")
Back to Journals » International Journal of General Medicine » Volume 16
The Diagnostic Value of Blood Next-Generation Sequencing in Early Surgical Site Infection After Spine Surgery
Received 20 October 2022
Accepted for publication 28 December 2022
Published 5 January 2023 Volume 2023:16 Pages 37—45
DOI https://doi.org/10.2147/IJGM.S394255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Nan Zhang, Lei Ma, Wenyuan Ding
Department of Spine Surgery, 3rd Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
Correspondence: Wenyuan Ding, Department of Spine Surgery, 3rd Hospital of Hebei Medical University, Shijiazhuang, Hebei Province, 050051, People’s Republic of China, Email [email protected]
Objective: To determine the diagnostic value of blood next-generation sequencing (NGS) in early surgical site infection after spine surgery. Because the blood is sterile in healthy individuals, it is expected that blood NGS is both sensitive and specific for the detection of infection.
Methods: A total of 28 patients with definitive spinal surgical site infections and controls (n=30) were retrospectively included. The postoperative results of NGS and culture on different samples, such as blood and drainage fluid, were obtained and compared to evaluate the diagnostic value of blood NGS. The diagnostic value parameters (sensitivity, specificity, etc.) were calculated.
Results: Among the four bacteriological exam methods, blood NGS was both sensitive and specific for the determination of infection after spine surgery. The sensitivities of blood and drainage fluid NGS were similar (0.82 vs 0.89, P=0.617). However, the specificities of the two assessments differed, which were 0.97 for blood NGS and 0.40 for drainage fluid NGS (P< 0.001). The sensitivities of bacterial culture were lower than those of NGS (blood: 0.82 vs 0.25, P< 0.001; drainage fluid: 0.89 vs 0.61, P< 0.001), regardless of the sample type. However, the specificities of bacterial culture were equal to or higher than those of NGS (blood: 0.97 vs 0.97, P=1.000; drainage fluid: 0.40 vs 0.80, P=0.002).
Conclusion: This article emphasizes the superiority of blood NGS in infection detection and bacterial determination in patients undergoing spine surgery. Compared with traditional drainage fluid bacterial culture and NGS, blood NGS was more sensitive and specific, and its extensive application could be expected.
Keywords: next-generation sequencing, diagnostic test, surgical site infection, spine surgery
Introduction
Spinal surgeries are commonly performed in patients with degenerative spine diseases, such as lumbar disc herniation, spinal stenosis, and spondylolisthesis.1 For these patients, discectomy and vertebral fusion with internal fixation via a posterior approach is the most classic surgical treatment protocol.2–4 However, Aleem et al5 reported that the incidence of deep postoperative infection following spine surgery, which is one of the most common complications resulting in hospital readmission and results in an extension of hospital length of stay by approximately 9.7 days, ranges from 1% to 4%. Nasser et al6 emphasized that over 156,000 spine infections could potentially be averted with appropriate screening. Therefore, the on-time diagnosis of infection and the accurate identification of the nature of the bacterial infection become crucial when managing such a patient who is suspected to be infected postoperatively.7
Bacterial culture is the most classic method commonly used for bacterial identification.8 Other methods, such as 16S RNA sequencing and PCR-hybridization, are also used in some cases.9–11 The predominant limitation of these methods is their relatively low sensitivity.12,13 For example, Esteban9 reported that PCR could identify 71.6% of implant-related infections. Behera11 found that 16S rRNA could identify the presence of bacterial pathogens in only 54.63% of cases. Yin et al14 reported that the sensitivity of culture in patients with periprosthetic joint infection was 46.7%. To overcome this issue, next-generation sequencing (NGS) has recently been introduced and used for the identification of surgical site infections in orthopedic patients.15 Yin et al14 reported that the sensitivity of intraoperative NGS was up to 0.933 for the identification of periprosthetic joint infections. However, this does not mean that NGS is a perfect exam method without any limitations. Indeed, for samples from germ-free sites, such as the blood, cerebrospinal fluid, and deep tissues, the sensitivity, specificity and accuracy of NGS are higher than those of other diagnostic methods.16–18 Therefore, the diagnostic value of intraoperative NGS is reliable.19 However, not every infected patient undergoes debridement surgery.20 For these patients, a lack of intraoperative NGS results might increase the occurrence of misdiagnosis. In addition, intraoperative NGS results could not be used before surgery to aid the determination of whether infection is present or to determine the identities of the infected bacteria. Incision drainage fluid, such as purulence, might also contain infectious bacteria.21 NGS could be used to identify these bacteria from incision drainage samples.22 However, as an extraordinarily sensitive diagnostic method, the specificity of NGS in these samples could be dramatically decreased due to the existence of resident bacteria on the skin surface.17 Especially for noninfected individuals, false positive results might be identified, resulting in the misdiagnosis of infection.22
Consequently, understanding how to skillfully use the ultrahigh sensitivity of NGS in the determination of early surgical site infection is crucial. Ideally, the infection should be identified immediately after occurrence with high sensitivity and specificity.23 In this case, blood is considered to be a perfect sample, since the infected bacteria might be identified and cultured from the blood of patients with surgical site infection.24 The ultrahigh sensitivity enables NGS to be used to correctly identify infectious bacteria even if there are only a small amount of bacteria in the blood.25,26 Moreover, blood samples are less affected by contamination from resident bacteria.26 Therefore, NGS is expected to be both sensitive and specific when blood samples are used for examination.27 In this study, patients undergoing spinal surgery for degenerative diseases via a posterior approach with early surgical site infection were retrospectively analyzed. Blood NGS was performed to assess for infection, and its diagnostic value was compared with those of other traditional bacterial detection methods. The hypothesis was that blood NGS is both sensitive and specific.
