Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Difference of COVID-19 Vaccination Attitude, Preventive Measures and Knowledge of SARS-COV-2 Between Diabetic Patients and Healthy Citizens in China
Authors Bao Y, Dong C, Liang Q, Zhang X, Gu Z, Cheng C
Received 25 October 2022
Accepted for publication 5 January 2023
Published 23 February 2023 Volume 2023:16 Pages 493—502
DOI https://doi.org/10.2147/JMDH.S394790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yanfeng Bao,1,2,* Chen Dong,2,* Qian Liang,2 Xiaoming Zhang,3 Zhifeng Gu,2 Chun Cheng1
1School of Medicine & Holistic Integrative Medicine, Nanjing University of Traditional Chinese Medicine, Jiangsu, People’s Republic of China; 2Department of Rheumatology, Affiliated Hospital of Nantong University, Jiangsu, People’s Republic of China; 3Key Laboratory of Molecular Virology & Immunology, Institut Pasteur of Shanghai, Chinese Academy of Sciences, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhifeng Gu; Chun Cheng, Tel +86-13706291941 ; +86-13962952110, Email [email protected]; [email protected]
Purpose: The outbreak of coronavirus disease has become an evolving global health crisis with wide-ranging implications. Clinical researches from several countries have reported greater morbidity and mortality from COVID-19 patients with diabetes. SARS-CoV-2/COVID-19 vaccines are currently the relatively effective means of prevention. The research was aimed to explore the attitudes of diabetic patients towards COVID-19 vaccine and the knowledge of COVID-19 related epidemiology and epidemic prevention.
Methods: This case–control study was carried out in China via online and offline surveys. Knowledge questionnaire of COVID-19 and drivers of COVID-19 Vaccination Acceptance Scale (DrVac-COVID19S) were used to compare the difference of COVID-19 vaccination attitude, preventive measures, and knowledge of SARS-COV-2 between diabetic patients and healthy citizens.
Results: The diabetic patients showed lower vaccination willingness and insufficient knowledge of the transmission route and common symptoms of COVID-19. Only 60.99% diabetic patients were willing to be vaccinated. Less than half of diabetics knew the COVID-19 spread by surface touch (34.04%) or aerosol (20.57%). The common symptoms like shortness of breath/ anorexia/ fatigue/ nausea/vomiting/diarrhea (34.04%) and panic and chest tightness (19.15%) were not well comprehend too. Diabetes patients shown lower report intentions when they contact a person infected with the virus (81.56%) or have any of the disease symptoms (74.47%). Values, knowledge, and autonomy assessed by the DrVac-COVID19S scale also showed negative attitude of vaccination in patients with diabetes. Also, patient with diabetes pay less attention to national (56.03%) and international (51.77%) COVID-19 updates. The willingness to attend COVID-19 lectures (27.66%) or read information leaflets (70.92%) was low.
Conclusion: Vaccination is the effective available method for preventing the virus. Social and medical workers can increase the vaccination of diabetic patients through knowledge’s popularization and patient’s education based on the above differences.
Keywords: COVID-19, diabetic patients, COVID-19 vaccination, SARS-COV-2, knowledge-attitude-behavior
Introduction
Coronavirus disease 2019 (COVID-19), caused by syndrome coronavirus-2 (SARS-CoV-2), is an ongoing global pandemic. It has become the most impactful epidemic in the recent years.1 Recently, the comprehensive knowledge of the coronavirus and effective coping methods bring about a gradual decline in the mortality of COVID-19. However, due to the constant mutation of the virus, COVID-19 is still highly contagious among humans, which leads to side effects to human daily life and socioeconomic development.2 Hundreds of millions of people’s health, work and normal life are affected in varying degrees. Until December 2022, there are still tens of millions of confirmed cases and hundreds of thousands of new cases every day.3 Safe and effective COVID-19 vaccine is the most effective measure by far. More than 200 vaccines are in research around the world, and more than a dozen of them are in clinical trials.4 By the end of 2022, National Health Commission of the People’s Republic of China reported that 3.4 billion doses of COVID-19 vaccine had been administered. Almost all healthy people have been vaccinated against COVID-19 in China.5 The vast majority of people’s overall attitude towards vaccines has undergone a change from the suspicion and hesitation at the beginning to the confidence and acceptation at present.
