Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
The Difficulty Of Improving Quality Of Life In COPD Patients With Depression And Associated Factors
Authors Lim JU ![]() , Park CK
, Park CK ![]() , Kim TH
, Kim TH ![]() , Jang AS, Park YB
, Jang AS, Park YB ![]() , Rhee CK, Jung KS, Yoo KH
, Rhee CK, Jung KS, Yoo KH ![]() , Lee WY
, Lee WY ![]() , Yoon HK
, Yoon HK ![]()
Received 22 May 2019
Accepted for publication 16 September 2019
Published 9 October 2019 Volume 2019:14 Pages 2331—2341
DOI https://doi.org/10.2147/COPD.S216746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Jeong Uk Lim,1,* Chan Kwon Park,2,* Tae-Hyung Kim,3 An-Soo Jang,4 Yong Bum Park,5 Chin Kook Rhee,1 Ki Suck Jung,6 Kwang Ha Yoo,7 Won-Yeon Lee,8 Hyoung Kyu Yoon2
1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 3Division of Pulmonary and Critical Care Medicine, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Republic of Korea; 4Division of Respiratory and Allergy, Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Bucheon, Republic of Korea; 5Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Kangdong Sacred Heart Hospital, Seoul, Republic of Korea; 6Division of Pulmonary Medicine, Department of Internal Medicine, Hallym University Sacred Heart Hospital, Hallym University Medical School, Anyang, Republic of Korea; 7Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Republic of Korea; 8Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Republic of Korea
*These authors contributed equally to this work
Correspondence: Hyoung Kyu Yoon
Division of Pulmonology and Critical Care Medicine, Department of Internal Medicine, Yeouido St. Mary`s Hospital, School of Medicine, The Catholic University of Korea, #62 Yeouido-dong, Yeongdeungpo-gu, Seoul 150-713, Republic of Korea
Tel +82-2-3779-2213
Fax +82-2-784-5458
Email [email protected]
Objectives: Depression is a major comorbidity that affects clinical outcomes in patients with chronic obstructive pulmonary disease (COPD). COPD patients with depression are hospitalized more frequently, and show more acute exacerbations, decreased physical and social activities, and higher mortality compared to their non-depressed counterparts. In the present study, we investigated the clinical impact of depressive symptoms and associated clinical factors in Korean patients with COPD by evaluating multicenter cohort data.
Materials and methods: Patients with COPD enrolled in the Korean COPD Subtype Study, a multicenter observational study, from December 2011 to October 2014 were selected for evaluation. The initial evaluation of all patients included pulmonary function tests, 6 min walk distance (6MWD), the COPD Assessment Test (CAT), and the COPD-specific version of the St. George’s Respiratory Questionnaire (SGRQ-C). Significant depression was defined as a Beck Depression Inventory-II (BDI-II) score ≥17.
Results: Among the 270 study patients, 19.6% had significant depression. The depressed group showed a higher proportion of females (41.4%), lower body mass index (BMI), and lower education level compared to the non-depressed group (p = 0.002, p = 0.008, and p = 0.019, respectively). The depressed group had significantly higher CAT and SGRQ-C scores, as well as a lower 6MWD, compared to the non-depressed group based on 6 month-interval serial measurements over 3 years. The total SGRQ-C score and the symptoms, activity, and impact domain scores were significant predictors of depression (area under curves [AUCs] of 0.699 [0.613–0.786], 0.670 [0.581–0.758], 0.680 [0.589–0.770], and 0.689 [0.603–0.776], respectively). From CAT score domains, sleep and energy scores were significant predictors of depression (AUCs of 0.619 [0.522–0.715] and 0.595 [0.504–0.685], respectively). SGRQ-C score, low BMI, and decreased 6MWD were significantly associated with depression in a multivariable analysis.
Conclusion: A considerable proportion of patients with COPD had depression, and a high SGRQ-C score, low BMI, and low 6MWD were significantly associated with depression. As improving quality of life in this subgroup is difficult, physicians should be more active in screening patients with significant depression.
Keywords: association, COPD Assessment Test, depression, St. George’s Respiratory Questionnaire
Introduction
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality worldwide.1 COPD is expected to be the third leading cause of mortality in 2020 worldwide.2,3 In addition, with the increase in size of the older population, the burden of COPD is also increasing.4 Due to the slow debilitating nature and progressive breathing difficulty which is distressing to patients, patients with COPD are at risk of psychiatric disorders, particularly depression.5,6 The prevalence of depression is reported to be 10–42% in patients with COPD7–9 which is higher than that of other comorbidities, such as cancer, heart disease, and renal disease.10 Depression is associated with longer hospitalization, a poor survival rate, and impaired physical and social functioning in COPD patients,11 and accompanies higher rates of acute exacerbations (AEs) and more frequent hospital admissions due to AEs.12,13 Compared to the general population, the prevalence of depression in patients with COPD is higher; however, it is reported to be underdiagnosed.14,15 Considering that untreated depression may increase the risk of severe exacerbation, it is important to diagnose and manage depression at the initial evaluation phase.
