")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Content of Physiotherapy and Factors Impacting on Reablement – A National Study
Authors Olsson Möller U , Zingmark M, Ekstrand J , Haak M
Received 30 March 2023
Accepted for publication 14 September 2023
Published 20 October 2023 Volume 2023:16 Pages 3075—3088
DOI https://doi.org/10.2147/JMDH.S415112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ulrika Olsson Möller,1,2 Magnus Zingmark,2– 5 Joakim Ekstrand,1 Maria Haak1
1Department of Nursing and Health Sciences, Faculty of Health Science, Kristianstad University, Kristianstad, Sweden; 2Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden; 3Department of Epidemiology and Global Health, Faculty of Medicine, Umeå University, Umeå, Sweden; 4Health and Social Care Administration, Municipality of Östersund, Östersund, Sweden; 5Department of Community Medicine and Rehabilitation, Faculty of Medicine, Umeå University, Umeå, Sweden
Correspondence: Ulrika Olsson Möller, Department of Nursing and Health Sciences, Elmetorpsvägen 15, Kristianstad, 291 39, Sweden, Email [email protected]
Purpose: Reablement is a multidisciplinary intervention aimed at promoting function and independence for people with functional decline. Detailed descriptions of various professions’ actions are needed for organization and evaluation of reablement services. This study describes physiotherapy practice in a reablement context in Swedish municipalities, focusing on the content and magnitude of interventions.
Methods: Physiotherapists (n=108) from 34 municipalities answered a web-based survey covering the target group, content and duration of their actions, and number of contacts initiated over a 3-week period. Data were analyzed with descriptive statistics and multiple logistic regression.
Results: Overall, 1005 cases were reported, with a mean age of 78.9 years (SD: 11.7); about 91% (n=912) were aged ≥ 65 and 61% (n=612) were women. About 70% were allocated to home care; 16% (n=160) of these had minor functional limitations (eg, needing safety alarms/help with domestic tasks), and 55% (n=550) had major functional limitations (eg, needing help with personal activities of daily living). The most reported actions were providing technical aids (60.8%, n=576), instructions/counseling (41.5%, n=393), walking/climbing stairs (27.6%, n=262), strength training (27.2%, n=258), and fall prevention (25.5%, n=242). Almost half of the cases included one action (n=494) and about 89% (n=890) targeted primary needs (body functions, walking indoors, self-care, or domestic life), mainly in clients with major functional limitations (odds ratio=2.96; 95% confidence interval: 1.95– 4.49). About 50% (n=517) of the cases involved 1– 2 contacts; about 55% (n=549) were completed within 3 weeks. Exercise was associated with ≥ 6 visits over ≥ 7 weeks. Supervision of home care staff was performed in 19.1% (n=181) of cases.
Conclusion: Reablement physiotherapy mostly comprises a few actions over a relatively short period. Whether this is a conscious strategy based on the purpose of home-based physiotherapy or clients’ needs and wishes, or conversely an expression of limited resources, remains to be investigated.
Keywords: healthy aging, home care, physical activity, physiotherapy, reablement, technical aids
Introduction
In Sweden today, many people with physical disabilities live at home and receive the necessary health care and services there, instead of living in institutional care.1 Despite substantial actions to promote healthy aging, the number of older people living at home and needing professional care and services will most likely increase. Consequently, efforts to create good conditions for them to live at home as safely and independently as possible need to be prioritized. Reablement is a multidisciplinary intervention aimed at enhancing physical or other functioning, increasing or maintaining independence, and reducing the need for long-term services.2 It can be provided irrespective of a person’s age, ability, diagnosis, or setting,2 although older people living at home have been the overall target population in the context of reablement so far.3 Reablement focuses on the person’s abilities, resources, and possibilities to adapt to a declining function,4 and involves a person-centered, goal-oriented, and time-limited service5 from different health care professionals (HCPs).
To allow an individual to achieve their goals, reablement should include initial assessment and the development and implementation of an action plan, followed by regular reassessments to ensure that the actions are adjusted to the person’s needs during the process.2 Actions can involve training of daily activities, environmental modifications, assistive devices,2 or exercise6 depending on the person’s goals of daily living, including social, leisure, or physical activities. Through this approach, reablement has the potential to support older people in staying at home as safely and independently as possible. However, research so far shows inconsistent findings on the effects of reablement interventions.4,5 Moreover, there has been little research into how reablement is operationalized, which limits the ability to organize and evaluate reablement services. Accordingly, because of a lack of infrastructure, resources, capacity, training, and coordination/cohesion between professional groups, reablement programs are rarely implemented.3
Reablement often requires multiprofessional efforts, and the composition of the reablement team includes a mix of health care and social care professionals2 such as physiotherapists (PTs), occupational therapists (OTs), nurses, home care staff, and social workers. Rehabilitation professionals (OTs and PTs) play a major role in enabling people to live at home as safely and independently as possible.7–10 Reablement actions from the perspective of OTs and PTs in a Swedish context have recently been explored by Zingmark et al (2020),11 showing both similarities and differences between PTs and OTs in terms of the content, duration, and number of contacts. The client’s ability to walk indoors was the main focus of both professions, but was reported significantly more often by PTs than by OTs (72% vs 63%, p≥0.001). Among OTs, the second most common focus was clients’ self-care, while for PTs, the second most common focus was body function (strength, balance, etc.). Both groups of professionals placed the least focus on social contacts and communication.
