Back to Journals » Journal of Pain Research » Volume 13
The Context Matters: A Retrospective Analysis of Life Stage at Chronic Pain Onset in Relation to Pain Characteristics and Psychosocial Outcomes
Authors Owiredua C ![]() , Flink I
, Flink I ![]() , Vixner L
, Vixner L ![]() , Äng BO
, Äng BO ![]() , Tseli E
, Tseli E ![]() , Boersma K
, Boersma K ![]()
Received 18 May 2020
Accepted for publication 18 August 2020
Published 23 October 2020 Volume 2020:13 Pages 2685—2695
DOI https://doi.org/10.2147/JPR.S263035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Christiana Owiredua,1 Ida Flink,1 Linda Vixner,2 Björn O Äng,2– 4 Elena Tseli,2,3 Katja Boersma1
1Center for Health and Medical Psychology (CHAMP), School of Law, Psychology, and Social Work, Örebro University, Örebro, Sweden; 2School of Education, Health and Social Studies, Dalarna University, Falun, Sweden; 3Division of Physiotherapy, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden; 4Center for Clinical Research Dalarna, Uppsala University, Falun, Sweden
Correspondence: Christiana Owiredua
School of Law, Psychology, and Social Work, Örebro University, Örebro, Sweden
Tel +46-19-301-320
Email [email protected]
Background: Developmental life stage at chronic pain onset differs among chronic pain patients. Although pain affects multiple life domains, it is unknown whether the timing of chronic pain onset relates to pain characteristics and psychosocial outcomes. The purpose of this retrospective study was to investigate differences in pain characteristics and psychosocial outcomes in patients at different developmental life stages at chronic pain onset.
Methods: Cross-sectional baseline data from the Swedish Quality Registry for Pain Rehabilitation (2009 to 2016) were used, selecting the middle-aged patients (45– 65 years, n=6225) reporting chronic nonmalignant pain. Patients were categorized into three groups, depending on their developmental life stage at chronic pain onset: early onset (age ≤ 30 years), intermediate onset (age 31– 45 years), and late onset (age ≥ 46 years). Pain characteristics and psychosocial outcomes were assessed with validated self-reported measures.
Results: One-way MANCOVA indicated differences in number of pain locations and psychosocial outcomes among the groups. Post hoc analysis showed differences in the trends for how groups differed on outcome domains. Overall, patients with earlier chronic pain onset showed significantly poorer psychosocial outcomes and more spreading of pain.
Conclusion: Developmental life stage at chronic pain onset is associated with different pain outcomes. Pain onset early in life is linked to worse outcomes in multiple domains, pointing to a need for identifying these patients early.
Keywords: chronic pain, developmental stage of onset, aging, psychosocial outcomes, life course, outcomes
Introduction
Chronic pain is a huge public health problem worldwide, affecting both sexes in all age-groups.1–3 Although the majority of chronic pain sufferers are middle-aged,4–6 developmental life stage at chronic pain onset varies, from childhood and early adolescence to late adulthood. In adults (18–60/65 years), up to 50% report chronic pain,6,7 while about 55% are affected in older populations (60/65+).8–10 Also, prevalence among children and adolescents can be up to 88%, depending on pain location.11,12 As such, chronic pain debuts at different life stages in every pool of chronic pain patients, and the question is whether if and how time of onset is related to adaptation to pain.
Different life stages have their own developmental agendas, tasks, and expectations, as highlighted in the life-course view of aging.13,14 While no stage in the life course is considered more important than the other, earlier phases set the stage for later development,15,16 due to accumulation of risks.16–18 Further, the illness-intrusiveness framework posits that contextual factors influence to what extent ill health interferes with lifestyle, tasks, and goals.19–22 From these perspectives, the life stage at which ill health arises may be central for subsequent problem development.18,21 In chronic pain, this may be even more important, as pain in one area of the body induces a risk of future spread of pain to other areas.23 Moreover, research illuminating demographic factors, such as age and sex, has emphasized that these form the context for beliefs, expectancies, and ways of coping with pain.24 In other words, the developmental life stage when chronic pain emerges may be important for how it is experienced, its effect, and how it is managed. Still, little is known about the importance of pain onset in pain characteristics and outcomes.
While chronic pain has a detrimental impact on health and well-being,6,25,26 few studies have explored chronic pain from a life-course perspective.27 The life stage for chronic pain onset serves as a proxy for the developmental context in which pain begins to interfere with patients’ lifestyle, tasks, and goals. As such, the aim of the current study was to apply a life-course perspective to chronic pain to enhance our understanding of variations in pain experiences and outcomes. The main research question was whether developmental life stage at chronic pain onset is related to pain characteristics and psychosocial outcomes (recovery expectancy, emotional distress, social functioning, general health functioning, life interference, and life control) in a large sample of chronic pain patients.
Methods
Design/Data Source
This retrospective study used cross-sectional data from the Swedish Quality Register for Pain Rehabilitation (SQRP). The SQRP is a national registry database of people with disabling chronic nonmalignant musculoskeletal pain who have been referred for multimodal assessment and/or treatment at specialist pain clinics in Sweden.28 Patients living with chronic malignant pain are excluded from the registry. Approximately 40 specialist pain clinics routinely deliver data to the register.29 Data in the registry are collected at three time points: baseline for all patients who have been referred to the specialist clinics, posttreatment and a 1-year follow-up for those who have been on a multimodal rehabilitation (MMR) program. A thorough description of the SQRP and MMR programs is provided elsewhere.28,30 In the current study, only baseline data were used. All participants gave informed consent for their data to be included in the registry, which forms the basis of this study. Further, ethical clearance was obtained from the Ethical Review Board in Uppsala, Sweden (2018/036; 2019–02167) to undertake this study using the SQRP.
