Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Effect of a Low-Carbohydrate, High-Fat Diet versus Moderate-Carbohydrate and Fat Diet on Body Composition in Patients with Lipedema
Authors Jeziorek M ![]() , Szuba A, Kujawa K, Regulska-Ilow B
, Szuba A, Kujawa K, Regulska-Ilow B
Received 8 June 2022
Accepted for publication 22 July 2022
Published 22 August 2022 Volume 2022:15 Pages 2545—2561
DOI https://doi.org/10.2147/DMSO.S377720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Małgorzata Jeziorek,1 Andrzej Szuba,2 Krzysztof Kujawa,3 Bożena Regulska-Ilow1
1Department of Dietetics, Faculty of Pharmacy, Wroclaw Medical University, Wroclaw, Poland; 2Department of Angiology, Hypertension & Diabetology, Wroclaw Medical University, Wroclaw, Poland; 3Statistical Analysis Center, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Małgorzata Jeziorek, Wroclaw Medical University, Borowska 211, Wroclaw, 50-556, Poland, Tel +48 71 784 01 11, Email [email protected]
Introduction: Lipedema is a disorder characterized by an excessive accumulation of subcutaneous body fat, mainly bilateral and symmetrical accumulation of fat deposits, particularly in the lower extremities excluding feet. Pain (spontaneous or with palpation) and increased capillary fragility with bruising are also part of clinical presentation. It is estimated to occur in approximately 11.0% of women worldwide. Management of obesity among patients with lipedema is a key component in its treatment.
Purpose: The aim of this study was to compare effectiveness of two diets: low-carbohydrate-high-fat diet (LCHF) and medium-fat-medium-carbohydrate diet (MFMC) in body weight, body fat and limb circumference reduction in patients with lipedema.
Material and Methods: The studied women (n = 91) were divided into 2 groups and submitted to 1 of the 2 diets for 16 weeks. Anthropometric measurements such as body height [cm], body weight [kg], body fat percentage [%], body fat [kg], lean body mass [kg], and visceral fat level were collected at the beginning and end of the study.
Results: We have not found any significant differences in anthropometric measurements at the baseline between groups. Body weight and all anthropometric parameters decreased significantly in both groups after 16 weeks of diets, excluding the circumference above the right ankle for the MFMC diet which did not change. The LCHF diet contributed to reduction of body weight (− 8.2 ± 4.1 kg vs − 2.1 ± 1.0 kg; p < 0.0001), body fat (− 6.4 ± 3.2 kg vs 1.6 ± 0.8 kg; p < 0.0001), waist (− 7.8 ± 3.9 cm vs − 2.3 ± 1.1 cm; p < 0.0001), hips (− 7.4 ± 3.7 cm vs − 2.5 ± 1.3 cm; p < 0.0001), thighs and calves’ circumferences compared with the MFMC diet. We observed reduction of pain in the extremities and mobility improvement in LCHF group (data not shown).
Conclusion: The LCHF diet was more effective than MFMC in body weight, body fat and lower limb circumferences reduction.
Keywords: lipedema, low carbohydrate high fat diet, low-glycemic index diet, anti-inflammatory diet, body composition
Introduction
Lipedema is a disorder characterized by an excessive accumulation of subcutaneous body fat, characterized by soreness as well as mainly bilateral and symmetrical accumulation of fat deposits, particularly in the lower extremities. Pain (spontaneous or with palpation) and increased capillary fragility with bruising are also part of clinical presentation.1 It usually affects lower extremities, excluding feet. Lipedema is a common disorder almost exclusively found in women.2 It is estimated to occur in approximately 11.0% of women worldwide.3 Typical clinical signs of lipedema include disproportionate lower body adipose tissue deposition excluding feet, pain in the extremities and easy bruising. The onset of the disease usually occurs during a period of significant hormonal changes in the female body, ie, during puberty, after pregnancy, or during menopause.2,4 Adipose tissue soreness occurs in 89.7% of patients with lipedema.2 The pathophysiology of the pain is not fully understood, but increased inflammation, compression of peripheral nerves by proliferating adipose tissue, and fluid accumulation in the area occupied by lipedema have been implicated as possible causes.2 Pain, disfiguration and reduced mobility are strongly associated with lower quality of life and deterioration of psychological functioning. Lack of acceptance of own body is associated with reduced self-esteem, anxiety and social isolation.2,5,6 Patients often experience stigma because of their looks.7 Some suffer from depression and eating disorders.2,5–7 Because of high proportion of patients with psychological disorders, including eating disorders, any change in diet should be accompanied by psychological support.8
Lipedema is often misdiagnosed as obesity; however, they frequently co-occur.9 Managing obesity in patients with lipedema is a key component of this disorder’s treatment.10,11 Weight loss can be accomplished by implementation of appropriate energy-reduced diet and regular physical activity, such as marching, swimming, Pilates or yoga.9–12 The authors of lipedema management guidelines indicate that weight and body fat reduction are very difficult, particularly concerning lower extremities.8–10,13–16 Moreover, it was found that 95.0% of patients were not able to lose fat from the areas affected by lipedema.17 Untreated lipedema and concomitant obesity may lead to secondary lymphedema.2,9 In patients with lipedema, weight gain is one of the characteristic symptoms, associated with accumulation of body fat. On the other hand, accumulation of adipose tissue leads to increased synthesis of pro-inflammatory adipokines. Chronic positive energy balance and low physical activity lead to weight gain and increased influx of nutrients to adipose tissue. This, in turn, contributes to adipocyte hypertrophy and hypoxia.18 The authors also indicate that lipedema is a disorder characterized by inflammation that is independent of concomitant obesity and not fully understood.2,19,20 Therefore, a diet that reduces inflammation may be important in lipedema treatment.19,21
A specific role of estrogens in the development of lipedema is proposed, which may be related to the regulation of lipogenesis and lipolysis.1,2 Estrogens promote fat storage by enhancing insulin secretion, increasing sensitivity of target tissues to this hormone, and in part by inhibiting fatty acid oxidation.2 In women with excessive body weight, lipolysis in buttock regions is reduced compared to the area of adipose tissue located in the abdomen. This may be due to differences in the distribution of estrogen receptors.22 Polygenic alteration in the distribution of alpha- and beta-estrogen receptors (ER) (decreased ER-alpha expression and increased ER-beta expression) in white adipose tissue from areas involved in lipedema may also play a role in pathogenesis of this disease.23 However, to date, the importance of estrogen in the pathogenesis of lipedema has not been fully elucidated.