Another study used data from the same survey to explore OTs’ actions with a focus on social participation.12 The findings showed that most occupational therapy actions did not focus on social participation, but rather on basic needs such as personal activities of daily living and indoor mobility, particularly for clients with major functional limitations. Given the multidisciplinary and complex nature of reablement, there is a need to explore physiotherapy in the same context to understand how reablement is operationalized. This will bring new knowledge of the similarities and differences between professionals, which is important to ensure that the overall intervention for the client is sufficient and optimal. The present study therefore used data from the same survey11,12 to explore physiotherapy in this context.
Home-based PTs’ actions play a vital role in improving their clients’ functional capacity in order to maintain independence, increase overall physical wellbeing, and enhance social functioning.13,14 However, there are considerable variations in how home-based physiotherapy is organized.10 A recent study15 exploring physiotherapy in the context of teamwork in reablement in Norway found a large variation in the practice of physiotherapy in reablement teams. Observations of reablement interventions and interviews with PTs revealed three features of practice: division of labor, assessment, and intervention. Based on differences in the features, two typologies with different characteristics emerged: a fixed structure and a flexible structure. In the fixed, hierarchical structure, the assessments were limited to standardized measurement tools, and the rehabilitation plans mainly included general exercise programs. Conversely, in the flexible, flat structure, assessments of physical function were conducted in addition to standardized measurements, and PTs were more involved in the process of tailoring interventions to the users’ goals and functional decline.15
The abovementioned Norwegian study15 clearly shows that within physiotherapy, different structures of labor are practiced in the reablement setting. This creates challenges, not only in terms of the ability to demonstrate the impact of interventions, but also in relation to equity of care. Moreover, it makes it challenging to provide person-centered care in this context. In addition, a recent systematic review failed to identify the “black box” of reablement, and was unable to name the most promising features in reablement in terms of increasing clients’ daily functioning, in part due to poorly described intervention content.16 Taken together, this emphasizes the importance of continuing to investigate the content of physiotherapy practice. The purpose of the present study was therefore to describe physiotherapy in the reablement context in Swedish municipalities, with a focus on the content and duration of the intervention and the number of contacts, and to explore how age, gender, and level of functioning had an impact on the interventions delivered by PTs.
Methods
Context and Participants
The context of reablement in Sweden has been described in detail by Zingmark et al (2020)11 and Bergström et al (2019).7 In brief, reablement in Sweden is regulated both by social care legislation and by health care legislation, and there is variation in how reablement is organized, which professions are involved, and which population is targeted (all adults in need of social care vs only adults with extensive needs for support in daily living). PTs and OTs usually work closely together, and the assessments and actions usually take part in the client’s home. Within this context, PTs and OTs initiate rehabilitation, habilitation, housing adaptation, and provision of technical aids. PTs and OTs also provide supervision of home care staff.
Of the 290 municipalities in Sweden, 60 employ a local authority senior rehabilitation advisor (LASRA) (at the time of the study). LASRAs are responsible for quality assurance of the home healthcare in their municipalities.11 At the beginning of the present study, these 60 municipalities were invited to take part via the national network of LASRAs. They received information by email about the study, including how it was to be conducted, and were assured that participation would be voluntary. The type of intervention relevant to the study was defined as follows: (a) OTs or PTs were the main coordinators in the reablement work; (b) interventions were implemented in the clients’ own homes (standard housing, ie care homes excluded); (c) the main focus was on daily activities that were important to the clients; (d) the interventions included collaboration with home care staff; (e) interventions were organized within a municipal context (also including private companies); and (f) interventions included collaboration with other professionals, such as district nurses, social workers, and the managers of the home care staff.11
In the 38 municipalities willing to participate, PTs were invited by email via the LASRA and received information about the aim, content, and procedure of the study, including the voluntary nature of participation. The municipalities were geographically spread over the country and included urban as well as rural areas. In total, 108 PTs from 34 municipalities participated in the present study (representing 32% of the PTs in the participating municipalities). At the time of data collection, the populations of these municipalities ranged from 9011 to 333,633, with an overall total of 2,466,799 (representing 24% of the entire population of Sweden). The number of full-time equivalent positions in the municipalities ranged from 1.5 to 60.11
Data Collection
The present study used data from a web-based survey specifically developed for the study to collect information about the target group, the content and focus of interventions, the use of assessments, and collaboration with other professionals. The content of the survey was discussed within the national network of LASRAs to ensure that the questions were relevant. The PTs were instructed to describe interventions initiated over a 3-week period in September–October 2017 for first-time clients or for ongoing clients in whom a “new need” had been identified. Each description represented a “case”. For each case, the PT answered 30 questions including data on the client (age, gender, allocation to homecare), type of intervention (several options could be specified), and frequency (number of contacts) and duration (number of weeks) of the intervention (Appendix 1). The survey mainly included fixed response options, such as lists of common physiotherapy actions, with the possibility to add answers as free text. The action list included training in activity, strength and balance training, range of motion, standing training, walking/climbing stairs, pain treatment, respiratory training, fall prevention, technical aids, environmental modifications, instruction/counseling, advice to relatives, and supervision of home care staff. Each case was followed for as long as the intervention was ongoing, with a maximum of 15 weeks. A detailed description of the data collection procedure is given elsewhere.11
Data Analysis
Descriptive statistics were used to explore the content and magnitude (duration, number of contacts) of the PTs’ actions. All response alternatives except age were at the nominal or ordinal level. Prevalence rates were calculated to explore the content of physiotherapy actions in relation to level of functioning, number of contacts (1–2, 3–5, 6–9, ≥10), and duration of intervention (<1 week, 1–3 weeks, 4–6 weeks, 7–9 weeks, ≥10 weeks). Level of functioning was categorized into three groups in relation to dependency (allocation to home care): no home care, minor functional limitations (needing safety alarms and/or help with domestic tasks), or major functional limitations (needing help with personal activities of daily living). Pearson’s chi-square test was used to identify associations between group variables, and p≤0.05 was considered statistically significant. Differences between groups were interpreted using 95% confidence intervals (CIs).
