Back to Journals » Clinical Epidemiology » Volume 18
The Danish Database for Hepatitis B and C (DANHEP): A Nationwide, Prospective, Ongoing Cohort Study
Authors Bollerup S ![]() , Sølund C, Hallager S, Jespersen S
, Sølund C, Hallager S, Jespersen S ![]() , Balslev U, Andersen ES, Pedersen J, Winckelmann A, Barfod TS, Clausen MR
, Balslev U, Andersen ES, Pedersen J, Winckelmann A, Barfod TS, Clausen MR ![]() , Omland LH
, Omland LH ![]() , Hobolth L, Madsen LG
, Hobolth L, Madsen LG ![]() , Leth S
, Leth S ![]() , Mygind LH, Rasmussen TA, Laursen AL, Svensgaard S, Røge B, Tarp B
, Mygind LH, Rasmussen TA, Laursen AL, Svensgaard S, Røge B, Tarp B ![]() , Thielsen P, Bukh J, Øvrehus A, Christensen PB
, Thielsen P, Bukh J, Øvrehus A, Christensen PB ![]() , Krarup H
, Krarup H ![]() , Weis N
, Weis N ![]()
Received 12 August 2025
Accepted for publication 9 April 2026
Published 4 June 2026 Volume 2026:18 557020
DOI https://doi.org/10.2147/CLEP.S557020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Signe Bollerup,1 Christina Sølund,1 Sofie Hallager,1 Sofie Jespersen,1 Ulla Balslev,2 Ellen Sloth Andersen,2 Jannie Pedersen,2,3 Anni Winckelmann,1 Toke S Barfod,4,5 Mette Rye Clausen,6 Lars Haukali Omland,5,7,8 Lise Hobolth,9 Lone Galmstrup Madsen,10 Steffen Leth,11,12 Lone Hagens Mygind,13,14 Thomas A Rasmussen,15 Alex Lund Laursen,15 Siri Svensgaard,15 Birgit Røge,16 Britta Tarp,17 Peter Thielsen,18 Jens Bukh,19,20 Anne Øvrehus,3 Peer Brehm Christensen,3,21 Henrik Krarup,14,22 Nina Weis1,5
1Department of Infectious Diseases; Copenhagen University Hospital, Hvidovre, Denmark; 2Department of Infectious Diseases; Copenhagen University Hospital, Herlev, Denmark; 3Department of Infectious Diseases; Odense University Hospital, Odense, Denmark; 4Department of Infectious Diseases; Zealand University Hospital, Roskilde, Denmark; 5Department of Clinical Medicine; Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 6Department of Digestive Diseases, Transplantation and General Surgery; Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark; 7Department of Infectious Diseases; Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark; 8Department of Bacteria, Parasites & Fungi; Statens Serum Institut, Copenhagen, Denmark; 9Department of Gastroenterology; Copenhagen University Hospital, Hvidovre, Denmark; 10Department of Gastroenterology; Zealand University Hospital, Køge, Denmark; 11Department of Infectious Diseases-Medicine; Regional Hospital Gødstrup, Gødstrup, Denmark; 12Department of Clinical Medicine; Aarhus University, Aarhus, Denmark; 13Department of Infectious Diseases; Aalborg University Hospital, Aalborg, Denmark; 14Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 15Department of Infectious Diseases; Aarhus University Hospital, Aarhus, Denmark; 16Department of Medicine; Kolding Hospital, Kolding, Denmark; 17Medical Diagnostic Center, University Clinic for Innovative Patient Pathways, Regional Hospital Central Jutland, Silkeborg, Denmark; 18Department of Gastroenterology; Copenhagen University Hospital, Herlev, Denmark; 19Copenhagen Hepatitis C Program (CO-HEP); Copenhagen University Hospital, Hvidovre, Denmark; 20Department of Immunology and Microbiology; Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 21Clinical Institute, University of Southern Denmark, Odense, Denmark; 22Department of Clinical Medicine, Aalborg University Hospital, Aalborg, Denmark
Correspondence: Signe Bollerup, Department of Infectious Diseases, Copenhagen University Hospital, Kettegaard Alle 30, Hvidovre, DK 2650, Denmark, Email [email protected]
Introduction: The Danish Database for Chronic Hepatitis B and C (DANHEP) was established in 2002 to support research into the clinical, epidemiological, virological, and immunological aspects of chronic viral hepatitis in Denmark. The objective of this paper is to describe methods of data acquisition, content, completeness and accuracy of data in DANHEP.
Methods: Since 2002 all individuals with chronic viral hepatitis B or C at least 16 years of age, who has presented to a hospital department specialized in infectious diseases or gastroenterology in Denmark, have been enrolled in DANHEP. Information on co-infections, viral DNA/RNA detection, serology, liver parameters, liver fibrosis, treatment initiation, -cessation and -efficacy is manually transferred from electronic patient files and recorded in DANHEP annually. In 2004, a biobank storing annual blood samples was established.
Results: By December 2023 DANHEP stored data on 15,886 individuals with chronic hepatitis B or C and the biobank held approximately 38,180 samples. We verified a random sample of key variables by comparing with electronic patient files and found an error proportion of less than 5%.
Conclusion: DANHEP is well suited for studying the epidemiology, virology and immunology of chronic viral hepatitis. We encourage future collaborations to address the many remaining questions in the field of viral hepatitis.
Keywords: biobank, chronic viral hepatitis, Denmark, database
Introduction
The Danish Database for Hepatitis B and C (DANHEP) was established in 2002, to support research into clinical, epidemiological, virological, and immunological aspects of chronic viral hepatitis in Denmark, a Northern European country with around 6 million inhabitants.
The cohort has over the years provided valuable data for scientific studies on prevalence of chronic viral hepatitis, clinical management, disease progression including translational studies of virus–host interactions, risk factors for complications, treatment efficacy and antiviral resistance in persons with chronic viral hepatitis presenting to hospitals in Denmark. In the coming years, chronic viral hepatitis will continue to be an important area of research. The World Health Organization aims to eliminate viral hepatitis as a public health threat by 2030.1 DANHEP will be useful for tracking progress as well as potential barriers towards elimination in Denmark. DANHEP will also be a valuable resource for research topics like complication risk stratification, predictors of functional cure for chronic hepatitis B (CHB), role of comorbidities and real-world safety and efficacy of novel therapies.
A thorough description of DANHEP has never been published. To aid and encourage utilization of DANHEP the objective of this paper is to describe methods of data acquisition, content, completeness and accuracy of data in DANHEP.
Setting
In 2016, the prevalence of chronic viral hepatitis in Denmark was estimated to be 0.3% for CHB and 0.2% for chronic hepatitis C (CHC), corresponding to 14,500 and 10,000 individuals, respectively.2,3 The majority with CHB in Denmark migrated from areas with higher CHB prevalence. Consequently, the population with CHB in Denmark is diverse in regard to ethnicity as well as hepatitis B virus (HBV) genotypes.4 Due to the variable natural history of CHB, Danish national guidelines recommend that all patients carrying hepatitis B surface antigen (HBsAg) are monitored every 3–12 months.5 Guidelines recommend treatment with entecavir, tenofovir disoproxil or tenofovir alafenamide for individuals with prolonged active hepatitis, family history of hepatocellular carcinoma (HCC), liver cirrhosis, or pregnancy with high viral load. Antiviral treatment is provided free of charge for the individual. Guidelines recommend surveillance for HCC for selected groups.5–7 The majority with CHC in Denmark were exposed through intravenous drug use. The most common hepatitis C virus (HCV) genotypes are 1 and 3. For CHC, direct acting antiviral (DAA) treatment has been available since 2014 and has been provided free of charge for all residents with CHC in Denmark since 2018.8 Danish national guidelines recommend lifelong biannual surveillance for HCC for individuals who have liver cirrhosis before receiving DAA treatment.9,10 Guidelines recommend that chronic viral hepatitis be managed by infectious disease or gastroenterology specialists, who are also the only providers licensed to prescribe antiviral treatment.
