Back to Journals » International Journal of General Medicine » Volume 15
The “CONNECT” Protocol: Delivering Bad News by Phone or Video Call
Authors Sobczak K ![]()
Received 16 January 2022
Accepted for publication 15 March 2022
Published 31 March 2022 Volume 2022:15 Pages 3567—3572
DOI https://doi.org/10.2147/IJGM.S358723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Krzysztof Sobczak
Department of Sociology Medicine and Social Pathology, Medical University of Gdansk, Gdansk, Poland
Correspondence: Krzysztof Sobczak, Department of Sociology Medicine and Social Pathology, Medical University of Gdansk, Tuwima 15 Str., 80-210 Gdansk, Poland, Tel +48 58 349 15 51, Email [email protected]
Abstract: The COVID-19 pandemic has changed the principles of communication within the health-care setting. Communication skills as developed for use in the context of a direct and personal encounter have become insufficient. As a result, numerous health professionals came to believe they were not sufficiently prepared to deliver bad news in relation to medical care. The CONNECT protocol is a tool designed to help health-care professionals in the delivery of such messages. The name of the protocol is an acronym derived from C – context, O – organization, NN – near and niceties, E - emotions, C – counseling, T – taking care. The objective of the protocol is to improve the effectiveness of the delivery of bad news in relation to medical care by ensuring proper organization of the key elements of the encounter with the patient and/or their family.
Keywords: truth disclosure, physician–patient relations, communication, COVID-19, pandemic
Introduction
There are three basic types of bad news (BN) in medicine: the news on unfavorable diagnosis, the news on unfavorable prognosis, and the news on the patient’s death. Each type of these news contains a message which will negatively affect the lives of the recipients. Not only receiving, but also delivering bad news (DBN) is a difficult experience potentially associated with adverse behavioral and emotional consequences.1 Numerous notification tools have been developed over the years to minimize the tension on the part of the parties delivering and receiving BN in order to improve communication efficiency. The most widely known protocols include the SPIKES,2 the ABCDE3 and the BREAKS.4 Other tools to facilitate DBN can also be found in the literature such as the PACIENTE,5 PEWTER6 or EMPATHY protocols,7 the dialectic method,8 the “in person, in time” death notification procedure9 or the GRIEV_ING protocol.10
All these types of communication tools share a number of common points. Firstly, they encourage news providers to thoroughly prepare for the DBN process. Among other factors, this includes the adequate and sufficient time being reserved by the physician for the patient or his/her family. It is very important since haste is one of the major errors in the communication process. The second important aspect is that information should be provided promptly and as soon as possible. Personal encounter with bad news recipients is also an important premise that is being highlighted in all known strategies. It provides the basis for the fulfillment of the remaining conditions of proper communication. Exemptions to this premise were allowed in extraordinary situations.11 These included information of patient’s death being provided by telephone to their family living at a considerable distance.12 In-person meeting is an important condition for empathetic and compassionate relationship between the physician and the patient and/or their family. Observation of non-verbal behaviors, particularly facial expressions of the recipients, is an important axis of communication for the providers. It determines the dynamics of the meeting, and the appropriate communication strategy is adopted largely in response to non-verbal behaviors of the recipients. Certain solutions emphasize another important element of the notification process, namely the physicians working in pairs to support each other in the delivery of the news.13 This strategy is aimed at maximizing the safety of the recipients who can be provided with appropriate care in case of a sudden psychophysical reaction. It provides an important plane of mutual emotional and cognitive support between both providers.
In order to meet the challenges brought by the COVID-19 pandemic in the area of communicating bad news, we created a communication protocol. Its purpose is to facilitate passing of bad news via telephone or an audio-video link. The tool sets out to organise the key aspects of meetings in order to improve the efficiency of communication and reduce the likelihood of errors. The CONNECT protocol aims at improving remote communication with patients and their relatives. It could also be a potentially useful resource for developing communication competencies during medical studies.
