studied students according to their clinical data. Over three-quarters of the studied students reported no history of substance dependence, even on cigarettes. Two-thirds of both groups spent more than 8 hours using their mobile phones. Social media is the primary cause of internet use among both groups, with 56.7% for the study group and 70% for the control group. There is no statistically significant difference between the two groups in their clinical data, which means both groups are matched.
 |
Table 3 Comparison Between the Two Studied Groups According to Clinical Data |
Scores of distress tolerance scale at pretest, post-test, and 3-month follow-up are shown in Table 4. As hypothesized, students of the intervention group demonstrated significant mean increase in their distress tolerance from 20.75 to 72.75 and lasting for 3 months to 62.44 with statistical significant (Fr= 7.090, p= 0.006) and large effect size 0.751. However, opposing to predictions, students in control group show no changes in their mean scores of distress tolerance with insignificant tests, denoting that nursing students who completed the distress tolerance skills training, their tolerance toward distress increase and remain steady 3 month post-intervention.
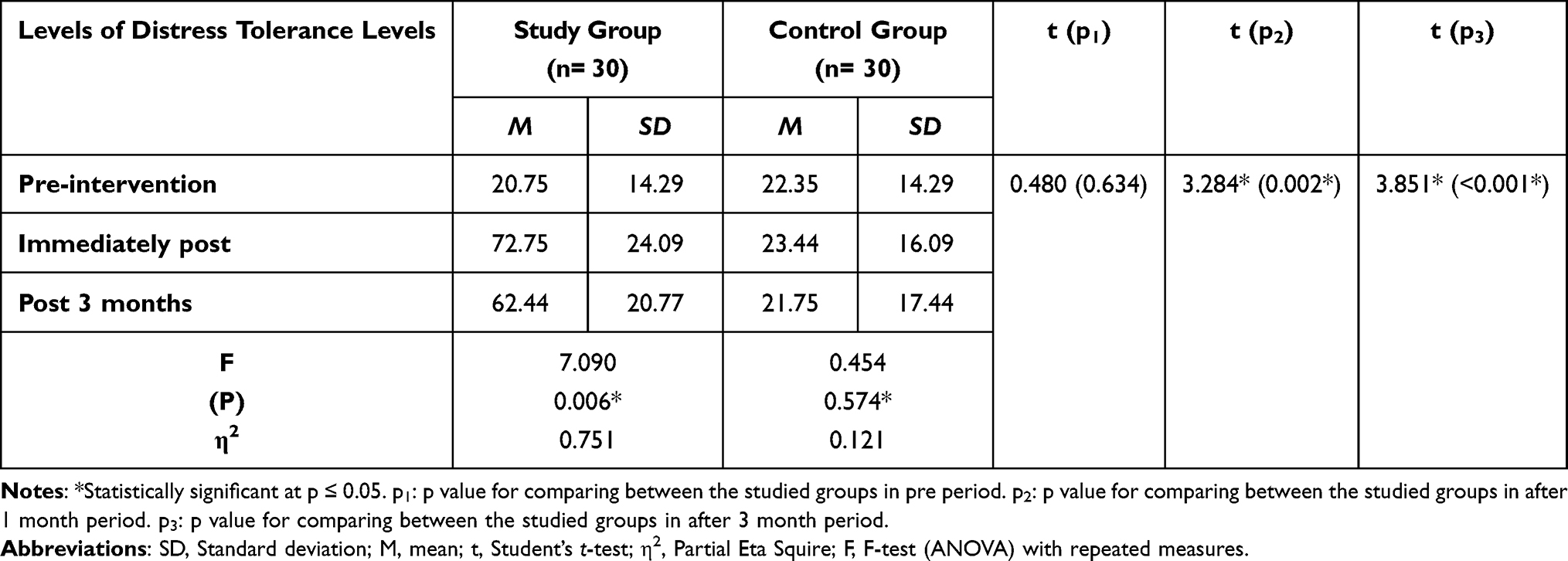 |
Table 4 Comparison of the Study and Control Group in Relation to Distress Tolerance Levels (DTS) at Pretest, Post-Test, and 3-Month Follow Up of DBT |
Table 5 compares the mean scores between both groups of problematic internet use in three different periods. The table shows the decreasing mean score of problematic internet use and each subscale. The obsession subscale means score decrease from 20.27 to 16.43 post-test, and this decrement is sustained for three months after the therapy session ended. Compared to the control group that shows no change in the mean score of the same subscale. The same results appear in the neglect and control disorder subscales for study and control groups with the same sustainability. Subsequently, the total mean score of the problematic internet use questionnaire shows a highly statistically significant decrement in the study group between the pre- and post-test. The decrement is sustained for three months using an independent t-test (p= 95.029, sig = 0.001) and repeated measures ANOVA with large effect size 0.78. Compared to the control group, no change is noticed.