Treatment of lipedema should encompass a holistic approach to the patient and include psychological support, effective weight loss and compression therapy.9,19 The authors of lipedema studies point out that proper nutritional management and moderate physical activity are key components of therapy.2,9,15 Dietary recommendations provide general information indicating diet low in refined carbohydrates, especially added sugars (particularly fructose) and refined grain products, as well as salty and animal-based products. The diet should primarily include unprocessed products, mainly plant-based, different colored vegetables, fruits (excluding juices) and fermented products, as well as use herbs for seasoning.21 Therefore, demonstrating link between specific dietary intervention and reduction of lipidemic adipose tissue may have strategic impact on lipedema treatment. To date, one paper has been published that demonstrates the efficacy of a modified Mediterranean diet in body weight reduction in lipedema patients.19 Published data also suggest the potential efficacy of the ketogenic diet in the treatment of lipedema, but this has not yet been confirmed by intervention studies.2,12,16 We have found no published studies on the efficacy of different dietary models for patients with lipedema.
The aim of this study was to compare effectiveness of two diets: low carbohydrate high fat (LCHF) and medium fat medium carbohydrate (MFMC) in body weight, body fat and lower limb circumference reduction in patients with lipedema.
Materials and Methods
Study Design and Description of the Study Group
A total of 108 women diagnosed with lipedema based on typical clinical signs were enrolled in the study between January 2020 and June 2021.4 Clinical evaluation and diagnosis of lipedema was confirmed by a physician specialized in angiology. The age of the participants ranged from 18 to 76 years (mean 43.2 ± 12.8 years; median = 40.0). A total of 91 female participants completed the study (n = 91). They were referred to the Department of Dietetics, Faculty of Pharmacy, Wroclaw Medical University (Poland), by an angiologist.
The participants were subsequently divided into 2 groups. The participants enrolled between January and October 2020 were enrolled to the MFMC group, and the participants enrolled from November to June 2021 were enrolled to the LCHF group. One group received a low-carbohydrate-high-fat diet (LCHF; n = 46) and the other group a low glycemic index medium-fat-medium-carbohydrate (MFMC; n = 45). Patients were measured for resting metabolic rate (RMR) assessment to determine energy requirements at baseline. Both diets were applied for 16 weeks in each group. Anthropometric measurements including body weight, body fat, lean body mass, visceral fat, waist, hip, and thigh and calf circumferences were collected at the beginning and at the end of the study.
The exclusion criteria included: male gender, lymphedema of the lower limbs and factors preventing the performance of body composition analysis by electrical bioimpedance method: pregnancy, metal elements in the body as well as pacemaker, stents or other elements emitting electrical signals. The patients were not on an ongoing treatment for lipedema (compression or surgical treatment) and they were not adhered to any specific diet.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Bioethics Committee at Wroclaw Medical University, Poland (KB - 456/2019). Written informed consent was obtained from all patients.
Anthropometric Measurements and Body Composition Analysis Measured by Electrical Bioimpedance
A TANITA HR- 001 growth meter (Tanita, Japan) and a Jawon Medical X-Contact 353 8-electrode body composition analyzer (Jawon Medical co., Ltd., Republic of Korea) were used for anthropometric measurements. Parameters such as body height [cm], body weight [kg], body fat percentage [%], body fat [kg], lean body mass [kg], and visceral fat level were obtained. Patients were instructed not to consume food or drink for 4 hours, not to engage in vigorous physical activity for 12 hours, and not to use diuretics for 6 hours prior to the study. Body Mass Index (BMI) was calculated as the ratio of body weight [kg] to height [m] squared. Waist, hip, thigh, and calf circumferences were measured with a standard tape measure to the nearest 1 cm.
Measurement of Resting Metabolic Rate (RMR) by Indirect Calorimetry
Actual resting metabolic rate was obtained by Fitmate device (Cosmed, Rome, Italy) with the indirect calorimetry method. The participants were instructed to avoid food and beverage consumption (except water) for a minimum of 8 hours prior to the measurement and to refrain from intense exercise 48 hours in advance. The measurement was performed in a supine position in a ventilated and darkened room at moderate temperature. Participants were instructed to take the test in the morning after sleeping for a minimum of 7–9 hours. Before the measurement, each participant was allowed several minutes of rest in a sitting position to optimize the conditions. Participants were connected to the measuring device through a specially designed mask attached to the device by a sampling tube. The measurement took between 10 and 20 minutes and was performed in conditions aimed at isolating the participant from external noise. The device was calibrated before each measurement and the progress was monitored on the screen. The participants were informed about the exact course of the study procedure in advance.