Since many individuals received more than one type of action per visit, multiple logistic regression was used to analyze which type of actions affected the probability of receiving many contacts or a long duration of intervention. The number of contacts was dichotomized to 1–5 contacts versus ≥6 contacts, and the duration of the intervention was dichotomized to ≤6 weeks versus ≥7 weeks. These thresholds were adopted in order to identify resource-intensive interventions, as most cases involved 1–5 visits and lasted ≤6 weeks. Hence, the dependent variables were number of contacts (1–5 contacts = 0, ≥6 contacts = 1) and duration of the intervention (≤6 weeks = 0, ≥7 weeks = 1), with action types as independent variables.
Multiple logistic regression (manual backward) was also used to analyze whether age, gender, and level of functioning affected the probability of receiving interventions that focused mainly on primary needs or on social participation. The dependent variable in this case was specified as primary needs (= 1)/social participation (= 0), with age, gender, and level of functioning as independent variables. Primary needs included the variables body functions, walking indoors, self-care, and domestic life. Social participation included walking outdoors, social contacts, communication, and leisure. No formal power calculation was made a priori, but the sample size was deemed sufficient (n=1005). Data from the multiple logistic regression are presented here as odds ratios (ORs) with 95% CIs. The analyses were performed using version 27 of IBM SPSS Statistics (IBM Corporation, Armonk, NY, USA).
Results
The 108 PTs reported a total of 1005 cases with a mean age of 78.9 years (SD 11.7); the majority (90.7%, n=912) were ≥65 years of age and 61% (n=612) were women. When divided by gender, the mean age was 79.4 years (SD 11.7) among the women and 78.1 years (SD 11.6) among the men. Concerning level of functioning and dependency, 29.4% (n=295) were not allocated to home care (mean age: 73.9 years, SD 12.6), 15.9% (n=160) had minor functional limitations (mean age: 79.4 years, SD 11.2), and 54.7% (n=550) had major functional limitations (mean age: 81.4 years, SD 10.4). The proportion of women was 61.9% (n=182), 58.8% (n=94), and 61.1% (n=336) in these three groups, respectively.
An intervention was reported in 948 of the 1005 cases (94.3%), and the most frequently reported actions were related to technical aids (60.8%, n=576), instructions/counseling (41.5%, n=393), walking/climbing stairs (27.6%, n=262), strength training (27.2%, n=258), and fall prevention (25.5%, n=242) (Table 1). A case could include more than one action/intervention (for example, a combination of technical aids, balance training, and fall prevention). Almost half of the cases (49.2%, n=494) had 1 type of action, 34.2% (n=344) had 2 types, 13.6% (n=137) had 3 types, and 3.0% (n=30) had 4–7 types. Most of the actions (88.6%, n=890) targeted primary needs while the remainder (11.4%, n=115) targeted social participation.