 |
Table 5 Comparison Between the Two Studied Groups According to Score of Problematic Internet Use Questionnaire (PIUQ) |
Table 6 compares the mean psychological well-being scores between both groups in three periods. The table reveals that the mean scores of autonomy, environmental mastery, and positive relation, purpose in life, self-acceptance, and personal growth statistically increase among the study group after therapy and sustain for three months. The table shows that among study group, the autonomy means score increase to 24.50 post-therapy and 25.40 after three months with f=33.784, p=<0.001. Personal growth mean score increase to 25.73 post-therapy and to 26.87 after three months with f=21.234, p=<0.00. Also, the positive relation mean score increase to 25.37 post-therapy and 25.77 after three months with f=26.441, p=<0.001. The mean self-acceptance score was increase to 23.90 post-therapy and 24.77 after three months with f=29.810, p=<0.001. The same results are seen in all subscales of the psychological well-being scale, and the increase is found to be statistically significant by repeated measures ANOVA test. In compared to, no changes in the mean scores of psychological wellbeing subscales observe among the control group.
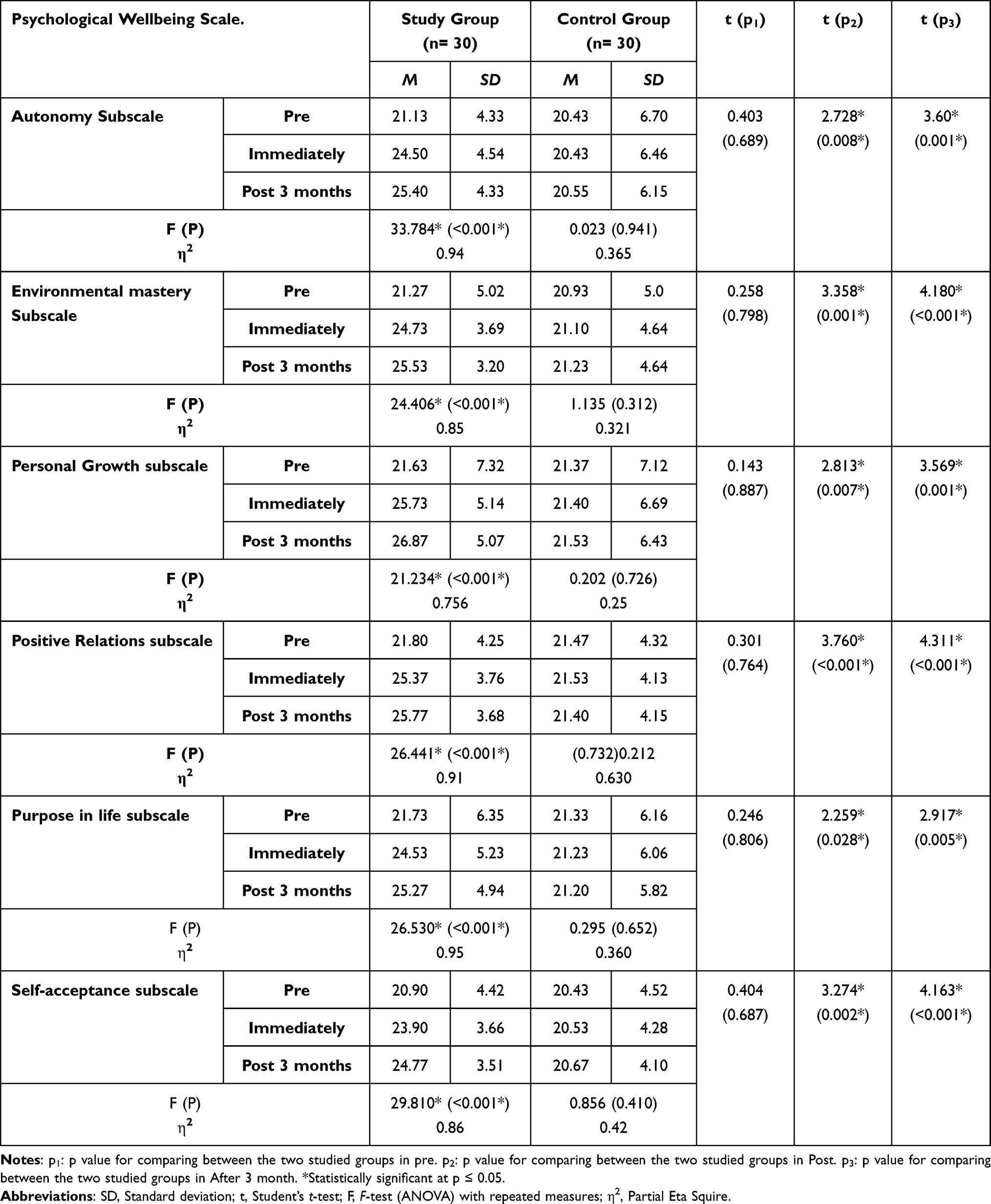 |
Table 6 Comparison Between the Two Studied Groups According to Mean Scores of Psychological Wellbeing Scale |
