Back to Journals » Journal of Pain Research » Volume 16
The Cortical Bone Trajectory Screw Technique Assisted by the Mazor Renaissance Robotic System as a Salvage Strategy for Failed Lumbar Spine Surgery: Technical Note and Case Series
Authors Han J ![]() , Guo J
, Guo J ![]() , Ma X, Zhang G, Han S
, Ma X, Zhang G, Han S ![]() , Zhang H
, Zhang H ![]() , Liu H
, Liu H ![]() , Chen M, Wang Y
, Chen M, Wang Y ![]()
Received 16 June 2023
Accepted for publication 21 August 2023
Published 29 August 2023 Volume 2023:16 Pages 2971—2980
DOI https://doi.org/10.2147/JPR.S423058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rushna Ali
Jialuo Han, Jianwei Guo, Xuexiao Ma, Guoqing Zhang, Shuo Han, Hao Zhang, Houchen Liu, Mingrui Chen, Yan Wang
Department of Spinal Surgery, the Affiliated Hospital of Qingdao University, Shandong, People’s Republic of China
Correspondence: Yan Wang, Department of Spinal Surgery, the Affiliated Hospital of Qingdao University, No. 59 Haier Road, Qingdao, Shandong, 266000, People’s Republic of China, Tel +86 17853297089, Email [email protected]
Purpose: The objective of this study was to describe the Mazor Renaissance robotic system-assisted CBT (cortical bone trajectory) screw technique as a salvage strategy for failed lumbar spine surgery.
Patients and Methods: Between January 2018 and June 2022, 7 patients underwent salvage surgery with the CBT screw fixation technique assisted by the Mazor Renaissance robot system in our institution. Intraoperative observations were recorded for blood loss, duration of operation, and fluoroscopy time. Complications related to CBT screws were also recorded. The accuracy of CBT screws was recorded in accordance with the modified Gertzbein-Robbins classification. The JOA (Japanese Orthopedic Association) score for low back pain was used to evaluate surgical outcomes.
Results: A total of 26 CBT screws were placed in 7 patients, including 4 females and 3 males. Three patients underwent ASD (adjacent segment disease) and four patients underwent lumbar union failure with loose or compromised PSs (pedicle screws). The mean operation time was 129.29 ± 32.97 minutes, the mean blood loss was 180 ± 52.60 mL, and the mean intraoperative fluoroscopy time was 14.29 ± 3.15 s. All screws were clinically acceptable according to the Gertzbein-Robbins classification. There were no complications related to CBT screws in any of the cases. The JOA scores for low back pain of all patients were significantly improved at the final follow-up.
Conclusion: The CBT screw fixation technique supplemented the traditional PS fixation technique, which can be performed as a salvage strategy for failed lumbar spine surgery and achieved good clinical results. The spinal robot was very helpful in evaluating pedicle size and determining CBT screw direction, especially in a previously instrumented lumbar pedicle.
Keywords: CBT screw, robot-assisted, salvage strategy, ASD
Introduction
The pedicle screw (PS) fixation technique is one of the most common procedures in lumbar fusion surgery. However, the PS fixation technique often leads to problems due to screw loosening and pullout in osteoporotic patients, which often causes insufficient strength of pedicle screw fixation and further internal fixation failure.1 In addition, while performing revision surgery for adjacent segment degenerative diseases, it is often necessary to extensively expose the entire previous wound and remove all of the previous hardware, so this technique has certain limitations in clinical applications.1,2
Santoni et al3 first proposed the cortical bone trajectory (CBT) screw fixation technique for the surgical treatment of lumbar spondylosis with osteoporosis, spinal deformities, spinal infections, and revision surgery for the failure of lumbar fusion. The CBT screw fixation technique improves fixation strength by increasing the contact surface of the screw with cortical bone, and the CBT procedure is minimally invasive.4,5 However, the CBT method is technically challenging and requires multiple fluoroscopies during the process of CBT trajectory preparation.6,7 Moreover, the learning curve of the CBT fixation technique is long, and the technical difficulty of the CBT method is greatly increased when the anatomical structure of the pedicle is abnormal or the direction of CBT screws must be adjusted in revision surgery to avoid attachment to previous pedicle screws.2,6,7 Improving the precision of screw placement is a technical difficulty that urgently needs to be addressed in CBT screw application.
As robotic spinal surgery has become widely used, the advantages of a relatively short learning curve, high accuracy of robot-assisted screw placement, and short radiation exposure time have been highlighted.8–12 In view of this, this study presented an analysis of the clinical data of 7 cases treated by the CBT screw fixation technique as a salvage strategy with the help of the Mazor Renaissance robot system to evaluate the therapeutic effect of this technique for failed lumbar spine surgery.
