")
Back to Journals » Journal of Inflammation Research » Volume 16
The Disease Experience of Women with Granulomatous Lobular Mastitis. A Qualitative Interview Study
Authors Wang YT , Tang YQ, Xu JY, Bian XM
Received 29 April 2023
Accepted for publication 25 August 2023
Published 28 September 2023 Volume 2023:16 Pages 4347—4361
DOI https://doi.org/10.2147/JIR.S419347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yan Ting Wang,1,* Ya Qin Tang,2 Jia Yuan Xu,1 Xue Mei Bian2,*
1School of Nursing, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2Department of Nursing, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xue Mei Bian, Department of Nursing, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Tel +8613588492353, Email [email protected]
Background: The incidence of granulomatous lobular mastitis (GLM) is increasing year by year, and the breast wounds of women patients with GLM can develop into abscesses, fistulas, sinuses, and sometimes orange-like degeneration similar to malignant tumors, which seriously affects the quality of life of women patients with GLM. In China, breast wounds in women patients with GLM have not been better managed. Therefore, the purpose of this study is to explore the disease experience of women patients with GLM, to provide a basis for the development of precise intervention and support strategies for women patients with GLM, and to further improve the quality of nursing management and enrich the research types of GLM.
Methods: In this study, 10 cases of GLM women patients from a tertiary hospital in Hangzhou, Zhejiang Province were selected by purposive sampling. After obtaining the informed consent of GLM women patients, semi-structured interviews were conducted with GLM women patients using the interview outline to collect qualitative data. The interview was recorded, transcribed verbatim in the local language, and then translated into English, and the content analysis method was used to analyze the data. The Consolidated Criteria for Reporting Qualitative Research (CORE-Q) checklist follows the report ‘s findings.
Results: Our study identified six themes: (a) Perception of the disease, (b) Emotional discomfort (c) Variety of changes (d) Lack of specific skills (e) Coping strategies adopted to rebuild health, (f) Expectation.
Conclusion: The experience of women with GLM is characterized by diversity and specificity. After experiencing physical trauma, most patients use support systems to change negative attitudes and rebuild physical and mental health. Family, hospital and society should be fully linked to strengthen the prevention of GLM and the popularization of nursing management knowledge; nurses should provide targeted nursing services. Nursing leaders should improve the medical security system, broaden the medical channels, and reduce the pain experience and pressure of patients.
Keywords: granulomatous lobular mastitis, non-puerperal mastitis, qualitative study, nursing
Background
Granulomatous lobular mastitis (GLM) is a sterile chronic inflammatory disease of the breast.1 GLM can occur in both men and women, but mostly young women of childbearing age with a history of breastfeeding and childbearing.2 Its etiology and pathogenesis are still unclear.3 Studies have shown that nipple depression, trauma, viruses, bacterial and parasitic infections, hyperprolactinemia, breastfeeding, oral contraceptives, family history of breast cancer, diabetes, autoimmune dysfunction can induce GLM4–8 Chinese medicine believes that: Emotional distress, of qi and blood stasis, breast milk deposition;9 or viscera dysfunction;10 postpartum exogenous wind-cold-dampness- evil;11 careless living, Chong Ren imbalance can also lead to the occurrence of GLM.12 At present, there is no uniform treatment standard and scheme for GLM. Some studies have pointed out that surgical treatment cannot completely cure GLM.13 Studies have pointed out that the incidence and recurrence rate of GLM have increased year by year.14 It is particularly common in developing countries in the Mediterranean and Asia, such as China.15 In clinical work, it was found that nulliparous women, adolescent women and elderly male patients also suffer from GLM,16 which has attracted the attention of researchers around the world. Because GLM is similar to breast cancer in imaging and clinical manifestations, GLM is easily misdiagnosed as breast cancer, which leads to miscut breast tissue and destroys the morphological aesthetics of breast.17 The course of GLM is long and recurrent. The local tissue of the breast has redness, swelling, pain, ulcers, fistula.18,19 Accompanied by symptoms such as lower limb joint pain and erythema. It seriously affects normal social activities, and causes a great physiological and psychological burden on patients.
Through clinical work and literature review, it was found that women patients with GLM had a low awareness of the disease, and most patients did not pay attention to it at the beginning of the disease. When women patients with GLM in remote areas were treated in primary hospitals, primary hospitals were often misdiagnosed as acute mastitis according to the clinical manifestations of the disease, which delayed the best treatment of the disease and increased the economic burden of treatment. In addition, patients often seek surgical treatment for unbearable long-term breast pain and breast skin ulceration. However, most patients after surgery, the breast will still appear congestion, swelling, fever and pain, and even in the breast wound there are still a lot of pus flow. Although many studies have shown that oral corticosteroids can effectively reduce the scope of surgical resection of breast tissue, and even reduce the surgical needs of some GLM women patients, long-term use of corticosteroids may lead to many complications, such as weight gain, osteoporosis, liver and kidney function damage.20 During the development of GLM, deep or subcutaneous abscesses are easy to form at the breast lesions, and can gradually develop into fistulas in the late stage.21 Studies have pointed out that chronic wounds formed by breast ulceration in women patients with GLM require long-term debridement, dressing change and other interventions to promote wound healing.22 However, the breast is different from other parts of the body. The structure of the breast tissue is special and the breast belongs to the sensitive part of the human body, and the tolerance to pain is low. On the other hand, the necrotic substances and pus in the mammary duct are difficult to clean up. In the process of debridement and dressing change, patients still need to endure severe pain after taking analgesics. This state of repeated pus, pain and prolonged healing of the breast wound has caused great changes in the physical and mental state of women patients with GLM, such as the emergence of negative emotions, reduced self-confidence in life, low self-efficacy, breast pain, and decreased sleep quality.
Due to the lack of authoritative unified path and treatment guidelines for GLM management, the management of women patients with GLM is challenging for medical staff who care for a large number of women patients with GLM in clinical practice. On the other hand, the current research on GLM at home and abroad mainly focuses on quantitative research such as disease mechanism, treatment methods, and recurrence factors. There is a lack of attention to the disease experience of women patients with GLM, and there are few studies on disease management of GLM patients. In order to better provide appropriate help to women patients with GLM and provide disease management support for medical staff engaged in nursing GLM women patients, we need to understand their inner world and disease experience. Therefore, this study comprehensively understands the disease experience of women patients with GLM in China, and provides a basis for formulating precise intervention and support strategies for women patients with GLM.
Methods
Design
This study used descriptive qualitative research methods to explore the disease experience of women patients with GLM in China. The descriptive qualitative research method is based on the general principles of naturalistic inquiry and does not elaborate any views in advance.23 In view of the lack of research on GLM women disease experience, and this study is a small sample size study, and descriptive qualitative research is particularly suitable for research areas where there is not much information to refer to. Therefore, this study uses descriptive qualitative research methods. In this study, semi-structured interviews were used to collect qualitative data, and content analysis was used to analyze the data. In the course of the study, we did not use a pre-determined verification answer scale.