Analysis of clinical and epidemiological data on COVID-19 show that specific comorbidities such as diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular diseases (CVD), HIV, increased the risk of infection, leading to more severe lung damage and death.6,7 Clinical studies shown acute viral respiratory tract infection in diabetic patients often leads to serious complications, such as respiratory distress syndrome like pneumonia, acute respiratory or organ failure and death. Diabetes has been reported as an independent predictor of mortality from SARS-COV infection. A meta-analysis of 2455 COVID-19 cases revealed that diabetic people with COVID-19 were more likely to develop into critical illness.8 The report also noted that diabetes is a high proportion of comorbidities among COVID-19 deaths. In the case report of 72,314 COVID-19 samples from the Chinese Center for Disease Control and Prevention, the mortality rate among patients with diabetes was 7.3% compared with 2.3% overall.9 Data from Italy also suggested that two-thirds of these dead patients also suffered from diabetes or other comorbidities.10 Patients with diabetes have always been in chronic inflammatory state. The state of COVID-19 viral infection may contribute to cytokine storms, which lead to adverse results and eventually death.11,12
The high morbidity and mortality suggested more personalized and effective treatments were needed for patients with diabetes.13 However, there is no effective treatment for COVID-19 worldwide. Diabetic patients not only are confronted with increased risk of infection, but also poor outcome in SARS-CoV-2 infections.14 In this novel coronavirus pandemic, it was reported that diabetic patients had a 2- to 3-fold increase risk of endpoint of ICU and death for COVID-19.14,15 A new study shows that diabetes patients have increased levels of antiviral antibodies after being vaccinated. Also, large sample studies shown that antibody response and seropositivity in diabetes patients were lower than control group after COVID-19 vaccination dose.16,17 Strengthening the vaccination for diabetic patients would be one of the most convenient, effective, and more affordable strategy. There is little report focused on the diabetes patients’ attitude to COVID-19 vaccination and contributing factors. This study collected 141 Chinese diabetic patients to explore their attitudes towards COVID-19 vaccination, and investigated the patients’ knowledge about COVID-19, vaccination and prevention measures, so as to provide information for promoting the vaccination of COVID-19 vaccine in patients with diabetes.
Methods
Participants
This case–control study was conducted in China in June 2021. We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments. Due to the pandemic situation, this study was conducted mainly based on the online software of Wen Juan Xing (Changsha Ranxing Information Technology Co., Ltd., Hunan, China), which is the most common online survey platform in China. Due to the software background design, questionnaires were collected without blank in this survey. All the participants clicked the link and completed the questionnaire were considered as consent informed. Considering the selection bias caused by internet use, age, knowledge level and other factors, we also conducted an offline study in rural area in Nantong, Jiangsu Province, and informed consent form was signed by all of them. Based on self-report, participants reported their health status, such as healthy, diabetes, tumor, auto-immune diseases and any other type of diseases. Participants who chose the option of healthy and diabetes were included in the study. Among them, who chose the option of tumor, auto-immune diseases, and other disease were excluded, except for hypertension. In the present study, 307 participants were included and divided into two groups (141 diabetic patients and 166 healthy participants). All the participants had not been infected with SARS-CoV-2.
Self-Reported Questionnaires
Demographic variables including gender, age, place of residence, marital status, educational level, tobacco use, alcohol use, income, attitude of vaccination.
Knowledge questionnaire of COVID-19 was design according to the disease symptoms and existing researches. The main reference was the reports by Abdelhafiz AS.18
COVID-19 Vaccination Acceptance Scale (DrVac-COVID19S)19 was conducted in this study, which reveal different attitude mechanism and considerations to COVID-19 vaccination. DrVac-COVID19S contains nine positive items (1 to 6, 8, 9 and 12) and three negative items (7, 10 and 11). The scale helped the researchers analyze the subjects’ attitudes toward vaccines from four dimensions: value, impacts, knowledge, and autonomy. A higher DrVac-COVID19S score indicates higher COVID-19 vaccine acceptance.
Data Analysis
The data were expressed as mean ± SD for normally distributed variables and analyzed by Student’s t-test. Median and interquartile range (IQR) for nonnormally distributed variables and analyzed by Mann–Whitney U-tests. Number and frequencies (%) for categorical variables. Group differences were assessed using the chi-square test. Statistical significance was considered when P<0.05 (two-sided). All analyses were performed in SPSS version 21.0.
Results
Participant Characteristics
141 diabetic patients and 165 healthy individuals were enrolled in the current study. The whole experimental process is shown in Figure 1. Age and sex were matched in the two groups. The median age of the healthy individuals was 50, and 53.01% of the respondents were male. 52% of diabetic patients were men, and the median age was 45. There was no significant difference in the ages and genders between the two groups. Table 1 presents their attitude about COVID-19 vaccines and the sociodemographic data. In this study, 98.8% healthy individuals were willing to be vaccinated, 0.6% refused and 0.6% hesitated. While only 60.99% diabetic patients were willing to be vaccinated and the percentage of refusal and hesitation even up to 24.82% and 14.18%.