Methods
Study Design
This study was designed as a diagnostic test. Patients with spinal surgical site infections and controls were retrospectively involved. For each patient, the final clinical diagnosis, which comprehensively integrated the results of radiological examinations, the antibiotic treatment effects, the bacterial culture results and the NGS results, was considered to be the “gold standard” diagnosis. The diagnostic values (sensitivity, specificity, etc.) obtained using both NGS and bacterial culture of the blood samples and drainage samples were calculated and compared.
Participants
Patients who underwent spinal surgery for degenerative diseases via a posterior approach and were diagnosed with postoperative surgical site infection from Jan 2019 to Dec 2021 were retrospectively involved in this study. This study was approved by the Institutional Review Board of the Third Hospital of Hebei Medical University (No. K2022-005-027) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all individuals before they participated in the study. The diagnosis of surgical site infection was based on the guidelines for the prevention of surgical site infection.28–30 In this study, superficial infection, deep infection and organ/space infection were not distinguished since the deep fascia tissue might not heal in the early stage after surgery.31 Only patients who underwent surgery via the posterior approach were included because the posterior approach is the classic approach and is commonly used in spinal surgery for lumbar disc herniation, spinal stenosis and spondylolisthesis.24,32 Therefore, the impact of the results and conclusion of this study should be limited to those surgeries performed via the posterior approach.
The inclusion criteria are described as follows: (1) Patients with degenerative spinal diseases; (2) patients in which spinal surgery was performed via the posterior approach; (3) patients with early surgical site infection (infection occurrence within 30 days after surgery); (4) patients who had undergone debridement surgery and in whom the infection was confirmed by an intraoperative sample, or if the bacterial culture of the intraoperative sample was negative, the bacterial cultures of the drainage sample were positive at least three times (with the same bacteria being identified). The exclusion criteria were as follows: (1) patients in whom minimally invasive techniques were used without an incision bigger than 5 cm;31 (2) patients with definitive infectious lesions in other tissues or organs before surgery; (3) patients who were suspected to have infection but not finally diagnosed with infection; and (4) patients with insufficient definitive bacteriological diagnosis.
According to the inclusion and exclusion criteria above, a total of 28 patients were included and analyzed. In addition, 30 healthy volunteers were also involved in this study and were regarded as the control group. These healthy volunteers had undergone spinal surgery, but no surgical site infection was identified. Initial sample size calculations were performed assuming that blood bacterial culture was 40% sensitive for the diagnosis of these patients. Moreover, blood NGS was 80% sensitive.33 When the test power and significance level were set to 0.80 and 0.05, respectively, the numbers of patients and controls needed were 20 for each. Therefore, the sample size in this study was considered sufficient.
Clinical Evaluation and Assessment of Infection
Demographic information (such as age, sex, etc.) of the patients in both groups was obtained from the medical records. Complete blood count, C-reactive protein and erythrocyte sedimentation rate and procalcitonin levels were routinely examined on the first day and 5th day postoperatively in both groups. If infection was suspected by clinical surgeons, additional laboratory examination was performed. For infected patients, the first-time laboratory examination results after the identification of infection were obtained and analyzed. For the other patients, the results of laboratory examination on the 5th day postoperatively were used for analysis.
Bacterial Culture
For the infected patients, drainage fluid bacterial culture was performed immediately after the suspicion of infection. The bacterial cultures of the drainage fluid were performed at least three times (every 24 hours) before the debridement surgery, including at least one bacterial culture performed before the application of antibiotics. For the healthy volunteers, drainage fluid bacterial cultures were performed on the second day after surgery when fresh dressings were changed. Blood bacterial culture was also performed immediately after the suspicion of infection. The intraoperative samples, including local tissues and fluid, were also collected and cultured (also underwent NGS). For each patient, the results of the first drainage fluid bacterial culture, blood bacterial culture and intraoperative bacterial culture were used for analysis. Both aerobic and anaerobic cultures were performed for at least 7 days.
Next-Generation Sequencing
The samples used for NGS were obtained together with the corresponding bacterial culture samples. Metagenomic NGS was performed in this study according to a previously described method.34,35 Here, the NGS detection procedures are briefly described. ① Either the blood sample or the drainage fluid sample was transferred to a 2 mL microcentrifuge tube, which was attached to a horizontal platform on a vortex mixer and vigorously agitated at 3000 rpm for 20 min. The centrifugal supernatant was obtained and used for further analysis. ② DNA was extracted by using the QIAamp Micro DNA Kit (TIANGEN BIOTECH) according to the manufacturer’s instructions. The extracted DNA was quantified by Qubit 2.0 (Invitrogen, USA), and up to 200 ng was used to generate libraries. ③ A QIAseq™ Ultralow Input Library Kit (Illumina) was then used to generate the DNA libraries. PCR amplification was then performed since the DNA concentration in blood samples was potentially extremely low. ④ The samples were sequenced on a NextSeq 550 platform (Illumina) using a NextSeq 500/550 High Output Kit v2.5 (Illumina) for 75 cycles. A negative and positive control was set for each sequencing run. The raw data were analyzed on PACEseq (Hugobiotech, Beijing). The human DNA was filtered out after alignment to the human reference database (hg38). ④ Microbial Genome Databases (ftp://ftp.ncbi.nlm.nih.gov/genomes/) were downloaded and used for bacterial identification. ⑤ A positive result was defined according to the guidelines within the report from Chen et al.34
Only when the bacteria determined by NGS were the same as the clinically diagnosed bacteria was the NGS result finally considered to be positive and correct.
