Back to Journals » Nature and Science of Sleep » Volume 17

The Dyadic Relationship of Illness Uncertainty, Social Support, and Coping Styles in Patients with OSA and Their Co-Residents: An Actor-Partner Interdependence Mediation Model Analysis
Authors Niu Y ![]() , Shao Y, Chen L, Zhang X
, Shao Y, Chen L, Zhang X ![]()
Received 6 August 2025
Accepted for publication 20 September 2025
Published 8 October 2025 Volume 2025:17 Pages 2501—2516
DOI https://doi.org/10.2147/NSS.S558190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yuqi Niu, Yefan Shao, Linlin Chen, Xiaochun Zhang
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of China Medical University, Shenyang City, Liaoning Province, People’s Republic of China
Correspondence: Xiaochun Zhang, The First Affiliated Hospital of China Medical University, 155 North Nanjing Street, Heping District, Shenyang City, Liaoning Province, People’s Republic of China, Email [email protected]
Background: Obstructive Sleep Apnea (OSA) patients experience significant illness uncertainty, impacting coping. Social support mitigates uncertainty, while coping styles influence management. Research predominantly examines individual patients, neglecting dyadic interactions between patients and co-residents.
Objective: To examine the dyadic interrelationships of illness uncertainty, social support, and coping styles in OSA patient–co-resident pairs using the Actor–Partner Interdependence Model (APIM).
Methods: A cross‑sectional study of 242 patient–co‑resident dyads from a tertiary hospital examined self‑reported illness uncertainty, social support, and coping styles. APIM analyzed actor and partner effects.
Results: Patients reported higher illness uncertainty (P< 0.001), whereas co‑residents reported greater social support (P< 0.001). Social support was positively associated with active coping and negatively associated with passive coping within dyads. Actor effects indicated that illness uncertainty in both patients and co-residents was associated with lower levels of their own social support, which in turn correlated with decreased active coping and increased passive coping (β=0.203 and 0.038, P< 0.05). Partner effects analyses indicated that one member’s uncertainty or social support was associated with the other member’s coping via specific indirect paths.
Conclusion: The findings reveal bidirectional, dyadic interdependence among illness uncertainty, social support, and coping styles in OSA patient–co-resident pairs, with social support appearing as a prominent within‑individual associative pathway. These results support considering family‑oriented strategies that aim to strengthen mutual social support to be explored further as a means to promote adaptive coping in this population.
Keywords: obstructive sleep apnea, illness uncertainty, social support, coping styles, actor-partner interdependence model
Introduction
Obstructive sleep apnea (OSA) is a growing respiratory disorder marked by recurrent airway collapse during sleep, affecting approximately 936 million adults aged 30–69 worldwide, with an estimated prevalence of 11% in China.1,2 Factors such as rising obesity, smoking, and an aging population contribute to this growing burden.3 OSA presents with symptoms like snoring, daytime sleepiness, and cognitive issues, but its subtle and non-specific nature often delays diagnosis, increasing the risk for cardiovascular and neurocognitive disorders.4–6 Worryingly, fewer than 50% of affected individuals recognize their condition, and under 5% seek treatment, leading to significant underdiagnosis and undertreatment.7 Thus, despite its high prevalence and serious complications, OSA remains poorly understood by patients, causing delays in therapy and uncertainty in management.
Illness uncertainty arises from impaired interpretation of health-related information,8 is increasingly recognized in chronic conditions. For patients with OSA, this uncertainty is particularly pronounced due to several unique disease characteristics. OSA patients struggle to evaluate disease severity and prognosis due to symptom dissociation (nocturnal events and daytime sequelae), comorbidities, and long-term treatment demands.6 Although Continuous Positive Airway Pressure (CPAP) therapy and lifestyle modifications are effective, the long-term nature of CPAP treatment and challenges related to comfort and adherence significantly exacerbate management complexity and uncertainty.9 Co-residents face parallel challenges from chronic sleep disruption, emotional strain, and caregiving burdens.10,11 The co-residents experiences impaired sleep quality directly caused by the patient’s nocturnal symptoms (loud snoring, apneas), alongside emotional strain and caregiving burdens.10 Evidence links illness uncertainty to reduced treatment adherence, aggravated anxiety/depression, and impaired patient-family-clinician communication.12–14 While dyadic interactions are documented in chronic populations,15 no studies have explored this dynamic in OSA patient-co-resident dyads. Managing the nighttime symptoms of OSA presents unique challenges that necessitate active co-residents involvement, particularly in supporting and monitoring CPAP adherence, a factor critical to treatment success yet distinct from many other chronic diseases.
Social support and coping styles critically modulate illness uncertainty.16,17 Support networks mitigate uncertainty through informational and emotional buffering, accounting for 23.1% of variance in uncertainty levels,18 while adaptive coping enhances psychological resilience and clinical outcomes.19,20 Traditional research, however, neglects dyadic interactions in disease management. The Actor-Partner Interdependence Model (APIM) addresses this gap by disentangling actor effects (intra-individual variable-outcome relationships) from partner effects (inter-individual cross-over influences), providing a robust framework to examine OSA-related social support, coping, and uncertainty within dyads.
This study employs APIM to analyze paired data from OSA patient-co-resident dyads, elucidating interrelationships among illness uncertainty, social support, and coping styles. The research findings will provide an evidence base for designing family-centred interventions, thereby enhancing understanding of and interventions targeting psychosocial factors in the long-term management of OSA.
Methods
Design
This study employed a cross-sectional design with convenience sampling. Participants (patient-co-resident dyads) were recruited between June 2024 and December 2024 from the Sleep Monitoring Unit of the Department of Respiratory and Critical Care Medicine at a tertiary care hospital in Shenyang, China.
Participants
All participants were informed that their participation in the study was entirely voluntary and that they could withdraw at any time. Written and verbal consent was obtained from all participants. OSA patients and their co-residents were enrolled only if they met predefined inclusion and exclusion criteria (Specific inclusion and exclusion criteria are shown in Table 1).
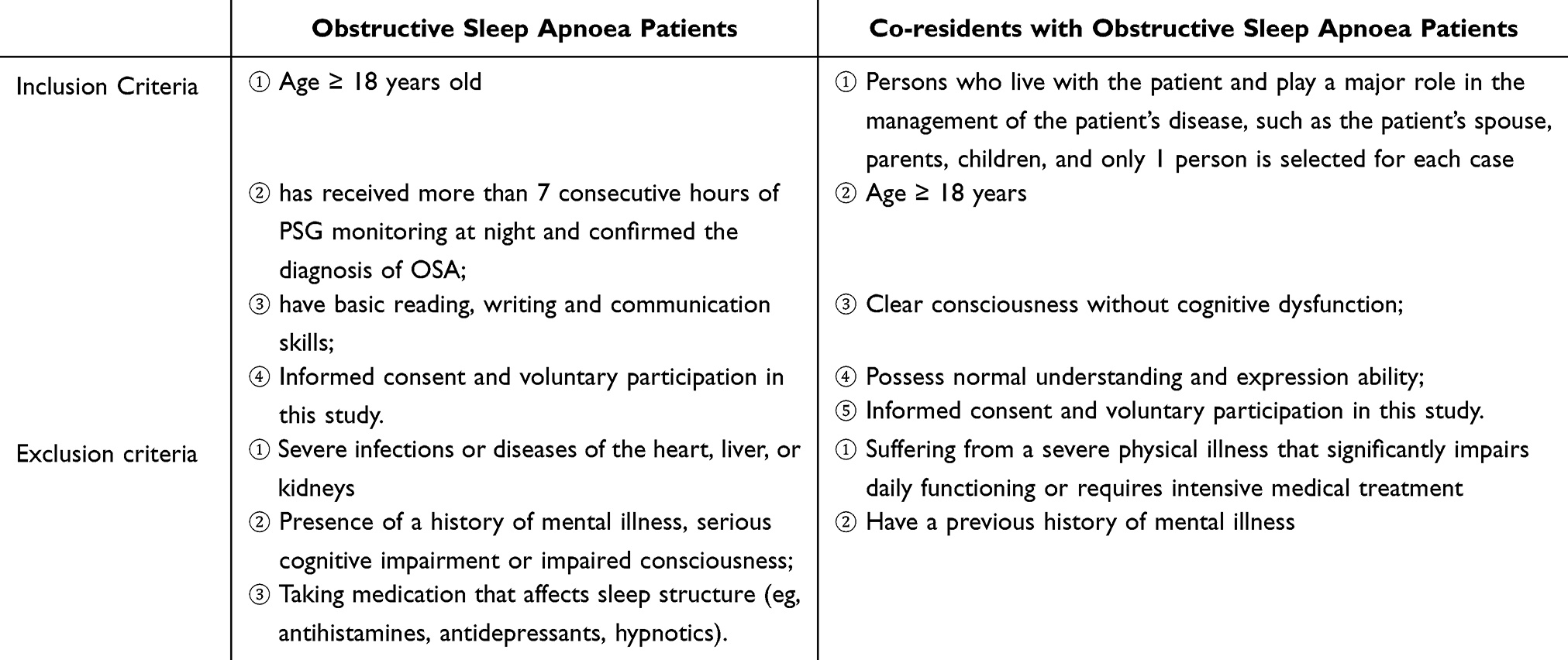 |
Table 1 Inclusion and Exclusion Criteria for Patients with Obstructive Sleep Apnoea and Their Co-Residents |
Data Collection
The sample size was calculated using G*power3.1. Based on a multifactorial analysis with an assumed medium effect size f2 = 0.25,21 two-tailed α=0.05, 1-β=0.85, the required sample size was 220 dyads (440 participants). To account for a 10% attrition rate and invalid responses, we planned to recruit 242 dyads (484 participants). Following standardized training in instrument administration and quality control, researchers conducted the survey. Both patients and co-residents independently completed the questionnaires. Before beginning, researchers explained the informed consent process and provided instructions without intervention. All questionnaires were reviewed on-site upon completion, and any missing or inconsistent entries were promptly clarified and corrected with the participants.
