")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
The Cost of Maternal Complications and Its Associated Factors Among Mothers Attending Public Hospitals in Harari Region and Dire Dawa City Administration, Eastern Ethiopia: An Institution-Based Cross-Sectional Study
Authors Shawel S , Hawulte Ayele B , Dessie Y, Tura AK , Dinsa G, Tekola A , Mandefro M , Masrie A , Tamire A , Tefasa OK
Received 2 May 2023
Accepted for publication 30 August 2023
Published 7 September 2023 Volume 2023:15 Pages 645—658
DOI https://doi.org/10.2147/CEOR.S416562
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Samrawit Shawel,1 Behailu Hawulte Ayele,1 Yadeta Dessie,1 Abera Kenay Tura,2 Gimaye Dinsa,1,3 Abainash Tekola,1 Miheret Mandefro,1 Awoke Masrie,1 Aklilu Tamire,1 Obsan Kassa Tefasa1
1School of Public Health, Haramaya University, Harar, Ethiopia; 2School of Nursing and Midwifery, Haramaya University, Harar, Ethiopia; 3School of Population and Public Health, University of British Columbia, Vancouver, Canada
Correspondence: Samrawit Shawel, Tel +251 913 705 953, Email [email protected]
Background: Pregnant women face high costs for health-care services despite being advertised as free. These costs include non-medical expenses, lost productivity, difficulties caring for family members, and long-term financial impact from complications. Limited research has been done on the cost burden of maternal services and complications, despite numerous studies on maternal health service provision. This is notable considering the government’s claim of providing free maternal health-care services.
Methods: A cross-sectional study was conducted in July (1– 30) 2022 among 425 randomly selected mothers in Harari and Dire Dawa City, Eastern Ethiopia. Data were collected through structured questionnaires and medical record reviews. The collected data was entered into Epi-Data version 3.02 and analyzed using STATA version 14.0 after data cleaning. Descriptive statistics and linear regression analysis were used to examine the data, ensuring assumptions of linearity, independence, homoscedasticity, and normality were met. The correlation coefficient was used to assess the strength of the association.
Results: The median cost of maternal complications was around 4250 ETB (81.3 USD; IQR = 2900– 5833.3), factors that predicted cost were monthly family income of ≥ 3001 birr (β=1.13; 95% CI: 1.00, 1.26), distance from hospital (β=0.73; 95% CI = 0.64– 0.83), being admitted for less than 4 days (β=0.60; 95% CI = 0.53– 0.69), accompanied by relatives besides their husbands (β=1.93; 95% CI = 1.52– 2.46), caesarian sections delivery (β=1.17; 95% CI = 1.04– 1.31), and giving birth to a normal baby (β=0.86; 95% CI = 0.77– 0.97).
Conclusion: Maternal complications incur significant costs, with factors such as family income, travel time, hospital stay, caregiver presence, mode of delivery, and neonatal outcome predicting these costs. The Ethiopian health system should address the additional expenses faced by mothers with complications and their caregivers.
Keywords: direct cost, indirect cost, medical-cost, maternal complication, Eastern Ethiopia
Background
Maternal health-related complications occur during any stage of pregnancy, delivery, and postpartum. They have an impact on the women’s physical, social, psychological, and economic wellbeing. In developing countries, these complications are the most significant public health challenge because of the cultural norms, poverty, lack of access to basic education, inaccessibility of essential health-care services.1
The concept of cost is referred as a measurement in monetary terms measuring the number of resources used for production of goods or for rendering health services. It is classified as direct non-medical costs, direct payment owed for service provided in money or in kind, such as for travel, food, and nutritional supplements during care and the medical costs related with the diagnosis and treatment services received, Financial constraints can happen due to direct medical and non-medical costs that are directly related with seeking any maternal health services and the indirect costs are related with productivity loss due to absenteeism from work.2,3
In measuring the costs related to delivering health-care services, the indirect type of cost valuation measuring productivity loss uses two important methods, such as the human capital approach (HCA) and the friction cost approach (FCA). HCA is based on the neoclassical theory that values production losses based on labor costs, while all productivity losses up to retirement are included. FCA values production loss in the friction period and the transaction costs of training and replacing with previously unemployed person.2,4,5
Ethiopia's average per capita income in 2022 was 857.32 USD and the health system expenditure is mainly (37%) covered by out-of-pocket spending followed by donor agencies 33% and the government spending 8.2%. According to the WHO, above 15–20% out-of-pocket expenditure on health care is a catastrophic expenditure; recent works have been done to improve the risk people face due to high financial burden using schemes including health insurance, majorly community-based health insurance (CBHI).6,7
The cost of seeking care is very high for pregnant women even if the service is free. Other associated expenditures like non-medical costs, productivity loss, not being able to take care of other family members, and the cost of acute health problems and long-term disabilities from complications during pregnancy and delivery are still very high.8,9
Although Ethiopia has tried to subsidize the cost of facility-based delivery services, women and households are being pushed into extreme poverty by the high cost of seeking delivery care, which is not considered in the government’s attempt to give free-of-charge service. For example, in a study conducted in public health facilities in Bale Zone, the median hidden cost was 877.5 ETB (32.03USD), whereas 5120 ETB in Mekelle General Hospital.6,10
So far, many maternal health-related research were conducted in the magnitude and the service provision of maternal health. There is thus limited research conducted to assess the cost burden of maternal service, including maternal complication, where the government is claiming every maternal health service is free of charge. Therefore, this study is aimed at assessing the cost of maternal complications and associated factors among mothers attending public hospitals in the Harari region and Dire Dawa City Administration, Eastern Ethiopia.
Methods and Materials
Study Setting, Design and Participants
An Institutional-based cross-sectional study design was conducted in public hospitals in the Harari region and Dire Dawa city administration from July 1–30, 2022. Dire Dawa (chartered city) city is located 530km east of the capital of Ethiopia, Addis Ababa. Based on the 2007 census conducted by the central statistical agency (CSA) population of the city is projected to be about 341,834 of which 171,461 are men and 170,461 women. In the city administration, there are 2 public hospitals, 14 health centers, and 58 health posts the expected number of delivery in Dil Chora hospital is 295 and 203 for Sabian general hospital and the number of women expected to be admitted with complication were 142 and 93 for Dil Chora hospital and Sabian general hospital, respectively, based on the review of last year’s same month data.