Statistical Analysis
Statistical analyses were performed using SPSS 19.0 statistical software for Windows (IBM, Armonk, NY) and Excel 2016 for Windows (Microsoft Corporation, Seattle, WA). Continuous variables are expressed as the mean ± standard deviation, and categorical variables are expressed as frequencies. Sensitivity, specificity, accuracy, Youden’s index, positive predictive value and negative predictive value were calculated to indicate the diagnostic value of the different bacteriological detection methods. Chi-square tests and McNemar tests were used to identify the differences in these parameters between the groups. A P value less than 0.05 was considered to be significant.
Results
General Characteristics of the Patients
A total of 28 patients with surgical site infections were identified. The mean time period from surgery to the identification of infection was 8.46±1.84 days (5 days to 11 days). All patients underwent continuous incision drainage.
No differences were found regarding the clinical characteristics of the patients in the infection group and the control group (Table 1). The C-reactive protein concentration (43.62±6.54 vs 30.35±8.74, P<0.001) and erythrocyte sedimentation rate (51.57±17.91 vs 40.03±18.77, P=0.017) were obviously higher in the infection group than in the control group. However, the procalcitonin concentration showed no difference between the two groups. Intraoperative NGS suggested positive results in all infected patients, which indicated that the correct bacteria were identified. Similarly, in 25/28 patients, the infectious bacteria were also correctly detected by intraoperative bacterial culture. The predominant infectious bacteria identified in this study were gram-positive bacteria (23/28), including Staphylococcus in 12 patients, Streptococcus in 5 patients and Enterococcus in 6 patients. Gram-negative bacteria were identified in the other 5 patients, including Escherichia in 2 patients, Pseudomonas aeruginosa in 2 patients and Salmonella in one patient. The characteristics of the infections are shown in Table 2.
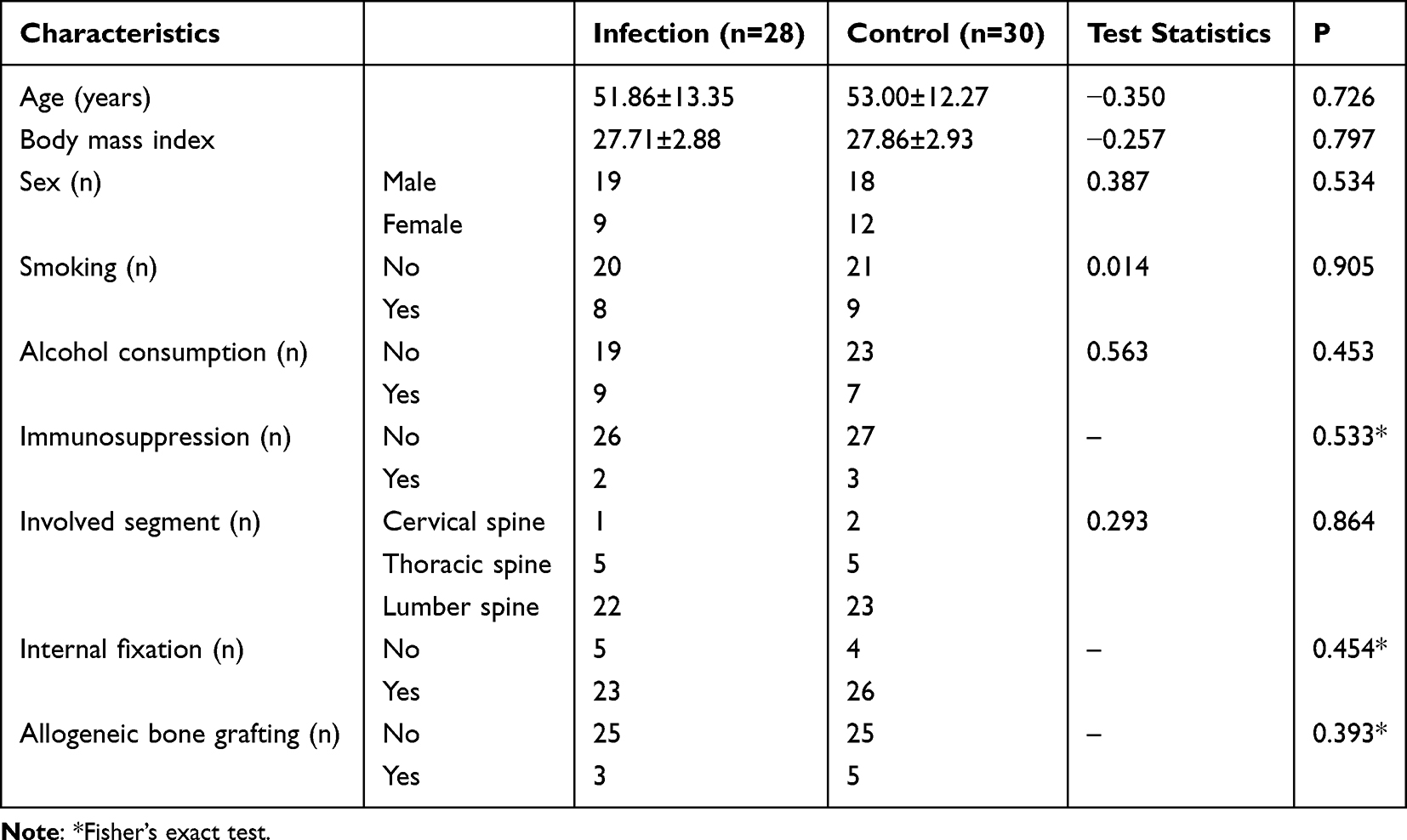 |
Table 1 Clinical Features of Patients Undergoing Spinal Surgery for Degenerative Diseases via the Posterior Approach |
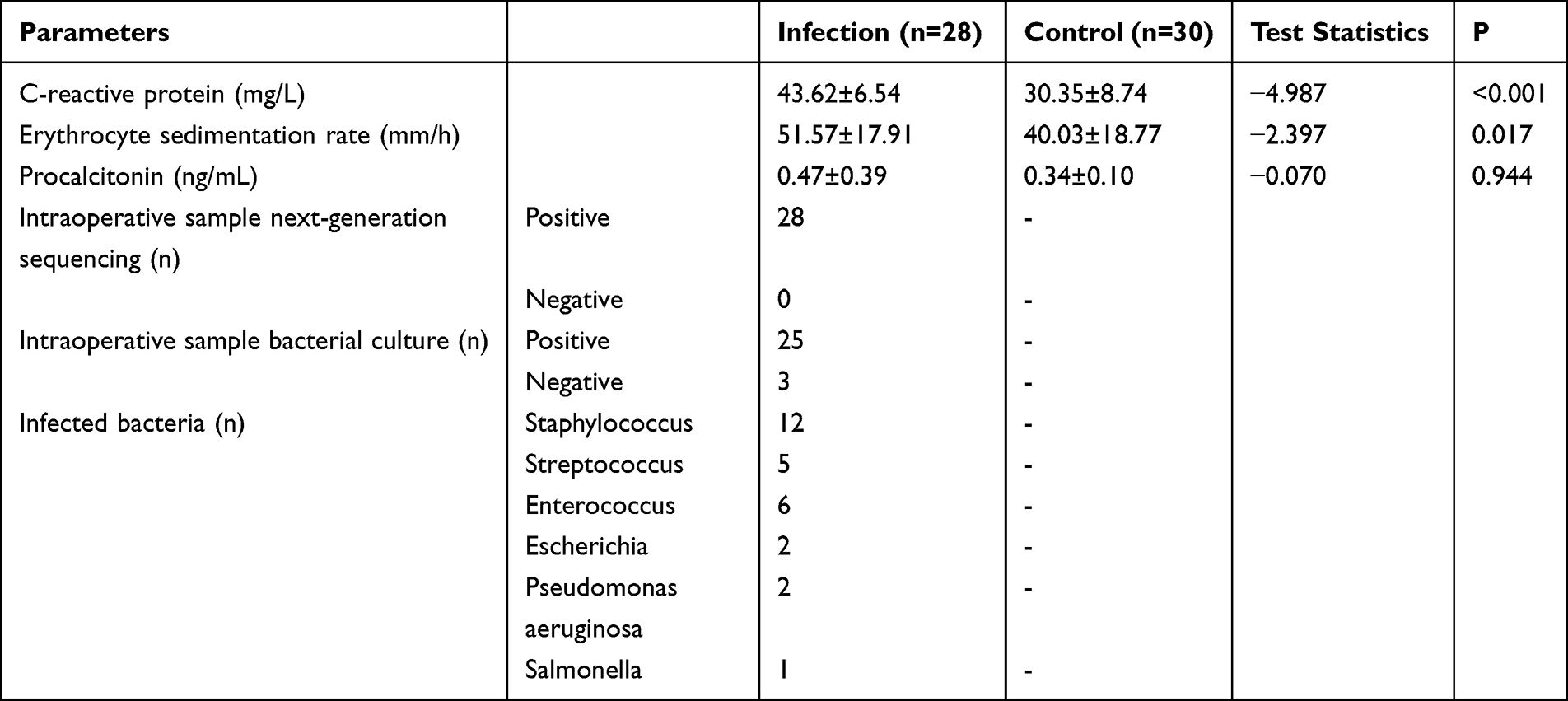 |
Table 2 Infection Features of Patients Undergoing Spinal Surgery for Degenerative Diseases via the Posterior Approach |
Results of Next-Generation Sequencing and Bacterial Culture
Regarding the blood sample tests (Table 3), 23/28 infected patients showed positive results by blood NGS, which indicates that the correct bacteria could be identified from the blood samples. The other 5/28 infected patients showed negative results by blood NGS. However, only 7/28 infected patients showed positive blood bacterial culture results. In the control group, all patients showed negative blood NGS results and negative blood culture results except one patient with a false positive NGS result and one other patient with a false positive blood culture result.