Compared to psychologists, pulmonologists are more likely to first evaluate and manage COPD patients with depression. Nevertheless, the diagnostic tools used to screen and assess the severity of depression by psychologists are not easy to use for pulmonologists. If we can also use the clinical parameters assessing COPD activity for the purpose of predicting depression, it would enable pulmonologists to manage depression among the COPD patients more easily. Furthermore, depressive moods complaint by patients with COPD could be due to physical symptoms, which makes them harder to discriminate, and more clinical data on the COPD group with depression are necessary.
There have been few studies on depression in Korean patients with COPD compared to studies on Western populations. The clinical characteristics of depressive patients are different depending on geographic location and race.16 For example, depressive patients from Asian countries and the US were shown to have different clinical presentations: Asian patients score higher on depressive symptoms compared to US participants and show different responses to questions regarding positive affect.17–19 Moreover, only a few longitudinal studies with significant observation periods have been conducted worldwide on the clinical course of patients with COPD and depression.20,21 By evaluating a multicenter cohort of patients with COPD, we sought to determine the clinical importance of depression and its associated factors to COPD and to improve the ability to predict depression in Korean patients with COPD.
Materials And Methods
Data Collection
Patients with COPD enrolled in the Korean COPD Subtype Study (KOCOSS) between December 2011 and October 2014 were selected for analysis, drawn from among 49 study centers throughout Korea. Inclusion criteria were the diagnosis of COPD by a pulmonologist, age ≥40 years,22,23 and symptoms including cough, sputum, dyspnea, and post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <70. The medical history at the first visit included frequency and severity of exacerbations in the previous 12 months, smoking status, and patient-reported education level. We used the Beck Depression Inventory (BDI) to screen for depression. The modified Medical Research Council (mMRC) dyspnea score, COPD Assessment Test (CAT) and COPD-specific version of the St. George’s Respiratory Questionnaire (SGRQ-C) were applied. The 6-min walk distance (6MWD) was measured using the 6-min walk test (6MWT). All data were reported using case report forms completed by physicians or trained nurses, and patients were evaluated at 6-month intervals after the initial examination. The major exclusion criteria were asthma, bronchiectasis, tuberculosis-destroyed lung, inability to complete the pulmonary function tests, myocardial infarction or cerebrovascular event within the previous 3 months, pregnancy, rheumatoid disease, malignancy, irritable bowel disease, or steroid use for conditions other than a COPD exacerbation within 8 weeks before enrollment. Exacerbation was defined as worsening of any respiratory symptom, such as increased sputum volume, purulence, or increased dyspnea, which required treatment with systemic corticosteroids, antibiotics, or both.
Diagnosis Of Depression
The BDI-II is a self-reported measure of depression that contains 21 questions. The BDI-II is a widely used instrument for detecting depression,24,25 including Korea.26,27 Each item is scored on a scale ranging from 0 to 3 and a higher total score indicates more severe depressive symptoms. The following guidelines have been suggested to classify scores on the BDI-II:28 no depression = 0–13, mild depression = 14–19, moderate depression = 20–28, and severe depression = 29–63. Beck et al recommended raising the cut-off score for depression diagnosis to 17 for research purposes.29 Carney et al reported 81% sensitivity, 79% specificity, and an area under curve (AUC) value of 83.8% for diagnosing depression in insomnia outpatients using a BDI-II cut-off value of 17.30 By reference to previous studies, the “depressed” group in this study comprised patients with scores ≥17 on the BDI-II in this study; patients with scores <17 were assigned to the “non-depressed” group. Baseline clinical parameters and exacerbation history were compared between the depressed and non-depressed groups.
Pulmonary Function, Disease Severity, And Exercise Assessment
Spirometry was performed according to a previously reported protocol.31 COPD severity was categorized by reference to spirometry results alone: stage I COPD was defined as FEV1% predicted ≥80%, stage II as FEV1% predicted <80% to ≥50%, stage III as FEV1% predicted ≤50% to >30%, and stage IV as FEV1% predicted <30%.32
Quality Of Life And Dyspnea Scores
The SGRQ-C was used as a measure of self-reported health status. The SGRQ-C is a 14-item questionnaire that yields a total score, as well as three component scores for symptoms, activities, and impacts. Total and component scores were calculated according to algorithms provided in the SGRQ-C instruction manual.33 Dyspnea was evaluated using the mMRC dyspnea scale, which is a 5-point scale with higher scores indicating more severe dyspnea. The CAT was also used to evaluate dyspnea. It consists of eight items, each scored from 0 to 5, with higher scores indicating more severe symptoms.34
Ethics Statements
The KOCOSS cohort was approved by the ethics and review board of each participating study center (SC12RIM10078). The names of approving ethics committees are in the Supplementary material. All patients gave written informed consent before inclusion in the study.