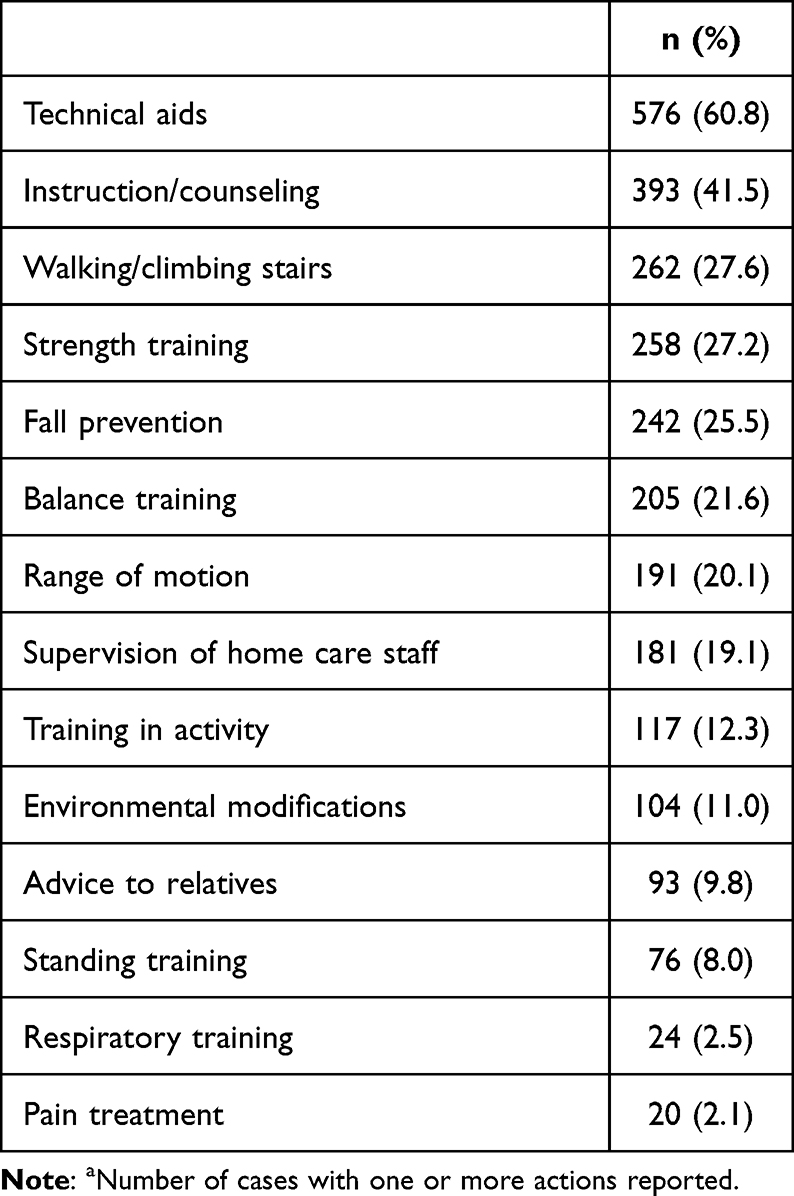 |
Table 1 Actions (n=948a) Reported by Physio-therapists (PTs) |
Level of Functioning
Exploring type of intervention in relation to level of functioning among the 1005 cases (Table 2) revealed that having major functional limitations (n=550) was associated with receiving training in walking/climbing stairs (n=183), range of motion (n=131), supervision of home care staff (n=163), standing training (n=58) (p<0.001), and respiratory training (n=22) (p=0.001). This means that clients with major functional limitations received these actions more often than clients with no or only minor functional limitations. By contrast, having no functional limitations (n=295) was associated with fall prevention (n=88) (p=0.02) and technical aids (n=193) (p<0.001).
 |
Table 2 Type of Action in Relation to Level of Functioning (n=1005) |
Number of Contacts
Data on the number of contacts were available for 1003 cases (Table 3), showing that 51.5% (n=517) received 1–2 visits, 27.0% (n=271) received 3–5 visits, 11.8% (n=118) received 6–9 visits, and 9.7% (n=97) received ≥10 visits. The physiotherapy action involving technical aids (n=576) was associated with the number of contacts (p<0.001); those who had ≤5 contacts (n=788) received this action more often. Moreover, walking/climbing stairs (n=262), strength training (n=258), fall prevention (n=242), balance training (n=205), range of motion (n=191), supervision of home care staff (n=181), training in activity (n=117), advice to relatives (n=93), standing training (n=76), respiratory training (n=24), and pain treatment (n=20) were also associated with the number of contacts (p<0.001–p=0.024) but in the other direction, meaning that those with ≥6 contacts (n=215) received those actions more frequently. No significant associations were seen between number of contacts and either instruction/counseling (n=393) or environmental modifications (n=104) (Table 3).
 |
Table 3 Type of Action in Relation to Number of Contacts (n=1003) |
Duration of the Intervention
Considering the duration of the intervention (Table 4), 27.6% (n=277) of interventions were completed in <1 week, 27.1% (n=272) within 1–3 weeks, 15.7% (n=158) within 4–6 weeks, 8.6% (n=85) within 7–9 weeks, and 21.0% (n=211) in ≥10 weeks. Overall, almost 30% of the interventions lasted for 7 weeks or more. Technical aids (n=576) were associated with shorter duration (p<0.001), as those with this action more often had ≤6 weeks of intervention. Several other actions were associated with longer duration (p<0.001), with cases that received these actions more often having ≥7 weeks of intervention (n=296): walking/climbing stairs (n=262), strength training (n=258), balance training (n=205), range of motion (n=191), supervision of home care staff (n=181), training in activity (n=117), advice to relatives (n=93), and standing training (n=76). No significant associations were seen between duration and instruction/counseling (n=393), fall prevention (n=242), environmental modifications (n=104), respiratory training (n=24), or pain treatment (n=20) (Table 4).
