Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Cost of Frontline Nursing: Investigating Perception of Compensation Inadequacy During the COVID-19 Pandemic
Authors Ali H ![]() , Fatemi Y
, Fatemi Y ![]() , Hamasha M
, Hamasha M ![]() , Modi S
, Modi S
Received 18 January 2023
Accepted for publication 20 March 2023
Published 10 May 2023 Volume 2023:16 Pages 1311—1326
DOI https://doi.org/10.2147/JMDH.S402761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Haneen Ali,1,2 Yasin Fatemi,2 Mohammad Hamasha,3 Shikha Modi1
1Health Services Administration Program, Auburn University, Auburn, AL, USA; 2Department of Industrial and Systems Engineering, Auburn University, Auburn, AL, USA; 3Department of Industrial Engineering, Faculty of Engineering, The Hashemite University, Zarqa, Jordan
Correspondence: Haneen Ali, Health Services Administration Program, Auburn University, 351 W Thach Concourse, 7080 Haley Center, Auburn, AL, 36849, USA, Email [email protected]
Background: Nursing professionals experienced greater levels of stress and burnout during the COVID-19 pandemic. Studies examining stress and burnout have found a relationship between compensation and burnout. However, further studies are needed to examine the relationship between the mediating effects of supervisor and community support and coping strategies and the effects of burnout on compensation.
Objective: The purpose of this study is to build on previous burnout research by examining the mediation effects of supervisor and community support and coping strategies on the relationship between sources of stress and burnout on feelings of compensation inadequacy, or the desire for more compensation.
Methods: Using Qualtrics survey responses from 232 nurses, this study used correlation testing and mediation analyses of indirect, direct, and total effects to explore the relationships between critical factors influencing stress, burnout, nurses’ use of coping skills, and the perception of supervisor and community support on perceived compensation inadequacy.
Results: This study found that the support domain has a significant and positive direct effect on compensation, with supervisor support increasing the desire for additional compensation. Support was also found to have a significant and positive indirect effect and a significant and positive total effect on the desire for additional compensation. This study’s results also found that coping strategies had a significant, direct positive effect on the desire for additional compensation. While problem solving and avoidance increased the desire for additional compensation, transference had no significant relationship.
Conclusion: This study found evidence of the mediation effect of coping strategies on the relationship between burnout and compensation.
Keywords: compensation, COVID-19, frontline nursing, support, survey
Introduction
Within the United States, nurse retention remains an ever-growing concern in hospital settings, as deficits in nurse labor are expected to reach over 248,964 full-time employees (FTE) lost by 2030, with the largest shortages in the South.1 Nurse shortages are associated with higher patient mortality, lower nurse performance, and lower job satisfaction.1–4 Burnout has been demonstrated to increase turnover intention, as seen during the recent pandemic.2,3,5–7 As a result, more information is needed to examine what factors help nurses impact their perception of burnout.
Turnover intention is associated with high amounts of stress and workload that are not adequately managed using a work–life balance or adequate rewards.8,9 As a result, hospitals that do not provide adequate compensation and organizational support that facilitates work–life balance will have more difficulty retaining high-quality or highly experienced nurses.8,9 COVID-19 patients present additional work-related stresses for nurses, such as higher patient acuity, higher stress and anxiety, and limited task autonomy.7,10 In addition to work-related stress, frontline nurses face personal risks, such as increased exposure to COVID-19 infection.3,6 Nurses who feel a heightened sense of workload and stress desire additional resources, such as compensation, to account for the additional time and energy used to overcome their perceived labor demands.9,11,12 Factors such as psychosocial and emotionally taxing work6 and inadequate work–life balance9 can lead to a desire for more compensation. However, the extent to which this hypothesized relationship between job demands and compensation is mediated by factors such as organizational support and community and social support remains unclear. Therefore, additional research is required to examine the mediating factors that increase the desire for greater compensation among frontline nurses working in hospitals.
Mediating Effects of Coping and Support on Stress, Burnout, and Compensation
Understanding the factors that mediate the relationship between two variables is important because it can provide insight into how and why the relationship exists.13 In the context of nursing work with COVID patients, understanding the factors that mediate the relationship between nurse burnout and low compensation, for example, can help organizations and policymakers develop effective strategies to address the issue and support the well-being of nurses. The importance of mediation analysis is to better understand the relationship between nurse retention and perception of inadequate compensation. Gottlieb and Zenilman (2020) examined 2018–2020 data from Health Carousel, one of the US’s ten largest healthcare staffing firms, for data on job postings and filled jobs for frontline RNs.14 While COVID-19 was presented in the media as a dangerous virus that disproportionately impacted healthcare workers, the results from Gottlieb and Zenilman (2020) suggest that much of the turnover intention of frontline nurses during this time might have been caused by financial incentives, such as sign-on bonuses and increased salaries offered to nurses willing to leave their current general positions to specialize in caring for COVID-19 patients.14
Additionally, while the importance that compensation can play on outcomes such as turnover intention is apparent,2,7,14,15 the importance of compensation in explaining the relationship between job demands and resources is less clear.16 A 2021 study found that over a third of the 215 frontline nurses listed financial compensation as the least influential stress reliever, while most of the nurses in the study disavowed compensation as a coping mechanism or motivator for the intense emotional strains they experienced.17 This suggests that differences likely exist between the coping strategies frontline nurses use, perceived support, and how those coping strategies and perceptions of support inform a nurse’s feelings of compensation inadequacy.