Instruments
Patient Section
General Information Questionnaire
A self-designed General Information Questionnaire was utilized to collect demographic and disease-related data.
Mishel’s Uncertainty in Illness Scale for Adults (MUIS-A)
The MUIS-A, originally developed by Mishel et al17 was adapted into Chinese by Hsu Shu-Lian.22 This 33-item scale comprises four subscales: ambiguity (13 items), complexity (7 items), lack of information (7 items), and unpredictability (5 items). The Chinese version demonstrates strong reliability (Cronbach’s α=0.872),22 with subscale α coefficients ranging 0.772–0.857.
Co-Resident Section
General Information Questionnaire
Co-resident demographics included sex, age, ethnicity, educational level, marital status, employment status, monthly household income, and relationship to the patient.
Mishel’s Uncertainty in Illness Scale for Family Members (MUIS-FM)
The MUIS-FM17 was translated and validated by Cui Hongyan.23 This 30-item Chinese version includes four subscales: ambiguity (13 items), complexity (8 items), lack of information (5 items), and unpredictability (4 items). The original scale demonstrates Cronbach’s α=0.89 and content validity=0.87.17
Shared Patient-Co-Resident Instruments
To facilitate dyadic analysis via the Actor-Partner Interdependence Model (APIM), identical scales were administered to both patients and co-residents.
Social Support Rating Scale (SSRS)
The SSRS, developed by Xiao Shuiyuan24 and revised in 1990, assesses perceived social support through 10 items across three dimensions: subjective support (items 1,3–5), objective support (items 2,6–7), and support utilization (items 8–10). The scale demonstrates strong internal consistency (total α=0.78; subscales: 0.73–0.88).25
Simplified Coping Style Questionnaire (SCSQ)
Developed by Xie Yaning26 for Chinese populations, this 20-item tool measures two coping dimensions: active coping (items 1–12) and passive coping (items 13–20). The scale shows excellent reliability (total α=0.90; subscales: α=0.89 and 0.79, respectively).26
For a detailed description of the research instruments, please refer to the Supplementary Materials.
Ethical Consideration
The study was granted ethical approval by the Research Ethics Committee of the First Affiliated Hospital of China Medical University Approval No. [2024]1020 and was conducted in accordance with the principles set forth in the Declaration of Helsinki.
Data Analysis
Data entry and verification were performed using EpiData 3.1 software. Statistical analyses were conducted with SPSS 26.0 and Amos 28.0, with a significance threshold of P<0.05 for all tests.
Statistical Description
Demographic characteristics, disease-related variables, illness uncertainty scores, social support scores, and coping style scores underwent statistical and normality analyses. Normally distributed variables were reported as mean ± standard deviation (SD), non-normally distributed continuous variables as median and interquartile range (IQR), and categorical variables as frequencies and percentages.
Univariate Analysis
For normally distributed illness uncertainty, social support, and coping style scores: Independent samples t-tests and one-way ANOVA were used to identify influencing factors of these variables in OSA patients and co-residents. Paired t-tests compared score differences between patients and co-residents. Pearson correlation analysis assessed relationships among illness uncertainty, social support, and coping styles. For non-normally distributed data, non-parametric tests and Spearman correlation analysis were applied.
Multivariate Analysis
A multiple linear regression model was constructed with coping style scores as the dependent variable. Independent variables included demographic characteristics, illness uncertainty, and social support identified as statistically significant in univariate and correlation analyses.
Structural Equation Modeling
Actor–Partner Interdependence Mediation Models (APIM) were developed using Amos 28.0 to examine relationships among illness uncertainty, social support, and coping styles in patient–co-resident dyads. The APIM framework was chosen because our primary research questions concern both actor effects and partner effects within naturally paired data.
To determine the appropriate specification for our paired data, we conducted a distinguishability test by comparing a saturated model (including all actor and partner paths without equality constraints) with an alternative constrained model that imposed equality constraints by setting actor effects equal to partner effects. A chi-square difference test was used to compare the two models. Following common practice, a non-significant chi-square difference (P>0.20) was interpreted as evidence that the dyads are empirically indistinguishable and that the constrained model is acceptable; a significant chi-square difference supports retaining the less constrained specification. Path-specific actor and partner effects were examined. Mediation effects were tested using a bias-corrected bootstrap method with 5000 resamples.
Results
Descriptive Characteristics
The final analysis included 242 dyads (484 participants) of OSA patients and their co-residents. The mean age of patients was 47.25±17.84 years (range: 18–86 years), while co-residents had a mean age of 44.22±11.74 years (range: 19–76 years). Patients were predominantly male (71.1%), whereas co-residents were mostly female (72.3%), with spouse/partner relationships being the most common (61.6%). Patients exhibited significant clinical characteristics: 57.9% reported severe snoring, 41.7% had snoring duration >10 years, 72.7% had a family history of OSA, and 62.0% had ≥3 chronic comorbidities. The mean BMI was 28.17±4.65 (obesity threshold ≥28), apnea-hypopnea index (AHI) was 32.97±23.49 (moderate-severe OSA threshold AHI ≥15). Neck circumference (38.83±4.41cm), waist circumference (98.67±11.47cm), and hip circumference (102.76±9.50cm) all exceeded healthy population standards. Socioeconomic data revealed that 85.5% of patients used urban resident/employee medical insurance, 44.2% had a monthly household income of 418–694 USD per capita, and occupational distribution was highest in “private sector salaried employee” categories, followed by civil servant salaried employee and students. Detailed information is provided in Table 2 and Supplementary Table 1.
