Back to Journals » Clinical Epidemiology » Volume 8
The Danish Bladder Cancer Database
Authors Hansen E, Larsson H, Nørgaard M ![]() , Thind P, Jensen JB
, Thind P, Jensen JB
Received 24 December 2015
Accepted for publication 29 February 2016
Published 25 October 2016 Volume 2016:8 Pages 439—443
DOI https://doi.org/10.2147/CLEP.S99491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Erik Hansen,1–3 Heidi Larsson,4 Mette Nørgaard,4 Peter Thind,3,5 Jørgen Bjerggaard Jensen1–3
1Department of Urology, Hospital of West Jutland-Holstebro, Holstebro, 2Department of Urology, Aarhus University Hospital, Aarhus, 3The Danish Bladder Cancer Database Group, 4Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, 5Department of Urology, Copenhagen University Hospital, Copenhagen, Denmark
Aim of database: The aim of the Danish Bladder Cancer Database (DaBlaCa-data) is to monitor the treatment of all patients diagnosed with invasive bladder cancer (BC) in Denmark.
Study population: All patients diagnosed with BC in Denmark from 2012 onward were included in the study. Results presented in this paper are predominantly from the 2013 population.
Main variables: In 2013, 970 patients were diagnosed with BC in Denmark and were included in a preliminary report from the database. A total of 458 (47%) patients were diagnosed with non-muscle-invasive BC (non-MIBC) and 512 (53%) were diagnosed with muscle-invasive BC (MIBC). A total of 300 (31%) patients underwent cystectomy. Among the 135 patients diagnosed with MIBC, who were 75 years of age or younger, 67 (50%) received neoadjuvent chemotherapy prior to cystectomy. In 2013, a total of 147 patients were treated with curative-intended radiation therapy.
Descriptive data: One-year mortality was 28% (95% confidence interval [CI]: 15–21). One-year cancer-specific mortality was 25% (95% CI: 22–27%). One-year mortality after cystectomy was 14% (95% CI: 10–18). Ninety-day mortality after cystectomy was 3% (95% CI: 1–5) in 2013. One-year mortality following curative-intended radiation therapy was 32% (95% CI: 24–39) and 1-year cancer-specific mortality was 23% (95% CI: 16–31) in 2013.
Conclusion: This preliminary DaBlaCa-data report showed that the treatment of MIBC in Denmark overall meet high international academic standards. The database is able to identify Danish BC patients and monitor treatment and mortality. In the future, DaBlaCa-data will be a valuable data source and expansive observational studies on BC will be available.
Keywords: bladder cancer, cystectomy, neoadjuvant chemotherapy, curative-intended radiation therapy
Aim of database
Patients diagnosed with invasive bladder cancer (BC) in Denmark are treated according to the national guidelines at one of the five uro-oncological centers. The aim of the Danish Bladder Cancer Database (DaBlaCa-data) is to monitor treatment and general survival of patients diagnosed with BC in Denmark. The goal of the database is to provide standards of the highest level of clinical evidence based on expert knowledge in the area.
To guide the selection of quality indicators suitable for monitoring treatment and outcome of BC in Denmark, a report reviewing the existing literature on the treatment of BC was made.1 In 2015, DaBlaCa-data consisted of three process indicators and ten outcome indicators concerning the diagnostic and treatment quality of patients diagnosed with BC in Denmark. Indicators may change over the years as the database evolves. Patients with noninvasive tumors (urothelial papillomas or carcinoma in situ) are not included in the database. To avoid extensive manual registration of data, the database is largely based on secondary data from the Danish National Registry of Patients (DNRP) and the Danish National Pathology Register (DNPR).2,3 Consequently, extensive validation of the data has been done to secure that the algorithms used to identify patients diagnosed with BC (stage T1–T4) and the treatment provided for these patients had sufficient quality. Only variables regarding the cause of death, used for estimating cancer-specific mortality, and use of neoadjuvant chemotherapy are registered manually. Patients are identified in the database by their personal security number, making it possible to link DaBlaCa-data to other Danish registries if so desired with a purpose of research or monitoring the quality of treatment.
Study population
All patients diagnosed with BC in Denmark are included in the database. Inclusion is based on the data generated by the algorithms, which subtracts patients from the DNRP and the DNPR on a regular basis from all hospitals and private clinics in Denmark.
In 2013, 970 patients were referred or allocated to one of the five uro-oncological treatment centers treating BC in Denmark and were included in the database. Of the diagnosed patients, 26% were women. The median age was 74 years for women and 73 years for men.