Coping strategies have been found to reduce the effects on frontline nurse outcomes, such as burnout and stress.5,6,18,19 Coping strategies can take multiple forms, such as problem solving, transference, and avoidance.6,18,19 Problem solving is theorized to increase the feeling of compensation inadequacy due to the higher workload required to overcome challenges using greater job processes and specialized knowledge.6,18,19 By comparison, transference is associated with socially driven approaches to reducing stress and anxiety, as this coping strategy requires nurses to engage in interpersonal communication to transfer the negative feelings associated with their lived experiences.5,6,18,19 Studies also suggest that support reduces the impact of job stress among frontline nurses;3,5–7,10 however, it is unclear to the extent that different types of support influence the desire for additional compensation. As a result, this study seeks to examine the mediating factors in feelings of inadequate compensation to understand what factors impact the desire for additional compensation. Therefore, this study aims to investigate the determinants of perceived compensation inadequacy and determine what mediating effects (if any) exist between the determinants of compensation inadequacy of frontline nurses, the coping strategies used, and the level of support felt at the time.
Materials and Methods
Nurses dealing with COVID-19-infected patients at Alabama hospitals were given a cross-sectional survey to capture their experiences in working on the frontlines. Two hundred thirty-two frontline nurses responded from May 6, 2020 to June 30, 2020. Information about the study and an invitation to participate were disseminated on social media platforms, such as LinkedIn. Nurses who showed interest were also provided with a link to the online survey. Only Alabama frontline nurses who had direct contact with COVID-19 patients in the three months prior to the start of data collection were included in this study.
According to the Declaration of Helsinki, the ethics committee at Auburn University accepted this study (Institutional Review Board [IRB] protocol reference: 20–238 EX 2005). The survey’s objectives and any potential risks were explained to participants, and a consent form was provided. After being made aware that no personally identifying data would be collected, participants volunteered to participate in the study by completing the survey. In exchange for continuing to fill out the survey, participants received $20.
Questionnaire Development
The main items for the questionnaire were based on Lee et al investigation of medical personnel during the 2003 Severe Acute Respiratory Syndrome (SARS) pandemic. Furthermore, a questionnaire created by Cai et al,19 which was used to assess frontline nurses in China, was utilized to create pandemic-specific questions. The questionnaire was also a follow-up to tools developed by Ali et al,5,6 studies that examined what factors influence the stress and burnout symptoms of frontline nurses in Alabama.
Six major domains were used to develop and arrange a total of 68 items: perceived workload, stress, burnout, coping strategies, support, and the desire for additional compensation. A group of subject-matter experts with research experience received this set of questions (two general nurses, four nurses who work in intensive care units (ICUs), two nursing professors, two nurse managers, and one expert in public health). A virtual focus session with a group of experts was convened to discuss the initial list of items after one week. In response to input from the experts, the community support items were revised by rewording three of the items for clarity.
Demographic and work-related questions were included in the questionnaire (seven items). Sixteen items were used to measure the stress experienced by frontline nurses and were broken down into five categories: stress from assignments and workload, stress from taking care of patients, stress from a lack of knowledge about COVID-19, stress from colleagues and personal life, and stress from the environment. 15 items divided into three constructs were used to record frontline nurses’ impressions of burnout: emotional and physical exhaustion, depersonalization, and a lack of personal accomplishment. Fourteen items were used to collect nurses’ perceptions of social support and were separated into two constructs: community/social support and supervisor support. Using 12 items, nurses’ coping mechanisms were recorded and separated into three constructs: avoidance, problem solving, and transference. Lastly, three items were used to capture perceived workload, while one item was used to capture the desire for more compensation. A five-point Likert scale was used to score the perception items (from strongly disagree to strongly agree). In this study, a template for a questionnaire was provided in Table S1.
The survey tool was pilot tested by fifteen nurses working in nearby hospitals who were invited through personal connections. Each construct’s item interrelatedness was evaluated using Cronbach’s alpha, and the constructs’ values were within the acceptable range (α > 0.70).20
Framework
This study’s design employed the job-demands and resource (JDR) model.7,11 The JDR model assumes a relationship between job demand and resources: the greater the job demands, the more resources individuals will need to overcome those demands and avoid burnout.7,11 The JDR model was used to investigate the hypothesized relationship between the mediating factors of social and community support and coping strategies on symptoms such as feelings of compensation inadequacy. This model was used to test whether certain coping strategies helped explain how specific sources of stress translated into burnout and, from there, a desire for more income.
Operationalization of Domain Constructs
Perceived Workload
Perceived workload captures the perceived amount of work frontline nurses experienced during the pandemic’s early months.3,5–7,10,19 Three questions were used to test to what degree that perceived workload, in general, influenced the desire for additional compensation.
Stress from Taking Care of Patients
Frontline nurses experience greater stress from taking care of infected patients.3,5–7,10,19 These questions aimed to identify specific features of stress brought on by daily contact with COVID-19-infected people.
Stress from Nurse Assignments and Workload
Nurse assignments and tasks must remain flexible to ensure that individuals can balance less-preferred tasks with easier-to-manage tasks.3,5–7,10,19 The COVID-19 pandemic created workforce demand issues that restricted the flexibility of nurses in dealing with their daily workloads. This construct was used to test the degree to which the lack of task autonomy influences the desire for additional compensation.