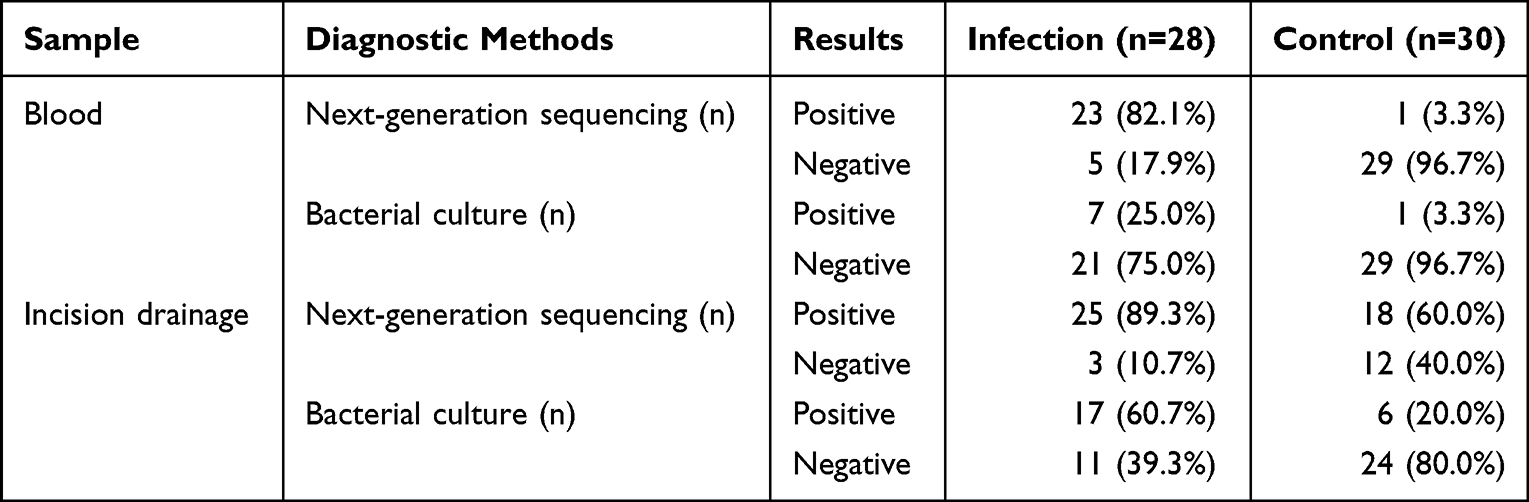 |
Table 3 Results of Next-Generation Sequencing and Bacterial Culture in Patients Undergoing Spinal Surgery for Degenerative Diseases via a Posterior Approach |
Regarding the incision drainage sample tests (Table 3), up to 25/28 infected patients showed positive NGS results. Another 3/28 infected patients showed negative NGS results. A total of 17/28 infected patients showed positive incision drainage bacterial culture results. In the control group, 18/30 patients showed false-positive NGS results. In contrast, only 6/30 patients showed false positive results by incision drainage bacterial culture.
To prevent duplication, these results were not statistically compared since the following diagnostic value parameters (sensitivity, specificity, etc.) were calculated based on these results, which were statistically compared.
Diagnostic Value of Blood Next-Generation Sequencing
The comparison of the diagnostic values between the results of NGS and bacterial culture assessments of both blood samples and drainage fluid samples is summarized in Table 4.
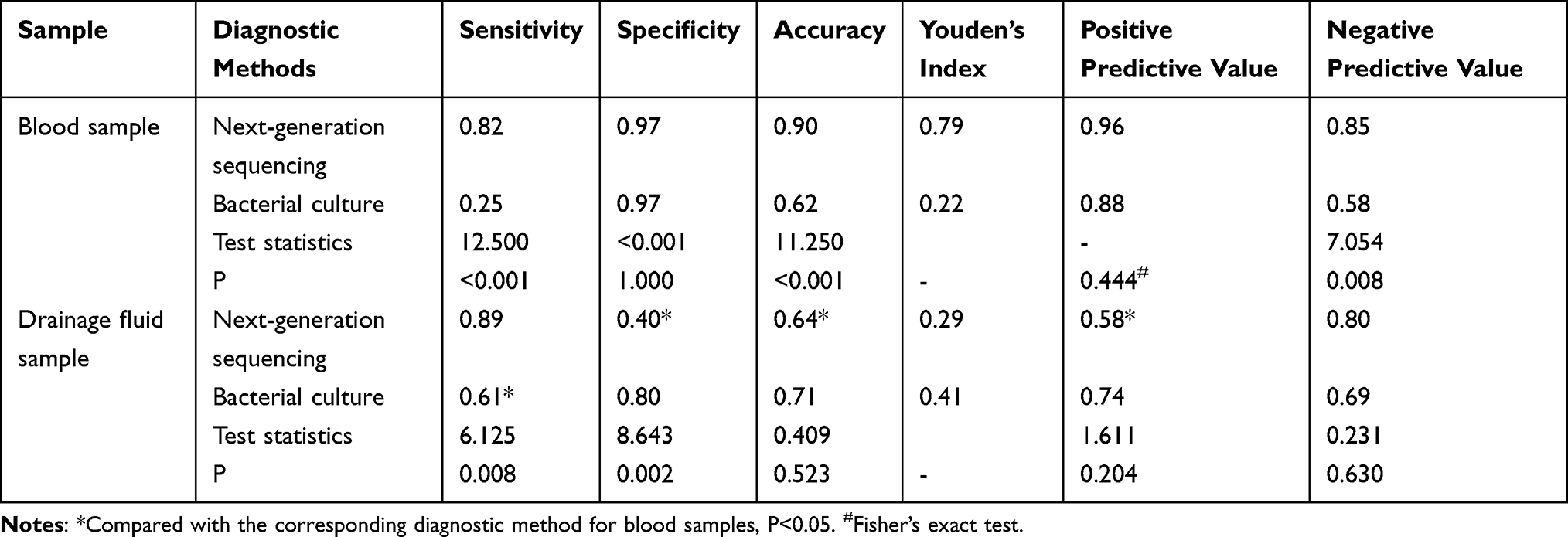 |
Table 4 Infection Diagnostic Value of Blood Next-Generation Sequencing in Patients Undergoing Spinal Surgery for Degenerative Diseases via a Posterior Approach and Who Suffered from Surgical Site Infection |
Except for the sensitivity, all the diagnostic value parameters obtained using blood NGS (including specificity, accuracy, Youden’s index, positive predictive value and negative predictive value) were equal to or higher than those of any other diagnostic methods. Generally, NGS of both blood samples and drainage fluid samples was sensitive for infection identification (sensitivity: 0.82 and 0.89). However, the specificity (0.97 vs 0.40, P<0.05) and positive predictive value (0.96 vs 0.58, P<0.05) of blood NGS were significantly higher than those of drainage fluid NGS. The accuracy (0.90 vs 0.64, P<0.05) and Youden’s index (0.79 vs 0.29) also differed.