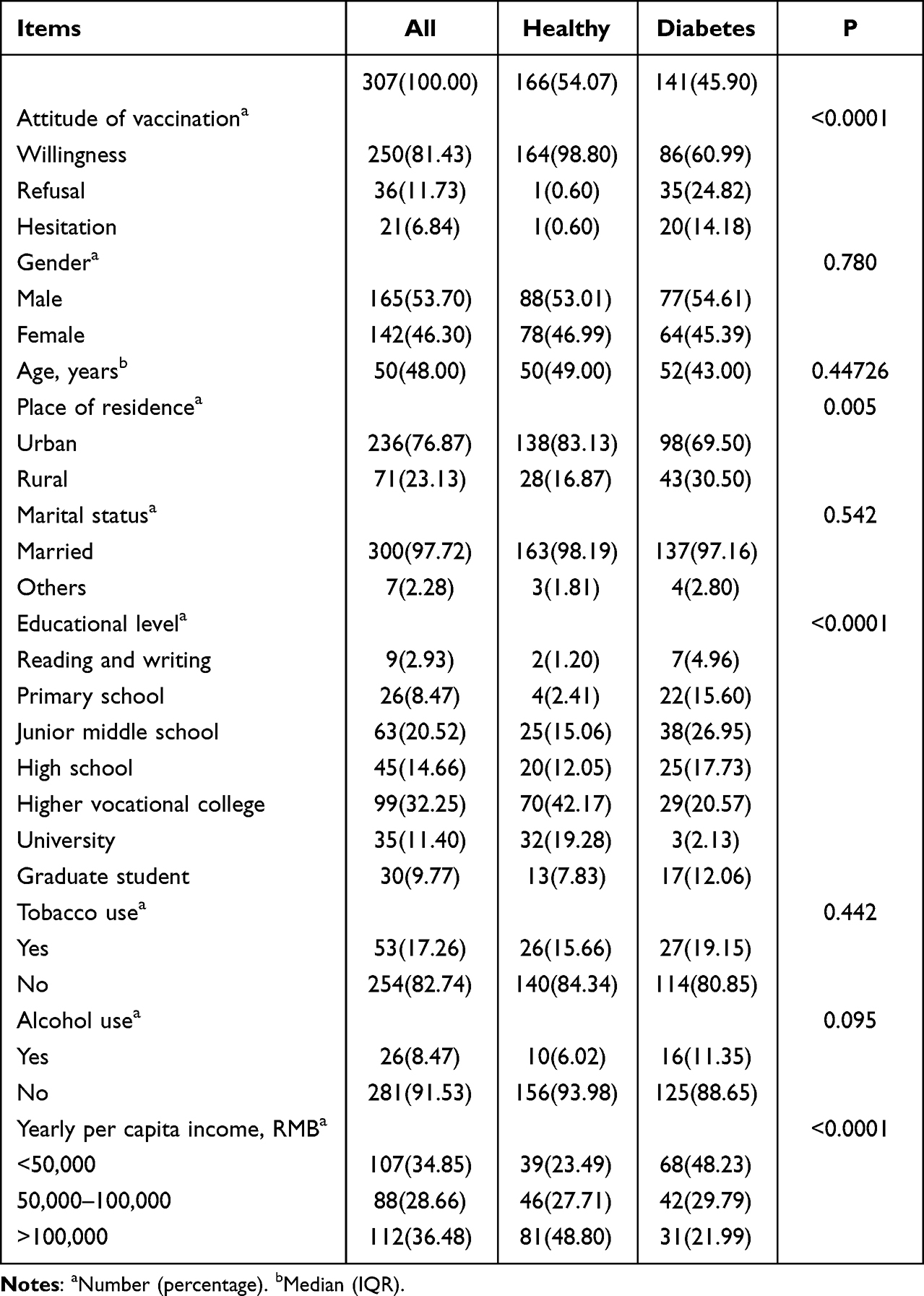 |
Table 1 Attitude About COVID-19 Vaccines and the Sociodemographic Data |
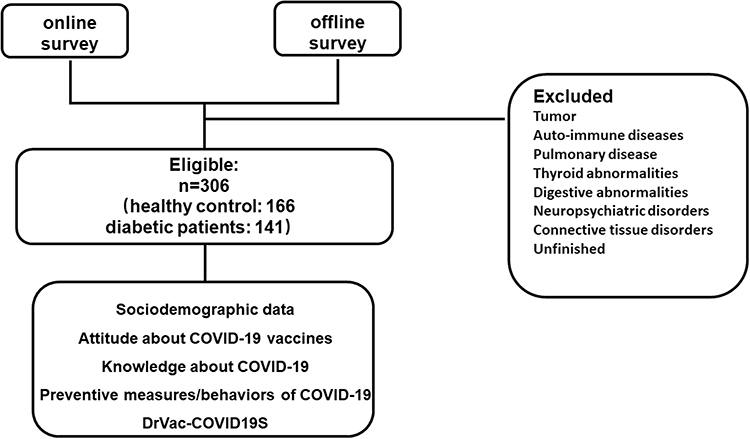 |
Figure 1 Study process. |
Knowledge About COVID-19 in Diabetic Patients and Healthy Individuals
Compared with healthy control, patients with diabetes showed poorer knowledge on COVID-19 both in terms of transmission routes and common symptoms. Most healthy participants were aware of the main route of transmission of SARS-COV-2. As is shown in Table 2, 96.99% healthy individuals knew COVID-19 spreads by droplets of affected person, but only 76.6% diabetic patients know about this. 66.87% and 66.27% healthy individuals knew COVID-19 spreads by surfaces touched by affected person and aerosol transmission. However, 65.96% and 79.63% diabetic patients do not know the spread way of surfaces touched by affected person and aerosol transmission. Both the diabetic patients and healthy individuals do not know the virus spread through food and oral-fecal transmission way (healthy control: 61.45% and 62.05%; diabetic patients: 87.94% and 90.07%).