Total energy expenditure was calculated by multiplying RMR by the appropriate physical activity level (PAL) selected individually for each patient.24
Lipedema Staging
Clinical evaluation of the stages of lipedema in our study was confirmed by physician specialized in angiology. Figure 1 depicts different stages of lipedema.2
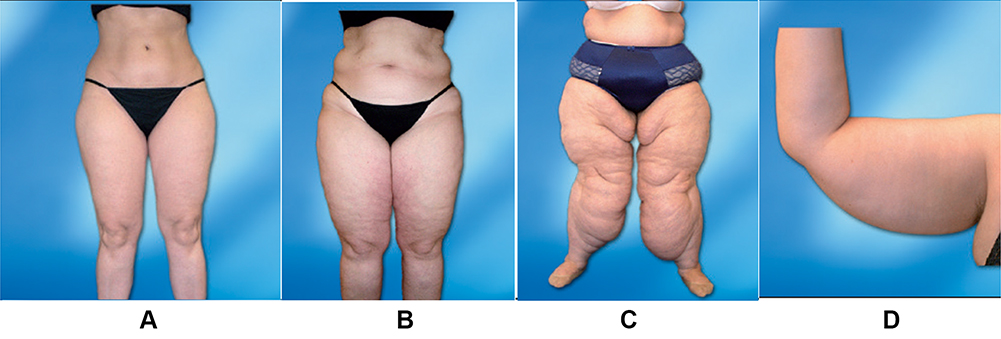 |
Figure 1 Lipedema staging. (A) Stage 1 - skin appears smooth, but the thickened subcutaneous tissue contains small nodules. (B) Stage 2 - skin has an irregular texture, subcutaneous nodules occur that vary from the size of walnut to that of an apple in size. (C) Stage 3 - deformed lobular fat deposits form, especially around thighs and knees, and may cause considerable distortion of limb profile. (D) Stage 4 - lipedema with lymphoedema (lipolymphoedema). |
Dietary Intervention
A diet with an energy deficit accounting for 15–25% of total energy expenditure depending on the degree of obesity was administered to each study participant. The total energy expenditure was divided into 3, 4 or 5 meals. The intervals between meals were 4 to 6 hours during the day and a minimum of 12 hours at night.18,25 The patients were also advised not to have any snacks or drinks (except mineral water) between meals.
Both diets characterized by high proportion of anti-inflammatory nutrients,26 such as monounsaturated (MUFA) and polyunsaturated fatty acids (PUFA). Sources of MUFA in the diet included products such as olive oil, almonds, hazelnuts, avocados, and olives, and sources of PUFA were canola oil, flaxseed oil, walnuts, oil seeds, and oily marine fish such as herring, sardines, salmon, and mackerel. The diets were characterized by antioxidants, vitamin C, beta-carotene, and dietary fiber. The diets included foods rich in magnesium, such as cocoa, dark chocolate, nuts and seeds, as well as vitamin E: nuts, oil seeds, and vegetable oils. Additionally, spices such as cloves, garlic, ginger, rosemary, oregano, thyme, pepper and turmeric were added to the diets. Patients were instructed to avoid salty foods to limit dietary sodium intake and to drink a minimum of one green or black tea daily. Pro-inflammatory foods which are sources of saturated fatty acids, such as butter, mayonnaise, and cream were limited. Both diets completely excluded products such as lard, tropical oils (coconut and palm oil), sunflower oil, grapeseed oil, corn oil, margarines made from these oils, pork, fatty processed meats, offal, salty snacks, sweets, fruit juices and drinks. Dairy products were limited to 2 portion per day.
The LCHF diet was designed to maximally reduce the intake of processed foods and products rich in saturated fatty acids (eg, fatty meat, offal, lard, butter) and to increase the intake of products typical for the Mediterranean diet, such as: vegetables, fruits (berries), nuts and seeds, olive oil and oily marine fish.19 The diet limited meat consumption to 3–4 portions per week (1 portion was 100–200 g of lean poultry meat, chicken or turkey). It was also recommended that the consumption of lean red meat (eg, beef or veal) should not exceed 1 portion per week (maximum 150 g). The diet increased the supply of oily marine fish from 2 to 3 portions per week (1 portion was 100–150 g).
The MFMC diet had a low glycemic load and a high proportion of low and medium glycemic index products. Products with a high glycemic index were completely excluded from the diet. The diet included foods typical of the Mediterranean diet: fruits, vegetables, pulses, whole-grain cereals, olive oil, oily marine fish, and low-fat dairy products.19 Fiber was increased above the recommended standard for adults because of its anti-inflammatory properties.26,27
All products type included and not included in the LCHF and MFMC diets are shown in Table 1.
 |  |  |  |
Table 1 Products Recommended and Not Recommended in LCHF and MFMC Diets |
Each participant received an individual 7-day dietary plan along with a detailed shopping list for the week. The dietary plans were created by a dietician using Dietetyk Pro software (Dietetyk Pro, Wroclaw, Poland). All diets were individually modified and tailored to the dietary preferences and lifestyles of the patients while maintaining the principles of applied nutritional intervention. The individualization of the dietary plans contributed to increased adherence to the diet by the study patients. Additionally, each patient received detailed dietary recommendations that facilitated adherence to the dietary plan. The participants stayed contact with dietician every week to assess the diet adherence and self-body weight measurement. The energy and nutritional value of diets was calculated based on the Polish tables of nutritional value of products and dishes28 and using the USDA (U.S. Department of Agriculture) food products database.29
Statistical Analyses
Results are presented as mean values ± standard deviation or median and values from Q1 and Q3. The conformity of the distribution in the evaluated data sets to the normal distribution was verified using the Shapiro–Wilk test. If the distribution was significantly different from normal, non-parametric tests were applied (Mann–Whitney U for independent samples and Wilcoxon test for repeated measurements), otherwise - Student’s t-test (for variances not significantly different) or Cochran-Cox test (for differing variances). The variances of the compared sets were compared using the Brownian-Forsythe test. Differences in energy and nutritional value of the diets used were assessed with the Mann–Whitney U-test. The differences at lipedema stages in both groups were assessed by Chi-squared test. The anthropometric parameters at baseline were assessed by Student’s t-test and Mann–Whitney U-test. Changes in anthropometric parameters before and after the application of each diet were assessed by Student’s t-test for dependent samples and Wilcoxon test. To compare the value of differences between baseline and final anthropometric measurements as a result of following the two diets, three types of tests were used: Student’s t-test, Cochran-Cox test and Mann–Whitney U-test (depending on the results of the test checking normality of distribution and the test checking homogeneity of variation). Correlations between baseline anthropometric measurements and the difference in these values after both diets were evaluated using Pearson correlation. Results for all analyses were considered statistically significant when p < 0.05. STATISTICA v 13.0 from StatSoft Inc. (StatSoft Inc., USA) was used for statistical analysis of the results.
