Back to Journals » Patient Preference and Adherence » Volume 17
Perspective and Experience of Patients with Aplastic Anemia on Medication Adherence
Authors Li H, Wu X, Shen J, Lou S
Received 1 June 2023
Accepted for publication 25 August 2023
Published 6 September 2023 Volume 2023:17 Pages 2215—2225
DOI https://doi.org/10.2147/PPA.S390409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Hangting Li,1,* Xiaolian Wu,1,* Jiaoni Shen,2 Shuhui Lou2
1Department of Hematology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, People’s Republic of China; 2School of Nursing, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuhui Lou, School of Nursing, Zhejiang Chinese Medical University, 548 Binwen Road, Binjiang District, Hangzhou City, Zhejiang Province, People’s Republic of China, Email [email protected]
Background: Drug treatment is critical for patients with aplastic anemia, and medication adherence directly impacts the therapeutic effect. Poor medication adherence is common among patients with chronic diseases. However, knowledge of the perceptions and experiences of patients with aplastic anemia regarding taking prescribed medicines is limited.
Objective: To gain insights into the perceptions and experiences of patients with aplastic anemia regarding taking prescribed medicines.
Methods: A descriptive qualitative design was used. Fifteen patients with aplastic anemia were recruited from the hematology department. Individual semi-structured interviews were conducted. The data were analyzed using the thematic analysis method and conceptualized using the Health Belief Model.
Results: Five themes emerged: the perceived threat of aplastic anemia, perceived benefits and barriers of taking prescribed medicines, cues to action, self-efficacy, and modifying factors. While patients’ knowledge was limited, they acknowledged the threat of aplastic anemia and the necessity of drug treatments, but they also encountered some barriers in practice. The desire for health and healthcare providers’ opinions were the main clues to medication adherence. The expectation of the future and the sense of self-competency made participants adopt good behavior.
Discussions: This study provided new perspectives on the medication adherence of patients with aplastic anemia, which may be valuable in clinical work and research. Further interventions should be developed for intentional and unintentional non-compliance. Future research can start with developing professional assessment tools addressing the influence of cognition and emotion on compliance.
Keywords: aplastic anemia, China, health belief model, medication adherence, perception, qualitative research
Introduction
Aplastic anemia is a refractory haematologic disease characterized by pancytopenia and hypocellular bone marrow.1 The incidence of this disease is 2 per million in Western countries and up to 6 per million in Asia.2 Notably, chronic aplastic anemia accounts for 4/5 of these cases.3 Oral immunosuppressive therapy, such as cyclosporin A (CsA), is often used as the initial treatment for aplastic anemia, with the addition of eltrombopag and androgen.4 A long-term treatment, at least six months, is often required in aplastic anemia.5 Therefore, applying the above oral agents at home is inevitable, where direct supervisions of drug administration from healthcare providers are unavailable.6 Thus, posing the problem of medication adherence to the patients.
Good medication adherence is crucial for aplastic anemia, as minor deviations from the treatment regimens may result in drug resistance and failure.5 However, contrary to the many pathophysiology and treatment studies, sparse literature covers medication adherence in aplastic anemia patients. Although some studies explore interventions to improve patient medication compliance, the status of medication implementation, medication persistence, and related factors are unclear, which is not conducive to the substantive progress of interventions.7,8
As demonstrated by multiple studies, medication adherence is a common but complex individual behavior faced by patients with chronic medical problems related to multiple factors.9–11 When it comes to aplastic anemia patients, the oral medications mentioned, like androgens, often show significant side effects, such as severe acne, local skin reactions, mood swings, or sexual arousal.12 On the other hand, it is reported that aplastic anemia patients have significant symptom burdens, poor quality of life, and anxiety,13 which are all expected to affect medication adherence. Given the complexity of medication adherence itself and the unclarity of medication adherence in patients with aplastic anemia, we intend to use a qualitative method to provide in-depth insights into the behaviors, experiences, and perceptions of medication adherence from patients’ perspectives.
The Health Belief Model (HBM) is a theoretical framework for conceptualizing individuals’ attitudes and beliefs to explain and predict health behaviors.14 The HBM includes seven key domains that influence health behaviors: perceived severity, perceived susceptibility, perceived benefits, perceived barriers, cues to action, modifying factors, and self-efficacy.14 Among them,15 perceived severity and susceptibility describe patients’ subjective belief that they know the hazards and risks of poor medication adherence. Perceived benefits and barriers refer to patients’ prediction of the benefits and obstacles in taking prescribed medicines. Self-efficacy refers to patients’ subjective judgment on whether he or she can successfully follow doctors’ prescription. Cues to action refer to internal and external motivators that encourage patients’ medication adherence.16 Modifying factors include demographic variables and personality traits that can play a role in shaping medication taking behavior.17 HBM has been applied in various studies to predict and improve adherence to long-term therapy for various chronic diseases.18 Therefore, in this study, we utilized the HBM to explore how patients’ perceptions may influence their medication adherence and identify the trigger factors and challenges they encountered.
We expect that the findings of this study will contribute to a better understanding of aplastic anemia patients’ medication adherence. Importantly, this work can identify problems and obstacles in implementing and persisting oral medication and find entry points for a better care scheme.
Methods
Study Design
We used a descriptive qualitative design that directly describes experiences and perceptions.19 Data were collected and analyzed based on the seven essential dimensions of the HBM.