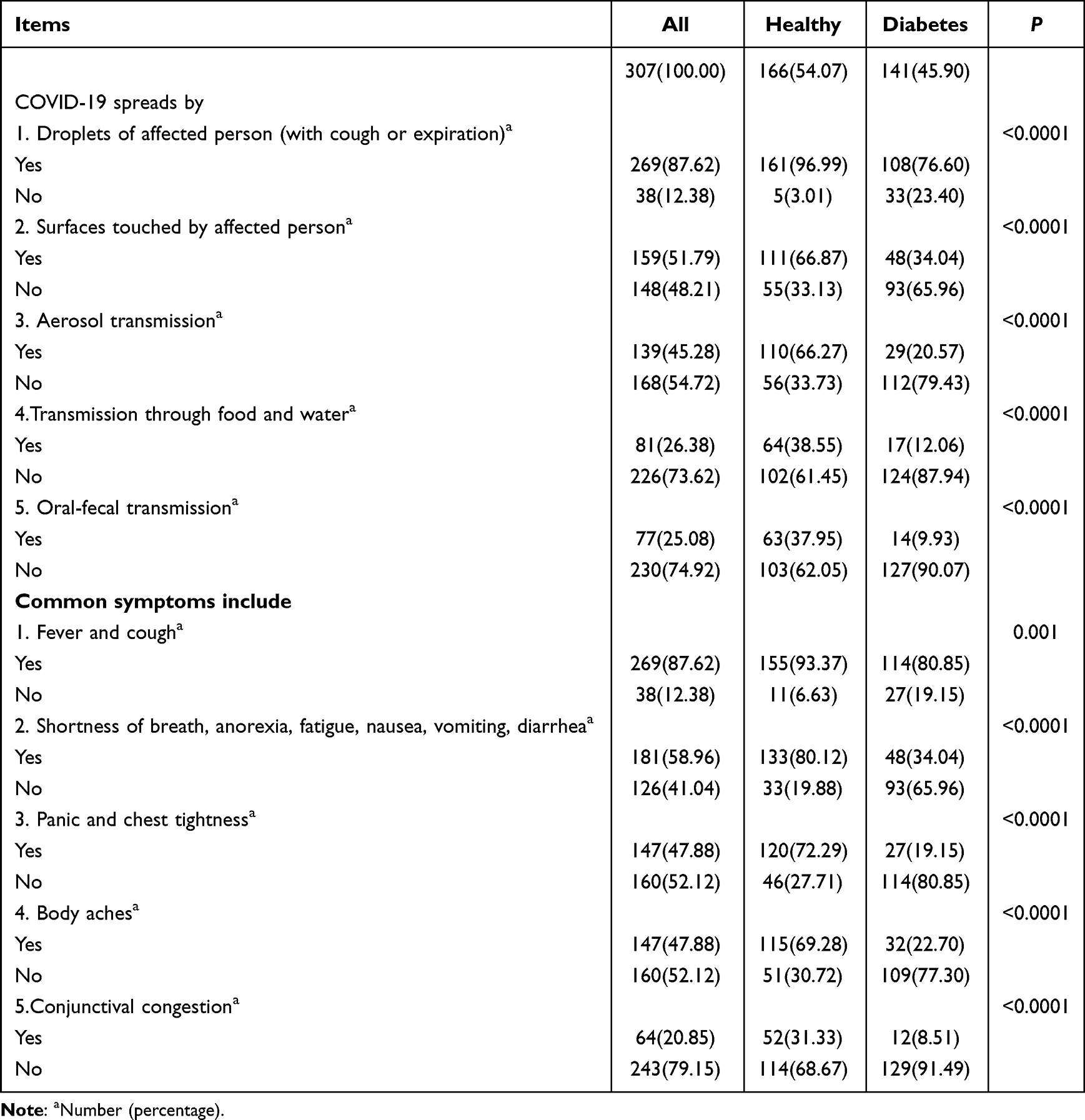 |
Table 2 Knowledge About COVID-19 in Diabetic Patients and Healthy Control |
Healthy people have a good knowledge of common symptoms, such as fever and cough (93.37%), shortness of breath/anorexia/fatigue/nausea/vomiting/diarrhea (80.12%), panic and chest tightness (72.29%) and body aches (69.28%). 80.85% diabetic patients knew the fever and cough were the common symptoms. However, diabetic patients showed poor knowledge about common symptoms like shortness of breath/anorexia/fatigue/nausea/vomiting/diarrhea (65.96%), panic and chest tightness (80.85%) and body aches (77.3%). It is worth noting that most patients with diabetes (91.49%) and healthy individuals (68.87%) do not know much about conjunctival congestion. All showed in Table 2.
