")
Back to Journals » Vascular Health and Risk Management » Volume 19
The Diagnostic Utility of Natural Killer Cell Subsets in Deep Vein Thrombosis
Authors Alhabibi AM , Wahab MA , Sakr AK, Abd El-Hamid SM , Zakaria MY , Althoqapy AA, El Sayed HME , Kasim SA , Ibrahim HF, Saleh OI, Ahmed HA , Sayed AH, Lotfy M
Received 16 August 2023
Accepted for publication 16 November 2023
Published 23 November 2023 Volume 2023:19 Pages 779—787
DOI https://doi.org/10.2147/VHRM.S430466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Alshaymaa M Alhabibi,1 Maisa A Wahab,2 Ahmed Khairy Sakr,2 Samar M Abd El-Hamid,1 Mohamed Yahia Zakaria,3 Azza Ali Althoqapy,4 Hanaa Mohammed Eid El Sayed,5 Sammar Ahmed Kasim,5 Hanan F Ibrahim,4 Ola I Saleh,6 Howida A Ahmed,6 Alaa H Sayed,7 Mahmoud Lotfy8
1Department of Clinical Pathology, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 2Department of Vascular Surgery, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 3Department of Vascular and EndoVascular Surgery, Faculty of Medicine for Boys, Al-Azhar University, Cairo, Egypt; 4Medical Microbiology and Immunology Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 5Internal Medicine Department, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 6Department of Radio-Diagnosis, Faculty of Medicine for Girls, Al-Azhar University, Cairo, Egypt; 7Hormones Department, Medical Research and Clinical Studies Institute, National Research Centre, Giza, Egypt; 8Molecular Biology Department, Genetic Engineering & Biotechnology Research Institute, University of Sadat City, Sadat City, Minufiya, Egypt
Correspondence: Alshaymaa M Alhabibi, Tel +201002894075, Email [email protected]
Background: Natural killer (NK) cells are important components of adaptive and innate immune responses. NK cell subsets have different functions and may play a role in vascular disorders. This study aimed to evaluate the proportions of NK cells and their subsets to determine whether they can be used as markers of venous thrombosis and to identify whether there was a link between NK cell proportion and citrullinated histone (H3) levels.
Patients and Methods: This study included 100 participants divided into Group I (n=50, patients with deep venous thrombosis (DVT)) and Group II (n=50, age- and sex-matched healthy controls). Group I was further categorized into Group Ia (n=25, patients with acute DVT) and Group Ib (n=25, patients with chronic DVT). The proportions of NK cells and their subsets were evaluated by flow cytometry using CD3/CD16/CD56. The levels of citrullinated histones (H3) were estimated using enzyme-linked immunosorbent assay (ELISA).
Results: Compared to the control group, DVT patients had a significantly lower proportion of (CD56 dim/CD16+) NK cells, a significantly higher proportion of (CD56-/CD16+) NK cells and a high level of citrullinated histone (H3).
Conclusion: NK cell subsets and citrullinated histone (H3) could be used as markers for DVT and as targets for therapeutic drugs to inhibit the formation or progression of thrombosis.
Keywords: natural killer cell, natural killer cell subsets, citrullinated histone, deep venous thrombosis
Introduction
Venous thromboembolism (VTE) is the third most common cardiovascular disease affecting approximately 2% of the population. VTE is a critical condition that may result as a complication of many diseases such as cancer, major trauma, surgery, and systemic diseases. Therefore, VTE is considered an economic health problem worldwide.1–3
An important mechanism in the pathogenesis of VTE is the formation of neutrophil extracellular traps (NETs), which increase the risk of VTE threefold. NETs are composed of circulating nucleosomes and neutrophil granule proteins released in a net-like manner.4
Neutrophil extracellular traps are considered prothrombotic factors because they can activate both intrinsic and extrinsic pathways of the coagulation cascade. They initiate the activation of the intrinsic pathway by activating factor XII via its polyanionic surface. They activate the extrinsic pathway by binding to tissue factor.5,6
In addition, histones involved in NETs formation stimulate thrombin generation by platelets and promote the secretion of von Willebrand factor from endothelial cells, facilitating the adhesion of leukocytes and platelets.7
Although the mechanisms underlying NET release have been described, the triggers for their formation in VTE are not well understood. Previous studies have shown that interferon-γ (IFN-γ) stimulates NET formation. IFN-γ is a proinflammatory cytokine, which has a major role in VTE pathogenesis. IFN-γ stimulates NET formation in vivo and in vitro.8
One of the innate immune responses is that of natural killer cells (NK), which are a source of cytokines and chemokines that influence adaptive immune responses. NK cells are among the major IFN-γ producers; thus, they are major participants in NET formation.9,10
Animal models have shown that the depletion of NK cells leads to a reduction in NET formation within thrombi. This consequently proves that NK cells promote venous thrombosis through IFN-γ-dependent NET formation.11
The objective of this study was to correlate the proportions of NK cells and NK cell subsets with citrullinated histone H3 as a NET indicator in patients with deep vein thrombosis (DVT), as this may provide more details on the triggers of NET formation and provide a solution to decrease the risk of thrombosis.