Content and Data Collection
DANHEP is a nationwide, observational cohort with ongoing enrollment managed by a team of specialists in infectious diseases or gastroenterology. Table 1 lists the hospital departments that contribute to DANHEP. The database is hosted at Aalborg University Hospital. Each site updates DANHEP annually by manually transferring data from electronic patient files. Data is entered with single entry. When a new patient with chronic viral hepatitis presents to one of the contributing hospital departments, they are asked if they consent to their data being recorded in DANHEP and they fill out a consent form. All patients are also asked if they are willing to contribute blood samples to the DANHEP biobank. If so, a separate consent form is filled out. After the initial visit, a baseline chart is filled out. Hereafter, annual follow-up charts are completed for as long as the participant remains in care. If antiviral treatment is initiated, a treatment chart is filled out. If more than one value for a variable is available for a given year, eg. a laboratory result, the latest value is registered. If data is missing from the electronic patient file, it will be recorded as unknown or missing in DANHEP. Table 2 lists the data stored in DANHEP. At the initial visit a serum and a plasma sample are saved. Hereafter, plasma samples are saved annually. The DANHEP cohort consists of residents in Denmark at least 16 years of age who have chronic viral hepatitis B or C and have had at least one visit to a hospital department specialized in either infectious diseases or gastroenterology since January 1st, 2002. Participants are registered under their 10-digit personal identification number (PIN). The PIN is issued to all individuals born in Denmark or Greenland, individuals with work permits and individuals who legally reside in Denmark for at least 3 months.11 It includes date of birth as well as an indicator of sex. The PIN is used in all public registers and can therefore be used to link data from DANHEP to other national registers.
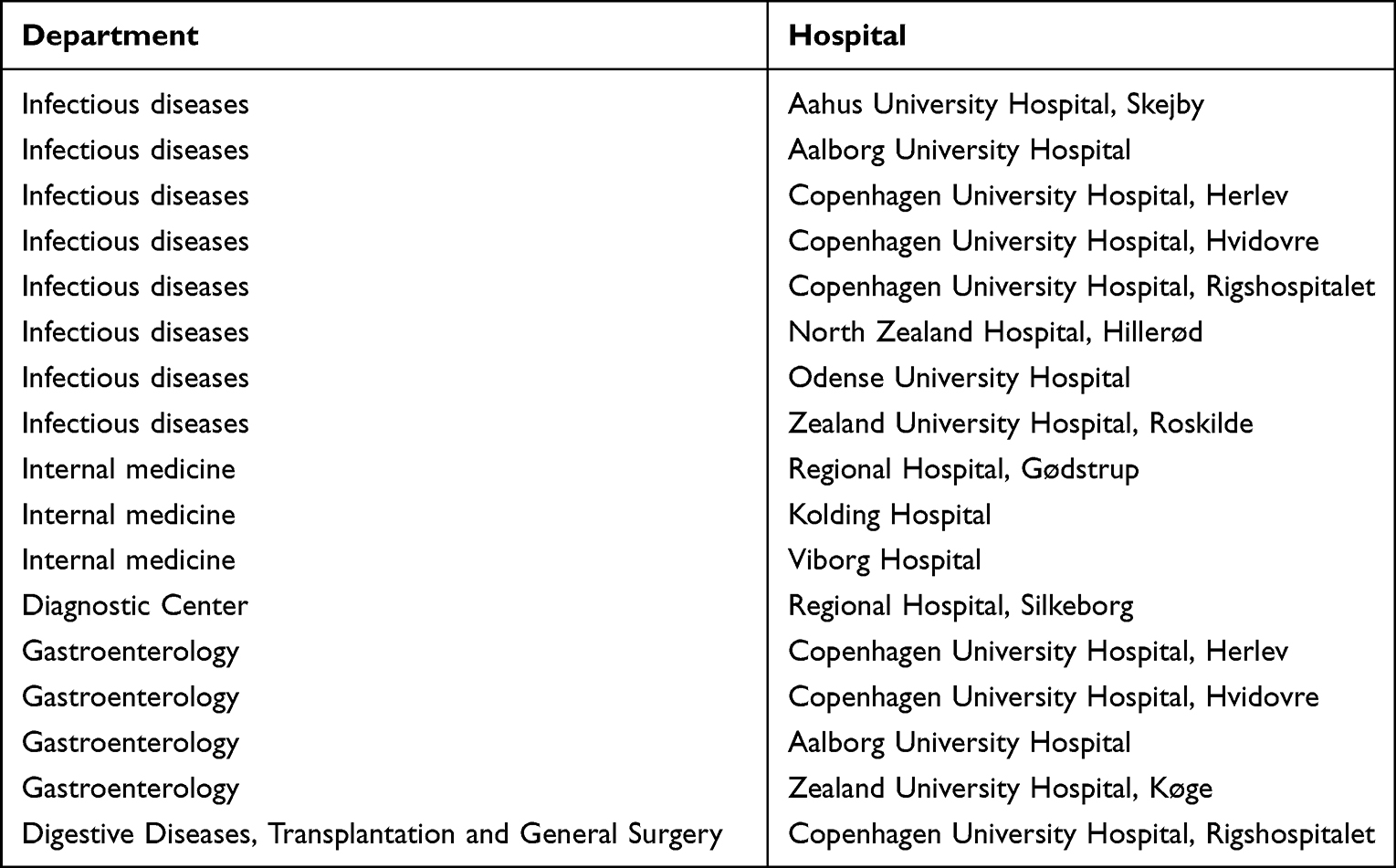 |
Table 1 Hospital Departments That Contribute to The Danish Database for Hepatitis B and C (DANHEP) |
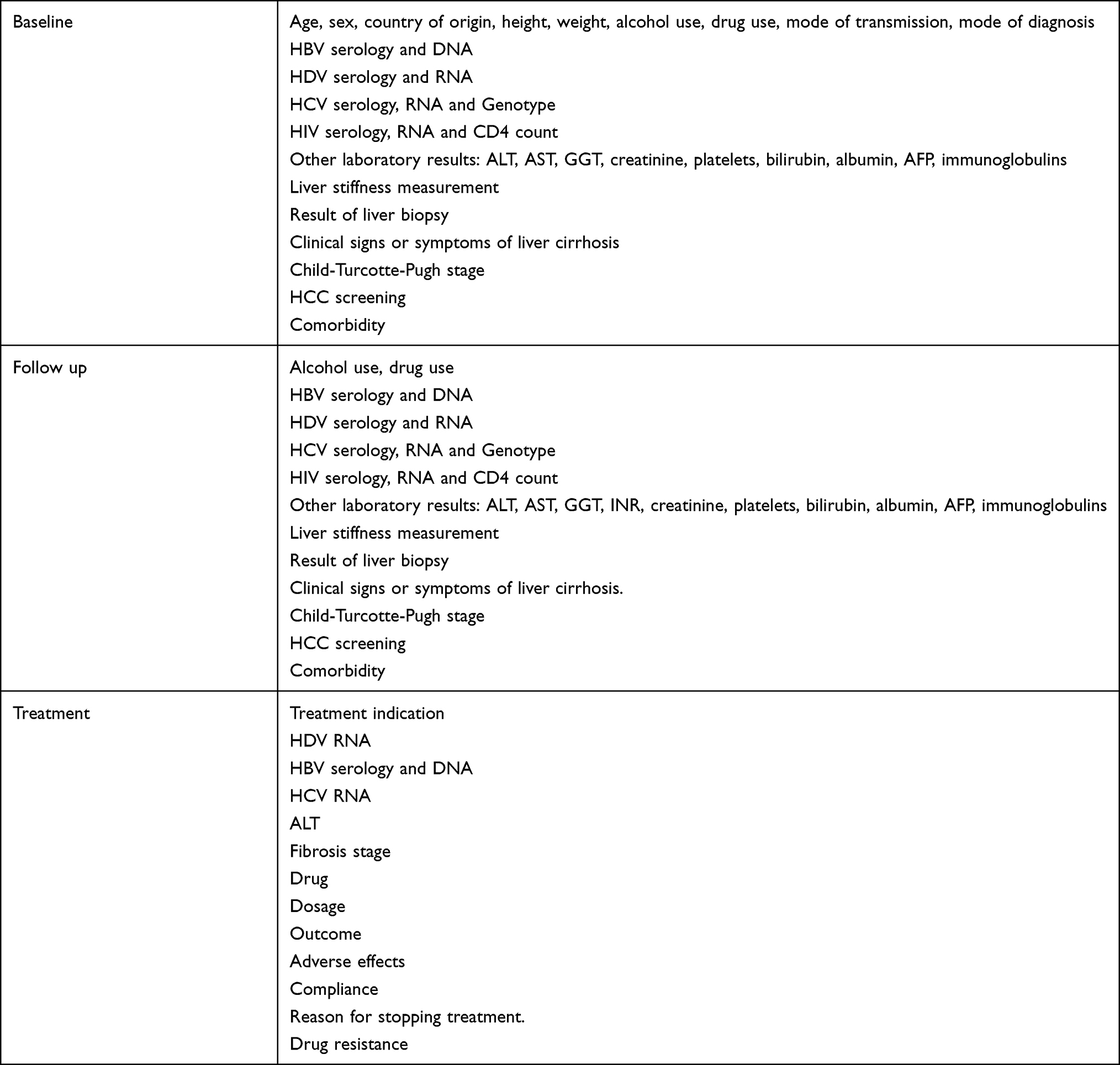 |
Table 2 Data Registered in The Danish Database for Hepatitis B and C (DANHEP) |
Ethical Statement
DANHEP (no. P-2022-352) and the attached biobank (no. P-2021-12) were both approved by the data review center of the Capital Region of Denmark as required by Danish law. Data was accessed, stored and managed in accordance with data protection and privacy regulations. No ethical board approval was required.
Changes to DANHEP Over Time