Preventive Measures/Behaviors of COVID-19 in Diabetic Patients and Healthy Individuals
People with diabetes shown better understanding of COVID-19 prevention. Diabetic patients tend to avoid handshake (63.83%) and hug (85.11%) in the daily life, while the behavior of wash hands (38.30%) needed to be improved. More than 90% of all the participants know the importance of wearing the facemask in the COVID-19 prevention and agreed to isolate at home or at an isolation hospital. But when the diabetic patients face the exposure of SARS-CoV-2 or the occurrence of possible symptoms related to COVID-19, they showed lower reporting rate (81.56% and 74.47%). Diabetic patients believe the isolation may affect the salary (p < 0.05). We also found out nearly half of diabetic patients show low attention on the updates on the national (56.03%) and international (51.77%) spread situation of the coronavirus. Meanwhile, diabetic participants showed lower intention to actively acquire knowledge via attending a lecture (27.66%) or following the instruction from a brochure (70.92%). All the above show in Table 3 and Table S1.
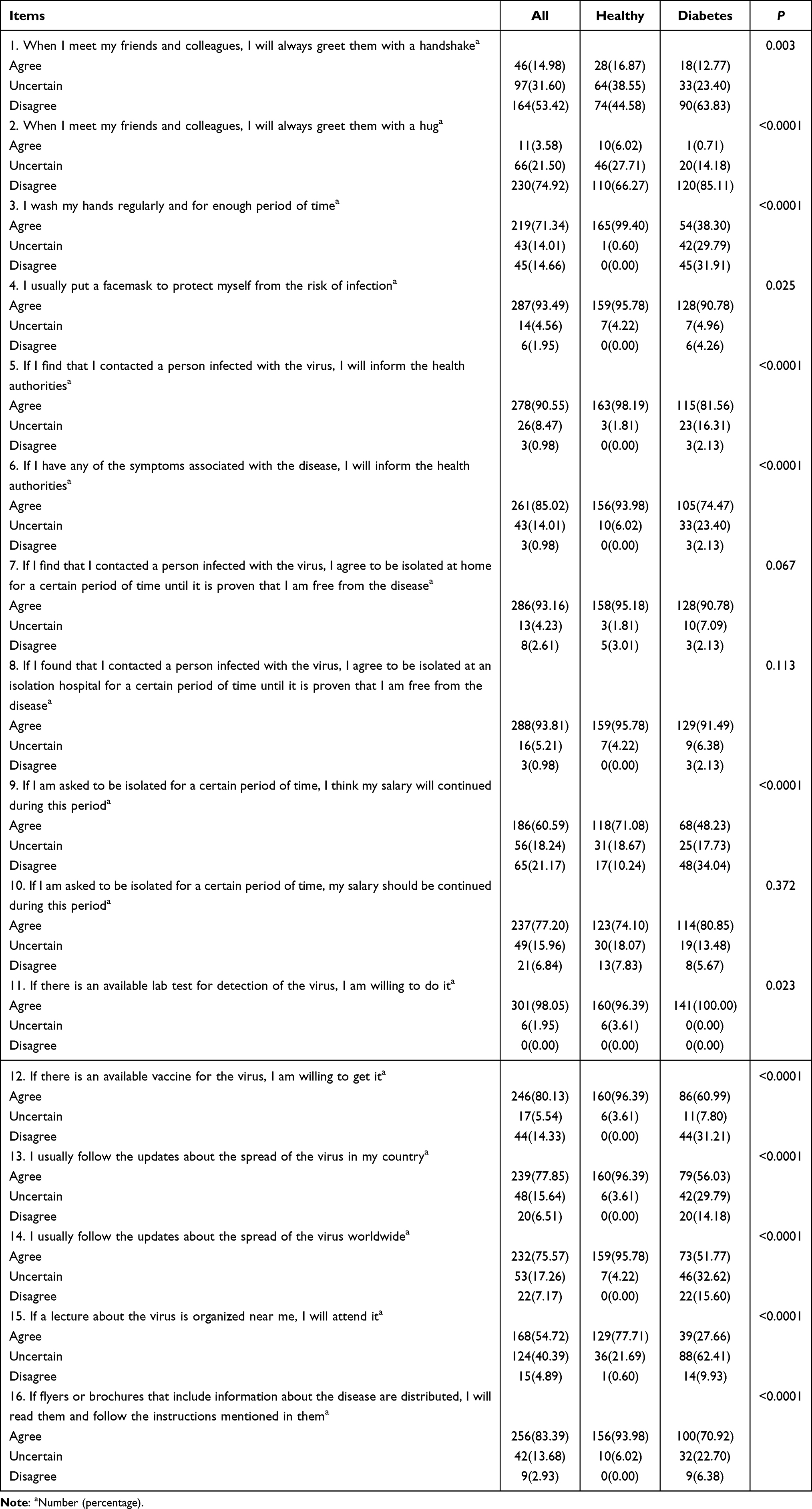 |
Table 3 Preventive Measures/Behaviors of COVID-19 in Diadetic Patients and Healthy Control |
Knowledge of COVID-19 Vaccination in Diabetic Patients and Healthy Individuals