COVID-19 Pandemic as a Source of Psychological Strain in Health-Care Workers
The COVID-19 pandemic has led to changes in numerous areas of life worldwide. According to data collected by the Center for Systems Science and Engineering at Johns Hopkins University, more than 326 million individuals contracted COVID-19 and more than 5.5 million patients died with the disease as of January 2022.14 Information on COVID-19 started being perceived as bad news as the disease may lead to death or serious complications.15 This type of bad news has become a psychological burden for physicians as well as patients. Physicians were forced to deliver mass-scale bad news when contacting patients and informing some of them of the potentially fatal diagnosis. Most of these physicians had not been prepared for this task.11
New hospitals and COVID departments were established at the peak of the disease wave. Due to the scale of demand, the medical staff at these institutions frequently consisted of physicians and nurses of different specialties. A vast number of health-care professionals involved in providing care to patients with COVID-19 had no previous clinical experience with infectious diseases. In addition, young physicians and nurses with no children were frequently delegated to COVID departments as a measure to minimize transmission at the peak of the pandemic. The COVID-19 pandemic has exposed the necessity for reorganization of medical care and procedures.16 The new working conditions have resulted not only in changes to the organization of the health-care system, but also in serious physical and mental burden to the providers. In a systematic review, Chirico et al described the depth of impact that the pandemic had on the mental health of health-care professionals. The pandemic resulted in increased frequency of anxiety disorders and depression, sleep disorders, burnout syndrome (BOS) and post-traumatic stress disorders (PTSD).17 In their study published in 2021, Rathnayake et al pinpointed the reasons for the physical and mental suffering of nurses taking care of patients with COVID-19. The leading distress factors included “(g)uilty feeling related to inefficiency of care, witnessing the suffering of patients, discomfort associated with wearing personal protective equipment (PPE), work-related issues (e.g., long hour shifts), negative impact to the family and rejection by others”.18
Anxiety related to the disease, the inefficacy of treatment, the risk of infection, and the need to communicate bad news was identified as the main causes of mental health disorders in the study by Galehdar et al.19 One can assume that these were the factors of key importance behind the symptoms of post-traumatic stress disorder (PTSD) being reported by medical staff.20 The level of anxiety and depressive disorders as caused by the COVID-19 pandemic among the health-care workers has become so clear that it requires urgent systemic solutions.21–23
Successive waves of COVID-19 infection have increased the spiraling dynamics of tension and negative experiences on the part of patients and their families. The fear of contracting the infection, the anxiety about the health of one’s family, as well as negative psychological conditions developing as the consequence of social isolation are associated with the increased rates of psychiatric disorders.24 The possibility of contracting COVID-19 has become realistic for many individuals, translating to psychological tension experienced while awaiting potential BN.25 The important mechanisms of social support responsible for physical and psychological well-being of patients were suspended by the requirements of social distancing and quarantine. Dying in solitude has become a rule, and so has the experience of facing the death of a close person without the ability to say goodbye in a face-to-face encounter.26 This new situation has triggered the need to develop solutions and support mechanisms involving novel forms for the delivery of bad news so as to normalize the processes of mourning.26,27
Transformed Communication Paradigm as the Consequence of the COVID-19 Pandemic
The DBN process is influenced by numerous knowledge and experience-related factors. Other contributors include the personal attitude and mental condition of the delivering party.28 The feeling of anxiety translates to the reluctance to communicate bad news as already described by A. Tesser and M.C. Conlee as the “MUM” effect.29 We know that improper delivery of BN reduces the acceptance level and increases the risk of depression and PTSD.30 In the case of information regarding an unfavorable diagnosis, the improperly delivered message has clinical consequences and negatively affects further treatment.31,32
One of the aftermaths of the COVID-19 pandemic consists in a large number of excess deaths. The pandemic resulted in the physicians being forced to deliver bad news more frequently than usual. This problem pertained mainly to the employees of hospitals where the largest numbers of deaths were documented.25 Psychological stress on the physicians might have been exacerbated by the lack of skills associated with remote delivery of bad news regarding medical care.33 As pointed out by Vitto et al, the “don’t do it over the phone!” approach was common before the pandemic.34 Remote communication skills had not been generally taught in medical schools.35
Meanwhile, remote contact was made necessary due to the pandemic situation. The key conditions for appropriate delivery of bad news as described in available protocols had to be modified.26 Available notification protocols were shown not to be fully functional in the new situation, their effectiveness being reduced by conditions including the necessity to deliver a larger number of BN (particularly at COVID departments), the requirement of extra time to establish remote connection, and functional limitations of the remote contact tools. Empathetic behaviors and expressions of concern being so important in DBN had been largely associated with observation of facial expressions and non-verbal behaviors.34,36 The importance of proxemic elements had also been stressed in our teaching. Communicating news over the telephone and/or in a teleconference setting requires slightly different skills.16,36 Therefore, a need arises to ensure the development of these skills by means of novel forms of training.18,34 Some authors point to the need of the existing notification protocols being modified32 or completely new protocols being developed.26 One of the proposals included adaptation of the SPIKES protocol as presented by Vitto et al.34 Also noteworthy are the available digital resources, such as VITALtalk,37 which may provide an important source of information to complement one’s communication competences with guidance on the remote delivery of bad news.11
CONNECT – A Protocol for Remote Communication of Bad News in Medical Care
Due to the growing need to deliver bad news via remote communication, I obtained the permission of the authors of the CONTACT protocol to adopt it to the challenges posed by the COVID-19 pandemic.38 Initially, the CONTACT protocol served as a tool for education, which was created to benefit students of medicine and health professionals. Its purpose was to optimise contact between practitioners and patients on the basis of previously completed research.