Sampling/Sampling Characteristics
Participants were chronic pain patients referred for multidisciplinary assessment and treatment at specialist pain clinics across Sweden from 2009 to 2016. Inclusion criteria were pain duration reflecting chronic pain (≥90 days) and being middle-aged (45–65 years). Middle age is an established category described as a bridge of growth and decline, and was selected in order to standardize the current life phase from which variability in life stages of pain onset could be explored.31 A total of 19,623 fulfilled these criteria. Immigrants with non-European background (n=3,073) were excluded, due to the likelihood of specific historical factors influencing their development of pain across the life span (eg, immigration-related stressors).32 Furthermore, participants with incomplete datasets on the study variables were excluded (n=10,325), the majority due to lacking data on one of the outcome variable — the Tampa Scale for Kinesiophobia (TSK),33 — as this is an optional measure for the SQRP. Hence, most clinics did not adopt it. These exclusion criteria resulted in a final sample of n=6,225. Comparison of the final sample with those excluded due to missing values (using p=0.001) revealed no significant differences in sex, education, or pain duration. However, minor differences were detected in developmental stage of pain onset (X22, 16,550=18.44, p=0.0001). Average age of onset for those included in the analysis was 41.32±11.49 years and 41.48±11.59 years for those excluded. Average age when referred to an MMR program (t2, 16,548=5.33, p=0) was 52.28±5.16 and 52.45±5.27 years for those excluded from the study.
Measures
Data in the registry are based on self-reported questionnaires, with information regarding patients’ sociodemographic variables, pain characteristics, expectations, psychosocial variables, and various measures of life impact, functioning, and well-being. Swedish versions of all measures were used.
Background Variables
Background variables were education, age, sex, and primary pain location. Education was initially measured on four levels, namely basic school, high school, university/college education, and “other”. For the purposes of this study, these were clustered into university/college education and below university. Age reflected participants’ age at baseline. Primary pain location was indicated by patients’ reports of body part(s) where their pain was centrally located.
Independent Variable
The main independent variable of interest was developmental life stage at chronic pain onset, defined as the stage at which the current chronic pain problem had started. This was categorized into three stages, namely early pain onset, intermediate pain onset, and later pain onset. Early pain onset was defined as chronic pain that started at age 30 years or before. Intermediate age of onset was defined as chronic pain that began at age 30–45 years, while later pain was defined as chronic pain with onset after age 45 years.
Outcome Variables
Based on previous recommendations by Kaiser et al and Turk et al and the study aims, the following outcome domains were covered.34,35
Pain Characteristics
Pain characteristics were defined in this study as pain intensity and number of pain locations.
Pain intensity was measured with the Multidimensional Pain Inventory (MPI) pain-severity dimension. This measures patients’ current pain intensity, as well as their pain intensity and suffering in the past 7 days due to chronic pain.36 The range of possible scores is 0–6. Higher scores on the scale indicate higher levels of pain. This scale has shown good psychometric properties in a Swedish population.37
The number of pain locations was assessed with a form with 36 predefined anatomical areas of the human body (18 defined areas on each left and right side): head/face, neck, shoulder, upper arm, elbow, forearm, hand, anterior aspect of chest, lateral aspect of chest, belly, sexual organs, upper back, lower back, hip/gluteal area, thigh, knee, shank, and foot.28 The number of areas marked by patients was summed to indicate the number of pain locations, with possible scores of 1–36.
Psychosocial Outcomes
Recovery expectancy was measured with a one-item question asking about patient expectations of the possibility of restored health (How convinced are you to recover?). The item was rated on a five-point Likert scale ranging from totally convinced (0) to not convinced (4). As such, higher scores represented poor recovery expectancy.
The Hospital Anxiety and Depression Scale (HADS) was used to assess patients’ overall emotional distress. The HADS is a self-rating scale that aims to measure symptoms of anxiety and depression in primary-care nonpsychiatric patients.38 The questionnaire comprises 14 items, with seven measuring anxiety and seven measuring depressive symptoms. Items are scored on a four-point Likert scale ranging from 0–3. Sample items on the questionnaire are “I get a sort of frightened feeling as if something awful is about to happen” (anxiety) and “I feel as if I am slowed down” (depressive symptoms). Although the HADS was originally developed to measure subscales of anxiety and depression, a recent study found that it has better psychometric properties as a measure of overall emotional distress in individuals with chronic pain.29 The authors proposed that the item response theory–based score be rescaled from logits to percentiles (ie, 0–100) to facilitate interpretation, and because their analyses were based on the same register as ours, the results should generalize particularly well. For a detailed description of scoring procedures, see LoMartire et al.29
Fear-avoidance beliefs were measured with the Tampa Scale for Kinesophobia (TSK).33 The TSK is a widely used 17-item measure of pain-related fear beliefs based on fear of movement and/or (re)injury represented by a somatic focus of pain and activity avoidance.39,40 Items are rated on a four-point scale with end points ranging between 1 (strongly disagree) and 4 (strongly agree). A sample item on this measure is “If I tried to overcome this fear, my pain would increase”. A total score was calculated after reversing the scores on items 4, 8, 12, and 16. High scores indicate high levels of fear-avoidance beliefs, with possible scores of 17–68.
Social functioning was measured with the Short Form 36 (SF36) social functioning subscale.41 This measures patients’ limitations in social life due to the extent to which their health problems interfere with social activities. It consists of two items, with higher scores indicating higher social functioning and lower scores indicating lower levels of social functioning. An item on the scale is
“During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbors, or groups?”.
The range of possible scores is 0–100. Good psychometric properties have been identified for the Swedish version.42
General health functioning was assessed with the SF36 general health subscale. This is a five-item questionnaire that measures patient’s perceptions of their overall health functioning.41 Lower scores represent perceptions of poor health with the possibility of getting worse, while higher scores represent good perceptions of overall health. The range of possible scores is 0–6. A sample item on this scale is “I am as healthy as anybody I know”. Good psychometric properties exist for the Swedish version of the scale.42
Life interference was measured with the MPI life-interference dimension.36 This measures patients’ evaluation of how chronic pain interferes with their everyday life, eg, housework, family responsibility, and work and leisure activities, on eleven items. Scores on the items range from 0 (no interference) to 6 (extreme interference). Higher scores indicate higher levels of interference. The scale has shown good psychometric properties in the Swedish population.37
Life control was measured with the MPI life-control dimension. This is a four-item measure that evaluates a patient’s control of his/her life, pain, and everyday problems encountered. Scores on the scale range from 0 (no control) to 6 (maximum control). Higher scores indicate greater levels of life control. The scale has shown good psychometric properties in the Swedish population.37
Data Preparation and Analysis
Prior to analysis, age at chronic pain onset was estimated from the duration of years that patients had lived with their pain and their at first assessment by subtracting years lived with pain from the age of participants. All analyses were conducted using SPSS version 26.00. Descriptive statistics are mainly made up of means, SDs, and percentage scores where explored. Data are expressed as means ± SD and in some cases numbers and percentages, unless otherwise specified. The main analysis was such that first, an overall test for differences in pain characteristics and psychosocial outcomes was done using one-way MANCOVA (sex, age, and education as covariates). This was followed up with testing differences in psychosocial outcomes only with one-way MANCOVA (sex, age, education, and pain characteristics as covariates). Significance for all tests was defined as p=0.001, due to the large sample.