Participants and Procedure
A purposive sampling method, combined with the snowballing technique and maximum variation (gender, age, and length of illness), was used to select patients with aplastic anemia from a public hospital in China from August 2020 to February 2021. The inclusion criteria were as follows: (1) diagnosed with aplastic anemia based on the Chinese criteria released in 2017,20 (2) aged ≥18 years old, (3) received aplastic anemia medication for at least three months, (4) volunteered to participate in the study. Participants were excluded if they had received hematopoietic stem cell transplantation or had cancer, other chronic diseases, or communication barriers. The researchers had face-to-face contact with potential participants at the hematology ward and outpatient clinic. If the patients were willing to participate, they were informed of the study information and required to complete a written consent form. We promised to protect anonymity, and the patients could terminate their participation in the research at any time. Data saturation was deemed met when no new themes were presented for three consecutive interviews after analyzing at least ten interviews.21
Data Collection
A semi-structured interview guide was designed based on literature reviews and the seven dimensions of HBM (see Appendix 1). The participants’ demographic and clinical information, including gender, age, occupation, marriage status, education, and duration of illness, was collected before each face-to-face interview. The lead researcher conducted all face-to-face interviews at the time and location arranged in advance, such as a free hospital classroom, consulting room, or single ward, by the researcher and participant. The interview started with the researcher’s self-introduction and casual conversations with the participants to create a relaxing atmosphere. Follow-up questions were used to encourage detailed responses. Additionally, the participants’ observations, interactions, and body language were recorded in field notes. The researcher remained neutral and avoided making any judgments about the interview contents. Interviews lasted an average of 29 (17–50 min) min. One participant withdrew midway because her son-in-law entered the ward during the interview and answered questions for the participant. The interview data before the interference were still included in the analysis.
Data Analysis
The interviews were transcribed verbatim in Chinese within 24 hours by the interviewer. We used thematic analysis to analyze the transcripts concurrently with the data collection.22 Initially, two researchers independently performed inductive coding. Researchers read the transcripts several times to familiarize themselves with the overall content. Then, they hand-coded all the narrative data related to the patients’ views and experiences on medication taking line-by-line. Subsequently, the generated codes were grouped into themes. Analysis was stopped when all the codes were consistent in each theme.23 Next, the themes were clearly defined, and supportive quotes were selected from the data. Finally, deductive analysis was conducted by categorizing the specific themes and codes into the most relevant dimensions of the HBM. Disagreements were resolved by discussing with a third researcher. Our team’s researcher, proficient in Chinese and English, translated the final results from Chinese into English. Two other researchers checked the translated text and discussed the questions until both sides agreed.
Rigor
This study’s rigor was established using the criteria of credibility, transferability, dependability, and confirmability.24 Firstly, peer debriefing and member checking were used to maintain credibility. The researchers negotiated with one another to address any disagreement on methodological issues or data analysis. Two participants were involved in the member-checking process to confirm whether the findings reflected their views, feelings, and experiences. Secondly, transferability was enhanced by thick, vivid descriptions collected through the interviews. Thirdly, dependability and confirmability were reached by audit trail and documentation of field notes, and every step in the analysis process was maintained.