Stress from Colleagues
Working with COVID-19 patients made frontline nurses nervous, but they were also worried about infecting their coworkers.3,5–7,10,18,19 These inquiries were utilized to measure the stress level related to the fear of COVID-19 infections, which would have a negative impact on their personal and professional lives.21
Stress from a Lack of Knowledge
The initial months of the pandemic presented multiple, and often conflicting streams of information related to social distancing and reducing infection.3,5–7,10,18 This construct’s questions were created to investigate if lack of knowledge throughout the pandemic caused confusion22 or stress.
Stress from the Environment
Nurses may have been more stressed about their upcoming or present shift as a result of persistent media coverage of particular concerns, including personal protective equipment (PPE) and ventilator shortages.3,5–7,10,23 This construct’s items of this concept were developed to represent the stress experienced by nurses who felt stress in their working environment. Due to inadequate job resources or medical resources.
Emotional and Physical Exhaustion
High levels of stress have been linked to emotional and physical exhaustion.3,5–7,10,19 Such fatigue is caused by physio-psychosocial exhaustion, such as poor diet, headaches, severe anxiety, and insomnia. Emotional and physical exhaustion were used in this study to measure the perceived levels of discomfort reported by nurses.
Depersonalization
Nurses feeling overwhelming stress may find ways to reduce their risk of stress or fatigue by reducing their efforts3,5–7,10,18 In this study, depersonalization was measured as the degree to which nurses depersonalized or disengaged from their activities.
Lack of Personal Accomplishment
Nurses feeling devalued by their supervisors or from feelings of inadequacy can affect a nurse’s ability to care for their current patients.3,5–7,10,18 This variable was used to test the degree to which feeling a lack of personal accomplishment affected the desire for more compensation.
Supervisor Support
The definition of supervisor support is the unofficial support and advice that frontline nurses receive from their supervisors to deal with stressful circumstances.3,5–7,10,18 This construct was created to investigate the impact of supervisor support on the relationship between the burnout and desire for the compensation.
Community Support
The term “nurse community support” refers to the formal or unofficial assistance that frontline nurses receive from their personal social networks, religious affiliations, and other organizations or support groups outside of their places of employment.3,5–7,10,18 The extent to which frontline nurses used social support outside of the hospital to lessen physical and mental symptoms was assessed using this construct.
Avoidance
Previous studies have observed that nurses reportedly engage in avoidance as a coping strategy by avoiding or withdrawing from a situation or a task that is perceived as a threat.5,18 For example, this construct measures how frontline nurses avoid working overtime to reduce exposure to COVID-19 or media news about COVID-19 and related infection and mortality rates patients rather than participating in types of therapy.
Problem Solving
Nurses engaging in problem solving as a coping strategy use deductive procedures to articulate and reduce the stress that they are experiencing.5,6,18 The frontline nurses’ efforts to identify and treat their sources of stress are measured using the problem-solving construct.
Transference
Nurses engaging in transference use interpersonal interaction to redirect their feelings or emotions from one person or situation to another, this could be done.5,6,18 Nurses could respond to stress by their preferred choice of transference such as religions, friends, and professional help such as psychiatric.24,25
Desire for Additional Compensation
Nurses who feel a desire for additional income perceive that their current compensation does not make up for the time and energy used to accomplish their current job demands.7,11 This study used the desire for more compensation construct as the dependent variable which measures the extent to which frontline nurses desired additional compensation in response changes in their job demands, resources, and support during the initial COVID-19 pandemic.
Statistical Analysis
Data collected from the survey questionnaire were analyzed using various approaches. First, general features of the nurses were examined using descriptive statistics of the demographic data. The Pearson correlation was then used to examine the correlation strength between the domains and compensation. Finally, mediation analysis was conducted to find the relationship between two variables (inputs: perceived workload, stress, and burnout; output: desire for compensation). By examining the indirect effect of one variable on another through mediator (coping strategies and support) variable, we can determine whether the relationship between the two variables is direct or is mediated by other factors.
Results
Descriptive Statistics of Demographic Analysis
Table 1 shows the descriptive analysis of the examined demographic variables. 232 nurses in all answered the study. The analysis showed that 43.5% (n = 101) of the participants were less than 30 years old. Also, the analysis of marital status showed that the percentage of married and single participants was relatively even at 47% (n = 109) and 44.8% (n = 108), respectively. Lastly, more than half of the respondents, 50.8% (n = 118), had less than 10 years of experience. An Analysis of Variance for the demographic and perceptions of compensation was conducted, and it shows that nurses between 41–50 years old (r [230] = −0.808, p = 0.001), having children (r[230] = −0.383, p = 0.010), and OR nurses (r[230] = −0.499, p = 0.008) tend to have less desire for compensation. In addition, female (r[230] = 0.407, p = 0.020) and more experienced nurses (r[230] = 0.902, p = 0.000) tend to have more desire for compensation.