Patients and Methods
Selection of Participants
A case-control study was conducted on 100 individuals at Al-Zahraa University Hospital who were divided into Group I (n=50, patients diagnosed with DVT) and Group II (n=50, apparently healthy individuals serving as controls). Group I was further subdivided into Groups Ia (n=25, acute DVT) and Ib (n=25, chronic DVT).
Calculation of Sample Size
Since there have been no previous studies on the association between the percentage of NK cell subsets and DVT published to our knowledge, we carried out a pilot study on 30 individuals (15 DVT patients and 15 controls) to determine the sample size. Data from the pilot study showed that the minimum sample size needed was 40 participants in each group, with the power set at 80% and α error at 0.05. The final sample size was 50 DVT patients and 50 healthy controls.
Inclusion Criteria
Patients were selected and diagnosed with DVT according to the reported criteria.12 The patients were divided into acute and chronic DVT groups based on history, duration of the insult, and physical examination. Diagnosis of DVT type and discrimination between DVT and other diseases with the same symptoms were confirmed by radiological examination using venous duplex ultrasonography.
Exclusion Criteria
Patients with congenital thrombophilia, antiphospholipid syndrome, superficial thrombophlebitis, malignancy, menopausal replacement therapy, or estrogen hormone contraceptive pills were excluded from the study. Patients with vein thrombosis at any site other than the lower limbs were also excluded.
Ethical Consideration
This study was conducted in accordance with the World Medical Association Helsinki Declaration for Human Subjects. This study was approved by the Institutional Review Board (IRB) of our university (Al-Azhar University Review Board, study code 1136, December 1, 2021), and all participants provided written informed consent.
Assessment and Procedures
Each individual involved was subjected to a full clinical and radiological examination as well as the following investigations:
- Routine laboratory investigations including complete blood count (CELL-DYN Ruby, Abbott, USA), coagulation profile (Stago STA, Stago Diagnostica, USA), and D-dimer levels (Cobas 6000, Roche, Germany).
- Estimation of serum levels of human citrullinated histone (H3) by enzyme-linked immunosorbent assay (ELISA) using a Bioassay Technology Laboratory kit (Cat No E7533Hu, Lot No 202205001, Zhejiang, China).
- Estimation of the proportions of NK cells and NK cell subsets using flow cytometry.
Immunophenotyping was conducted using ten-colors Navios Ex (Beckman Coulter, Marseille, France) and Navios software with the following monoclonal antibodies: FITC-conjugated CD3, PE-conjugated CD16, and APC-conjugated CD56 (Immunotech, Beckman Coulter, Marseille, France, Lot No. 200084, 200096, and 200065, respectively).
Titration experiments were performed to determine the optimal concentration of each antibody. The flow cytometry data were determined as the proportion (%) of cells expressing the markers.
Unstained samples were acquired after modifying the sample count (100,000 events) to detect autofluorescence.
Gating of NK cells (Figure 1)
- Lymphocytes were gated using the forward scatter/ side scatter characteristics.
- (CD3-) lymphocytes were gated using CD3 FITC/SSC.
- NK cell subsets were identified by quadrant analysis using CD16 PE/ CD56 APC and categorized as follows:
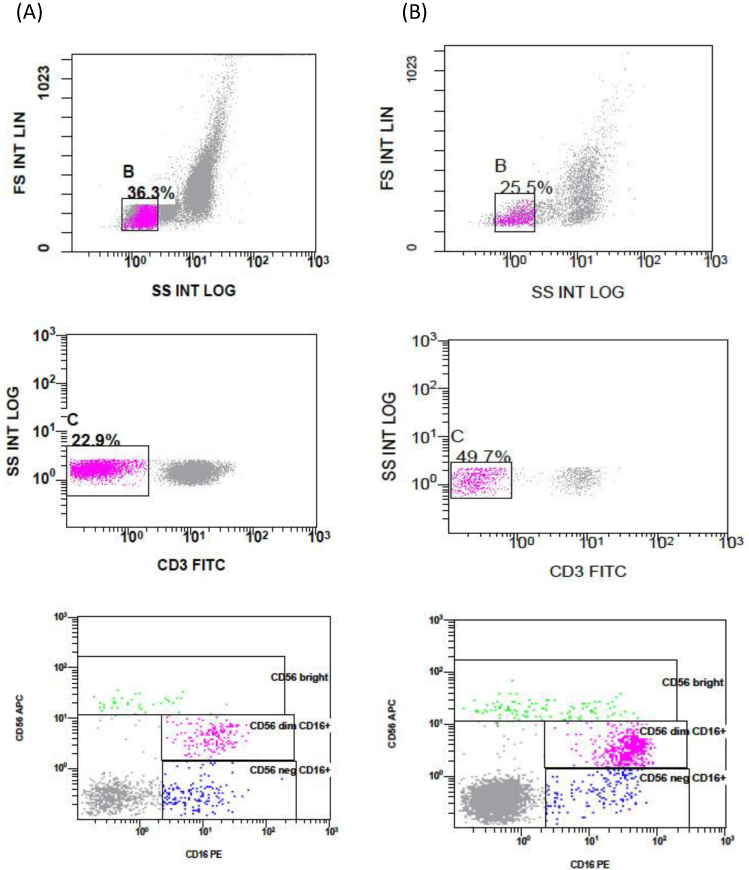 |
Figure 1 Representative dot plots showing gating of lymphocytes using forward scatter/ side scatter characteristics (FSC/SSC), gating of (CD3-) population, and different natural killer (NK) cell subsets. Dot plots showing: (A) a case of DVT, and (B) a sample of healthy control group. |
(Bright CD56) NK cells, (CD56 dim/ CD16+) NK cells and (CD56-/CD16+) NK cells.