Ethical Considerations
This study was approved by the ethics committee of the First Affiliated Hospital of Zhejiang Chinese Medical University. The whole research was also in line with the Declaration of Helsinki. Written informed consent was obtained from each participant, who was informed that what they said would be quoted and their information like gender, age, occupation would be listed in Table 1 anonymously, the data would access exclusively to the researchers.
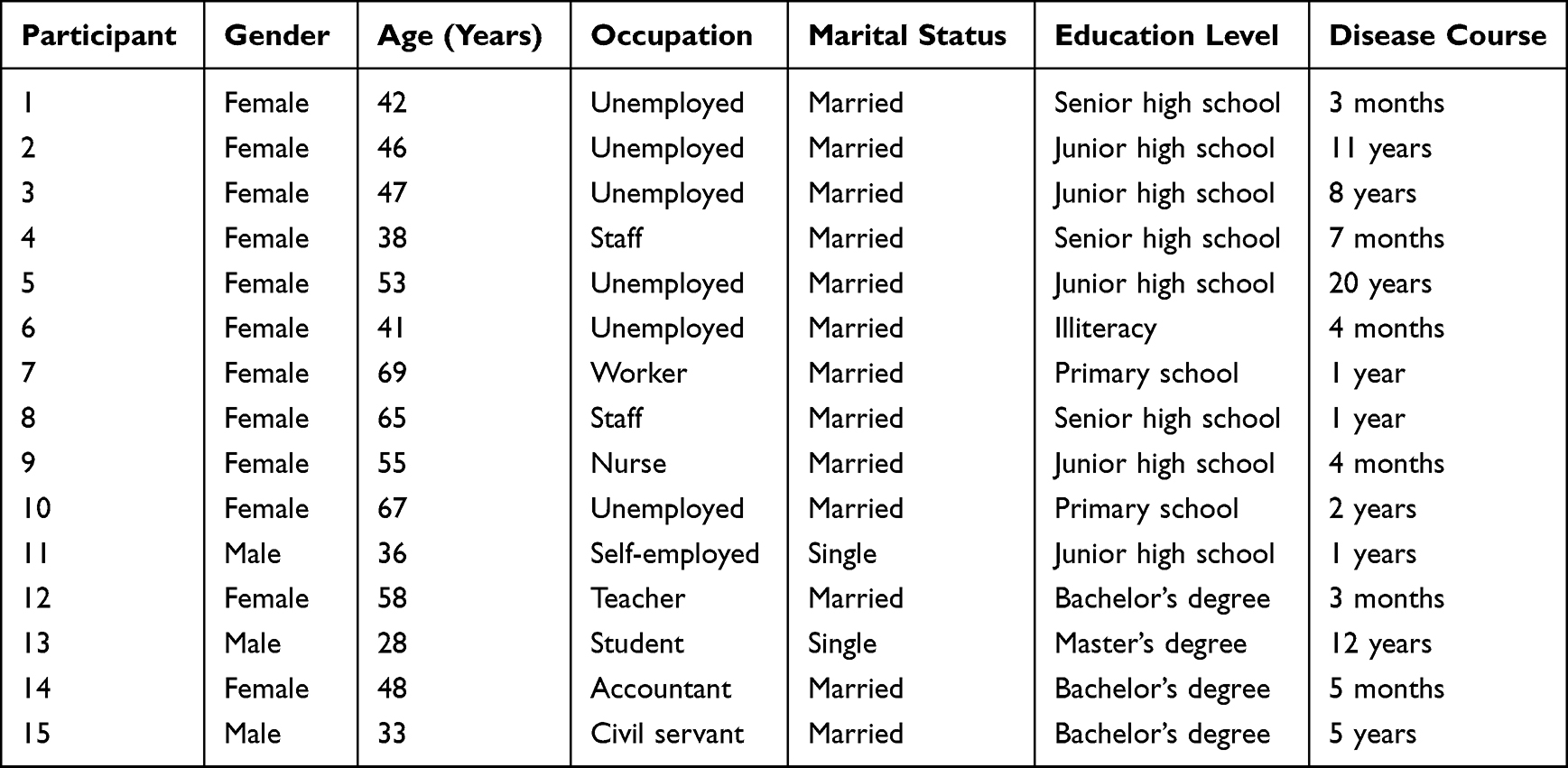 |
Table 1 Demographic and Clinical Characteristics of the Participants |
Results
Fifteen patients with aplastic anemia (3 males and 12 females, 28–69 years of age) from a public hospital were recruited. Demographic and clinical information is shown in Table 1. Notably, there were 12 minor themes grouped into five major themes: the perceived threat of aplastic anemia, perceived benefits and barriers of taking prescribed medicines, cues to action, self-efficacy, and modifying factors.
Perceived Threat of Aplastic Anemia
Understanding of Aplastic Anemia
Hematological diseases, especially aplastic anemia, have a low incidence in the population, so most participants knew little about it before they were diagnosed. They usually were diagnosed accidentally and described it as “suddenly” and “unexpected.” Furthermore, they could not accept that they had such an illness and were curious about the cause of the disease and its risk.
(Patient 1) At the beginning, I really could not accept the fact that I was ill [.]. Of course, this disease is incurable, and it is really unacceptable [.]. I really want to know the cause of this disease.
(Patient 5) I bumped into my electric bike and bled, and the blood did not seem to clot. After the blood test, I found that my blood index was very low. Later, I was hospitalized and diagnosed with aplastic anemia. I occasionally felt dizzy while I squatted and stood up sometimes. I wondered if it might be the common phenomenon of anemia like many women had and did not think of this kind of thing (aplastic anemia).
Life-Threatening
Patients believed that aplastic anemia was difficult to control, life-threatening, and susceptible to some fatal complications, so they had a negative attitude toward the prognosis. Additionally, their enthusiasm for treating the disease was poor, and the behavior of taking medicine was a helpless choice.
(Patient 2) Generally speaking, it is not serious if the platelet level is over 20,000 (=20×109/L). In contrast, if the platelet level is under 20,000 (=20×109/L), the risk is very high. I am afraid of intracranial hemorrhage and visceral hemorrhage. Bleeding is very dangerous to live.
(Patient 12) It is a dead end (voice trembling) [.]. Many patients died. No wonder [.]. It is unrealistic to recover from the disease, 1% survival rate at most. But I have no options besides taking medicine.
Effect on Personal and Family Life
Many participants used “pain” to describe the impact of aplastic anemia; some asked for help from doctors everywhere, and some had experienced protective isolation. They suffered from physical discomfort and were disturbed in daily life and work. Moreover, their families faced a heavy care burden.
(Patient 3) Later, I might get a bacterial infection or something like this, and I fainted. They used a plastic tent to protect me, and something was released inside. Then, I could not even move around in the room and was stuck in bed for about 50 days. I received an infusion for 24 h long every day and never stopped.
(Patient 4) My previous lifestyle was not like this, and now I cannot go to work anymore, which increases the burden on my family.
(Patient 13) The doctor suggested I go to a high-level hospital for further diagnosis. We went to the A Hospital for a checkup. Later, we went to B Hospital, um [.] I was diagnosed there, and after the diagnosis, we went to C Hospital [.]. After the diagnosis, we confirmed that it was aplastic anemia.
(Patient 15) Last year, the platelets kept falling and kept falling, um [.] it is necessary to rely on platelet and red blood cell transfusion for a long time to maintain life. It’s even better to die than to live in such pain.