Setting and Study Population
This study used qualitative research methods to conduct semi-structured in-depth interviews with GLM patients in the traditional Chinese medicine nursing clinic of a comprehensive third-grade Chinese medicine hospital in Hangzhou, Zhejiang Province, China. Each interview follows an interview outline.
In this study, the purpose sampling method24,25 was used to ensure the sample diversity of age, gender, functional status and course of disease in GLM patients. The principle of determining the sample size is as follows: If no new topic arises, further recruitment will be terminated. Inclusion criteria for GLM patients: (1) age ≥ 18 years; (2) Western medicine diagnosis is mainly based on pathological diagnosis, referring to the diagnostic criteria of breast pathological diagnosis and differential diagnosis; (3) Voluntary participation in research, no communication barriers. Exclusion criteria: individuals with major diseases such as other malignant tumors, communication disorders or minors. Two researchers introduced this study to women with GLM in detail and invited them to participate. Initially, we recruited 12 participants, and later two participants refused to participate in the interview because of interest. Therefore, we finally interviewed 10 participants.
Data Collection
The team of qualitative research contacted participants by email, phone to determine the time and place of interview and conducted semi-structured face-to-face interviews after signing informed consent. The interview language is Chinese, and the interview sites are quiet places (such as lounges and doctor ‘s offices). Initially, the interview outline was developed on the basis of clinical investigation and literature review. Later, the interview outline was further improved through pre-interview and team discussion. An interview guide mainly included the following questions: “1Can you share your illness experience with me?” 2 “Can you talk to me about your feelings when you were first diagnosed with GLM?”3 “What changes or effects do you think this disease has brought to you?” 5“What are the main problems you are facing now?” 6“How do you live with diseases in your daily life?” 7“How do you think others view the change of breast appearance after surgery?” 8“Are you satisfied with the nursing work of GLM in the whole medical system? What are the suggestions?” In interviews, we first ask open-ended questions and then encourage participants to elaborate if necessary. A researcher recorded other details such as the surrounding environment, participants facial expressions and body language.26 All participants interviews were recorded using a recording pen and the interview time was 30–45 minutes.
Data Analysis
After each interview, our research team will convert the recording into text within 24 hours, using content analysis method to analyze the data27,28 two nursing masters and a clinical head nurse who completed qualitative research courses analyzed each transcript. Qualitative nursing experts regularly check and guide the data of this study to improve the quality of data. In the first step, we conducted a deep and comprehensive understanding of the preliminary transcribed text data alone to fully understand the participants experiences and feelings. In the second step, we annotate meaningful transcripts and extract key sentences, and then manually encode them. In the third step, we divide them into sub-topics and topics based on similarity and difference. In addition, we compare and discuss each researcher coding results to determine sub-topics and topics. At the end of the 10th interview, we found that the information provided by the participants was repeated, and at this time, we believed that the theme reached saturation. In addition, we interviewed several additional women with GLM again to confirm the theme saturation. In this study, interview results and interview analysis data were published after obtaining the informed consent of each participant.
Results
The average age of the participants was 31.5 years old, ranging from 25 to 40 years old. Other characteristics of these participants were shown in Table 1
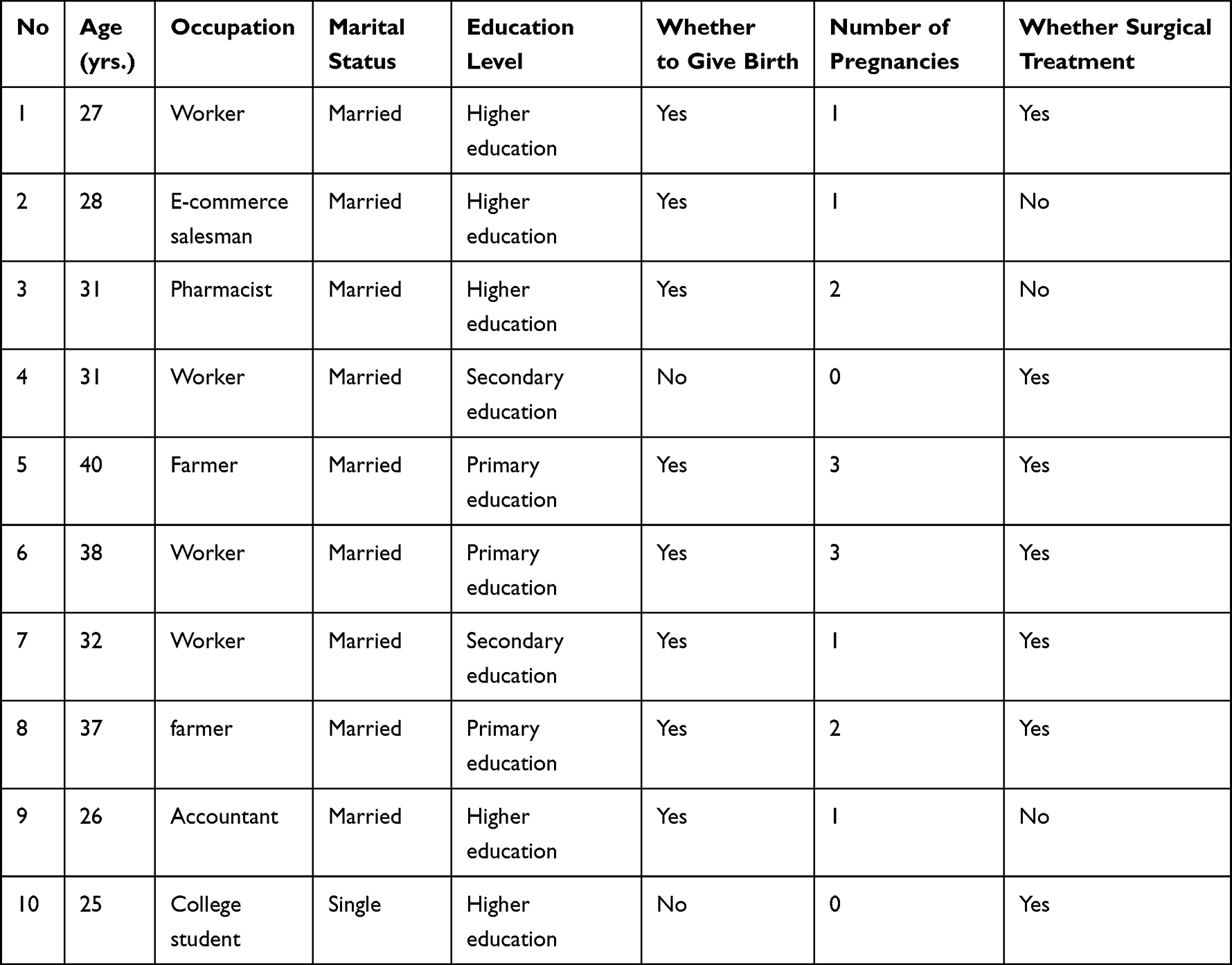 |
Table 1 Study Participants’ General Information and Clinical Characteristics (N=10) |
Six themes and 16 subthemes were emerged from data analysis (see to recommendation for Table 2 legend).