Results
Energy and Nutritional Value of Diets
The mean total energy value of two diets was significantly different (1677.0 kcal for LCHF vs 1724.3 kcal for MFMC; p = 0.001) due to individual estimation of energy requirements. The individualization of the dietary plans contributed to increased adherence to the diet by participants. The total energy value of the LCHF diet ranged from 1390 to 2022 kcal/day, compared to 1480 to 2088 kcal/day in the MFMC diet. The total carbohydrate content of the LCHF diet was 29.8 g/day, which accounted for 6.1% of the energy value, and that of the MFMC diet was 189.4 g/day, which equaled 39.1% of the energy value (p < 0.001). The proportion of fat in the diet was 134.6 g/day (72.3% of energy value) for LCHF and 78.0 g/day (39.1% of energy value) for MFMC; p < 0.001. Both diets did not differ significantly in protein content (p = 0.076). Protein supply in both groups was not less than 0.8–1.0g/kg of body weight. The detailed energy and nutritional values of both interventional diets used are shown in Table 2.
 |
Table 2 Comparison of the Energy and Nutritional Value of the Interventional Diets (n = 91) |
Anthropometric Measurements Before and After Dietary Intervention
Of the 108 patients included in the study, 91 women completed the entire intervention period. Seventeen women did not adhere to the diets for 16 weeks, so they were excluded from the study (10 women for LCHF diet and 7 women for MFMC diet).
44.0% of all the patients were in stage 1 of lipedema (47.8% in LCHF group; 40.0% in MFMC group), 41.8% of them were in stage 2 (43.5% in LCHF group; 40.0% in MFMC group), 13.2% of them were in stage 3 (8.7% in LCHF group; 13.2% in MFMC group) and 1.1% was in stage 4 (2.2% in MFMC group). At baseline, no statistical differences were observed between groups for stage of lipedema (p = 0.42).
Based on mean BMI, 78.0% of all the patients were characterized as being overweight (BMI ≥ 25.0 kg/m2)30–78.3% in MCMF group and 77.8% in LCHF group. The most participants in both groups had obesity class I (BMI 30.0–34.9 kg/m2) – 34.8% in MCMF group and 26.7% in LCHF group. 10.9% and 22.2% of patients in MCMF and LCHF group had obesity class II (BMI 35.0–39.9 kg/m2), respectively. 13.0% of participants in MCMF group and 17.8% in LCHF group were characterized by obesity class III (BMI ≥40.0 kg/m2). Normal body weight (BMI < 25.0 kg/m2) occurred in 21.7% of patients in MCMF group and in 22.2% in LCHF group.
The percentage of patients with body fat greater than or equal to 30.0% of body weight accounted for 84.6% of all patients, with the largest proportion of patients with body fat greater than 40.0% of body weight (58.0% of all obese patients). Table 3 shows the comparison of age, anthropometric measurements and RMR between both interventional groups at baseline. Table 4 shows the comparison of anthropometric measurements before and after the dietary intervention. Figures 2 and 3 present photographic documentation of the lower extremities of three patients with lipedema before and after the LCHF diet; Figure 4 – two patients before and after MCMF diet.