Perceived Benefits and Barriers of Taking Prescribed Medicines
Understanding of Prescribed Medications
The education level of patients with aplastic anemia affected their ability to acquire knowledge on medications. Additionally, patients with low educational levels often did not take the initiative to learn about medications. Moreso, concise and reliable sources of medication information were lacking. Although the online query is convenient, the information is not universally reliable. Some patients also read the medication labels, which are often too technical and difficult to understand. As a result, patients did not know enough about the medications. Furthermore, some patients believed doctors played a dominant role in their treatment, and their knowledge of medications would not affect their treatment plan. Thus, there was no need to understand the medication.
(Patient 3) I cannot understand some contents, especially stuff like this (medication instructions), which is as thick as a small book.
(Patient 7) I often search (for medication-related information) online using my mobile phone.
(Patient 11) I do not know what medications they prescribed to me and what effects they have. I am not going to find out because what I know is useless. You have to follow the doctor’s instructions when suffering from such a serious illness.
Life-Saving
Basically, patients could recognize the benefits of medication therapy and believed that maintaining life and controlling the condition were inseparable from medication therapies.
(Patient 2) You must take medications. That’s it. To control aplastic anemia, you have to follow the doctor and treatment.
(Patient 4) I think my medication adherence is good. If I do not take medicine, I will die.
(Patient 8) Medication is effective in controlling the condition.
Perceived Barriers
Medications for treating aplastic anemia in China mainly include immunosuppressants and androgens, which have certain toxic and side effects. Another experience of female patients was that the use of androgens had more side effects in women than in men.
(Patient 14) Taking androgens caused a lot of black hair on my face, and I was off for a while because of my wedding.
(Patient 5) These are hormone medications. For women, menstruation will be disordered or even never come again, but for men, it’s not a problem because this is an androgen.
(Patient 10) These medicines have side effects and are not good for the liver and kidneys. I have to check my liver and kidney function every few months.
Aplastic anemia has a long course; medication treatment also emphasizes a long course and slow dose reduction. Therefore, patients felt that medications acted slowly, and the condition reoccurred frequently. They expressed their most concern about the onset time of medications. Some patients also had a negative attitude toward this.
(Patient 12) I do not get any better after taking medicine. It is not very effective, and the condition goes back and forth. I do not know if I should continue with the treatment.
(Patient 14) I am mostly concerned about when the medication will take effect and whether the condition has improved.
In addition, some medications are expensive and not fully covered by medical insurance, which increases the financial burden of patients and impacts medication adherence.
(Patient 11) The price of this medication is extremely high, even higher than opium (a metaphor, not reality). Sometimes I have insufficient money to buy medications, so I quit taking medicine for days, then borrow money and buy medicine immediately.
Cues to Action
Living is More Important Than Everything
Patients’ inner fear of death and desire for life make them take medicine.
(Patient 6) I dare not skip taking medicine. I must take it, even if I become a man. I do not care [.]. If I do not take medicine. I am afraid of getting worse.
(Patient 8) When you are sick, you must take (medicine). I took a handful of them, but I still took them. No way out. If you cannot stand the trouble, do not treat the illness.
Health Care Providers Opinion
The physician’s recommendations and requirements are the primary external clues to patients’ medication behavior.
(Patient 10) I insist on taking medicine. The doctor said that the process could not be terminated, and he also used real cases to tell me that if I did not follow the treatment, there would be serious consequences.
(Patient 4) I only followed the words that the doctor told me. He always helped me timely when I encountered discomfort and doubts during treatment. If my doctor told me to stop the medicine, I would stop it. If not, I would keep taking it.
Self-Efficacy
Persistence Has Hopes
Medical treatment is directly linked to life. Participants believed taking medication was necessary, and they thought it possible to control or cure the disease through persistence.
(Patient 1) The doctor told me that it was not cancer. I was very happy and felt there was hope.
(Patient 6) Taking the medications for so many years has had no obvious effect, but I still insist on taking them. If not, there is no hope. There may be miracles if I do it.
Persistence is Not Difficult
Patients believed that it was not difficult to insist on taking medication. Some patients had already developed a habit of taking the medication without supervision, and the medication time was also strictly followed. Thus, they had confidence in their good medication behavior.
(Patient 4) The matter (remember to take medications) is not difficult. I am used to doing it. As soon as I eat meals, I remember to take my medications.
(Patient 9) I take medications very regularly, at 8 o’clock in the morning, 8 o’clock in the evening. This is very important.
Modifying Factors
Forgetfulness
Some interviewees said that they had missed medication due to forgetfulness.
(Patient 7) The main reason for missing medication is my poor memory, especially after the diagnosis of this disease. In addition, I am 69 years old, and my memory will decline.
Daily Routine
Some patients forgot to take the medication on time due to their daily routines and then took it afterward.
(Patient 13) Winter times now make people easy to oversleep. When I woke up, I found that medication time had passed, and then I took the medication immediately.
Discussion
Although numerous studies have used the theoretical framework of the HBM to understand health behaviors,25–27 this study is the first to apply this framework to patients with aplastic anemia to explore their perceptions and experiences in taking prescribed medicines. Notably, our findings indicate that the HBM provides a structured method to guide data collection and analysis and helps us understand patients’ perceptions and experiences.