Materials and Methods
From January 2018 to June 2022, 7 patients who underwent salvage surgery with the CBT screw fixation assisted by the Mazor Renaissance robot system in our institution were included. The diagnosis was confirmed by clinical symptoms and imaging findings. All procedures were performed by the same team of experienced surgeons. The details of the 7 patients are given in Table 1.
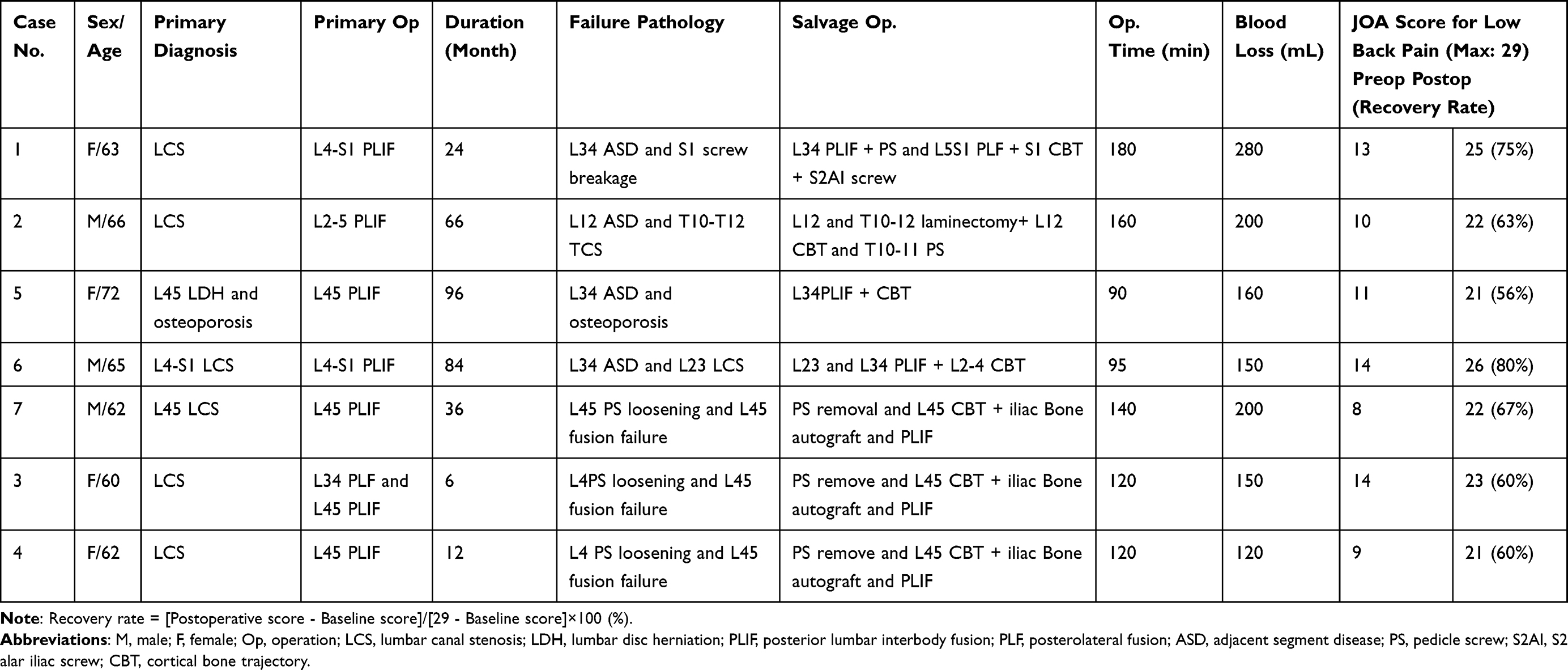 |
Table 1 Patient Basic Information and Clinical Parameters |
Data Collection
Intraoperative observations were recorded for blood loss, duration of operation, and fluoroscopy time. Complications related to CBT screws, such as inadequate screw holding, pedicle or isthmus splitting, and surrounding nerve or dural sac injury, were also recorded.
Immediate postoperative x-ray and CT scans were used to observe the accuracy of CBT screw insertion and the accuracy of CBT screws were recorded in accordance with the modified Gertzbein-Robbins classification13 (grade A, no breach or deviation; B, breach <2 mm; C, 2 mm < breach ≤4 mm; D, breach >4 mm). Screw grades A and B were considered clinically acceptable, and screw grades C and D were defined as malposition. The JOA score for low back pain14 was used to evaluate surgical outcomes at the final follow-up. The mean follow-up duration was 24.43 months (with a range of 8–46 months).