Harari regional state is located 525km east of Addis Ababa. The projected total population is 183,415, of whom 92,316 were men and 91,099 women, in this region, there are two public hospitals, one teaching and the other a general hospital, and 10 health centers and 32 health posts are serving the population. The expected number of deliveries for Hiwot Fana specialized university hospital is 590 and 154 for Jugal hospital, those expected to be admitted with complications were 209 and 38 for Hiwot Fana specialized university hospital and Jugal hospital, respectively. The study population includes all randomly selected mothers with complications who were admitted to the public hospitals of the Harari region and Dire Dawa city administration at the time of data collection. Mothers who were admitted with gynecological complications and those who were referred out from the institutions for further management were excluded from the study.
Sample Size and Sampling Procedure
Maximum sample size of 429 was obtained considering the assumption for single population mean formula with the 337.42 and 156 mean direct cost and standard deviation, respectively, were derived from a study conducted in Bale zone,7 d assumed to be 15.12 (derived by calculating the margin of error using the formula  ), sample size (409) and standard deviation (156), using the same study conducted in Bale zone,7 95% confidence interval and using the formula,
), sample size (409) and standard deviation (156), using the same study conducted in Bale zone,7 95% confidence interval and using the formula, 
Where n = required sample size, z = reliability coefficient for 95% confidence interval (1.96), δ = standard deviation (156), and d = assumed marginal error (15.12). By adding a 5% non-response rate, the final sample size for this study was 429.
There are two public hospitals in Dire Dawa city administration and one teaching and one general hospital found in Harari regional state and these four hospitals are the study areas where the study was undertaken. The monthly expected mothers admitted with complications to Dil-Chora Hospital, Sabian General Hospital, Jugal general Hospital, and Hiwot Fana specialized university Hospital is 142, 93, 38, and 209, respectively, based on last year’s same month report of the institutions.
Sampling with proportional to population size was considered to select the study units. Accordingly, by proportionally allocating samples based on their last year’s same month report of mothers with complications, 126 mothers from Dil Chora Hospital, 83 from Sabian General Hospital, 34 from Jugal General Hospital, and 186 mothers from Hiwot Fana specialized university Hospital were selected. All individual mothers who were admitted within the data collection month were recruited to participate in this study, as the number of mothers admitted with complications based on last year’s report is comparable with the calculated sample size (Table 1).
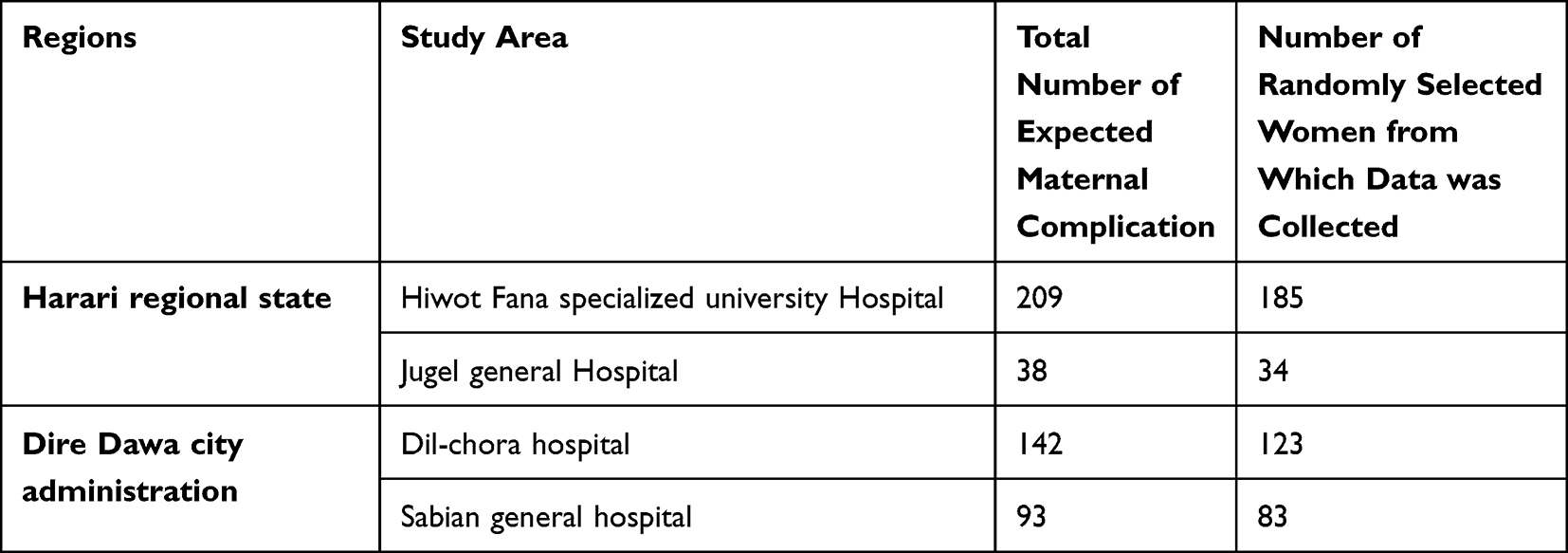 |
Table 1 Sampling Procedure for Selecting Mothers with a Complication Within Harari Regional State and Dire Dawa City Administration, Eastern Ethiopia 2022 |
Data Collection Tools and Methods
Data Collection Tool
The data was collected using a structured questionnaire adapted from the National health account 2016,11 Mini EDHS 201910 and a study done in the bale zone7 to assess the cost of maternal complication. The first part of the questionnaire contains the socio-demographic status of participants and their partners from mini EDHS 201910 and National health account 2016,11 clinical characteristics of the mothers with a complication from a study done in bale zone7 and the last part contains the institutional factors that are related with the diagnosis, treatment and other services the mothers and their attendant’s use from National health account 2016.11
Data Collection Methods
The data were collected using face-to-face interviews of mothers admitted with complications and document review by using a pretested structured questionnaire that was administered by trained data collectors to women who were going to be discharged from their admission and their partner.