Statistical Analysis
Normal data, according to the Kolmogorov–Smirnov test, are presented as mean ± SD; non-normally distributed data are presented as median ± interquartile range [IQR, 25–75% percentile]. Continuous clinical variables were compared between the depressed and non-depressed groups using Student’s t-test and the Mann–Whitney U-test for normal and non-normally distributed data, respectively. Categorical clinical variables were compared using the chi-square test and Fisher’s exact test.
For comparison at different timepoints, CAT scores and SGRQ scores were also compared between the two groups using either Student’s t-test or the Mann–Whitney U-test depending on whether the data were normally distributed.
Four subgroups were defined using cutoff of BDI-II =17 and SGRQ-C =25. Continuous clinical variables were compared between the four subgroups using ANOVA and the Kruskal–Wallis test for normal and non-normally distributed data, respectively. Because multiple simultaneous comparisons was done between the four groups, pairwise comparisons were done using Bonferroni correction for continuous variables. For the pairwise comparison of categorical variables, the cutoff of p-value for statistical significance was lowered (p<0.008).
A receiver operating characteristic (ROC) curve analysis was used to assess the ability of the clinical parameters to predict depression. A logistic regression analysis was performed to evaluate the association between baseline clinical factors and depressive symptoms. Factors significant in the univariate analysis were entered in a multivariable analysis. The statistical analysis was performed using SPSS software (ver. 20.0; SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered significant.
Results
Patient Clinical Characteristics
Table 1 shows the clinical characteristics of the study patients and a comparison between the depressed and non-depressed groups. The total number of patients was 270, and the depressed and non-depressed groups included 53 and 217 patients, respectively. The proportion of patients with depression according to the BDI-II score was 19.6%.
 |
Table 1 Comparison Of Clinical Data Between Depression And No Depression Of COPD Patients |
The proportion of females was significantly higher in the depressed group than the non-depressed group (p = 0.002). Mean age was not significantly different between the groups. The depressed group had a significantly lower BMI (p = 0.008) and a lower proportion of college graduates (p = 0.002) compared to the non-depressed group. The CAT score also showed no significant group difference, whereas the total SGRQ-C score was significantly higher in the depressed group than the non-depressed group (p < 0.001). The depressed group displayed a lower baseline 6MWD (p < 0.001), and higher proportion of exacerbators and admissions due to AEs in the year prior to study enrollment (p < 0.001 and p < 0.001, respectively).
The depressed group had a higher proportion of patients who experienced at least one AE of COPD in the first year of follow-up compared to the non-depressed group. However, the group differences were not significant (Table 1).
Predictability For Depression
The ability of baseline total SGRQ-C score and individual component scores (symptoms, activity, and impact) to predict depression, defined as a BDI-II score ≥17, was evaluated using ROC curve analysis. The AUCs were 0.699 (0.613–0.786), 0.670 (0.581–0.758), 0.680 (0.589–0.770), and 0.689 (0.603–0.776) for the total SGRQ-C score and the symptoms, activity, and impact domain scores, respectively (all p < 0.05; Supplementary Figure 1).
Baseline total CAT score, and scores for the activity limitations at home, confidence leaving home, sleep, and energy domains were also evaluated for their ability to predict depression. The total CAT score, activity limitations at home, and confidence leaving home domain scores did not show significant predictability for depression, whereas sleep and energy scores (AUCs of 0.619 (0.522–0.715) and 0.595 (0.504–0.685), respectively) showed significant association (all p < 0.05; Supplementary Figure 2).
Correlation Between BDI-II Score And Other Parameters
Figure 1 shows the results of the correlation analysis between BDI-II score and other baseline parameters. The BDI-II score had a linear negative correlation with 6MWD (r = −0.358, p < 0.001) (Figure 1A) and a linear positive correlation with SGRQ score (r = 0.298, p < 0.001) (Figure 1B). However, no significant correlation with CAT score was present (r = 0.082, p = 0.199) (Figure 1C). The BDI-II score also was weakly but significantly negatively correlated with BMI (r = −0.150, p = 0.014) (Figure 1D).