 |
Table 1 Descriptive Statistics |
Correlation Analysis
The Pearson correlations found in Table 2 were used to investigate the relationships between the constructs. The strongest associations, shown in Table 2, were emotional and physical exhaustion, which correlated significantly and positively with depersonalization (r [230] = 0.765, p = 0.000), and a lack of personal accomplishment (r [230] = 0.563, p = 0.000). Next, stress from a lack of knowledge about COVID-19 correlated significantly with depersonalization (r [230] = 0.524, p = 0.000), problem solving as a coping strategy (r [230] = 0.548, p = 0.000), and perceived workload (r [230] = 0.753, p = 0.000). Additionally, stress from assignments and workload correlated significantly with stress from colleagues, staff, and personal life (r [230] = 0.697, p = 0.000) and compensation (r [230] = 0.583, p = 0.000). Stress from taking care of patients had a significant positive correlation with emotional and physical exhaustion (r [230] = 0.517, p = 0.000). Stress from colleagues, staff, and personal life correlated significantly and positively with stress from the environment (r [230] = 0.548, p = 0.000) and emotional and physical exhaustion (r [230] = 0.500, p = 0.000). Lastly, stress from the environment correlated significantly with emotional and physical exhaustion (r [230] = 0.547, p = 0.000) and lack of personal accomplishment (r [230] = 0.617, p = 0.002).
 |
Table 2 Pearson Correlation Analysis- Constructs |
Mediation Analysis
Figure 1 shows the mediation analysis model, which includes the relationships between the domains. As the model represents, perceived workload, stress, and burnout were the inputs, support, and coping strategies were the mediators, and compensation was the response variable.
 |
Figure 1 The framework. |
Table 3 represents the direct effects of the different domains. As Table 3 shows, the largest direct relationship was significant and positive between burnout and coping strategies (b = 0.8564, p = 0.000). Next, burnout, support, and coping strategies had significant and positive direct relationships with compensation (b = 0.6921, p = 0.000; b = 0.8134, p = 0.000; and b = 0.5401, p = 0.000, respectively). The direct relationship was significant, and the positive relationship between stressors and burnout was significant (b = 0.5728, p = 0.000). Lastly, there was a significant and positive direct relationship between perceived workload and stressors (b = 0.233, p = 0.000).
 |
Table 3 Bootstrapping Results for the Direct Relationships Between the Domains |
The direct effect between the constructs. Table 4 shows the direct effects of the different constructs.
 |
Table 4 Bootstrapping Results for the Direct Relationships Between the Constructs |
The direct relationship was also applied to test the relationship between burnout as both a domain and mediator construct, as well as between the mediator constructs and compensation, as shown in Table 4. The analysis shows that burnout as a domain had a significant direct and positive relationship with all the coping strategy constructs: avoidance (b = 0.6657, p = 0.000), transference (b = 0.2592, p = 0.028), and problem solving (b = 1.6445, p = 0.000). Burnout also had a significant and negative direct effect on social support (b = −0.1735, p = 0.026). The direct relationship between compensation and avoidance, and between compensation and problem solving were significant and positive (b = 0.3370, p = 0.000; b = 0.2411, p = 0.000, respectively). Compensation and supervisor support had a significant and positive direct relationship (b = 0.65, p = 0.000).
The direct relationship between the burnout constructs and the coping strategies constructs showed that depersonalization, emotional and physical exhaustion, and lack of accomplishment had a significant and positive direct relationship with avoidance (b = 0.444, p = 0.000; b = 0.5040, p = 0.0008; and b = 0.4886, p = 0.0033, respectively). The results also show significant and positive direct relationships between emotional and physical exhaustion and problem solving (b = 1.617, p = 0.000) and lack of accomplishment and transference (b = 0.2275, p = 0.016).
The investigation between the stress constructs and burnout constructs showed that there was a significant and positive direct relationship between emotional and physical exhaustion and stress from taking care of patients, stress from assignments and workload, and stress from colleagues and personal life (b = 0.3100, p = 0.000; b = 0.3245, p = 0.000; and b = 0.5377, p = 0.000, respectively). Stress from a lack of knowledge about COVID-19 and depersonalization had a significant direct relationship (b = 0.7884, p = 0.000). Stress from the environment and lack of personal accomplishment also have a direct relationship (b = 0.7454, p = 0.000).
The direct relationship between compensation and avoidance and problem solving was significant and positive (b = 0.3370, p = 0.000; b = 0.2411, p = 0.000, respectively). Compensation and supervisor support had a significant and positive direct relationship (b = 0.65, p = 0.000). There was also a significant direct relationship between compensation and depersonalization (b = 0.5452, p = 0.0009) and lack of accomplishment (b = 0.5407, p = 0.0017).
The direct relationships between burnout and supervisor support, stress from the environment and emotional and physical exhaustion, transference and compensation, community support and compensation, and emotional and physical exhaustion and compensation were not significant.
Indirect Effect Between Domains
The relationships between the mediators and the response variables can be analyzed as either serial or parallel. When there are X, Y, and a mediator, the effect of X on Y can be defined by the average direct effect (ADE) and the average causal mediation effects (ACME). ADE shows the linear relationship between the input and output, while there is a mediator. ADE is not the only relationship between X and Y; ACME shows the indirect relationship between X and Y, while there is a mediator. The sum of ACME and ADE is the total effect. In the analysis, ADE shows the direct effect, and ACME represents the indirect relationship.
This type of analysis could show that if there is burnout among nurses, mediators including coping strategies and support could positively or negatively affect compensation.
Applying three packages in R-Studio, named mediation, MeMoBootR, and Process, the indirect relationship between the domains was implemented. The packages’ results reveal two terminologies: ADE and ACME.