Four BSC public health officers were recruited for data collection and the investigator closely supervised the data collection process.
Study Variables
Dependent Variable
Cost of maternal complications.
Independent Variables
Socio-demographic factors: Age, Marital status, Educational status, Place of residence, Income, Expenditure, Occupation, Living arrangement, Family size.
Institutional factors: Payment modalities, Distance from facility, Availability of medication, Availability of diagnostic modalities, Availability of treatment services, Admission Unit, Length of stay.
Clinical characteristics of the respondents: Hemorrhage, Obstructed labor, Preeclampsia, Antepartum hemorrhage, Post-partum hemorrhage, Sepsis, Abortion.
Measurement
Maternal complications: are defined as “potentially life-threatening conditions”. This is an extensive category of clinical conditions, including diseases that can threaten a woman’s life during pregnancy and labor and after the termination of pregnancy.12
Non-medical direct costs are out-of-pocket payments made by mothers (who are admitted with complications) or guardians for the transportation, accommodation, food, and nutritional supplements.6
Direct medical costs: are out-of-pocket payments made by mothers (who are admitted with complications) or guardians for medical services (consultations, laboratory tests, medicines, and medical procedures).6
Indirect cost: Productivity and economic costs of a mother or household incurred as a result of delivery service and during admission. Indirect costs are estimated using a total period of absence in hours multiplied by the hourly wage rate of the absent mother from their workplace.6
The human capital approach: was used to value the productivity time losses which uses the multiplication of the daily income of the women with the number of days being absent from work for treatment and recovery and it estimates the productivity loss of the mother.
Income: The amount of money received by a household during the reference period in exchange for labor or services, from the sale of goods or property, or as a profit from financial investments.3
The total cost: was estimated by adding the direct non-medical, indirect and direct medical cost.
Data Quality Control
To assure the quality of data, a two days of training was given to data collectors before the data collection time. To check the validity and reliability of the questionnaire to the objectives of the study, pre-test was conducted on 5% of the participants at Bisidimo Hospital. The questionnaire was translated to “Amharic”, “Afaan Oromo” and “Somali” language and back translation was done to English for the consistency of the data. The principal investigator led the team and supervised the correct implementation of the procedure by checking the completeness and logical consistency immediately at the collection site. Double data -entry was performed by two different individuals to minimize errors.
Data Processing and Analysis
The collected data was checked for completeness and consistency and each questionnaire was assigned a unique code before entering it into EPI- DATA statistical software.
Then, the data was exported to STATA version 14.0 for cleaning and analysis. Descriptive statistics such as frequencies, appropriate measures of central tendency, and dispersion was used to describe the data.
The parameters connected to the overall cost of maternal complications were found using simple and multivariate linear regression. In order to measure the strength of the association and factors associated with the outcome variable, variables with a p-value 0.25 during bivariable analyses were entered into multiple linear regression analysis after checking the assumptions for a linear relationship, independence, homoscedasticity, normality, and correlation coefficients along with 95% confidence intervals. At a p-value of 0.05 or lower, statistical significance was judged to have been reached.
The variance inflation factor (VIF), whose mean value was 5 (mean VIF = 1.90), was used to test for multicollinearity. Using the Shapiro–Wilk fit test, normality was evaluated. This is due to the Swilk test’s finding of insignificance at p0.05 (p = 0.000) and the model did not fit.
Results
Sociodemographic Characteristics of Respondents
A total of 425 mothers participated in this study yielding a response rate of 99%. In the current study, around half of the respondents (52.2%) were in the age group 25–34 years with the mean (±SD) age of 25.7 (±5). More than half (54.5%) of the respondents were from urban area and 56.5% came to the health facility through referral from other facilities. More than two-third (70.1%) of the respondents were Muslim, and 98.8% were currently married. More than one-fourth (28.5%) of the participants and 15.1% of their partners have never attended formal education. Around two-third (67.3%) of the participants were housewife and 28.9% of their partners were government employees. Around 80.5% of the respondents obtain a total family income of ≥3000 ETB (57.4 USD) with mean 8145.9 (±5627.3) (±SD) (Table 2).