The one-way MANCOVA Pillai trace test was used, as this is considered more robust when dealing with unequal sample size and homogeneity of covariance is not achieved. Univariate ANOVA was used as a follow-up test to explore for which outcome variables a statistically significant difference was observed. Further, Bonferroni post hoc tests were used to explore between-groups differences on outcome measures that were significant on univariate ANOVA with a Bonferroni correction. ηp2 values can be explained as small (0.0099), medium (0.0588), and large (0.14) effect sizes, as suggested by Cohen and recommended by Richardson in situations where covariates are used.43,44
Results
Descriptive Statistics
The majority of the participants were female (71.4%) and had educational background lower than a university/college degree (74.3%). Most participants reported their primary pain locations to be back and neck (33.2%) and without a specific location (36.1%). Further, the majority of the participants had intermediate chronic pain onset (age 30–45 years, 42.1%) followed by those with later onset (after age 45 years, 38.6%) and then those with early chronic pain onset (30 years or younger, 19.3%). Overall descriptive statistics and for the different categories of age at chronic pain onset are presented in Table 1.
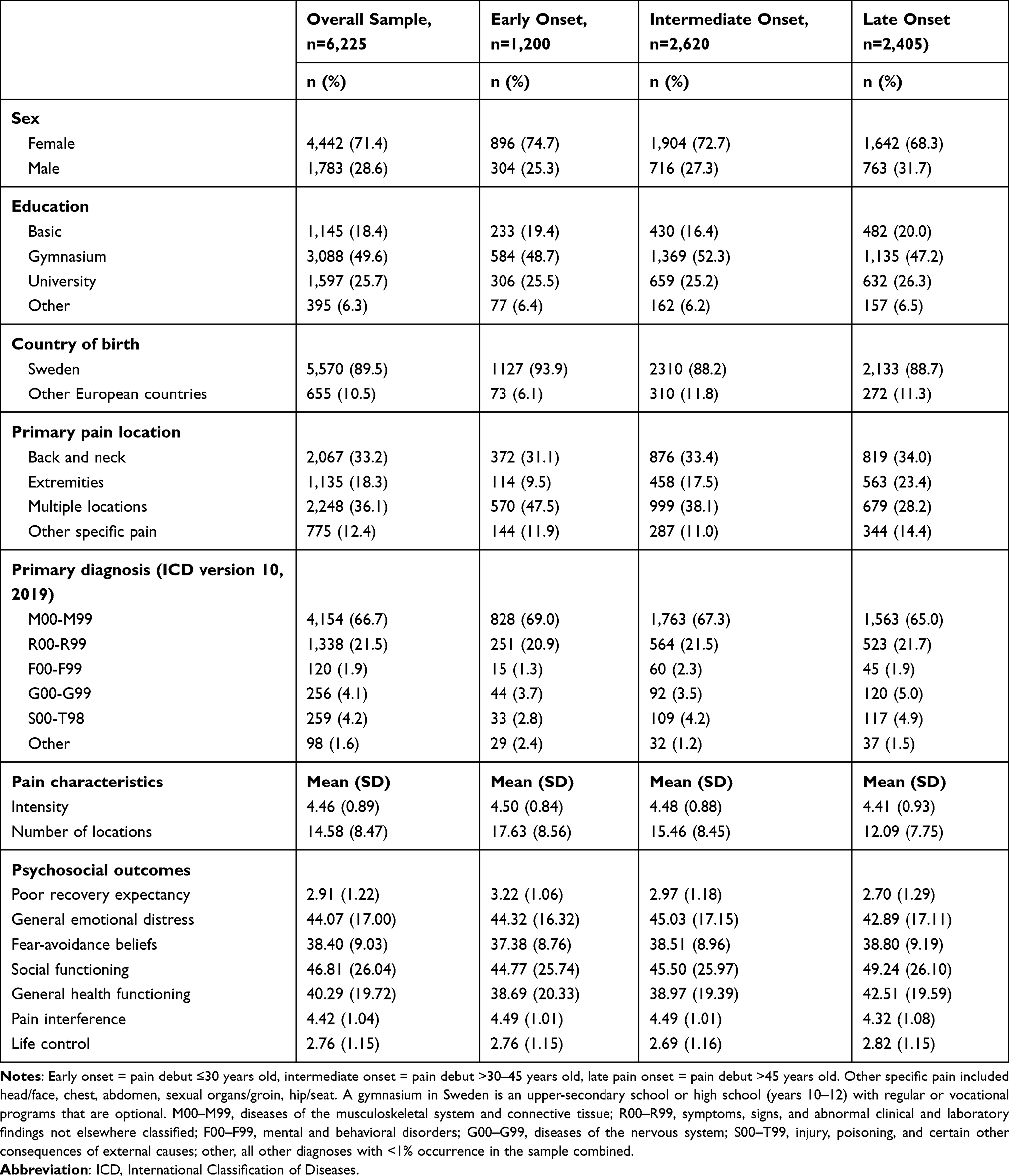 |
Table 1 Descriptive Overview of Demographic Variables, Pain Characteristics, and Psychosocial Outcomes |
Are There Differences in Pain Characteristics and Psychosocial Outcomes Based on Age at Chronic Pain Onset?