Surgical Procedures
All patients underwent thin-slice CT scanning (0.625-mm thick) of the surgical site before surgery. The original CT data (Dicom format) were imported into the specialized software of the spinal robot (Mazor Renaissance, Israel) for preoperative design. The ideal length, diameter, insertion point, and angle of the CBT screw were set on the corresponding CT sagittal, coronal, and cross-sectional images of the surgical segment.
Patients underwent successful general anesthesia and were placed prone on a robot-assisted specialized operating table. After mounting the spinous fixation needle and the multidirectional bridge platform a 3D positioning device was fixed. Anteroposterior and oblique fluoroscopy was performed under the C-arm, and fluoroscopic data were transferred into the spine robot. Subsequently, the fluoroscopic data were matched with preoperative CT data in a single vertebral registration fashion, followed by error rating and minor adjustments of individual nail tract positions.
Then, the terminal robot was guided precisely to a predetermined position according to the preoperative plan, with subsequent placement of a mechanical arm and cannulated dilator under the guidance of the spine robot. Drilling by the electric drill and guide wire placement were subsequently completed. These steps were repeated for subsequent guide wire insertions. Anteroposterior and lateral fluoroscopy were performed to confirm the position of the guide wires. After decompression of the corresponding segment was completed, tapping and CBT screw placement were performed. Fluoroscopy was performed again to confirm placement of the CBT screws.
Results
As shown in Table 1, a total of 26 CBT screws were placed in 7 patients, including 4 females and 3 males. The mean operation time was 129.29 ± 32.97 minutes, the mean blood loss was 180 ± 52.60 mL, and the mean intraoperative fluoroscopy time was 14.29 ± 3.15 s. The mean duration between the salvage CBT screw fixation technique and the previous surgery was 53.4 ± 31.0 months (with a range of 12–96). There were no intraoperative complications or complications related to CBT screws in any of the cases. Among all screws, the immediate postoperative CT results showed that 92.31% (24) were grade A and 7.69% (2) were grade B; therefore, all screws were clinically acceptable. At the final follow-up, the JOA score for low back pain of all patients was significantly improved, and all patients had no signs of screw loosening on x-ray.
Case 1 (Figures 1-3)