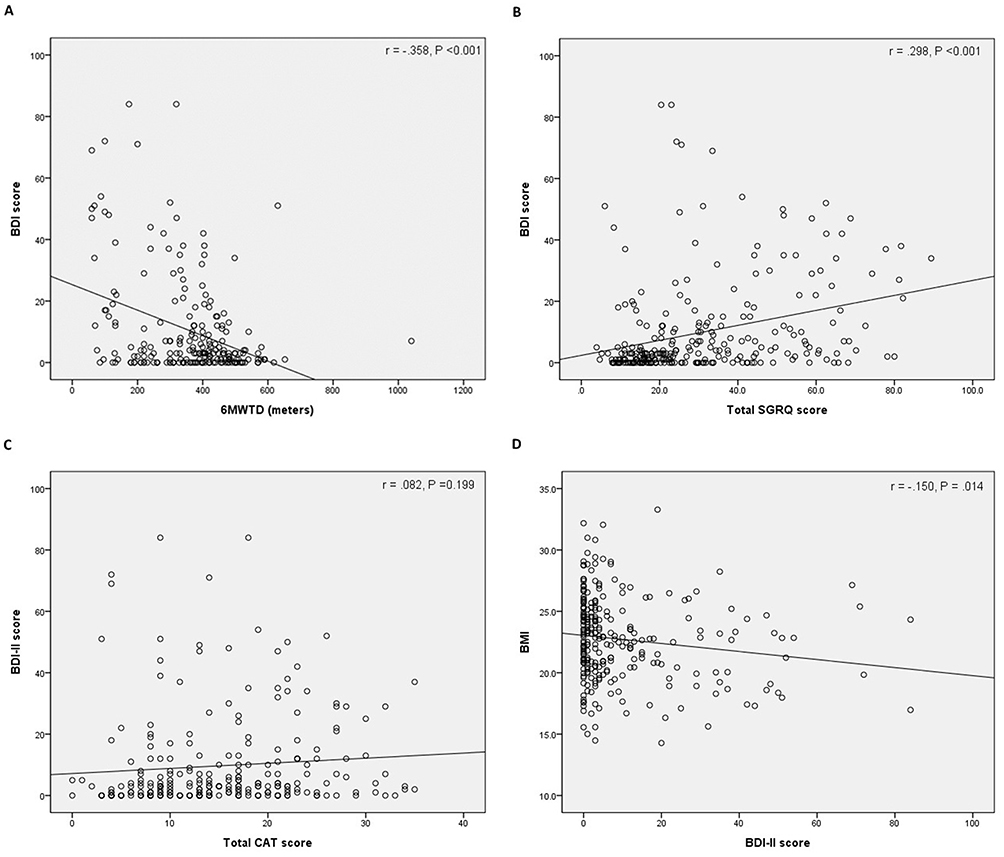 |
Figure 1 Correlation analyses between the BDI-II score and (A) total SGRQ-C score, (B) the 6MWD, (C) the CAT, and (D) BMI. Abbreviations: BDI, Beck Depression Inventory; SGRQ-C, the COPD-specific version of the St George’s Respiratory Questionnaire; 6MWD, 6 min walk distance; CAT, COPD Assessment Test; BMI, body mass index. |
Group Comparison Of Baseline Parameters And Serial Measurements
Table 2 shows the total SGRQ scores and individual component scores (symptoms, activity, and impact) of both groups. Scores on all four factors were significantly different between the two groups, at baseline and for the two serial measurements (6 and 12 months), with the depressed group showing higher scores compared to the non-depressed group. Figure 2A shows the total SGRQ scores of the two groups during the 3-year follow-up. The depressed group had a significantly higher SGRQ score compared to the non-depressed group.
 |
Table 2 St. George’s Respiratory Questionnaire Score |
 |
Figure 2 Changes in (A) SGRQ-C score, (B) CAT score, (C) 6MWD, and (D) number of acute exacerbations/year by follow-up timepoint. Abbreviations: SGRQ-C, the COPD-specific version of the St George’s Respiratory Questionnaire; 6MWD, 6 min walk distance; CAT, COPD Assessment Test. |
Table 3 shows the total CAT scores and individual component scores of the depressed and non-depressed groups at baseline, 6 months, and 1 year. The total CAT score was significantly different between the two groups at 6 months and 1 year (both p < 0.001) with scores being higher in the depressed group. A significant difference was observed between the two groups in the activity limitations, confidence, and energy domain scores at all three measurement timepoints. The scores for the chest tightness and breathlessness domains were significantly different between the groups only at 6 months and 1 year. Figure 2B shows the CAT scores of the two groups during the 3-year follow-up. The depressed group had significantly higher CAT scores at all measurement timepoints than the non-depressed group.
 |
Table 3 COPD Assessment Test (CAT) Score And Depression |
Figure 2C shows the 6MWD of both groups at baseline, 1 year, 2 years, and 3 years. The non-depressed group covered more distance on the 6MWD test than the depressed group. Figure 2D shows the frequency of AEs per year after 1, 2, and 3 years. The baseline and second-year follow-up AEs were significantly more frequent in the depressed group than in the non-depressed group.