 |
Table 3 Comparison of Age, Anthropometric Measurements and RMR at Baseline (n = 91) |
 |
Table 4 Comparison of Anthropometric Measurements Before and After Dietary Intervention (n = 91) |
 |
Figure 2 Lower limb photos of two patients (no. 1 and no. 2) with lipedema before and after the LCHF diet. Patient 1 and 2: (A) - photo before intervention; (B) - photo after intervention (own documentation). |
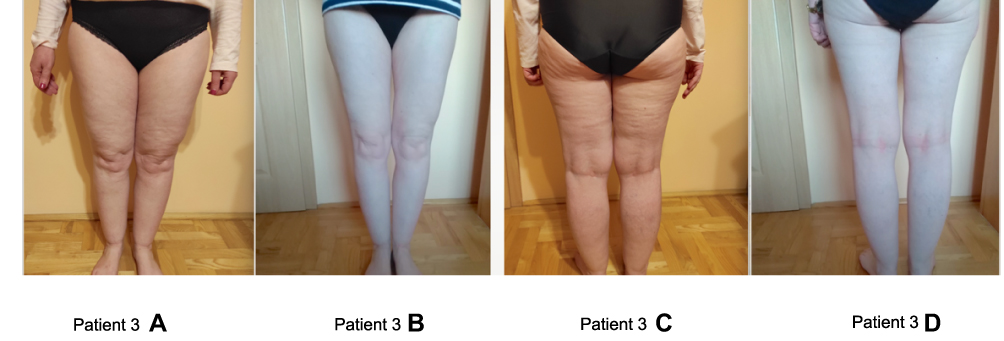 |
Figure 3 Lower limb photos of patient (no. 3) with lipedema before and after the LCHF diet. (A and C) - photos before intervention; (B and D) - photos after intervention (own documentation). |
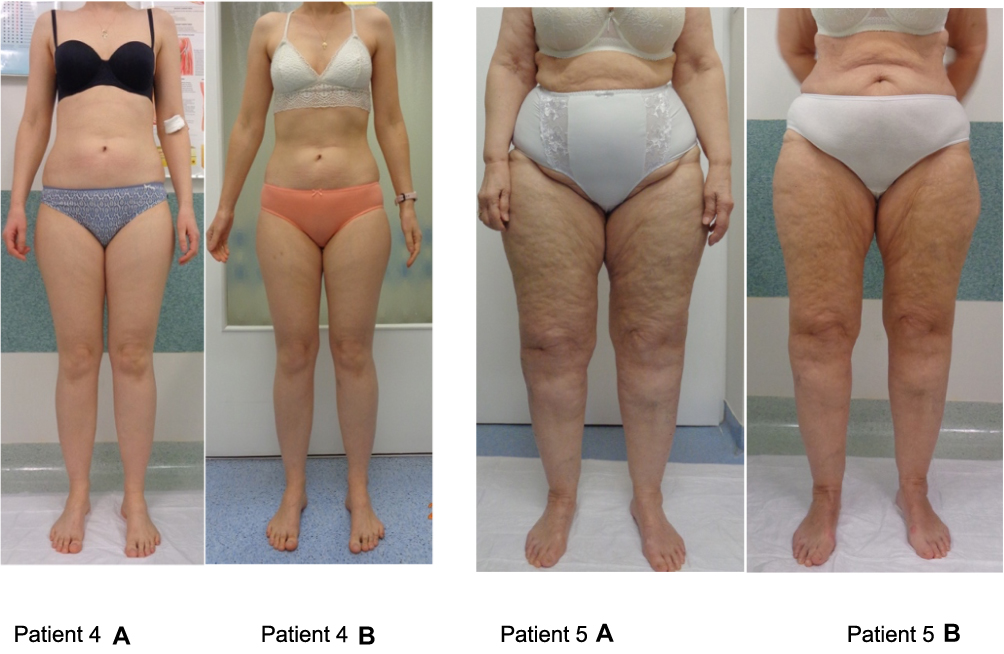 |
Figure 4 Lower limb photos of two patients (no. 4 and no. 5) with lipedema before and after the MCMF diet. Patient 4 and 5: (A) - photo before intervention; (B) - photo after intervention (own documentation). |
Discussion
Patients with lipedema typically follow restrictive, low-energy diets that often prove ineffective and result in increased hunger.2 Weight loss failures lead to compulsive eating and weight gain. An appropriate dietary strategy can break the vicious cycle of successive restrictive diets and simultaneous weight gain.9 Diet may slow the progression of the disease by inflammation and pain reduction, decrease tissue fluid content and improve quality of life.12 However, nutritional management should include body weight and body fat reduction through a tailored and caloric restriction diet.21 Caloric restriction is necessary because excess of energy is considered as pro-inflammatory.26 Energy expenditure was estimated using the indirect calorimetry (IC). IC is considered gold standard, especially when estimating actual energy requirement is complicated due to the disease. Main advantage of this method is to prevent overfeeding by precise assessment and control of patients’ energy requirements.31 Differences in the total energy values of the LCHF and MFMC diets were due to individual estimation of energy requirements and dependent on patient’s body weight. Both diets were iso-protein because the main purpose of the study was to determine efficacy of diets given the differences in fat and carbohydrate content. However, appropriate protein contents may prevent lean body mass reduction during body weight loss.32
The MFMC diet was more nutritionally balanced and characterized by significantly higher vitamin and mineral content (except for sodium, niacin, and riboflavin) compared to the LCHF diet. Data analysis showed that the LCHF diet was deficient in thiamine, folate, vitamin D as well as potassium, manganese, iodine, iron, calcium, magnesium and fiber. Conversely, the MFMC diet included insufficient iodine and vitamin D content relative to the recommended daily nutrient allowance for the Polish population.33 Implementation of deficient nutrients supplementation in LCHF diet can be remedied so women with lipedema can follow this diet long-term. Both diets maintained a ratio of n-6 to n-3 fatty acids of less than 4–5:1, which was to help reduce inflammation.27
The study was aimed to compare effectiveness of two diets with caloric restrictions and different fat and carbohydrate contents in body weight and anthropometric parameter reduction in patients with lipedema. Body weight, waist and hip circumference, body fat, lower extremity body fat content as well as thigh and calf circumference measurements were used to evaluate effectiveness of the diets. Because of the disproportionate lower extremity fat relative to upper body fat, BMI and body mass have been considered imperfect tools for assessing the prevalence of obesity.9,10 Waist circumference is considered more effective measure of obesity for the management of lipedema.10
Body weight and anthropometric parameters decreased significantly in both groups after 16 weeks, with one exception: no difference in circumference above the right ankle in MFMC diet. LCHF diet contributed to more significantly body weight, body fat and body circumferences reduction than MCMF diet (Table 4). Disproportion between upper and lower body decreased (Figures 2 and 3) but it was not so visible in patients in MCMF group (Figure 4). Additionally, we observed decrease of pain, swelling and increase of mobility and subjective improve patients’ quality of life in LCHF group, inversely to MFMC group (data not shown).