The CONNECT protocol was enriched with new functionality and is meant to optimise remote communication between the health practitioner, the patient and, where appropriate, the patient’s relatives. The purpose of the protocol is to organise the key aspects of remote communication: (a) preparation of the medical professional for the discussion with the patient, (b) organising physical resources, (c) focusing on key messages relating to delivery of bad news, (d) provision of support (Table 1).
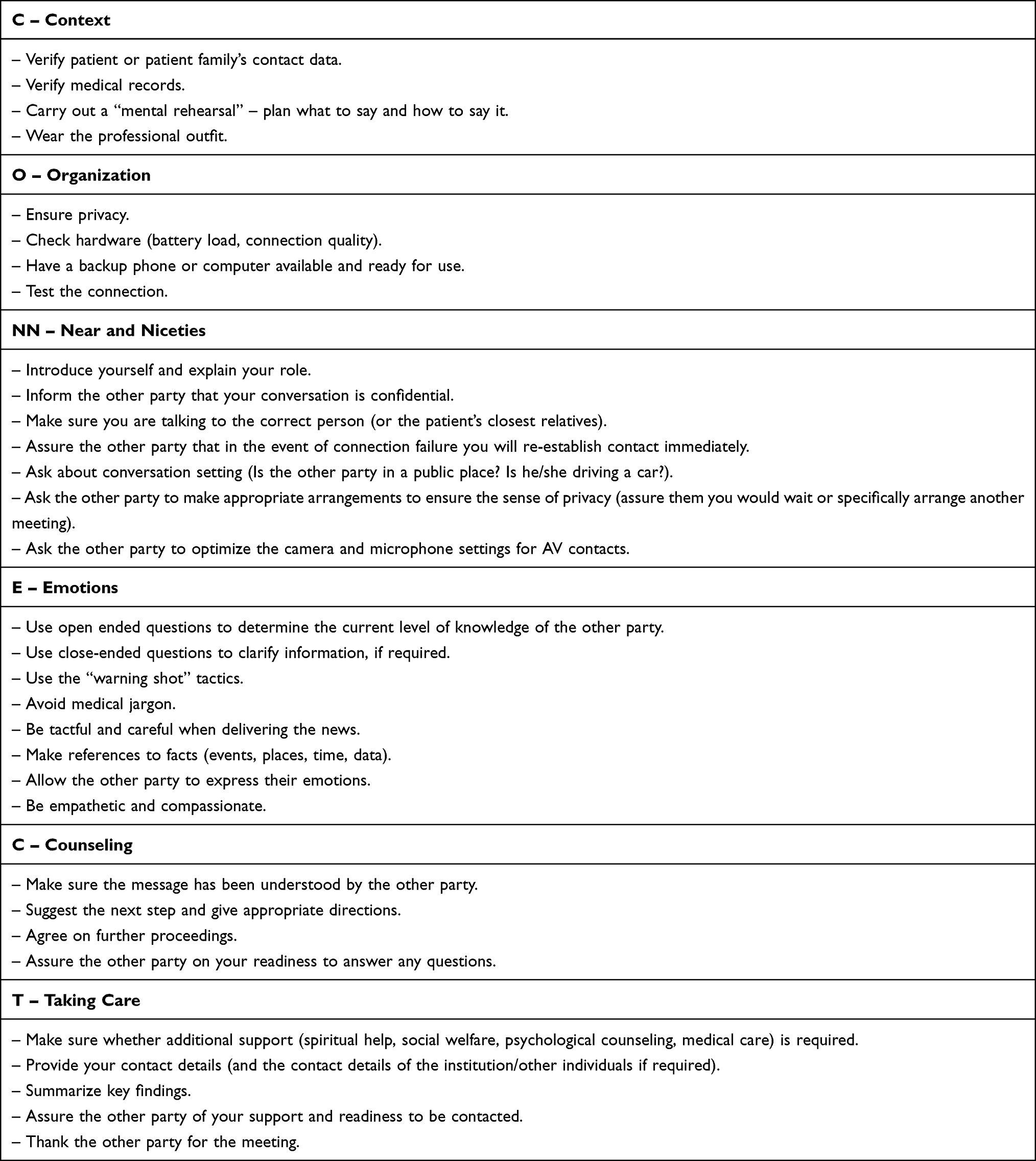 |
Table 1 The Model of the CONNECT Communication Procedure |
In relation to currently existing notification tools, the proposed protocol puts emphasis on key functionality that was not included in tools facilitating face-to-face communication. The CONNECT protocol accentuates the necessity to prepare the medical professional for the meeting not only in terms of mental preparation but also in relation to available technical resources. These are important factors. The extent to which remote communication can convey non-verbal context of a meeting is significantly limited. This could also be the reason why such mode of communication may prove to be more difficult for the medical professional, and the patient, to handle. Furthermore, remote communication makes it more complicated to read emotions and respond empathetically. Another key element is reliability of technology used to conduct the meeting, which could be interrupted by circumstances that are not controlled by any of the participants. To alleviate this, alternative mode of connection should be available so that, should an interruption occur, the meeting can be quickly resumed. In case of an audio-video link, the quality of the connection is also a concern as this will have impact on the quality of the experience for those involved. Since remote communication introduces certain barriers, which often affect how messages are transmitted and received by individuals, it is important to ensure that appropriate environment is provided, with the view of maximising the feeling of privacy and confidentiality. The attention of the speaker must be focused on the receiver and their reactions. Limitations that remote communication imposes on mimics, body