Understanding of the Disease and Medications
This study found that patients with aplastic anemia had an inadequate understanding of the disease and prescribed medicines, which affected the patient’s determination to overcome the disease and treatment adherence. One reason is the lack of appropriate information sources. As a rare disease,28 aplastic anemia is not well-known to the public. There is little disease and treatment information available to patients. Notably, the education level of most patients in our study was senior high school and below. Their ability to seek information is limited. We also found that the main information sources were the Internet and medication labels, which failed to meet patients’ needs. A previous study,29 consistent with the results of this study, pointed out that written information often lacks the necessary details of how medications work, especially the nature of the benefits, concerns about the risks, and side effects have hardly been resolved. Informal channels, including the internet, are also ineffective in alleviating worries and solving problems.29 Therefore, providing appropriate educational material and enhancing the guiding role of medical staff is crucial. Another reason for low awareness was that the patients believed disease management was the doctors’ business. In our study, patients had a passive attitude toward understanding medications. This finding corresponds to individuals using methotrexate who adopt avoidance strategies for medication information.29 However, compared with information evasion, information seeking can help suppress disharmony by reducing uncertainty and pressure.30 Another interview explained that occasionally the physicians are too authoritative,31 which may cause patients to lose their sense of responsibility for self-management. Therefore, healthcare providers should strive to establish an equal relationship with patients with a guiding attitude, enabling them to proactively improve the information literacy required for good disease self-management and medication adherence.
Trade-off Between the Pros and Cons
Compared with previous studies on patients with other chronic medical problems reporting intentional reduction or cessation of medications,32,33 the patients in our study showed a stronger willingness to adhere to the medication due to the advantages outweighing the disadvantages of taking the prescribed medicines. The serious consequences of aplastic anemia and its unpredictable course contributed to patients’ perceived susceptibility and severity, belonging to a perceived threat in HBM. Notably, they entailed the hope of not becoming sicker than they were already experiencing. Therefore, patients created subjective beliefs about carrying out required treatments for better health. Still, these perceived threats also posed a risk for non-compliance, as patients were more likely to give up curing disease. In addition to the perceived threat, the perceived benefits and barriers of the prescribed medications are strong predictors of behavior.34 Although a number of new approaches are being tested to meet the needs of patients with aplastic anemia, patients who are not candidates for transplant and patients with the non-severe forms, and those who are economically disadvantaged often receive non-transplant medical interventions.35,36 This study showed that participants knew the benefit of excellent medication adherence. The enhancement of awareness of these benefits increased the willingness of patients to follow doctors’ prescriptions and prompted them to form good behavior in compliance with the medication. On the contrary, the higher the level of perceived barriers, the lower the willingness of patients to behave well. These findings are consistent with previous studies.37,38 Others also have found that many patients cannot adhere to prescriptions due to medication toxicity and side effects, inconspicuous effects, the high cost of medications, and incomplete health insurance,39–41 consistent with the results of our study. In treating aplastic anemia, self-paid medications account for a relatively high proportion. Some patients discontinued treatment due to unaffordable costs, which is considered the most common barrier to successful adherence in many studies.42,43 This finding suggests that Chinese authorities should appropriately expand the medical insurance coverage of aplastic anemia medications and reduce patients’ out-of-pocket expenditures. According to Kassavou and Sutton,44 the underlying affective state associated with the medication is vital to motivate continuous compliance. Therefore, we should respond to patients’ perceptions of disease and medication and help them deal with the barriers that they encounter by performing interventions such as physician–nurse–pharmacist collaborative management and clarification of feeling≠actual state and setting achievable goals.31,44,45
Cues to Action
The desire of patients with aplastic anemia to live was the primary intrinsic motivation for their insistence on taking medication. A previous study has identified that individual’s perceptions relate to how important they regard health,46 indicating that the desire to live not only contributes to healthy behaviors directly but also affects patients’ cognition and perceptions of diseases and treatments, which are life-threatening and life-saving, respectively. Additionally, the advice and requirements from health professionals, especially physicians, provided aplastic anemia patients with external motivators and strengthened their determination to persist in treatment. This finding is consistent with previous research,47 which reported that medical advice is an essential motivator for active behavior.
Self-Efficacy
Self-efficacy is a component of Bandura’s social cognition theory and defined as an individual’s conjecture or judgment about the ability to perform a behavior, which was later added to the HBM.48 Self-efficacy is pivotal in HBM and is the most critical factor in determining behavior. In our study, patients with aplastic anemia expressed their expectations for the control of the illness, and the fact that they were capable of compliance in practice made them optimistic and confident in persisting with the treatment. This is because people with strong self-efficacy see complex tasks as challenges to overcome rather than threats to avoid.49 Although perceptions of susceptibility and severity made participants knowledgeable and aware of the costs of non-adherence, the awareness of the benefits and barriers of adherence and the confidence and determination to overcome difficulties allowed them to integrate this knowledge into action.
Modifying Factors
The medication-taking behaviors of patients with aplastic anemia were affected by daily routine and forgetfulness, which suggested that attention should be paid to reducing objective obstacles whilst improving patients’ willingness to comply subjectively. Daily routine and forgetfulness are causes of non-compliance outside patients’ consciousness, named non-intentional non-adherence (NINA).44 The interview study in the U.K,44 also identified the coping strategies of nurses and patients with NINA: adding reminders in their environment and linking medications with existing habits, such as placing tablets next to the toothbrush in the morning and the glass of water they drink before going to bed. In addition, a systematic review found that automatic telephone-based intervention can double medication adherence compared with conventional treatment by using automated interactive voice response.50 Thus, these studies provide references for intervening non-adherence caused by non-subjective factors.