Diet for lipedema patients should include anti-inflammatory nutrients.12,19,21 Nourollahi et al34 demonstrated, limitation of pro-inflammatory nutrients and/or using herbal supplementation can be effective in lipedema treatment. Some nutrients can modulate inflammation in the body.35 Anti-inflammatory nutrients include vitamins (B6, niacin, folic acid, riboflavin, thiamine, beta-carotene, A, C, E, and D), minerals (selenium, zinc, magnesium), fatty acids (mono- and polyunsaturated: omega-3 and omega-6), fiber, polyphenols, components of herbs and spices (onion, garlic, turmeric, ginger, saffron, pepper, thyme, oregano, rosemary, and cloves), coffee (caffeine) as well as black and green tea. Pro-inflammatory components include an energy-dense diet high in carbohydrates, saturated fatty acids and trans fatty acids, cholesterol and fat, protein, iron, and vitamin B12.26 Mediterranean diet may contribute to inflammatory markers reduction due to its high content of antioxidant compounds such as polyphenols, tocopherols, resveratrol, vitamin C and vitamin A.19,36
Hyperinsulinemia is a major cause of chronic inflammation and insulin resistance may contribute to the onset of lipedema and it co-occur with visceral obesity.18,25,37 Treatment of hyperinsulinemia and insulin resistance is essential in lipedema management. Recent research showed that the gynoid adipose tissue was negatively correlated with insulin resistant, which suggested that lipodemic adipose tissue of the thighs, hips and buttocks may protect against metabolic disorders, including diabetes.16,25 Herbst et al38 demonstrated low incidence of type 2 diabetes in lipedema patients (2%) and concluded that lipodemic adipose tissue was not insulin resistant and may have contributed to reduce risk of diabetes. However, postprandial hyperglycemia contributes to the formation of Advanced Glycation End-Products (AGEs).38 AGEs contribute to increased insulin resistance and have been found to induce vascular endothelial growth factor (VEGF) and inflammatory responses in the body.39,40 There was a fourfold increase in VEGF levels in patients with lipedema compared to control group.41 Dietary VEGF inhibitors which may play a role in reducing inflammation include: polyphenols, flavonoids, anthocyanidins and proanthocyanidins, catechins, genistein, omega-3 fatty acids, lycopene, beta-cryptoxanthin, glucosinolates, isothiocyanates, indole-3-carbinol, 3,3’-diindolylmethane (DIM) (cruciferous vegetables), turmeric, vitamin K2, fermented foods, and prebiotics.42 Therefore, a low glycemic index diet, which avoids fluctuations in blood glucose and insulin levels, may be beneficial in the lipedema treatment.8,17,25
Di Renzo et al19 evaluated efficacy of a modified Mediterranean diet (mMeD) in body weight reduction in lipedema patients compared to women without lipedema for 4 weeks. The diet was mainly plant-based and included seasonal fruits and vegetables, whole meal cereal products, pulses, and nuts. Butter was replaced with oil, salt was replaced with herbs and spices, and products rich in polyunsaturated fatty acids were included. Canned and processed foods such as cured meats, canned products, ready-made and frozen foods, cheeses (except ricotta), potatoes, as well as foods with a high glycemic index, alcohol, and non-alcoholic sweetened beverages were excluded from the diet. Carbohydrate content was 40–45% of total energy, including 25g of fiber, protein content was 25–30% of total energy (>50% was plant-based protein), and fat content was 25–30% of total energy, <10% kcal/day SFA, 6–10% PUFA, 15% MUFA, <1% trans fatty acids, and the ratio of n-6 to n-3 fatty acids was 3:1. The authors assessed the patients’ quality of life using the European Quality of Life (EQ-5D) test. The obtained information included the intensity of pain and discomfort, anxiety and depression, as well as the ability to perform daily activities. The patients’ responses allowed to determine presence or absence of difficulties in daily activities and their intensity. After 4 weeks of dietary intervention, the authors observed a significant body weight and BMI reduction in both groups, with no significant differences in outcomes between the groups. Body weight significantly decreased by an average of 2.96 kg in the lipedema group (91.06 ± 28.63 kg in the lipedema group vs 88.1 ± 27.7 kg in the non-lipedema group). A significant lower and upper extremity body fat reduction was also observed after 4 weeks of diet in these patients (data not shown). Increase of daily physical activity abilities after diet was also demonstrated. Patients performed daily activities with less pain and fatigue, which contributed to quality of life improvement.
Keith et al2 hypothesized that the ketogenic diet may contribute to lipedema symptom reduction. Ketogenic diet used in lipedema patients may contribute to body weight, body fat and pain reduction which leads to quality of life improvement. The diet may cause metabolic and hormonal changes, contribute to tissue water and inflammation reduction, and also counteract tissue fibrosis. The diet increases adenosine levels, which may contribute to pain relief and anti-inflammatory effect. Ketogenic diet contributes to lower blood glucose and insulin levels.43 Nagpal et al44 indicated that a modified Mediterranean ketogenic diet can affect metabolic functions by modulating certain genes involved in carbohydrate and fat metabolism as well as immune functions, including inflammatory responses in the body. Ketogenic diet reduce hunger43,45,46 which may be helpful in lipedema patients characterized by leptin resistance.37 However, side effects such as constipation, unpleasant breath, headache, muscle cramps and weakness may be frequently observed. The association of ketogenic diet with lipid profile and the development of hepatic steatosis remains inconclusive. Therefore, it would be important to demonstrate relationship between ketogenic diet and lipid profile in lipedema patients.45
For the first time, low-carbohydrate and high-fat diet was found to be more effective in patients with lipedema compared to low-glycemic index diet. The limbs body fat reduction induced by a low-carbohydrate diet may be key in alleviating symptoms of the disease and improving patients’ quality of life. The results of this study may be crucial in implementing nutritional management in lipedema patients.