 |
Table 4 Type of Action in Relation to the Duration of the Intervention (n=1003) |
Factors Impacting Physiotherapy Practice
Analysis of the probability of receiving interventions mainly focused on either primary needs or social participation. The regression analyses (Table 5) showed that clients with major functional limitations had a three times greater probability of receiving physiotherapy for primary needs (OR=2.96, 95% CI=1.95–4.49). The probability of receiving physiotherapy for primary needs or social participation was not affected by age or gender.
 |
Table 5 Factors Impacting the Focus of the Intervention, the Number of Contacts, and the Duration of the Intervention |
Several actions were associated with increased odds of having ≥6 visits: pain treatment (OR=7.87, 95% CI=2.46–25.19), strength training (OR=6.14, 95% CI=3.68–10.22), training in activity (OR=3.80, 95% CI=2.28–6.33), balance training (OR=3.13, 95% CI=1.85–5.32), supervision of home care staff (OR=2.95, 95% CI=1.76–4.94), walking/climbing stairs (OR=2.85, 95% CI=1.88–4.32), and standing training (OR=2.39, 95% CI=1.20–4.54). None of the actions were related to lower odds of having ≥6 visits.
Actions associated with increased odds of receiving physiotherapy for ≥7 weeks were supervision of home care staff (OR=3.37, 95% CI=2.20–5.15), strength training (OR=3.33, 95% CI=2.07–5.34), balance training (OR=2.57, 95% CI=1.54–4.36), range of motion (OR=2.44, 95% CI=1.62–3.67), training in activity (OR=2.42, 95% CI=1.47–3.96), and standing training (OR=2.01, 95% CI=1.07–3.75). Actions associated with lower odds of receiving intervention for ≥7 weeks were technical aids (OR=0.68, 95% CI=0.48–0.97), instruction/counseling (OR=0.65, 95% CI=0.46–0.94), and fall prevention (OR=0.62, 95% CI=0.41–0.95).
Discussion
In this study, which focused primarily on persons aged ≥65 years, about 55% of the clients had a major functional limitation. The most frequently reported physiotherapy action was related to technical aids, mainly targeting clients with no or minor functional limitations. This action involved few contacts, and the intervention lasted only a short period of time. A previous study,11 exploring the same cohort but focusing instead on the assessment, goalsetting, and/or intervention, showed that walking indoors was the most prevalent focus for PTs in this setting; this implies that most of the technical aids reported in this study, such as sticks, canes, or walkers, were aimed at increasing walking capacity. The use of walking aids is important, as it helps to maintain balance and improve mobility;17 well-maintained mobility, in turn, can improve life satisfaction in aging by lowering mortality and fall risk, increasing physical strength and independence, and allowing social connectedness to be maintained.18 The results of the present study indicate that providing technical aids seems to be an action requiring very few resources from the PT. The importance of training HCPs for the proper prescription, fitting, user training, and follow-up of assistive products has been emphasized,19 and future studies need to explore the actions, goals, and effects related to technical aids and PTs’ actions in reablement settings.
Different forms of exercise and physical activity (strength, balance, training in activity), although surprisingly only constituting 22–27% of the actions, required a high number of contacts over a longer period of time. These actions were executed independently of the clients’ functional status (no/minor/major limitations). Most of the actions required >6 contacts and a duration of 7 weeks or more; strength training was the most common action that required ≥10 contacts over a period of ≥10 weeks. This shows that physiotherapy actions directed toward exercise or physical activity are resource-intensive. It is well known that physical exercise must be undertaken on a regular basis to increase and maintain function in older persons,20 and this is important to consider when planning care for older persons living at home. A combination of exercise-based and activity-based approaches has been suggested to enhance clients’ functional abilities.21 Physical activity and exercise are a cornerstone of healthy aging, and are also the interventions with the highest evidence for preventing falls in older people.22 They should therefore constitute a major part of the work conducted in this population by PTs, who are experts in motor learning and re-learning. From the older person’s perspective, PTs’ expertise and the person-centered approach in home-based exercise is invaluable.23
Fall prevention, constituting 25.5% of the actions, was given statistically significantly more often to clients with no functional limitations, in comparison to those with minor or major functional limitations. This is promising, as fall prevention should be introduced before the first fall; the reason for this is that many older people experience fear of falling and loss of confidence after a fall, which further increases the risk of recurrent falls.24 In the majority of cases (80%), fall prevention required 10 or more contacts but was executed in <7 weeks. It is therefore reasonable to assume that although fall prevention may include multifactorial and multi-component actions, as recommended,25 strength and balance training did not seem to be a consistent part of fall prevention interventions despite recommendations.22 This is in contrast to the evidence that fall prevention should be a multifactorial intervention that includes components such as exercise, environment/assistive technology, and knowledge/educational interventions.25 However, the previously mentioned study on the same cohort11 showed no difference in the number of actions related to fall prevention, which indicates that fall prevention, at least, is an OT/PT team-based intervention. As exercise is currently the single most important intervention to prevent falls,22 future studies are needed to further explore the composition of exercise interventions as part of the multidomain, person-centered interventions that are recommended by the global initiative to prevent falls.26 In a qualitative interview study conducted in Norway,27 HCPs perceived barriers and facilitators to promoting physical activity as a part of reablement at the participant, professional, organizational, and system level, and suggested that a “whole-system perspective” is required to promote physical activity in real-life health care settings.