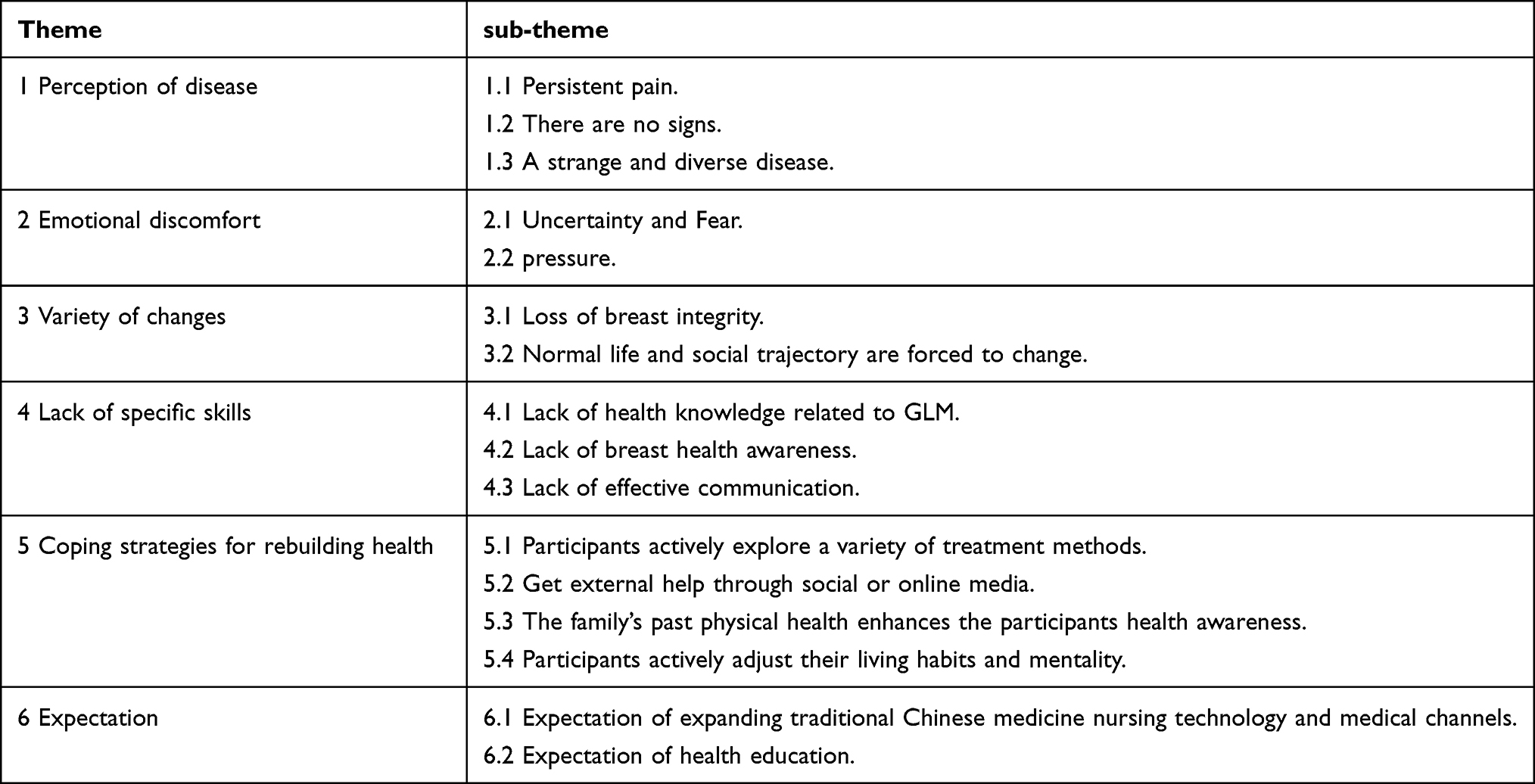 |
Table 2 Theme and Sub-Theme of the Disease Experience of the Participants |
Topic 1 Perception of Disease
This topic is mainly related to the characteristics of the disease. Each participant’s own disease perception is different, but they all experienced persistent breast pain.
Persistent Pain
Participants said that persistent breast pain can lead to upper limb dysfunction, decreased mobility, and decreased sleep quality.
P1: My breast is very hard and painful, when walking also pain, sitting also pain, when sleeping at night also pain, breast often spontaneous pain.
P2: I do not know how to sleep, I dare not turn over, the degree of breast pain so that my arm cannot be lifted.
There are No Signs
Participants said that GLM had a sudden onset and had no signs before the disease.
P4: Once on the New Year, the breast suddenly began to redness and pain. The whole breast is particularly swollen.
P5: On the third morning, my breasts exploded like a balloon. I was scared to death, and my breasts swelled very high and red.
P2: In November last year, one morning, I suddenly couldn’t lift my arm, and it was a little painful. I thought it was lymph.
A Strange and Diverse Disease
Participants described GLM as a strange and diverse disease. The clinical characteristics of the participants are not the same, the nipple or the broken breast wound will secrete a variety of colors of pus, and it is difficult to directly extract pus from the breast puncture, which is not available in traditional breast inflammatory diseases. In addition, other organs of the participant ‘s body also suffered from disease. For example: the decline in the physical function of the participants, physical weakness, elevated body temperature, lower extremity erythema and accompanied by leg pain and other symptoms, the digestive system will appear to weaken the digestive function, loss of appetite and other symptoms, the nervous system can be manifested as dizziness.
P6: I am often weak. I sometimes feel dizzy.
P2: My leg appeared erythema, very painful itch. In addition, my mouth has been acid and bitter, I don ‘t want to eat any food. The pus of the breast is diverse in color, but mainly white pus, sometimes bloody pus.
P1: One day suddenly there was a hard mass, and then in the menstrual period, and then I felt caused by menstruation, because I had a little lobular hyperplasia, so I thought it was breast hyperplasia caused by pain.
P3:I have asked several people who also have this disease, they have more pus in their breasts. Some patients with breast ulcer is more serious, pus and blood mixed together.
Emotional Discomfort
During the illness, participants often feel anxious and fearful about the uncertainty of their disease status, development direction and outcome. At the same time, long-term treatment forces participants to face various pressures.
Uncertainty and Fear
Participants mentioned that they did not know how long it would take to completely cure the disease, and could not predict the development of the disease, and sometimes breast physicians could not do anything about the disease. Participants indicated that they did not see the dawn of healing, lived in an uncertain state with persistent breast pain, and therefore often felt fear, pain, and anxiety. Some participants said they tried to respond by actively cooperating with treatment, but with little success.