Table 7 compares the total mean score of psychological well-being between both groups. The table reveals that the total mean score of psychological well-being among the study group increased to 148.77 immediately after therapy and to 153.60 three months after therapy. This increase is found to be highly statistically significant (f=41.197, p=0.001) with large effect size 0.851. Compared to the unchanged total mean psychological well-being score among the control group.
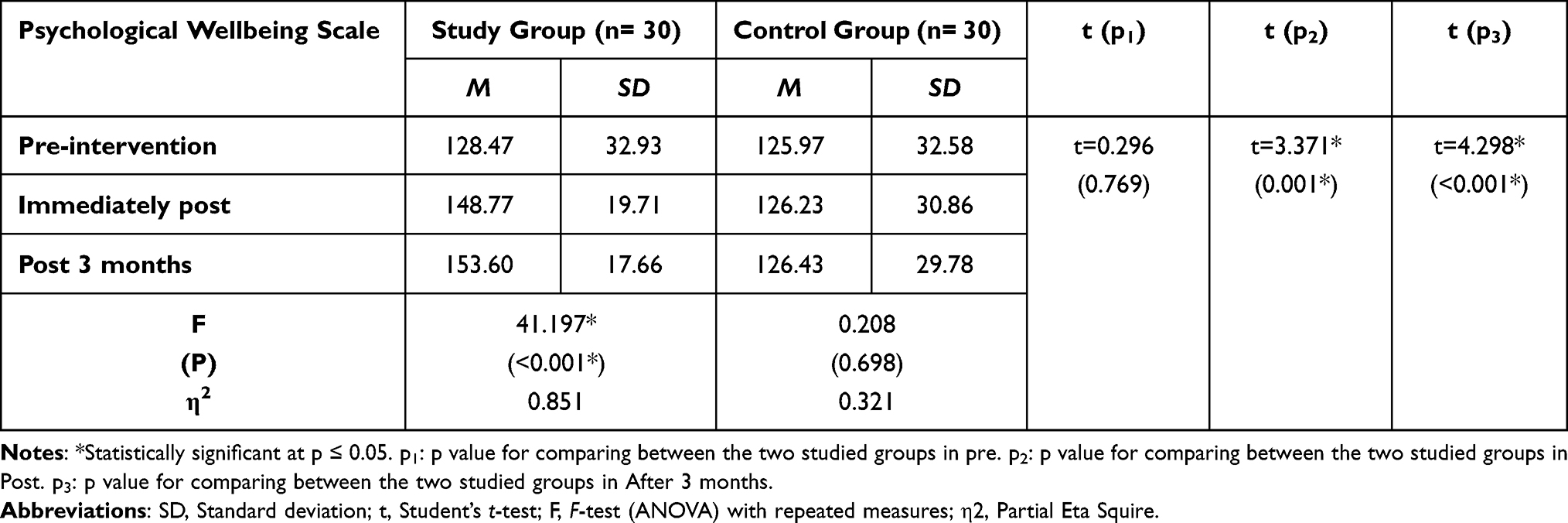 |
Table 7 Comparison Between the Two Studied Groups According to Overall Mean Score of Psychological Wellbeing Scale |
Discussion
Internet use has become crucial to students’ experiences because of distance learning, age-accepted network, and gaming. Internet addiction criteria include impaired control over activities, elevated or continued activity despite adverse consequences, increased prioritization over other activities, and severe impairment.1,26,30
The detrimental effects of Internet addiction can be reflected in poor academic achievement, comorbid mental disorders, a lack of physical activity, and worsening social relationships. Individuals with Internet addiction also have a lower quality of physical, psychological, and general health and social relations compared to those without Internet addiction.31–34 Therefore, this study targeting these consequences aimed to determine the impact of distress tolerance training on problematic internet use and psychological well-being among university nursing students.
Dialectical behavioral therapy (DBT) emphasizes distress tolerance as building the ability to tolerate and survive crises and accept life as it is. Distress tolerance skills include radical acceptance, burning bridges, directing the mind toward acceptance, and will versus desire. DBT has been demonstrated to improve outcomes in patients with substance use disorders.18,20,21
The main results of this study are as follows: the study group, who received distress tolerance skills training, demonstrated an increase in their tolerance toward distress levels at post-treatment and at the 3-month follow-up. The study group exhibited a significant decrease in problematic internet use scores across all subscales (obsession, neglect, control disorders) post-treatment, and this reduction was sustained for three months. In contrast, the control group showed no change in problematic internet use scores. Furthermore, the study group showed significant improvements in psychological well-being scores across various domains (autonomy, environmental mastery, positive relations, purpose in life, self-acceptance, personal growth) after therapy, and these improvements were sustained at the 3-month follow-up.
The results suggest that the Distress Tolerance Skills Training was effective in increasing the tolerance toward distress levels among nursing students who scored low on the pretest. Specifically, the study group showed a significant increasing in the distress tolerance at post-treatment and at the 3-month follow-up. This finding is consistent with the hypothesis that the training would improve distress tolerance skills among participants.