A 63-year-old woman had undergone L45 and L5S1 posterior lumbar interbody fusion (PLIF) for a diagnosis of L4-S1 lumbar canal stenosis. Two years after the first surgery, she had back pain and radiation pain in both lower limbs caused by an accidental fall. The plain radiograph and MR images showed adjacent segment disease (ASD) in L34 and S1 pedicle screw fractures. Conservative treatment had no effect on her low back pain, and salvage surgery was performed. After removal of the posterior rod and S1 screw tail, L34 decompression and TLIF were performed. By the preoperative planning of the screw trajectory, we found that the previous hardware does not block the trajectory of the CBT screws, So the S1 screw bodies were retained to prevent further destruction of the vertebral body, and S1 CBT and S2AI screw fixation were used to construct the lumbosacral stability under guidance of a spine robot. Finally, PLF was performed in L5S1. The radicular pain and back pain disappeared after the second surgery. Postoperative CT showed that S1 CBT and S2AI screws were all grade-A according to the Gertzbein-Robbins classification, and an x-ray at 12 months after the last surgery illustrated no signs of screw loosening or displacement.
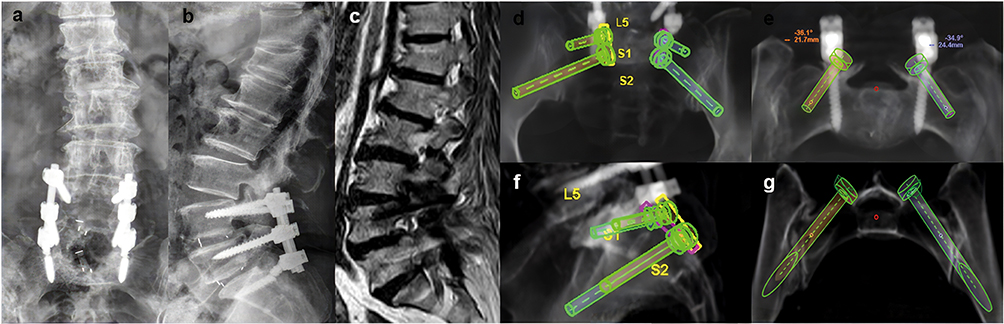 |
Figure 1 Preoperative x-ray showed S1 PS (a and b). Preoperative MRI showed L34 ASD (c). S1 CBT and S2AI screws were designed in the platform of the Mazor Renaissance spinal robot (d–g). |
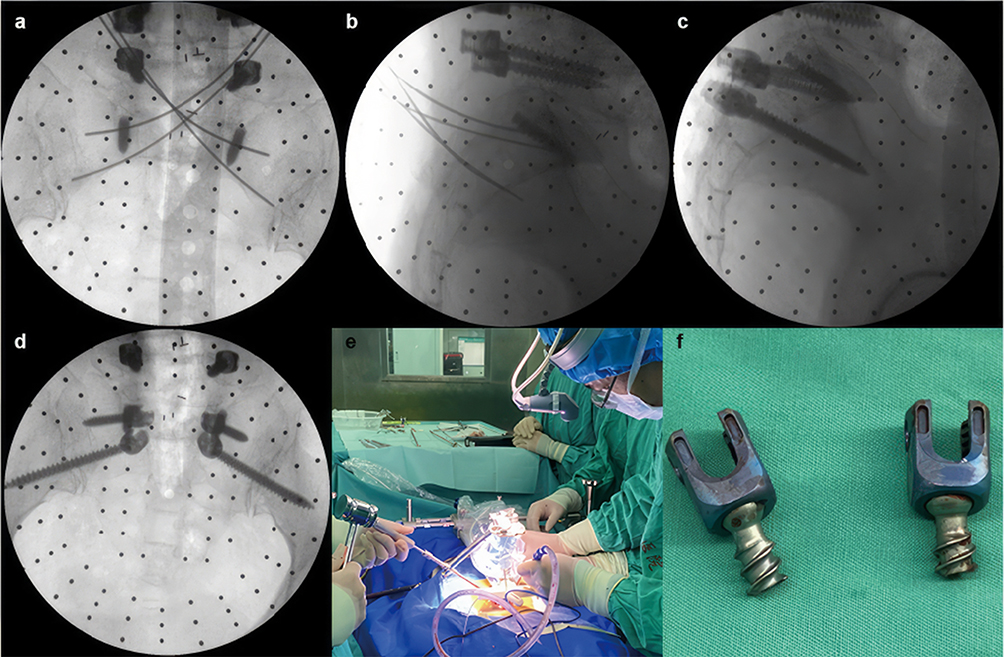 |
Figure 2 Intraoperative position of K-wires and screws in intraoperative fluoroscopy (a–d). An intraoperative pilot hole of the S1 CBT screw was prepared (e). Fractured S1 pedicle screw tails were removed (f). |
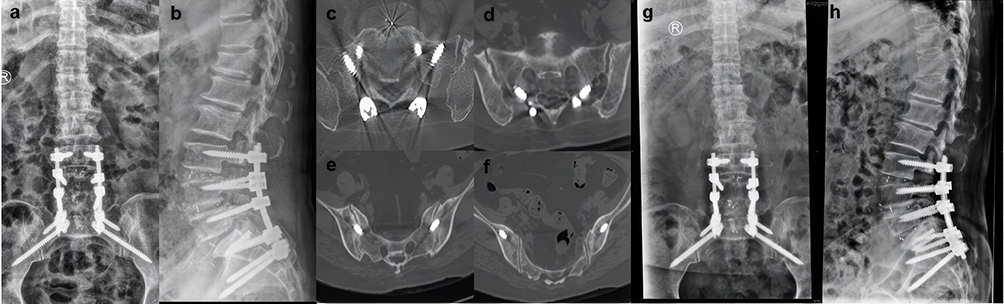 |
Figure 3 Immediate postoperative x-ray (a and b) and CT (c–f) showed that S1 CBT and S2 AI screws reached grade A according to the modified Gertzbein-Robbins classification. X-ray at 12 months after surgery (g–h). |
Case 2 (Figures 2-6)
A 66-year-old man was admitted to our hospital due to numbness and weakness in the lower limbs for half a year, accompanied by difficulty urinating. The patient had previously undergone posterior L2-L5 lumbar fusion surgery 5 years prior. Preoperative CT showed L12 ASD and T10/11 and T11/12 ossification of the ligamentum flavum (OLF). Posterior laminectomy and decompression were performed on T10/11, T11/T12, and L1/2. The stress in the thoracolumbar segment was high, and instead of prolonged fixation, we used short segmental fixation with CBT screws in order to distribute the stress. L1-L2 bilateral CBT screws were placed with robot assistance, and T10-T11 pedicle screws were inserted freehand. Local bone was used as autograft bone to fill the facet joint space for fusion. Postoperative and final follow-up x-rays showed that CBT and PS screws were in a good position.