language, tone of voice, as well as the absence of the proxemical factor, exert significant influence on the quality of communication. Hence, it is crucial to ensure that messages are understood correctly. A key aspect of the meeting is that a caring attitude and willingness to provide support are clearly conveyed. Difficulties, which originate from limitations to the eye-to-eye contact and lack of haptic perception, can pose a challenge. For reasons such as those, demonstrating compassion, willingness to support and maintain contact are an important component of the meeting.
It appears that systemising the key aspects of remote DBN may improve provider’s perception of their own efficiency and reduce the level of anxiety and stress. The protocol can also contribute to elimination of errors that could otherwise occur during the meeting. I believe that like other tools, the CONNECT protocol may also be useful in promoting awareness of the consequences of not delivering bad news in a professional way.39 It is worth pointing out that the efficiency of the CONNECT protocol requires analysis. The protocol constitutes a proposition, which requires its efficiency and functionality to be measured in relation to the needs of the doctors and the patients.
Conclusion
Undoubtedly, the COVID-19 pandemic has caused changes to the forms of communication in medical settings. More effective forms of support are required by patients and their families alike. Health-care professionals highlight the need for appropriate education and training of new skills related to remote communication. What remains unchanged is the need to build a caring, empathetic relationship with the recipient to provide recipient-focused solutions. The CONNECT protocol can be helpful in the teaching and the accomplishment of these goals. A standardized communication framework may contribute to improving the quality of remote contacts for health-care professionals as well as patients and their families. One should keep in mind that according to the protocol’s premises, its supportive role is that of a framework which is to be filled with personalized content tailored to the perception of the recipients as well as with adequate and empathetic responses to their difficult experience.