DANHEP started as a nationwide, clinical quality assurance database in 2002. From 2010 departments in the Western and Eastern parts of Denmark used different systems to record DANHEP data.12 In 2020, the system used by Region Zealand and the Capital Region in Eastern Denmark was discontinued. A new database framework using the Research Electronic Data Capture (REDCap) system hosted on servers in the North Jutland Region was set up and started data collection in 2024. Data from 2020 to 2023 had to be imported hereafter. In the rest of the country, reporting continued unaffected until 2023, when the managing group decided to transfer data to the new REDCap database to reestablish national coverage.13 This process was completed in July 2025. Thus, today all historical DANHEP data from both Western and Eastern Denmark is stored in REDCap, and DANHEP is updated annually. DANHEP changed legal status several times since 2002. The legal status for a database in Denmark has implications for whether participant consent is required. According to Danish law research databases require participant consent while clinical quality assurance databases do not. DANHEP started as a clinical quality assurance database in 2002. In 2013 DANHEP changed status to a research database. From 2017 to 2019 DANHEP was once again a clinical quality assurance database. Since 2019, DANHEP has been a research database requiring written participant consent. The DANHEP biobank has consistently required written participant consent since its establishment.
Cohort Description
We extracted data from 2002 until the end of 2023, which was the last updated year at the time of data extraction. During 2002–2023, 15,886 participants were included in DANHEP, of whom 9552 have CHC, 5868 have CHB and 466 are co-infected. Figure 1 shows the number of participants enrolled per year with CHC and CHB, respectively. Many were enrolled in 2002, as both prevalent and incident cases were included that year. For both CHB and CHC, yearly inclusion increased initially, but since 2015 both have gradually decreased; CHB likely due to decreased immigration from countries with high prevalence because of restrictions to immigration to Denmark, and CHC due to a decrease in incidence.14 Table 3 shows selected baseline characteristics for DANHEP participants. In the CHB group, participants had a median age of 35 years at first visit, 19% were HBeAg positive, and there was an equal distribution of men and women. Participants with CHB had predominantly migrated to Denmark from areas with a high endemic prevalence of HBV, and the most common route of infection was vertical transmission. HBV genotyping is not routinely performed, as it does not influence the choice of nucleos(t)ide analogue for antiviral therapy. A previous study using samples from the DANHEP biobank found that the most common HBV genotype in Denmark was D (46%) followed by C (21%), B (17%) and A (11%).4 In the CHC group, the median age was 45 years at first visit, the majority were male, and 75% were born in Denmark. The most common route of infection was intravenous drug use, and the prevailing genotypes were 1 and 3.