The scale of DrVac-COVID19S in Table 4 and Table S2 represented the knowledge of COVID-19 vaccination. At the same time, DrVac-COVID19S value the underline attitude mechanism to COVID-19 vaccination in dimensions like value, impacts, knowledge and autonomy. The score of diabetic patients (62.6) was quite lower than the control (69.94). The score of value, knowledge and autonomy were all lower among diabetic patients. Moreover, most related dimension items of DrVac-COVID19S shows the statistical difference between two groups. These results revealed the underlying attitude mechanism of diabetic patients to the COVID-19 vaccination. All the above are shown in Table 4 and Table S2.
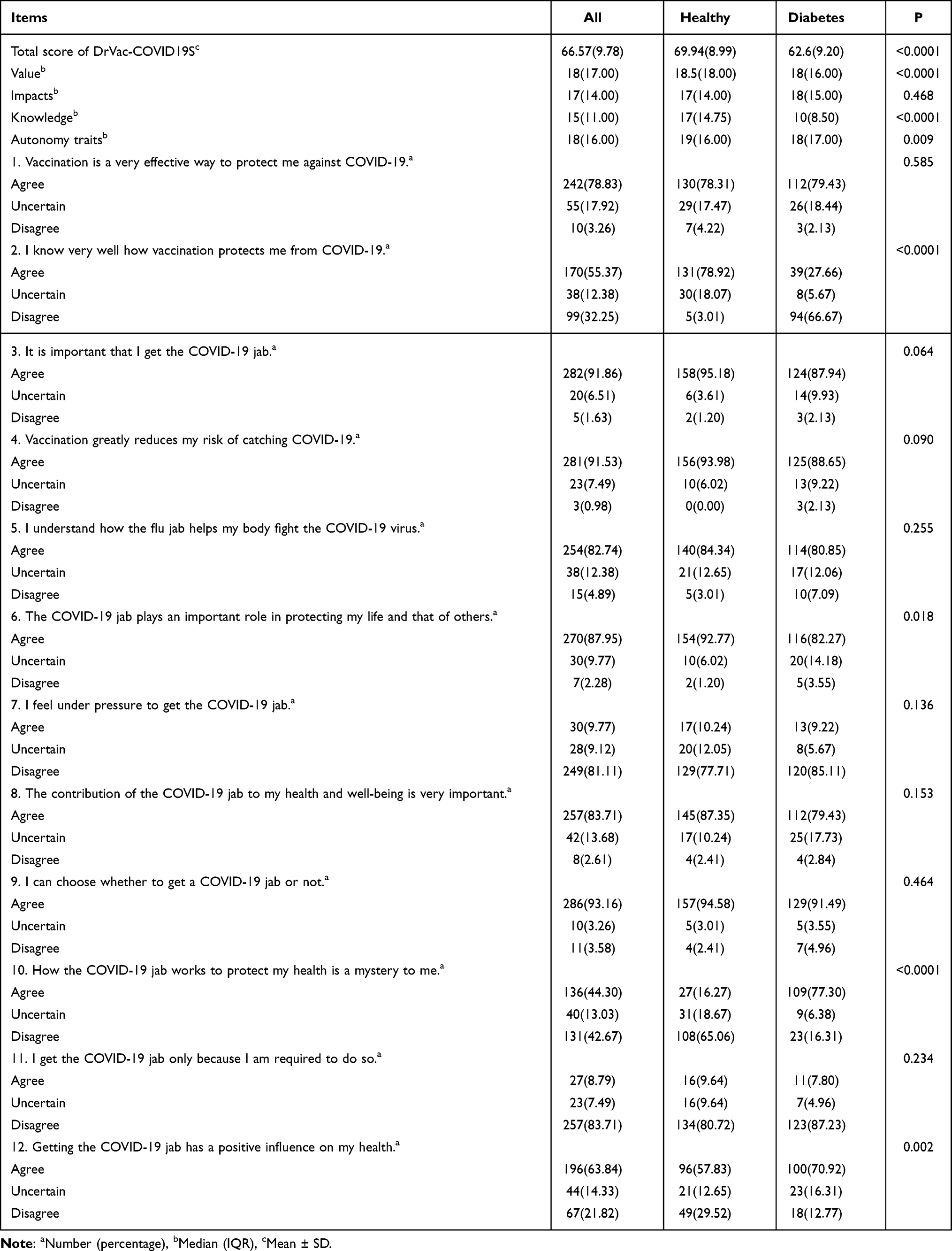 |
Table 4 Knowledge of COVID-19 Vaccination in Diabetic Patients and Healthy Control |
Discussion
With the constant variation of SARS-CoV-2, prevention, and control of COVID-19 still take a heavy burden. Antiviral drugs and immunosuppressants can relieve symptoms to a certain extent, but there is no effective treatment for COVID-19.20,21 COVID-19 vaccine is currently a relatively effective and safe approach. Patients with diabetes need to strengthen self-protection in the COVID-19 epidemic, especially to be vaccinated.22 Therefore, people with diabetes should receive vaccination according to dose and schedule, and may receive vaccine booster as a priority.