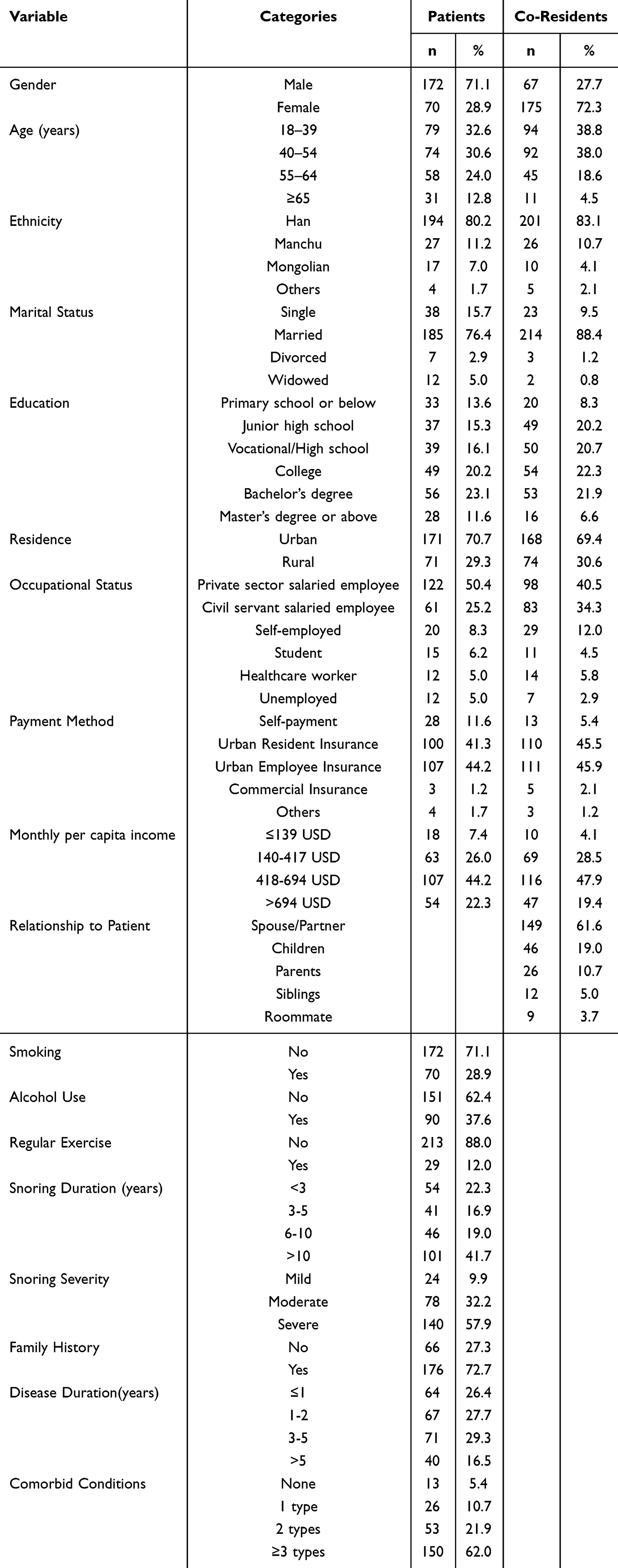 |
Table 2 Demographic and Clinical Characteristics of OSA Patients and Their Co-Residents |
Status of Three Variables in Patients and Their Co-Residents
Illness Uncertainty
Patients reported significantly higher total illness uncertainty scores than co-residents (100.85±10.17 vs 96.42±9.22, t=8.191, P<0.001, d=0.53). Subscale differences were significant for complexity (16.80±2.15 vs 20.66± 2.99, P<0.001, d=−1.29), unpredictability (15.30±2.38 vs 11.37±1.79, P<0.001, d=1.66), and information deficiency (23.73±2.76 vs 18.76±2.19, P<0.001, d=1.78). No significant difference was observed in the ambiguity subscale (P=0.091). Notably, the overall illness uncertainty difference (d=0.53) represents a moderate standardized effect, whereas some subscale contrasts show large effects, indicating clinically meaningful differences in specific dimensions of uncertainty between patients and co‑residents.
Social Support
Co-residents exhibited significantly higher total social support scores than patients (43.31±3.22 vs 41.09±4.78, t=−7.284, P<0.001, d=−0.47). Subscale analysis revealed significant differences in subjective support (23.97±2.31 vs 22.27±2.98, P<0.001, d=−0.58). Differences in objective support (P=0.051, d=−0.13) and support utilization (P=0.054, d=0.12) did not reach conventional significance thresholds and their effect sizes are small, suggesting limited practical divergence between groups on these dimensions.
Coping Styles
Patients had a slightly higher total coping style score than co‑residents (28.14±4.74 vs 27.00±5.69, t=2.952, P=0.003, d=0.19), which corresponds to a small standardized effect. Passive coping differed significantly (11.68 ± 6.67 vs 9.79 ± 5.03, P<0.001, d=0.31), indicating a small-to-moderate effect size, whereas active coping showed no statistical difference (P=0.123, d=−0.10). Overall, several contrasts yield statistically significant but small standardized effects. Detailed scores for each of the other dimensions are shown in Table 3.
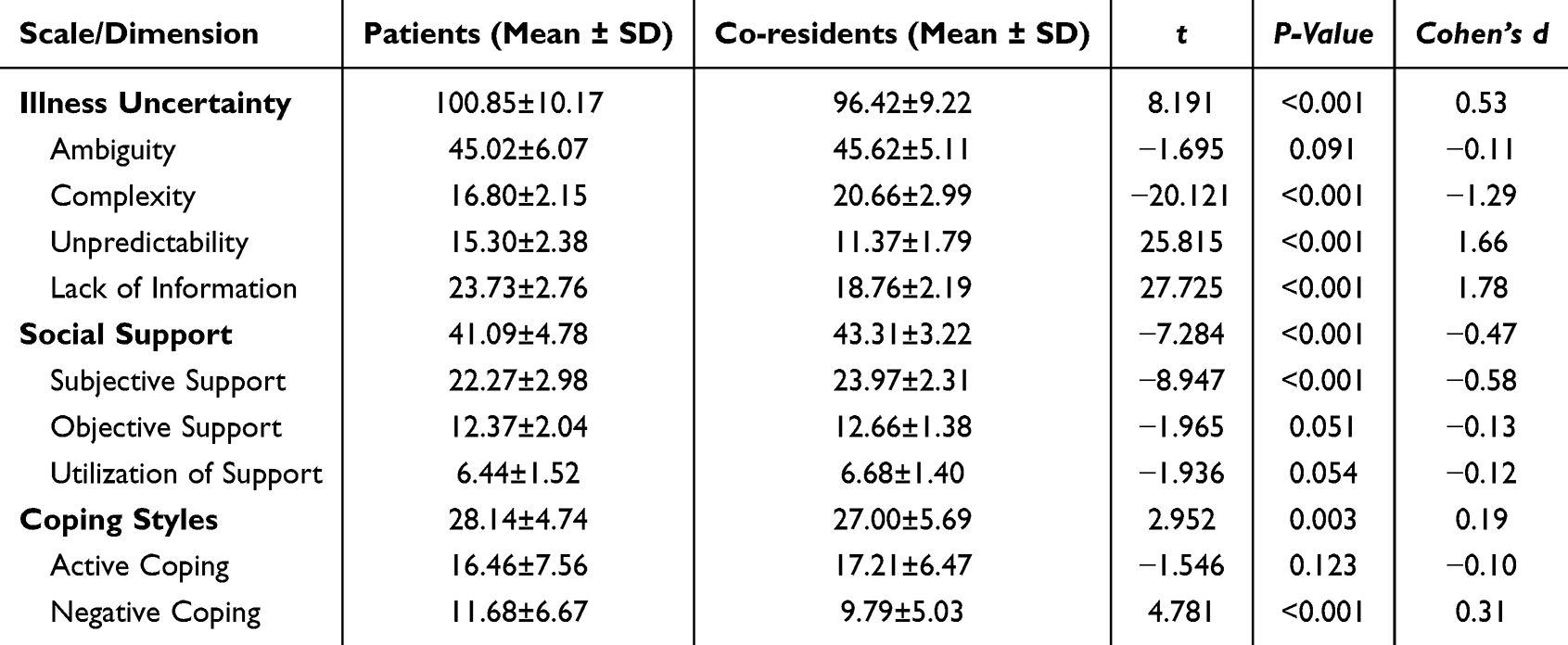 |
Table 3 Comparison of Differences in Illness Uncertainty, Social Support, and Coping Styles Between OSA Patients and Their Co-Residents |
Univariate Analysis
Univariate analysis revealed group differences in illness uncertainty, social support, and coping styles between OSA patients and co-residents (Supplementary Table 2 and Supplementary Table 3).
In patients with OSA, females reported higher total illness uncertainty than males (103.63±11.59 vs 99.72±9.34, P=0.013), with scores increasing stepwise with age (≥65 years: 110.13±8.50 vs 18–39 years: 95.90±9.47, P<0.001). Rural patients had higher uncertainty than urban counterparts (108.54±8.74 vs 97.65±8.96, P<0.001), and those with elementary education scored highest (110.91±7.08, P<0.001 vs higher-educated groups). Clinical parameters (BMI: r=0.201; AHI: r=0.298) showed significant positive correlations with illness uncertainty (P<0.01). Unemployed exhibited the highest illness uncertainty (105.42±10.60, P<0.001). Rural co-residents (100.64±9.54) scored higher than urban counterparts (P<0.001), and low-educated individuals (106.25±5.67) exceeded higher-educated groups (P<0.001).
Aspects of social support, male patients scored higher than females (41.69±4.56 vs 39.60±5.02, P=0.002). High-income patients (>694 USD: 41.89±4.83) outperformed low-income groups (P<0.001). Among co-residents, students reported the highest social support (42.55±2.81), and high-income groups (>694 USD: 44.13±3.02) surpassed low-income counterparts (P=0.010).
