Back to Journals » Patient Preference and Adherence » Volume 20
The Decision-Making Process of Antidepressant Use Among Patients with Depression: A Grounded Theory Study
Authors Liu L, Zhang L, Wu J, Li S
Received 21 March 2026
Accepted for publication 7 July 2026
Published 15 July 2026 Volume 2026:20 611068
DOI https://doi.org/10.2147/PPA.S611068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ling Liu, Lin Zhang, JiaXin Wu, Shuiying Li
Mental Health Center, West China Hospital/West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Correspondence: Shuiying Li, Mental Health Center, West China Hospital/West China School of Nursing, Sichuan University, No. 37 Guoxue Lane, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]
Objective: To explore how patients with depression and prior antidepressant use make decisions about antidepressant treatment and to construct a theoretical model from their perspectives.
Methods: A constructivist grounded theory study was conducted. Semi-structured in-depth interviews were undertaken with 26 patients with depression who had used antidepressants for at least one continuous treatment period of one month or longer, including current users and those who had discontinued medication. Data were collected through iterative theoretical sampling and analyzed using open, axial, and selective coding until theoretical saturation was achieved.
Results: The core process was conceptualized as “Weighing the Pros and Cons: Navigating Between the Quagmire of Illness and the Hope of Treatment.” This process comprised three dynamic, non-linear stages: decision trigger, active evaluation, and dynamic adaptation. Decision-making was initiated when patients’ tolerance threshold was broken by internal distress and/or external prompts, including authoritative advice. During active evaluation, patients balanced the perceived necessity of medication as a “chemical lever” against concerns about stigma, side effects, alienation, and dependence. Trust in physicians and individualized benefit-cost-risk trade-offs shaped initial decisions. During dynamic adaptation, medication-taking behaviors formed a continuum from strict adherence and negotiated self-adjustment to avoidance-oriented or distress-driven discontinuation. Treatment feedback continuously reshaped subsequent decisions.
Conclusion: Antidepressant decision-making is a dynamic process of sense-making and negotiation. The findings suggest that not all non-adherence should be interpreted as strategic self-management, highlight authoritative third-party advice as a trigger for treatment initiation, and indicate that identity tension may shape some patients’ medication experiences during long-term adaptation.
Keywords: depression, antidepressants, decision-making, medication adherence, constructivist grounded theory, qualitative research
Introduction
Depression is one of the most common mental disorders, affecting approximately 350 million people worldwide.1 It manifests as a loss of interest or pleasure in daily activities, persistent low mood, and significant behavioral changes.2,3 Depression is recognized as one of the leading causes of disability,4 and is closely associated with comorbid physical illnesses,5–7 suicidal behavior, and reduced life expectancy.5,8,9 Furthermore, depression ranks among the most costly diseases globally,6,10 resulting in nearly $925 billion in annual productivity losses worldwide and imposing a significant economic burden on society.11,12 Depression is projected to become the leading cause of global disease burden by 203012. In light of this, alleviating the escalating burden of mental illnesses such as depression has become a priority task in the global healthcare sector.10
Oral antidepressants are the first-line treatment for depression, yet their effectiveness is significantly constrained by a critical factor—patient adherence to medication. Although antidepressants are theoretically effective, studies indicate that as many as 50% to 70% of patients exhibit poor adherence,13–16 with approximately half discontinuing treatment prematurely.17 This non-adherence behavior is directly associated with increased risk of relapse, greater disease severity, and higher rates of emergency department visits and hospitalizations, ultimately leading to treatment failure and healthcare resource consumption.13,18,19 For this very reason, the World Health Organization has designated depression as one of the nine chronic diseases requiring special attention to improve treatment adherence.20
Existing research generally holds that patient medication adherence is a complex issue influenced by the interplay of multiple factors, including the patient, the disease, the medication, the healthcare system, and sociocultural aspects.21,22 Previous research has explored both barriers and facilitators of medication adherence among individuals with depression.15,21–23 However, current understanding tends to focus on listing and categorizing isolated “factors” or simplifying adherence into a static “behavioral outcome”. Medication adherence is increasingly understood as a temporal process that involves treatment initiation, implementation of the regimen, and eventual discontinuation rather than a single fixed behavior.24 In antidepressant treatment, qualitative evidence further suggests that the factors shaping adherence may differ across these stages, including initial acceptance of medication, day-to-day implementation, and decisions about continuation or discontinuation.25 These studies have failed to fully elucidate the complete psychosocial process by which patients dynamically process conflicting information, weigh pros and cons, and ultimately make medication decisions within complex real-world settings.
Medication adherence among individuals with depression is fundamentally an external manifestation of their treatment decision-making process, which is intertwined with internal conflicts and external constraints.26,27 This decision-making process may involve not only patients’ evaluation of symptom relief and side effects, but also their preferences, values, expectations, perceived autonomy, and interactions with healthcare professionals. Shared decision-making has therefore been increasingly emphasized in depression care because antidepressant selection and continuation require patients and clinicians to consider treatment benefits, adverse effects, costs, and personal preferences together.28,29 At the same time, patients’ medication decisions may also reflect attempts at self-management, particularly when they adjust medication use in response to perceived bodily feedback, daily life demands, or concerns about long-term treatment.25,30 In addition, antidepressant use may affect patients’ illness identity and self-perception, especially when medication is experienced as both a source of recovery and a reminder of being ill; emotional blunting and stigma-related concerns have also been shown to influence patients’ medication experiences and treatment decisions.31 However, the underlying logic and core mechanisms of this decision-making process remain insufficiently explored. In particular, limited attention has been paid to how patients move across decision stages, how they negotiate competing meanings of medication over time, and how shared decision-making, self-management attempts, and identity-related concerns are integrated into antidepressant use decisions.
This study aims to employ grounded theory research methodology to systematically construct a theoretical model explaining patients’ decision-making behaviors from their subjective perspective. By focusing on patients with prior antidepressant use, including both current users and those who had discontinued medication, this study seeks to capture how patients initiate, evaluate, adjust, continue, or discontinue antidepressant treatment in real-world contexts. This model seeks to provide a theoretical foundation for designing patient-centered clinical interventions that precisely enhance medication adherence.
Methods
Aims
This study was aimed at utilizing grounded theory to explore the decision-making process by which patients suffering from depression initiate, continue, adjust, or discontinue antidepressant treatment. Specifically, the study endeavored to identify how patients perceive and interpret obstacles and enablers, how they evaluate the anticipated benefits, costs, and risks, and how these appraisals develop over time. Based on this, a theoretical model was inductively developed to explain the underlying logic of antidepressant decision-making and to provide guidance for patient - centered adherence interventions.