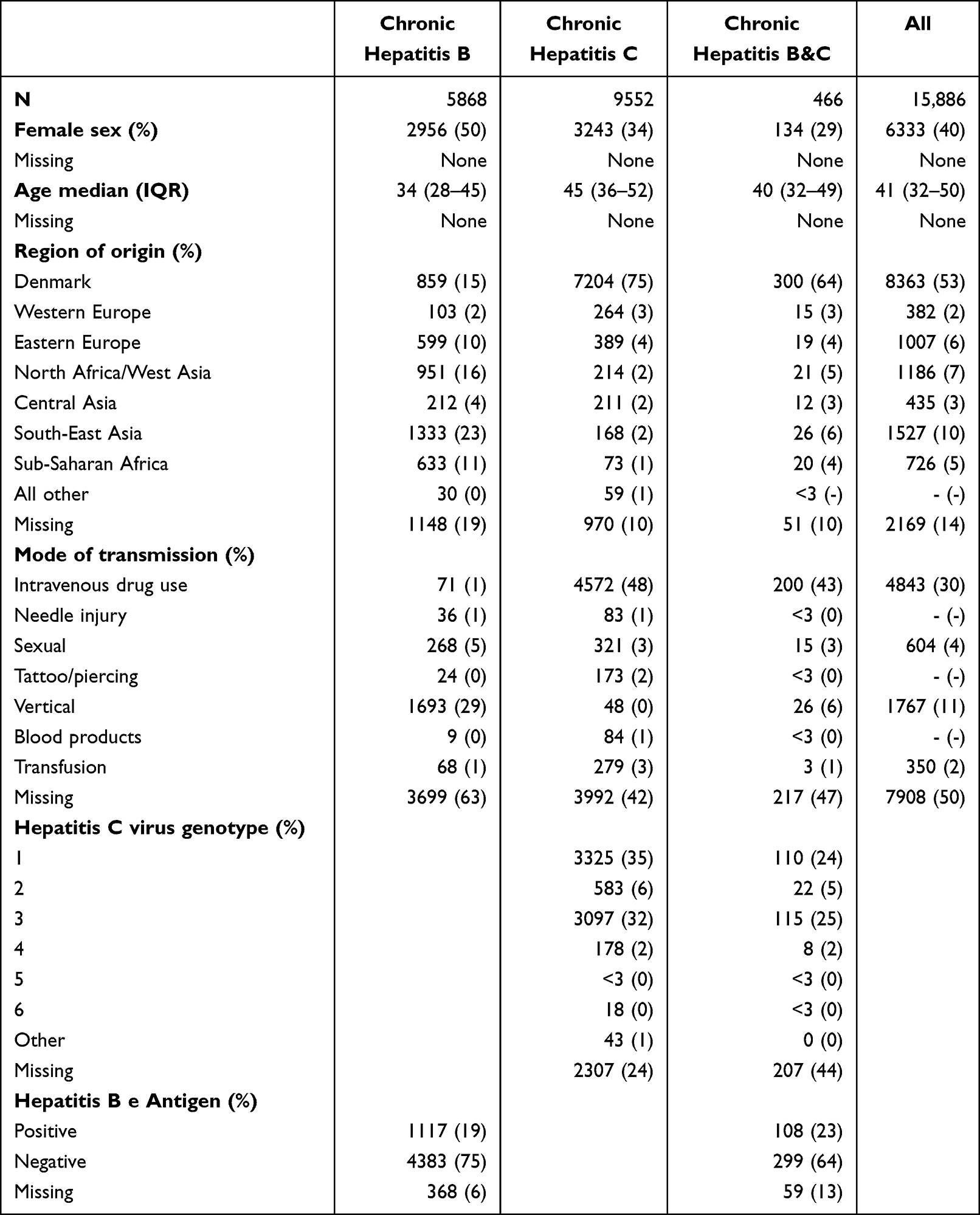 |
Table 3 Characteristics for 15,886 Participants at Inclusion in The Danish Database for Hepatitis B and C (DANHEP) During 2002–2023 |
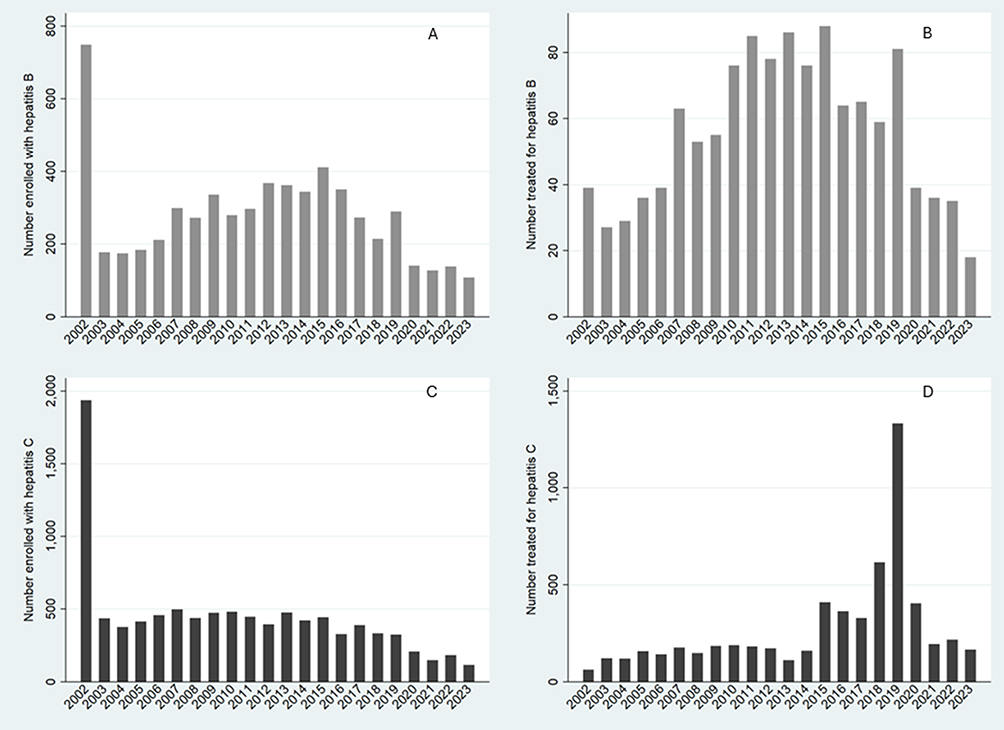 |
Figure 1 Annual enrollment and treatment uptake in the Danish Database for Hepatitis B and C (DANHEP). (A) Individuals with hepatitis B enrolled per year. (B) Number of new hepatitis B treatments per year. (C) Individuals with hepatitis C enrolled per year. (D) Number of new hepatitis C treatments per year. Lack of data input from seven departments in Eastern Denmark from 2020–2023, likely caused the apparent reduction in new hepatitis B/C cases and treatment uptake during this time. |
Since inclusion in DANHEP, 1370 (23%) with CHB and 6386 (66%) participants with CHC have initiated antiviral treatment. Figure 1 shows the number of treatments initiated by year. For CHB, treatment initiation increased since 2007, after nucleos(t)ide analogues with high barrier to resistance were approved. There was a decrease in treatment initiation from 2020. For CHC, treatment initiation peaked in 2019, as treatment was made available free of charge for everyone with CHC in Denmark regardless of liver fibrosis level in November 2018.
The biobank contains 38,180 samples from 9812 individuals.
Completeness and Accuracy
We have previously compared registrations of chronic viral hepatitis in DANHEP with chronic hepatitis diagnoses in the national patient register (NPR) to assess coverage. The NPR records all in- and out-patient hospital visits in Denmark. In 2016, we found that 85% of those who, according to the NPR, had an outpatient visit to a hospital department with CHB as the main diagnosis were registered in DANHEP. However, it has previously been found that the NPR has low positive predictive value for chronic viral hepatitis diagnoses.15 Therefore, we chose to only accept diagnoses of viral hepatitis in the NPR that were also reported to either the communicable diseases register,16 which is a national register that must be notified of all chronic viral hepatitis diagnoses by the diagnosing physicians,2 or had two positive HBsAg measurements recorded in DANVIR, a laboratory register that collects viral hepatitis-specific tests.17 Using this definition, we found that 95% of people with CHB who were linked to specialized care were registered in DANHEP (data not published). Changing consent requirements may also have affected DANHEP coverage. To assess if this is the case, we examined the overlap between DANHEP and the NPR from 2002 to 2019. While NPR diagnoses may lack accuracy, a substantial impact of consent on DANHEP coverage should be reflected in the degree of overlap. We did not include data from 2020 to 2023 as we know that DANHEP is currently incomplete for those years. During 2002–2012, 61% (3686/6040) of individuals with chronic viral hepatitis who were recorded in the NPR were also recorded in DANHEP. During 2013–2016 when consent was required, the overlap was 74% (2299/3120). During 2017–2018 when no consent was required, the overlap was 81% (1163/1443). In 2019, 81% registered in the NPR were recorded in DANHEP. Thus, overlap between DANHEP and the NPR increased over time, seemingly regardless of consent requirements. To test if there was a statistically significant effect of consent requirement, we performed quasi-binomial regression adjusting for calendar year and consent and found no statistically significant effect of consent (p = 0.255).