The sensitivities of bacterial culture were lower than those of NGS (blood sample: 0.82 vs 0.25, P<0.001; drainage fluid sample: 0.89 vs 0.61, P<0.001), regardless of the kind of sample. However, the specificities of bacterial culture were equal to or higher than those of NGS (blood sample: 0.97 vs 0.97, P=1.000; drainage fluid sample: 0.40 vs 0.80, P=0.002). In short, the bacterial culture was relatively specific for the identification of infection in this study, but it was not sensitive.
Discussion
As hypothesized, the results demonstrated that NGS of blood samples was both sensitive and specific for the identification of infection in patients undergoing spine surgery. In addition to determining whether the infection occurred, the assessment of blood NGS could also help in determining the accurate species and genus of the infectious bacteria, since the results obtained using NGS were the same as those obtained during the clinical diagnosis of the infectious bacteria. Considering that peripheral blood is convenient to obtain and blood samples are not vulnerable to bacterial contamination,36 blood NGS could be recommended when infection is suspected to occur in such a patient undergoing spinal surgery. Moreover, although metastatic abscesses following surgical site infection are rarely observed,37 the results of this study still suggested that the bacteria could enter the bloodstream, which may be more serious than previously estimated. A previous study demonstrated that the rate of positivity in blood culture might be relatively low in patients with surgical site infections following spine surgery.38–40
Although blood NGS is rarely used in the determination of orthopedic infections, it has already been widely used in other fields. For instance, Zhou et al26 reported that multiorgan sepsis, including lumbar spine sepsis caused by Klebsiella pneumoniae, could be diagnosed by blood NGS. Haston et al41 found that the pathogens underlying encephalitis in children could be identified by NGS from plasma. Chen et al25 reported that blood NGS could be used in the determination of the pathogens in pneumonia patients. Geng et al42 also suggested that in critical patients, NGS could help identify pathogens in the blood. Consistent with the results of those previous studies, the results of this study demonstrated that in patients with orthopedic infections, especially the patients in this study who had undergone spinal surgery for degenerative diseases via the posterior approach, the bacteria could be correctly determined by blood NGS. In order to increase the sensitivity of blood NGS, it is necessary to prevent the interference of human DNA.43 Therefore, in this study, the blood was first centrifuged, and the cellular components were subsequently removed.44 This might be a reason why the sensitivity of blood NGS was higher than that observed in some similar studies.26,44 Moreover, in this study, a control group including noninfected patients was set, which could help in accurately determining the specificity of NGS for the diagnosis of infection. In some other studies, due to the lack of a noninfected control group, the specificity might be overestimated.16,19,36 In this study, the results demonstrated that the specificity for the identification of infection using drainage fluid NGS was relatively low, which might be a result of bacterial contamination from the skin surface.45
The diagnostic values of four different diagnostic methods were compared in this study (Table 4). Drainage fluid NGS and blood NGS had the highest sensitivities among the methods. However, false positive results are commonly identified in drainage fluid NGS. Consequently, the specificity of drainage fluid NGS was the lowest among those of all the diagnostic methods, as was the positive predictive value. This result suggested that for definitively infected patients, drainage fluid NGS could be used to correctly identify infectious bacteria. However, some noninfected patients might be misdiagnosed as infected patients by drainage fluid NGS assessment. Because the blood was sterile in the noninfected patients,25,38,42 blood NGS could be used to accurately distinguish the infected patients from the noninfected patients in this study. Blood culture was also performed in this study. Despite a low sensitivity, the positive predictive value of blood culture was relatively high. Therefore, for a patient who had a positive blood culture result, he or she was very likely to be infected. Moreover, the results of this study also suggested that the comprehensive diagnostic value of traditional drainage fluid samples was still acceptable, with moderate sensitivity, specificity, accuracy, positive predictive value and negative predictive value. Therefore, if blood NGS cannot be performed in a patient, traditional bacterial culture of incision drainage fluid could be considered an alternative diagnostic method.
There were several limitations of this study. Here, the major two are listed. First, only infected patients who had undergone debridement surgery were included in this study. Although intraoperative samples could be used to accurately confirm the infection status of these patients, some patients with mild or moderate surgical site infections (cured by only antibiotics and the changing of dressing to maintain fresh dressings for wounds) might be excluded. In these patients with “mild or moderate infection”, the diagnostic value of NGS, especially when performed in blood samples, might be different from that obtained from those patients who had to undergo debridement surgery. However, this study ignored this difference. Patients with “mild or moderate infection” were ultimately excluded, which ensured that all patients included in the study were definitely infected. Second, for the patients in the control group, the time point of sample collection might be different from that chosen for the patients in the infection group. This approach might affect the estimation of the diagnostic values between the different methods. In reality, however, it is impossible to determine which patients would be infected before the infection occurs. Therefore, except for these volunteers, these diagnostic methods for identifying infection were performed only if the surgeons suspected that the patient was infected. This approach might also increase the possibility of misestimating the diagnostic value. Finally, the sample size of this study is limited. Therefore, the comparisons of false positives might not be accurate because of the limited sample size. A large prospective study is urgently needed to assess the practical use of NSG in infection diagnosis and management. In addition, diagnosing infection relying only on blood NSG can be challenged by sample contamination. The infection should be established based on both clinical manifestations and bacteriological exams.
Conclusions
For patients undergoing spinal surgery for degenerative diseases via a posterior approach with surgical site infection, the current study confirmed that in most circumstances, the infectious bacteria could be correctly identified by blood NGS. Blood NGS could also be used to correctly identify noninfected individuals with a performance better than that obtained from NGS performed in drainage fluid. Therefore, as blood can be collected using a minimally invasive sample acquisition method, blood samples should be recommended for NGS in patients undergoing spinal surgery for degenerative diseases via a posterior approach who are suspected to suffer from a surgical site infection.