Design
This study employed Charmaz’s constructivist grounded theory approach to investigate how patients with depression make decisions concerning the use of antidepressants.26 This approach was chosen because the study aimed not only to describe patients’ experiences, but also to develop an explanatory model of how antidepressant decision-making is formed, negotiated, and adjusted over time. Compared with phenomenology, which primarily focuses on the essence of lived experience, and descriptive qualitative or content analysis approaches, which mainly identify themes or categories, constructivist grounded theory is more suitable for explaining dynamic psychosocial processes and generating a theory grounded in participants’ accounts. Therefore, this approach was appropriate for examining how patients interpreted medication-related benefits, risks, social influences, and identity concerns across different stages of antidepressant use.
Participants
This study focuses on individuals with depression. Participants were recruited from the psychiatric outpatient department and mental health center of a tertiary hospital in Chengdu, China. Initial participants were recruited using purposive sampling. Subsequently, based on concepts and categories emerging from open coding of the initial data, theoretical sampling was conducted to continuously develop theoretical categories and validate relationships between categories until theoretical saturation was achieved. To increase variation in medication experiences, recruitment included patients who were currently taking antidepressants, those who had discontinued medication under physician guidance, and those who had discontinued medication by self-decision.
Inclusion criteria were as follows: (1) meeting diagnostic criteria for depression (single episode or recurrent) according to ICD-10 or DSM-5; (2) Age ≥ 18 years; (3) having a history of antidepressant medication use with at least one continuous treatment period of ≥1 month, including current users and those who had discontinued medication, to ensure sufficient experience and reflection on the treatment process; (4) being able to communicate clearly in spoken Chinese and complete an in-depth interview; and (5) providing voluntary informed consent to participate in the study. Exclusion criteria were as follows: (1) severe somatic illnesses, such as advanced malignant tumors, that might significantly interfere with survival prognosis or treatment priorities; (2) clear and urgent risk of self-harm or suicide (as determined by clinical assessment or self-report); (3) severe cognitive impairment, such as dementia or profound intellectual disability, or an acute psychotic state that could make interview information unreliable; and (4) any other circumstances determined by the investigator to potentially impede the safe and effective completion of study interviews.
Data Collected
Data were collected primarily through semi-structured in-depth interviews, supplemented by field notes documenting non-verbal cues and contextual information. An initial interview guide was developed based on the literature and the study aim, piloted with three eligible patients, and refined through team discussion and feedback obtained from the pilot interviews. Subsequently, the final interview guide was employed for formal data collection. The interview guide has been presented in Supplement 1.
The interview guide was designed according to the logic of constructivist grounded theory. It focused on participants’ experiences of treatment initiation, medication evaluation, adjustment, continuation, discontinuation, and the meaning of antidepressant use in daily life. The guide was intended to elicit process-oriented narratives rather than simply collect a list of barriers and facilitators. All interviews were conducted by LL, a female researcher with training in qualitative interviewing and mental health nursing research. The interviewer was not involved in participants’ routine clinical care, and no therapeutic relationship existed between the interviewer and participants before the interviews. At the beginning of each interview, the interviewer introduced her research role, explained the purpose of the study, and encouraged participants to describe their experiences in their own words. An open and non-judgmental interviewing style was adopted to reduce potential power imbalance and social desirability effects.
All interviews were conducted in quiet, private settings on a one-to-one basis. With participants’ informed consent, each interview was audio-recorded and accompanied by field notes. During the interviews, the interviewer used clarification, probing, paraphrasing, reflection, and summarizing to encourage participants to elaborate on their experiences and meanings. The interviews lasted 29 to 87 minutes, with an average duration of approximately 58 minutes. The variability in interview duration reflected differences in participants’ illness course, medication experience, willingness to disclose personal experiences, and the complexity of their decision-making trajectories. At the conclusion of each interview, the interviewer briefly summarized the discussion and confirmed key points with the participant. If any discrepancies arose, the participant was invited to correct or supplement the information to enhance accuracy.
Data Analysis
All interview recordings were transcribed verbatim by a researcher with extensive transcription experience, capturing the interviewees’ tone and pauses. The recordings and transcripts were cross-checked repeatedly to ensure accuracy. Analysis was conducted using Nvivo 12 software, following the principles of constructivist grounded theory proposed by Charmaz. Analysis commenced with initial coding, during which the transcripts were meticulously examined line by line to identify significant actions, meanings, and processes reflected in the participants’ accounts. By means of the method of constant comparison, similar codes were compared, refined, and grouped into more focused conceptual categories. Subsequently, focused coding was carried out to synthesize the most analytically significant and frequent initial codes into higher - level categories. During this phase, the relationships among categories were further explored and refined. Theoretical coding was then conducted to integrate these categories into a coherent explanatory framework and to identify the core category that captured the central process underlying the participants’ antidepressant medication decision-making. Throughout the analytical process, memo - writing was employed to record emerging ideas, conceptual links, and theoretical insights, thus supporting ongoing category development and interpretation.
Data collection and analysis continued until theoretical saturation was reached. In this study, theoretical saturation was judged according to the following criteria: no new initial codes emerged from additional interviews; the properties and dimensions of the main categories were sufficiently developed; the relationships among categories were repeatedly confirmed through constant comparison; and the core category could coherently integrate the three stages of decision trigger, active evaluation, and dynamic adjustment. Following the 26th interview, the research team agreed that theoretical saturation had been achieved.
To enhance coding rigor, the interview transcripts were coded independently by two researchers (LL and ZL). Any discrepancies detected during the coding process were systematically resolved through consensus meetings among the coders. Throughout the entire analytical process, all disagreements were successfully settled via discussion, thus attaining a high level of intercoder agreement. A third researcher (WJX) was on standby to arbitrate any unresolved discrepancies; however, this contingency was not needed in the end.
Ethical Considerations
Guided by the ethical tenets of the Declaration of Helsinki, this research protocol received formal review and approval from the Biomedical Ethics Committee of Sichuan University (Ethics Number: 20221171). All participants provided written informed consent prior to participation. They were explicitly informed that their anonymized responses and direct quotations would be used for publication and academic dissemination, and all gave their consent to this use. Participants were also assured of their right to withdraw from the study at any stage without penalty. To protect privacy, strict confidentiality was maintained through full anonymization of all data. Identifiable information was securely stored separately and will be destroyed after the retention period mandated by the institutional guidelines, while the anonymized dataset is retained solely for research integrity and archival purposes.
Results
Participant Characteristics
Following interviews with the 26th participant, no substantially new core concepts or category relationships emerged, which indicates theoretical saturation. The durations of the interviews ranged from 29 to 87 minutes, with an average duration of approximately 58 minutes. Out of the 26 participants, 16 were female (61.5%) and 10 were male (38.5%). The participants’ ages ranged from 19 to 64 years. The duration of depression since the initial diagnosis ranged from 6 months to 20 years. Detailed characteristics of the participants are presented in Table 1.