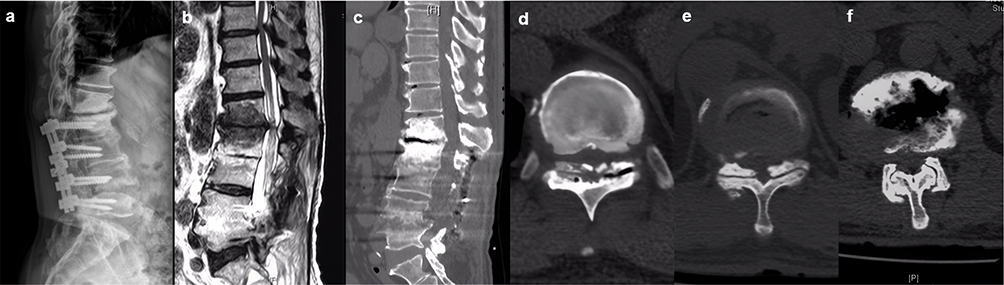 |
Figure 4 Preoperative x-ray and MRI showed previous L2-5 PLIF (a) and L12 ASD (b). Preoperative CT showed L12 ASD (c), T10-12 LCS, and OLF (d–f). |
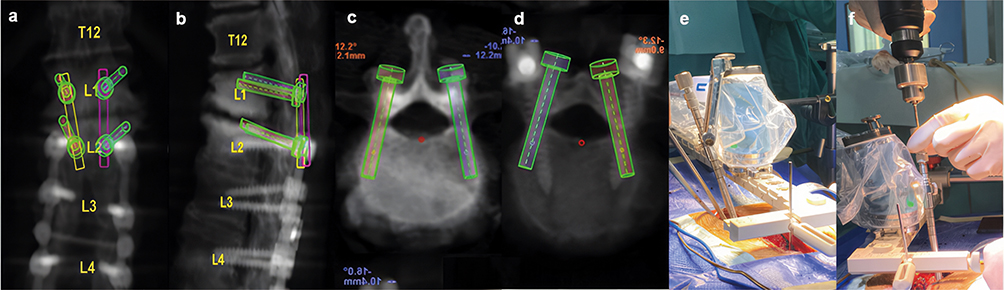 |
Figure 5 CBT screws were designed in the Mazor Renaissance spinal robot platform (a–d). Preparing the pilot hole of the CBT screw with the assistance of a spinal robot (e and f). |
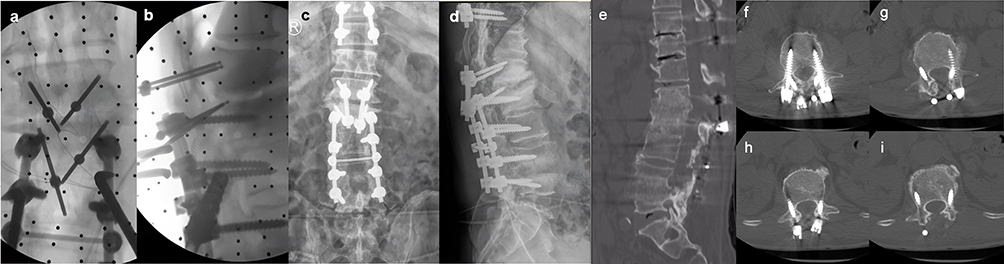 |
Figure 6 Intraoperative position of guided pins (a and b). Immediate postoperative x-ray (c and d). Postoperative CT at the final follow-up (e–i). |
Case 3 (Figure 7)
A 60-year-old woman who had undergone L34 PLF and L45 PLIF for lumbar canal stenosis (LCS) 6 months prior to visiting our clinic for severe low back pain. The radiograph and CT images showed pedicle screws and L45 fusion failure. We performed salvage surgery for L4/L5 fusion failure, and the CBT screw fixation technique was used for stability reconstruction. After the L3-L5 pedicle screws were removed, we found that osseous destruction due to loosening of the PS at the L45 level allowed us to perform CBT only unilaterally. The L45 cage was also removed, and lumbar interbody fusion was reperformed using autograft bone taken from the ilium. Her low back improved completely after the second surgery, and x-ray and CT images taken 1 year after the last surgery illustrated successful bone union at the affected level.