Association Between Depression (BDI-II Score ≥17) And Baseline Parameters
Two models were used to evaluate the associations of various parameters with depression (BDI-II score ≥17). In model 1, baseline parameters including age, sex, FEV1 (%), SGRQ score, BMI, 6MWD, education level, and smoking history were entered in a univariate analysis (Table 4). Sex, SGRQ score, BMI, and 6MWD were significantly associated with depression in the univariate analysis (p = 0.003, p < 0.001, p = 0.009, p < 0.001 and p = 0.001, respectively) and were thus entered in a multivariable analysis. The multivariable analysis revealed that SGRQ score (odds ratio [OR] 1.038, 95% confidence interval [CI] 1.018–1.059, p < 0.001), BMI (OR 0.855, 95% CI 0.758–0.964, p = 0.010), and 6MWD (OR 0.994, 95% CI 0.991–0.997, p < 0.001) were significantly associated with depression.
 |
Table 4 Multivariable Logistic Regression Analysis For Factors Predictive Of Probable Depression (BDI-II ≥17) |
The CAT component scores (activity limitations at home, confidence leaving home, sleep, and energy) were entered into model 2, in addition to the other baseline parameters (excluding SGRQ score) included in model 1. Sex, all four CAT component scores, BMI, 6MWD, and education level were significantly associated with depression in the univariate analysis and were thus entered into the multivariable analysis. Sex (OR 3.375, 95% CI 1.102–10.334, p = 0.033), BMI (OR 0.818, 95% CI 0.716–0.933, p = 0.003), and 6MWD (OR 0.994, 95% CI 0.991–0.997, p < 0.001) were significantly associated with depression in the multivariable analysis, whereas the CAT score components were not (Supplementary Table 1).
Comparison Of The Four Subgroups Stratified By BDI-II Cutoff Score Of 17 And SGRQ Cutoff Score Of 25
Patients with baseline BDI-II and total SGRQ score data (n = 268) were stratified into four groups for subgroup analysis, using cutoff scores of 17 and 25 on the BDI-II and SGRQ, respectively. Table 5 shows the baseline clinical characteristics and clinical outcomes of the four subgroups. Among the 268 patients, 40, 13, 91, and 124 were grouped into the high SGRQ depressed group (SGRQ ≥ 25), the low SGRQ depressed group (SGRQ < 25), the high SGRQ non-depressed group (SGRQ ≥ 25), and the low SGRQ non-depressed group (SGRQ < 25), respectively. The proportion of males was significantly different among the subgroups, with the low SGRQ depressed group showing the lowest percentage (69.2%). The high SGRQ depressed group displayed a significantly lower BMI compared to the low SGRQ non-depressed group (p = 0.013). The low SGRQ non-depressed group demonstrated the highest proportion of college graduates among the subgroups (21.8%) (p = 0.002). The high SGRQ depressed group had the highest proportion of GOLD stage IV patients (15%) (p = 0.007). A significant difference in FEV1 (%) was present between the high SGRQ depressed group and the low SGRQ depressed group (51.9 vs 58.2) (p = 0.001). The two groups with high SGRQ scores had the highest proportions of patients with mMRC scores ≥2 (p < 0.001), and the highest CAT scores (p < 0.001). Among the four subgroups, 6MWD was significantly shorter (250.6 m) in the high SGRQ depressed group compared to the other groups (p < 0.001).
 |
Table 5 Comparison Of The Four Subgroups Stratified By BDI-II ≥17 And SGRQ ≥25 (n=268) |
Discussion
Depression is an important comorbidity with a high prevalence in patients with COPD. Previous studies have shown that the prevalence of depression is 10–42% in patients with COPD. In another study, 70% of patients with severe to very severe COPD exhibited depression.35 The present study demonstrated that patients with COPD and depression had poorer quality of life, and decreased activity compared to non-depressed patients during the 3-year treatment course. Furthermore, SGRQ and CAT scores significantly predicted depression, and the SGRQ score, a low BMI, and low 6MWD showed significant associations with depression.
Although many studies have shown that depression is a major comorbidity in patients with COPD, most of them focused on Western populations. Xu et al reported a depression prevalence of 23% based on the Hospital Anxiety and Depression Scale (HADS) score in a cohort of 491 Chinese patients with COPD. To the best of our knowledge, the present study is the first large-sized multicenter cohort study to demonstrate the clinical importance of depression in Korean patients with COPD. It has previously been shown that patients with COPD are more likely to have depression compared to the general population of Korea.36 The prevalence of depression was 19.6% in our study, which was lower than that in other studies.6,7
It is also notable that, in the present study, the proportion of females was higher, while BMI was lower, in the depressed versus non-depressed group. In addition, the depressed group had fewer college graduates compared to the non-depressed group. These demographic features are consistent with some previous studies. Schane et al showed that patients with COPD, a lower education status, and female gender are more likely to have depression.6 It has also been reported that anxiety and SGRQ scores are higher in women than in men.37 Tsai et al revealed that older patients with COPD have many comorbidities and a low income, and are thus at a higher risk of depression.4 Despite the absence of income data in our study, we assume that patients with COPD and depression are more likely to have a lower income. The depressed group had a lower proportion of college graduates, which indirectly suggests a lower income in this group; however, this correlation should be confirmed in a future study.