Parallel Mediators
Figures 2 and 3 show the relationship between burnout and compensation, while the mediators are support and coping strategies.
 |
Figure 2 The direct relationship between X and Y, while coping strategies are the mediator. |
 |
Figure 3 The direct relationship between X and Y, while support is the mediator. |
Table 5 represents the indirect relationships between the domains, while coping strategies are the mediator. The total effect, the relationship between X and Y without considering the mediator, was (b = 0.6921, p = 0.000). ADE, the direct effect of burnout on compensation after considering the mediation effect of coping strategies, was not significant (b = 0.313, p = 0.18). Finally, ACME, which shows an indirect effect of burnout on compensation, was significant (b = 0.380, p = 0.000).
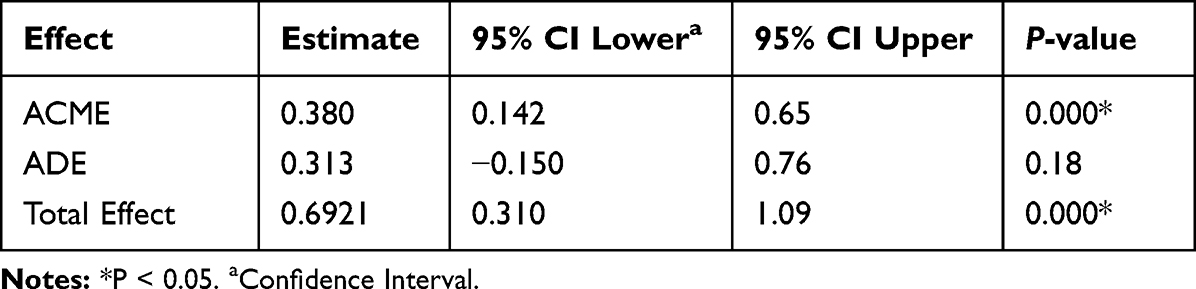 |
Table 5 Nonparametric Bootstrap Confidence Intervals with the Percentile Method, Size 232, Simulation 5000, Mediator: Coping Strategies |
Table 6 shows the total effect between burnout and compensation, while support was the mediator (b = 0.6921, p = 0.000). The ADE of burnout on compensation after considering the mediation effect of support was significant (b = 0.7856, p = 0.000). Finally, ACME was not significant (b = −0.0934, p = 0.130).
 |
Table 6 Nonparametric Bootstrap Confidence Intervals with the Percentile Method, Size 232, Simulation 5000, Mediator: Support |
Table 7 shows the total effect between burnout and compensation, while coping was the mediator. The results showed that the total effect (c) of burnout on compensation was significant (b = 0.6921, p = 0.0012). Burnout significantly predicted coping strategies (a2), (b = 0.8655, p = 0.000). Both mediators, support and coping strategies, significantly predicted compensation (b = 0.8611, p = 0.000) and (b = 0.4075, p = 0.004), respectively.
 |
Table 7 Analysis of Serial Mediators’ Model, Size 232, Simulation 5000 |
Table 8 shows a summary of the indirect relationships between the domains.
 |
Table 8 Indirect Relationship Summary (X: burnout, mediators: support and coping strategies, Y = compensation) |
Mediators are serial, which means that the factors affecting compensation can be linked to a causal chain. Additionally, Figure 4 shows that the mediators are serial, so the mediators could affect the response variable in three ways: m1, m1m2, and m2. M1 and m2 are support and coping strategies, respectively.
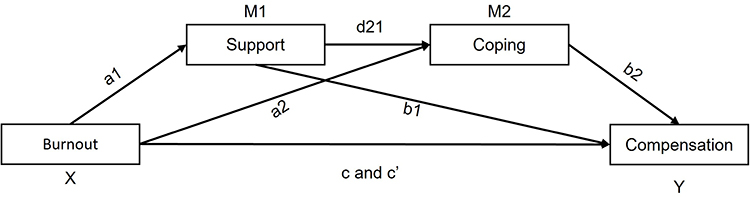 |
Figure 4 Serial mediators. |
Note that the total effects are equal to the sum of the direct and indirect effects. Indirect effects include indirect effects through m1, m2, and m1 and m2. The indirect effect of X on Y was significant only through coping strategies (b = 0.3490, [Lower limit confidence interval (LLCI) = 0.1195, Upper limit confidence interval (ULCI)= 0.6020]).
Serialized and parallel mediation was implemented to further investigate the indirect relationship between different variables and compensation.
Table 9 shows the indirect relationships between X = depersonalization, mediator = avoidance, and Y = compensation.
 |
Table 9 Nonparametric Bootstrap Confidence Intervals with the Percentile Method, Size 232, Simulation 5000, Mediator: Avoidance |
The total effect between depersonalization and compensation, while avoidance was the mediator, was significant (b = 0.5721, p = 0.0056). The ADE of depersonalization on compensation after considering the mediation effect of avoidance was significant (b = 0.4262, p = 0.0148). Finally, ACME was also significant (b = 0.1460, p = 0.0036).
Table 10 shows the indirect relationships between X = stress, mediator = exhaustion, and Y = compensation.
 |
Table 10 Nonparametric Bootstrap Confidence Intervals with the Percentile Method, Size 232, Simulation 5000, Mediator: Exhaustion |
The total effect between stress and compensation, while exhaustion was the mediator, was significant (b = 0.5933, p = 0.022). The ADE of stress on compensation after considering the mediation effect of exhaustion was significant (b = 2.755, p = 0.000). Finally, ACME was also significant (b = −2.1619, p = 0.0036).