One-way MANCOVA was run to explore if differences existed in overall pain characteristic variables and psychosocial outcome variables based on age at chronic pain onset while controlling for sex, age, and level of education. Differences in age at chronic pain onset for combined dependent variables were statistically significant, F18, 12,424=33.48, p<0.001; Pallia’s trace =t0.09, ηp2=0.046). Follow-up univariate ANOVA indicated that significant differences existed in number of pain locations, poor recovery expectancy, fear-avoidance beliefs, general health functioning, and pain interference. However, patients at different life stages at chronic pain onset did not differ significantly on pain intensity, social functioning, general emotional distress, or life control.
Bonferroni post hoc analysis showed different patterns among the groups for which significant differences existed. For instance, those with early-life chronic pain onset had more pain locations and poorer recovery expectancy that those with intermediate and later onset. Further, those with intermediate-onset pain had higher levels of fear-avoidance beliefs than those with early onset, as well as higher levels of pain interference than the late chronic pain–onset group. However, the late-onset chronic pain group had higher levels of general health functioning than those with early and intermediate-onset pain. A summary of one-way MANCOVA, univariate ANOVAs, and post hoc analyses is presented in Table 2.
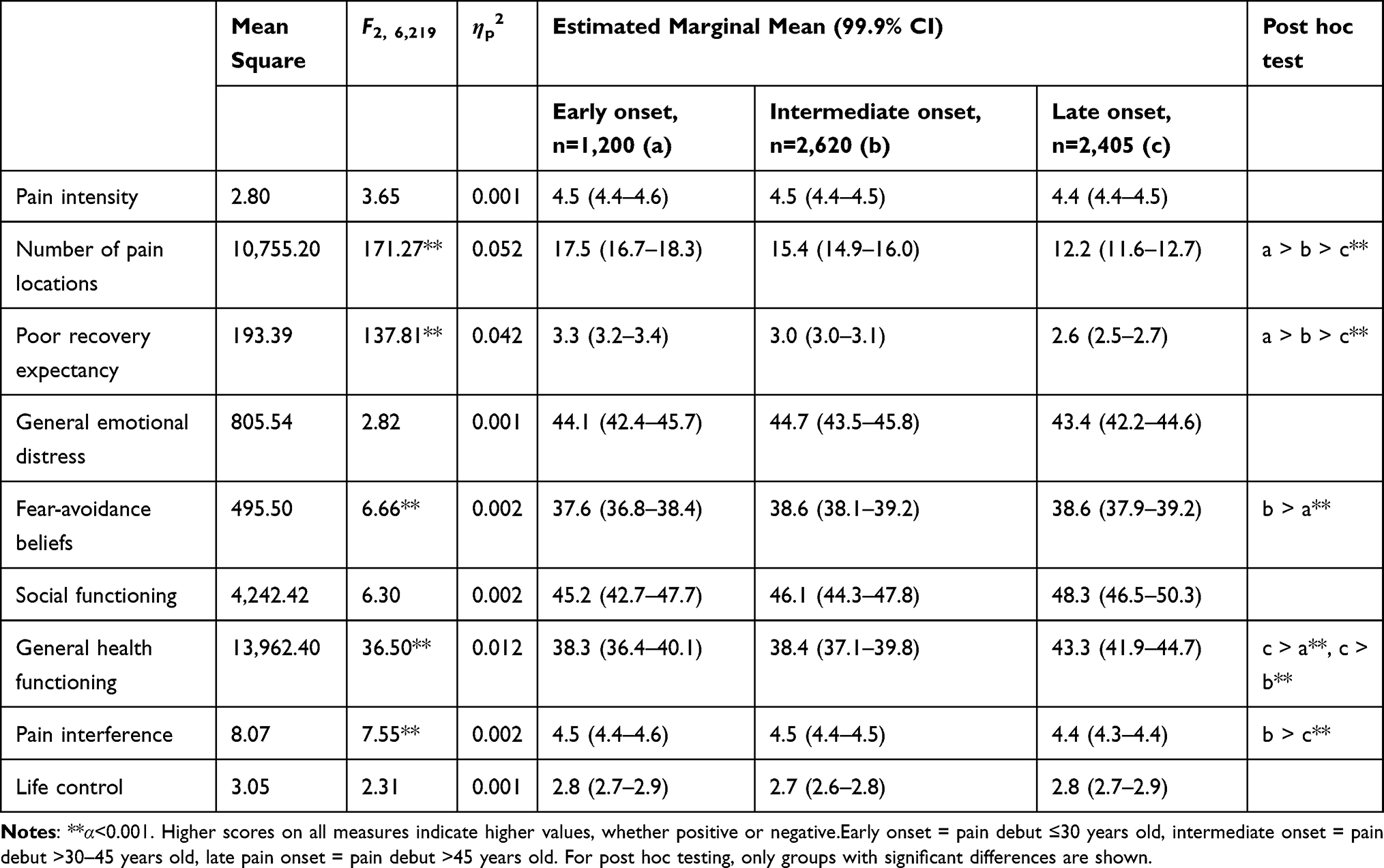 |
Table 2 Summary Findings of One-Way MANCOVA Exploring Differences in Pain Characteristics and Psychosocial Outcomes Based on Developmental Life Stage at Chronic Pain Onset While Controlling for Demographic Variables (Sex and Education) |
Does Life Stage at Chronic Pain Onset Predict Psychosocial Outcomes after Controlling for Sociodemographic Variables and Pain Characteristics?
One-way MANCOVA revealed differences between at least two of the age-groups at chronic pain onset on combined psychosocial outcomes after controlling for patient demographic variables and pain characteristics (F14, 12,424=19.08, p<0.001; Pallia’s trace = 0.04, ηp2=0.021). Follow-up univariate ANOVA showed that individual psychosocial outcomes for which significant differences existed in at least two of the groups were recovery expectancy, fear-avoidance beliefs, and general health functioning, ie, no significant differences were observed for general emotional distress, social functioning, pain interference, or life control. From Bonferroni post hoc analysis, those with early-onset pain had poorer recovery expectancy than those with intermediate and later onset, as well as those with intermediate onset having poorer recovery expectancy than those with later onset. However, on fear-avoidance beliefs, those with later onset and intermediate onset had higher levels of fear-avoidance beliefs than those with early onset. However, those with later chronic pain onset reported higher levels of general health functioning than those with intermediate chronic pain onset. A summary of one-way MANCOVA, univariate ANOVA and post hoc analysis is presented in Table 3.