Of the 16 hospital departments contributing to DANHEP, 7 did not update files in 2020–2023. Consequently, data from 2020 to 2023 are not complete. As an example, only 84% (6326/7541) of all HCV treated individuals in Denmark by the end 2023 are identified in DANHEP (PB. Christensen personal communication). We are currently updating records to include newly enrolled participants and treatments initiated between 2020 and 2023.
Table 3 indicates that data on region of origin are missing for 14% and that only 50% of the cohort has a documented mode of transmission. In contrast, routine blood test results are much more complete: alanine aminotransferase levels are available for 97% of all individuals registered in DANHEP, HBV DNA levels for 93% of those with CHB, and HCV RNA titers for 99% of those with CHC.
To evaluate data accuracy, we selected 7 key variables in DANHEP and randomly chose 50 values for each variable to verify by comparing with electronic patient files. Dates of blood samples were considered correct within a three-month window, as it is the date of consultation and not the date of sample collection that is recorded in DANHEP. We were unable to verify some values due to introduction of new filing systems and excluded them from this account. Table 4 shows that only HBsAg loss had an error proportion >5%. This was due to registration of HBsAg loss in participants with CHC who were always HBsAg negative, and up to two years delayed registrations of HBsAg loss for two participants.
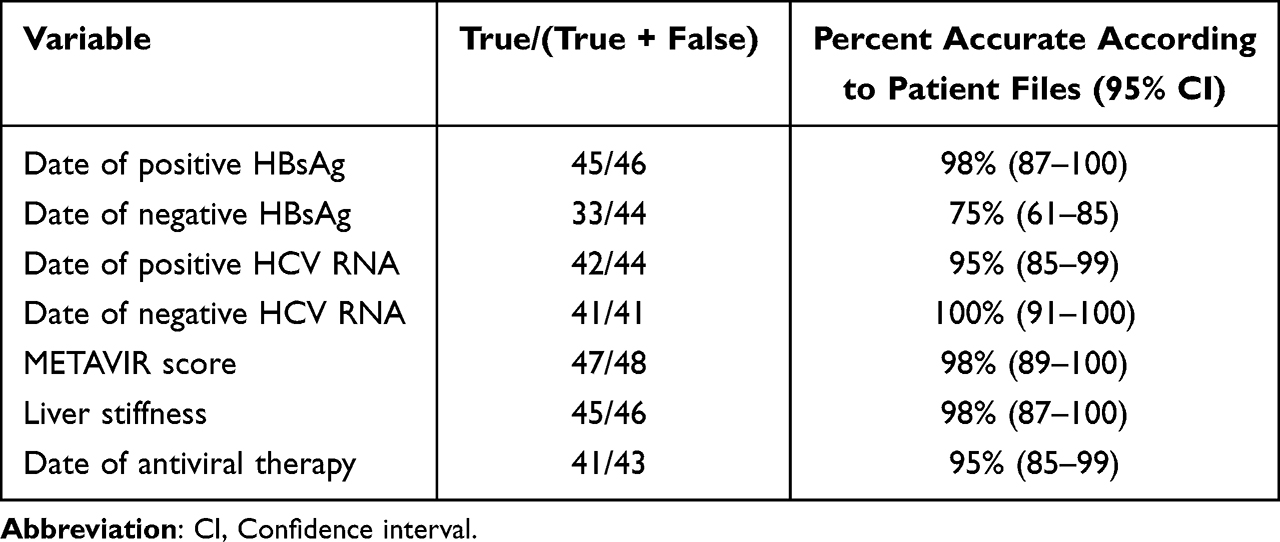 |
Table 4 Accuracy of Key Variables in the Danish Database for Hepatitis B and C (DANHEP) from 2010 to 2023 |
Discussion
This is the first detailed description of DANHEP, a nationwide clinical database and biobank with data and blood samples from 15,886 participants collected prospectively over more than 20 years. All main departments managing chronic viral hepatitis in Denmark report to it. Moreover, registration by PIN allows linkage to other national registers. DANHEP has contributed data to studies on prevalence, long-term outcomes, natural history, barriers to treatment initiation, treatment efficacy and the role of comorbidities in patients with CHB/CHC in Denmark. Moreover, samples from the DANHEP biobank have been used to characterize antiviral resistance, test hepatitis C virus (HCV) vaccine candidates, test diagnostic platforms, establish viral culture systems, as well as translational virus–host interaction studies. Supplementary Table 1 lists previous studies utilizing DANHEP data or samples from the DANHEP biobank.2–4,18–58
As all individuals with chronic viral hepatitis are managed in hospital settings in Denmark, DANHEP represents a broader spectrum of disease stages than for instance databases from tertiary hospitals or general practitioners.59,60 Contrary to claims data from insurance providers or notifications to a national register, DANHEP holds clinical data such as results of imagery, laboratory tests and physical examinations.61,62 Host and viral factors have been shown to impact both risk of long-term complications and efficacy of some antiviral therapies.63,64 The population with chronic viral hepatitis in Denmark is more diverse regarding genotypes, sex and ethnicity compared with large cohorts in Asia or Veteran Administration registers in the US with larger male concentration.65,66 Thus, DANHEP would be well suited to investigate for instance if effects of novel viral therapies depend on host or viral factors. The setting and epidemiology of chronic viral hepatitis in Sweden is similar to that of Denmark. In 2009, Infcare Hepatitis, a nationwide, clinical quality register for chronic viral hepatitis was established in Sweden.12 Like DANHEP, Infcare Hepatitis holds data on route of transmission, sex, age, region of origin, laboratory results, antiviral treatment, and long-term complications. Coverage for persons treated for CHC is >90%. Coverage for CHB has to our knowledge not been reported. Nonetheless, DANHEP and Infcare Hepatitis provide an opportunity for collaboration for instance when examining rare events. The Hepatitis C Virus (HCV) Research UK Clinical Database and Biobank, established in 2012, holds similar data on around 10,000 participants with past or current CHC attending specialized care in the United Kingdom (UK).67 The UK HCV population is similar to the one in Denmark with the majority being male, route of infection most commonly being intravenous drug use and most common genotypes being 1 and 3. Like DANHEP the UK cohort is limited by the fact that a large part of the population with CHC are either undiagnosed or not linked to specialized care.