Statistical Analysis
Statistical package for social sciences, version 23.0 (SPSS Inc., Chicago, Illinois, USA) was used to analyse the data. Normality tests were conducted using the Kolmogorov–Smirnov and Shapiro–Wilk tests. For normally distributed quantitative data, the mean and standard deviation were used, whereas the median and interquartile range were used to define non-normally distributed variables. Based on the normality of the data, two groups were compared using the independent-samples t-test or Mann–Whitney U-test, and more than two groups were compared using one-way ANOVA or Kruskal–Wallis test.
Receiver operating characteristic (ROC) curve analysis was performed and Youden’s index was used to select the optimal cut-off value for the markers. Spearman´s correlation was used to detect the strength of the association among continuous variables. Statistical significance was set at p <0.05.
Results
This study included 100 individuals categorized into two groups: Group I (n=50): DVT patients (29 men and 21 women) ranging in age from 25 to 68 years with a mean age of 42.9 ± 8.7 years, and Group II (n=50): age- and sex- matched healthy controls (20 men and 30 women) ranging in age from 24 to 62 years with a mean age of 42.2 ± 10.2 years. Group I was further subdivided into: Group Ia (n=25): acute DVT (13 men and 12 women) ranging in age from 25 to 68 years with a mean age of 42.4 ± 9.5 years, and Group Ib (n=25): chronic DVT (16 men and 9 women) ranging in age from 31 to 60 years with a mean age of 43.4 ± 8.1 years.