Aspects of coping styles, Patients’ passive coping increased significantly with disease duration (>5 years: 14.05±5.58 vs ≤12 months: 9.53±6.53, P=0.002). Patients with bachelor’s degrees or higher had the highest active coping scores (19.84±7.36, P< 0.001). Co-resident private sector salaried employee exhibited the highest passive coping (12.91±6.93, P=0.039), with low-income groups (≤139 USD: 16.80±4.49) exceeding high-income counterparts (P<0.001). Urban-rural disparities significantly influenced illness uncertainty (patients: P<0.001; co-residents: P<0.001) and coping styles, while economic status inversely correlated with illness uncertainty (patients: P<0.001; co-residents: P<0.001).
Correlation Analysis Results
The correlation analysis (see Table 4) demonstrated significant associations between illness uncertainty, social support, and coping styles in patients and co-residents. Patients’ illness uncertainty exhibited a negative correlation with social support (r=−0.411, P<0.01) and a positive correlation with passive coping (r= 0.538, P< 0.01). A strong positive correlation was observed between patients’ social support and active coping (r=0.745, P<0.01). Cross-individual analysis revealed a moderate positive correlation between patients’ and co-residents’ illness uncertainty (r= 0.628, P< 0.01), indicating mutual cognitive influence.
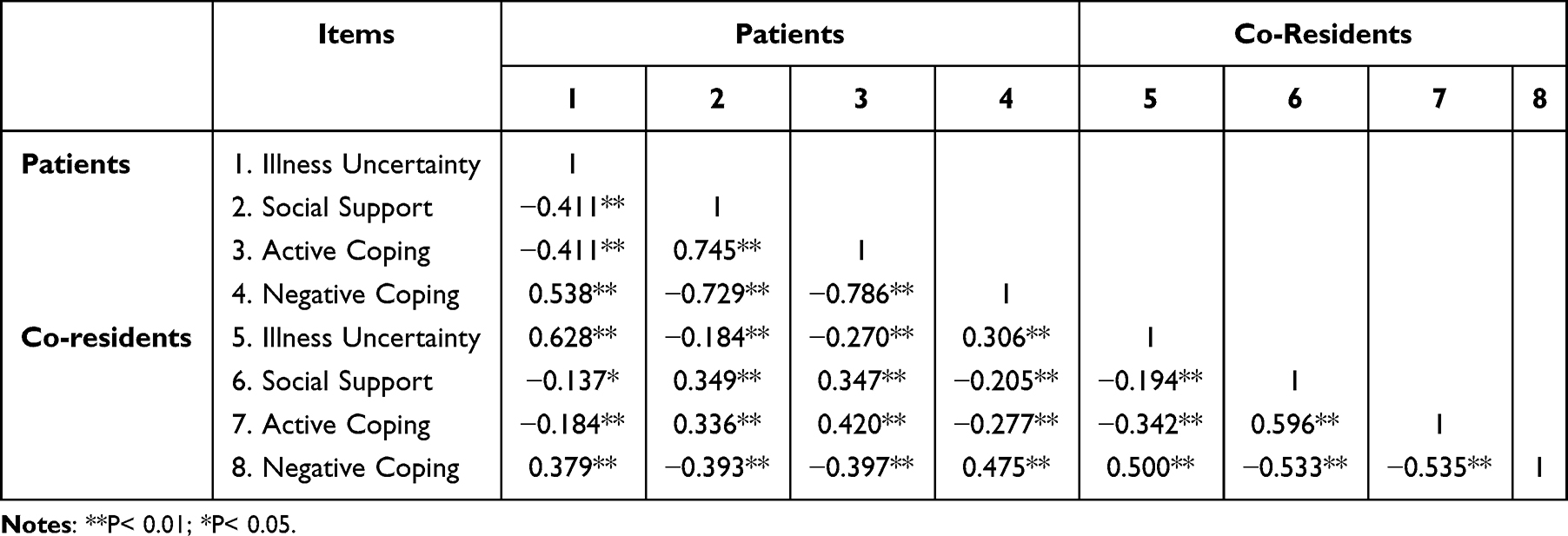 |
Table 4 Bivariate Correlation Matrix of Variables Between Patients and Co-Residents |
Co-residents’ social support positively correlated with their own active coping (r=0.596, P<0.01) and negatively with patients’ passive coping (r=−0.393, P<0.01). Significant dyadic correlations included patients’ and co-residents’ passive coping (r=0.475, P<0.01), co-residents’ active coping and social support (r=0.420, P<0.01), and patients’ illness uncertainty with co-residents’ passive coping (r=0.379, P<0.01). A weak positive correlation between co-residents’ and patients’ social support (r=0.349, P<0.01) suggested systemic synergy. All correlations were statistically significant (P<0.05 or P<0.01), reflecting complex psychosocial interdependence.
Regression Analysis Results
Multivariable linear regression models identified multiple factors associated with coping styles. In the patient active coping model (See Table 5), mid-income (418–694 USD /month: β=0.464, P=0.001) and regular exercise (β=0.154, P=0.017) were positively associated with higher active coping. Illness uncertainty was negatively associated with active coping (β=−0.222, P=0.009), while co‑resident social support was positively associated with patient active coping (β=0.313, P<0.001). The model explained approximately 33.6% of the variance (ΔR²=11.0%). The patient passive coping model (Supplementary Table 5) showed that mid‑income (β=−0.530, P< 0.001), physical inactivity (β=−0.161, P=0.008), and disease duration >5 years (β= 0.197, P=0.009) were associated with passive coping. Illness uncertainty was positively associated with passive coping (β=0.446, P<0.001), and co‑resident social support was negatively associated with passive coping (β=−0.157, P=0.005). This model explained about 34.3% of variance.
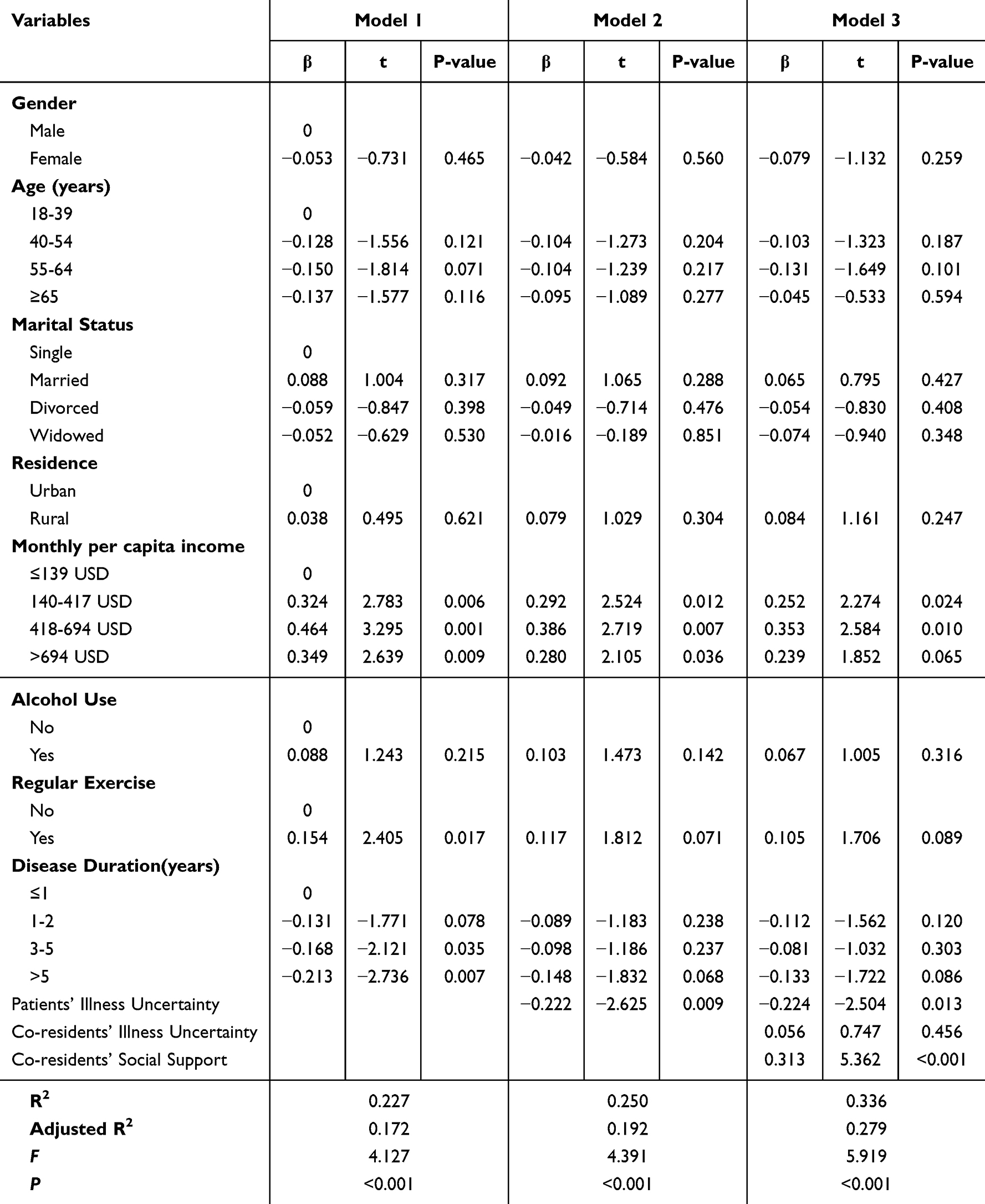 |
Table 5 Multiple Linear Regression Analysis of Patients’ Positive Coping Styles |
For co-resident active coping (Supplementary Table 7), Manchu ethnicity was a baseline correlate (β=0.147, P=0.021). Co‑resident illness uncertainty showed a negative association with their active coping (β=−0.438, P<0.001), and patient social support was positively associated with co‑resident active coping (β=0.320, P<0.001); the explained variance increased from 20.1% to 36.8% with these variables. The co-resident passive coping model (Supplementary Table 8) identified age 55–64 years (β=0.201, P=0.010) and Mongolian ethnicity (β=0.176, P=0.004) as correlates, and high income (>694 USD/month: β=−0.468, P=0.005) was negatively associated with passive coping. Illness uncertainty (β=0.385, P<0.001) and patient social support (β=−0.326, P<0.001) were associated with approximately 38.6% of explained variance. All models reached statistical significance (P<0.001) and showed no problematic multicollinearity (VIF<2.5). Dummy‑coding details are provided in Supplementary Tables 4 and 6.