P3: I started the surgery in October last year. It has been going on until now, it has been half a year (the patient’s facial expression is lonely), but I feel that there is no light in sight, and I am afraid that it will change viciously. The doctor said that there may be something that can irritate your breasts and cause other parts of the breast to recur, so I am often worried.
P5: The doctor told me that this disease is difficult to treat, and even if it is treated, it will recur.
P2: I’ve been ill for nine months. If the disease does not progress, it just stays in one stage. I was terrified of this puncture and pus. The most terrifying thing in the whole process is to draw pus, and every time I drag out time and do not go to the hospital to draw pus.
Pressure
Participants shared that long-term treatment not only causes physical and emotional exhaustion, but also forces them to face a variety of pressures, including psychological pressure, economic pressure, and pressure from family health. Stress is an ‘invisible burden, but it is very common.
Some participants have shared with researchers that in the state of breast abscess ruptured wound is difficult to heal, their original positive and optimistic attitude towards life and personality will be involuntary into negative pessimism, depression or run-down emotions. This pessimism and depression will often be released without warning, affecting the normal interpersonal communication and work of participants.
P3: My breast wound isn’t healing now, sometimes the mood is really bad. I used to be a more optimistic person. (Patients cry) In fact, everyone ‘s psychology seems to be going through, because the disease lasts for a long time, it will give people an invisible burden.
P4: But this disease will not die, but it makes you painful.
P7: Now the burden of this disease is still quite large. Compared with the previous normal state, I am indeed depressed and sad.
Participants who had been misdiagnosed with breast cancer said their fears were reduced after the correct diagnosis, but were replaced by feelings of helplessness and anxiety. This is related to the complexity or difficulty of the disease treatment procedure.
P5:At first, I was scared to death, I was scared, I thought it was breast cancer. Later, it was diagnosed, although it was not cancer, but I knew that the disease was very troublesome, and I didn’t know what to do at that time. Especially affect the mood, I will lose my temper for no reason, and the feeling of collapse.
P8: This disease is not easy to treat, I am very anxious, my breasts collapse every time they have pus, and then I have to drink Chinese medicine every day.
Participants also cited their own financial burden and barriers to returning to work as sources of stress.
P6: This disease has a certain impact on our economy. The most important problem is money.
P9: I have great economic pressure.
Participants said that a stable job is very important for themselves. Leaders and colleagues’ awareness of the disease and understanding of their current state are important factors in retaining work.
P10: I dare not lose my job. But I really don ‘t know how to speak to leaders and colleagues to explain that after the operation is the beginning of treatment, for fear that they do not understand. Because of the privacy of my breast parts, I can’t show them the actual condition of the breast ulcer surface.
P8: My work is temporarily suspended. This disease affects my work.
A participant whose daughter had myelitis said she felt powerless about the changes and stress of life caused by the disease. Two complex diseases accumulate in a family, leaving her in a difficult and desolate life, with a strong sense of despair and powerlessness.
P6: I can’t do anything, because I have a daughter at home who is not well, she has myelitis, (the patient looks dejection), I know that myelitis is really difficult to treat, because my daughter had myelitis when she was fourteen, but I can’t do anything.
Variety of Changes
Participants experienced a variety of changes in the process of diagnosis and treatment, including the loss of breast integrity, changes in life and social circles, and loss of self-image. Participants often feel regret or loss of attraction, or fear of not being able to better integrate and return to their original life and social circle, because sometimes they feel misunderstood and devalued by people around them, especially younger patients.
Loss of Breast Integrity
Participants believe that the integrity of the breast is an indispensable part of both the emotional aspect of the couple and the symbol of female identity and the beauty of the appearance. Postoperative breast scars led to the loss of female characteristics, emotion and self-confidence of the participants. However, some participants ‘personal resilience and spiritual strength of yearning for life have prompted them to actively face the lack.
P4: No matter how good the recovery after breast surgery is, it is impossible to restore the original, Surgical treatment will have a great impact on the appearance of our breasts. My breasts are too ugly.
P3: If the whole breast is cut off, the whole person ‘s mentality must have changed, I feel incomplete.
P1: breast is the characteristics of women, breast too ugly must also affect the relationship between husband and wife. Truth be told, I am very low self-esteem after surgery, the husband ‘s thoughts I will take into account. If the breast has been cut off, it must be very low self-esteem ah.
P10: There are too many breast scars, I feel too ugly, too ugly.
Normal Life and Social Trajectory Forced to Change
Participants said that the disease did not seem to affect life, but it was actually very bad, and the wound of breast ulceration was difficult to manage. Most women say their lives have stagnated with pus, pain, and treatment in their breast ulcer wounds, starting a different journey, The only focus of the journey is disease and its effects. Participants stopped working, social circles were forced to change, self-image was forced to give up, and normal emotional communication with children was impossible; they focus on their own medical care. Disease limits all aspects of the participants.
P8: is mainly the problem of breast pain is not convenient to go out. I have always been at home, feel out more trouble, and go out for a while is very tired, I do not want to go out with friends to play.
P1: I can ‘t fully concentrate on doing other things, and you can ‘t wear underwear at ordinary times. It has seriously affected my life.
P10: Before I got sick, I still care about my external image, and now I ‘m in no mood.
P5: I can ‘t do anything at home, I can ‘t take care of the child.
Lack of Specific Skills
Participants from rural areas and primiparas said that they lack health awareness.
Some participants also mentioned that medical staff lacked effective communication with patients in clinical decision-making.
Lack of Health Knowledge Related to GLM
Participants said that they had never been exposed to GLM before they fell ill, or even knew nothing.
P9: No medical staff ever taught me to do breast self-examination.
P7: There is no medical staff to go to the countryside to popularize the disease, really to popularize it, because many people still do not know this aspect.
Lack of Breast Care Awareness
Participants said they were busy taking care of their children and ignored breast care. The local cultural background and surrounding environment of the participants are an important reason for the lack of breast health awareness.
P1: I spend more time taking care of children, so I don ‘t have extra time to focus on breasts.
P9: I myself do not have a breast disease examination, rural people do not have this consciousness at all, only the people around me have a disease, will think of paying attention to it myself.
Lack of Effective Communication
In our interviews, participants reflected their disappointment with the expected medical services and treatment and care work of medical staff. One participant said that when some treatment methods were ineffective, professional medical staff did not actively explain the clinical decision-making of treatment, nor did they actively explain the precautions for preventing disease recurrence and the possible development direction of the disease. Participants are in a state of ignorance, which further aggravates participants ‘stress, fear of disease and helplessness.
P2: I entered the anti-inflammatory drug is useless, no one told me, I should do next, no one told me I have other options. How will my disease develop next? No one told me, I am confused.