Results of Laboratory Parameters of the Study Participants (Table 1)
There was a highly significant increase in absolute monocyte count (p<0.001), prothrombin time (p<0.004), international normalization ratio, activated partial thromboplastin time, D-dimer levels, and citrullinated histone (H3) (p< 0.001 for all). Furthermore, Group Ia showed a highly significant increase in both D-dimer and citrullinated histones (H3) compared to Group Ib, and Group Ib compared to the control group (p <0.001).
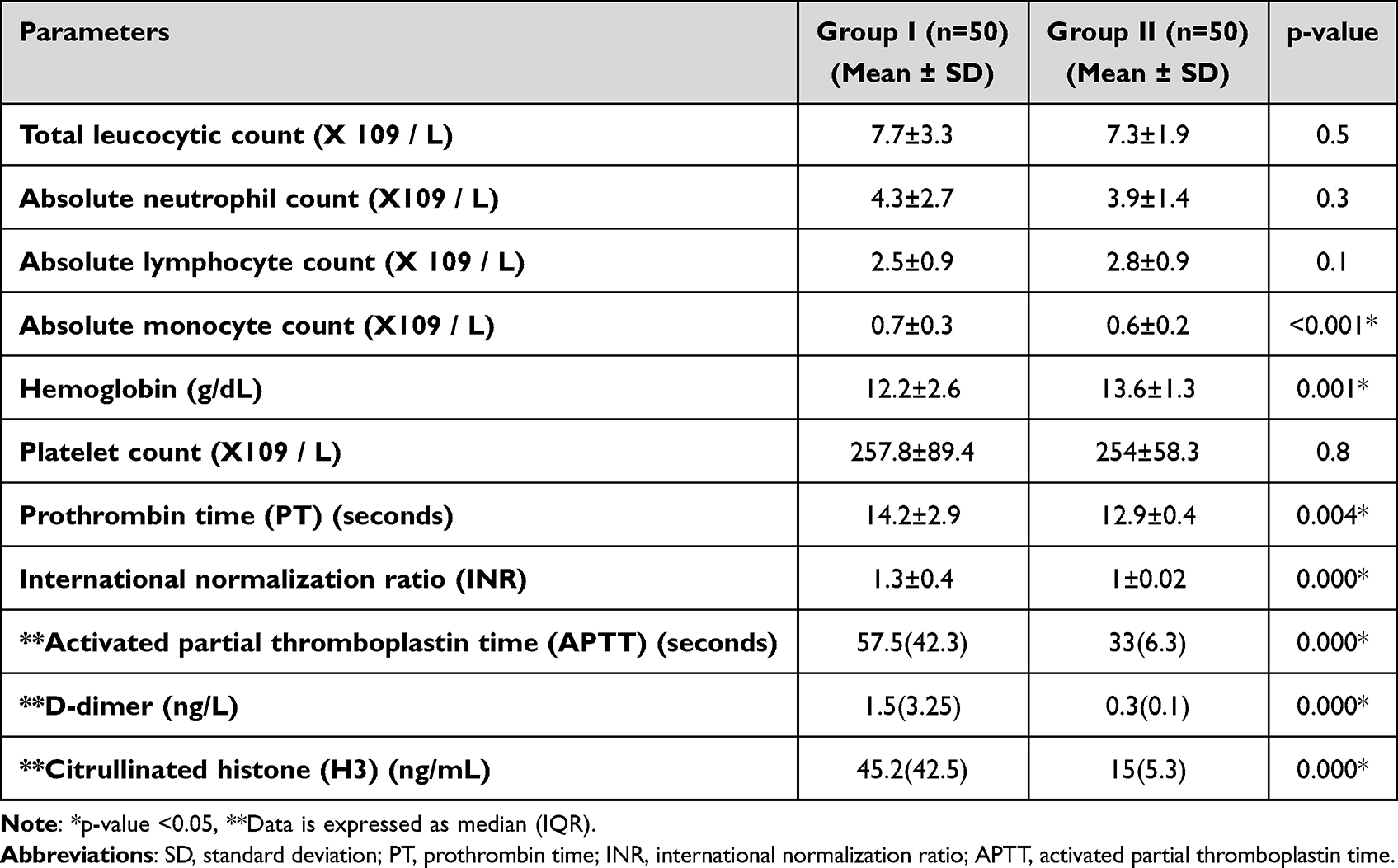 |
Table 1 Results of Different Laboratory Parameters of the Study Participants |
Proportions of NK Cells and NK Cell Subsets Detected by Immunophenotyping (Table 2 and Table 3)
Comparison Between Group I and Group II (Table 2)
There was no significant difference in the proportion of NK cells between Groups I and II. Regarding NK cell subsets, when comparing Groups I and II, there was a highly significant decrease in the proportion of (CD16+/CD56 dim) NK cells (p<0.001) and a highly significant increase in the proportion of (CD16+/CD56-) NK cells (p<0.001). The proportion of (CD56 bright) NK cells did not differ significantly between the two groups.
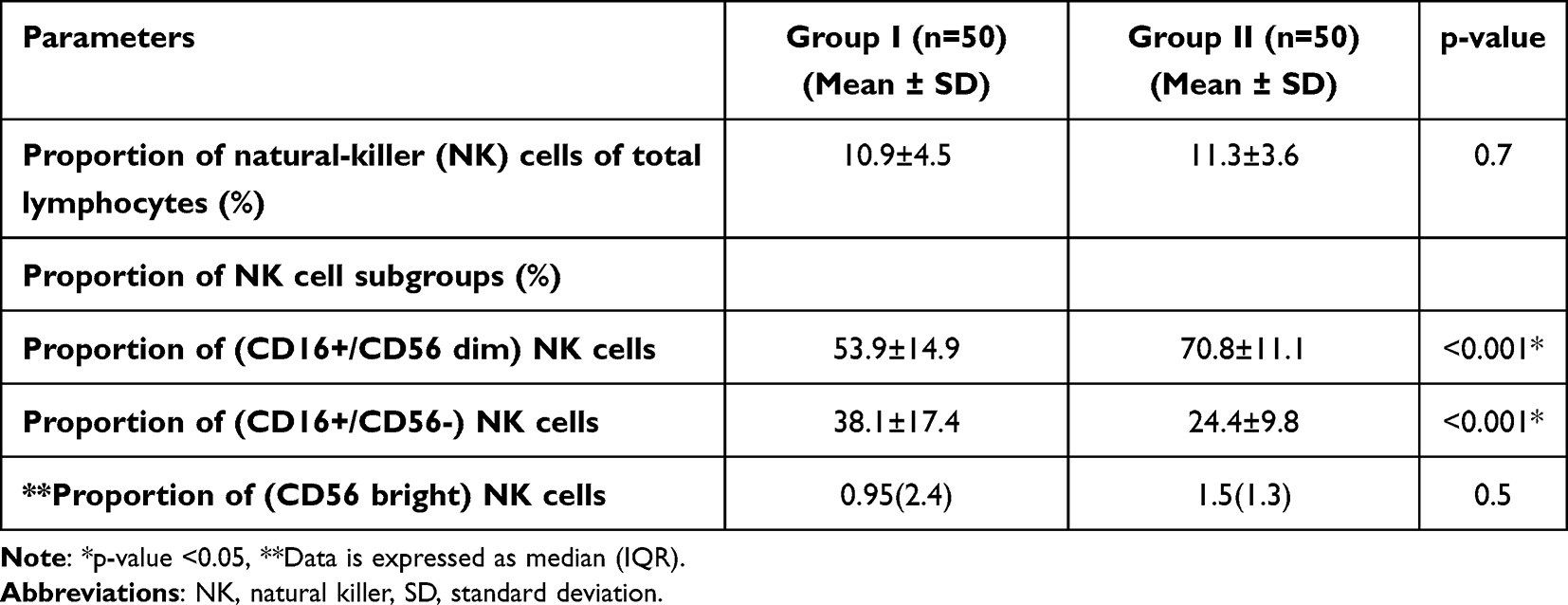 |
Table 2 Proportion of Natural Killer (NK) Cells and NK Cell Subsets of the Study Participants |
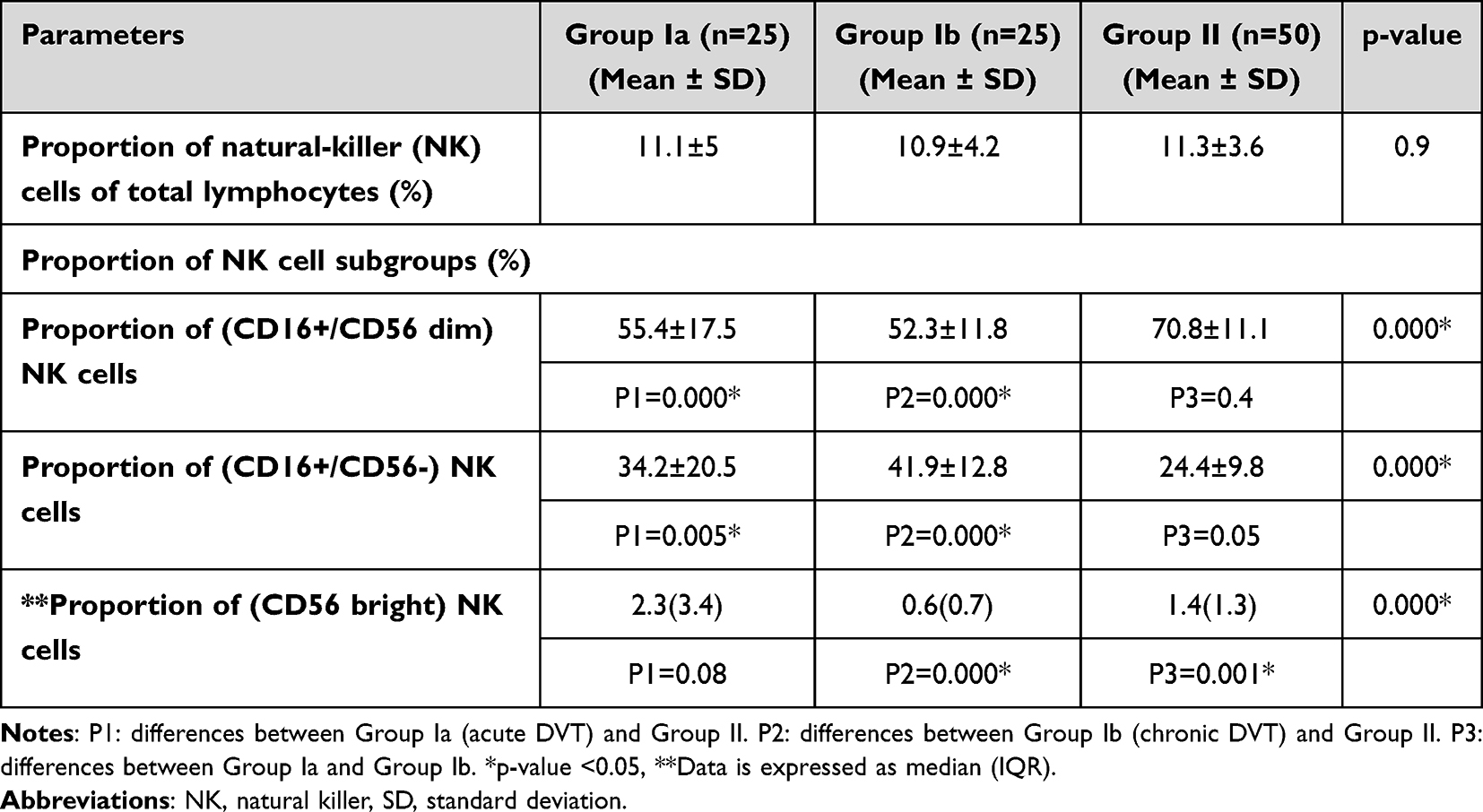 |