Main variables
In 2013, a total of 970 patients were diagnosed with BC in Denmark. Among them, 512 (53%) were diagnosed with muscle-invasive BC (MIBC) and 458 were diagnosed with non-muscle-invasive BC (non-MIBC).
Survival
Of the 970 BC patients included in 2013, 698 were still alive 1 year after diagnosis, corresponding to a 1-year mortality rate of 28% (95% confidence interval [CI]: 25–31). The national standard had been set to 35% prior to evaluation based on a literature review.4 All five treatment centers met the standard.
In 2013, cancer-specific mortality 1 year after BC diagnosis was 25% (95% CI: 22–27). Of the 970 patients, 226 had died because of BC within 1 year after diagnosis, whereas for 54 cases (6%), registration regarding the cause of death was missing. Therefore, cancer-specific death may in reality be higher than 25% but not higher than 31%. The national standard was set at 15% or less.5 Only one of the five treatment centers met the standard (Table 1).
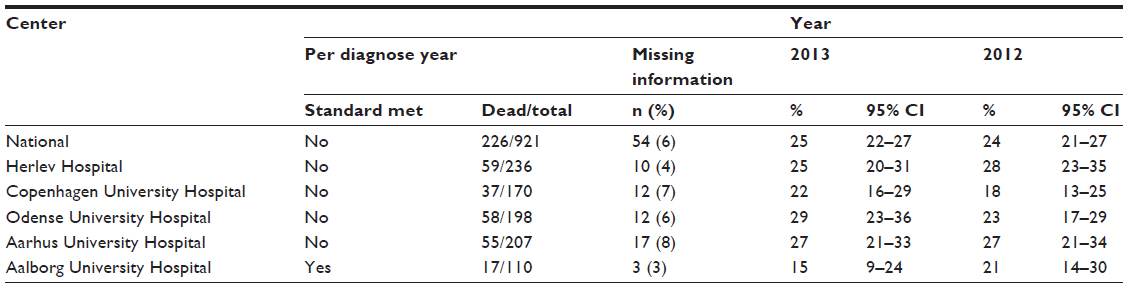 | Table 1 One-year cancer-specific mortality after invasive bladder cancer diagnosis on a national level and per treatment center |
A total of 300 patients, diagnosed in 2013, underwent cystectomy due to BC. At cutoff date (April 15, 2015), last date for data to be included in the preliminary report, 1-year follow-up after cystectomy was available for 270 patients, whereas data were missing for two patients. Therefore, 268 patients were included in this variable. Of them, 230 were still alive 1 year after BC diagnosis, corresponding to a 1-year mortality of 24% after cystectomy due to BC (95% CI: 21–28) (Table 2). The standard was set at 30% as the highest.6 All treatment centers met the standard.
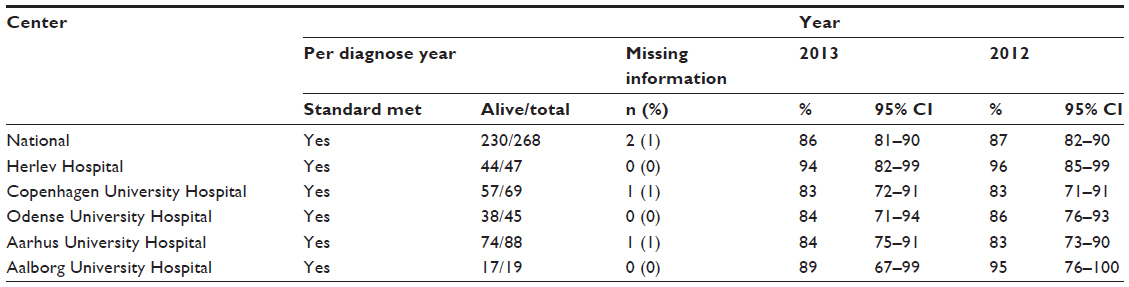 | Table 2 One-year survival after cystectomy on a national level and per treatment center |
In 2013, 1-year cancer-specific mortality after cystectomy due to invasive BC was 7% (95% CI: 5–11). A total of 19 patients were registered with BC as the cause of death, while 13 patients had missing data regarding the cause of death. The national standard was set at 12% or lower.7 All five centers met the standard.