P10: In fact, when I first saw a doctor, the doctor should tell me some of the circumstances of the disease, some doctors do not tell me what this is a disease, will not tell me the severity of the disease. if I tell, I will pay attention to.
Coping Strategies for Rebuilding Health
After the participants bodies, lives, and social interactions were completely disrupted by the disease, the participants would still actively explore or use tools to obtain supportive strategies for health reconstruction after experiencing morbid and disordered bodies and lives. This may be related to participants individual psychological resilience.
Participants Actively Explore a Variety of Treatment Methods
Participants take the initiative to explore traditional Chinese medicine treatment measures, try different treatment methods.
P9: Later I found a Traditional Chinese Medicine clinic and did local Traditional Chinese Medicine fumigation for the breast. It was thirty minutes at a time, and I did it seventeen times.
P2: I’ve smoked it with moxibustion strips before, and I feel okay. Then I came to the hospital this time for infrared treatment, and I saw if infrared treatment could eliminate breast lumps.
Get External Help Through Social or Online Media
Participants mentioned the importance of social media. Participants communication with other patients or the power of media communication alleviated participants anxiety and fear during the illness, obtained psychological emotional support, increased their awareness of the disease, and prompted participants to actively face the future.
P10: When I first knew about this disease, then I looked at Baidu and ‘Little Red Book, and I looked at which hospital other patients went to and how they were treated.
P2: After I got sick, I looked up the disease on the Internet, and there are many treatments for this disease on Douyin, there is a Chinese medicine doctor in Beijing, he advocates the use of Chinese herbal medicines on the breast, and his patients are also optimistic. So I wanted to give it a try too.
P7: I asked them (patients) in the WeChat group if there were any good ways to eliminate breast swelling, and some of them used houttuynia to reduce swelling, but I didn’t dare to try.
The Family ‘S Past Physical Health Enhances the Participants ‘Health Awareness
The health status of family members is one of the important factors in disease screening and prevention.
P1:My mother has breast cancer and I know that I have the genetic component of malignant disease, so I check my thyroid and breast once a year.
Participants Actively Adjust Their Living Habits and Mentality
Some participants mentioned that they are trying to accept and support, although it is a difficult process for them, but they have the belief to continue. Many people are committed to adjusting their living habits and mentality, such as changing eating habits, losing weight, exercising more than usual, maintaining emotional stability, and complaining less.
P1: Now after the surgery, I have maintained a regular routine in all aspects of my life and sleep.
P8: I think diet and lifestyle are more important, I think that going to bed early can improve immunity, and then in terms of diet, I try not to eat seafood or foods with higher hormones.
P9: I begin to pay attention to light diet now ‘. Before I got sick, I did not think about these problems. I came completely according to my own preferences. Now, I have to pay attention to my health. I also follow the doctor ‘s advice to lose weight.
P7: The doctor told me that illness and mood are also related. I try to make myself happy and not think about the things that bother me.
Expectation
Expectation of Expanding Traditional Chinese Medicine Nursing Technology and Medical Channels
Participants said that due to the long recovery period of the disease, it was necessary to take medicine and repair treatment in the hospital many times, wasting a lot of time and increasing the sense of fatigue. Promote Traditional Chinese Medicine acupoint massage technology, expand the scope of network service functions, continuously optimize the allocation of resources, and increase the convenience of participants in medical treatment.
P2: It would be much more convenient if you could prescribe medicine and send it home after seeing a doctor online. Because I still have to work. There is a long wait in the hospital, and a lot of it is wasted waiting.
Expectations for Health Education
Participants hope to popularize the knowledge of disease prevention and choose the appropriate time, methods and tools to promote the effective prevention of the next generation of expectant mothers.
P10: I definitely want the doctor or nurse to tell me how far my disease has progressed, because it takes so long and people are a little impetuous.
P1: I think that just after giving birth, at this time, to popularize the knowledge of GLM prevention for her, she may be more interested and more acceptable, I think it is better to explain the effect on the spot with real cases.
P7: I think we should popularize the people with nipple depression, how to prevent GLM.
P6: We should popularize what causes diseases, how to better treat them, and how to care for them?
P5: I think the right time is to stop breastfeeding breast swelling after the time, this time is already about their health. so that mothers in the corresponding environment, will attract the attention of mothers.
P8: After giving birth to a baby and returning home from the hospital, you can go to the door to popularize what diseases the breast may have, explain it first and then give the manual, I will remember it very well.
Discussions
The Perception of Disease is a Signal or Manifestation of the Participant’s Body ‘S Invasion of the Disease Most Participants ‘Perception of Disease is Long and Slow
In this study, participants indicated that they and breast surgeons did not realize the severity of the disease at the initial stage of it, and sometimes misjudged themselves or were misdiagnosed with other diseases. Meagan29 pointed out that some women patients with GLM feel pain and fatigue from the diagnosis and management experience of breast surgeons, because clinicians cannot alleviate and explain the symptoms of GLM. Some women patients with GLM have also been misdiagnosed as inflammatory breast cancer, which further delays their time to obtain the correct treatment. The low awareness of GLM among participants and some physicians is related to the lack of health knowledge of GLM and the similar clinical manifestations of GLM with breast cancer and mastitis30 When the symptoms of the disease are considered to be familiar, have little effect on function or cause no concern, people may ignore. But only when the symptoms persist for a period of time or pose a risk to them, people will reflect on its origin.31 In addition, people perception of disease depends not only on people personal situation, but also on the socio-cultural background. For example, the participants ‘gender, age, family, and social relations all affect people understanding of physical changes. This is consistent with the opinion of the psychiatrist Arthur Kleinman32 That is, the body exists in the cultural intermediary. For women patients with GLM who have suffered from breast pain for a long time, a variety of analgesic measures can be used to intervene, such as three-step analgesic ladder, wrist-ankle acupuncture, auricular point pressing beans, acupoint application and other analgesic methods.33–35 Relevant studies have shown that the treatment of external treatment of traditional Chinese medicine such as wrist-ankle acupuncture 12 hours before breast wound dressing change will significantly reduce the pain level of women patients with GLM during dressing change, but there are fewer nursing staff who master the operation of wrist-ankle acupuncture.34 On the other hand, the work of medical staff in China is quite heavy. Medical staff are busy with their work and ignore the importance of full communication, which is also one of the reasons why women patients with GLM have lower cognitive ability and weaker self-care efficacy. Therefore, it is necessary to strengthen the training of specialized theoretical knowledge for medical staff engaged in nursing GLM women patients, and strengthen the publicity of GLM health knowledge, so as to improve the attention of women patients with GLM to their own health.