The strengths of DANHEP are that it is a large database with nationwide coverage and over 15,000 participants followed prospectively over a 20-year period. Moreover, it is one of few nationwide databases connected to a biobank with over 38,0000 samples likewise collected over a 20-year period. Hereby providing the opportunity to investigate the connection between long-term disease outcome or treatment response based on viral characteristics, host immune response and the interplay between the two. Moreover, DANHEP uses PINs to identify participants making it possible to link data from DANHEP to national registers on for instance socio-economic status, emigration, mortality, comorbidity, hospitalization and use of medicines.
A limitation is that DANHEP does not cover persons with chronic viral hepatitis who are not linked to care. Although it is recommended by national guidelines, far from all receive specialized care. Previous studies have estimated that only 32% of individuals diagnosed with CHB and 48% of individuals diagnosed with CHC in Denmark receive specialized care.2,3 As a result, DANHEP only covers 30–50% of the population with chronic viral hepatitis in Denmark with the current setup. The remedy for this limitation is also an important step toward viral hepatitis elimination namely improving linkage to care. A previous study among HBsAg positive mothers indicated that the main barrier was referral.54 Currently both notification and referral are the responsibility of the diagnosing physician. Perhaps automatic referrals from laboratories would improve linkage to the care. Another limitation is the changing requirements for informed consent for patients to be included in DANHEP. Inclusion in DANHEP required participant consent during 2013–2017 and from 2019 onward. We evaluated changes in overlap between DANHEP and the NPR and found no significant effect of consent requirement on coverage. Coverage increased over time regardless of whether patient consent was required for inclusion in DANHEP. This suggests a minor or negligible impact. However, further examination is needed to draw firm conclusions.
A further limitation is that 7/16 hospital departments did not report to DANHEP from 2020 to 2023. We are currently updating DANHEP with data on antiviral treatments and new diagnoses from those years. Nonetheless, there is a risk that data from 2020 to 2023 from the Eastern part of Denmark will be less complete which is important to consider when using DANHEP data for research.
Data in DANHEP is transferred from electronic patient files. Consequently, only data that physicians choose to record is available. As a result, variables such as mode of transmission and country of origin are prone to missing values, as evident in Table 3. Compared to, for instance, the Hepatitis C Virus (HCV) Research UK Clinical Database, we find a high amount of missing baseline characteristics. Some baseline characteristics such as country of origin, intravenous drug use, alcohol use may be retrieved from national registers. Other data such as smoking or BMI is not available elsewhere. For routine laboratory results, we find lower rates of missing values ranging from 3% to 7%.
The manual data collection also makes DANHEP susceptible to typing errors. To address this, we assessed the accuracy of seven key variables in DANHEP by verifying 50 randomly selected values in patient files. We found an error proportion of less than 5% for most variables. Date of HBsAg loss however had an error proportion of 25%. Thus, caution should be exhibited when using this variable for research purposes. As not all values could be verified due to new electronic patient filings systems, statical power ended up being low for this analysis with confidence intervals ranging from 1% to 15% error proportion. Thus, a repeated analysis with a larger sample size would be useful.
In conclusion, DANHEP is a nationwide database with over 15,000 participants with CHB and/or CHC registered since 2002. The use of PINs allows for precise linkage to Danish national registries. DANHEP contains information on coinfections, viral DNA/RNA titers, serology, liver parameters, liver stiffness measurements, liver biopsy results, treatment initiation, – cessation and efficacy as well as viral resistance. Coverage is good for the chronic viral hepatitis population linked to care in Denmark. Moreover, the DANHEP biobank holds approximately 38,000 samples collected since 2004. This makes DANHEP well suited for studying the epidemiology, virology and immunology of chronic viral hepatitis. Numerous studies from the DANHEP database have already been published (see supplementary Table 1), and we invite the scientific community to contact us for collaboration in the field of chronic viral hepatitis.
Data Sharing Statement
Data from DANHEP may be requested by application to the DANHEP steering group and must be approved by the Danish health data authorities. The application must be submitted in collaboration with the steering group. Data transfer requires a data transfer agreement approved by the Danish health data authorities. The process may take several months. For more information, please contact the corresponding author.
Acknowledgments
We sincerely thank all DANHEP participants for their valuable contribution, and all persons who have contributed with inclusion of participants and registration of data in DANHEP, as well as all technicians who have handled blood samples.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
DANHEP has been funded by the contributing hospital departments. Coverage of exemption from clinical work to write this manuscript was funded by regional research funds to SB (grant# A7558) from the Capital Region of Denmark.
Disclosure
Dr Signe Bollerup reports grants from Capital Region research funds, during the conduct of the study. Dr Sofie Jespersen reports grants from Novo Nordisk Foundation, outside the submitted work. Professor Nina Weis reports grants from Novo Nordisk Foundation, Elsass Foundation, Aase and Ejnar Danielsens Fund; payment for expert testimony from The Danish Council of Medical Examiners, outside the submitted work. Dr Thomas Rasmussen reports speaker fees from Viiv Healthcare and Gilead, reports conference invitation from Gilead, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global hepatitis report 2024: action for access in low- and middle-income countries. Available from: https://www.who.int/publications/i/item/9789240091672.
2. Bollerup S, Wessman M, Hansen JF, et al. Increasing prevalence of chronic hepatitis B virus infection and low linkage to care in Denmark on 31 December 2016 - an update based on nationwide registers. Infect Dis Lond Engl. 2023;55(1):17–11. doi:10.1080/23744235.2022.2125065
3. Nielsen S, Hansen JF, Hay G, et al. Hepatitis C prevalence in Denmark in 2016-An updated estimate using multiple national registers. PLoS One. 2020;15(9):e0238203. doi:10.1371/journal.pone.0238203
4. Krarup H, Andersen S, Madsen PH, et al. HBeAg and not genotypes predicts viral load in patients with hepatitis B in Denmark: a nationwide cohort study. Scand J Gastroenterol. 2011;46(12):1484–1491. doi:10.3109/00365521.2011.619273
5. Weis N, Lauersen A, Brehm Christensen P, Galmstrup Madsen L, Clausen MR, Bygum Krarup H. Hepatitis B 9. udgave. Available from: https://infmed.dk/site/tools/download.php?UID=3b4eb296d38ffeea5259239611f3724023c6b59f.
6. Lampertico P, Agarwal K, Berg T; European Association for the Study of the Liver (EASL). EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021
7. Weis N, Brehm Christensen P, Lauersen A, Bygum Krarup H, Galmstrup Madsen L, Clausen MR. Treatment of hepatitis C virus infection 9th edition. Available from: https://infmed.dk/site/tools/download.php?UID=284cf8a543ca4fadb22e8e326ab8f7cd15cd72d5.
8. Aabye MG. Sundhedsstyrelsen: national Strategy for Hepatitis C. 2023.
9. Weis N, Clausen MR, Christensen PB, Krarup H, Laursen AL, Madsen LG. Treatment of hepatitis B virus (HBV) and hepatitis C virus (HCV) infection - a guideline. Available from: http://www.infmed.dk/guidelines.
10. Reiberger T, Lens S, Cabibbo G, et al. EASL position paper on clinical follow-up after HCV cure. J Hepatol. 2024;81(2):326–344. doi:10.1016/j.jhep.2024.04.007
11. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–25. doi:10.1177/1403494810387965
12. About InfCareHepatit | infCareHepatit. Available from: https://www.infcarehepatit.se/about-infcarehepatit.
13. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
14. Christensen PB, Hansen JF. Patients with viral hepatitis B Og C region south, mid and north annual report 2021-2022. 2024.