The second most commonly reported action was instruction/counseling. This action could target the home care staff as well as clients and their relatives; the frequency can therefore be considered low, as most of the PTs’ actions, not least fall prevention, require some kind of information or instruction. However, the frequency of the action did not differ significantly between levels of functioning, number of contacts, or duration of the intervention, and so it is difficult to interpret the significance of this action in physiotherapy practice.
Pain management was the intervention most likely to involve several visits (OR=7.87, 95% CI=2.46–25.19). However, given that pain management was a rare physiotherapy action (2.1%), it is difficult to draw any conclusions on the resources that this action requires.
Supervision of home care staff was performed in 19% of cases, mainly for clients with major functional limitations. This action was also the strongest indicator for receiving ≥7 weeks of physiotherapy. According to a qualitative study investigating interdisciplinary care,28 PTs initiate various interventions that relate to body function (ie the ability to move about safely and securely) and then delegate the actions to home care staff, who proceed to support the client to further improve function while maintaining safety. Close collaboration between the PT and home care staff is essential for individually tailored service aimed at achieving quality of movement.29 Flexible teamwork with a focus on person-centered reablement that aims to make the client an active co-creator of their care may be more resource-intensive,29,30 but this might be a necessary shift in work culture to meet future health care needs.30 Home care staff competence and experience in reablement is also important in promoting physical activity.27 Our study highlights the extent of teamwork in physiotherapy, which is necessary knowledge for planning future resources to achieve the goals of healthy aging and an independent older population.
As in the previously-mentioned study which explored occupational therapy interventions in the same cohort as the present one,12 very few actions (11.4%) in our study population targeted social participation (walking outdoors, social contacts, communication, and leisure). The factor that determined whether a client received an intervention focusing on primary needs or social participation was level of functioning, not age or gender. The results also showed that having a major functional limitation tripled the odds of receiving physiotherapy for primary needs. This indicates that, from a physiotherapy as well as an occupational therapy perspective, few interventions are aimed at increasing social participation for clients with major functional limitations. Specifically, the actions walking/climbing stairs, range of motion, and standing training were significantly more often targeted at clients with major functional limitations than at clients with no or minor functional limitations. Together with the results that most interventions (83%) only had 1–2 foci, and that about half of the interventions involved only 1–2 visits and lasted a maximum of 3 weeks, this may indicate that achievements relating to primary needs are seen as “good enough.” This should, however, not be considered a sufficient goal, as social participation is important for increasing health and quality of life among older people.31,32 A recent scoping review33 aiming to investigate the volume of evidence for physical activity interventions among adults aged 60+ showed that very few reviews assessed outcomes of social participation. More PT-led reablement actions to address clients’ wishes and needs for social participation are needed, but this area remains to be explored.
Taken together, several of our findings indicate that physiotherapy mainly comprises one or a few actions executed over a few weeks, mainly involves technical aids, and mainly focuses on primary needs. This illustrates that physiotherapy in reablement principally aims to compensate for an impairment (ie, using a passive approach), rather than trying to improve/maintain physical function (which would mean having an active approach). Whether this is a conscious strategy based on the purpose of home-based physiotherapy or clients’ needs and wishes, or conversely an expression of limited resources, needs to be investigated in future studies.
Limitations
The municipalities included may not be representative of all Swedish municipalities, since recruitment was based on the national network of LASRAs. Many municipalities do not have LASRAs (or at least did not have them at the beginning of the study). However, the study included municipalities across the country, with various population sizes, representing approximately a quarter of the entire population. This study therefore provides the first detailed picture of the content and composition of physiotherapy in a Swedish reablement context. Detailed information about the study and data collection has been provided, but a different approach to organizing reablement and a different study population may have resulted in a different interpretation of the questions, and hence different responses. This risk was reduced by using a standardized survey. However, the low response rate (32%) is a limitation to be considered when interpreting the results.
No data on clients’ health was collected in this study, but it is reasonable to assume that their health and function were similar to that presented in other articles in the Nordic reablement context.34,35 The data analyses were based on our assumption that aspects such as outdoor mobility, leisure, social contacts, and communication are related to social participation, and so the results should be interpreted with this in mind. Another limitation is that our data do not include information on whether informal care was provided. It is likely that in many cases informal care was provided in parallel to municipal home care, including for those who had not been allocated to home care. Although some years have passed since the study was conducted, including the pandemic years, no major reforms have been conducted during this time in the field of reablement or in home health care in Sweden. We therefore consider the results to be highly relevant as a basis for describing and reflecting over physiotherapy practice in reablement. Finally, the multidisciplinary nature of reablement means that there is a possibility of other professions performing interventions that are usually performed by PTs, and vice versa. This must be considered when interpreting the results of this study. To further explore the content of reablement, future studies need to investigate interventions that are generic as well as interventions that are, and must be, specific for each profession.