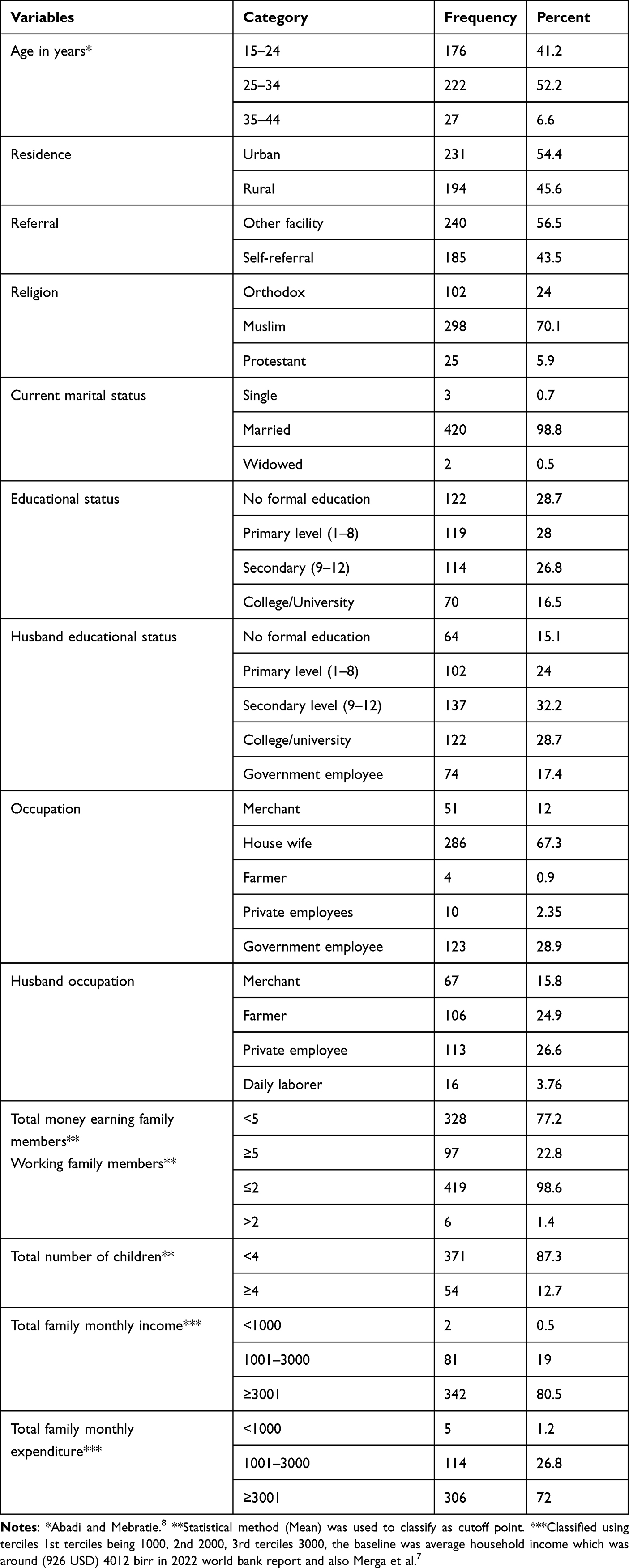 |
Table 2 Socio-Demographic Characteristics of Mothers with Complications Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
The Institutional Factors Related with Cost of Maternal Complications
About 60% of the respondents came from a distance of less than 20km with mean 19.03 (±20.25). Around 32% of the participants used ambulance as a mode of transportation, while 38.8% used taxi (Bajaj). The majority (96.7%) of respondents were accompanied by their relatives besides their husbands when coming to the institutions (Table 3).
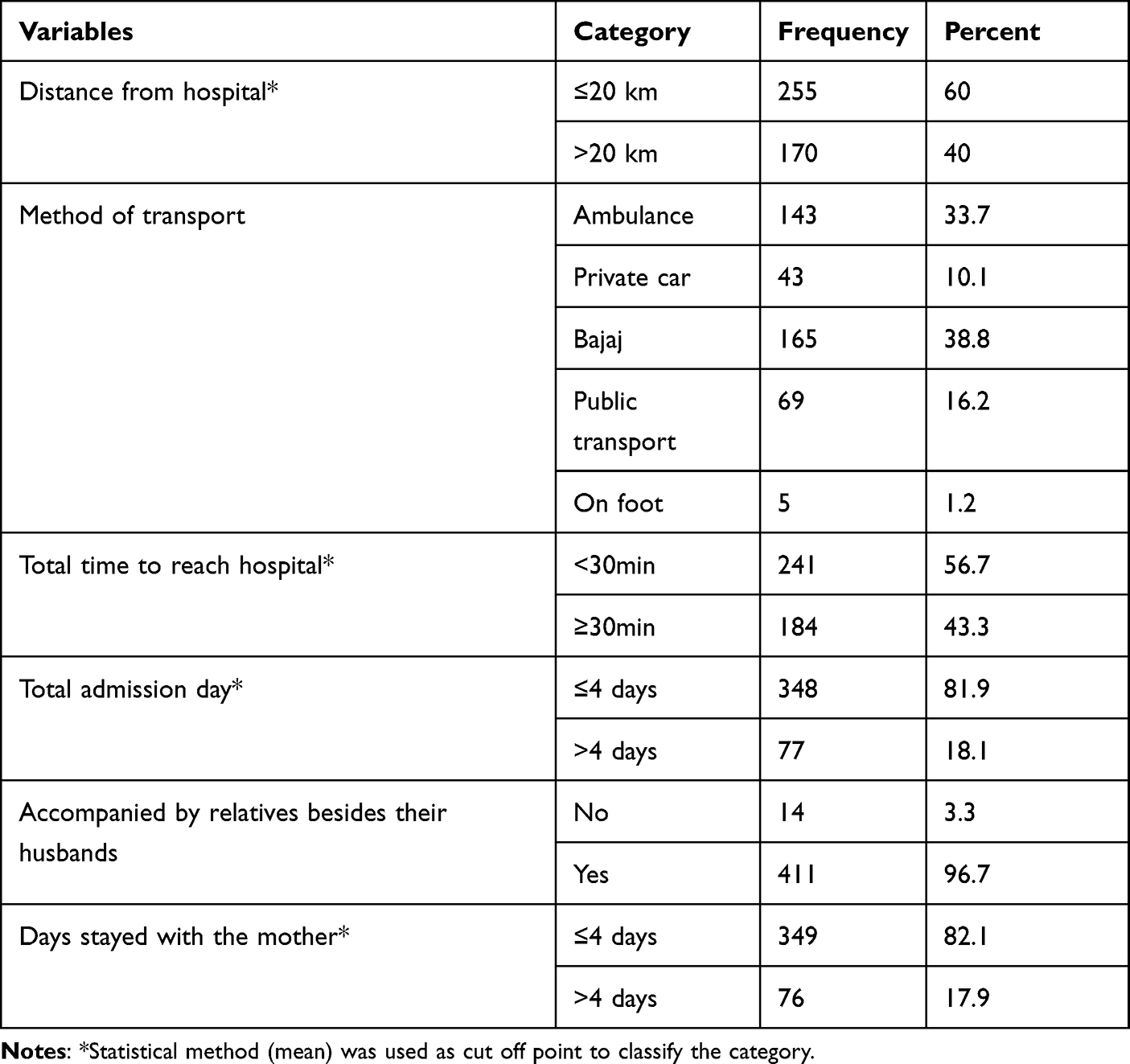 |
Table 3 Institutional Factors Related with Cost of Maternal Complications Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
Clinical Characteristics of the Respondents
When we see the clinical characteristics of mothers, 56% of the respondents were multigravida and 83.1% of them were multiparous. From the total respondents, 43.8% mothers were admitted with obstructed labor, and 65.4% gave birth through caesarian section. Around 80% gave birth to a normal baby and 11.8% end up with dead child (Table 4).