The strength of our study was that significant parameters, including SGRQ, CAT score, and 6MWD were measured longitudinally. Depression predicts poor quality of life in patients with COPD;20,21 however, few studies have shown that patients with COPD and depression have high SGRQ and CAT scores during the treatment course. In addition, AEs were more frequent during the follow-up period in our depressed group compared to the non-depressed group, despite the lack of a significant difference in baseline FEV1 between the groups.
In our subgroup analysis, after stratification using the BDI-II and SGRQ cutoffs, the group with a high SGRQ and depression tended to complain more of respiratory symptoms, as they experienced more AEs prior to study enrolment and had shorter 6MWD compared to the other subgroups. It is also notable that patients in the depressed group with a low SGRQ score tended to have a lower BMI, a higher likelihood of current smoking, and a higher proportion of exacerbators, while also having a significantly shorter 6MWD compared to their non-depressed counterparts. Even in less symptomatic patients with COPD and depression, it is likely that the clinical course is unfavorable compared to non-depressed patients. However, a future study distinguishing respiratory symptoms from COPD and depressive symptoms is necessary, as a subgroup of patients with COPD complain of major symptoms other than dyspnea, such as fatigue.38
It is unknown why depression has an unfavorable impact on quality of life, activity, and exacerbation frequency during the clinical course of COPD. Activation of the hypothalamic-pituitary-adrenal axis is associated with anxiety and depression, which in turn increases the systemic inflammatory response.39 Du et al suggested that pro-inflammatory cytokines and cortisol play a crucial role in the etiology of COPD and depression.40 In addition, the prevalence of current smokers tended to be higher in our depressed group compared to the non-depressed group. Considering the positive association between smoking and depression shown in previous studies,11,41 we assumed that depressed patients have a tendency to continue smoking and this may have contributed to the difficulty in improving their quality of life during the treatment course.42,43
Considering the negative clinical impact and relatively high prevalence of depression in patients with COPD, diagnosing depression in the initial phase of management is important. We assumed that consulting a psychologist after screening for significant depressive symptoms would result in increased compliance with COPD treatment. In addition, a depressed mood is likely to be an important reason for poor quality of life in patients with COPD, so we believe that active management of depression may lead to improved SGRQ scores in patients with COPD. However, this hypothesis needs further study. Our multivariable analysis demonstrated that a high SGRQ score, low BMI, and shorter 6MWD are associated with significant depressive symptoms in patients with COPD. In addition, patients with a high SGRQ score and depressive symptoms need a more individualized treatment program, as they have poorer lung function and decreased exercise capacity.
The CAT score was not associated with depressive symptoms in our study, but had significant predictive value for depressive symptoms in the ROC curve analysis; it was also reported to have an association with depression in a previous study.13 Along with a high SGRQ score, a high CAT score should also be considered likely to accompany depression. The BDI-II, Patient Health Questionnaire-9 (PHQ-9), and HADS are unfamiliar to pulmonologists who are likely to first encounter patients with COPD.13,44 Patients with a high SGRQ or CAT score, low BMI, and decreased 6MWD may require psychiatric assistance to achieve a better clinical outcome.
Some limitations of our study should be mentioned. First, data on treatments of depression were not acquired, so it is difficult to determine whether depression management has a positive effect on COPD treatment based on this study. Second, we used only the BDI-II to screen for depression, although this does accord with previous studies.45,46
Conclusions
Depression is highly prevalent in patients with COPD; managing such COPD patients is more difficult compared to the management of COPD patients who are not depressed. Physicians should more actively screen and manage depression by considering the associated patient factors, such as high SGRQ, low BMI, and low 6MWD.
Acknowledgments
This research was supported by Research of Korea Centers for Disease Control and Prevention (2016ER670100, 2016ER670101, 2016ER670102 and 2018ER670100, 2018ER670101).
Disclosure
Chin Kook Rhee has received consulting/lecture fees from MSD, AstraZeneca, GSK, Novartis, Takeda, Mundipharma, Boehringer-Ingelheim, Teva, and Bayer. The authors report no other conflicts of interest in this work.