In this study, 98.80% participants were willing to be vaccinated, which is like the other study in China.23,24 While only 60.99% diabetes patients show the willingness to COVID-19 vaccination. 39% patients had vaccine hesitancy, including 14.18% who were unsure and 24.82% who were unwilling. Another cross-sectional survey about the attitude of diabetic patients to COVID-19 Vaccine, in Shanxi, China, show the same low willingness.25 Therefore, it is necessary to explore the contributing factors behind the low willingness and help the public health experts promote vaccination for diabetic groups and extend herd immunity. According to health behavior theory, risk perception is the core of individual preventive behavior. Risk communication forms the basis of risk perception, thereby promoting accurate knowledge and making preventive behaviors and practices possible.26,27 In conclusion, public compliance with preventive measures is critical to reducing the widespread spread of COVID-19. Therefore, raising public awareness and stepping up vaccination is an essential element of the overall public health response to the COVID-19 pandemic.
The correlation between the attitude to vaccination and the knowledge about COVID-19 was reported before.28 In this study, most healthy citizens comprehend the knowledge of COVID-19, while the diabetes patients showed significant lack in knowledge. The diabetic patients need good education about the mode of transmission and the common symptoms of COVID-19. Perhaps because of the long-term state of illness, diabetic patients show a good sense of protection, reducing handshaking, hugging, and wearing masks, even stronger than healthy citizens.
Even though the Chinese government has given preferential policies for COVID-19 diseases, such as free medical treatment and vaccines, participants with diabetes still show concern about the impact of illness. Also, patients with diabetes showed lower attention to the disease than healthy citizens, which may be related to the exhaustion of medical information for patients with long-term illness. Upon this, clinicians can introduce the COVID-19 vaccine during regular medical visits of participants with diabetes. At the same time, participants with diabetes have less knowledge about vaccines than the healthy citizens. Governments and health experts can provide information to people with diabetes about the value of vaccines, knowledge about vaccines and encouraging them to be vaccinated. There are also some limitations in this study. First, the sample size is not enough to form different subgroups explore the effect of disease status or other interesting variables. Secondly, it is found that there are significant differences between residence, and education level, which needed more attention in the future.
Conclusion
It was revealed in this study that diabetic patients show negative acceptance of COVID-19 vaccination than healthy individuals. Patients have insufficient attention to the transmission of COVID-19, and symptoms in the pandemic. Meanwhile, patients showed differences in the values, knowledge, and autonomy of COVID-19 vaccine. Based on these results, government and social workers can take measures to increase vaccination coverage among participants with diabetes.
Data Sharing Statement
All the data could be available from the corresponding author (Zhifeng Gu).
Ethics Approval
The study was approved by the Ethics Committee of the Affiliated Hospital of Nantong University (approval number:2021-K059-01).
Funding
This work was supported by the National Key Research and Development Program of China [Grant Number 2021YFE0200600].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tian D, Sun Y, Xu H, Ye Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 Omicron variant. J Med Virol. 2022;94:2376–2383. doi:10.1002/jmv.27643
2. Salzberger B, Buder F, Lampl B. Epidemiology of SARS-CoV-2. Infection. 2021;49:233–239. doi:10.1007/s15010-020-01531-3
3. Li J, Lai S, Gao GF, Shi W. The emergence, genomic diversity and global spread of SARS-CoV-2. Nature. 2021;600:408–418.
4. Kostoff RN, Briggs MB, Porter AL, Spandidos DA, Tsatsakis A. COVID‑19 vaccine safety. Int J Mol Med. 2020;2020(46):1599–1602.