Table 3 Comparison Between the Two Subgroups and the Control Group Regarding the Proportion of Natural Killer (NK) Cells and the Proportion of Their Subsets |
Comparison Between Groups Ia, Ib, and II (Table 3)
Both groups Ia and Ib showed a highly significant increase in the proportion of (CD16+/CD56 dim) NK cells and a highly significant reduction in the proportion of (CD16+/CD56-) NK cells (p<0.001) compared to the control group. There was a highly significant increase in the proportion of (CD56 bright) NK cells among all the groups (p<0.001), which was highest in Group Ia followed by Group II and Group Ib.
Correlation Between Citrullinated Histones (H3) and the Proportions of NK Cells of the Total Lymphocytes and NK Cell Subsets (Table 4)
There was no significant correlation between citrullinated histones and any of the proportions of NK cells or NK cell subgroups, except for a significant positive correlation between citrullinated histones (H3) and the proportion of (CD56 bright) NK cells (r = 0.3 and p = 0.02).
 |
Table 4 Correlation Between Citrullinated Histones (H3) and the Natural Killer (NK) Cell Proportion of the Total Lymphocytes and NK Cell Subgroup Proportion |
Results of the ROC Curve to Discriminate the Power of Citrullinated Histone (H3) and NK Cell Subsets for Distinguishing Cases and Controls (Figure 2)
The ROC curve revealed that citrullinated histones (H3), the proportion of (CD16+/CD56 dim) NK cells and the proportion of (CD16+/CD56-) are sensitive and specific markers for distinguishing between DVT cases and controls.