References
1. Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
2. Hurd S. The impact of COPD on lung health worldwide: epidemiology and incidence. Chest. 2000;117(2 Suppl):1s–4s. doi:10.1378/chest.117.2_suppl.1S
3. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: global Burden of Disease Study. Lancet. 1997;349(9064):1498–1504. doi:10.1016/S0140-6736(96)07492-2
4. Tsai TY, Livneh H, Lu MC, Tsai PY, Chen PC, Sung FC. Increased risk and related factors of depression among patients with COPD: a population-based cohort study. BMC Public Health. 2013;13:976. doi:10.1186/1471-2458-13-976
5. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
6. Schane RE, Walter LC, Dinno A, Covinsky KE, Woodruff PG. Prevalence and risk factors for depressive symptoms in persons with chronic obstructive pulmonary disease. J Gen Intern Med. 2008;23(11):1757–1762. doi:10.1007/s11606-008-0749-z
7. van Manen JG, Bindels PJ, Dekker FW, IJzermans CJ, van der Zee JS, Schade E. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax. 2002;57(5):412–416. doi:10.1136/thorax.57.5.412
8. Wagena EJ, Kant I, van Amelsvoort LG, Wouters EF, van Schayck CP, Swaen GM. Risk of depression and anxiety in employees with chronic bronchitis: the modifying effect of cigarette smoking. Psychosom Med. 2004;66(5):729–734. doi:10.1097/01.psy.0000138127.00991.cf
9. Yohannes AM, Baldwin RC, Connolly MJ. Depression and anxiety in elderly outpatients with chronic obstructive pulmonary disease: prevalence, and validation of the BASDEC screening questionnaire. Int J Geriatr Psychiatry. 2000;15(12):1090–1096.
10. Hynninen KM, Breitve MH, Wiborg AB, Pallesen S, Nordhus IH. Psychological characteristics of patients with chronic obstructive pulmonary disease: a review. J Psychosom Res. 2005;59(6):429–443. doi:10.1016/j.jpsychores.2005.04.007
11. Ng TP, Niti M, Tan WC, Cao Z, Ong KC, Eng P. Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Arch Intern Med. 2007;167(1):60–67. doi:10.1001/archinte.167.1.60
12. Dahlen I, Janson C. Anxiety and depression are related to the outcome of emergency treatment in patients with obstructive pulmonary disease. Chest. 2002;122(5):1633–1637. doi:10.1378/chest.122.5.1633
13. Lee YS, Park S, Oh YM, et al. Chronic obstructive pulmonary disease assessment test can predict depression: a prospective multi-center study. J Korean Med Sci. 2013;28(7):1048–1054. doi:10.3346/jkms.2013.28.7.1048
14. Kunik ME, Roundy K, Veazey C, et al. Surprisingly high prevalence of anxiety and depression in chronic breathing disorders. Chest. 2005;127(4):1205–1211. doi:10.1378/chest.127.4.1205
15. Montserrat-Capdevila J, Godoy P, Marsal JR, et al. Overview of the impact of depression and anxiety in chronic obstructive pulmonary disease. Lung. 2017;195(1):77–85. doi:10.1007/s00408-016-9966-0
16. Kanazawa A, White PM, Hampson SE. Ethnic variation in depressive symptoms in a community sample in Hawaii. Cultur Divers Ethnic Minor Psychol. 2007;13(1):35–44. doi:10.1037/1099-9809.13.1.35
17. Jang Y, Kwag KH, Chiriboga DA. Not saying I am happy does not mean I am not: cultural influences on responses to positive affect items in the CES-D. J Gerontol B Psychol Sci Soc Sci. 2010;65(6):684–690. doi:10.1093/geronb/gbq052
18. Iwata N, Buka S. Race/ethnicity and depressive symptoms: a cross-cultural/ethnic comparison among university students in East Asia, North and South America. Soc Sci Med. 2002;55(12):2243–2252. doi:10.1016/s0277-9536(02)00003-5
19. Li Z, Hicks MH. The CES-D in Chinese American women: construct validity, diagnostic validity for major depression, and cultural response bias. Psychiatry Res. 2010;175(3):227–232. doi:10.1016/j.psychres.2009.03.007
20. Sundh J, Stallberg B, Lisspers K, Montgomery SM, Janson C. Co-morbidity, body mass index and quality of life in COPD using the Clinical COPD Questionnaire. COPD. 2011;8(3):173–181. doi:10.3109/15412555.2011.560130
21. von Leupoldt A, Taube K, Lehmann K, Fritzsche A, Magnussen H. The impact of anxiety and depression on outcomes of pulmonary rehabilitation in patients with COPD. Chest. 2011;140(3):730–736. doi:10.1378/chest.10-2917
22. Lim JU, Lee JH, Kim JS, et al. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int J Chron Obstruct Pulmon Dis. 2017;12:2465–2475. doi:10.2147/COPD.S141295
23. Lim JU, Kim K, Kim SH, et al. Comparative study on medical utilization and costs of chronic obstructive pulmonary disease with good lung function. Int J Chron Obstruct Pulmon Dis. 2017;12:2711–2721. doi:10.2147/COPD.S143244
24. Grothe KB, Dutton GR, Jones GN, Bodenlos J, Ancona M, Brantley PJ. Validation of the Beck Depression Inventory-II in a low-income African American sample of medical outpatients. Psychol Assess. 2005;17(1):110–114. doi:10.1037/1040-3590.17.1.110
25. Steer RA, Clark DA, Beck AT, Ranieri WF. Common and specific dimensions of self-reported anxiety and depression: the BDI-II versus the BDI-IA. Behav Res Ther. 1999;37(2):183–190. doi:10.1016/s0005-7967(98)00087-4
26. Lee K, Kim D, Cho Y. Exploratory factor analysis of the Beck Anxiety Inventory and the Beck Depression Inventory-II in a psychiatric outpatient population. J Korean Med Sci. 2018;33(16):e128. doi:10.3346/jkms.2018.33.e101
27. Lee EJ, Kim JB, Shin IH, et al. Current use of depression rating scales in mental health setting. Psychiatry Investig. 2010;7(3):170–176. doi:10.4306/pi.2010.7.3.170
28. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996.