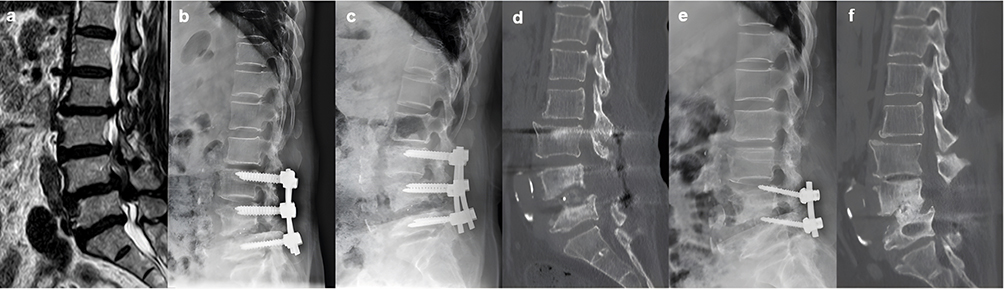 |
Figure 7 MRI showed L3-5 LCS before the initial operation (a). Immediate postoperative x-ray (b) and x-ray at 6 months after the first operation (c). CT before the revision surgery showed loosened PS and L45 union failure (d). Immediate postoperative x-ray and postoperative CT at the final follow-up (e and f). |
Discussion
CBT was first described by Santoni and colleagues to obtain a stable fixation in osteoporotic lumbar vertebrae.3 Anatomical studies and radiological evidence have demonstrated that CBT can obtain 4-point contact between the dorsal cortex at the site of insertion, the medially oriented posterior pedicle wall, the laterally oriented anterior pedicle wall, and the curvature of the vertebral body wall.15 Additionally, biomechanical studies have shown that CBT screws have similar or greater fixation and pullout strength in comparison with traditional PS or bone cement screw internal fixation.16–18 CBT screw insertion from a more caudal and medial starting point requires less facet joint violation and less paraspinal muscle damage.5,15 Clinical outcomes showed equal or better results in the fusion rates, patient satisfaction, functional recovery, and perioperative complication rates from the review of the literature.1,4
However, CBT may be more technically challenging for cases in which the trajectory is narrower and more difficult to cannulate through multiple cortices compared to PS. Ishii et al19 performed CBT screw insertion using a freehand technique in PLIF with 3.3% unacceptable misplacements and 2.2% revisions because of subsequent neurological symptoms caused by unacceptable screw position. The study by Dayani et al20 demonstrated that the difference in surgical complications between the early and late experience groups trended toward statistical significance, and 66.7% of medial pedicle breaches and the only case of lateral vertebral body breach were identified in the early experience group. In addition, surgeons and patients may be exposed to greater radiation due to intraoperative multiplanar fluoroscopy during CBT screw insertion.8,11
Navigation-based and robot-assisted CBT screw placement has been described to increase CBT screw placement accuracy and reduce radiation exposure.8,10,11 In a retrospective study of 81 patients by Li et al,11 the safety and accuracy of CBT screw placement between robot-assisted and fluoroscopy-assisted approaches were compared, and the results showed that screw placement accuracy was higher in the robot-assisted group (93%) than in the fluoroscopy-assisted group (83%). They demonstrated that robot-assisted CBT screw placement improves screw placement accuracy and shortens screw placement time with a relatively smooth and short learning curve. Buza et al9 reviewed the technical aspects of utilizing MXSE (Mazor X Stealth Edition) for CBT screws and reported that the learning curve associated with CBT technology must be considered. Although robotic technology has been shown to increase pedicle screw placement accuracy, any technical errors during the procedure may lead to screw malposition.9 Khan et al10 reported initial experience with CBT screw insertion under robotic guidance and CT navigation in 40 patients with degenerative disc disease, and the study demonstrated that both robotic technology and CT navigation technology for CBT screw insertion were accurate and safe.
In this study, we performed robot-assisted salvage surgery with CBT in seven patients with fusion failure or ASD after PLIF. We also noted that all steps in the robot workflow must be performed accurately during CBT screw placement to ensure a safe outcome, and screw pilot hole exploration and intraoperative radiographs are still required for traditional freehand screw placement.
While most recent studies on robotic-assisted CBT screw placement have evaluated CBT screw trajectories in spine surgery, reports about the application of this technique under the guidance of robots for failed lumbar spine surgery or revision surgery are rare, and only a few studies on CBT screw fixation techniques for ASD have been reported. Several surgical approaches have been introduced for ASD, including decompression alone, anterior or lateral interbody fusion with posterior fixation, and posterior decompression and fixation with the fusion of the adjacent segments. The posterior approach is still the most commonly used method for ASD, with the advantages of long-term stability and sufficient decompression.2,6 However, extensive exposure was required for the connection to preexisting hardware, and subsequent soft-tissue damage was unavoidable in this procedure. The CBT screw fixation technique was used in several studies to solve this problem, with placement in the previous PS instrumented vertebral bodies as a domino system to connect adjacent levels. Chen et al2 introduced the freehand CBT screw fixation technique in previously instrumented vertebral bodies for ASD; this method can prevent the need for previous hardware removal and reimplantation. Rodriguez et al6 reported that the CBT screw fixation technique was used in a previously instrumented lumbar pedicle with CT-guided navigation in 5 consecutive patients for symptomatic ASD, and all the patients experienced good clinical results. Moreover, some authors have also suggested that the pedicle size should be evaluated before surgery to determine whether a pedicle with a preexisting pedicle screw can accommodate a CBT pedicle screw.2,6 In cases 2 and 6, the preoperative planning program in the Mazor Renaissance robot system was very helpful. The residual amount and the CBT screw size can be calculated accurately without being limited by scarring or preexisting PSs, thus providing precise directive guidance during cortical cannulation and screw placement. In addition, further destruction of the vertebral body can be avoided if the previous hardware can be retained. Postoperative CT demonstrates accurate screw placement, and the symptoms were clearly relieved.