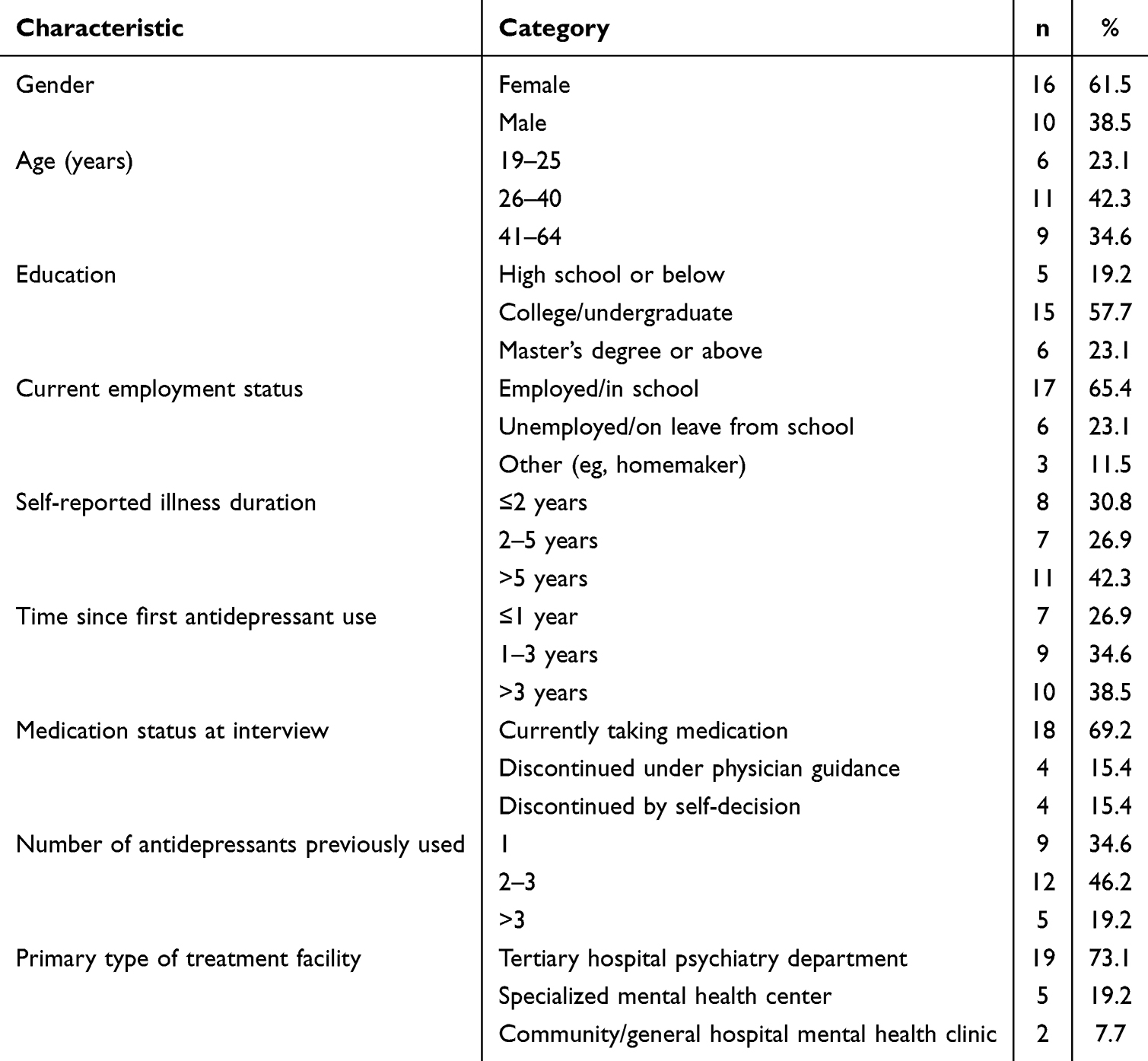 |
Table 1 Characteristics of the Participants |
Core Category
A decision-making process model centered on the core category of “Weighing the Pros and Cons: Navigating Between the Quagmire of Illness and the Hope of Treatment” has been generated by using grounded theory analysis. This model reveals that patient decision-making is not a one-time event but rather a dynamic, non-linear process encompassing three interrelated stages: decision trigger, active evaluation, and dynamic adjustment—while continuously interpreting feedback from both treatment and daily life.
Decision Trigger Stage: From Passive Endurance to Treatment Initiation
This stage represents the transition for patients from passively enduring symptoms to considering medication treatment. Its core characteristic is the “breaking of the tolerance threshold” with triggering factors falling into two categories: internal and external. These factors often intertwine to drive the initiation of treatment decisions.
Internal Trigger: Exceeding One’s Personal Pain Threshold
- Functional collapse: Severe impairment in work, study, or basic daily functioning. Patients describe feeling “like lying down all day, unable to get up” or “completely unable to focus during meetings, mind going blank”, leading to daily life grinding to a halt.
- Emotional Overwhelm: Emotional distress exceeds self-regulation capacity. Patients report: “I cry uncontrollably every day for no reason, breaking down over minor issues”, or “Evenings bring intense dread, as if something terrible is about to happen”. Negative emotions dominate daily life.
- Cognitive despair: Loss of faith in the future, coupled with a clear recognition of the limitations of self-regulation. Patients express thoughts like, “I’ve tried exercise, listening to music—nothing works. I can’t do this on my own anymore”, or “If this continues, I’ll lose my job, my family will fall apart, and I’ll be ruined”, leading to the conviction that “external help is essential”.
External Triggers: Key Agents and Precipitating Events
- Concern/pressure from significant others: Strong advice or worries from family members or partners become key catalysts, such as “My wife said I’d break down if I didn’t see a doctor soon”;
- Critical negative events: Specific incidents like interpersonal conflicts or work mistakes triggered by emotional issues make patients acutely aware of their symptoms’ destructive impact, as described by one patient: “I had a huge argument with a colleague because of my bad mood and lost an important project. That’s when I realized I couldn’t keep pushing through.”
- Advice from authoritative third parties: Professional recommendations from non-psychiatrists (eg, general practitioners, traditional Chinese medicine practitioners) provide the initial impetus to explore treatment. Patients mention: “During my physical exam, the doctor noticed I wasn’t well and suggested I see a psychiatrist, saying emotional issues might be affecting my physical health”;
Active Evaluation Stage: Constructing Decisions Amid Hope, Fear and Trust
After the tolerance threshold was broken, patients entered a stage of active evaluation in which they attempted to make sense of medication and form an initial treatment decision.
Contradictory Perceptions of Medications
- The Expectation of “Chemical Levers”: Medications are constructed as instrumental external forces to break vicious cycles and restore agency. As expressed in “I need an external force to give me a push, to pry my emotions out of the quagmire” (P07), this reflects an urgent demand for functional recovery above all else.