29. Steer RA, Brown GK, Beck AT, Sanderson WC. Mean Beck Depression Inventory-II scores by severity of major depressive episode. Psychol Rep. 2001;88(3 Pt 2):1075–1076. doi:10.2466/pr0.2001.88.3c.1075
30. Carney CE, Ulmer C, Edinger JD, Krystal AD, Knauss F. Assessing depression symptoms in those with insomnia: an examination of the beck depression inventory second edition (BDI-II). J Psychiatr Res. 2009;43(5):576–582. doi:10.1016/j.jpsychires.2008.09.002
31. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
32. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2019 REPORT). Available from: https://goldcopd.org/.
33. St George’s respiratory questionnaire for COPD Patients (SGRQ-C) Manual. 2016. Available from: http://www.healthstatus.sgul.ac.uk,
34. Lee JY, Chon GR, Rhee CK, et al. Characteristics of patients with chronic obstructive pulmonary disease at the first visit to a pulmonary medical center in Korea: the Korea Copd Subgroup Study Team Cohort. J Korean Med Sci. 2016;31(4):553–560. doi:10.3346/jkms.2016.31.4.553
35. Dowson CA, Town GI, Frampton C, Mulder RT. Psychopathology and illness beliefs influence COPD self-management. J Psychosom Res. 2004;56(3):333–340. doi:10.1016/S0022-3999(03)00040-0
36. Chin HJ, Lee KH, Park CS, et al. Prevalence and risk factors of depression in patients with chronic obstructive pulmonary disease. Tuberc Respir Dis. 2010;69(4):243–249.
37. Gut-Gobert C, Cavailles A, Dixmier A, et al. Women and COPD: do we need more evidence? Eur Respir Rev. 2019;28(151):180055. doi:10.1183/16000617.0055-2018
38. Raherison C, Tillie-Leblond I, Prudhomme A, et al. Clinical characteristics and quality of life in women with COPD: an observational study. BMC Womens Health. 2014;14(1):31. doi:10.1186/1472-6874-14-31
39. Bremmer MA, Beekman AT, Deeg DJ, et al. Inflammatory markers in late-life depression: results from a population-based study. J Affect Disord. 2008;106(3):249–255. doi:10.1016/j.jad.2007.07.002
40. Du YJ, Yang CJ, Li B, et al. Association of pro-inflammatory cytokines, cortisol and depression in patients with chronic obstructive pulmonary disease. Psychoneuroendocrinology. 2014;46:141–152. doi:10.1016/j.psyneuen.2014.04.020
41. Munafo MR, Araya R. Cigarette smoking and depression: a question of causation. Br J Psychiatry. 2010;196(6):425–426. doi:10.1192/bjp.bp.109.074880
42. Chun EM. Smoking cessation strategies targeting specific populations. Tuberc Respir Dis (Seoul). 2019;82(1):1–5. doi:10.4046/trd.2017.0101
43. Lim G, Park I, Park S, Song S, Kim H, Kim S. Effectiveness of smoking cessation using motivational interviewing in patients consulting a pulmonologist. Tuberc Respir Dis (Seoul). 2014;76(6):276–283. doi:10.4046/trd.2014.76.6.276
44. Kim SH, Kim JS, Choi JY, Lee KY, Park TJ, Lee JH. Factors associated with depressive symptom in chronic obstructive pulmonary disease based on the third (2005) and fourth (2008) Korea National Health and Nutritional Examination Survey (KNHANES III, IV). Korean J Fam Med. 2011;32(4):234–242. doi:10.4082/kjfm.2011.32.4.234
45. Kunik ME, Veazey C, Cully JA, et al. COPD education and cognitive behavioral therapy group treatment for clinically significant symptoms of depression and anxiety in COPD patients: a randomized controlled trial. Psychol Med. 2008;38(3):385–396. doi:10.1017/S0033291707001687
46. Phan T, Carter O, Waterer G, et al. Determinants for concomitant anxiety and depression in people living with chronic obstructive pulmonary disease. J Psychosom Res. 2019;120:60–65. doi:10.1016/j.jpsychores.2019.03.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.