Funding
The author received no financial support.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Alelwani SM, Ahmed YA. Medical training for communication of bad news: a literature review. J Educ Health Promot. 2014;3:51. doi:10.4103/2277-9531.134737
2. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES - a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302–311. doi:10.1634/theoncologist.5-4-302
3. Rabow MW, McPhee SJ. Beyond breaking bad news: how to help patients who suffer. West J Med. 1999;171(4):260–263.
4. Narayanan V, Bista B, Koshy C. ‘BREAKS’ protocol for breaking bad news. Indian J Palliat Care. 2010;16(2):61–65. doi:10.4103/0973-1075.68401
5. Pereira CR, Calonego MA, Lemonica L, Barros GA. The P-A-C-I-E-N-T-E protocol: an instrument for breaking bad news adapted to the Brazilian medical reality. Rev Assoc Med Bras. 2017;63(1):43–49. doi:10.1590/1806-9282.63.01.43
6. Nardi TJ, Keefe-Cooperman K. Communicating bad news: a model for emergency mental health helpers. Int J Emerg Ment Health. 2006;8(3):203–207.
7. Witt MM, Jankowska KA. Breaking bad news in genetic counseling-problems and communication tools. J Appl Genet. 2018;59(4):449–452. doi:10.1007/s13353-018-0469-y
8. Sobczak K, Rudnik A. The dialectical method as a way of delivering bad news. Palliat Med Pract. 2020;12(4):19.
9. Moldovan E. The bad news bearers: the most difficult assignment in law enforcement. In: ProQuest Discovery Guides. Ann Arbor: ProQuest; 2009:1–23.
10. Hobgood C, Harward D, Newton K, Davis W. The educational intervention “GRIEV_ING” improves the death notification skills of residents. Acad Emerg Med. 2005;12(4):296–301. doi:10.1197/j.aem.2004.12.008
11. Soosaipillai G, Archer S, Ashrafian H, Darzi A. Breaking bad news training in the COVID-19 era and beyond. J Med Educ Curr Dev. 2020;7:2382120520938706. doi:10.1177/2382120520938706
12. Dyer KA. Death pronouncement and death notification: what the resident needs to know. Dealing with death and dying in medical education and practice. AMSA Convention; 2001. Available from: http://journeyofhearts.org/kirstimd/AMSA/pronounce.htm.
13. Sobczak K. The procedure for death notification -”In Person, in Time … ”. Anaesthesiol Intensive Ther. 2013;45(4):241–243. doi:10.5603/AIT.2013.0046
14. Johns Hopkins University, Coronavirus resource center. Baltimore: Johns Hopkins University. Available from: https://coronavirus.jhu.edu/map.html.
15. Adeniyi OV, Kayembe DK. Skills for communicating severe acute respiratory syndrome-coronavirus-2 result to patients and/or relatives. S Afr Fam Pract. 2021;63(1):e1–e5. doi:10.4102/safp.v63i1.5221
16. Tanzi S, Alquati S, Martucci G, De Panfilis L. Learning a palliative care approach during the COVID-19 pandemic: a case study in an infectious diseases unit. Palliat Med. 2020;34(9):1220–1227. doi:10.1177/0269216320947289
17. Chirico F, Ferrari G, Nucera G, Szarpak L, Crescenzo P, Ilesanmi O. Prevalence of anxiety, depression, burnout syndrome, and mental health disorders among healthcare workers during the COVID-19 pandemic: a rapid umbrella review of systematic reviews. J Health Soc Sci. 2021;6(2):209–220. doi:10.19204/2021/prvl7
18. Rathnayake S, Dasanayake D, Maithreepala SD, Ekanayake R, Basnayake PL. Nurses’ perspectives of taking care of patients with Coronavirus disease 2019: a phenomenological study. PLoS One. 2021;16(9):e0257064. doi:10.1371/journal.pone.0257064
19. Galehdar N, Kamran A, Toulabi T, Heydari H. Exploring nurses’ experiences of psychological distress during care of patients with COVID-19: a qualitative study. BMC Psychiatry. 2020;20(1):489. doi:10.1186/s12888-020-02898-1
20. Marco CA, Larkin GL, Feeser VR, Monti JE, Vearrier L, Committee AE. Post-traumatic stress and stress disorders during the COVID-19 pandemic: survey of emergency physicians. J Am Coll Emerg Physicians Open. 2020;1(6):1594–1601. doi:10.1002/emp2.12305