- The fear of “stigma and alienation”: Concerns that taking medication equates to “admitting mental illness” or “personal weakness”, or the dread that drugs might strip away one’s “true self”—as in “Will I still be myself after taking medication?(P10)”—reveal how societal stigma subtly constrains patients’ decision-making.
- “Side Effect Panic”: Concerns about side effects such as weight gain and diminished sexual function, particularly reflecting fears of losing bodily autonomy and control over intimate relationships. As one patient candidly stated, “I’d rather endure discomfort than gain weight from medication. What I dread most is becoming emotionless—like a wooden doll” (P09). For some patients, fears of emotional numbness, bodily change, or loss of self became highly salient concerns in medication decision-making.
A Preliminary Exploration of Trust Relationship
- The binary differentiation of trust models: Based on the study’s observations, physician-patient trust models exhibit a binary differentiation in terms of decision-making authority allocation, which can be categorized into two typical types. The first is “Paternalistic Trust”, where patients, based on their recognition of professional authority, transfer decision-making power to physicians, manifesting as passive adherence to medical instructions (eg, “Doctors are experts; I strictly follow their advice”). The second is “Shared Decision-making Trust”, where patients expect to become collaborative partners in decision-making based on information symmetry, demanding explanations for treatment plans and seeking the integration of their own preferences (eg, “I hope the doctor will discuss with me and explain why this treatment option was chosen”). These two trust patterns suggested different ways in which patients positioned themselves in the treatment process.
- “Trial-and-Error” as a Cognitive Strategy: Regardless of their preferred trust model, many patients approached medication use as a process of individualized trial and error. They not only accept “trial” but also view potential ineffectiveness or side effects as information guiding subsequent adjustments. As one patient stated: “Let’s take it and see how it works—that’s the only way to try it (P16)”. By reframing treatment as an “exploratory trial” rather than a “final verdict”, patients alleviate decision-making pressure, creating psychological space for establishing and dynamically adjusting doctor-patient trust.
Individualized Cost-Benefit Trade-Offs
- Benefit Assessment: Patients do not seek comprehensive symptom relief but focus on alleviating the most urgent “pain points”, such as rapidly curbing suicidal thoughts or improving severe insomnia.
- Cost Assessment: Considering the combined financial burden (medication costs, follow-up fees), time costs (time spent on appointments, impact of taking leave), and lifestyle adjustments required, patients mention, “The monthly medication and follow-up fees add up to a lot of money. Going to the hospital requires taking time off work, which means lost wages—that’s a significant pressure for me.”
- Risk Assessment: Concerns about drug dependency and lifelong reliance form a long-term risk narrative centered on the “future self.” One patient confessed, “I’m afraid once I start taking them, I won’t be able to stop. Having to rely on medication for the rest of my life would be utterly miserable (P18)”.
Dynamic Adjustment Stage
Medication adherence decisions are not a one-time choice but an ongoing dynamic process after starting treatment. Patients continually adjust their behavioral choices and psychological identification based on bodily feedback, emotional fluctuations, and shifts in social contexts. The core finding of this study is that “medication adherence” is not a binary state of “following/not following medical advice”, but rather a complex behavioral continuum formed by patients’ ongoing micro-decisions. Some behaviors conventionally viewed as poor adherence were described by participants as deliberate adjustments made in response to perceived risks, side effects, or situational demands.
Physical Feedback
- Searching for and attributing positive signals: Patients keenly notice any slight improvement (such as “my sleep seems a bit better”) and directly attribute it to the medication’s effect, thereby reinforcing the initial treatment decision.
- Multifaceted Attribution and Impact of Side Effects: Patients interpret side effects with significant variation, perceiving them either as “the drug taking effect” or “the body adapting”, or viewing them as “unbearable costs.” The latter represents a critical turning point leading to reduced adherence—for instance, some patients interpret “emotional numbness” as “losing the capacity for joy, anger, sorrow, and pleasure, becoming less than human (p11)”, bluntly stating, “I’d rather experience emotional fluctuations than become a lifeless puppet. What’s the point of living like that? (p26)”, thereby questioning the fundamental value of treatment.
Adherence Behavior Continuum: From Strict Adherence to Medical Advice to Strategic Deviation
- Strict Adherence: Strict adherence to medication regimens is primarily driven by either deep trust in the physician or intense fear of disease recurrence, commonly observed in patients during the initial stages of decision-making or those who have experienced severe relapses.
- Strategic Self-Adjustment: This is a key finding of the study: most instances of “non-adherence” are not passive resistance, but rather patients’ proactive “self-management of medication” based on self-monitoring. The core principle is balancing therapeutic efficacy, side effects, and personal life demands.
- “Take medicine as needed” model: Regard the medicine as an “emergency drug” rather than a “maintenance drug”, and adjust the medication behavior according to the situational needs, such as “I have a meeting today and am under great pressure, so I take one pill; I stay at home and relax on the weekend, so I don’t take any” (P07). This is essentially an instrumental cognition of the medicine.
- “Dosage Fine-Tuning” Mode: Self-adjusting medication to balance efficacy and side effects, such as “My doctor prescribed one tablet, but I found that taking half a tablet alleviated my dizziness and stabilized my mood, so I’ve been taking half a tablet long-term” (P15), reflecting patients’ individualized exploration of the “minimum effective dose”.
- “Medication Break” Approach: Periodically discontinuing medication due to concerns about long-term side effects or to test one’s condition, such as: “I stop taking it for a week or two every three months to see if I can manage without it and give my body a ‘rest’ (P22)”.
- Interrupted due to socializing: Due to social stigma, patients intentionally skip doses in social settings (such as business trips or gatherings) to avoid others noticing their medication use and to manage situations like drinking. One patient explained, “When I drink with friends, taking medication isn’t safe, and I’m afraid they’ll find out I’m on meds and think I’m abnormal (p06)”.
- Unilateral Discontinuation: The core reasons for abruptly stopping medication without consulting a doctor include: ① The illusion of “recovery”—mistaking symptom relief for disease cure, such as “I feel better now, so I don’t need to take the medicine anymore” (P04); ② Unbearable side effects—particularly weight gain, sexual dysfunction, and other side effects affecting self-identity and interpersonal relationships; ③ Deep fear of “addiction”, such as “I’m afraid I’ll be dependent on it forever, and that would be the end of me” (P18); ④ Frustration over “ineffective” treatment—experiencing weeks of waiting without achieving expected improvement, leading to despair and abandonment.
Decision-Making Cycles and the Oscillation of Identity
- Positive feedback loop: When patients perceive the benefits of taking medication, it has a positive feedback effect on adherence behavior, which is manifested as: symptom improvement → strengthening the belief that “the drug is effective and the treatment is safe” → consolidating standard adherence behavior → decision-making tends to stabilize.