Table 11 shows the parallel indirect relationship between stress from a lack of knowledge and compensation, while the mediators were avoidance and depersonalization. The analysis showed that the indirect effect between X and Y was significant through avoidance (b = 0.1366, [LLCI = 0.0007, ULCI = 0.3002]).
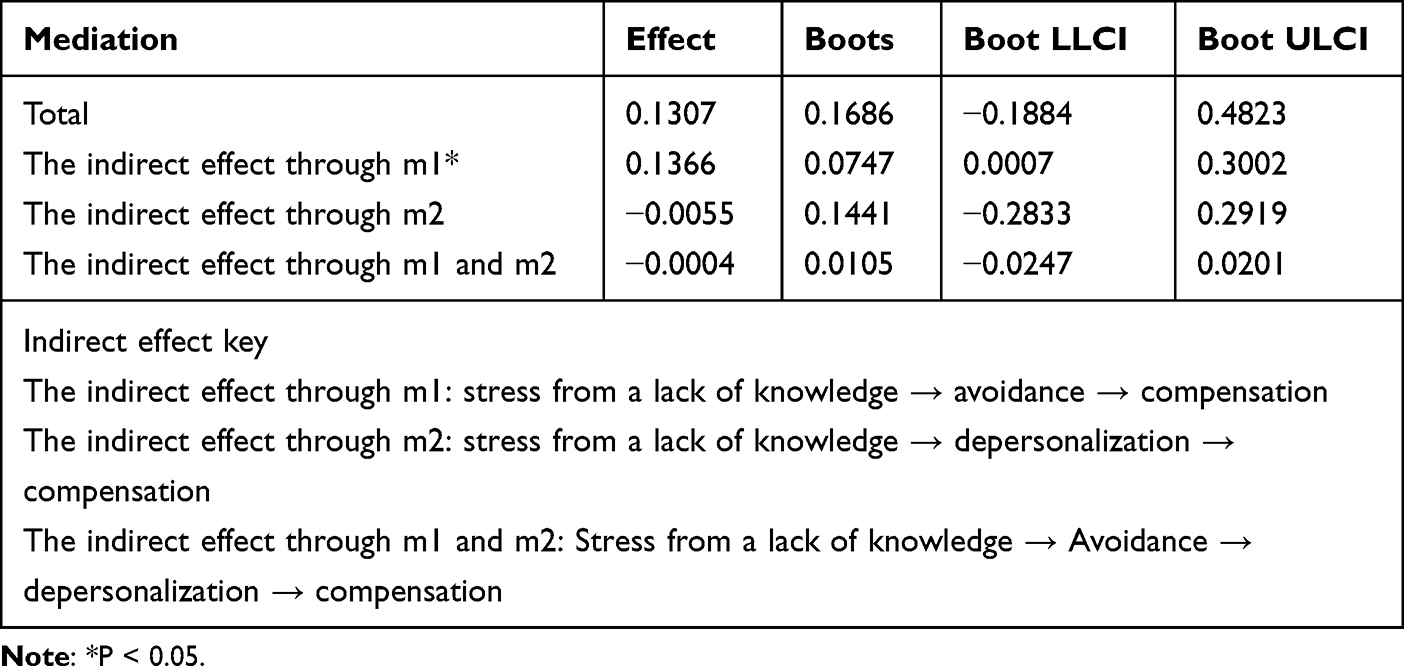 |
Table 11 Indirect Relationship Summary (X: Stress from a lack of knowledge, mediators: Avoidance and depersonalization, Y = compensation) |
Table 12 shows the parallel indirect relationship between stress from a lack of knowledge and compensation, while the mediators were burnout and supervisor support. The analysis showed that the indirect effect between X and Y was significant through supervisor support (b = 0.1881, [LLCI = 0.0551, ULCI = 0.3570]).
 |
Table 12 Indirect Relationship Summary (X: Stress from a lack of knowledge, mediators: burnout and supervisor support, Y = compensation) |
Table 13 shows the relationship between X = stress from a lack of knowledge, Y = compensation, mediator 1 = physical and emotional exhaustion, and mediator 2 = avoidance. The indirect effect between X and Y was significant through avoidance (b = 0.1265, [LLCI = 0.0101, ULCI = 0.2805]).
 |
Table 13 Indirect Relationship Summary (X: Stress from a lack of knowledge, mediators: emotional and physical exhaustion and avoidance, Y = compensation) |
Discussion
Task Assignment and Depersonalization
This study’s Pearson correlation analysis in Table 2 found a strong relationship between task assignment and workload and stress from colleagues, staff, personal life, and compensation. Job flexibility and task autonomy are crucial tools that help nurses find a work–life balance.3,5–7,10 A lack of flexibility and task autonomy can increase the perceived workload of nurses and thereby increase the perceived need for compensation.
In addition, this study found evidence of a relationship between depersonalization and a lack of knowledge about COVID-19, as well as a lack of knowledge and emotional and emotional and physical exhaustion. It can be inferred that the fast-changing nature of information related to the COVID-19 pandemic, coupled with the immediate concerns about patient acuity, frontline nurses were likely to feel the desire to disengage from their tasks More data may be required to evaluate this relationship. Interestingly, a lack of knowledge about COVID-19 also correlated strongly with problem-solving coping strategies. This study’s results suggest that while some nurses felt the need to disengage from their frontline tasks, other nurses refocused their attention on ways to mitigate their sources of stress.5,6,18 Further research is needed to understand possible linear relationships between a perceived lack of knowledge and depersonalization, as well as what factors encourage problem-solving strategies when individuals lack knowledge.