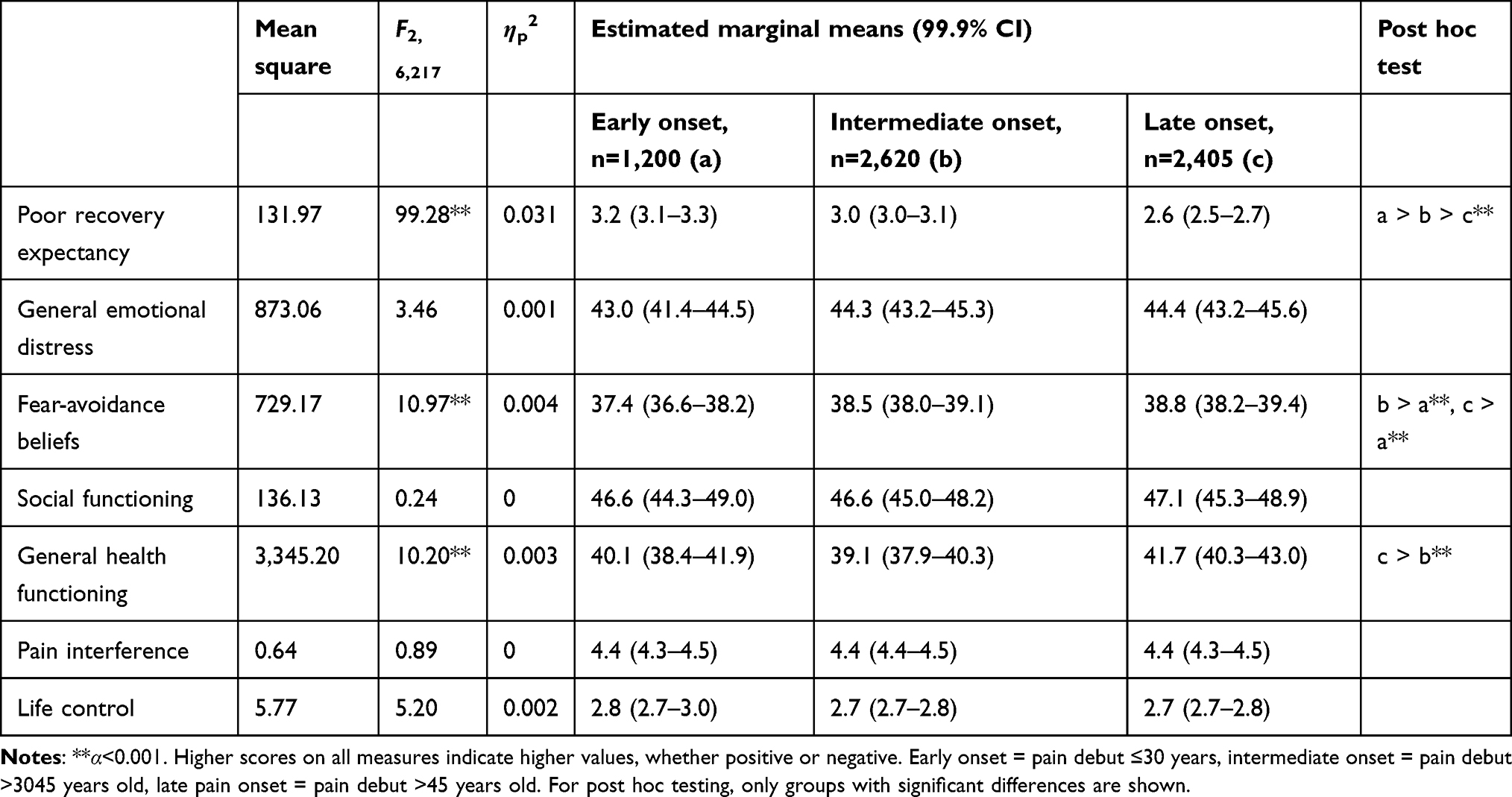 |
Table 3 Summary Findings of One-Way MANCOVA Exploring Differences in Developmental Life Stages of Chronic Pain Onset on Psychosocial Outcome Variables While Controlling for Sex, Education, Age and Pain Characteristic |
Discussion
The aim of this study was to explore possible differences in pain characteristics and psychosocial outcomes in chronic pain patients based on their developmental stage at chronic pain onset. We argued that since opportunities and disadvantages tend to accumulate over the life course,17,18 patients with chronic pain onset at different points of their life were likely to experience distinct life trajectories and hence differ in their adaptation to and experience of chronic pain. The results showed that indeed chronic pain onset at earlier stages in life was associated with an increased spreading of pain in terms of number of pain locations, yet no difference was found in pain intensity. Moreover, patients whose pain debut was early in life reported significantly poorer psychosocial outcomes in the domains of expectancy of recovery, general health functioning, and life interference. However, fear avoidance beliefs were higher among those with late pain onset. Nevertheless, when controlling for pain characteristics, only differences in recovery expectancy, general health functioning, and fear-avoidance beliefs remained significant.
The finding that early pain onset was linked to increased spreading of pain is consistent with previous research, where pain in one area of the body has been linked to an increased risk of pain in other body regions later in life.23 This goes hand in hand with research on central sensitization showing that ongoing nociceptive input (eg, pain onset early in life) may intensify pain sensitivity in other body regions.45–47 Our findings are further supported from a life-course epidemiological perspective, which points at early onset and longer duration of exposure to disadvantages as a risk factor for cumulative strain to biological systems over the life course.16
A life-course aging perspective can be used as a framework for understanding why patients with earlier pain onset had poorer psychosocial outcomes. Early pain onset may increase the accumulation of risks across the life course, affecting several life domains as chronic pain impact is noted to diffuse across many domains.6,16,18,26 This assertion of accumulation of risk has been exemplified in longitudinal studies on life trajectories of adolescents with chronic pain, where early onset was linked to educational failure, lost productivity, and social impairment, aspects that in themselves are risk factors for other poor outcomes over the life course.6,27 Chronic pain early in life may thus interfere with the acquisition of skills and abilities for future life tasks and disrupt fundamental life demands.