- Negative Feedback Loops and Decision Restarts: Strategic adjustments or unilateral discontinuation of medication are not the end of the decision-making process, but rather the starting point for a new round of “proactive evaluation.” Fluctuations in condition following self-adjustments may prompt patients to return to standard treatment or seek treatment plan modifications. Relapse after complete discontinuation often leads patients to re-enter the healthcare system with complex emotions such as self-blame and helplessness. At this stage, their perceptions of medication and expectations for the doctor-patient relationship have shifted, making the decision-making process more cautious.
- The Tension of Identity: The fundamental conflict running throughout is the tug-of-war between the identities of “a patient under management” and “an autonomous, normal person.” Patients who successfully manage their medication as a “chronic disease” (like hypertension) tend to stabilize more easily; most who struggle, however, persistently experience an identity split: “On the days I take my medicine, I am a patient; on the days I skip it, I strive to be a normal person” (p19).
Theoretical Model of Antidepressant Decision-Making
Based on the core category of “Weighing the Pros and Cons: Navigating Between the Quagmire of Illness and the Hope of Treatment”, this research has developed a theoretical model for antidepressant decision-making among patients with depression (Figure 1). The model portrays decision-making as a dynamic and cyclical process that encompasses three stages: decision trigger, active evaluation, and dynamic adjustment. Patients initially enter the decision-making process when their tolerance threshold is exceeded by internal distress or external prompting factors. Subsequently, they actively evaluate the use of medication by weighing hope against fear, establishing trust, and assessing individualized benefits, costs, and risks. After commencing treatment, the use of medication is continuously adjusted in response to bodily feedback and contextual influences, thereby forming a continuum of adherence behavior. Feedback from medication experiences may further prompt a re - evaluation and restart the decision-making process. Throughout this process, identity tension acts as a cross - cutting theme that influences how patients perceive illness, treatment, and their own selves.
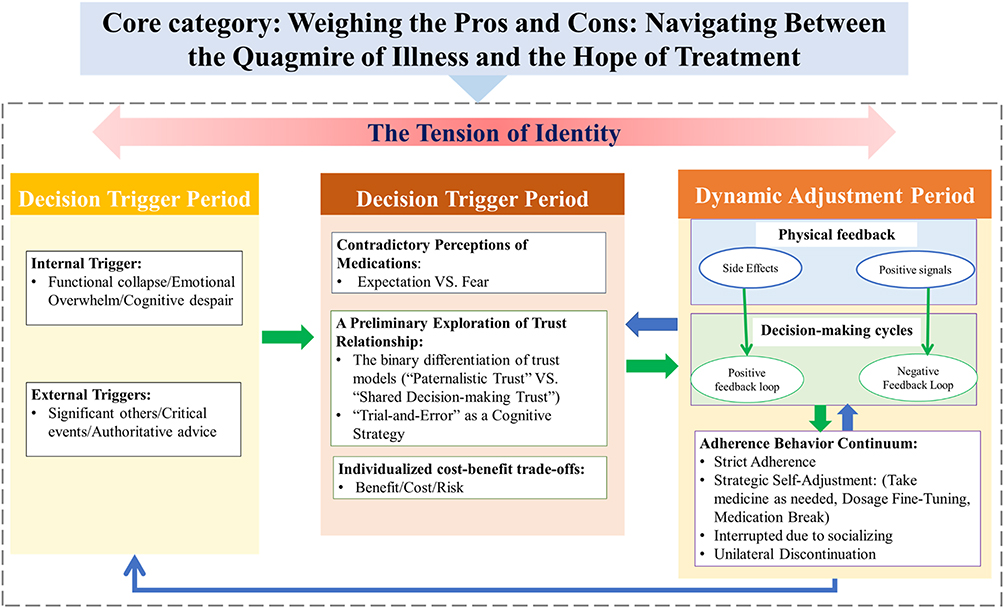 |
Figure 1 A grounded theory model of antidepressant decision-making among patients with depression. |
Discussion
Through in-depth interviews and grounded theory analysis, this study constructed a decision-making model for antidepressant medication among individuals with depression, centered on the core category “Weighing Pros and Cons: Navigating Between the Quagmire of Illness and the Hope of Treatment”. It revealed the dynamic cyclical nature of this decision-making process and its three-stage progressive logic, namely “Trigger–Evaluation–Adjustment”, and put forward the core finding of the “Adherence Behavior Continuum”. Rather than suggesting that all forms of non-adherence share the same meaning, this continuum highlights the heterogeneous nature of medication-taking behaviors, ranging from strict adherence and negotiated adjustment to avoidance-oriented or distress-driven discontinuation. This study enhances our understanding of the treatment decision - making mechanisms among individuals with depression, providing a theoretical foundation for developing intervention research aimed at improving antidepressant medication adherence among this population.
Although studies have examined barriers and facilitators of treatment adherence among individuals with depression, most have focused on listing isolated factors without revealing how patients dynamically weigh these factors and make decisions in real-world contexts.22,32,33 This study focuses on the “evolutionary logic of decision-making stages”, revealing the dynamic mechanisms by which barriers and facilitators operate across different decision-making phases. This addresses the existing research gap in exploring the “process of factor influence”. Furthermore, the findings of this study align with Mahtani-Chugani’s research on Spanish patients’ experiences with antidepressant use,26 both identifying the “struggles” patients face during decision-making (such as weighing efficacy against side effects) and validating the cross-cultural universality of patient decision dilemmas. Notably, this study further constructs a three-stage dynamic process model revealing the complete cycle of decision-making from initiation and assessment to ongoing adaptation, emphasizing that decision-making is not a one-time event. This is also consistent with evidence that different factors may influence antidepressant adherence at different phases, including initiation, implementation, and discontinuation.25
The proposed model should be understood as complementary to, rather than a replacement for, existing adherence theories. The WHO multidimensional adherence framework emphasizes that adherence is shaped by interacting patient-related, therapy-related, condition-related, health-system, and socioeconomic factors.34 The ABC taxonomy further conceptualizes adherence as a temporal process involving initiation, implementation, and discontinuation.25 Our model extends these perspectives by explaining how these factors are subjectively interpreted and reorganized by patients across the stages of decision trigger, active evaluation, and dynamic adjustment. In addition, the Necessity–Concerns Framework highlights the balance between perceived medication necessity and concerns about adverse consequences,35 which is reflected in participants’ weighing of medication as a “chemical lever” against fears of stigma, side effects, alienation, and dependence. The Common-Sense Model of self-regulation emphasizes how illness representations guide coping and self-management responses,36 while shared decision-making theory stresses the importance of collaboration, option comparison, and preference-sensitive deliberation in treatment decisions.37 Compared with these models, the contribution of the present grounded theory model lies in integrating medication beliefs, contextual triggers, self-management attempts, trust relationships, and identity-related concerns into a staged and cyclical account of antidepressant decision-making.