21. Thai T, Nguyen T, Pham P, Bui H, Bui T. Healthcare workers’ emotions, stressor experiences and coping strategies during the COVID-19 Pandemic in Vietnam. Risk Manag Healthc Policy. 2021;14:4281–4291. doi:10.2147/RMHP.S322929
22. Bahamdan A. Review of the psychological impact of COVID-19 pandemic on healthcare workers in Saudi Arabia. Risk Manag Healthc Policy. 2021;14:4105–4111. doi:10.2147/RMHP.S324938
23. Chirico F, Ferrari G. Role of the workplace in implementing mental health interventions for high-risk groups among the working age population after the COVID-19 pandemic. J Health Soc Sci. 2021;6(2):145–150. doi:10.19204/2021/rlft1
24. Barzilay R, Moore TM, Greenberg DM, et al. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl Psychiatry. 2020;10(1):291. doi:10.1038/s41398-020-00982-4
25. Landa-Ramírez E, Domínguez-Vieyra NA, Hernández-Nuñez ME, Díaz-Vásquez LP, Santana-García IA. Psychological support during COVID-19 death notifications: clinical experiences from a hospital in Mexico. Psychol Trauma. 2020;12(5):518–520. doi:10.1037/tra0000679
26. Campbell I. Paramedic delivery of bad news: a novel dilemma during the COVID-19 crisis. J Med Ethics. 2021;47(1):16–19. doi:10.1136/medethics-2020-106710
27. Borghi L, Menichetti J. Strategies to cope with the COVID-related deaths among family members. Front Psychiatry. 2021;12:622850. doi:10.3389/fpsyt.2021.622850
28. Cialkowska-Rysz A, Dzierzanowski T. Personal fear of death affects the proper process of breaking bad news. Arch Med Sci. 2013;9(1):127–131. doi:10.5114/aoms.2013.33353
29. Tesser A, Conlee M. Recipient emotionality as a determinant of the transmission of bad news. Proc ACAP. 1973;1973:247–248.
30. Johnson J, Panagioti M. Interventions to improve the breaking of bad or difficult news by physicians, medical students, and interns/residents: a systematic review and meta-analysis. Acad Med. 2018;93(9):1400–1412. doi:10.1097/ACM.0000000000002308
31. Sobczak K, Leoniuk K, Janaszczyk A. Delivering bad news: patient’s perspective and opinions. Patient Prefer Adherence. 2018;12:2397–2404. doi:10.2147/PPA.S183106
32. Sobczak K, Leoniuk K. Doctors’ attitudes in the situation of delivering bad news: patients’ experience and expectations. Arch Med Sci. 2021. doi:10.5114/aoms/112756
33. Rivet EB, Edwards C, Lange P, Haynes S, Feldman M, Cholyway R. Telehealth training for surgeons to empathetically deliver bad news via video-mediated communication. Am Surg. 2021;31348211030458. doi:10.1177/00031348211030458
34. Vitto C, Del Buono B, Daniel L, Rivet E, Cholyway R, Santen SA. Teaching toolbox: breaking bad news with virtual technology in the time of COVID. J Cancer Educ. 2021. doi:10.1007/s13187-021-01975-7
35. Rivet EB, Cholyway R, Edwards C, et al. Video-mediated breaking bad news simulation. Clin Teach. 2021;18(4):424–430. doi:10.1111/tct.13387
36. Collini A, Parker H, Oliver A. Training for difficult conversations and breaking bad news over the phone in the emergency department. Emerg Med J. 2021;38(2):151–154. doi:10.1136/emermed-2020-210141
37. Ehrman S, Gustin J, Lockwood B, Scott E. Communicating about Death and Dying on the Phone. Columbus, OH: The Ohio State University; 2020. Available from: https://www.vitaltalk.org/wp-content/uploads/Communication-Communicating-about-Death-on-the-Phone-FINAL-041320-1.pdf. Accessed December 20, 2021.
38. Sobczak KJ, Leoniuk K. CONTACT – communication protocol for family practitioners and specialists. J Med Sci. 2017;86(4):300–307. doi:10.20883/jms.2017.251
39. De Leo D, Zammarrelli J, Viecelli Giannotti A, et al. Notification of unexpected, violent and traumatic death: a systematic review. Front Psychol. 2020;11:2229. doi:10.3389/fpsyg.2020.02229
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.