Physical symptoms, such as pain, are considered normal characteristics of the aging body.24,48,49 As such, pain with its related losses might be more accepted as part of an expected reduction in overall health at an older age. This may partly explain why late pain onset was linked with less negative psychosocial functioning. This same reasoning could explain why participants with later pain onset had higher levels of fear-avoidance beliefs. The assumption that pain is a natural biological mechanism of the aging body, coupled with feelings of frailty, may induce a higher somatic focus and activity avoidance due to fear of (re)injury.49,50 Older participants may thus view pain as a symptom of frailty due to age and avoid activities that are expected to cause harm, although they still function quite well in other areas of life.
Strengths and Limitations
This study highlights that spreading of pain and psychosocial profiles differ depending on patients’ developmental stage at pain onset. This finding points to the potential benefits of applying a life-course perspective to pain research and clinical work to understand patients’ overall needs and target them in interventions. This is especially important as chronic pain is a life-span problem, affecting people at different points of their life.1,2 In addition, the findings buttress the view that different life courses (here referred to as the developmental stage of onset) likely exude varied mechanisms, which result in the unique psychosocial outcomes observed.18 As such, this study provides a first step in exploring the different pathways through which patients with different pain-onset life stages develop their psychosocial profiles and how to address these in the clinic. The study also has the strength of including a large nationwide sample of chronic pain patients seeking specialized care in Sweden.
Likewise, some limitations of the study need to be mentioned. First, the cross-sectional design used does not indicate causality, although the focus of the current study did not seek such conclusions. Second, all measures were self-report instruments, which may bring potential biases. However, when exploring patients’ own experiences, these are the best means, and all measures are widely used with good psychometric properties documented. In addition, there was no information on the life expectancy of participants living with chronic pain, and hence the extent of bias in selection of the current study sample is unknown. Moreover, our sample did not include an older population (>65 years), as the database used focuses on a working population. Therefore, future research should explore chronic pain among older adults and its associated psychosocial outcomes, as the experience of pain may change in different contexts. In addition, developmental stage at chronic pain onset was used as a proxy of patients’ life-course exposure to chronic pain, and this does not capture the mechanism of the life-course process. In other words, in this study we were able to detect variations among groups with chronic pain onset at different life stages, but not why these variations develop. However, the current study may be a first step to understanding chronic pain from a life-course perspective. In line with this, it should also be highlighted that we sought to explore outcomes of normative life-course exposure to chronic pain. As such, we chose to exclude immigrants of non-European background with the assumption that this important subgroup is exposed to nonnormative life experiences, which in multiple and interacting ways may influence both chronic pain development directly (eg, by increasing its likelihood and severity through other immigration-related stressors)32,51 and also indirectly (eg, by influencing psychosocial outcomes through emerging educational and job-market disadvantages).52 Indeed, we found in a recent study that not only did the immigrant subgroup suffer from much higher pain burden but also their likelihood of rehabilitation participation and good rehabilitation outcomes were negatively influenced.53 Therefore, there is a dire need for future studies specifically to explore the probably complex reasons for these differences in both clinical practice and research.
Study Implications
The study has several implications for research and clinical consideration. It identifies variability in the pain characteristics and psychosocial outcomes of chronic pain based on when in an individual’s life chronic pain appears. While general health functioning and recovery expectancy were worse in patients who had chronic pain earlier in their life, fear-avoidance beliefs were lower than patients whose pain debut was later in their life course. Based on our findings, it is important to approach chronic pain research from a life-course perspective, especially using life-course longitudinal designs, in order to identify and address the mechanisms through which such psychosocial profiles emerge. Most importantly, longitudinal designs illustrating the pathways of risk accumulation over the life course may enhance our understanding of detected differences. In addition, expectancy and fear-avoidance beliefs have independent predictive values for disability, functioning, and prognosis for future functioning in patients with chronic pain.54,55 With patients with different stages at chronic pain onset differing on such domains even after controlling for demographics and pain characteristics, it is important to explore how such patient groups fare on interventions and treatment. Possibly, this will help to modify existing interventions, which are generalized, to those that target the needs of subgroups of patients with varying concerns.
Conclusion
With a sample of 6,225 chronic pain patients referred to MMR programs across Sweden, our results showed that the number of pain locations was higher in patients whose chronic pain began early in their life course. Further, this patient group had poorer psychosocial outcomes, reflected in general health functioning, life interference, and recovery expectancy. Nonetheless, patients whose pain began later in the life course reported the highest fear avoidance. Given that, developmental life stage at chronic pain onset is an important variable for determining differences in pain experience, and it is important to explore the potential driving mechanisms of such differences as potential targets in rehabilitation.
Abbreviations
HADS, Hospital Anxiety Depression Scale ; MPI, Multidimensional Pain Inventory; MMR, multimodal rehabilitation; SF36 (GH), Short Form 36 — general health; SF36, — social functioning; SQRP, Swedish Quality Register for Pain Rehabilitation; TSK, Tampa Scale for Kinesiophobia.
Data-Sharing Statement
The data set from the registry database used for this analysis is not publicly available, as the Ethical Review Board has not approved public availability of the database.
Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki, and ethical clearance was obtained from the Ethical Review Board in Uppsala, Sweden (2018/036; 2019-02167). All participants provided written consent to be included in the SQRP, the register forming the basis for this study.
Acknowledgments
We acknowledge Dalarna University for providing the infrastructure for the database used in this study. The creation of this database was supported by grants from the Swedish Research Council (dnr 2015-02512), Stockholm, Sweden and the Swedish Research Council for Health, Working Life, and Welfare (FORTE; dnr 2017-00177).
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This project has received funding from the European Union’s Horizon 2020 research and innovation program under a Marie Skłodowska-Curie grant agreement (754285).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The Global Burden of Musculoskeletal Pain—Where to From Here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
2. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602.