The concept of the “adherence behavior continuum” breaks through the traditional binary view of adherence as “adherence/non-adherence”. However, the present findings also suggest that non-adherence should not be uniformly interpreted as active self-management. In this study, some forms of non-adherence, such as dose fine-tuning, as-needed use, and medication breaks, reflected patients’ strategic attempts to balance perceived efficacy, side effects, and daily life demands. In contrast, unilateral discontinuation driven by the illusion of recovery, unbearable side effects, fear of dependence, or frustration over perceived ineffectiveness reflected a more vulnerable form of decision-making that may involve avoidance, fear, or despair rather than deliberate self-management. This more nuanced interpretation is supported by previous studies showing that antidepressant non-adherence is shaped by multiple patient-specific, medication-specific, health-system, sociocultural, and logistical barriers,22,33 and that adverse effects are closely associated with suboptimal adherence and treatment dropout.38 Therefore, the clinical value of the adherence continuum lies not in normalizing all non-adherence, but in helping clinicians distinguish between negotiated self-adjustment and high-risk discontinuation. Thus, these behaviors can be understood as partially overlapping with the desire for shared decision-making described by Zaini.27 Research findings suggest that structured interventions which integrate cognitive behavioral techniques with motivational interviewing are capable of effectively enhancing patients’ beliefs regarding medication and disease, augmenting self - efficacy, and consequently improving compliance.39 Similarly, shared decision-making interventions for antidepressant treatment have been shown to improve the quality of the decision-making process, even though their direct effects on adherence outcomes may be limited.29 This implies that clinical intervention ought not to be focused solely on “correcting” patients’ behaviors; instead, it should identify the meaning and risk level of different medication-taking patterns, incorporate patients’ self-management attempts into the therapeutic alliance when appropriate, and provide timely guidance when discontinuation reflects fear, side effects, or loss of hope.
During the decision-triggering stage, this study found that the “breaking of the tolerance threshold” is the core driving mechanism, which is jointly caused by the accumulation of internal pain and external events. This finding indicates that treatment initiation was often not triggered by symptom severity alone, but by the point at which patients could no longer maintain daily functioning or continue self-regulation without external support. Some scholars have pointed out that decision-making difficulties in individuals with depression may be associated with impaired executive function.40 However, the present qualitative data cannot directly determine the cognitive or neuropsychological mechanisms underlying delayed treatment initiation. Therefore, this interpretation should be regarded as a possible contextual explanation rather than a conclusion directly derived from the current data. Importantly, our study also identified suggestions from authoritative third parties, such as physical examination doctors, general practitioners, or traditional Chinese medicine practitioners, as external catalysts for treatment initiation. This finding has practical significance because depression care often involves gaps between symptom recognition, treatment initiation, adequate treatment, and response.41 Evidence also suggests that collaborative or integrated care, preference matching, and case management may help improve depression treatment initiation in primary care settings.42 Therefore, authoritative third-party advice may represent an important early intervention opportunity, particularly for patients who have not yet actively sought psychiatric care.
A study revealed that internalized stigma shows a significant negative correlation with medication adherence, whereas perceived stigma does not exhibit such a relationship. This precisely corroborates a key finding of this model: what truly impedes decision-making is not external societal judgment (perceived stigma), but rather the self-deprecation and fear of alienation that arise when patients internalize stigma—such as the belief that “taking medication equates to admitting weakness”.43 At the level of trust-building, the two models identified in this study, “authority trust” and “collaborative trust”, provide a classification framework for clinical communication. Integrating the “implicit prototype theory of shared decision-making between physicians and patients” proposed in prior research,44 future physician-patient communication training can focus on shaping physicians’ “collaborative” implicit prototypes to reduce patients’ anxiety about treatment uncertainty. However, the present findings also suggest that trust should be understood as a dynamic resource rather than a fixed physician-patient attribute. Patients may initially rely on authoritative trust to reduce uncertainty, but later require more collaborative communication when managing side effects, doubts, or medication adjustments.
This study reveals that patients’ interpretations of side effects directly lead to distinct behavioral pathways (continuing medication vs. strategic adjustments or discontinuation). This validates Chanie’s finding that side effects—particularly severe or identity-affecting ones—are key drivers of non-adherence.45 Recent systematic review evidence also indicates that antidepressant-related adverse effects are associated with suboptimal adherence, highlighting the importance of proactive side-effect education and doctor-patient communication.38 Research indicates that individuals with depression may show altered patterns of risk-related decision-making.46 However, the present study did not directly assess cognitive risk preference. Therefore, we interpret patients’ medication adjustments primarily as meaning-based responses to perceived efficacy, side effects, and daily life demands, rather than as evidence of a stable risk-taking tendency.
Finally, identity tension should be interpreted as an important but not yet fully exhaustive explanatory theme. In this study, identity tension was most clearly reflected in the dynamic adjustment stage, particularly when patients experienced medication as simultaneously enabling functional recovery and threatening their sense of being a “normal” or autonomous self. This interpretation is consistent with evidence that emotional blunting is common among patients with depression and that a substantial proportion of patients attribute emotional changes to antidepressants or consider stopping medication because of perceived emotion-related side effects.31 Thus, identity tension may help explain why some patients experience medication not merely as a therapeutic tool but also as a challenge to self-continuity and social identity. Nevertheless, because this theme was supported by a limited number of direct quotations in the present dataset, it should be presented as a salient interpretive finding rather than as a fully established mechanism across all decision-making stages. Future qualitative and longitudinal studies are needed to further examine how identity tension develops across treatment initiation, evaluation, and long-term adaptation.
Implications for Clinical Practice
The decision-making process model from this study provides a theoretical framework for intervention research aimed at improving medication adherence among patients with depression. Enhancing adherence should span the entire decision-making cycle. During the triggering phase, clinicians and non-psychiatric healthcare providers should pay attention to signs of functional breakdown and use timely, credible advice or referral to facilitate treatment initiation. During the evaluation phase, interventions should focus on resolving medication-related cognitive dissonance, discussing expected benefits and potential adverse effects, and building collaborative trust to reduce decision anxiety. During the adaptation phase, clinically common “non-adherence behaviors” should be carefully differentiated rather than uniformly reinterpreted as self-management. Through open communication, strategic self-adjustments can be discussed and guided within a safe therapeutic alliance, whereas abrupt discontinuation driven by fear, side effects, perceived recovery, or despair should be identified as a potential risk signal requiring timely clinical support. This necessitates establishing a dynamic adherence monitoring system in clinical practice, shifting from a binary assessment of “whether instructions were followed” to a continuous evaluation of “why such decisions were made”. Ultimately, this facilitates a paradigm shift from passive compliance to active participation in adherence.