5. Lai X, Zhu H, Wang J. Public perceptions and acceptance of COVID-19 booster vaccination in china: a cross-sectional study. Vaccines. 2021;9(12):1461. doi:10.3390/vaccines9121461
6. Zhou F, Yu T, Du R. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
7. Ejaz H, Alsrhani A, Zafar A. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Health. 2020;13(12):1833–1839. doi:10.1016/j.jiph.2020.07.014
8. Wu J, Zhang J, Sun X. Influence of diabetes mellitus on the severity and fatality of SARS-CoV-2 (COVID-19) infection. Diabetes Obes Metab. 2020;22(10):1907–1914. doi:10.1111/dom.14105
9. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in china: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
10. Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet. 2020;395:1225–1228. doi:10.1016/S0140-6736(20)30627-9
11. Mehta P, McAuley DF, Brown A, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033–1034. doi:10.1016/S0140-6736(20)30628-0
12. Maddaloni E, Buzzetti R. Covid-19 and diabetes mellitus: unveiling the interaction of two pandemics. Diabetes Metab Res Rev. 2020;36(7):e33213321. doi:10.1002/dmrr.3321
13. Zhou Y, Chi J, Lv W, Wang Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (Covid-19). Diabetes Metab Res Rev. 2021;37:e3377. doi:10.1002/dmrr.3377
14. Hamer M, Gale CR, Batty GD. Diabetes, glycaemic control, and risk of COVID-19 hospitalisation: population-based, prospective cohort study. Metabolism. 2020;112:154344. doi:10.1016/j.metabol.2020.154344
15. McGurnaghan SJ, Weir A. Risks of and risk factors for COVID-19 disease in people with diabetes: a cohort study of the total population of Scotland. Lancet. 2021;9:82–93. doi:10.1016/S2213-8587(20)30405-8
16. Ali H, Alterki A, Sindhu S. Robust antibody levels in both diabetic and non-diabetic individuals after BNT162b2 mRNA COVID-19 vaccination. Front Immunol. 2021;12:752233. doi:10.3389/fimmu.2021.752233
17. Soetedjo NNM, Iryaningrum MR, Lawrensia S, Permana H. Antibody response following SARS-CoV-2 vaccination among patients with type 2 diabetes mellitus: a systematic review. Diabetes Metab Syndr. 2022;16:102406. doi:10.1016/j.dsx.2022.102406
18. Abdelhafiz AS, Mohammed Z, Ibrahim ME. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;45:881–890. doi:10.1007/s10900-020-00827-7
19. Yeh YC, Chen IH, Ahorsu DK. Measurement invariance of the drivers of COVID-19 vaccination acceptance scale: comparison between Taiwanese and Mainland Chinese-speaking populations. Vaccines. 2021;9:297. doi:10.3390/vaccines9030297
20. Jamaati H, Hashemian SM, Farzanegan B. No clinical benefit of high dose corticosteroid administration in patients with COVID-19: a preliminary report of a randomized clinical trial. Eur J Pharmacol. 2021;897:173947. doi:10.1016/j.ejphar.2021.173947
21. Sterne JAC, Murthy S, Diaz JV; Group, W. H. O. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: a meta-analysis. JAMA. 2020;324(13):1330–1341. doi:10.1001/jama.2020.17023
22. Powers AC, Aronoff DM, Eckel RH. COVID-19 vaccine prioritisation for type 1 and type 2 diabetes. Lancet. 2021;9:140–141. doi:10.1016/S2213-8587(21)00017-6
23. Wang J, Jing R, Lai X. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines. 2020;8(3):482. doi:10.3390/vaccines8030482
24. Lin Y, Hu Z, Zhao Q. Understanding COVID-19 vaccine demand and hesitancy: a nationwide online survey in China. PLoS Negl Trop Dis. 2020;14(12):e0008961. doi:10.1371/journal.pntd.0008961
25. Wang Y, Duan L. COVID-19 vaccine hesitancy and associated factors among diabetes patients: a cross-sectional survey in Changzhi, Shanxi, China. Vaccines. 2022;10:129.
26. Brug J, Aro AR, Richardus JH. Risk perceptions and behaviour: towards pandemic control of emerging infectious diseases: international research on risk perception in the control of emerging infectious diseases. Int J Behav Med. 2009;16:3–6. doi:10.1007/s12529-008-9000-x
27. Brug J, Oenema A, Ferreira I. Theory, evidence and Intervention Mapping to improve behavior nutrition and physical activity interventions. Int J Behav Nutr Phys Act. 2005;2:2. doi:10.1186/1479-5868-2-2
28. Dong C, Liang Q, Ji T. Determinants of vaccine acceptance against COVID-19 in China: perspectives on knowledge and DrVac-COVID19S scale. Int J Environ Res Public Health. 2021;18(21):11192. doi:10.3390/ijerph182111192
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023