3. Kohrt BA, Griffith JL, Patel V. Chronic pain and mental health: integrated solutions for global problems. Pain. 2018;159(Suppl1):S85–S90. doi:10.1097/j.pain.0000000000001296
4. Malon J, Shah P, Koh WY, Cattabriga G, Li E, Cao L. Characterizing the demographics of chronic pain patients in the state of Maine using the Maine all payer claims database. BMC Public Health. 2018;18(1):810. doi:10.1186/s12889-018-5673-5
5. Gibson SJ, Chambers CT. Pain over the Lifespan: A developmental perspective. In: Hadjistavropoulos T, Craig KD, editors. Pain: Psychological Perspectives. US: Lawrence Erlbaum Associates Publishers; 2004:113–153.
6. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287. doi:10.1016/j.ejpain.2005.06.009
7. Tsang A, Von Korff M, Lee S, et al. Common Chronic Pain Conditions in Developed and Developing Countries: gender and Age Differences and Comorbidity With Depression-Anxiety Disorders. J Pain. 2008;9(10):883–891. doi:10.1016/j.jpain.2008.05.005
8. Larsson C, Ekvall Hansson E, Sundquist K, Jakobsson U. Impact of pain characteristics and fear-avoidance beliefs on physical activity levels among older adults with chronic pain: a population-based, longitudinal study. BMC Geriatr. 2016;16(1):50. doi:10.1186/s12877-016-0224-3
9. Patel KV, Guralnik JM, Dansie EJ, Turk DC. Prevalence and impact of pain among older adults in the United States: findings from the 2011 National Health and Aging Trends Study. PAIN®. 2013;154(12):2649–2657. doi:10.1016/j.pain.2013.07.029
10. Jakobsson U. The epidemiology of chronic pain in a general population: results of a survey in southern Sweden. Scand J Rheumatol. 2010;39(5):421–429. doi:10.3109/03009741003685616
11. King S, Chambers CT, Huguet A, et al. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain. 2011;152(12):2729–2738. doi:10.1016/j.pain.2011.07.016
12. Gobina I, Villberg J, Välimaa R, et al. Prevalence of self-reported chronic pain among adolescents: evidence from 42 countries and regions. Eur J Pain. 2019;23(2):316–326. doi:10.1002/ejp.1306
13. Baltes PB. Theoretical propositions of life-span developmental psychology: on the dynamics between growth and decline. Dev Psychol. 1987;23(5):611. doi:10.1037/0012-1649.23.5.611
14. Baltes PB, Smith J. Lifespan Psychology: from Developmental Contextualism to Developmental Biocultural Co-constructivism. Res Hum Dev. 2004;1(3):123–144. doi:10.1207/s15427617rhd0103_1
15. Bengtson VL, Elder GH, Putney NM. The life course perspective on ageing: linked lives, timing, and history. In: Katz J, Peace S, Spurr S, editors. Adult Lives: A Life Course Perspective. Policy Press; 2011:9–17.
16. Kuh D, Ben-Shlomo Y, Lynch J, Hallqvist J, Power C. Life course epidemiology. J Epidemiol Community Health. 2003;57(10):778–783. doi:10.1136/jech.57.10.778
17. Dannefer D. Cumulative Advantage/Disadvantage and the Life Course: cross-Fertilizing Age and Social Science Theory. J Gerontol. 2003;58(6):S327–S337. doi:10.1093/geronb/58.6.S327
18. Ferraro KF, Shippee TP. Aging and Cumulative Inequality: how Does Inequality Get Under the Skin? Gerontologist. 2009;49(3):333–343. doi:10.1093/geront/gnp034
19. Devins GM, Binik YM, Hutchinson TA, Hollomby DJ, Barré PE, Guttmann RD. The Emotional Impact of End-Stage Renal Disease: importance of Patients’ Perceptions of Intrusiveness and Control. Int J Psychiatry Med. 1984;13(4):327–343. doi:10.2190/5DCP-25BV-U1G9-9G7C
20. Devins GM. Illness Intrusiveness and the Psychosocial Impact of Lifestyle Disruptions in Chronic Life-Threatening Disease. Adv Ren Replace Ther. 1994;1(3):251–263. doi:10.1016/S1073-4449(12)80007-0
21. Devins GM, Bezjak A, Mah K, Loblaw DA, Gotowiec AP. Context moderates illness-induced lifestyle disruptions across life domains: a test of the illness intrusiveness theoretical framework in six common cancers. Psycho Oncol. 2006;15(3):221–233. doi:10.1002/pon.940
22. Dorian P, Jung W, Newman D, et al. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J Am Coll Cardiol. 2000;36(4):1303. doi:10.1016/S0735-1097(00)00886-X
23. Andersen LL, Clausen T, Carneiro IG, Holtermann A. Spreading of chronic pain between body regions: prospective cohort study among health care workers. Eur J Pain. 2012;16(10):1437–1443. doi:10.1002/j.1532-2149.2012.00143.x
24. Riley JL, Wade JB, Robinson ME, Price DD. The stages of pain processing across the adult lifespan. J Pain. 2000;1(2):162–170. doi:10.1016/S1526-5900(00)90101-9
25. Harris S, Morley S, Barton SB. Role loss and emotional adjustment in chronic pain. Pain. 2003;105(1):363–370. doi:10.1016/S0304-3959(03)00251-3
26. Svanberg M, Stålnacke B-M, Enthoven P, Brodda-Jansen G, Gerdle B, Boersma K. Impact of emotional distress and pain-related fear on patients with chronic pain: subgroup analysis of patients referred to multimodal rehabilitation. J Rehabilitation Med. 2017;49(4):354–361.
27. Murray CB, Groenewald CB, de la Vega R, Palermo TM. Long-term impact of adolescent chronic pain on young adult educational, vocational, and social outcomes. Pain. 2020;161(2):439–445.