Abbreviations
NGS, next-generation sequencing; DNA, deoxyribonucleic acid.
Data Sharing Statement
The data associated with this study are retained at a central repository at the Department of Spine Surgery, the 3rd Hospital of Hebei Medical University. If there are any questions, please contact the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of the Third Hospital of Hebei Medical University and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all individuals before they participated in the study.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Funding
There is no funding to report.
Disclosure
All the authors declare that they have no competing interests.
References
1. Elsarrag M, Soldozy S, Patel P, et al. Enhanced recovery after spine surgery: a systematic review. Neurosurg Focus. 2019;46(4):E3. doi:10.3171/2019.1.FOCUS18700
2. Arif S, Brady Z, Enchev Y, Peev N. Is fusion the most suitable treatment option for recurrent lumbar disc herniation? A systematic review. Neurol Res. 2020;42(12):1034–1042. doi:10.1080/01616412.2020.1787661
3. Castillo H, Chintapalli RTV, Boyajian HH, et al. Lumbar discectomy is associated with higher rates of lumbar fusion. Spine J. 2019;19(3):487–492. doi:10.1016/j.spinee.2018.05.016
4. Dower A, Chatterji R, Swart A, Winder MJ. Surgical management of recurrent lumbar disc herniation and the role of fusion. J Clin Neurosci. 2016;23:44–50. doi:10.1016/j.jocn.2015.04.024
5. Aleem IS, Tan LA, Nassr A, Riew KD. Surgical site infection prevention following spine surgery. Global Spine J. 2020;10(1 Suppl):92s–98s. doi:10.1177/2192568219844228
6. Nasser R, Kosty JA, Shah S, Wang J, Cheng J. Risk factors and prevention of surgical site infections following spinal procedures. Global Spine J. 2018;8(4 Suppl):44s–48s. doi:10.1177/2192568218806275
7. Anderson PA, Savage JW, Vaccaro AR, et al. Prevention of surgical site infection in spine surgery. Neurosurgery. 2017;80(3s):S114–s123. doi:10.1093/neuros/nyw066
8. Ojo OA, Owolabi BS, Oseni AW, Kanu OO, Bankole OB. Surgical site infection in posterior spine surgery. Niger J Clin Pract. 2016;19(6):821–826. doi:10.4103/1119-3077.183237
9. Esteban J, Alonso-Rodriguez N, del-Prado G, et al. PCR-hybridization after sonication improves diagnosis of implant-related infection. Acta Orthop. 2012;83(3):299–304. doi:10.3109/17453674.2012.693019
10. Liu L, Luo L, Zhao C, Zhou Q. Postoperative management strategy of surgical site infection following lumbar dynesys dynamic internal fixation. Pain Res Manag. 2021;2021:2262837. doi:10.1155/2021/2262837
11. Behera HS, Chayani N, Bal M, et al. Identification of population of bacteria from culture negative surgical site infection patients using molecular tool. BMC Surg. 2021;21(1):28. doi:10.1186/s12893-020-01016-y
12. Deng H, Chan AK, Ammanuel S, et al. Risk factors for deep surgical site infection following thoracolumbar spinal surgery. J Neurosurg Spine. 2019;32(2):292–301. doi:10.3171/2019.8.SPINE19479
13. Yao R, Tan T, Tee JW, Street J. Prophylaxis of surgical site infection in adult spine surgery: a systematic review. J Clin Neurosci. 2018;52:5–25. doi:10.1016/j.jocn.2018.03.023
14. Yin H, Xu D, Wang D. Diagnostic value of next-generation sequencing to detect periprosthetic joint infection. BMC Musculoskelet Disord. 2021;22(1):252. doi:10.1186/s12891-021-04116-9
15. Ringeval N, Decrucq F, Weyrich P, et al. Diagnostic performance of suction drainage fluid culture for acute surgical site infection after aseptic instrumented spine surgery: a retrospective analysis of 363 cases. Eur J Orthop Surg Traumatol. 2021;31(1):155–160. doi:10.1007/s00590-020-02755-7
16. Slatko BE, Gardner AF, Ausubel FM. Overview of Next-Generation Sequencing Technologies. Curr Protoc Mol Biol. 2018;122(1):e59. doi:10.1002/cpmb.59
17. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
18. Yohe S, Thyagarajan B. Review of clinical next-generation sequencing. Arch Pathol Lab Med. 2017;141(11):1544–1557. doi:10.5858/arpa.2016-0501-RA
19. Mitchell SL, Simner PJ. Next-generation sequencing in clinical microbiology: are we there yet? Clin Lab Med. 2019;39(3):405–418. doi:10.1016/j.cll.2019.05.003
20. Castellà L, Sopena N, Rodriguez-Montserrat D, et al. Intervention to reduce the incidence of surgical site infection in spine surgery. Am J Infect Control. 2020;48(5):550–554. doi:10.1016/j.ajic.2019.09.007
21. Goldberg L. Developing a surgical site infection prevention bundle for patients undergoing elective spine surgery. Aorn j. 2020;112(2):158–164. doi:10.1002/aorn.13130
22. Ballester LY, Luthra R, Kanagal-Shamanna R, Singh RR. Advances in clinical next-generation sequencing: target enrichment and sequencing technologies. Expert Rev Mol Diagn. 2016;16(3):357–372. doi:10.1586/14737159.2016.1133298
23. Lasry O, Ailon T, Charest-Morin R, et al. Accuracy of hospital-based surveillance systems for surgical site infection after adult spine surgery: a Bayesian latent class analysis. J Hosp Infect. 2021;117:117–123. doi:10.1016/j.jhin.2021.07.005
24. Snopko P, Kolarovszki B, Opšenák R, Hanko M, Richterová R. Surgical site infections after degenerative lumbar spine surgery. Rozhl Chir. 2018;97(12):539–545.