Limitations
This study has some noted limitations. Firstly, though we adopted a purposive sampling to cover as various backgrounds of aplastic anemia patients as possible, the participants seemed underrepresented in the current study. Most participants in our study were married females treated at a single centre, with similar educational backgrounds, a longer disease course, and who expressed high medication adherence. More interviews with non-adherent and diverse demographic traits would help gain a better understanding of the patients’ perceptions and experiences. Secondly, the participants were mainly hospitalized patients recruited in one tertiary hospital. The extrapolation of the research results was limited because outpatients were in a home care environment, and their medication adherence was considered more challenging. Finally, the HBM has certain limitations. It mainly discusses and analyzes the influencing factors of behavior from a subjective level, but they are multifaceted. To fully grasp the formation mechanism of behavior, multiple theoretical models from all aspects should be combined to explore the influencing factors of behavior comprehensively.
Conclusion and Implications
This study conducted face-to-face and semi-structured interviews with 15 aplastic anemia patients to analyze their views and feelings about medication treatment. The findings indicated that medication-taking behaviors of patients with aplastic anemia are influenced by various factors, including patients’ understanding of the disease and medications, trade-off between the pros and cons, desire and confidence to live, health care providers’ opinion, and forgetfulness. These results offer valuable insights for targeted medication management strategies. Enhancing patients’ health literacy through appropriate education and addressing physical and psychosocial barriers they encounter is crucial. However, this study has certain limitations. Thus, further research is needed to explore the influence of the living environment on the perceptions and experiences of patients with aplastic anemia. Notably, the results of this research should also be supplemented by discussing the mechanism of medication adherence willingness and behavior and developing quantitative measurement tools in future studies. Additionally, considering the dynamic landscape of research in this field, it is recommended that future studies encompass more descriptive investigations and systematic reviews.
Acknowledgment
We would like to thank all the participants who participated and shared their experiences in this study. The authors thank AiMi Academic Services (www.aimieditor.com) for English language editing and review services.
Funding
This work was supported by the Research Project of Zhejiang Chinese Medical University [NO. 2020SZ02] and a provincial health technology plan [NO. 2022RC216]. The funders had no role in the study design, data collection, analysis, publication decision, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Solimando AG, Palumbo C, Pragnell MV, Bittrich M, Argentiero A, Krebs M. Aplastic anemia as a roadmap for bone marrow failure: an overview and a clinical workflow. Int J Mol Sci. 2022;23(19):11765. doi:10.3390/ijms231911765
2. Ahmed P, Chaudhry QUN, Satti TM, et al. Epidemiology of aplastic anemia: a study of 1324 cases. Hematology. 2020;25(1):48–54. doi:10.1080/16078454.2019.1711344
3. Kuang YM, Zhu Y, Gao RL, et al. Clinical study of pai-neng-da capsule in the treatment of chronic aplastic anemia. Chin J Integr Med. 2016;22(2):124–129. doi:10.1007/s11655-015-2158-6
4. Gavriilaki E, Tragiannidis A, Papathanasiou M, et al. Aplastic anemia and paroxysmal nocturnal hemoglobinuria in children and adults in two centers of Northern Greece. Front Oncol. 2022;12:947410. doi:10.3389/fonc.2022.947410
5. Pan P, Chen C, Hong J, Gu Y. Autoimmune pathogenesis, immunosuppressive therapy and pharmacological mechanism in aplastic anemia. Int Immunopharmacol. 2023;117:110036. doi:10.1016/j.intimp.2023.110036
6. Murphy CC, Lee SJC, Gerber DE, Cox JV, Fullington HM, Higashi RT. Patient and provider perspectives on delivery of oral cancer therapies. Patient Educ Couns. 2019;102(11):2102–2109. doi:10.1016/j.pec.2019.06.019
7. Bänziger S, Weisshaar K, Arokoski R, et al. Feasibility of electronic patient-reported outcome monitoring and self-management program in aplastic anemia and paroxysmal nocturnal hemoglobinuria-a pilot study (ePRO-AA-PNH). Ann Hematol. 2023;102(1):199–208. doi:10.1007/s00277-022-05012-5
8. Shen W, Liu X, Zhou A. Analysis of continuous nursing intervention on aplastic anemia patients based on the “information-motivation-behavioral skills model”. Evid Based Complement Alternat Med. 2021;8204522. doi:10.1155/2021/8204522
9. Upamali S, Rathnayake S. Perspectives of older people with uncontrolled type 2 diabetes mellitus towards medication adherence: a qualitative study. PLoS One. 2023;18(8):e0289834. doi:10.1371/journal.pone.0289834