Limitations
This study needs to pay attention to the following limitations: First, there is a certain selection bias in the research sample. All participants have a history of taking medication, and the group of patients who have always refused drug treatment has not been covered. This may lead to the incompleteness of the model in explaining the obstacles to the initiation of drug treatment. Second, the data collection mainly relies on retrospective self-reports, which may have memory bias and social desirability effects. Future studies can combine real-time ecological assessment or objective monitoring data to improve the reliability of the results. Third, the cross-sectional design makes it difficult to capture the dynamic evolution of the decision-making process. The feedback loop mechanism proposed in the model needs to be verified through long-term follow-up studies. Fourth, qualitative research is difficult to quantify the relative weights and causal relationships of various influencing factors. Future studies can adopt a mixed-method design and conduct large-scale surveys to verify and expand the theoretical model. Finally, the study mainly focuses on the patient’s perspective and does not sufficiently explore the impact of doctors’ behaviors and clinical situations in the doctor-patient interaction. Subsequent studies can deepen the understanding of this dimension through doctor-patient paired interviews or observations of the clinical process.
Conclusion
This study suggests that decision-making regarding antidepressant medication is a dynamic, iterative process of sense-making and negotiation, rather than a singular act of compliance. The constructed model shows that patients weigh the burden of illness against the ambivalent hope offered by treatment across three interrelated stages: decision trigger, active evaluation, and dynamic adaptation. The central theoretical contribution of this study is the identification of an adherence behavior continuum, which reframes antidepressant medication-taking as a spectrum of evolving decisions rather than a simple binary distinction between adherence and non-adherence. This continuum ranges from strict adherence and negotiated self-adjustment to avoidance-oriented or distress-driven discontinuation. Therefore, not all non-adherence should be interpreted as strategic self-management, and patients’ agency should be understood as context-dependent and constrained by symptoms, side effects, stigma, fear, and available support. The findings also highlight the role of authoritative third-party advice in triggering treatment initiation and suggest that identity tension may shape some patients’ experiences of medication, particularly during long-term adaptation. These findings indicate that clinical interventions should move beyond a simplistic compliance framework by addressing medication-related fears, supporting collaborative trust, identifying high-risk discontinuation, strengthening early recognition and referral, and, when relevant, supporting patients in reconciling medication use with self-identity. Future studies should use longitudinal qualitative designs to follow changes in medication decision-making over time and mixed-methods studies to quantitatively test the relationships among decision triggers, benefit-risk evaluation, adherence behaviors, identity tension, and treatment outcomes.
Data Sharing Statement
Details of data and materials can be obtained by contacting the corresponding author. All data included in this study are being published for the first time and have not been partially or wholly published in any other article.
Ethics Approval and Consent to Participate
This study was performed in accordance with the Declaration of Helsinki and was approved by the Biomedical Ethics Committee of Sichuan University [Ethics Number:20221171]. We introduced the study to all participants and obtained their consent.
Acknowledgments
We are grateful to all researchers for their efforts and all people who are willing to participate the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zald D, McHugo M, Ray K, et al. Meta-analytic connectivity modeling reveals differential functional connectivity of the medial and lateral orbitofrontal cortex. Cereb Cortex. 2014;24(1):232–14. doi:10.1093/cercor/bhs308
2. Chand SP, Arif H, Kutlenios RM. Depression (Nursing) 2023. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK568733/.
3. Arif SPCH. Depression 2023. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430847/.
4. WHO. Depresión. Available from: https://www.who.int/es/news-room/fact-sheets/detail/depression.
5. Liu B, Qin P, Liu Y, et al. Mental disorders and suicide attempt in rural China. Psychiatry Res. 2018;261:190–196. doi:10.1016/j.psychres.2017.12.087
6. W HA, D L, R JR, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010. Lancet. 2013;382(9904):1575–1586. doi:10.1016/S0140-6736(13)61611-6
7. Graaf RD, Tuithof M, Dorsselaer SV, et al. Verzuim door psychische en somatische aandoeningen bij werkenden. Resultaten van de ‘Netherlands mental health survey and incidence study-2’ (NEMESIS-2) [Absenteeism due to psychological or somatic disorders in workers. Results of the ‘Netherlands Mental H. 2011.
8. Rock PL, Roiser JP, Riedel WJ, et al. Cognitive impairment in depression: a systematic review and meta-analysis. Psycholog Med London. 2014;44(10):2029–2040. doi:10.1017/S0033291713002535
9. Roca M, Vives M, López-Navarro E, et al. Cognitive impairments and depression: a critical review. Actas espanolas de psiquiatria. 2015;43(5):187–193.
10. Chisholm D, Sweeny K, Sheehan P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry. 2016;3(5):415–424. doi:10.1016/s2215-0366(16)30024-4
11. Kazdin AE, Rabbitt SM. Novel models for delivering mental health services and reducing the burdens of mental illness. Clin Psychol Sci. 2013;1:170–191. doi:10.1177/2167702612463566
12. World Bank Group and W. Out of the shadows: making mental health a global development priority organized by World Bank Group & WHO Washington D.C2016. Available from: http://www.worldbank.org/en/events/2016/03/09/out-of-the-shadows-making-mental-health-a-global-priority.
13. Sriharsha M. Alekhya P treatment and disease related factors affecting non-adherence among patients on long term therapy of antidepressants. J Depress Anxiety. 2015;04(02). doi:10.4172/2167-1044.1000175
14. Alekhya P, Sriharsha M, Ramudu RV, et al. Adherence to antidepressant therapy: sociodemographic factor wise distribution. Int J Pharmaceu Clin Res. 2015;7(3):180–184.