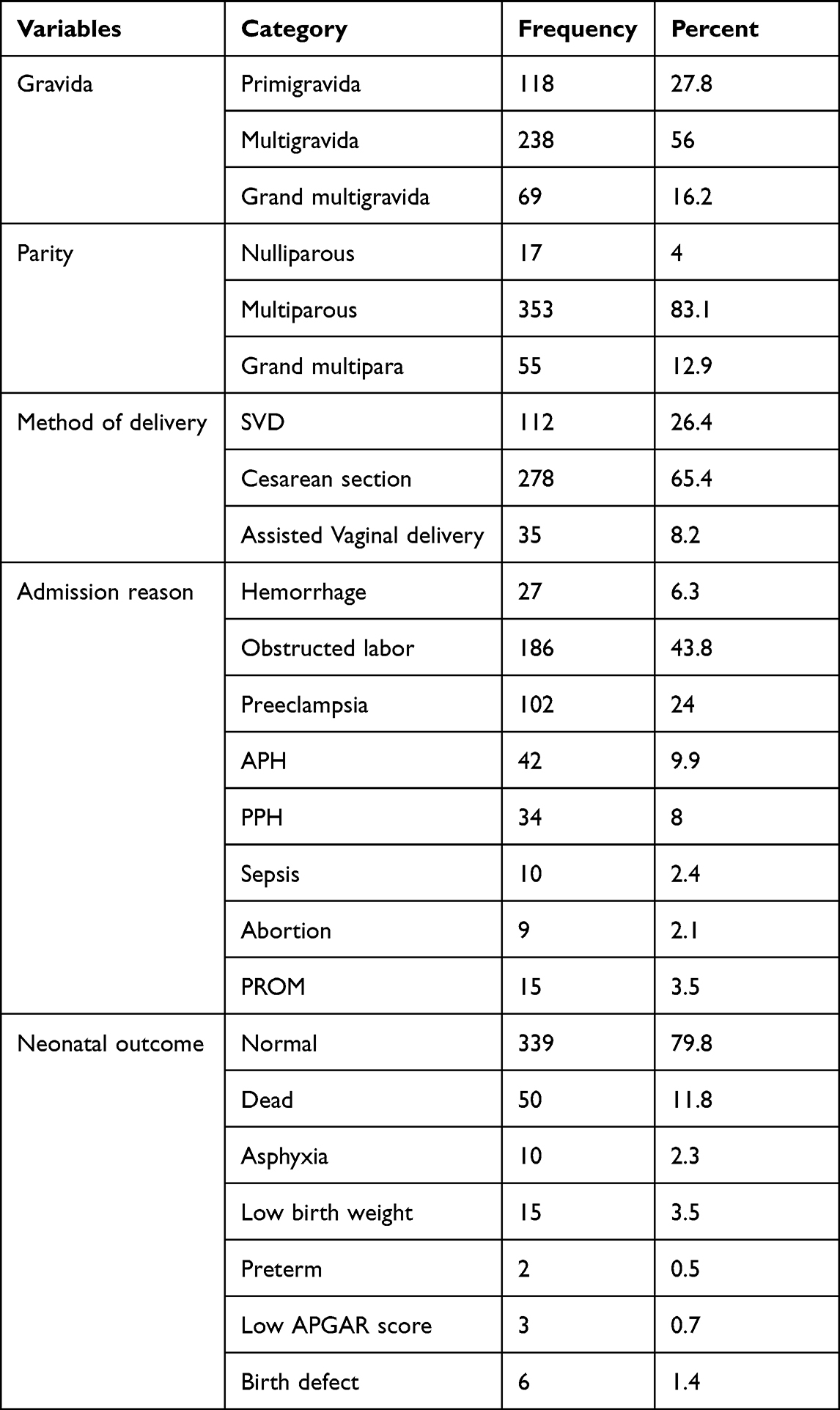 |
Table 4 Clinical Characteristics Related with Mothers with Complications Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
The Cost of Maternal Complications
In this study, the total median (IQR) cost of maternal complications was around 4250 ETB (81.3 USD; IQR = 2900–5833.3), while the median (IQR) direct medical cost incurred by mothers was 1300 ETB (24.9 USD; IQR = 800–1933) and the direct nonmedical cost was 1560 ETB (29.8 USD; IQR = 795–2850). Among the direct nonmedical costs, the median costs of food expense was 800 ETB (15.3 USD), while the drinking expense was 300 ETB (5.7 USD). The median transportation expense was 300 ETB (5.7 USD) and the lodging expenses was 300 ETB (5.7 USD). The Indirect median (IQR) cost was about 800 ETB (15.3 USD; IQR = 400–1400) median productivity loss of the caregivers was around 700 ETB (13.4 USD) (Table 5 and 6).
 |
Table 5 The Costs of Maternal Complication in Mothers with Complications Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
Factors Predicting the Cost of Maternal Complication Among Admitted Mothers
Factors that predict the cost of maternal complications were identified after performing simple linear regression. Factors with a p-value less than 0.25 were entered into a multiple linear regression model. These variables were residence, referral, marital status, education status of the mother and their husbands, husbands occupational status, the total family size of the household, working family members in the household, number of children in the household, family income, distance from the residence, method of transportation used, time taken to reach the hospital, hospital length of stay (HLoS), accompanied by relatives besides their husbands, gravidity, parity, mode of delivery, admission reason, and neonatal outcome.