28. Gerdle B, Åkerblom S, Brodda Jansen G, et al. Who benefits from multimodal rehabilitation - an exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish Quality Registry for Pain Rehabilitation. J Pain Res. 2019;12:891–908. doi:10.2147/JPR.S190003
29. LoMartire R, Äng BO, Gerdle B, Vixner L. Psychometric properties of Short Form-36 Health Survey, EuroQol 5-dimensions, and Hospital Anxiety and Depression Scale in patients with chronic pain. Pain. 2020;161(1):83–95. doi:10.1097/j.pain.0000000000001700
30. Alföldi P, Wiklund T, Gerdle B. Comorbid insomnia in patients with chronic pain: a study based on the Swedish quality registry for pain rehabilitation (SQRP). Disabil Rehabil. 2014;36(20):1661–1669. doi:10.3109/09638288.2013.864712
31. Lachman ME, Teshale S, Agrigoroaei S. Midlife as a pivotal period in the life course: balancinggrowth and decline at the crossroads of youth and old age. Int J Behav Dev. 2015;39(1):20–31. doi:10.1177/0165025414533223
32. Strømme EM, Haj-Younes J, Hasha W, Fadnes LT, Kumar B, Diaz E. Chronic pain and migration-related factors among Syrian refugees: a cross-sectional study. Eur J Public Health. 2019;29(Supplement_4). doi:10.1093/eurpub/ckz185.422
33. Miller RP, Kori SH, Todd DD. The Tampa Scale: a Measure of Kinisophobia. Clin J Pain. 1991;7(1):51. doi:10.1097/00002508-199103000-00053
34. Kaiser U, Kopkow C, Deckert S, et al. Developing a core outcome domain set to assessing effectiveness of interdisciplinary multimodal pain therapy: the VAPAIN consensus statement on core outcome domains. Pain. 2018;159(4):673–683. doi:10.1097/j.pain.0000000000001129
35. Turk DC, Dworkin RH, Revicki D, et al. Identifying important outcome domains for chronic pain clinical trials: an IMMPACT survey of people with pain. PAIN®. 2008;137(2):276–285. doi:10.1016/j.pain.2007.09.002
36. Kerns RD, Turk DC, Rudy TE. The west haven-yale multidimensional pain inventory (WHYMPI). Pain. 1985;23(4):345–356. doi:10.1016/0304-3959(85)90004-1
37. Bergström G, Jensen IB, Bodin L, Linton SJ, Nygren ÅL, Carlsson SG. Reliability and factor structure of the Multidimensional Pain Inventory – swedish Language Version (MPI-S). Pain. 1998;75(1):101–110. doi:10.1016/S0304-3959(97)00210-8
38. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. J Acta psychiatrica scandinavica. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
39. French DJ, France CR, Vigneau F, French JA, Evans RT. Fear of movement/(re)injury in chronic pain: A psychometric assessment of the original English version of the Tampa scale for kinesiophobia (TSK). Pain. 2007;127(1):42–51. doi:10.1016/j.pain.2006.07.016
40. Boersma K, Linton SJ. Expectancy, fear and pain in the prediction of chronic pain and disability: A prospective analysis. Eur J Pain. 2006;10(6):551. doi:10.1016/j.ejpain.2005.08.004
41. Ware JE, Sherbourne CD, The MOS. 36-ltem Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
42. Sullivan M, Karlsson J, Ware JE. The Swedish SF-36 Health Survey—I. Evaluation of data quality, scaling assumptions, reliability and construct validity across general populations in Sweden. Soc Sci Med. 1995;41(10):1349–1358. doi:10.1016/0277-9536(95)00125-Q
43. Cohen J. Statistical power Analysis for the Behavioral Sciences.. San Diego: Academic Press; 1969.
44. Richardson JTE. Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev. 2011;6(2):135–147. doi:10.1016/j.edurev.2010.12.001
45. Ge H-Y, Fernández-de-las-Peñas C, Madeleine P, Arendt-Nielsen L. Topographical mapping and mechanical pain sensitivity of myofascial trigger points in the infraspinatus muscle. Eur J Pain. 2008;12(7):859–865. doi:10.1016/j.ejpain.2007.12.005
46. Harte SE, Harris RE, Clauw DJ. The neurobiology of central sensitization. J Appl Biobehav Res. 2018;23(2):e12137.
47. O’Neill S, Manniche C, Graven-Nielsen T, Arendt-Nielsen L. Generalized deep-tissue hyperalgesia in patients with chronic low-back pain. Eur J Pain. 2007;11(4):415–420. doi:10.1016/j.ejpain.2006.05.009
48. Leventhal EA, Prohaska TR. Age, symptom interpretation, and health behavior. J Am Geriatr Soc. 1986;34(3):185–191.
49. Thielke S, Sale J, Reid MC. Aging: are these 4 pain myths complicating care? J Fam Pract. 2012;61(11):666–670.
50. Stubbs B, Eggermont LHP, Patchay S, Schofield PA. Pain Interference Is Associated With Psychological Concerns Related to Falls in Community-Dwelling Older Adults: multisite Observational Study. Phys Ther. 2014;94(10):1410–1420. doi:10.2522/ptj.20140093
51. Kurita GP, Sjøgren P, Juel K, Højsted J, Ekholm O. The burden of chronic pain: A cross-sectional survey focussing on diseases, immigration, and opioid use. PAIN®. 2012;153(12):2332–2338. doi:10.1016/j.pain.2012.07.023
52. Fernandez Macias E, Paniagua T. Labour Market Integration of Migrants and Their Descendants. Dublin: European Foundation for the Improvement of Living and Working Conditions; 2018.
53. Gerdle B, Boersma K, Åsenlöf P, B-M S, Larsson B, Ringqvist Å. Influences of Sex, Education, and Country of Birth on Clinical Presentations and Overall Outcomes of Interdisciplinary Pain Rehabilitation in Chronic Pain Patients: A Cohort Study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J Clin Med. 2020;9:8. doi:10.3390/jcm9082374
54. Boersma K, Linton SJ. Screening to Identify Patients at Risk: profiles of Psychological Risk Factors for Early Intervention. Clin J Pain. 2005;21(1):38–43. doi:10.1097/00002508-200501000-00005
55. Tseli E, Vixner L, Lomartire R, Grooten WJA, Gerdle B, Äng BO. Prognostic Factors for Improved Physical and Emotional Functioning One Year After Interdisciplinary Rehabilitation in Patients with Chronic Pain: results from a National Quality Registry in Sweden. J Rehabilitation Med. 2020;52(2):1–10.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.