15. Obel N, Reinholdt H, Omland LH, Engsig F, Sørensen HT, Hansen ABE. Retrivability in The Danish National Hospital Registry of HIV and hepatitis B and C coinfection diagnoses of patients managed in HIV centers 1995-2004. BMC Med Res Methodol. 2008;8:25. doi:10.1186/1471-2288-8-25
16. Statens Serum Institut. Hepatitis B, acute and chronic - prevalence in 2019. Available from: https://www.ssi.dk/sygdomme-beredskab-og-forskning/sygdomsovervaagning/h/hepatitis-b-akut-og-kronisk-opgoerelse-over-sygdomsforekomst-2019.
17. Andersen ES, Omland LH, Jepsen P, et al. Risk of all-type cancer, hepatocellular carcinoma, non-Hodgkin lymphoma and pancreatic cancer in patients infected with hepatitis B virus. J Viral Hepat. 2015;22(10):828–834. doi:10.1111/jvh.12391
18. Pedersen J, Moukandja IP, Ndidi S, et al. An adaptable platform for in-house hepatitis C serology. J Virol Methods. 2022;308:114586. doi:10.1016/j.jviromet.2022.114586
19. Schønning K, Johansen K, Nielsen LG, Weis N, Westh H. Analytical performance of the Hologic Aptima HBV Quant Assay and the COBAS Ampliprep/COBAS TaqMan HBV test v2.0 for the quantification of HBV DNA in plasma samples. J Clin Virol. 2018;104:83–88. doi:10.1016/j.jcv.2018.05.007
20. Jespersen S, Bollerup S, Madsbad S, et al. Cardiometabolic comorbidities in patients with chronic hepatitis B and impact on incidence of liver complications. A Danish nationwide cohort study. Int J Gen Med. 2025;18:1591–1604. doi:10.2147/IJGM.S471083
21. Brinck-Jensen NS, Erichsen P, Tarp B, et al. Clinical findings in a multi-ethnic adult hepatitis B virus patient population in Denmark with emphasis on genotypic characteristics. Scand J Gastroenterol. 2015;50(8):1032–1038. doi:10.3109/00365521.2014.974202
22. Sølund C, Hallager S, Pedersen MS, et al. Direct acting antiviral treatment of chronic hepatitis C in Denmark: factors associated with and barriers to treatment initiation. Scand J Gastroenterol. 2018;53(7):849–856. doi:10.1080/00365521.2018.1467963
23. Fahnøe U, Madsen LW, Christensen PB, et al. Effect of direct-acting antivirals on the titers of human pegivirus 1 during treatment of chronic hepatitis C patients. Microbiol Spectr. 2024;12(9):e0064124. doi:10.1128/spectrum.00641-24
24. Hansen N, Obel N, Christensen PB, et al. Effectiveness of treatment with pegylated interferon and ribavirin in an unselected population of patients with chronic hepatitis C: a Danish nationwide cohort study. BMC Infect Dis. 2011;11:177. doi:10.1186/1471-2334-11-177
25. Jensen SB, Fahnøe U, Pham LV, et al. Evolutionary pathways to persistence of highly fit and resistant hepatitis C virus protease inhibitor escape variants. Hepatology. 2019;70(3):771–787. doi:10.1002/hep.30647
26. Clausen LN, Weis N, Ladelund S, et al. Genetic variants in the apoptosis gene BCL2L1 improve response to interferon-based treatment of hepatitis C virus genotype 3 infection. Int J Mol Sci. 2015;16(2):3213–3225. doi:10.3390/ijms16023213
27. Fahnøe U, Pedersen MS, Sølund C, et al. Global evolutionary analysis of chronic hepatitis C patients revealed significant effect of baseline viral resistance, including novel non-target sites, for DAA-based treatment and retreatment outcome. J Viral Hepat. 2021;28(2):302–316. doi:10.1111/jvh.13430
28. Christensen PB, Hay G, Jepsen P, et al. Hepatitis C prevalence in Denmark -an estimate based on multiple national registers. BMC Infect Dis. 2012;12:178. doi:10.1186/1471-2334-12-178
29. Sherwood AV, Rivera-Rangel LR, Ryberg LA, et al. Hepatitis C virus RNA is 5’ capped with flavin adenine dinucleotide (FAD). Nature. 2023;619(7971):811–818. doi:10.1038/s41586-023-06301-3
30. Bollerup S, Hallager S, Baek O, et al. Implementation of treatment recommendations for chronic hepatitis B in patients attending specialized hospital care in Denmark - a region wide study. Scand J Gastroenterol. 2020;55(7):843–847. doi:10.1080/00365521.2020.1779803
31. Alzua GP, Pihl AF, Offersgaard A, et al. Inactivated genotype 1a, 2a and 3a HCV vaccine candidates induced broadly neutralising antibodies in mice. Gut. 2023;72(3):560–572. doi:10.1136/gutjnl-2021-326323
32. Bollerup S, Engsig F, Hallager S, et al. Incidence of hepatocellular carcinoma and decompensated liver cirrhosis and prognostic accuracy of the PAGE-B HCC risk score in a low endemic hepatitis b virus infected population. J Hepatocell Carcinoma. 2022;9:1093–1104. doi:10.2147/JHC.S372571
33. Ruhwald M, Andersen ES, Christensen PB, Moessner BK, Weis N. IP-10 can be measured in dried plasma spots in patients with chronic hepatitis C infection. PLoS One. 2012;7(9):e45181. doi:10.1371/journal.pone.0045181
34. Lau FF, Bollerup S, Engsig F, et al. Ischemic heart disease in chronic hepatitis B: a Danish nationwide cohort study. Clin Epidemiol. 2022;14:879–888. doi:10.2147/CLEP.S361910
35. Christensen PB, Krarup HB, Møller A, et al. Liver biopsy performance and histological findings among patients with chronic viral hepatitis: a Danish database study. Scand J Infect Dis. 2007;39(3):245–249. doi:10.1080/00365540600978864
36. Hallager S, Ladelund S, Christensen PB, et al. Liver-related morbidity and mortality in patients with chronic hepatitis C and cirrhosis with and without sustained virologic response. Clin Epidemiol. 2017;9:501–516. doi:10.2147/CLEP.S132072
37. Søholm J, Hansen JF, Mössner B, et al. Low incidence of HCC in chronic hepatitis C patients with pretreatment liver stiffness measurements below 17.5 kilopascal who achieve SVR following DAAs. PLoS One. 2020;15(12):e0243725. doi:10.1371/journal.pone.0243725
38. Andersen ES, Moessner BK, Christensen PB, et al. Lower liver stiffness in patients with sustained virological response 4 years after treatment for chronic hepatitis C. Eur J Gastroenterol Hepatol. 2011;23(1):41–44. doi:10.1097/MEG.0b013e328341b891
39. Eriksen MB, Jørgensen LB, Krarup H, et al. Molecular and epidemiological profiles of hepatitis C virus genotype 4 in Denmark. J Med Virol. 2010;82(11):1869–1877. doi:10.1002/jmv.21896
40. Bollerup S, Hallager S, Engsig F, et al. Mortality and cause of death in persons with chronic hepatitis B virus infection versus healthy persons from the general population in Denmark. J Viral Hepat. 2022;29(9):727–736. doi:10.1111/jvh.13713