Among these variables, family income, time taken to reach the hospital, hospital length of stay, accompanied by relatives besides their husbands, mode of delivery, neonatal outcome appeared to be statistically significant at a p-value of <0.05. The model explained about 32.6% (R2 = 0.3261, P < 0.0000) of variance.
Accordingly, holding other variables constant, households with monthly family income of ≥3001 birr have 13% increased cost than those with less income groups (β=1.13; 95% CI: 1.00, 1.26). The cost of maternal complication was decreased by 27% (β=0.73; 95% CI = 0.64–0.83) among women who reached the hospital within 30 minutes compared to those who came longer than 30 minutes.
The cost of mothers admitted for less than 4 days was decreased by 40% than those staying more than 4 days (β=0.60; 95% CI = 0.53–0.69). Additionally, mothers who were accompanied by relatives besides their husbands cost increased by 93% than those who came only with their husbands (β=1.93; 95% CI = 1.52–2.46) and the cost incurred by mothers who had undergone caesarian sections was increased by 17% than those who gave birth through other SVD (β=1.17; 95% CI = 1.04–1.31). Giving birth to a normal baby decreased the cost by 14% than those mothers delivering with different neonatal outcomes (β=0.86; 95% CI = 0.77–0.97) (Table 7)
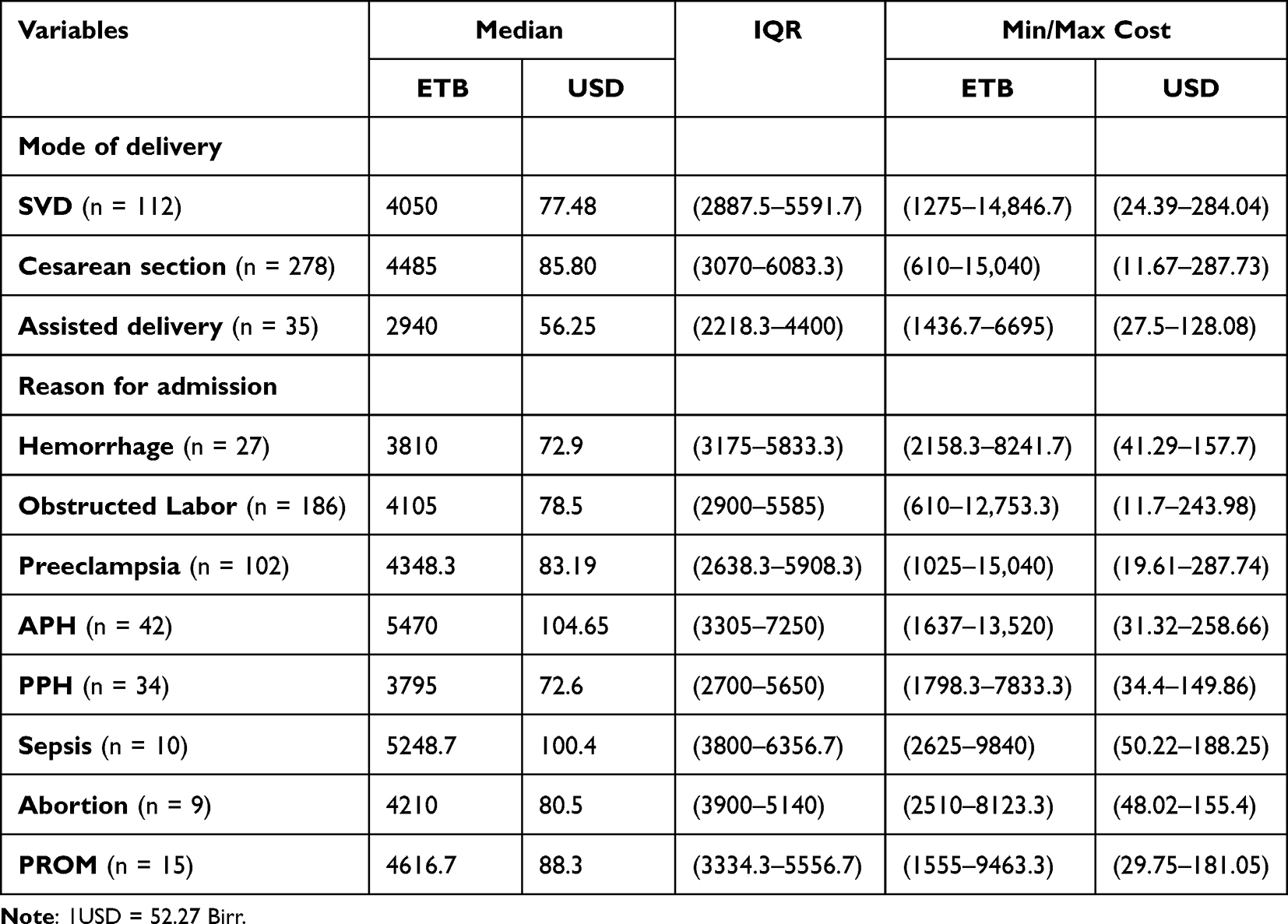 |
Table 6 The Cost of Maternal Complication by Mode of Delivery and by Reason for Admission in Mothers with Complications Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
 |
Table 7 Factors Predicting the Cost of Maternal Complication Among Admitted Mothers Attending Public Hospitals in the Harari Region and Dire Dawa City Administration July 1–31, 2022 (n = 425) |
Discussion
The Ethiopian government is implementing a free service delivery strategy for mothers giving birth at public health institutions. However, the services are not entirely free of charge. Mothers and households are paying out-of-pocket payments, which leads mothers and households to face economic challenges. This study aimed to assess the direct and indirect medical and non-medical costs related with maternal complication, and also identifying predictors of for the cost spent are family income, time it takes to reach hospital, admission days, and mode of delivery, neonatal outcome and caregiver accompanied.