Positive and Effective Psychological Intervention is an Important Measure to Reduce the Negative Emotions of Participants
Breast abscesses, fistulas, leading to persistent breast pain and local skin damage in the breast.36 The persistent characteristics of GLM make participants feel strongly about their experiences. These feelings include uncertainty, anxiety, fear, helplessness, depression and stress. This negative emotion is “invisible” but common, highlighting the sadness participants must face when life is suddenly forced to change. At present, the study of negative emotions in GLM patients is still in its infancy, but psychological interventions for other chronic diseases provide us with a research basis. Resilience theorists believe that resilience is the result of people ‘s active and dynamic adaptation.37 Enhancing resilience is seen as a strategy to shift from disease-focused to health-focused, as well as a strategy to prevent disease-related stress and reduce psychological distress.38 Therefore, by providing participants with relevant resources and methods of disease treatment, patients can enhance their ability to cope with challenging problems in life, and help participants to reconstruct their cognition, which will help participants to view their own situation from different perspectives and transform negative emotions into positive emotions, thereby enhancing psychological resilience.39 Studies have shown that regular patient seminars or group meetings for participants with the same disease can help reduce anxiety and depression and enhance psychological flexibility.40 In this study, participants face a variety of pressures brought by the disease, and medical staff can develop diversified and adaptive programs based on the pressure situation to reduce the anxiety of patients. Most of the participants were forced to stop working during the treatment period, and the family’s income decreased, which would increase the risk of families falling into poverty, thus indirectly affecting the patient’s access to medical resources, especially for rural patients and patients seeking medical treatment in other places. Therefore, improving the medical security system is one of the measures to reduce economic pressure.41,42 Interventions such as enhancing psychological resilience, improving psychological resilience, cognitive behavioral therapy, decompression method based on mindfulness, and group meetings for people with the same disease can help patients relieve negative emotions, cope with stress, and improve quality of life.43,44 However, medical staff should also focus on studying the individual differences of patients in order to locate patients in the best practice program for them.
The Lack of Body Image and the Change of Life Trajectory Limit the Participants ‘Life
This study found that participants will face a variety of changes during treatment, including scar formation, loss of breast integrity, changes in life trajectories, and lack of effective communication between doctors and participants. At the same time, the lack of body image is an important social psychological problem that plagues the participants, affecting the individual’s appearance, physical function, marital emotion and overall self-esteem. At present, some scholars45 do not recommend surgical treatment for women patients with GLM, because surgery can cause many problems, such as breast deformation and poor wound healing, and high recurrence rate. On the other hand, studies46 have also shown that expanding the scope of breast resection will reduce the recurrence rate. But for GLM women patients who cannot accept breast defects, this will be an unacceptable treatment. Another study47 showed that for some women with GLM caused by Corynebacterium infection, local hyperthermia of the breast may promote the repair of breast wounds. Because the growth of Corynebacterium is significantly inhibited at 42°C, local temperature control may lead to the stagnation of Corynebacterium growth, so local hyperthermia can reduce breast inflammation and promote breast wound healing, so as to achieve the purpose of breast repair. At this stage, it is impossible to determine which treatment is best for women patients with GLM. Each patient has different expectations for the degree of breast repair. We need to provide personalized nursing management measures in the face of different women patients with GLM. For example, in the face of some GLM women patients who choose surgical treatment and are afraid of breast defects, we can provide psychological education before surgery, improve surgical methods, and perform breast skin repair after surgery, which will help participants accept the loss of breast integrity. Otherwise, Providing psychological education in advance before surgery, improving surgical methods, and performing breast skin repair after surgery will help participants accept the loss of breast integrity. Studies have shown that people’s beliefs about health and the predisposing factors of disease can affect their health-related decisions.48,49 Therefore, medical staff should improve participants ‘understanding of the etiology, alternative treatment options and processes, preventive care, and self-care management precautions of GLM normalize it and promote participants’ acceptance, strengthen effective communication between medical staff and patients, and provide professional strategies to manage modifiable factors to help participants make the most favorable health decisions. Medical service is a complex and dynamic process. Medical staff should maintain self-reflection and critical thinking to provide multi-dimensional medical services.
Actively Seeking Other Effective Treatment Measures and Making Full Use of Social or Media, Following a Healthy Lifestyle, and Strengthening the Active Awareness of Patient Rehabilitation are Conducive to Reshaping Health
This study found that participants took multiple measures to cope with the pain while facing the pain caused by the disease. Participants will actively use their contacts or social resources to obtain favorable medical resources for rapid recovery. They manage their condition through information acquisition, moderate exercise, healthy diet, and self-dredging emotions and strengthen their awareness and beliefs in fighting the disease, and use the accumulated knowledge and experience to reduce the impact of the disease on daily activities. This is consistent with the findings of Dena and John that proper self-management of chronic diseases can improve patient self-efficacy and reduce depressive symptoms50,51 A study52 exploring the tongue characteristics of GLM patients shows that the tongue coating of most GLM patients is white, thick and greasy, and the tongue body is bright red. This thick and greasy tongue coating is one of the risk factors for GLM; on the other hand, Chinese medicine believes that white greasy tongue coating is related to phlegm-dampness constitution, and red tongue body is related to heat evil invading the body. The main ways to improve phlegm-dampness constitution and prevent heat evil invading the body are to maintain a regular lifestyle, eat lightly, avoid drinking and smoking, adhere to physical exercise for a long time, and keep a comfortable mood. This is similar to the way of disease management advocated in this study. In addition, our medical staff should tailor health exercise schedules, diet recipes, and traditional Chinese medicine health care methods to improve the overall health of participants and enhance immune function to resist diseases.
Broadening Medical Channels Will Increase the Convenience of Medical Treatment in Different Places, Actively Popularize GLM Related Knowledge, and Improve People ‘S Awareness
This study found that whether it is a primary medical institution or a large hospital, there is little science popularization of GLM disease-related knowledge, and most participants have less knowledge of GLM. Participants said that they first heard of GLM at the time of diagnosis. In addition, participants in remote areas said that going to the hospital for follow-up medication would consume a lot of their rest time and increase their sense of exhaustion. Medical staff should establish an Internet platform or WeChat applet for women patients with GLM to facilitate medical counseling services for women patients with GLM. This Internet-mediated medical service platform also helps medical staff to dynamically track and follow up women patients with GLM and provide full guidance and support for home care of breast wounds. Therefore, Medical staff should establish an Internet platform or WeChat applet for women patients with GLM to facilitate medical counseling services for women patients with GLM. This Internet-mediated medical service platform also helps medical staff to dynamically track and follow up women patients with GLM and provide full guidance and support for home care of breast wounds. Medical staff also can increase the publicity of GLM disease knowledge. Medical institutions should actively expand Traditional Chinese Medicine nursing technology and medical channels, promote the innovation of medical and health service mode, continuously optimize the allocation of resources, improve service efficiency, and improve patients ‘medical experience.