Actor-Partner Interdependence Mediation Model of Illness Uncertainty, Social Support, and Coping Styles in OSA Patients and Co-Residents
Mediation Model of Social Support Between Illness Uncertainty and Active Coping
We constructed an actor-partner interdependence mediation model (APIMeM) with illness uncertainty as the independent variable, social support as the mediator, and active coping as the dependent variable for OSA patients and co-residents. We tested whether the paired observations could be treated as indistinguishable by comparing a saturated APIM (no path constraints) with a constrained APIM in which actor and partner effects were set equal. The two models were compared using a chi-square difference test. The chi-square difference test yielded P=0.015, indicating a significant difference between the saturated and constrained models; therefore, the dyads in our sample are empirically distinguishable and the constrained (equal-effects) specification is not supported. On this basis, we retained the saturated APIM specification for primary analyses. Therefore, the model is saturated (model fit indices: X²and df both 0; CFI, GFI, NFI all 1; RMSEA 0), demonstrating good model fit (Figure 1). Direct and indirect effects of illness uncertainty on active coping are presented in Table 6.
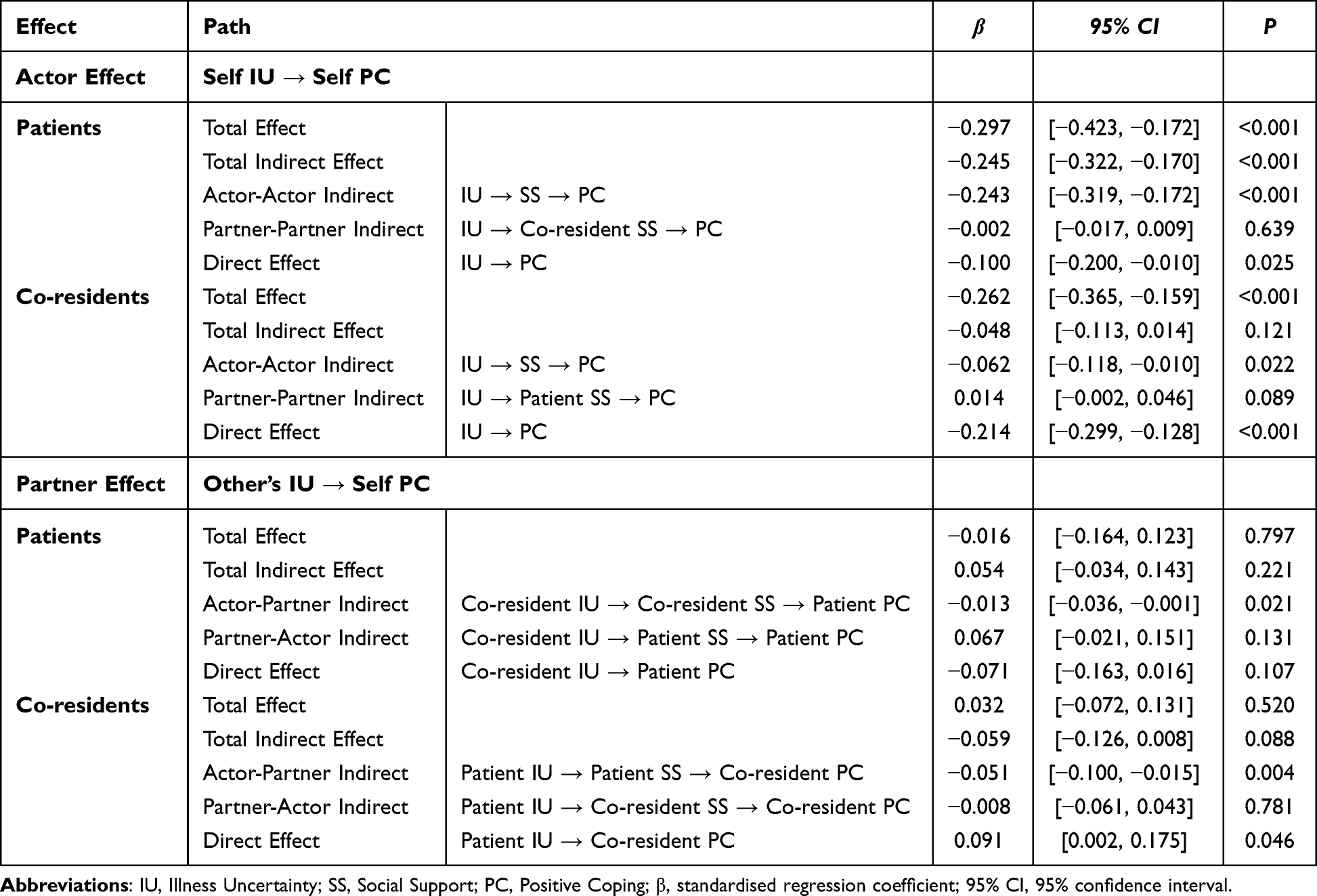 |
Table 6 Actor-Partner Interdependence Mediation Effects of Social Support Between Illness Uncertainty and Positive Coping Styles |
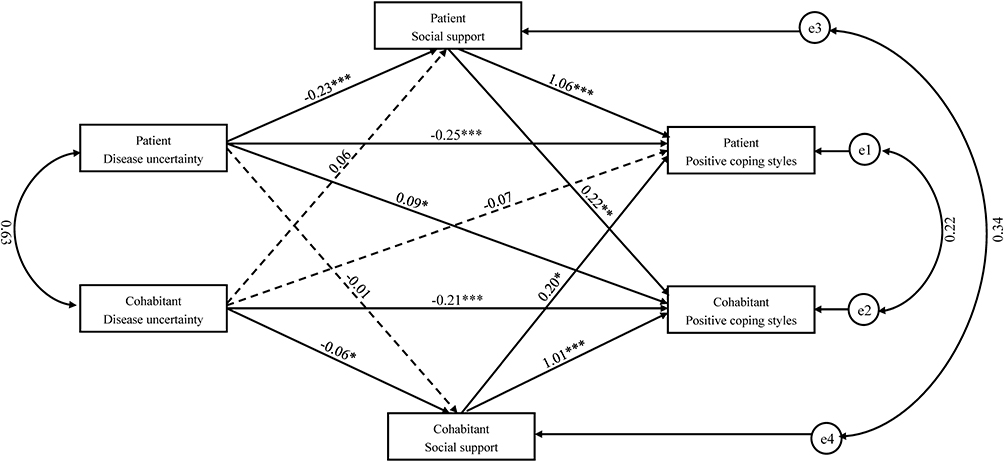 |
Figure 1 The Actor-Partner Interdependence Mediation Model of Social Support Between Illness Uncertainty and Positive Coping Styles. Notes: Dashed lines indicate insignificant path coefficients and solid lines indicate significant path coefficients. *P<0.05, **P<0.01, ***P<0.001. |
Within‑individual (subject/actor) associations: Patients’ own illness uncertainty was negatively associated with their active coping in the cross‑sectional analysis (total association β=−0.297, P<0.001). Decomposing the cross‑sectional paths showed that the patient’s own social support (subject→subject path) was associated with this total association (β=−0.243, P<0.001) and accounted for approximately 81.82% of the total association; the direct path remained statistically significant but small in magnitude (β=−0.100, P=0.025). Co‑residents’ own illness uncertainty was also negatively associated with their active coping (β=−0.262, P<0.001); in co‑residents the social support path was only partially related to this association (subject–subject pathway: β=−0.062, P=0.022), while the direct path represented the main cross‑sectional association (β=−0.214, P<0.001).