This study reveals that the median total cost of maternal complications was 4250 ETB (81.3 USD; IQR = 2900–5833.3). This result is lower than the study conducted in Southern Ethiopia which reported the median of 95.6 USD,13 including in Bangladesh (261 USD for severe complication and 29 USD for less severe complications)14 and Myanmar (176.8 USD).15 This difference may be explained by the difference in sample size as sample size increases the total cost, and also the types of complications included in these studies were different that may result in increased cost.
On the other hand, the cost in my study is higher compared to the study conducted in Bale Zone Ethiopia, ie, 877.5 ETB (32.03USD),7 Ghana (32.03 USD),16 and Nigeria (ranging from 9 to 99 USD).17 This difference may be due to the recent inflation creating changes in the cost of medications, food, drinking and other related expenses applied to treat these mothers including other services the mothers and caretakers use while they were staying in the hospital. Moreover, the differences in socioeconomic status between and within the countries may contribute to this difference in cost.
In this study, the median direct non-medical cost 1560 (29.8 USD) is higher than the direct medical 1300 ETB (24.9 USD) and indirect medical costs 800 ETB (15.3 USD). This is in line with studies done in Ghana,16 Bangladesh14 and rural Tanzania;18 where the cost of food, drinking and transportation was higher than the direct medical cost. This implies that the medical costs covered by the health system are not exempting mothers of costs associated with maternal health services.
My study result of direct non-medical cost is higher than studies done in Southern Ethiopia (6.5 US),13 Bale Ethiopia (282 0.5 USD),7 Mekelle Ethiopia (609 USD)8 and Ghana (23.35 USD).16 This may be due to the current global market instability because of war and conflicts in Ethiopia and around the world. It affects the cost of food and other supplies, including the covid-19 post pandemic inflation leading to higher price for food and other commodities.
Looking at the median direct medical cost, the median direct medical cost is 1300 ETB (24.9 USD) in this study, which is lower than a study conducted in Mekelle Ethiopia (3480 ETB)8 and Southern Ethiopia (89.1 USD).13 On the other hand, it is higher than studies conducted in Ghana (8.68 USD)16 and Bale Ethiopia (295 ETB) (10.80 USD).7 This shows that there are still some medical costs that are associated with maternal health services delivery covered by out-of-pocket expenditure.
The median indirect cost incurred in this study is 800 ETB (15.3 USD). This cost is lower than the study done in Ethiopia Mekelle (1031 ETB),8 while it is higher than the study conducted in Ethiopia Bale (1291 ETB; 47.11 USD)7 and Ghana (5.2 USD).16 This result implies that the indirect costs that are associated with attending maternal health services are substantially high, and households are being affected by the hidden type of expenditure besides the direct medical and non-medical expenditures.
The median cost of mothers who delivered with the cesarean section (4485 ETB (85.80 USD)) is higher than the cost of other modes of delivery (SVD, assisted delivery). This finding is in line with studies done in Ethiopia Balle7 and Nepal.19 This could be explained by the fact that cesarean section admission is longer and it needs different type of care, which could be costly.
In this study, the cost of APH is 5470 ETB (104.7 USD) and 5248.7 ETB (100.4 USD) for sepsis, which is higher than the cost of other type of complications. On the contrary, the cost of treating preeclampsia was 483.46 USD and abortion was 921 0.74 USD in Myanmar. This difference may be due to the difference in health-care system between the countries, and the cost that is spent to give service for mothers coming with APH and sepsis may differ as their treatment plan includes longer period of admission and a wide range of antibiotics may be needed.
In this study, the cost of maternal complication is predicted by monthly family income (β=1.13; 95% CI = 1.00–1.26). This finding is in line with the studies conducted in Nepal,19 Mekelle Ethiopia,8 and India.20 This shows that as income increases the ability to buy different commodities also increases, which in turn increases the extra cost person spends.
The time to reach the hospital (β=0.73; 95% CI = 0.64–0.82) and total admission days (β=0.60; 95% CI = 0.53–0.69) are also other predictors. This is in line with studies done in Nepal,19 Mekelle Ethiopia,8 Bangladesh14 and Bale Ethiopia7 and India.20 This could reflect that as distance from institution increases, the cost to travel also increases, including the length of stay, which may increase the money spent on different services increases.
In addition, mode of delivery (β=1.17; 95% CI = 1.04–1.31) and caregivers accompanied the mothers besides their husbands (β=1.93; 95% CI = 1.52–2.46) predict the cost of maternal complication positively. This result corresponds with studies done in Nepal19 and Ethiopia Bale.7 It may show that mothers giving birth through caesarian section have longer time of recovery and higher expense than those delivering through SVD. Also, as the number of people who came as caregivers increases, the cost they incur for different non medical services increases which directly increases the cost that is spent during admission time than those mothers who only have their husbands as their caretaker. On the other hand, giving birth to a normal baby (β=0.86; 95% CI = 0.77–0.97) negatively predict the cost of maternal complication. This could be related to the fact that women giving birth to a normal baby may be discharged earlier than those with neonates with different complications, which leads to decreased expenses in their admission time.
This study has limitation in measuring productivity loss, as the monthly/daily income of the mothers and caretakers is hard to measure especially for women who are house wives. Also, there may be bias of over or under estimation of cost paid for the service they get, to tackle this drugs materials bought were asked, listed and the cost was estimated by the data collectors and supervisors using that periods price of medical equipments accordingly.
Conclusion
The result of this study indicates that the cost of maternal complication in mothers admitted within the study area was high. The factors that predicted cost of maternal complication among mothers admitted were family income, time it takes to reach hospital, admission days, mode of delivery, neonatal outcome and caregiver accompanied the mother. The general conclusion of this study is that, despite official claims to the contrary, women and households are paying more for maternity care. Even the direct medical costs are greater, indicating that they are buying medications and other medical supplies from private pharmacies.