The present study demonstrated a significant improvement in problematic internet use and psychological well-being after intervention with distress tolerance. This finding is concordant with evidence that has shown improvement in addiction symptoms and craving, as well as induced remission in patients with substance addiction.18,20,21
In a study conducted by Siste et al to explore the efficacy of online DBT for Internet addiction compared to cognitive-behavioral therapy, significant positive changes were observed in Internet addiction and overall well-being.18,21 Similarly, Moeinedini et al concluded that DBT was effective in reducing defense styles and Internet addiction among the participants compared to the control group. Another study also highlighted the benefits of adapting DBT to treat problematic internet use in adolescents, as it was found to be helpful in addressing their excessive and dysregulated use of interactive media and electronic devices.20,21
It could be attributed to most current study subjects having good insight into their pathological internet use, as they report using the internet most of the time. So, they felt the need for therapy in the form of actualized help-seeking behavior and emphasizing resolution directed toward internet addiction. The participants could commit to all therapy sessions and demonstrated clinical improvement. Students also disclosed a preference for a group-based format for sharing their experiences. Intervention-based distress tolerance skills are practical solutions to operate during the education process, maintain therapy adherence, and reduce the overall cost of therapy.23,24,35
Obsession of problematic internet use and self-acceptance improvement after distress tolerance skill intervention may be related to distress tolerance skills. These skills are intended to help distract students and get them through difficult emotional situations one moment at a time. Accepts skill focus attention on a task you need to complete and teaches the student to compare his feelings to when they felt different.20,23,24 A way to remember this skill is with the acronym: ACCEPTS, which focuses on different skills, such as practicing distraction skills, comparisons between the usual way of coping and the new adaptive way they learned, focusing on their emotions, thoughts, and sensations without resistance or pushing them away.20
Furthermore, the radical acceptance skill helps students achieve complete and total acceptance of reality. This means that students accept the reality of a situation in their minds, hearts, and bodies and stop fighting against it. Therefore, there is a statistically significant difference between study subjects after a distress tolerance skills intervention related to self-acceptance.22,23,35
Pushing the situation away by leaving it is the skills that will help students improve obsession and autonomy. It leaves the situation mentally, builds an imaginary wall between self and the situation, and blocks thoughts and images from your mind. Adding to that, these skills help to notice ruminating, refuse to think about painful situations, and put the pain on a shelf.33
The TIP skill is intended to change body chemistry quickly to reduce the effects of an overwhelmed emotional mind, where students’ thinking and behaviors are controlled by overwhelming emotions. Performing intense exercise to calm the body when it is revved by emotion and expend your body’s stored physical energy by running, walking fast, and playing.20,35 The TIP skill enhances environmental mastery as a psychological well-being subscale.
The findings showed improvement in the control disorder subscale after the training, which may be related to self-soothing skills. This skill involves looking for a beautiful sunrise or sunset, the stars at night, pictures of these things, or listening to music students enjoy. It involves doing pleasant, comforting things that relieve stress or pain. It helps to pass the time without making things worse. Furthermore, this result may be attributed to the fact that problem-solving skills can be beneficial once a problem has arisen, and it is the students’ problem to solve. Sometimes students experience unpleasant emotions about the actions of others or situations that we cannot change.20,24 This skill helps students collect the facts and take steps to solve a problem that can change, improving control.
This improvement can also be attributed to meaning skills, as they aim to improve the moment with meaning and find purpose or meaning in students’ daily activities. Adding to that, this skill helps to improve the moment with encouragement from oneself and saying positive affirmations aloud to oneself. Also, meaning skills may be a positive factor in improving life as a psychological well-being subscale after training.18,20,35
The IMPROVE skill is to improve the moment by replacing the immediate event that has caused unpleasant emotions with more positive action, thereby making the moment more pleasant and easier to tolerate, as imagine a beautiful scene on the beach or in the mountains.20,35 Therefore, the mean score of neglect decreases after applying the distress tolerance intervention.
It is worth mentioning that environmental mastery means the score decreases, while the purpose of life means the score increases after distress tolerance training due to the pros/cons skill. This skill can be beneficial when students need to make a decision between two or more options. The objective when using this skill is for students to realize that accepting reality and tolerating distress leads to better outcomes than rejecting reality and refusing to tolerate distress. It describes the dilemma at the hand of realizing internet addiction. If the dilemma involves crisis behavior that students hope to avoid and want to look at the pros and cons of the behavior. It also helps to examine the pros and cons of the crisis behavior or acting on a student’s urge to use the internet. Then examine the advantages and disadvantages of each of the viable options. Writing out the pros and cons and carrying them with you is helpful so that students can be reminded and rehearse the skill repeatedly.18,35
Conclusively, this study emphasizes the effectiveness of distress tolerance training in improving students’ distress tolerance, problematic internet use, and psychological well-being. Healthcare professionals, especially psychiatric nurses, can consider incorporating distress tolerance training as a significant part of their therapeutic interventions for individuals struggling with problematic internet use. The findings of this study can contribute to the practice of psychiatric nursing and other healthcare professionals by offering insights into effective interventions for problematic internet use, advancing evidence-based practice, and addressing the broader impact of internet misuse on students’ well-being.