Stress, Burnout, and Compensation
This study’s mediation analysis found that burnout had a significant direct effect on frontline nurse’s desire for additional compensation. This evidence suggests that frontline nurses who felt a heightened sense of workload and stress desired additional resources to compensate for the extra time and energy they used to overcome. Moreover, this study found evidence that the desire for additional compensation increased as their level of burnout increased.9 The desire for additional resources in response to additional perceived workloads has been observed in works examining the JDR model.5,7,11 However, the indirect relationship between stress, burnout, and compensation remains unclear. As a result, further information is needed to better understand which symptoms of burnout contribute to the desire for more compensation.
Mediation of Support and Coping Strategies
By identifying the specific mediators that were responsible for the relationship between two variables, we could develop targeted interventions that focused on those mediators and were more likely to be effective in producing the desired outcome. This study found that support, in general, has a significant and positive direct effect on compensation, with supervisor support increasing the desire for additional compensation. Support was also found to have a significant and positive indirect effect and a significant and positive total effect on the desire for additional compensation. On the one hand, supervisor support is expected to provide frontline nurses with guidance and a chain of command to inform their overall decision making. On the other hand, a hierarchical relationship between supervisor and nurse could create opportunities for micromanagement and, thereby, instances where nurses feel increased expectations of their overall performance.3,10,11 The increased expectations of their overall performance could result in additional stress pertaining to nurses’ job demands rather than provide the nurse with organizational resources to help mitigate their stress. This would be counterintuitive to the support that the nurses are expecting to receive from their supervisors. More information is needed to understand the extent to which supervisor interactions help encourage or support frontline nurses and how this may impact the desire for additional compensation.
This study’s results also found that coping strategies significantly and positively affected the desire for additional compensation. Moreover, coping strategies appear to have a nuanced influence on the desire for additional compensation, which varies based on the strategy. Table 3 shows that the mediation effects of coping strategies varied based on the strategy. While problem solving and avoidance increased the desire for additional compensation, transference had no significant relationship. The very nature of transference as a coping strategy suggests that, rather than seeking tangible goods to distract oneself or to compensate for job demands, the individual is seeking a form of interpersonal support.5,6,18 As a result, a lack of a significant relationship between transference and the desire for additional compensation is expected. However, more information is needed to verify whether transference has the potential to decrease the desire for additional compensation under certain circumstances.
The indirect analyses found in Tables 8–13 suggest that while support and coping strategies indirectly affect the desire for additional compensation, this study, was unable to explain other measures such as avoidance as a stress coping strategy. While this study found a significant and positive indirect relationship between stress from a lack of knowledge, emotional and physical exhaustion, and the desire for additional compensation, it was not able to identify the significance of coping strategies, such as avoidance and problem solving, in a serialized model. Similarly, while this study discovered that the indirect relationship between the stress from a lack of knowledge about COVID-19, avoidance, and the desire for additional compensation was significant and positive, we found a significant indirect relationship with sources of burnout, such as exhaustion, and strategies for coping, such as problem solving and avoidance, acting as mediators on the relationship between the lack of knowledge and the desire for additional compensation.
One factor that has drawn little attention in current frontline nurse scholarship is the concept of intrinsic motivation as a determinant of nurse resilience.3,7,10 Additional variables must be considered to examine what factors related to nurses’ intrinsic motivations are associated with coping strategies used in response to sources of stress and burnout. A future study can use the insights from this analysis to test the implications of whether such relationships between motivations and coping strategies reduce the desire for additional compensation.
Limitations
Gender and ethnicity could not be tested empirically using the current sample. A future study that captures a more diverse nurse population would be necessary to test whether nurses of different genders or ethnicities have different compensation inadequacy levels.
Conclusion
This study found evidence of the mediation effects of coping strategies on the relationship between burnout and compensation. This study’s findings largely support the theory proposed by the JDR model that nurses can perceive how organizational resources should be used to address their current job demands (Demerouti et al, 2001). However, further research is needed to tease out the causal mechanisms that would explain what factors help to influence the way nurses perceive supervisor support. Additionally, more research is needed to examine the implications of feelings of depersonalization and avoidance as coping strategies for professional outcomes, such as the desire for additional compensation and turnover intentions. Longitudinal methods could provide more comprehensive research, that allows an understanding of the degree and direction of changes in perceptions of supervisor support over time, track changes in feelings of depersonalization and avoidance over time, and identify their effects on professional outcomes, such as compensation and turnover intentions. This will allow researchers to identify which factors may influence these outcomes, such as job demands, job resources, and support, in addition to job satisfaction.
Acknowledgment
The authors would like to thank Auburn University for supporting this research project. The study was funded through Dr. Ali’s (corresponding author) start-up funds.
Disclosure
The authors have no conflicts of interest to disclose.