Cross‑partner (object/partner) associations: Cross‑subject associations differed between patients and co‑residents. Although the total cross‑sectional association from co‑resident uncertainty to patient active coping was not significant (β=−0.016, P=0.797), there was a small but significant cross‑sectional indirect association via co‑resident social support (co‑resident uncertainty → co-residents social support → patients positive coping styles; β=−0.013, P=0.021). Conversely, the total association from patient uncertainty to co‑resident active coping was not significant (β=0.032, P=0.520), but a significant negative cross‑sectional indirect association existed via patient social support (patient uncertainty → patient social support → co‑resident active coping; β=−0.051, P=0.004), while the direct cross‑sectional association in that model was positive and significant (β=0.091, P=0.046). These cross‑sectional patterns indicate that individual illness uncertainty is associated with changes in one’s own social support and active coping, while cross‑partner associations tend to appear through specific social‑support transmission pathways, with co‑existing direct and indirect cross‑sectional associations.
Overall, both patients’ and co‑residents’ illness uncertainty were associated in cross‑sectional analyses with lower active coping, and these associations were more strongly reflected within individuals through their own social support. Cross‑partner associations were primarily observed through particular cross‑sectional indirect paths.
Mediation Model of Social Support in the Interdependence Between Illness Uncertainty and Negative Coping Strategies
This study constructs a mediation model of interdependence using illness uncertainty in patients with obstructive sleep apnea and their cohabiting partners as the independent variable, social support as the mediator, and negative coping strategies as the dependent variable. The model is saturated (model fit indices: X²and df both 0; CFI, GFI, NFI all 1; RMSEA 0), demonstrating good model fit, as shown in Figure 2. The direct and indirect effects of illness uncertainty on negative coping strategies are presented in Table 7.
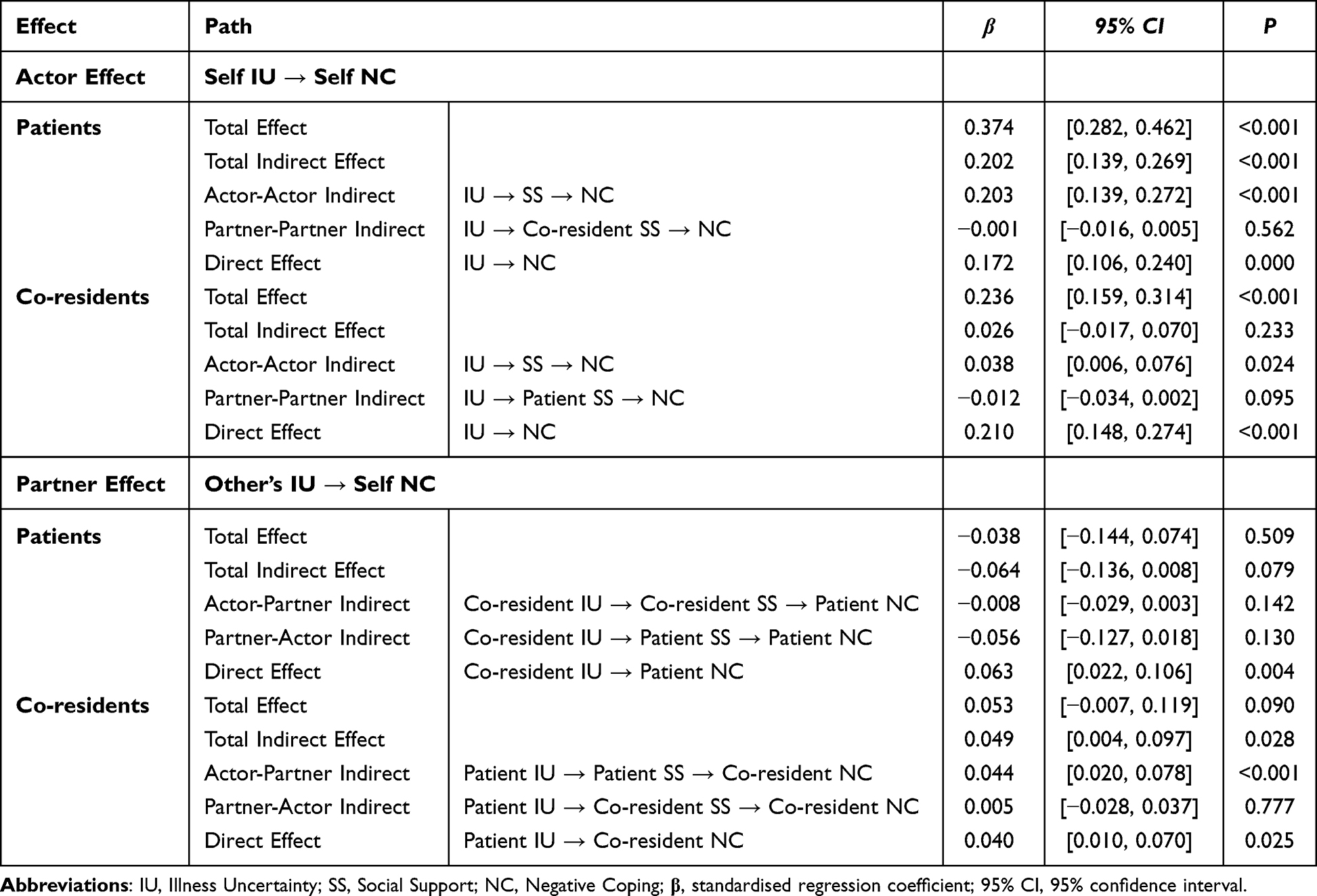 |
Table 7 Actor-Partner Interdependence Mediation Effects of Social Support Between Illness Uncertainty and Negative Coping Styles |
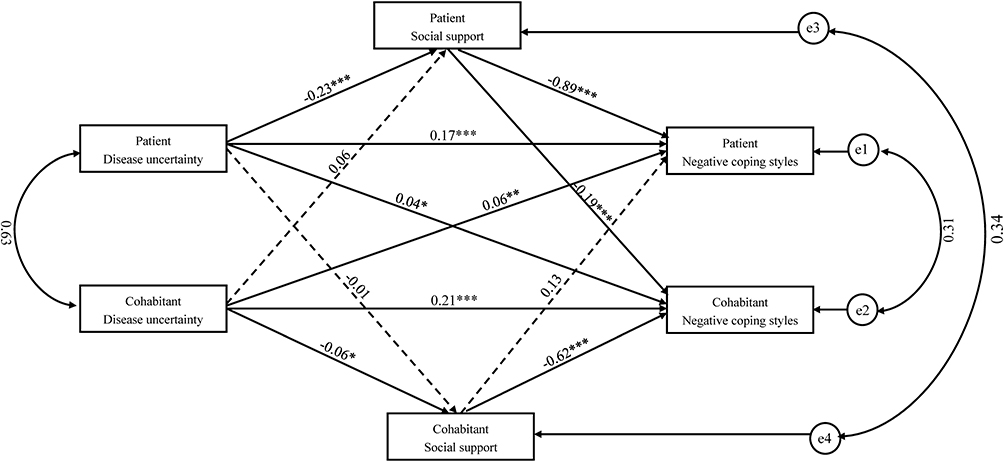 |
Figure 2 The Actor-Partner Interdependence Mediation Model of Social Support Between Illness Uncertainty and Negative Coping Styles. Notes: Dashed lines indicate insignificant path coefficients and solid lines indicate significant path coefficients. *P<0.05, **P<0.01, ***P<0.001. |
In the cross‑sectional analysis, patients’ illness uncertainty was positively associated with their own negative coping (total effect β=0.374, P<0.001). The cross‑sectional indirect association via patients’ own social support (actor→actor) was significant (β=0.203, P<0.001), whereas the cross‑sectional partner→partner indirect association via cohabiting partners’ social support was not significant (β=−0.001, P=0.562). The direct cross‑sectional association remained significant (β =0.172, P<0.001).