Diet effectiveness at body weight and body fat reduction depends on caloric restrictions but also on proportion of individual macronutrients.45 Nutritional management resulting in a long-term effect among lipedema patients to prevent the yo-yo effect is essential.18 A meta-analysis by Bueno et al46 found that low-carbohydrate diets (<50 g per day) are effective in weight reduction in long term (12 and 24 months). It would be reasonable to conduct a long-term efficacy of LCHF diet evaluation in lipedema patients. A pain scale before and after dietary intervention would be an added advantage. This study was also limited by lack of a control group including female patients without lipedema, so that effectiveness of the diet could be compared across different groups of individuals.
Conclusion
The LCHF diet was more effective than MFMC in body weight, body fat and lower limb circumferences reduction in patients with lipedema in this study.
Acknowledgments
The authors thank Andrzej Szuba and Angelika Chachaj from Department of Angiology, Hypertension & Diabetology, for referee of the patients to the Department of Dietetics, Faculty of Pharmacy (Wroclaw Medical University). The authors thank Monika Sowicz and Agnieszka Adaszyńska from Department of Angiology, Hypertension & Diabetology, for cooperation, including taking and sharing photos of patients with lipedema.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Szél E, Kemény L, Groma G, et al. Pathophysiological dilemmas of lipedema. Med Hypotheses. 2014;83(5):599–606. doi:10.1016/j.mehy.2014.08.011
2. Keith L, Seo CA, Rowsemitt C, et al. Ketogenic diet as a potential intervention for lipedema. Me Hypotheses. 2021;146:110435. doi:10.1016/j.mehy.2020.110435
3. Foeldi M, Foeldi E. F¨oldi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists. München: Elsevier Urban & Fischer; 2012.
4. Dayan E, Kim JN, Smith ML, et al. Lipedema – The Disease They Call Fat. The Lipedema Project at The Friedman Center for Lymphedema Research and Treatment in collaboration with Lymphatic Education & Research Network (LE&RN); 2017.
5. Erbacher G, Bertsch T. Lipoedema and pain: what is the role of the psyche? – Results of a pilot study with 150 patients with lipoedema. Phlebologie. 2020;49(5):305–316. doi:10.1055/a-1238-6657
6. Dudek JE, Białaszek W, Ostaszewski P, et al. Depression and appearance-related distress in functioning with lipedema. Psychol Health Med. 2018;23(7):846–853. doi:10.1080/13548506.2018.1459750
7. Alwardat N, Di Renzo L, Alwardat M, et al. The effect of lipedema on health-related quality of life and psychological status: a narrative review of the literature. Eat Weight Disord. 2020;25(4):851–856. doi:10.1007/s40519-019-00703-x
8. Reich-Schupke S, Schmeller W, Brauer WJ, et al. S1 guidelines: lipedema: guidelines. JDDG J Dtsch Dermatol Ges. 2017;15(7):758–767. doi:10.1111/ddg.13036
9. Wounds UK. Best Practice Guidelines: The Management of Lipoedema. London: Wounds UK; 2017.
10. Halk AB, Damstra RJ. First Dutch guidelines on lipedema using the international classification of functioning, disability and health. Phlebol J Venous Dis. 2017;32(3):152–159. doi:10.1177/0268355516639421
11. Damstra RJ, Halk AB, Damstra RJ, et al. The Dutch lymphedema guidelines based on the international classification of functioning, disability, and health and the chronic care model. J Vasc Surg Venous Lymphat Disord. 2017;5(5):756–765. doi:10.1016/j.jvsv.2017.04.012
12. Al-Ghadban SL, Herbst K, Bunnell B. Lipedema: a painful adipose tissue disorder. In: Szablewski L, editor. Adipose Tissue - an Update. IntechOpen; 2019. doi:10.5772/intechopen.88632
13. Child AH, Gordon KD, Sharpe P, et al. Lipedema: an inherited condition. Am J Med Genet A. 2010;152A(4):970–976. doi:10.1002/ajmg.a.33313
14. Crescenzi R, Donahue PMC, Petersen KJ, et al. Upper and lower extremity measurement of tissue sodium and fat content in patients with lipedema. Obesity. 2020;28(5):907–915. doi:10.1002/oby.22778
15. Buck DW, Herbst KL. Lipedema: a relatively common disease with extremely common misconceptions. Plast Reconstr Surg. 2016;4(9):e1043. doi:10.1097/GOX.0000000000001043
16. Torre YS-D, Wadeea R, Rosas V, et al. Lipedema: friend and foe. Horm Mol Biol Clin Investig. 2018;33(1):20170076. doi:10.1515/hmbci-2017-0076
17. Dudek JE, Białaszek W, Ostaszewski P. Quality of life in women with lipoedema: a contextual behavioral approach. Qual Life Res. 2016;25(2):401–408. doi:10.1007/s11136-015-1080-x
18. Bertsch T, Erbacher G, Corda D, et al. Lipoedema – myths and facts, part 5: European best practice of lipoedema – summary of the European lipoedema forum consensus. Phlebologie. 2020;49(01):31–50. doi:10.1055/a-1012-7670
19. Di Renzo L, Cinelli G, Romano L, et al. Potential effects of a modified Mediterranean diet on body composition in lipoedema. Nutrients. 2021;13(2):358. doi:10.3390/nu13020358
20. AL-Ghadban S, Cromer W, Allen M, et al. Dilated blood and lymphatic microvessels, angiogenesis, increased macrophages, and adipocyte hypertrophy in lipedema thigh skin and fat tissue. J Obes. 2019;2019:1–10. doi:10.1155/2019/8747461
21. Ehrlich C, Iker E, Herbst KL, et al. Lymphedema and Lipoedema Nutrition Guide. Foods, Vitamins, Minerals, and Supplements. San Francisco, CA, USA: Lymph Notes; 2015.