Fraction undergoing neoadjuvant treatment
In all, 135 patients younger than 75 years were diagnosed with MIBC (stage T2–T4) and underwent cystectomy. Among them, 65 (48%) received neoadjuvant chemotherapy prior to cystectomy. The national standard was set at 25% or higher.6 All treatment centers met the standard.
Fraction undergoing cystectomy
In 2013, a total of 512 patients were diagnosed with MIBC (stage T2–T4) in Denmark. Among them, 166 (32%) were cystectomized within 6 months. We found a variation of 23%–40% in this proportion among the five centers. The national standard for this variable is still undetermined.
Post-cystectomy mortality
The 90-day mortality in patients undergoing cystectomy due to invasive BC in Denmark was found to be 3% (95% CI: 1–5) in 2013. The national standard was set at 7% or below and was met by all five centers.8
Postsurgical admission after cystectomy
For patients undergoing cystectomy due to BC in 2013, the median postsurgical admission including primary length of stay and readmissions after cystectomy during the first 90 days was 11 days (interquartile range [IQR]: 8–20 days). All admissions among the patients during the first 90 days were included, no matter the cause and the department. The national standard was set at a median admission of no more than 20 days.9,10 All five centers met this standard.
Oncological treatment
In 2013, 147 patients diagnosed with BC received their first radiation therapy with curative intent. Of these, 99 were still alive 1 year after the date of first radiotherapy. One patient had undetermined status and was not included. Thus, 1-year mortality after curative radiation therapy due to BC was 32% (95% CI: 24–39). The national standard was set at 40% or lower.11 Two of the five centers did not meet the standard (1-year mortality of 42% and 43%, respectively). The other three centers met the standard (27%, 32%, and 31%, respectively).
Among the 147 patients receiving curative-intended radiation therapy in 2013, cancer-specific mortality was 23%. Thirty-three patients were registered with BC as the cause of death. Three patients lacked information regarding the cause of death. The national standard was set at 18% or less.12 Only one of the five centers met the standard (11%) (Table 3).
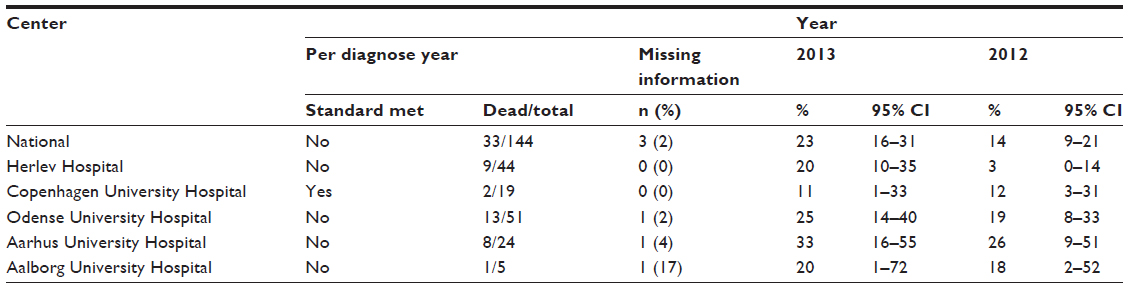 | Table 3 One-year cancer-specific mortality after first curative-intended radiation therapy due to MIBC on a national level and per treatment center |
Follow-up
By April 15, 2015, patients registered in DaBlaCa-data are followed for only 2 and 3 years (2012 and 2013). The follow-up is continuous for each patient and ends at death of that patient. The data presented in this paper are based on a preliminary report including all patients diagnosed with BC in Denmark in the period between January 1, 2012 and December 31, 2013. DaBlaCa-data is an ongoing database enrolling all patients diagnosed with BC in Denmark from 2012 onward.
Examples of research
A validation report based on the validation of algorithms prior to the final establishment of DaBlaCa-data is in preparation. Further studies based on the results found in DaBlaCa-data are planned with a longer follow-up period.
Conclusion
DaBlaCa-data is able to identify Danish BC patients and monitor treatment and mortality. The preliminary DaBlaCa-data report showed comparable results between the five uro-oncological treatment centers responsible for the treatment of all patients diagnosed with BC in Denmark. Differences in mortality among the BC patients may reflect differences in the general mortality in different regions of Denmark.