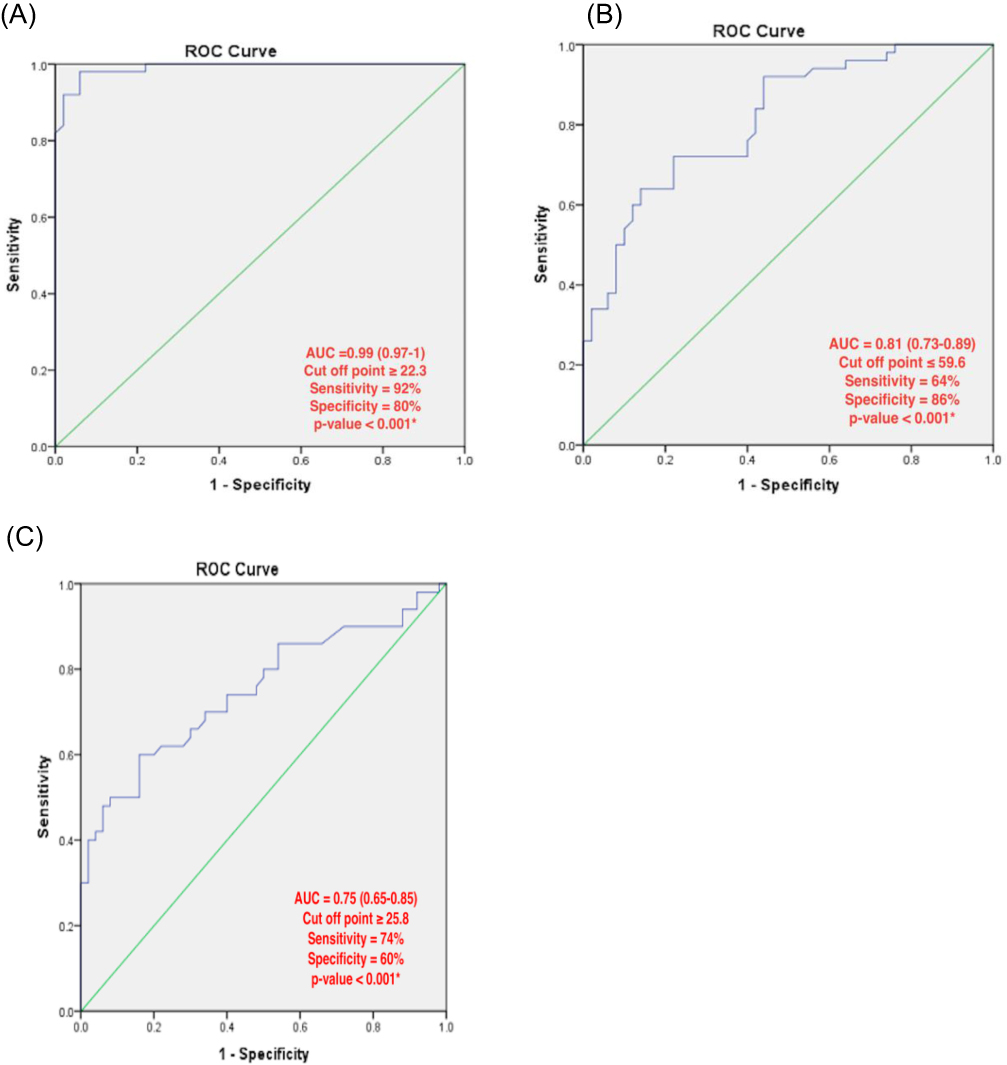 |
Figure 2 The output data of the receiver operating characteristic (ROC) curve to discriminate the power of: (A) citrullinated histone (H3), (B) proportion of (CD16+/CD56 dim) natural killer (NK) cell subset, (C) proportion of (CD16+/CD56-) NK cell subset, to distinguish between cases and controls. |
Discussion
NK cells are an important element of the immune system´s adaptive and innate responses.10 They are defined as (CD3-/ CD56+) cells, as detected by immunophenotyping. Peripheral blood NK cells can be divided into two subsets: (CD56 bright) NK cells (the minor compartment of peripheral blood NK cells with immunomodulatory functions and poor killing ability) and (CD56 dim/CD16+) NK cells (terminally differentiated NK cells, which constitute the major compartment of peripheral blood NK cells that secrete variable cytokines).13–15
A third compartment of NK cells is detected as (CD56-/CD16+) NK cells, which increase during certain pathological conditions, such as autoimmune disorders and viral infections.16
In addition to chemokine secretion, engagement of CD16 is enough to induce IFN-γ and tumor necrosis factor-α secretion. Downregulation of CD56 and acquisition of CD16 are characteristics of NK cell maturation.17
In this study, we aimed to determine the proportion of different NK cell subgroups and the level of citrullinated histone (H3), a marker of NETs, in the peripheral blood of DVT patients as well as to investigate whether there was any relationship between NK cells and NK cell subsets and citrullinated histone (H3).
Our study found no significant difference in the proportion of NK cells in total lymphocytes between patients and the control group or between patients with acute DVT, chronic DVT, and the control group.
Regarding NK cell subtypes, patients with DVT showed a highly significant decrease in the proportion of (CD56 dim/CD16+) NK cells compared to the control group, in addition to acute and chronic cases showing a decrease in the same subset compared to the control group. In contrast, DVT patients showed a highly significant increase in the proportion of (CD56-/CD16+) NK cells compared to the control group, and acute and chronic cases showed an increase in the same subset of NK cells compared to the control group. The ROC curve also demonstrated that the proportions of (CD56 dim/CD16+) and (CD56-/CD16+) NK cells were sensitive and specific markers for discrimination between DVT cases and the control group.