Abbreviations
ANC, Antenatal Care; APH, Antepartum Hemorrhage; BSC, Balanced Score Card; CSA, Central Statistical Agency; DMC, Direct Medical Cost; DNMC, Direct non-medical cost; EDHS, Ethiopian Demographic Health Survey; EPHI, Ethiopian Public Health Institute; ETB, Ethiopian Birr; FCA, Friction Cost Approach; IC, Indirect cost; IQR, Interquartile Range; HCA, Human Capital Approach; HFSUH, Hiwot Fana Specialized University Hospital; HLoS, Hospital Length of Stay; MMR, Maternal Mortality Ratio; MOH-E, Ministry of Health – Ethiopia; MPH, Masters of Public Health; NHA, National Health Accounts; OOP, Out of Pocket; PI, Principal Investigator; PIH, Pregnancy Induced Hypertension; PPH, Post-Partum Hemorrhage; PROM, Premature rupture of member; SD, standard deviation; SDG, Sustainable Development Goals; SGS, School of Graduate Studies; SVD, Spontaneous Vaginal Delivery; USD, United States dollar; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee of Haramaya University College of Health and Medical science (HU, IHRERC), with reference number of IHRERC/120/2022, which was in line with Helsinki's declaration. Additionally, permission was obtained from the Dire Dawa City Administration and Harari regional state health beuro. Informed, Written, Voluntary and Signed consent was obtained from each respondent and for those participants below 18 years their husbands/parents/legal guardians gave consent before the interview after informing the respondents. Signed consent forms were stored in a lockable board. Confidentiality of the information collected was maintained by keeping the anonymity of the individual participants at all levels.
Acknowledgments
We would like to extend our gratitude to Haramaya university, College of health and medical sciences for giving us this chance to conduct this research. We also want to thank Dire Dawa City Administration and Harari regional state health beuros and to the community.
Author Contributions
All authors agreed to be held accountable for all aspects of the work and agreed to make a significant contribution to the work reported, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. All authors also participated in the article’s drafting, revision, or critical review and gave final approval of the version to be published. All authors also agreed on the journal to which the article was submitted.
Funding
Haramaya University supported this work. The funders had no role in study design, data collection, and analysis, interpretation of data, the decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO Recommendations on Maternal Health. Geneva: WGR Committee; 2017.
2. Barber SL, Lorenzoni L, Ong P. Price Setting and Price Regulation in Health Care: Lessons for Advancing Universal Health Coverage. World Health Organization; 2019.
3. World Health Organization. Tuberculosis Patient Cost Surveys: A Hand Book. Geneva: World Health Organization; 2017.
4. Shiell A, Donaldson C, Mittonand G. Health economic evaluation. J Epidemiol Community Health. 2002;56:85–88. doi:10.1136/jech.56.2.85
5. World Health Organization. Guide to Identifying the Economic Consequences of Disease and Injury. Geneva, Switzerland: World Health Organization; 2009.
6. FMOH. Ethiopia’s Fifth National Health Accounts Highlight of Major Findings Briefing Notes. Addis Ababa, Ethiopia: Ethiopia Federal Ministry of Health; 2014.
7. Merga M, Debelaand TF, Alaro T. Hidden costs of hospital-based delivery among women using public hospitals in bale Zone, Southeast Ethiopia. J Prim Care Community Health. 2019;10:1–9. doi:10.1177/2150132719896447
8. Abadi T, Mebratie AD. Cost of treating maternal complications and associated factors in Mekelle general hospital, Northern Ethiopia. Risk Manag Healthc Policy. 2021;2021:87–95.
9. World Health Organization, UNICEF. Trends in Maternal Mortality 2000 to 2017. Geneva: World Health Organization; 2019.
10. EPHI. Ethiopia Mini Demographic and Health Survey, Final Report, 2019. Rockville, Maryland, USA: Ethiopian Public Health Institute EPHI and ICF; 2021.
11. FMOH. Household health expenditure and utilisation surveyenha. Addis Ababa: NHA; 2016.
12. World Health Organization. Evaluating the quality of care for severe pregnancy complications; The WHO near-miss approach for maternal health; 2011.
13. Borde MT, Loha E, Johanssonand KA, Lindtjørn B. Financial risk of seeking maternal and neonatal healthcare in southern Ethiopia: a cohort study of rural households. Int J Equity Health. 2020;19. doi:10.1186/s12939-020-01183-7
14. Hoque ME, Powell-Jackson T, Dasgupta SK, Chowdhuryand ME, Koblinsky M. Costs of maternal health-related complications in Bangladesh. J Health Popul Nutr. 2012;30(2):205–212. doi:10.3329/jhpn.v30i2.11315
15. Shwe ID, W. AT, Riewpaiboon A, Chaikledkaewand U, Hackney DN. Treatment cost and costing model of obstetric complications at a hospital in Myanmar. PLoS One. 2019;14(3):e0213141. doi:10.1371/journal.pone.0213141
16. Dalaba MA, Akweongo P, Aborigo RA, et al. Cost to households in treating maternal complications in northern Ghana: a cross sectional study. BMC Health Serv Res. 2015;15. doi:10.1186/s12913-014-0659-1
17. Kalu-Umeh NN, Sambo MN, Idrisand SH, Kurfi AM. Costs and patterns of financing maternal health care services in rural communities in northern Nigeria: evidence for designing national fee exemption policy. Int J MCH AIDS. 2013;2(1):163–172. doi:10.21106/ijma.21
18. Ciaranello AL, Perez F, Engelsmann B, et al. Cost-effectiveness of world health organization 2010 guidelines for prevention of mother-to-child HIV transmission in Zimbabwe. Clin Infect Dis. 2012;56(3):430–446. doi:10.1093/cid/cis858
19. Acharya J, Kaehler N, Marahatta SB, Mishra SR, Subediand S, Adhikari B. Hidden costs of hospital based delivery from two tertiary hospitals in Western Nepal. PLoS One. 2016;11(6):e0157746. doi:10.1371/journal.pone.0157746
20. Govil D, Purohit N, Guptaand SD, Mohanty SK. Out-of-pocket expenditure on prenatal and natal care post Janani Suraksha Yojana: a case from Rajasthan, India. J Health Popul Nutr. 2016;35:15. doi:10.1186/s41043-016-0051-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.