Limitations of the Study
Delivering a randomized control group provides reliable proof that the observed positive outcomes are attributable to the implementation of distress tolerance skills. They are further applying distress tolerance skills according to a fidelity reference of Linehan’s training manual. However, this study was conducted on a small sample size that inadvertently might affect the obtained findings. Nevertheless, it is possible to warrant further investigation in more extensive randomized controlled trials in future research. Also, a long-term intervention to detect the sustainable effect of the program leads to the loss of some students during the follow-up period.
Strength of the Study
Distress tolerance skills for internet addiction are most effective when used in conjunction with others peers, such group therapy. DBT complements these other treatments by teaching you the necessary skills to effectively cope with your emotions and manage stress without turning to internet addiction. This is very important because the recovery journey can be a stressful and emotional time, and it is during these times that students are most likely to relapse. Distress tolerance provides students with the tools student need to deal with these difficult emotions and situations in a healthy way.
Conclusion
Overall, the current finding suggests it is feasible to adapt and implement DBT for managing Internet use problems and psychological well-being among nursing students and this intervention has real potential as an adjunctive treatment for these students. The current findings call for more research in more significant randomized controlled trials that examine treatment outcome modifiers, including the severity of participant emotion dysregulation. Future research should focus on identifying the variables that predict treatment response and further exploring the impact of skill development in predicting more outcomes.
Implications to Psychiatric Nursing
The present study holds important practical implications for reducing problematic internet use and improving psychological well-being among faculty nursing students. Enhancing distress tolerance skills among nursing students is highly recommended. These skills would begin with assessing the pros and cons of distress (adaptive and maladaptive) and then promoting the adaptive strategies. Distress tolerance skills training for teachers and professionals working with nursing students is needed to teach and help them learn adaptive ways of managing stress. Moreover, educational institutions should consider integrating distress tolerance training into the curriculum for faculty nursing students. This training can be provided separately or integrated into existing courses or workshops.
Moreover, family psychoeducational interventions should be developed to increase families’ awareness of distress tolerance. Further research is needed to investigate the effect of different psychiatric nursing interventions, such as mindfulness skill training, on improving students with PIU.
Abbreviations
DT, Distress Tolerance; IGD, Internet Gaming Disorder; PIU, Problematic Internet Use; DBT, Dialectical Behavior Therapy; RCT, Randomized Control Trial; CONSORT, Consolidated Standards of Reporting Trials; PWBS, Psychological Well-being Scale.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Every method was used following the pertinent rules and regulations of the Helsinki Declaration (DoH-Oct2008). The Research Ethics Committee (Institutional Review Board) of the Faculty of Nursing at Alexandria University in Egypt provided the necessary formal approval and authority to perform the study (IRB: IRB00013620-48-13-9-2022).
Acknowledgement
The authors extend their appreciation to Princess Nourah bint Abdulrahman University Researchers Supporting Project for funding this research work trough the project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Funding
Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R279), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. King DL, Delfabbro PH, Billieux J, Potenza MN. Problematic online gaming and the COVID-19 pandemic. J Behav Addict. 2020;9(2):184–186. doi:10.1556/2006.2020.00016
2. Schmidt SC, Anedda B, Burchartz A, et al. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: a natural experiment. Sci Rep. 2020;10(1):1–2. doi:10.1038/s41598-020-78438-4
3. Gong Z, Wang L, Wang H. Perceived stress and internet addiction among Chinese college students: mediating effect of procrastination and moderating effect of flow. Front Psychol. 2021;28(12):632461. doi:10.3389/fpsyg.2021.632461
4. World Health Organization. Excessive screen use and gaming considerations during COVID19; 2020. Available from: http://www.emro.who.int/mnh/news/considerations-for-young-people-on-excessive-screen-use-during-covid19.html.