Patients with screw loosening resulting in fusion failure often have a combination of many unfavorable factors such as osteoporosis. Combined with the difficulty in exposure due to scar formation and loss of bony structures from previous surgery, salvage surgery is highly challenging. There are currently several techniques are available for salvaging loose or compromised PSs, such as changing the previous screws with PSs with greater diameters and lengths, using bone cement screws, and vertebral augmentation.18 The CBT screw fixation technique is another option that uses a different screw trajectory or insertion technique, with no need for additional level fusion and vertebral augmentation.3 A human cadaveric and biomechanical study using this technique by Zhang et al21 demonstrated that the original torque increased by 50%, an average of 81% of the pullout strength of the initial PS screws was retained, and the fatigue performance was equal to that of the PS screws, which were considerably stronger than the loose PS screws. Calvert et al22 investigated the biomechanical properties of rescue CBT screws in osteoporotic lumbar spines and demonstrated that CBT rescue screws retained 60% of the pullout strength of the original PS. This study reported similar stiffness in flexion/extension and axial rotation between CBT rescue screws and the initial PS. We supported this opinion that CBT screws may serve as a suitable salvage technique for failed PS (cases 1, 3, and 7). The patient achieved good symptom relief and spinal fusion. Moreover, sufficient bone grafting was required for fusion in these revision surgeries.
This study suffered from several potential limitations. First, the study had a small sample size due to the rarity of the etiology, and this limited the broad generalizability of the results. Second, the robot-assisted CBT screw fixation technique can be performed as a replacement for or supplement to the traditional PS fixation technique in spine surgery, but this technique may need long-term follow-up to confirm the clinical results. Third, the learning curve associated with the adoption of spinal robots must be considered. Future studies are required to address these concerns.
Conclusion
The robot-assisted CBT screw fixation technique supplemented the traditional PS fixation technique and can be performed as a salvage strategy for failed lumbar spine surgery. We introduced the robot-assisted CBT screw fixation technique in ASD and loose and compromised PSs. Moreover, the spinal robot was very helpful in evaluating the pedicle size and determining the CBT screw direction, especially in cases with previously instrumented lumbar pedicles. The robot-assisted CBT screw fixation technique provides an option for surgeons to perform salvage surgeries safely and efficiently.
Ethical Approval
The study was approved by the ethical committee of the Affiliated Hospital of Qingdao University (approval number: QYFY WZLL 27404). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Pre-operative explanation of the procedure was made to all patients before obtaining informed consent. All patients mentioned in this article have read the manuscript, consented to publication and signed the patient consent form.
Funding
This work was supported by National Natural Science Foundation of China (82100940) and Qingdao Postdoctoral Application Research Project (2019).
Disclosure
All authors declare that they have no conflicts of interest related to this work.
References
1. Hu JN, Yang XF, Li CM, et al. Comparison of cortical bone trajectory versus pedicle screw techniques in lumbar fusion surgery: a meta-analysis. Medicine. 2019;98(33):e16751. doi:10.1097/MD.0000000000016751
2. Chen CH, Huang HM, Chen DC, et al. Cortical bone trajectory screws fixation in lumbar adjacent segment disease: a technique note with case series. J Clin Neurosci. 2018;48:224–228. doi:10.1016/j.jocn.2017.11.008
3. Santoni BG, Hynes RA, McGilvray KC, et al. Cortical bone trajectory for lumbar pedicle screws. Spine J. 2009;9(5):366–373. doi:10.1016/j.spinee.2008.07.008
4. Kim KT, Song MG, Park YJ, et al. Cortical Trajectory Screw Fixation in Lumbar Spine Surgery: a Review of the Existing Literature. Asian Spine J. 2022;16(1):127–140. doi:10.31616/asj.2020.0575