10. Dashputre AA, Gatwood KS, Gatwood J. Medication adherence, health care utilization, and costs among patients initiating oral oncolytics for multiple myeloma or chronic lymphocytic leukemia/small lymphocytic lymphoma. Manag Care Spec Pharm. 2020;26(2):186–196. doi:10.18553/jmcp.2020.26.2.186
11. Zhou H, Wang X, Yu D, et al. Adherence to oral targeted anti-lung cancer therapy: a qualitative interview study. Patient Prefer Adherence. 2022;16:995–1004. doi:10.2147/PPA.S341966
12. Fang M, Song H, Zhang J, Li S, Shen D, Tang Y. Efficacy and safety of immunosuppressive therapy with or without eltrombopag in pediatric patients with acquired aplastic anemia: a Chinese retrospective study. Pediatr Hematol Oncol. 2021;38(7):633–646. doi:10.1080/08880018.2021.1895924
13. Escalante CP, Chisolm S, Song J, et al. Fatigue, symptom burden, and health-related quality of life in patients with myelodysplastic syndrome, aplastic anemia, and paroxysmal nocturnal hemoglobinuria. Cancer Med. 2019;8(2):543–553. doi:10.1002/cam4.1953
14. Janz NK, Becker MH. The Health Belief Model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
15. Ge P, Liu S-T, Xu S-X, et al. The influence of parents on medication adherence of their children in China: a cross-sectional online investigation based on health belief model. Front Public Health. 2022;10:845032. doi:10.3389/fpubh.2022.845032
16. Hobani F, Alhalal E. Factors related to parents’ adherence to childhood immunization. BMC Public Health. 2022;22(1):819. doi:10.1186/s12889-022-13232-7
17. Limbu YB, Gautam RK, Pham L. The health belief model applied to COVID-19 vaccine hesitancy: a systematic review. Vaccines. 2022;10(6):973. doi:10.3390/vaccines10060973
18. Sazali MF, Rahim S, Mohammad AH, et al. Improving tuberculosis medication adherence: the potential of integrating digital technology and health belief model. Tuberc Respir Dis. 2023;86(2):82–93. doi:10.4046/trd.2022.0148
19. Doyle L, McCabe C, Keogh B, Brady A, McCann M. An overview of the qualitative descriptive design within nursing research. J Res Nurs. 2020;25(5):443–455. doi:10.1177/1744987119880234
20. Red Blood Cell Disease (Anemia) Group, Chinese Society of Hematology, Chinese Medical Association. Chinese expert consensus on the diagnosis and treatment of aplastic anemia. Chin J Hematol. 2017;38(1):1–5. doi:10.3760/cma.j.issn.0253-2727.2017.01.001
21. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
22. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
23. Bowen GA. Naturalistic inquiry and the saturation concept: a research note. Qual Res. 2008;8(1):137–152. doi:10.1177/1468794107085301
24. Holloway I, Galvin K. Qualitative Research in Nursing and Healthcare.
25. Avancini A, Tregnago D, Rigatti L, et al. Factors influencing physical activity in cancer patients during oncological treatments: a qualitative study. Integr Cancer Ther. 2020;19:1534735420971365. doi:10.1177/1534735420971365
26. Myers SL, Siegel EO, Hyson DA, Bidwell JT. A qualitative study exploring the perceptions and motivations of patients with heart failure who transitioned from non-adherence to adherence. Heart Lung. 2020;49(6):817–823. doi:10.1016/j.hrtlng.2020.09.010
27. Yu B, Zhou J, Gong Y, et al. Self-efficacy mediates perceived benefits and barriers of adherence of heroin-dependent patients to methadone for addiction treatment: a health belief model study. J Addict Med. 2020;14(4):e110–e117. doi:10.1097/ADM.0000000000000640
28. Yeung C, Relke N, Good D, Satkunam N, Mates M. Antithymocyte globulin for aplastic anemia secondary to pembrolizumab: a case report and review of literature. Immunotherapy. 2023;15(5):323–333. doi:10.2217/imt-2022-0210
29. Hayden C, Neame R, Tarrant C. Patients’ adherence-related beliefs about methotrexate: a qualitative study of the role of written patient information. BMJ Open. 2015;5(5):e006918. doi:10.1136/bmjopen-2014-006918
30. Yang C, Lee DTF, Chair SY. Validation and adaption of an information-motivation-behavioral skills model of medication adherence in older patients with multimorbidity. Patient Educ Couns. 2023;113:107756. doi:10.1016/j.pec.2023.107756
31. Leung J, Baker EA, Kim AHJ. Exploring intentional medication non-adherence in patients with systemic lupus erythematosus: the role of physician-patient interactions. Rheumatol Adv Pract. 2021;5(1):rkaa078. doi:10.1093/rap/rkaa078
32. Doya IF, Yahaya JJ, Ngaiza AI, Bintabara D. Low medication adherence and its associated factors among patients with type 2 diabetes mellitus attending Amana Hospital in Dar es Salaam, Tanzania: a cross-sectional study. Int Health. 2023;ihad042. doi:10.1093/inthealth/ihad042
33. Milkias H, Yewhalaw D, Abebe G. High non-compliance rate among presumptive tuberculosis cases referred from peripheral health facilities in silti district of Southern Ethiopia: a mixed methods study. Arch Public Health. 2023;81(1):50. doi:10.1186/s13690-023-01071-w