22. Gavin KM, Cooper EE, Hickner RC. Estrogen receptor protein content is different in abdominal than gluteal subcutaneous adipose tissue of overweight-to-obese premenopausal women. Metabolism. 2013;62(8):1180–1188. doi:10.1016/j.metabol.2013.02.010
23. Kruppa P, Georgiou I, Biermann N, et al. Lipedema—pathogenesis, diagnosis, and treatment options. Dtsch Ärztebl Int. 2020;117:396.
24. United Nations University; World Health Organization. Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation: Rome, 17–24 October 2001. Vol. 1. Rome, Italy: Food & Agriculture Organization of the United Nations; 2004.
25. Buso G, Depairon M, Tomson D, et al. Lipedema: a call to action! Obesity. 2019;27(10):1567–1576. doi:10.1002/oby.22597
26. Shivappa N, Steck SE, Hurley TG, et al. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689–1696. doi:10.1017/S1368980013002115
27. Schönenberger KA, Schüpfer AC, Gloy VL, et al. Effect of anti-inflammatory diets on pain in rheumatoid arthritis: a systematic review and meta-analysis. Nutrients. 2021;13(12):4221. doi:10.3390/nu13124221
28. Kunachowicz H, Nadolna J, Przygoda B, et al. Tabele składu i wartości odżywczej żywności [Food composition tables]. Warsaw, Poland: PZWL; 2005. In Polish.
29. U.S. Department of Agriculture, Agricultural Research Service. FoodData central; 2019. Available from: fdc.nal.usda.gov.
30. Euro World Health Organization; Fact Sheets: A healthy lifestyle - WHO recommendations, 6 May 2010. Available from: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi.
31. Delsoglio M, Achamrah N, Berger MM, et al. Indirect calorimetry in clinical practice. J Clin Med. 2019;8(9):1387. doi:10.3390/jcm8091387
32. Lobley GE, Johnstone AM, Fyfe C, et al. Glucose uptake by the brain on chronic high-protein weight-loss diets with either moderate or low amounts of carbohydrate. Br J Nutr. 2014;111(4):586–597. doi:10.1017/S0007114513002900
33. Jarosz M, Rychlik E, Stoś K, et al. Normy żywienia dla populacji Polski i ich zastosowanie [Human nutrition recommendations for Polish population]. Warsaw, Poland: Narodowy Instytut Zdrowia Publicznego - Państwowy Zakład Higieny; 2020. In Polish.
34. Nourollahi S, Mondry TE, Herbst KL. Bucher’s broom and selenium improve lipedema: a retrospective case study. Altern Integr Med. 2013;02(04). doi:10.4172/2327-5162.1000119
35. Minihane AM, Vinoy S, Russell WR, et al. Low-grade inflammation, diet composition and health: current research evidence and its translation. Br J Nutr. 2015;114(7):999–1012. doi:10.1017/S0007114515002093
36. Nordmann AJ, Suter-Zimmermann K, Bucher HC, et al. Meta-analysis comparing Mediterranean to low-fat diets for modification of cardiovascular risk factors. Am J Med. 2011;124:841–851. doi:10.1016/j.amjmed.2011.04.024
37. Coetzee O, Filatova D. Lipidema and lymphedema: the “leaky lymph,” weight loss resistance and the intestinal permeability connection. EC Nutr; 2017;11:233–243.
38. Herbst KL, Mirkovskaya L, Bharhagava A, et al. Lipedema fat and signs and symptoms of illness, increase with advancing stage. Arch Med. 2015;7(4):8.
39. Wierusz-Wysocka B, Araszkiewicz A, Schlaffke J. Końcowe produkty glikacji - nowy biomarker cukrzycy i jej powikłań? [Advanced glycation end products. A new biomarker of diabetes and late complications of disease?]. Diabetol Klin. 2013;3:96–103. In Polish.
40. Chen YJ, Chan DC, Chiang CK, et al. Advanced glycation end-products induced VEGF production and inflammatory responses in human synoviocytes via RAGE-NF-ΚB pathway activation: AGEs induce inflammation in synoviocytes. J Orthop Res. 2016;34(5):791–800. doi:10.1002/jor.23083
41. Szolnoky G, Nemes A, Gavallér H, et al. Lipedema is associated with increased aortic stiffness. Medicines. 2022;9. doi:10.3390/medicines9080041
42. Li WW, Li VW, Hutnik M, et al. Tumor angiogenesis as a target for dietary cancer prevention. J Oncol. 2012;2012:1–23. doi:10.1155/2012/879623
43. Dowis K, Banga S. The potential health benefits of the ketogenic diet: a narrative review. Nutrients. 2021;13(5):1654. doi:10.3390/nu13051654
44. Nagpal R, Neth BJ, Wang S, et al. Modified Mediterranean-ketogenic diet modulates gut microbiome and short-chain fatty acids in association with Alzheimer’s disease markers in subjects with mild cognitive impairment. EBioMedicine. 2019;47:529–542. doi:10.1016/j.ebiom.2019.08.032
45. Freire R. Scientific evidence of diets for weight loss: different macronutrient composition, intermittent fasting, and popular diets. Nutrition. 2020;69:110549. doi:10.1016/j.nut.2019.07.001
46. Bueno NB, de Melo ISV, de Oliveira SL, et al. V.ry-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Br J Nutr. 2013;110(7):1178–1187. doi:10.1017/S0007114513000548
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.