The standard for cancer-specific mortality 1 year after BC diagnosis (15%) is believed to be underestimated. Most studies of the existing literature focus on cancer-specific mortality in patients who had received treatment due to BC. The DaBlaCa-data includes all patients with BC; hence, 15% is an underestimate in this database, though 15% is the best estimate when reviewing the literature. The high 1-year survival rate after cystectomy could reflect the fact that all the five uro-oncological centers have high and uniform standards for selecting patients for cystectomy and high quality of the surgical procedure. The board members of DaBlaCa-data expect to see more variation in cancer-specific mortality over time, due to longer follow-up periods. Until now, the treatment strategy has differed concerning the trend to choose radiation therapy. All five centers strive toward more uniform treatment protocols in the future than in the past. The median length of stay in a hospital post-cystectomy was very low compared to the standard. This again may reflect the high and uniform surgical standard among the five uro-oncological centers in Denmark.
The variation seen among the centers regarding cancer-specific mortality after curative-intended radiotherapy may reflect differences in patient selection to radiotherapy. The fact that two of the five centers were slightly under the standard concerning 1-year survival after curative-intended radiotherapy is believed to be insignificant.
Acknowledgments
We deeply acknowledge Jakob Kristian Jakobsen for his reviewing report prior to the establishment of DaBlaCa-data; project nurse Anna Munk Nielsen for her huge validation work prior to the establishment of DaBlaCa-data; The Danish Cancer Society for their financial support; other board members in DaBlaCa-data: Niels Viggo Jensen, Anette Pedersen Pilt, Knud Fabrin; Elin Kallestrup, representative of the data controlling authority; and Anne Nakano Jensen, Quality Consultant MHSc.
DaBlaCa-data is an approved nationwide clinical quality database and is primarily financed by the Danish Regions. This paper was funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions. A grant of 450,000 Danish kroner was donated by The Danish Cancer Society to fund the validation process prior to the final establishment of DaBlaCa-data.
Disclosure
The authors report no conflicts of interest in this work.
References
Jakobsen JK. Dokumentalist Blærecancer, The Danish Clinical Registries. Available from: http://www.kcks-vest.dk/siteassets/de-kliniske-databaser/dablaca/dokumentalistrapport-dablaca-data.pdf. | |
Andersen TF, Madsen M, Jørgensen J, Mellemkjoer L, Olsen JH. The Danish National Hospital Register. A valuable source of data for modern health sciences. Dan Med Bull. 1999;46(3):263–268. | |
Erichsen R, Lash TL, Hamilton-Dutoit SJ, Bjerregaard B, Vyberg M, Pedersen L. Existing data sources for clinical epidemiology: the Danish National Pathology Registry and Data Bank. Clin Epidemiol. 2010;2:51–56. | |
Lund L, Erichsen R, Norgaard M, Larsen EH, Borre M, Jacobsen J. Survival of invasive bladder cancer patients, 1998–2009: a central and northern Denmark population-based cohort study. Clin Epidemiol. 2011;3(Suppl 1):47–51. | |
Lughezzani G, Sun M, Shariat SF, et al. A population-based competing-risks analysis of the survival of patients treated with radical cystectomy for bladder cancer. Cancer. 2011;117(1):103–109. | |
Leow JJ, Martin-Doyle W, Rajagopal PS, et al. Adjuvant chemotherapy for invasive bladder cancer: a 2013 updated systemic review and meta-analysis of randomized trials. Eur Urol. 2014;66(1):42–54. | |
Otto W, May M, Fritsche HM, et al. Analysis of sex differences in cancer-specific survival and perioperative mortality following radical cystectomy: results of a large German multicenter study of nearly 2500 patients with urothelial carcinoma of the bladder. Gend Med. 2012;9(6):481–489. | |
Nielsen ME, Mallin K, Weaver MA, et al. The association of hospital volume with conditional 90-day mortality after cystectomy: an analysis of the National Cancer Database. BJU Int. 2014;114(1):46–55. | |
Arumainayagam N, McGrath J, Jefferson KP, Gillatt DA. Introduction of an enhanced recovery protocol for radical cystectomy. BJU Int. 2008;101(6):698–701. | |
Berrum-Svennung I, Hedelin H, Holmang S. Costs of radical cystectomy. Scand J Urol Nephrol. 2005;39(1):36–41. | |
Fokdal L, Hoyer M, von der Maase H. Treatment outcome and prognostic variables for local and survival in patients receiving radical radiotherapy for urinary bladder cancer. Acta Oncol. 2004;43(8):749–757. | |
Shelley MD, Barber J, Mason MD. Surgery versus radiotherapy for muscle invasive bladder cancer. Cochrane Database Syst Rev. 2001;3:CD002079. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.