34. Sousa H, Ribeiro O, Christensen AJ, Figueiredo D. Mapping patients’ perceived facilitators and barriers to in-center hemodialysis attendance to the health belief model: insights from a qualitative study. Int J Behav Med. 2023;30(1):97–107. doi:10.1007/s12529-022-10075-9
35. Nassani M, Fakih RE, Passweg J, et al. The role of androgen therapy in acquired aplastic anemia and other bone marrow failure syndromes. Front Oncol. 2023;13:1135160. doi:10.3389/fonc.2023.1135160
36. Nakamura R, Patel BA, Kim S, et al. Conditional survival and standardized mortality ratios of patients with severe aplastic anemia surviving at least one year after hematopoietic cell transplantation or immunosuppressive therapy. Haematologica. 2023. doi:10.3324/haematol.2023.282781
37. Bond GG, Aiken LS, Somerville SC. The health belief model and adolescents with insulin-dependent diabetes mellitus. Health Psychol. 1992;11(3):190–198. doi:10.1037/0278-6133.11.3.190
38. Palardy N, Greening L, Ott J, Holderby A, Atchison J. Adolescents’ health attitudes and adherence to treatment for insulin-dependent diabetes mellitus. J Dev Behav Pediatr. 1998;19(1):31–37. doi:10.1097/00004703-199802000-00005
39. Lasseter G, Al-Janabi H, Trotter CL, Carroll FE, Christensen H. Understanding the role of peace of mind in childhood vaccination: a qualitative study with members of the general public. Vaccine. 2020;38(10):2424–2432. doi:10.1016/j.vaccine.2019.12.009
40. Wang H, He G, Jia J, et al. Efficacy and safety of avatrombopag in aplastic anemia patients with liver disease. J Transl Int Med. 2023;11(1):90–93. doi:10.2478/jtim-2023-0006
41. Hing M, Hoffman RM, Seleman J, Chibwana F, Kahn D, Moucheraud C. ‘Blood pressure can kill you tomorrow, but HIV gives you time’: illness perceptions and treatment experiences among Malawian individuals living with HIV and hypertension. Health Policy Plan. 2019;34(Suppl 2):ii36–ii44. doi:10.1093/heapol/czz112
42. Aremu TO, Oluwole OE, Adeyinka KO, Schommer JC. Medication adherence and compliance: recipe for improving patient outcomes. Pharmacy. 2022;10(5):106. doi:10.3390/pharmacy10050106
43. Karaca-Mandic P, Solid CA, Armer JM, Skoracki R, Campione E, Rockson SG. Lymphedema self-care: economic cost savings and opportunities to improve adherence. Cost Eff Resour Alloc. 2023;21(1):47. doi:10.1186/s12962-023-00455-7
44. Kassavou A, Sutton S. Reasons for non-adherence to cardiometabolic medications, and acceptability of an interactive voice response intervention in patients with hypertension and type 2 diabetes in primary care: a qualitative study. BMJ Open. 2017;7(8):e015597. doi:10.1136/bmjopen-2016-015597
45. Wu XY, Sun L, Xia MJ, Zhang J, He XW. Physician-nurse-pharmacist collaborative management for cancer pain. J Nurs Sci. 2018;33(21):34–35+42.
46. Williams A, Manias E. Exploring motivation and confidence in taking prescribed medicines in coexisting diseases: a qualitative study. J Clin Nurs. 2014;23(3–4):471–481. doi:10.1111/jocn.12171
47. Prusiński T. When does doctor’s recommendation become patient’s resolution? The regulatory potential of procedural justice in the context of compliance with medical advice and the treatment process. Front Med. 2023;10:1004994. doi:10.3389/fmed.2023.1004994
48. Strecher VJ, DeVellis BM, Becker MH, Rosenstock IM. The role of self-efficacy in achieving health behavior change. Health Educ Q. 1986;13(1):73–92. doi:10.1177/109019818601300108
49. Hanna A, Yael EM, Hadassa L, et al. ``It’s up to me with a little support” - Adherence after myocardial infarction: a qualitative study. Int J Nurs Stud. 2020;101:103416. doi:10.1016/j.ijnurstu.2019.103416
50. Kassavou A, Sutton S. Automated telecommunication interventions to promote adherence to cardio-metabolic medications: meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychol Rev. 2018;12(1):25–42. doi:10.1080/17437199.2017.1365617
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Patients’ Psychological Contract with Pharmacists on Medication Adherence: A Qualitative Study
Gu Y, Mu X, Zhang Y, Tang Y, Zhang T, Tang F
Patient Preference and Adherence 2023, 17:547-555
Published Date: 3 March 2023
Improving Assessment of Adherence Behaviors and Drivers: Targeted Literature Review and Concept Elicitation Interviews in Multiple Countries and Disease Populations
Bentley S, Exall E, Morgan L, Roche N, Khunti K, Rossom R, Piercy J, Arbuckle R, Higgins VS
Patient Preference and Adherence 2024, 18:1231-1242
Published Date: 17 June 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Understanding the Experiences of Women with Gestational Diabetes in Singapore: A Qualitative Study
Lazarus MA, Lee VV, Ong DLS, Yew TW, Shorey S, Young D, Eriksson JG
International Journal of Women's Health 2025, 17:1711-1724
Published Date: 8 June 2025
“I Probably Am Being a Naughty Boy, But…” Reasons for Non-Adherence to Prescribed Medication, as Perceived by People Living with Inflammatory Bowel Disease: A Qualitative Study

King K, Norton C, Jammeh A, Chalder T, Czuber-Dochan W
Patient Preference and Adherence 2025, 19:2391-2415
Published Date: 12 August 2025