Limitations
This certain research data provides some insights into the disease experience of GLM female patients for medical staff engaged in nursing management of women patients with GLM around the world. However, there are some unavoidable limitations in this study. In the course of this study, since the respondents are located in hospitals in Zhejiang Province, they cannot reflect the experience of women patients with GLM in other regions of China. In the future, the research field can be expanded to further enrich the research results. This study uses the purposive sampling method to recruit participants, which may have selection bias; the sample size of this study is small. Despite these limitations, this study has some important implications. As far as we know, although there are many articles on the pathogenesis and treatment of GLM, this is the first qualitative study on women patients with GLM in the world, and this article is unique. We interviewed different groups of participants in order to maximize the diversity of the groups of participants, and the data of this study is reasonable.
Conclusions
The experience of women with GLM is characterized by diversity and specificity. In the process of seeking medical services, the huge physical and psychological pain experience is their common point, which is related to repeated pus at the abscess site, breast pain, economic pressure, reduced parent-child communication, and reduced social activities. In the process of treating the disease, some patients gradually shift from a negative attitude to a positive response to the disease, which is related to the individual ‘s level of disease cognition, economic pressure, family support, local medical and health level. In addition, in the face of changes in body image, the support of family and sexual partners is particularly important for patients, and the partner ‘s attitude towards the breast appearance of women with GLM is one of the important factors affecting the mental health of patients. This study found that there were differences in the cognitive level of GLM among doctors and nurses in medical institutions in different regions. Grassroots medical staff lacked the knowledge of GLM prevention and self-care management. The team discussed the reasons and summarized them as uneven distribution of medical resources, economic level, doctors and nurses.
Data Sharing Statement
Research data can be made available to interested parties upon reasonable request to the corresponding author.
Ethics Approval
Approval of this study was granted by the Research Ethics Committee of The First Affiliated Hospital of Zhejiang Chinese Medical University (reference number 2023-KLS-033-01). This study follows the basic ethical principles of medical research involving human subjects in the Helsinki Declaration. Informed consent was obtained from all participants, and all participants signed the informed consent form before the study began. All participants are aware of the purpose, methods and steps of the study, and participants have the right to withdraw from the study at any time. Each participant is informed and consents to the anonymous publication of their citations, interviews, personal information, and anonymous responses.
Acknowledgments
Thanks to the people involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Zhejiang Province Medical and Health Science and Technology Plan Project (2023KY866). The funders have no role in research design, data collection and analysis, publication, manuscript writing.
Disclosure
The authors report no conflicts of interest in this work
References
1. Kuba S, Yamaguchi J, Ohtani H, et al. Vacuum-assisted biopsy and steroid therapy for granulomatous lobular mastitis: report of three cases. Surg Today. 2009;39(8):695–699. doi:10.1007/s00595-008-3891-7
2. Li XQ, Wu HL, Yuan JP, et al. Bacteria associated with granulomatous lobular mastitis and the potential for personalized therapy. J Invest Surg. 2022;35(1):164–170. doi:10.1080/08941939.2020.1833262
3. Wang Y, Song J, Tu Y, et al. Minimally invasive comprehensive treatment for granulomatous lobular mastitis. BMC Surg. 2020;20(1):34. doi:10.1186/s12893-020-00696-w
4. Wang J, Xu H, Li Z, et al. Pathogens in patients with granulomatous lobular mastitis. Int J Infect Dis. 2019;81:123–127. doi:10.1016/j.ijid.2019.01.034
5. Akcan A, Akyildiz H, Deneme MA, et al. Granulomatous lobular mastitis: a complex diagnostic and therapeutic problem. World J Surg. 2006;30(8):1403–1409. doi:10.1007/s00268-005-0476-0
6. Shin YD, Park SS, Song YJ, et al. Is surgical excision necessary for the treatment of granulomatous lobular mastitis? BMC Womens Health. 2017;17(1):49. doi:10.1186/s12905-017-0412-0
7. Lee JH, Oh KK, Kim EK, et al. Radiologic and clinical features of idiopathic granulomatous lobular mastitis mimicking advanced breast cancer. Yonsei Med J. 2006;47(1):78–84. doi:10.3349/ymj.2006.47.1.78
8. Emsen A, Köksal H, Uçaryılmaz H, et al. The alteration of lymphocyte subsets in idiopathic granulomatous mastitis. Turk J Med Sci. 2021;51(4):1905–1911. doi:10.3906/sag-2012-192
9. Kaiyun C, Lixia G, Yuehua L, et al. observation of the curative effect of ultrasound-guided pricking and cupping combined with traditional Chinese medicine in the treatment of 48 patients with granulomatous lobular mastitis. World J Integr Med. 2021;16(08):1520–1524+1529. doi:10.13935/j.cnki.sjzx.210828
10. Jiaxuan Z, ZENG Y. Treatment of granulomatous lobular mastitis from the thought of ‘surgical orthodoxy ‘carbuncle gangrene. Sichuan Chin med. 2022;40(03):40–42.
11. Haijiao H, Zhihua W, Ling L, et al. Discussion on the treatment of granulomatous mastitis from the theory of viscera rheumatism. Shanxi J Trad Chin Med. 2020;36(04):1–3.
12. Jiali W, Zhongli G. Treatment progress of granulomatous mastitis. Trad Chin Med in Xin Jiang. 2022;40(02):114–116.
13. Yuan QQ, Xiao SX, Farouk O, et al. Management of granulomatous lobular mastitis: an international multidisciplinary consensus (2021 edition). Mil Med Res. 2022;9(1):20. doi:10.1186/s40779-022-00380-5
14. Hovanessian Larsen LJ, Peyvandi B, Klipfel N, et al. Granulomatous lobular mastitis: imaging, diagnosis, and treatment. AJR Am J Roentgenol. 2009;193(2):574–581. doi:10.2214/AJR.08.1528
15. Martinez-Ramos D, Simon-Monterde L, Suelves-Piqueres C, et al. Idiopathic granulomatous mastitis: a systematic review of 3060 patients. Breast J. 2019;25(6):1245–1250. doi:10.1111/tbj.13446
16. Wolfrum A, Kümmel S, Theuerkauf I, et al. Granulomatous mastitis: a therapeutic and diagnostic challenge. Breast Care. 2018;13(6):413–418. doi:10.1159/000495146
17. Kanazawa S, Nagae T, Fukuda K, et al. Granulomatous lobular mastitis: difficulty of diagnosis. Int J Clin Oncol. 2000;5(1):57–61. doi:10.1007/s101470050011
18. Steuer AB, Stern MJ, Cobos G, et al. Clinical characteristics and medical management of idiopathic granulomatous mastitis. JAMA Dermatol. 2020;156(4):460–464. doi:10.1001/jamadermatol.2019.4516
19. Li J. Diagnosis and treatment of 75 patients with idiopathic lobular granulomatous mastitis. J Invest Surg. 2019;32(5):414–420. doi:10.1080/08941939.2018.1424270
20. Yaghan RJ, Ayoub NM, Shenawi HM, et al. Idiopathic granulomatous mastitis in the male population: a clinical analysis of 13 reported cases. Breast J. 2020;26(7):1481–1482. doi:10.1111/tbj.13778
21. Sheybani F, Naderi HR, Gharib M, et al. Idiopathic granulomatous mastitis: long-discussed but yet-to-be-known. Autoimmunity. 2016;49(4):236–239. doi:10.3109/08916934.2016.1138221
22. Liu H, Zhang HW, Ding ST, et al. Clinical Features of Granulomatous Mastitis. Chinese General Practice. 2016;19(18):2216–2218. doi:10.3969/j.issn.1007-9572.2016.18.021