Similarly, cohabiting partners’ illness uncertainty was positively associated with their own negative coping in cross‑sectional analysis (total association β=0.236, P<0.001). The actor→actor cross‑sectional indirect association via their own social support was significant (β=0.038, P=0.024); the direct association was also significant (β=0.172, P<0.001).
Regarding cross‑partner associations, cohabiting partners’ illness uncertainty was positively associated with patients’ negative coping in cross‑sectional analysis (β=0.063, P=0.004). Patient illness uncertainty was associated with cohabiting partners’ negative coping through both a direct cross‑sectional association (β=0.040, P=0.025) and a cross‑sectional indirect association via patient social support (patient uncertainty → patient social support → partner negative coping; β=0.044, P<0.001). Overall, these cross‑sectional findings indicate that social support is more prominently associated as an intra‑individual pathway in the relation between illness uncertainty and negative coping, while cross‑partner associations were mainly present in the patient→partner direction in this dataset.
All descriptions above are deliberately framed as exploratory cross‑sectional associations estimated by APIM; longitudinal or interventional designs are required to test temporal ordering and causal mediation.
Discussion
This study employed the APIM to investigate the interplay of illness uncertainty, social support, and coping strategies within OSA patient–co-resident dyads. The APIM framework allows separation of actor effects (how an individual’s own uncertainty or support relates to their own coping) from partner effects (how one member’s uncertainty or support relates to the other member’s coping).
The findings revealed multidimensional characteristics of illness uncertainty, with rural residents and individuals with lower education levels exhibiting heightened uncertainty, likely attributable to disparities in healthcare accessibility and health literacy.27 Poor health literacy may exacerbate challenges in disease management and decision-making, potentially amplifying illness uncertainty.28 Notably, dose-response relationships were observed between patients’ BMI and AHI with illness uncertainty, suggesting that physiological deterioration may intensify psychological distress through symptom perception.29,30 This finding corroborates the impact of OSA-specific diurnal-nocturnal symptom dissociation on illness perception.1
Dimensional analysis further revealed patients’ highest “information deficiency” scores versus co-residents’ “complexity” scores, highlighting dual challenges in symptom recognition (patients) and treatment comprehension (co-residents).31 Targeted interventions using personalized visual aids are recommended for high-risk groups (eg, elderly and less-educated individuals) to mitigate uncertainty.
Social support analysis showed co-residents scored significantly higher than patients (43.31±3.22 vs 41.09±4.78; P<0.001). High-income groups (>694 USD) exhibited 21.7% greater objective support (P<0.001), underscoring economic capital’s role in healthcare access.32 Occupational differences in co-residents’ support networks and age-stratified declines in social support mirror Tutuncu’s observations of aging-related support attenuation.33 While co-residents reported superior subjective support, nonsignificant objective support differences suggest systemic deficiencies in family-centered care resources.
Intergenerational coping differences revealed older patients employed more negative strategies than younger counterparts, consistent with Charles’ findings on reduced coping resilience in aging populations.34 Patients’ negative coping scores exceeded co-residents’, with a 37.2% increase per 5-year disease progression (β=0.197), aligning with Mishel’s chronic illness adaptation curve.35 Higher education correlated with improved active coping (bachelor’s degree: 19.84±7.36), echoing Huang’s emphasis on health literacy.20 These findings suggest the development of a patient-co-resident dichotomous intervention programme to improve patients’ coping patterns by empowering co-residents with social support.
Multivariate regression quantified relationships: patients’ social support explained 33.6% of active coping variance (β=0.313, P<0.001), while illness uncertainty explained 34.3% of negative coping variance (β=0.446, P<0.001). Cross-dyad analyses confirmed co-residents’ support explained 31.3% of patients’ active coping variance (β=0.313), consistent with family buffering mechanisms,36 potentially amplified by OSA’s nocturnal symptomatology.
In addition, although several comparisons and regression coefficients reached statistical significance, many reported standardized effect sizes are small. Hence, statistical significance observed here does not necessarily equate to clinical importance at the individual level. They may signal modest population-level associations or contribute cumulatively with other factors. To address these limitations, future research should employ multicentre or population-based sampling to improve external validity, adopt longitudinal or interventional designs to establish temporal and potentially causal relationships.
APIM revealed bidirectional mechanisms: patients’ illness uncertainty reduced active coping via diminished self-support (actor–actor path: 81.82% effect), while co-residents’ uncertainty influenced negative coping through “patient support → co-resident coping” pathways (β=0.044, P<0.001). These results extend systemic interaction models to respiratory chronic care,37 advocating mutual support systems integrating patient education and co-resident training in symptom monitoring and CPAP supervision. In future clinical practice, a family-based model of integrated OSA management can be established to include co-residents in the health education system for more effective disease management.
Compared with dyadic research in other chronic illnesses, OSA presents with distinctive characteristics: the nocturnal onset of symptoms, the pivotal role of bed partners in symptom recognition and treatment adherence, and the technical complexity of device-based therapies. These OSA‑specific aspects likely amplify the importance of partner knowledge and practical involvement (eg, monitoring mask fit, troubleshooting device issues), and they help explain why co‑resident support explained a substantial portion of variance in patients’ active coping (cross‑dyad β=0.313). Thus, while parallels exist with dyadic processes observed in other chronic conditions, the pathways identified here have particular operational relevance for OSA management.
Limitations
This study employed a cross‑sectional survey design, which limits conclusions to contemporaneous associations and precludes determination of temporal precedence or causal relationships among illness uncertainty, social support, and coping styles. We recruited participants by convenience sampling from a single tertiary hospital in Shenyang, which may have introduced selection bias. The sample’s single‑centre origin may therefore limit the generalizability of the findings. In light of these limitations, we recommend that future studies use multicentre or population‑based sampling strategies, adopt longitudinal designs to track intervention effects, and include objective physiological measures to validate the associations between psychosocial variables and clinical outcomes.
Conclusion
This study employed the Actor-Partner Interdependence Model to examine the dyadic relationships between illness uncertainty, social support, and coping styles in OSA patients and their co-residents. The findings reveal significant actor and partner effects, highlighting the interdependence within dyads. These findings provide empirical evidence of the relationship between co-resident relationships and patients’ illness cognition and coping strategies, demonstrating that effective illness management necessitates a dual perspective encompassing both patients and their co-residents.
To translate these findings into practice, clinical interventions should not only focus on the patient but also integrate co-residents into support and educational programs to foster mutual support and collaborative disease management. Looking forward, future research should prioritize longitudinal designs to trace the evolution of these dyadic relationships over time, as well as interventional studies that test tailored support strategies aimed at mitigating illness uncertainty and enhancing dyadic coping in OSA.
Abbreviations
OSA, Obstructive Sleep Apnoea; APIM, Actor-Partner Interdependence Model; APIMeM, Actor-Partner Interdependence Mediation Model; CPAP, Continuous Positive Airway Pressure; AHI, apnea-hypopnea index; MUIS-A, Mishel’s Uncertainty in Illness Scale for Adults; MUIS-FM, Mishel’s Uncertainty in Illness Scale for Family Members; SSRS, Social Support Rating Scale; SCSQ, Simplified Coping Style Questionnaire.
Data Sharing Statement
As the material analysed in this study contains sensitive personal data, the datasets generated and analysed are not publicly available and can be obtained from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was granted ethical approval by the Research Ethics Committee of the First Affiliated Hospital of China Medical University Approval No. [2024]1020 and was conducted in accordance with the principles set forth in the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study.
Acknowledgments
We extend our sincere gratitude to all participants and research team members.
Author Contributions
Yuqi Niu: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. Yefan Shao: Validation, Visualization, Formal analysis, Writing – review & editing. Linlin Chen: Conceptualization, Methodology, Supervision, Writing – review & editing. Xiaochun Zhang: Supervision, Validation, Project Administration, Writing – review & editing.