Conclusions
This study contributes detailed information on the content and magnitude of PTs’ actions in Swedish reablement settings. About 50% of the actions targeted clients with major functional limitations, and almost 90% of the actions targeted primary needs. Clients with major functional limitations had higher odds of being targeted with actions relating to primary needs, and were given actions related to walking/climbing stairs, range of motion, and standing training, while clients with no or minor functional limitations received technical aids and fall prevention actions. The most frequently reported physiotherapy action was the provision of technical aids, followed by instruction/counseling, walking/climbing stairs, strength training, and fall prevention. Half of the actions required one or two contacts. Pain treatment and actions related to exercise were the strongest indicators for several contacts, mainly in clients with no or only minor functional limitations. About half of the actions lasted <3 weeks, and about 30% lasted ≥7 weeks; supervision of home care staff and exercises were the strongest indicators for long duration. Technical aids, instructions/counseling, and fall prevention actions were associated with shorter physiotherapy duration. This new knowledge contributes to the continuing work to describe the content and extent of reablement, which is needed to be able to allocate adequate resources for achieving high-quality, equal, and person-centered care for older people living at home.
Abbreviations
CI, confidence interval; HCP, health care professional; LASRA, local authority senior rehabilitation advisor; OR, odds ratio; OT, occupational therapist; PT, physiotherapist; SD, standard deviation.
Data Sharing Statement
Data are available upon request from [email protected].
Ethics Approval and Informed Consent
The participants were LASRAs, OTs and PTs. At the beginning of the study, the LASRAs received information about the study, including the assurance that participation was voluntary, and were asked whether the municipality they represented would be willing to participate. Once they gave a positive response and their informed consent, the research team emailed information about the study to the OTs and PTs in the municipality. Each municipality decided the extent to which it would participate; that is, how many of its OTs and PTs would take part in the study. The study was approved by the Ethical Board at Umeå University (ref: 2015/268-31Ö).
Acknowledgments
The authors thank all the participants in this study for their valuable time. We would also like to thank Kake Pugh/Karin Fischer-Buder at Proper English AB for the language editing of our manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brändström A, Meyer AC, Modig K, Sandström G. Determinants of home care utilization among the Swedish old: nationwide register-based study. Eur J Ageing. 2021;19(3):651–662. doi:10.1007/s10433-021-00669-9
2. Metzelthin SF, Rostgaard T, Parsons M, Burton E. Development of an internationally accepted definition of reablement: a Delphi study. Ageing Soc. 2022;42(3):703–718. doi:10.1017/S0144686X20000999
3. Clotworthy A, Kusumastuti S, Westendorp RGJ. Reablement through time and space: a scoping review of how the concept of ‘reablement’ for older people has been defined and operationalised. BMC Geriatr. 2021;21(1):61. doi:10.1186/s12877-020-01958-1
4. Aspinal F, Glasby J, Rostgaard T, Tuntland H, Westendorp RG. New horizons: reablement - supporting older people towards Independence. Age Ageing. 2016;45(5):572–576. doi:10.1093/ageing/afw094
5. Cochrane A, Furlong M, McGilloway S, Molloy DW, Stevenson M, Donnelly M. Time-limited home-care reablement services for maintaining and improving the functional Independence of older adults. Cochrane Database Syst Rev. 2016;10:CD010825. doi:10.1002/14651858.CD010825.pub2
6. Mjøsund HL, Moe CF, Burton E, Uhrenfeldt L. Integration of physical activity in reablement for community dwelling older adults: a systematic scoping review. J Multidiscip Healthc. 2020;13:1291–1315. doi:10.2147/JMDH.S270247
7. Bergström A, Borell L, Meijer S, Guidetti S. Evaluation of an intervention addressing a reablement programme for older, community-dwelling persons in Sweden (ASSIST 1.0): a protocol for a feasibility study. BMJ Open. 2019;9(7):e025870. doi:10.1136/bmjopen-2018-025870
8. Sims-Gould J, Tong CE, Wallis-Mayer L, Ashe MC. Reablement, reactivation, rehabilitation and restorative interventions with older adults in receipt of home care: a systematic review. J Am Med Dir Assoc. 2017;18(8):653–663. doi:10.1016/j.jamda.2016.12.070
9. Tuntland H, Aaslund MK, Espehaug B, Forland O, Kjeken I. Reablement in community-dwelling older adults: a randomised controlled trial. BMC Geriatr. 2015;15(1):145. doi:10.1186/s12877-015-0142-9
10. Meisingset I, Bjerke J, Taraldsen K, et al. Patient characteristics and outcome in three different working models of home-based rehabilitation: a longitudinal observational study in primary health care in Norway. BMC Health Serv Res. 2021;21(1):887. doi:10.1186/s12913-021-06914-2
11. Zingmark M, Evertsson B, Haak M. Characteristics of occupational therapy and physiotherapy within the context of reablement in Swedish municipalities: a national survey. Health Soc Care Community. 2020;28(3):1010–1019. doi:10.1111/hsc.12934
12. Pettersson C, Zingmark M, Haak M. Enabling social participation for older people: the content of reablement by age, gender, and level of functioning in occupational therapists’ interventions. Scand J Occup Ther. 2022;29(6):522–529. doi:10.1080/11038128.2021.1967442
13. Parsons J, Mathieson S, Parsons M. Home care: an opportunity for physiotherapy. NZJP. 2015;43(1):23–30. doi:10.15619/NZJP/43.1.04
14. Canadian Physiotherapy Association. The value of physiotherapy. Home-based physiotherapy. Available from: https://physiotherapy.ca/app/uploads/2022/08/cpa_valuept_homebasedphysio-en.pdf.