25. Chen X, Ding S, Lei C, et al. Blood and bronchoalveolar lavage fluid metagenomic next-generation sequencing in pneumonia. Can J Infect Dis Med Microbiol. 2020;2020:6839103. doi:10.1155/2020/6839103
26. Zhou S, Ren G, Liu Y, et al. Challenge of evolving Klebsiella pneumoniae infection in patients on hemodialysis: from the classic strain to the carbapenem-resistant hypervirulent one. Int J Med Sci. 2022;19(3):416–424. doi:10.7150/ijms.69577
27. Hui P. Next generation sequencing: chemistry, technology and applications. Top Curr Chem. 2014;336:1–18. doi:10.1007/128_2012_329
28. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital infection control practices advisory committee. Infect Control Hosp Epidemiol. 1999;20(4):250–278; quiz 279–280. doi:10.1086/501620
29. O’Hara LM, Thom KA, Preas MA. Update to the Centers for Disease Control and Prevention and the Healthcare Infection Control Practices Advisory Committee Guideline for the Prevention of Surgical Site Infection (2017): a summary, review, and strategies for implementation. Am J Infect Control. 2018;46(6):602–609. doi:10.1016/j.ajic.2018.01.018
30. Ban KA, Minei JP, Laronga C, et al. American college of surgeons and surgical infection society: surgical site infection guidelines, 2016 update. J Am Coll Surg. 2017;224(1):59–74. doi:10.1016/j.jamcollsurg.2016.10.029
31. Mueller K, Zhao D, Johnson O, Sandhu FA, Voyadzis JM. The difference in surgical site infection rates between open and minimally invasive spine surgery for degenerative lumbar pathology: a retrospective single center experience of 1442 cases. Oper Neurosurg. 2019;16(6):750–755. doi:10.1093/ons/opy221
32. Gorensek M, Kosak R, Travnik L, Vengust R. Posterior instrumentation, anterior column reconstruction with single posterior approach for treatment of pyogenic osteomyelitis of thoracic and lumbar spine. Eur Spine J. 2013;22(3):633–641. doi:10.1007/s00586-012-2487-5
33. Zhang B, Li M, Liu Y, et al. The diagnostic value of blood sample NGS in patients with early periprosthetic joint infection after total Hip arthroplasty. Int Wound J. 2022. doi:10.1111/iwj.13943
34. Chen H, Zhang Y, Zheng J, et al. Application of mNGS in the etiological diagnosis of thoracic and abdominal infection in patients with end-stage liver disease. Front Cell Infect Microbiol. 2021;11:741220. doi:10.3389/fcimb.2021.741220
35. Podnar J, Deiderick H, Hunicke-Smith S. Next-generation sequencing fragment library construction. Curr Protoc Mol Biol. 2014;107:7.17.11–16. doi:10.1002/0471142727.mb0717s107
36. Aly SM, Sabri DM. Next generation sequencing (NGS): a golden tool in forensic toolkit. Arch Med Sadowej Kryminol. 2015;65(4):260–271. doi:10.5114/amsik.2015.61029
37. Norman G, Atkinson RA, Smith TA, et al. Intracavity lavage and wound irrigation for prevention of surgical site infection. Cochrane Database Syst Rev. 2017;10(10):Cd012234.
38. Halavaara M, Jääskeläinen IH, Hagberg L, Järvinen A. Factors associated with blood culture positivity in patients with complicated skin and skin structure infection-a population-based study. Eur J Clin Microbiol Infect Dis. 2019;38(7):1351–1357. doi:10.1007/s10096-019-03560-9
39. Abdul-Jabbar A, Takemoto S, Weber MH, et al. Surgical site infection in spinal surgery: description of surgical and patient-based risk factors for postoperative infection using administrative claims data. Spine. 2012;37(15):1340–1345. doi:10.1097/BRS.0b013e318246a53a
40. Litrico S, Recanati G, Gennari A, Maillot C, Saffarini M, Le Huec JC. Single-use instrumentation in posterior lumbar fusion could decrease incidence of surgical site infection: a prospective bi-centric study. Eur J Orthop Surg Traumatol. 2016;26(1):21–26. doi:10.1007/s00590-015-1692-4
41. Haston JC, Rostad CA, Jerris RC, et al. Prospective cohort study of next-generation sequencing as a diagnostic modality for unexplained encephalitis in children. J Pediatric Infect Dis Soc. 2020;9(3):326–333. doi:10.1093/jpids/piz032
42. Geng S, Mei Q, Zhu C, et al. Metagenomic next-generation sequencing technology for detection of pathogens in blood of critically ill patients. Int J Infect Dis. 2021;103:81–87. doi:10.1016/j.ijid.2020.11.166
43. Hogan CA, Yang S, Garner OB, et al. Clinical impact of metagenomic next-generation sequencing of plasma cell-free DNA for the diagnosis of infectious diseases: a multicenter retrospective cohort study. Clin Infect Dis. 2021;72(2):239–245. doi:10.1093/cid/ciaa035
44. Tilley L, Grimsley S. Is next generation sequencing the future of blood group testing? Transfus Apher Sci. 2014;50(2):183–188. doi:10.1016/j.transci.2014.02.013
45. Byrd AL, Belkaid Y, Segre JA. The human skin microbiome. Nat Rev Microbiol. 2018;16(3):143–155. doi:10.1038/nrmicro.2017.157
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.