References
1. Zhang X, Tai D, Pforsich H, Lin VW. United States registered nurse workforce report card and shortage forecast: a revisit. Am J Med Qual off J Am Coll Med Qual. 2018;33(3). doi:10.1177/1062860617738328
2. Labrague LJ, McEnroe-Petitte DM, De Los Santos JAA, Edet OB. Examining stress perceptions and coping strategies among Saudi nursing students: a systematic review. Nurse Educ Today. 2018;65:192–200. doi:10.1016/j.nedt.2018.03.012
3. Labrague LJ, De Los Santos JAA. COVID-19 anxiety among front-line nurses: predictive role of organisational support, personal resilience and social support. J Nurs Manag. 2020;28(7):1653–1661. doi:10.1111/jonm.13121
4. Yang YT, Mason DJ. COVID-19’s impact on nursing shortages, the rise of travel nurses, and price gouging. Health Aff Forefr. 2022. doi:10.1377/forefront.20220125.695159
5. Ali H, Fatemi Y, Ali D, Hamasha M, Hamasha S. Investigating frontline nurse stress: perceptions of job demands, organizational support, and social support during the current COVID-19 pandemic. Front Public Health. 2022;10:839600. doi:10.3389/fpubh.2022.839600
6. Ali H, Cole A, Ahmed A, Hamasha SD, Panos G. Major stressors and coping strategies of frontline nursing staff during the outbreak of coronavirus disease 2020 (COVID-19) in Alabama. J Multidiscip Healthc. 2020;13. doi:10.2147/JMDH.S285933
7. Cole A, Ali H, Ahmed A, Hamasha M, Jordan S. Identifying patterns of turnover intention among Alabama frontline nurses in hospital settings during the COVID-19 pandemic. J Multidiscip Healthc. 2021;14:1783–1794. doi:10.2147/JMDH.S308397
8. Holland P, Tham TL, Sheehan C, Cooper B. The impact of perceived workload on nurse satisfaction with work-life balance and intention to leave the occupation. Appl Nurs Res ANR. 2019;49. doi:10.1016/j.apnr.2019.06.001
9. Leiter MP, Maslach C. Nurse turnover: the mediating role of burnout. J Nurs Manag. 2009;17(3):331–339. doi:10.1111/j.1365-2834.2009.01004.x
10. Labrague LJ, De Los Santos JA, Falguera CC, et al. Predictors of nurses’ turnover intention at one and five years’ time. Int Nurs Rev. 2020;67(2):191–198. doi:10.1111/inr.12581
11. Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. doi:10.1037/0021-9010.86.3.499
12. Pertiwi NKAY, Supartha IWG. The effect of compensation and organizational commitment on employee satisfaction and retention. Am J Humanit Soc Sci Res. 2021;1:333–342.
13. MacKinnon DP, Fairchild AJ. Current directions in mediation analysis. Curr Dir Psychol Sci. 2009;18(1):16. doi:10.1111/j.1467-8721.2009.01598.x
14. Gottlieb JD, Zenilman A. When Workers Travel: Nursing Supply During COVID-19 Surges. National Bureau of Economic Research; 2020.
15. Sharif Nia H, Arslan G, Naghavi N, et al. A model of nurses’ intention to care of patients with COVID-19: mediating roles of job satisfaction and organisational commitment. J Clin Nurs. 2021;30(11–12). doi:10.1111/jocn.15723
16. Weninger Henderson M. The economic case for meeting employees’ needs. J Nurs Manag. 2020;28(1). doi:10.1111/jonm.12897
17. Al Muharraq EH. The psychological impact of coronavirus disease 2019 on nurses in Saudi Arabia and their coping strategies. SAGE Open Nurs. 2021;7:23779608211011320. doi:10.1177/23779608211011322
18. Babore A, Lombardi L, Viceconti ML, et al. Psychological effects of the COVID-2019 pandemic: perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020;293:113366. doi:10.1016/j.psychres.2020.113366
19. Cai H, Tu B, Ma J, et al. Psychological impact and coping strategies of frontline medical staff in Hunan between January and March 2020 during the outbreak of coronavirus disease 2019 (COVID‑19) in Hubei, China. Med Sci Monit Int Med J Exp Clin Res. 2020;26:e924171. doi:10.12659/MSM.924171
20. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53. doi:10.5116/ijme.4dfb.8dfd
21. Sarfraz M, Ji X, Asghar M, Ivascu L, Ozturk I. Signifying the relationship between fear of COVID-19, psychological concerns, financial concerns and healthcare employees job performance: a mediated model. Int J Environ Res Public Health. 2022;19(5). doi:10.3390/ijerph19052657
22. Qutishat M, Abu Sharour L, Al-Dameery K, Al-Harthy I, Al-Sabei S. COVID-19-related posttraumatic stress disorder among Jordanian nurses during the pandemic. Disaster Med Public Health Prep. 2021;1–8. doi:10.1017/dmp.2021.199
23. Nantsupawat A, Kunaviktikul W, Nantsupawat R, Wichaikhum OA, Thienthong H, Poghosyan L. Effects of nurse work environment on job dissatisfaction, burnout, intention to leave. Int Nurs Rev. 2017;64(1):91–98. doi:10.1111/inr.12342
24. Shorey S, Chan V. Lessons from past epidemics and pandemics and a way forward for pregnant women, midwives and nurses during COVID-19 and beyond: a meta-synthesis. Midwifery. 2020;90:102821. doi:10.1016/j.midw.2020.102821
25. Seyedfatemi N, Tafreshi M, Hagani H. Experienced stressors and coping strategies among Iranian nursing students. BMC Nurs. 2007;6(1):11. doi:10.1186/1472-6955-6-11
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.