15. Eliassen M, Henriksen NO, Moe S. Variations in physiotherapy practices across reablement settings. Physiother Theory Pract. 2018;36(1):108–121. doi:10.1080/09593985.2018.1481162
16. Buma LE, Vluggen S, Zwakhalen S, Kempen G, Metzelthin SF. Effects on clients’ daily functioning and common features of reablement interventions: a systematic literature review. Eur J Ageing. 2022;19(4):903–929. doi:10.1007/s10433-022-00693-3
17. Bateni H, Maki BE. Assistive devices for balance and mobility: benefits, demands, and adverse consequences. Arch Phys Med Rehabil. 2005;86(1):134–145. doi:10.1016/j.apmr.2004.04.023
18. Pantelaki E, Maggi E, Crotti D. Mobility impact and well-being in later life: a multidisciplinary systematic review. Res Transp Econ. 2021;86:100975. doi:10.1016/j.retrec.2020.100975
19. World Health Organization. Assistive technology. Available from: https://www.who.int/news-room/fact-sheets/detail/assistive-technology.
20. McPhee JS, French DP, Jackson D, Nazroo J, Pendleton N, Degens H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. 2016;17(3):567–580. doi:10.1007/s10522-016-9641-0
21. Eliassen M, Lahelle A. Enhancing functional improvement in reablement – a qualitative study. Eur J Physiother. 2021;23(6):355–361. doi:10.1080/21679169.2020.1761449
22. Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2019;31(1):CD012424.
23. Arkkukangas M, Sundler AJ, Söderlund A, Eriksson S, Johansson AC. Older persons’ experiences of a home-based exercise program with behavioral change support. Physiother Theory Pract. 2017;33(12):905–913. doi:10.1080/09593985.2017.1359869
24. Jorstad EC, Hauer K, Becker C, Lamb SE. Measuring the psychological outcomes of falling: a systematic review. J Am Geriatr Soc. 2005;53(3):501–510. doi:10.1111/j.1532-5415.2005.53172.x
25. Hopewell S, Adedire O, Copsey BJ, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. 2018;7(7):CD012221. doi:10.1002/14651858.CD012221.pub2
26. Montero-Odasso M, van der Velde N, Martin FC, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. 2022;51(9):afac205.
27. Mjøsund HL, Uhrenfeldt L, Burton E, Moe CF. Promotion of physical activity in older adults: facilitators and barriers experienced by healthcare personnel in the context of reablement. BMC Health Serv Res. 2022;22(1):956. doi:10.1186/s12913-022-08247-0
28. Hjelle KM, Skutle O, Alvsvåg H, Førland O. Reablement teams’ roles: a qualitative study of interdisciplinary teams’ experiences. J Multidiscip Healthc. 2018;11:305–316. doi:10.2147/JMDH.S160480
29. Eliassen M, Henriksen N, Moe S. The practice of support personnel, supervised by physiotherapists, in Norwegian reablement services. Physiother Res Int. 2019;24(1):e1754. doi:10.1002/pri.1754
30. Hjelle KM, Skutle O, Førland O, Alvsvåg H. The reablement team’s voice: a qualitative study of how an integrated multidisciplinary team experiences participation in reablement. J Multidiscip Healthc. 2016;9:575–585. doi:10.2147/JMDH.S115588
31. Levasseur M, Desrosiers J, Whiteneck G. Accomplishment level and satisfaction with social participation of older adults: association with quality of life and best correlates. Qual Life Res. 2010;19(5):665–675. doi:10.1007/s11136-010-9633-5
32. Douglas H, Georgiou A, Westbrook J. Social participation as an indicator of successful aging: an overview of concepts and their associations with health. Aust Health Rev. 2017;41(4):455–462. doi:10.1071/AH16038
33. Taylor J, Walsh S, Kwok W, et al. A scoping review of physical activity interventions for older adults. Int J Behav Nutr Phys Act. 2021;18(1):82. doi:10.1186/s12966-021-01140-9
34. Zingmark M, Bernspång B. Meeting the needs of elderly with bathing disability. Aust Occup Ther J. 2011;58(3):164–171. doi:10.1111/j.1440-1630.2010.00904.x
35. Tuntland H, Kjeken I, Langeland E, et al. Predictors of outcomes following reablement in community-dwelling older adults. Clin Interv Aging. 2016;12:55–63. doi:10.2147/CIA.S125762
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.