To the best of our knowledge, no study has investigated the proportion of NK cells and NK cell subsets in DVT; however, some studies have investigated other vascular abnormalities such as coronary heart disease and pulmonary embolism.
Our study agrees with that of Hak et al, who discovered that patients with coronary heart disease had lower proportions of (CD3-/CD56 dim) NK cells than the control group, suggesting that there is an impairment of the NK cell compartment in coronary heart disease. In contrast, the proportion of NK cells in the peripheral blood of the studied individuals decreased. This may be attributed to the fact that their study included elderly individuals with a mean age of 63 years and that old age affected the number and function of NK cells.17
The same results were obtained by Duan et al, who reported that the number of (CD56+/CD16+) NK cells decreased in individuals with pulmonary embolism compared to that in the control group, illustrating a strong relationship between vascular thromboembolism and immune dysfunction.18
This agrees with the results of Zheng et al, who showed a decrease in the percentage of (CD56 dim/ CD16+) NK cells in pulmonary embolism. Therefore, they suggested that the impairment of NK cell function plays a significant role in the development of acquired vascular thromboembolism.19
Regarding citrullinated histone (H3), a highly reliable and specific marker for NETs, which are a major contributor to the development of thrombosis,20 there was a highly significant increase in citrullinated histone (H3) in DVT cases compared to the level in the control group that could be used as a specific and sensitive indicator of DVT.
Liu et al, found that citrullinated histone (H3) was increased in patients with DVT (developed after fractures) and concluded that NETs could be used as a diagnostic marker for traumatic DVT.21
This agrees with the results of Mauracher et al, who found an increased concentration of citrullinated histone (H3) was associated with an increased risk of cancer-associated thrombosis, which explains the role of NETs in the pathogenesis of thrombosis.22
According to Bertin et al, NK cells are implicated in the pathogenesis of DVT through the production of NETs, as evidenced by the protection of mice from DVT after the ablation of NK cells. Furthermore, the depletion of NK cells in mice inhibited the release of NETs.11 For this reason, we wondered whether there was any association between the proportions of NK cells and NK cell subsets and the concentration of citrullinated histone (H3) in humans. However, there was no significant association between the level of citrullinated histone (H3) and the proportion of NK cells or NK cell subsets, except for a significant positive correlation with (CD56 bright) NK cells in individuals with DVT. The difference between this study and ours may be attributed to the fact that immune functions might differ significantly between mice and humans, especially NK cell function and regulation. Moreover, the function of NK cells and their subsets may be correlated with citrullinated histone (H3) rather than with their percentage.
One of the limitations of this study is that it did not involve checking NK cell function in DVT patients or whether the secreted cytokine levels might differ in DVT patients.
Conclusion
We concluded that both the proportion of NK cell subsets and the citrullinated histone (H3) level varied in patients with DVT compared with those in the control group, as well as in acute and chronic cases compared to those in the control group. Moreover, a strong relationship exists between vascular thromboembolism and immune dysfunction. Therefore, they could be used as specific and sensitive diagnostic markers for DVT as targets for new strategies for the treatment of DVT; drugs that inhibit NET formation or facilitate NET degradation may be used in the treatment of DVT. In addition, controlling the imbalance in the proportion of NK cell subsets in DVT may help prevent or treat DVT.
Abbreviations
VTE, Venous thromboembolism; NETs, neutrophil extracellular traps; IFN-γ, interferon-γ; NK cells, natural killer cells; DVT, deep vein thrombosis; IRB, Institutional Review Board; ELISA, enzyme-linked immunosorbent assay; FSC/SSC, forward scatter/ side scatter; PT, prothrombin time; INR, international normalization ratio; APTT, activated partial thromboplastin time; ROC curve, receiver operating characteristic curve; AUC, area under the curve.