5. Kim SJ, Mobbs RJ, Natarajan P, et al. Historical Note: the Evolution of Cortical Bone Trajectory and Associated Techniques. Spine Surg Relat Res. 2022;6(1):1–9. doi:10.22603/ssrr.2021-0059
6. Rodriguez A, Neal MT, Liu A, et al. Novel placement of cortical bone trajectory screws in previously instrumented pedicles for adjacent-segment lumbar disease using CT image-guided navigation. Neurosurg Focus. 2014;36(3):E9. doi:10.3171/2014.1.FOCUS13521
7. Ueno M, Imura T, Inoue G, et al. Posterior corrective fusion using a double-trajectory technique (cortical bone trajectory combined with traditional trajectory) for degenerative lumbar scoliosis with osteoporosis: technical note. J Neurosurg Spine. 2013;19(5):600–607. doi:10.3171/2013.7.SPINE13191
8. Le X, Tian W, Shi Z, et al. Robot-assisted versus fluoroscopy-assisted cortical bone trajectory screw instrumentation in lumbar spinal surgery: a matched-cohort comparison. World Neurosurg. 2018;120:e745–e751. doi:10.1016/j.wneu.2018.08.157
9. Buza JR, Good CR, Lehman RJ, et al. Robotic-assisted cortical bone trajectory (CBT) screws using the Mazor X Stealth Edition (MXSE) system: workflow and technical tips for safe and efficient use. J Robot Surg. 2021;15(1):13–23. doi:10.1007/s11701-020-01147-7
10. Khan A, Rho K, Mao JZ, et al. Comparing Cortical Bone Trajectories for Pedicle Screw Insertion using Robotic Guidance and Three-Dimensional Computed Tomography Navigation. World Neurosurg. 2020;141:e625–e632. doi:10.1016/j.wneu.2020.05.257
11. Li Y, Chen L, Liu Y, et al. Accuracy and safety of robot-assisted cortical bone trajectory screw placement: a comparison of robot-assisted technique with fluoroscopy-assisted approach. BMC Musculoskelet Disord. 2022;23(1):328. doi:10.1186/s12891-022-05206-y
12. Rho K, OConnor TE, Lucas JM, et al. Minimally invasive robot-guided dual cortical bone trajectory for adjacent segment disease. Cureus. 2021;13(8):e16822. doi:10.7759/cureus.16822
13. Wang C, Zhang H, Zhang L, et al. Accuracy and deviation analysis of robot‐assisted spinal implants: a retrospective overview of 105 cases and preliminary comparison to open freehand surgery in lumbar spondylolisthesis. Int J Med Robotics Computer Assisted Surgery. 2021;17(4). doi:10.1002/rcs.2273
14. Orita S, Nakajima T, Konno K, et al. Salvage strategy for failed spinal fusion surgery using lumbar lateral interbody fusion technique: a technical note. Spine Surg Relat Res. 2018;2(1):86–92. doi:10.22603/ssrr.2017-0035
15. Matsukawa K, Yato Y. Lumbar pedicle screw fixation with cortical bone trajectory: a review from anatomical and biomechanical standpoints. Spine Surg Relat Res. 2017;1(4):164–173. doi:10.22603/ssrr.1.2017-0006
16. Li Y, Wang S, Zhu Z, et al. Biomechanical Analysis of cortical bone trajectory screw versus bone cement screw for fixation in porcine spinal low bone mass model. Clin Spine Surg. 2022;36:E145–E152. doi:10.1097/BSD.0000000000001395
17. Matsukawa K, Yato Y, Imabayashi H, et al. Biomechanical Evaluation of Cross Trajectory Technique for Pedicle Screw Insertion: combined Use of Traditional Trajectory and Cortical Bone Trajectory. Orthop Surg. 2015;7(4):317–323. doi:10.1111/os.12212
18. Tandon V, Franke J, Kalidindi K. Advancements in osteoporotic spine fixation. J Clin Orthop Trauma. 2020;11(5):778–785. doi:10.1016/j.jcot.2020.06.028
19. Ishii M, Ohnishi A, Yamagishi A, et al. Freehand screw insertion technique without image guidance for the cortical bone trajectory screw in posterior lumbar interbody fusion: what affects screw misplacement? J Neurosurg Spine. 2022;36(1):1–7. doi:10.3171/2021.2.SPINE202145
20. Dayani F, Chen YR, Johnson E, et al. Minimally invasive lumbar pedicle screw fixation using cortical bone trajectory - Screw accuracy, complications, and learning curve in 100 screw placements. J Clin Neurosci. 2019;61:106–111. doi:10.1016/j.jocn.2018.10.131
21. Zhang RJ, Li HM, Gao H, et al. Cortical bone trajectory screws used to save failed traditional trajectory screws in the osteoporotic lumbar spine and vice versa: a human cadaveric biomechanical study. J Neurosurg Spine;2019. 1–8. doi:10.3171/2018.12.SPINE18970
22. Calvert GC, Lawrence RD, Abtahi AM, et al. Cortical screws used to rescue failed lumbar pedicle screw construct: a biomechanical analysis. J Neurosurg Spine. 2015;22(2):166–172. doi:10.3171/2014.10.SPINE14371
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.