15. Banerjee S, Varma RP. Factors affecting non-adherence among patients diagnosed with unipolar depression in a psychiatric department of a tertiary hospital in Kolkata, India. Depress Res Treat. 2013;2013:809542. doi:10.1155/2013/809542
16. Masand PS. Tolerability and adherence issues in antidepressant therapy. J Clinical Therapeutics. 2003;25(8):2289–2304. doi:10.1016/S0149-2918(03)80220-5
17. Sirey JA, Banerjee S, Marino P, et al. Adherence to depression treatment in primary care: a randomized clinical trial. JAMA Psychiatry. 2017;74(11):1129. doi:10.1001/jamapsychiatry.2017.3047
18. Bosworth H, Voils C, Potter G, et al. The effects of antidepressant medication adherence as well as psychosocial and clinical factors on depression outcome among older adults. Int J Geriatric Psychiatry. 2008;23(2):129–134. doi:10.1002/gps.1852
19. Liu X, Tepper P, Able S. Adherence and persistence with duloxetine and hospital utilization in patients with major depressive disorder. Int Clin Psychopharmacol. 2011;26(3):173–180. doi:10.1097/YIC.0b013e328343ba1e
20. Dell’Osso B, Albert U, Carrà G, et al. How to improve adherence to antidepressant treatments in patients with major depression: a psychoeducational consensus checklist. Ann General Psychiatry. 2020;19(1). doi:10.1186/s12991-020-00306-2
21. Ching HS, Anne JS, Balamurugan T, et al. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290. doi:10.1371/journal.pone.0179290
22. Meng Y, Chiu C, Kapoor M, et al. Patient perceived barriers and enablers to medication adherence in the treatment of depression: a qualitative study. J Primary Care Commun Health. 2024;15(000). doi:10.1177/21501319241286313
23. Jin-liang W, Chen-chen Y, Qi Y, et al. Influencing factors of antidepressant polypharmacy in inpatients with depression. Chin J Hospital Pharm. 2019;39(20):2081–2085. doi:10.13286/j.cnki.chinhosppharmacyj.2019.20.14
24. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
25. Srimongkon P, Aslani P, Chen TF. Consumer-related factors influencing antidepressant adherence in unipolar depression: a qualitative study. Patient Prefere Adher. 2018;12:1863–1873. doi:10.2147/ppa.S160728
26. Mahtani-Chugani V, Sanz-Alvarez E, Cuevas-Castresana CDL. Estrategias de manejo de los antidepresivos desde la perspectiva de los pacientes: luchando interna y externamente. Atención Primaria. 2012;44(8):463–470. doi:10.1016/j.aprim.2011.10.003
27. Syahrir Z, Harvin MB, Ahmad S, et al. Development of a strategic tool for shared decision-making in the use of antidepressants among patients with major depressive disorder: a focus group study. Int J Environ Res Public Health. 2018;15(7):1402. doi:10.3390/ijerph15071402
28. Hopwood M. The shared decision-making process in the pharmacological management of depression. Patient. 2020;13(1):23–30. doi:10.1007/s40271-019-00383-w
29. LeBlanc A, Herrin J, Williams MD, et al. Shared decision making for antidepressants in primary care: a cluster randomized trial. JAMA Intern Med. 2015;175(11):1761–1770. doi:10.1001/jamainternmed.2015.5214
30. Crowe M, Inder M, McCall C. Experience of antidepressant use and discontinuation: a qualitative synthesis of the evidence. J Psych Mental Health Nurs. 2023;30(1):21–34. doi:10.1111/jpm.12850
31. Christensen MC, Ren H, Fagiolini A. Emotional blunting in patients with depression. Part I: clinical characteristics. Ann Gen Psychiatry. 2022;21(1):10. doi:10.1186/s12991-022-00387-1
32. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
33. Ho SC, Jacob SA, Tangiisuran B. Barriers and facilitators of adherence to antidepressants among outpatients with major depressive disorder: a qualitative study. PLoS One. 2017;12(6):e0179290. doi:10.1371/journal.pone.0179290
34. De Geest S, Sabaté E. Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs. 2003;2(4):323. doi:10.1016/s1474-5151(03)00091-4
35. Tomás CC, Oliveira E, Sousa D, et al. Proceedings of the 3rd IPLeiria’s international health congress: leiria, Portugal. 6-7 May 2016. BMC Health Serv Res. 2016;16(Suppl 3):200. doi:10.1186/s12913-016-1423-5
36. Hagger MS, Orbell S. The common sense model of illness self-regulation: a conceptual review and proposed extended model. Health Psychology Review. 2022;16(3):347–377. doi:10.1080/17437199.2021.1878050
37. Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
38. Niarchou E, Roberts L, Naughton BD. What is the impact of antidepressant side effects on medication adherence among adult patients diagnosed with depressive disorder: a systematic review. J Psychopharmacol. 2024;38(2):127–136. doi:10.1177/02698811231224171
39. Khalifeh AH, Alhalaiqa FN, Hamaideh SH, et al. The effect of adherence therapy on medication adherence, health beliefs, self-efficacy, and depressive symptoms among patients diagnosed with major depressive disorder. Int J Mental Health Nurs. 2023;32(3):778–790. doi:10.1111/inm.13113
40. Singh S, Gupta A, Singh GP. Decision making and its correlates in recurrent depressive disorder. Indian J Psychiatry. 2023;65(11):1158–1164. doi:10.4103/indianjpsychiatry.indianjpsychiatry_633_23
41. Pence BW, O’Donnell JK, Gaynes BN. The depression treatment cascade in primary care: a public health perspective. Current Psychiatry Reports. 2012;14(4):328–335. doi:10.1007/s11920-012-0274-y
42. Moise N, Falzon L, Obi M, et al. Interventions to increase depression treatment initiation in primary care patients: a systematic review. J Gen Intern Med. 2018;33(11):1978–1989. doi:10.1007/s11606-018-4554-z
43. Shi J, Chen Y, Jiang Y, et al. Stigma and its associations with medication adherence in major depressive disorder. Psychiatry Res. 2024;331:115664. doi:10.1016/j.psychres.2023.115664
44. Yuan X-E, Zhao R, Zhu D. The psychological pathways through which individual characteristics of physicians and patients influence shared decision-making: an implicit prototype perspective. Adv Psycholog Sci. 2023;31(6):1044–1054. doi:10.3724/SP.J.1042.2023.01044
45. Chanie GS, Belachew EA, Limenh LW, et al. Prevalence and determinants of antidepressant non-adherence among patients with major depressive disorder in Ethiopia: a multi-center cross sectional study. Sci Rep. 2025;15(1). doi:10.1038/s41598-025-15102-9
46. Lu J, Zhao X, Wei X, et al. Risky decision-making in major depressive disorder: a three-level meta-analysis. Int J Clin Health Psycholog. 2024;24(1):100417. doi:10.1016/j.ijchp.2023.100417
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Patients’ Psychological Contract with Pharmacists on Medication Adherence: A Qualitative Study
Gu Y, Mu X, Zhang Y, Tang Y, Zhang T, Tang F
Patient Preference and Adherence 2023, 17:547-555
Published Date: 3 March 2023
Perspective and Experience of Patients with Aplastic Anemia on Medication Adherence
Li H, Wu X, Shen J, Lou S
Patient Preference and Adherence 2023, 17:2215-2225
Published Date: 6 September 2023
Improving Assessment of Adherence Behaviors and Drivers: Targeted Literature Review and Concept Elicitation Interviews in Multiple Countries and Disease Populations
Bentley S, Exall E, Morgan L, Roche N, Khunti K, Rossom R, Piercy J, Arbuckle R, Higgins VS
Patient Preference and Adherence 2024, 18:1231-1242
Published Date: 17 June 2024
Preclinical Evidence for the Use of Brexpiprazole + Antidepressant Treatment for Major Depressive Disorder and Post-Traumatic Stress Disorder: A Systematic Review
Brubaker M, Kapadia S, Maletic V, Chambers JS, Watling CP, Citrome L
Neuropsychiatric Disease and Treatment 2025, 21:421-436
Published Date: 28 February 2025
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025