5. Király O, Potenza MN, Stein DJ, et al. Preventing problematic internet use during the COVID-19 pandemic: consensus guidance. Compr Psychiatry. 2020;100:152180. doi:10.1016/j.comppsych.2020.152180
6. Kożybska M, Radlińska I, Kolwitz M, Karakiewicz B. Problematic internet use among Polish students: prevalence, relationship to sociodemographic data and internet usage patterns. Int J Environ Res Public Health. 2023;20(3):2434. doi:10.3390/ijerph20032434
7. Moreno M, Riddle K, Jenkins MC, Singh AP, Zhao Q, Eickhoff J. 2022 Measuring problematic internet use, internet gaming disorder, and social media addiction in young adults: cross-sectional survey study. JMIR Public Health Surveill. 2022;8(1):e27719. doi:10.2196/27719
8. Müller KW, Beutel ME, Dreier M, Wölfling K. A clinical evaluation of the DSM-5 criteria for internet gaming disorder and a pilot study on their applicability to further internet-related disorders. J Behav Addict. 2019;8(1):16–24. PMID: 30663331; PMCID: PMC7044592. doi:10.1556/2006.7.2018.140
9. Demetrovics Z, Szeredi B, Rózsa S. The three-factor model of internet addiction: the development of the problematic internet use questionnaire. Behav Res Methods. 2008;40(2):563–574. doi:10.3758/BRM.40.2.563
10. Reddy NY. Perceived wellbeing, happiness, and related challenges among Indian college students. Psychol Stud. 2023;68(1):70–81. doi:10.1007/s12646-022-00705-3
11. Elhusseiny A, Haggag WE, Abd Elmoez K, Elsayed M, Hassan H. Psychiatric symptoms associated with internet addiction among Suez Canal University students. Egypt J Psychiatry. 2022;43(3):149–154. doi:10.4103/ejpsy.ejpsy_50_21
12. Ryff CD. Psychological well-being in adult life. Curr Dir Psychol Sci. 1995;4(4):99–104. doi:10.1111/1467-8721.ep10772395
13. Tan Y, Huang C, Geng Y, Zhang S, Zhang S. Psychological well-being in Chinese college students during the COVID-19 pandemic: roles of resilience and environmental stress. Front Psychol. 2021;12:671553. doi:10.3389/fpsyg.2021.671553
14. Ko CH, Yen JY. Impact of COVID-19 on gaming disorder: monitoring and prevention. J Behav Addict. 2020;9(2):187–189. doi:10.1556/2006.2020.00040
15. Dieris-Hirche J, Te Wildt Bt B, Pape M, et al. Quality of life in internet use disorder patients with and without comorbid mental disorders. Front Psychiatry. 2022;13. doi:10.3389/fpsyt.2022.862208
16. Chen IH, Chen CY, Pakpour AH, et al. Problematic internet-related behaviors mediate the associations between levels of internet engagement and distress among schoolchildren during COVID-19 lockdown: a longitudinal structural equation modeling study. J Behav Addict. 2021;10(1):135–148. doi:10.1556/2006.2021.00006
17. Siste K, Hanafi E, Sen LT, Alison P, Beatrice E, Beatrice E. Online dialectical behavioral therapy for adults with internet addiction: a quasi-experimental trial during the COVID-19 pandemic. Psychiatry Res. 2022;1(315):114698. doi:10.1016/j.psychres.2022.114698
18. Cavicchioli M, Movalli M, Vassena G, Ramella P, Prudenziati F, Maffei C. The therapeutic role of emotion regulation and coping strategies during a stand-alone DBT skills training program for alcohol use disorder and concurrent substance use disorders. Addict Behav. 2019;1: 98:106035. doi:10.1016/j.addbeh.2019.106035