23. Lincoln YS, Guba EG. Naturalistic Inquiry. Thousand Oaks, CA: Sage Publications; 1985:37e9.
24. Ames H, Glenton C, Lewin S. Purposive sampling in a qualitative evidence synthesis: a worked example from a synthesis on parental perceptions of vaccination communication. BMC Med Res Methodol. 2019;19(1):26. doi:10.1186/s12874-019-0665-4
25. Palinkas LA, Horwitz SM, Green CA, et al. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
26. Ruan J, Wu L, Zhou YY. Experiences of body image changes in Chinese patients living with inflammatory bowel disease: a descriptive qualitative study. Asian Nurs Res. 2020;14(4):196–205. doi:10.1016/j.anr.2020.07.006
27. Moser A, Korstjens I. Series: practical guidance to qualitative research. Part 3: sampling, data collection and analysis. Eur J Gen Pract. 2018;24(1):9–18. doi:10.1080/13814788.2017.1375091
28. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
29. Brennan ME, Morgan M, Heilat GB, et al. Granulomatous lobular mastitis: clinical update and case study. Aust J Gen Pract. 2020;49(1–2):44–47. doi:10.31128/AJGP-08-19-5042
30. Boufettal H, Essodegui F, Noun M, et al. Idiopathic granulomatous mastitis: a report of twenty cases. Diagn Interv Imaging. 2012;93(7–8):586–596. doi:10.1016/j.diii.2012.04.028
31. Malterud K, Guassora AD, Graungaard AH, et al. Understanding medical symptoms: a conceptual review and analysis. Theor Med Bioeth. 2015;36(6):411–424. doi:10.1007/s11017-015-9347-3
32. Kleinman A. The illness narratives: suffering, healing, and the human condition: [excerpt]. Acad Med. 2017;92(10):1406. doi:10.1097/ACM.0000000000001864
33. Yuping Y. Effect observation of thumbtack needle therapy combined with acupoint application in the treatment of patients with cancer pain three-step analgesic ladder. Chin J Cancer Prevent. 2019;26(S1):163–165.
34. Chuan Q, Anfeng X, Meiyu C, et al. Multi-Frequency Resting-State fMRI Study of Wrist-Ankle Acupuncture Analgesia .
35. Wang Lingling LX, Biquan Q. Observation on the efficacy of wrist-ankle acupuncture combined with opioids in the treatment of liver cancer pain. Shanghai J Acupunct Moxibust. 2021;40(11):1336–1340. doi:10.13460/j.issn.1005-0957.2021.11.1336
36. Kornfeld HW, Mitchell KB. Management of idiopathic granulomatous mastitis in lactation: case report and review of the literature. Int Breastfeed J. 2021;16(1):23. doi:10.1186/s13006-021-00370-8
37. Russo SJ, Murrough JW, Han MH, et al. Neurobiology of resilience. Nat Neurosci. 2012;15(11):1475–1484. doi:10.1038/nn.3234
38. Kalisch R, Baker DG, Basten U, et al. The resilience framework as a strategy to combat stress-related disorders. Nat Hum Behav. 2017;1(11):784–790. doi:10.1038/s41562-017-0200-8
39. Luo YH, Xia W, He XL, et al. Psychological interventions for enhancing resilience in parents of children with cancer: a systematic review and meta-analysis. Support Care Cancer. 2021;29(11):7101–7110. doi:10.1007/s00520-021-06344-0
40. Baron nelson M, Riley K, Arellano K. Adding a parent to the brain tumor team: evaluating a peer support intervention for parents of children with brain tumors. J Pediatr Oncol Nurs. 2018;35(3):218–228. doi:10.1177/1043454218762797
41. Mengyi W. New rural cooperative medical system for rural patients with chronic disease risk sharing. Chin Prim Healthcare. 2013;27(07):15–17. doi:10.3969/j.issn.1001-568X.2013.07.0007
42. Lanxin C, Yueping L. Research on the impact of medical service accessibility on residents ‘health status-Empirical analysis based on CFPS data. J Nanjing Med Univ. 2022;22(03):278–284. doi:10.7655/NYDXBSS20220312
43. David D, Cotet C, Matu S, et al. 50 years of rational-emotive and cognitive-behavioral therapy: a systematic review and meta-analysis. J Clin Psychol. 2018;74(3):304–318. doi:10.1002/jclp.22514
44. Parsons CE, Crane C, Parsons LJ, et al. Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: a systematic review and meta-analysis of participants’ mindfulness practice and its association with outcomes. Behav Res Ther. 2017;95:29–41. doi:10.1016/j.brat.2017.05.004
45. Mizrakli T, Velidedeoglu M, Yemisen M, et al. Corticosteroid treatment in the management of idiopathic granulomatous mastitis to avoid unnecessary surgery. Surg Today. 2015;45(4):457–465. doi:10.1007/s00595-014-0966-5
46. Zhang Y, Zhou Y, Mao F, et al. Clinical characteristics, classification and surgical treatment of periductal mastitis. J Thorac Dis. 2018;10(4):2420–2427. doi:10.21037/jtd.2018.04.22
47. Chen X, Zhang W, Yuan Q, et al. A novel therapy for granulomatous lobular mastitis: local heat therapy. Exp Ther Med. 2021;22(4):1156. doi:10.3892/etm.2021.10590
48. Taber JM, Klein WMP, Persky S, et al. Interest in and reactions to genetic risk information: the role of implicit theories and self-affirmation. Soc Sci Med. 2017;190:101–110. doi:10.1016/j.socscimed.2017.08.010
49. Brogan A, Hevey D. The structure of the causal attribution belief network of patients with obesity. Br J Health Psychol. 2009;14(Pt 1):35–48. doi:10.1348/135910708X292788
50. Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annu Rev Public Health. 2019;40(1):127–146. doi:10.1146/annurev-publhealth-040218-044008
51. Schulman-Green D, Jaser S, Park C, et al. A meta synthesis of factors affecting self-management of chronic illness. J Adv Nurs. 2016;72(7):1469–1489. doi:10.1111/jan.12902
52. Chen J, Yang J, Qin Y, et al. Tongue features of patients with granulomatous lobular mastitis. Medicine. 2022;101(46):e31327. doi:10.1097/MD.0000000000031327
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.