41. Hallager S, Brehm Christensen P, Ladelund S, et al. Mortality rates in patients with chronic hepatitis C and cirrhosis compared with the general population: a Danish cohort study. J Infect Dis. 2017;215(2):192–201. doi:10.1093/infdis/jiw527
42. Sølund C, Krarup H, Ramirez S, et al. Nationwide experience of treatment with protease inhibitors in chronic hepatitis C patients in Denmark: identification of viral resistance mutations. PLoS One. 2014;9(12):e113034. doi:10.1371/journal.pone.0113034
43. Pedersen J, Lundbo LF, Krarup H, Bukh J, Weis N. Neutralizing antibodies in patients with chronic hepatitis C and correlation to liver cirrhosis and estimated duration of infection. J Med Virol. 2016;88(10):1791–1803. doi:10.1002/jmv.24537
44. Pham LV, Velázquez-Moctezuma R, Fahnøe U, et al. Novel HCV genotype 4d infectious systems and assessment of direct-acting antivirals and antibody neutralization. Viruses. 2022;14(11):2527. doi:10.3390/v14112527
45. Winckelmann A, Fahnøe U, Bajpai PS, et al. Novel hepatitis B virus reverse transcriptase mutations in patients with sustained viremia despite long-term tenofovir treatment. J Clin Virol. 2022;150-151:105159. doi:10.1016/j.jcv.2022.105159
46. Hansen N, Obel N, Christensen PB, et al. Predictors of antiviral treatment initiation in hepatitis C virus-infected patients: a Danish cohort study. J Viral Hepat. 2009;16(9):659–665. doi:10.1111/j.1365-2893.2009.01126.x
47. Bergløv A, Hallager S, Panum I, Weis N. Prevalence of herpes -, measles morbillivirus-, parvovirus B19 - and rubella viruses immunoglobulin G among women with chronic hepatitis B of reproductive age in Denmark: a cross-sectional study. Int J Infect Dis. 2020;101:269–275. doi:10.1016/j.ijid.2020.09.1477
48. Hansen N, Cowan S, Christensen PB, Weis N; DANHEP-styregruppen. Reporting chronic hepatitis B and C in Denmark. Ugeskr Laeger. 2008;170(18):1567–1570.
49. Dalgard O, Weiland O, Noraberg G, et al. Sofosbuvir based treatment of chronic hepatitis C genotype 3 infections-A Scandinavian real-life study. PLoS One. 2017;12(7):e0179764. doi:10.1371/journal.pone.0179764
50. Safreed-Harmon K, Blach S, Aleman S, et al. The consensus hepatitis C cascade of care: standardized reporting to monitor progress toward elimination. Clin Infect Dis. 2019;69(12):2218–2227. doi:10.1093/cid/ciz714
51. Weis N, Thomsen RW; DANHEP-styregruppen. The Danish Database for Hepatitis B and C. Ugeskr Laeger. 2012;174(42):2521.
52. Hallager S, Lundh A, Ladelund S, et al. The prevalence of human immunodeficiency virus coinfection among patients newly diagnosed with chronic hepatitis B or C in Denmark: a nationwide cohort study. Open Forum Infect Dis. 2018;5(12):ofy310. doi:10.1093/ofid/ofy310
53. Andersen ES, Weiland O, Leutscher P, et al. Low liver stiffness among cirrhotic patients with hepatitis B after prolonged treatment with nucleoside analogs. Scand J Gastroenterol. 2011;46(6):760–766. doi:10.3109/00365521.2011.565068
54. Weis N, Cowan S, Hallager S, et al. Vertical transmission of hepatitis B virus during pregnancy and delivery in Denmark. Scand J Gastroenterol. 2017;52(2):178–184. doi:10.1080/00365521.2016.1244704
55. Dalegaard MI, Winckelmann A, Fahnøe U, et al. Higher rates of viral evolution in chronic hepatitis B patients linked to predicted T cell epitopes. Viruses. 2025;17(5):684. doi:10.3390/v17050684
56. Bajpai PS, Collignon L, Sølund C, et al. Full-length sequence analysis of hepatitis C virus genotype 3b strains and development of an in vivo infectious 3b cDNA clone. APMIS. 2023;97(12):e00925–23. doi:10.1128/jvi.00925-23
57. Sølund C, Pedersen MS, Fahnøe U, et al. Pre-existing, treatment-specific resistance-associated substitutions in hepatitis C virus genotype 1 and 3 and viral RNA titers during treatment with direct-acting antivirals. Acta Pathol Microbiol Immunol Scand. 2023;131(8):426–433. doi:10.1111/apm.13335
58. Clausen LN, Weis N, Schønning K, et al. Correlates of spontaneous clearance of hepatitis C virus in a Danish human immunodeficiency virus type 1 cohort. Scand J Infect Dis. 2011;43(10):798–803. doi:10.3109/00365548.2011.589077
59. Brakenhoff SM, de Man RA, de Knegt RJ, Bindels PJE, de Schepper EIT. Epidemiology and management of hepatitis B and C in primary care in the Netherlands: data from the Rijnmond Primary Care database. Fam Pract. 2023;40(1):83–90. doi:10.1093/fampra/cmac070
60. Papatheodoridis GV, Manolakopoulos S, Touloumi G, et al. Hepatocellular carcinoma risk in HBeAg-negative chronic hepatitis B patients with or without cirrhosis treated with entecavir: hepNet.Greece cohort. J Viral Hepat. 2015;22(2):120–127. doi:10.1111/jvh.12283
61. Von den Hoff DW, Berden FAC, Atsma F, Schellekens AFA, Drenth JPH. Against all odds? Addiction history associated with better viral hepatitis care: a dutch nationwide claims data study. J Clin Med. 2022;11(4):1146. doi:10.3390/jcm11041146
62. Duberg AS, Törner A, Davidsdóttir L, et al. Cause of death in individuals with chronic HBV and/or HCV infection, a nationwide community-based register study. J Viral Hepat. 2008;15(7):538–550. doi:10.1111/j.1365-2893.2008.00982.x
63. European Association for the Study of the Liver. Clinical Practice Guidelines Panel: chair:, EASL Governing Board representative:, Panel members: EASL recommendations on treatment of hepatitis C: final update of the series☆. J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018
64. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2025;83(2):502–583. doi:10.1016/j.jhep.2025.03.018
65. Chen CJ, Yang HI. Natural history of chronic hepatitis B REVEALed. J Gastroenterol Hepatol. 2011;26(4):628–638. doi:10.1111/j.1440-1746.2011.06695.x
66. Mittal S, Kramer JR, Omino R, et al. Role of Age and Race in the Risk of Hepatocellular Carcinoma in Veterans With Hepatitis B Virus Infection. Clin Gastroenterol Hepatol. 2018;16(2):252–259. doi:10.1016/j.cgh.2017.08.042
67. McLauchlan J, Innes H, Dillon JF, et al. Cohort Profile: the Hepatitis C Virus (HCV) Research UK Clinical Database and Biobank. Int J Epidemiol. 2017;46(5):1391–1391h. doi:10.1093/ije/dyw362
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.