All authors have approved the final version of the paper for publication, agreed to submit this work to the current journal, and accept full accountability for all aspects of the research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. The Lancet Respiratory Medicine. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
2. Niu Y, Sun S, Wang Y, Chen L, Shao Y, Zhang X. Spatiotemporal Trends in the Prevalence of Obstructive Sleep Apnoea Across China: a Multilevel Meta-Analysis Incorporating Geographic and Demographic Stratification (2000-2024). Nature and Science of Sleep. 2025;17:879–903. doi:10.2147/NSS.S525547
3. Platon AL, Stelea CG, Boișteanu O, et al. An Update on Obstructive Sleep Apnea Syndrome-A Literature Review. Medicina (Kaunas, Lithuania). 2023;59(8). doi:10.3390/medicina59081459.
4. Sisson CB. A clinical review of obstructive sleep apnea. JAAPA: Official Journal of the American Academy of Physician Assistants. 2023;36(10):10–15. doi:10.1097/01.JAA.0000977668.78287.0c
5. Arredondo E, Udeani G, Panahi L, Taweesedt PT, Surani S. Obstructive Sleep Apnea in Adults: what Primary Care Physicians Need to Know. Cureus. 2021;13(9):e17843. doi:10.7759/cureus.17843
6. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive Sleep Apnea and Cardiovascular Disease: a Scientific Statement From the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
7. Pan Y, Wang D, Han D. Meta-analysis of the prevalence of obstructive sleep apnoea hypoventilation syndrome in adults in China. Medical Information. 2019;32(7):73–77.
8. Mishel MH, Braden CJ. Finding meaning: antecedents of uncertainty in illness. Nursing Research. 1988;37(2):98–103,127. doi:10.1097/00006199-198803000-00009
9. Van Loenhout L, Van der Zeijden H. An Unusual Cause of CPAP Intolerance. JCSM. 2019;15(10):1535–1537.
10. Ye L, Malhotra A, Kayser K, et al. Spousal involvement and CPAP adherence: a dyadic perspective. Sleep Medicine Reviews. 2015;19:67–74. doi:10.1016/j.smrv.2014.04.005
11. Rosa D, Amigoni C, Rimoldi E, et al. Obstructive Sleep Apnea and Adherence to Continuous Positive Airway Pressure (CPAP) Treatment: let’s Talk about Partners! Healthcare. 2022;10(5):943. doi:10.3390/healthcare10050943
12. Akberzie W, Hesselbacher S, Aiyer I, Surani S, Surani ZS. The Prevalence of Anxiety and Depression Symptoms in Obstructive Sleep Apnea. Cureus. 2020;12(10):e11203. doi:10.7759/cureus.11203
13. Wallace DM, Williams NJ, Sawyer AM, et al. Adherence to positive airway pressure treatment among minority populations in the US: a scoping review. Sleep Medicine Reviews. 2018;38:56–69. doi:10.1016/j.smrv.2017.04.002
14. Bonsignore MR, Mazzuca E, Baiamonte P, Bouckaert B, Verbeke W, Pevernagie DA. REM sleep obstructive sleep apnoea. European Respiratory Review: an Official Journal of the European Respiratory Society. 2024;33(171):230166. doi:10.1183/16000617.0166-2023
15. Guan T, Chapman MV, de Saxe Zerden L, et al. Illness uncertainty and quality of life in patients with advanced cancer and their family caregivers: an actor-partner interdependence model analysis. Psycho-Oncology. 2023;32(11):1744–1751. doi:10.1002/pon.6228
16. Mishel MH. Reconceptualization of the uncertainty in illness theory. Image--the Journal of Nursing Scholarship. 1990;22(4):256–262. doi:10.1111/j.1547-5069.1990.tb00225.x
17. Mishel MH. Uncertainty in illness. Image--the Journal of Nursing Scholarship. 1988;20(4):225–232. doi:10.1111/j.1547-5069.1988.tb00082.x
18. Wu S, Guo X, Tang H, et al. The Relationship Between Illness Uncertainty and Social Support Among Cancer Patients: a Meta-analysis. Cancer Nursing. 2024;48(5):416–423. doi:10.1097/NCC.0000000000001328
19. Chen SH, Liu ZQ. Correlation between uncertainty and coping styles in patients with acute myocardial infarction. Journal of Nursing: Comprehensive Edition. 2001;16(8):471–472.
20. Cc H, Hm R, Xy L. Disease uncertainty status after thyroid cancer surgery and the effects of coping styles and negative emotions. International Journal of Psychiatry. 2023;50:841–843.
21. Chang L, Xinchun W. Paired Patterns of Subject-Object Interdependence and Their Verification. Psychological Development and Education. 2017;33(01):105–112.
22. Xu SL, Huang XL, Lin HH. Disease uncertainty and coping behaviours of hospitalised patients with acute myocardial infarction. Taiwan Medicine. 1998;2(5):498–508.
23. Hongyan C. A study on the correlation between illness uncertainty and social support and coping styles among family members of patients with chronic diseases. dissertation, Yanbian University; 2010.
24. Xiao S. Theoretical basis and research application of the Social Support Rating Scale. Journal of Clinical Psychiatry. 1994;4(2):98–100.
25. Ji-Wen LIU, Fu-Ye LI, Yu-Long L. Reliability and validity of social support scale. Journal of Xinjiang Medical University. 2008;2008:1–3.
26. Xie Y. A preliminary study of the reliability and validity of the Brief Coping Style Scale. Chinese Journal of Clinical Psychology. 1998;6(2):114–115.
27. Busse AJ, Freilinger S, Eicken A, et al. Healthcare status of adults with pulmonary hypertension due to congenital heart disease. Cardiovasc Diagn Ther. 2022;12(6):840–852. doi:10.21037/cdt-22-281
28. Li JJ, Appleton SL, Wittert GA, et al. The relationship between functional health literacy and obstructive sleep apnea and its related risk factors and comorbidities in a population cohort of men. Sleep. 2014;37(3):571–578. doi:10.5665/sleep.3500
29. Yang L, He Z, Gu X, Cheng H, Li L. Dose-Response Relationship Between BMI and Hyperuricemia. International Journal of General Medicine. 2021;14:8065–8071. doi:10.2147/IJGM.S341622
30. Guglielmi O, Jurado-Gámez B, Gude F, Buela-Casal G. Job stress, burnout, and job satisfaction in sleep apnea patients. Sleep Medicine. 2014;15(9):1025–1030. doi:10.1016/j.sleep.2014.05.015
31. Luyster FS, Strollo Jr PJ, Zee PC, Walsh JK. Sleep: a health imperative. Sleep. 2012;35(6):727–734. doi:10.5665/sleep.1846
32. de Breij S, Huisman M, Deeg DJH. Macro-level determinants of post-retirement health and health inequalities: a multilevel analysis of 18 European countries. Social Science & Medicine. 2020;245:112669. doi:10.1016/j.socscimed.2019.112669
33. Tutuncu R, Karabulut H, Acar B, Babademen MA, Ciftçi B, Karaşen RM. Obstructive sleep apnea syndrome (OSAS) and social support in elder patients. Archives of Gerontology and Geriatrics. 2012;55(2):244–246. doi:10.1016/j.archger.2011.07.014
34. Charles ST, Piazza JR, Mogle JA, Urban EJ, Sliwinski MJ, Almeida DM. Age Differences in Emotional Well-Being Vary by Temporal Recall. The Journals of Gerontology Series B, Psychological Sciences and Social Sciences. 2016;71(5):798–807. doi:10.1093/geronb/gbv011
35. Mishel MH. Uncertainty in acute illness. Annual Review of Nursing Research. 1997;15(1):57–80. doi:10.1891/0739-6686.15.1.57
36. Yeh PM, Bull M. Use of the resiliency model of family stress, adjustment and adaptation in the analysis of family caregiver reaction among families of older people with congestive heart failure. International Journal of Older People Nursing. 2012;7(2):117–126. doi:10.1111/j.1748-3743.2011.00275.x
37. Ivziku D, Clari M, Piredda M, De Marinis MG, Matarese LR. Anxiety, depression and quality of life in chronic obstructive pulmonary disease patients and caregivers: an actor–partner interdependence model analysis. Quality of Life Research: an International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation. 2019;28(2):461–472. doi:10.1007/s11136-018-2024-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Social Support on the Mental Health Literacy of Parents Who Have Children with Special Needs: A Moderated Mediating Effect
Du X, Dong Q, Sun L, Chen X, Jiang J
Psychology Research and Behavior Management 2024, 17:1283-1294
Published Date: 20 March 2024
Fear of Cancer Recurrence and Its Associated Factors in Bladder Cancer Patients of Different Age Stages: A Cross-Sectional Study
Li J, Bai L, Yan S, Niu J, Li S, Ning X
Cancer Management and Research 2025, 17:2653-2664
Published Date: 8 November 2025