19. Linehan M. Building a Life Worth Living: A Memoir. United States: Random House Publishing Group; 2020.
20. Moeinedini M, Kashani FL, Shafiabadi A. The effectiveness of dialectical behavior therapy compared to integrative psychotherapy in defensive styles and internet addiction. Iran J Psychiatry Behav Sci. 2021;15(2):e111111. doi:10.5812/ijpbs.111111
21. Pluhar E, Jhe G, Tsappis M, Bickham D, Rich M. Adapting dialectical behavior therapy for treating problematic interactive media use. J Psychiatr Pract. 2020;26(1):63–70. doi:10.1097/PRA.0000000000000439
22. William E. Dialectical behavior therapy for addiction: the easy self - help guide - simple steps to conquering addictions to porn - eating disorders - substance abuse - alcohol and drugs - online gambling; 2019.
23. Lakeman R, King P, Hurley J, et al. Towards online delivery of dialectical behaviour therapy: a scoping review. Int J Ment Health Nurs. 2022;31(4):843–856. doi:10.1111/inm.12976
24. Abdelgany HY, Shalaby MH, ELattar NF. Problematic internet use and psychological problems among faculty of nursing students Benha University. Tanta Sci Nurs J. 2018;14(1):7–30. doi:10.21608/tsnj.2018.71024
25. Aquino AP, Kimong PJ. Boredom and distress tolerance on problematic internet use among public university students. MJSSH. 2022;7(5):e001477. doi:10.47405/mjssh.v7i5.1477
26. Beanlands H, McCay E, Fredericks S, et al. Decreasing stress and supporting emotional well-being among senior nursing students: a pilot test of an evidence-based intervention. Nurse Educ Today. 2019;76:222–227. doi:10.1016/j.nedt.2019.02.009
27. Van Hoek G, Portzky M, Franck E. The influence of socio-demographic factors, resilience and stress reducing activities on academic outcomes of undergraduate nursing students: a cross-sectional research study. Nurse Educ Today. 2019;72:90–96. doi:10.1016/j.nedt.2018.10.013
28. Simons JS, Gaher RM. The distress tolerance scale: development and validation of a self-report measure. Motiv Emot. 2005;29(2):83–102. doi:10.1007/s11031-005-7955-3
29. Shryock S, Meeks S. Internal consistency and factorial validity of the 42-item psychological well-being scales. Innov Aging. 2018;2(Suppl 1):690. doi:10.1093/geroni/igy023.2568
30. Chia DX, Ng CW, Kandasami G, et al. Prevalence of internet addiction and gaming disorders in Southeast Asia: a meta-analysis. Int J Environ Res Public Health. 2020;17(7):2582. doi:10.3390/ijerph17072582
31. Park JJ, Wilkinson-Meyers L, King DL, Rodda S. Access to health care for gaming disorder: a patient-centred approach to address the continuum of need. Res Sq. 2020. doi:10.21203/rs.3.rs-30827/v2
32. Chun J, Shim H, Kim S. A meta-analysis of treatment interventions for internet addiction among Korean adolescents. Cyberpsychol Behav Soc Netw. 2017;20(4):225–231. doi:10.1089/cyber.2016.0188
33. Daughters SB, Ross TJ, Bell RP, Yi JY, Ryan J, Stein EA. Distress tolerance among substance users is associated with functional connectivity between prefrontal regions during a distress tolerance task. Addict Biol. 2017;22(5):1378–1390. doi:10.1111/adb.12396
34. Mattingley S, Youssef GJ, Manning V, Graeme L, Hall K. Distress tolerance across substance use, eating, and borderline personality disorders: a meta-analysis. J Affect Disord. 2022;1(300):492–504. doi:10.1016/j.jad.2021.12.126
35. Zhang X, Zhang J, Zhang K, et al. Effects of different interventions on internet addiction: a meta-analysis of random controlled trials. J Affect Disord. 2022;313:56–71. doi:10.1016/j.jad.2022.06.013
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.