Acknowledgments
We would like to thank all participants in this study. Many thanks to Dr Walied Khereba for his help in the revision of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Geersing GJ, Cazemier S, Rutten F, Fitzmaurice DA, Hoes AW. Incidence of superficial venous thrombosis in primary care and risk of subsequent venous thromboembolic sequelae: a retrospective cohort study performed with routine healthcare data from the Netherlands. BMJ Open. 2018;8(4):e019967. PMID: 29678975; PMCID: PMC5914716. doi:10.1136/bmjopen-2017-019967
2. Ruppert A, Lees M, Steinle T. Clinical burden of venous thromboembolism. Curr Med Res Opin. 2010;26(10):2465–2473. PMID: 20825270. doi:10.1185/03007995.2010.516090
3. Lee LH, Gallus A, Jindal R, Wang C, Wu CC. Incidence of venous thromboembolism in asian populations: a systematic review. Throm Haemo. 2017;117(12):2243–2260. PMID: 29212112. doi:10.1160/TH17-02-0134
4. van Montfoort ML, Stephan F, Lauw MN, et al. Circulating nucleosomes and neutrophil activation as risk factors for deep vein thrombosis. Arter Throm Vas Biol. 2013;33(1):147–151. PMID: 23104849. doi:10.1161/ATVBAHA.112.300498
5. von Brühl ML, Stark K, Steinhart A, et al. Monocytes, neutrophils, and platelets cooperate to initiate and propagate venous thrombosis in mice in vivo. J Exp Med. 2012;209(4):819–835. PMID: 22451716; PMCID: PMC3328366. doi:10.1084/jem.20112322
6. Kambas K, Mitroulis I, Apostolidou E, et al. Autophagy mediates the delivery of thrombogenic tissue factor to neutrophil extracellular traps in human sepsis. PLoS One. 2012;7(9):e45427. PMID: 23029002; PMCID: PMC3446899. doi:10.1371/journal.pone.0045427
7. Brill A, Fuchs TA, Savchenko AS, et al. Neutrophil extracellular traps promote deep vein thrombosis in mice. J Throm Haemo. 2012;10(1):136–144. PMID: 22044575; PMCID: PMC3319651. doi:10.1111/j.1538-7836.2011.04544.x
8. Jorch SK, Kubes P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat Med. 2017;23(3):279–287. PMID: 28267716. doi:10.1038/nm.4294
9. Artis D, Spits H. The biology of innate lymphoid cells. Nature. 2015;517(7534):293–301. doi:10.1038/nature14189
10. Vivier E, Raulet DH, Moretta A, et al. Innate or adaptive immunity? The example of natural killer cells. Science. 2011;331(6013):44–49. PMID: 21212348; PMCID: PMC3089969. doi:10.1126/science.1198687
11. Bertin FR, Rys RN, Mathieu C, Laurance S, Lemarié CA, Blostein MD. Natural killer cells induce neutrophil extracellular trap formation in venous thrombosis. J Throm Haemo. 2019;17(2):403–414. PMID: 30456926. doi:10.1111/jth.14339
12. Qaseem A, Snow V, Barry P, et al. Joint American Academy of family physicians/American college of physicians panel on deep venous thrombosis/pulmonary embolism. current diagnosis of venous thromboembolism in primary care: a clinical practice guideline from the American Academy of family physicians and the American college of physicians. Ann Fam Med. 2007;5(1):57–62. PMID: 17261865; PMCID: PMC1783928. doi:10.1370/afm.667
13. Scoville SD, Freud AG, Caligiuri MA. Modeling human natural killer cell development in the era of innate lymphoid cells. Front Immunol. 2017;8:360. PMID: 28396671; PMCID: PMC5366880. doi:10.3389/fimmu.2017.00360
14. Cooper MA, Fehniger TA, Caligiuri MA. The biology of human natural killer-cell subsets. Trend Immunol. 2001;22(11):633–640. PMID: 11698225. doi:10.1016/s1471-4906(01)02060-9
15. Cooper MA, Fehniger TA, Turner SC, et al. Human natural killer cells: a unique innate immunoregulatory role for the CD56(bright) subset. Blood. 2001;97(10):3146–3151. PMID: 11342442. doi:10.1182/blood.v97.10.3146
16. Mikulak J, Di Vito C, Zaghi E, Mavilio D. Host immune responses in HIV-1 infection: the emerging pathogenic role of siglecs and their clinical correlates. Front Immunol. 2017;8:314. PMID: 28386256; PMCID: PMC5362603. doi:10.3389/fimmu.2017.00314
17. Dulphy N, Haas P, Busson M, et al. An unusual CD56(bright) CD16(low) NK cell subset dominates the early posttransplant period following HLA-matched hematopoietic stem cell transplantation. J Immunol. 2008;181(3):2227–2237. PMID: 18641363. doi:10.4049/jimmunol.181.3.2227
18. Duan Q, Gong Z, Song H, et al. Symptomatic venous thromboembolism is a disease related to infection and immune dysfunction. Int J Med Sci. 2012;9(6):453–461. PMID: 22859906; PMCID: PMC3410365. doi:10.7150/ijms.4453
19. Zhang X, Wang Q, Shen Y, Song H, Gong Z, Wang L. Compromised natural killer cells in pulmonary embolism. Int J Clin Exper Pathol. 2015;8(7):8244–8251. PMID: 26339393; PMCID: PMC4555721.
20. Thålin C, Daleskog M, Göransson SP, et al. Validation of an enzyme-linked immunosorbent assay for the quantification of citrullinated histone H3 as a marker for neutrophil extracellular traps in human plasma. Immun Res. 2017;65(3):706–712. PMID: 28161762; PMCID: PMC5440486. doi:10.1007/s12026-017-8905-3
21. Liu L, Zhang W, Su Y, Chen Y, Cao X, Wu J. The impact of neutrophil extracellular traps on deep venous thrombosis in patients with traumatic fractures. Clin. Chim. Acta. 2021;519:231–238. PMID: 34015302. doi:10.1016/j.cca.2021.04.021
22. Mauracher LM, Posch F, Martinod K, et al. Citrullinated histone H3, a biomarker of neutrophil extracellular trap formation, predicts the risk of venous thromboembolism in cancer patients. J Throm Haemo. 2018;16(3):508–518. PMID: 29325226; PMCID: PMC6294121. doi:10.1111/jth.13951
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.