Back to Journals » Journal of Inflammation Research » Volume 18
The Combined Prognostic Value of the Systemic Immune-Inflammation Index and LDL-C in Patients with AMI Undergoing PPCI
Authors Zhang X, Liu A, Li C, Pan Y, Jiao S, Wang Y, Pu H, Liu Y, Zhu H, Pan D
Received 17 May 2025
Accepted for publication 11 November 2025
Published 27 November 2025 Volume 2025:18 Pages 16579—16596
DOI https://doi.org/10.2147/JIR.S541090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Xiuli Zhang,1,* Ailin Liu,1,* Chenyang Li,1 Yanqing Pan,1 Songsong Jiao,2 Yumin Wang,1 Huijuan Pu,1 Yan Liu,1 Hong Zhu,1 Defeng Pan1
1Department of Cardiology, Xuzhou Medical University Affiliated Hospital, Xuzhou, Jiangsu, People’s Republic of China; 2Berlin Institute of Health Center for Regenerative Therapies (BCRT), Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Berlin, Germany
*These authors contributed equally to this work
Correspondence: Defeng Pan, Department of Cardiology, Xuzhou Medical University Affiliated Hospital, Xuzhou, Jiangsu, 221000, People’s Republic of China, Tel +8617660752236, Email [email protected] Hong Zhu, Department of Cardiology, Xuzhou Medical University Affiliated Hospital, Xuzhou, Jiangsu, 221000, People’s Republic of China, Tel +8613092323326, Email [email protected]
Background: The combined prognostic impact of the systemic immune-inflammation index (SII) and low-density lipoprotein cholesterol (LDL-C) after primary percutaneous coronary intervention (PPCI) in acute myocardial infarction (AMI) remains unclear. We evaluated their joint predictive value for clinical outcomes.
Methods: We retrospectively analyzed 487 AMI patients who underwent PPCI at the Affiliated Hospital of Xuzhou Medical University between January 2019 and December 2021. SII and LDL-C were assessed at baseline and 1 month post-discharge. Using the guideline LDL-C target (< 1.4 mmol/L or ≥ 50% reduction) and a receiver operating characteristic (ROC)–derived optimal SII cutoff (676.6 × 109 /L), patients were categorized as: both on-target, SII on-target only, LDL-C on-target only, or both off-target. The primary endpoint was the composite of major adverse cardiovascular events (MACEs): all-cause death, recurrent myocardial infarction, repeat revascularization, and ventricular arrhythmias. Candidate variables were selected with least absolute shrinkage and selection operator (LASSO); survival was analyzed using Cox proportional hazards models and Kaplan–Meier estimates.
Results: Versus the both off-target group, the both on-target group had significantly better outcomes (P < 0.001). The SII on-target only group also outperformed the LDL-C on-target only group (P < 0.001). Consistently, the both off-target group had markedly worse outcomes relative to the both on-target group (HR = 69.2; 95% CI: 16.8– 285.0; P < 0.001). At 1 month, SII showed good discrimination for MACEs (AUC = 0.76).
Conclusion: One month after PPCI, simultaneous achievement of SII and LDL-C targets was associated with a substantially lower 1-year risk of MACEs. Combined control of inflammation and lipids provided incremental benefit beyond lipid lowering alone, supporting a dual-target strategy in secondary prevention.
Keywords: systemic immune-inflammation index, low-density lipoprotein cholesterol, dual-target management, acute myocardial infarction, prognosis
Introduction
Cardiovascular disease (CVD) remains the leading cause of death worldwide, accounting for approximately 17.9 million deaths each year. Acute myocardial infarction (AMI), a principal presentation of coronary artery disease, continues to impose a substantial public health burden owing to its high incidence, high mortality, and risk of recurrence.1 Despite significant advances in therapy—particularly the widespread use of primary percutaneous coronary intervention (PPCI) and drug-eluting stents—adverse events after PPCI remain frequent even under intensive lipid-lowering treatment,2,3 underscoring limitations of current risk-management strategies and the urgent need for novel prognostic biomarkers to refine risk stratification and guide more effective secondary prevention.
Dyslipidemia—particularly elevated low-density lipoprotein cholesterol (LDL-C)—is a principal driver of atherogenesis and plaque instability.4 Although lipid-lowering therapies such as statins substantially reduce cardiovascular risk, many patients continue to experience residual risk after PPCI even when lipid targets are achieved,5 indicating that non-lipid factors—especially inflammation—play a pivotal role in prognosis.6 Systemic inflammation not only accelerates atherosclerotic progression but also precipitates plaque rupture and adverse myocardial remodeling, thereby increasing the risk of recurrent ischemic events.7,8 Accordingly, effective cardiovascular prevention requires integrated lipid management alongside comprehensive control of inflammation.
The systemic immune–inflammation index (SII), calculated as (platelet count × neutrophil count) / lymphocyte count, is a novel composite index that integrates innate immunity, adaptive immune suppression, and a prothrombotic state.9 Prior studies have shown that elevated admission SII independently predicts short- and long-term adverse outcomes in AMI patients undergoing PPCI,10–12 and it outperforms conventional inflammatory markers such as the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR).13–15 However, the literature has largely treated SII as a one-time baseline measure;16 potential interactions with established risk factors (eg, LDL-C) remain underexplored, and the prognostic relevance of longitudinal changes in SII has not been systematically evaluated.
Mechanistically, inflammation and lipid metabolism are tightly coupled: activation of inflammatory pathways promotes LDL oxidation and macrophage uptake, accelerating foam-cell formation;17 conversely, dyslipidemia triggers endothelial activation and the release of inflammatory mediators, perpetuating a vicious cycle.18,19 This bidirectional process suggests that an elevated SII together with suboptimal LDL-C control may act synergistically to increase plaque vulnerability and impede myocardial recovery. Because immune–inflammatory responses evolve dynamically after PPCI,20 we hypothesize that serial monitoring of SII could more precisely identify patients at high risk. Although existing data indicate that concurrent targeting of inflammation and lipids yields additional clinical benefit,21,22 the prognostic value of a joint SII–LDL-C framework after PPCI in AMI has not yet been systematically evaluated.
Building on these gaps, we evaluate whether a combined assessment of the SII and achievement of LDL-C targets improves prediction of 1-year major adverse cardiovascular events (MACEs) following PPCI. We hypothesize that, in AMI patients undergoing PPCI, concomitant elevation of SII with reduction of LDL-C at admission is associated with a higher risk of post-PPCI MACE and serves as an independent predictor of risk.
Methods
Participants and Study Design
From January 1 to December 31, 2019, the Department of Cardiology at the Affiliated Hospital of Xuzhou Medical University admitted 1,092 patients with AMI, including 713 with ST-segment elevation myocardial infarction (STEMI) and 379 with non-ST-segment elevation myocardial infarction (NSTEMI).A final cohort of 487 patients (STEMI, n=324; NSTEMI, n=163) met the inclusion criteria (Figure 1).MACEs were defined as the composite endpoint of all-cause death, recurrent myocardial infarction, repeat revascularization (percutaneous coronary intervention or coronary artery bypass grafting), and ventricular arrhythmias.Follow-up was conducted at 3-month intervals via telephone follow-up, outpatient reassessments, and review of the electronic medical record system; outcomes were adjudicated by clinical staff by integrating these sources with information from family members, and the total follow-up duration was 12 months.The study was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (approval no. XYFY2022-KL420-01).Owing to the retrospective design, the requirement for informed consent was waived by the ethics committee.All patient data were de-identified and handled confidentially to safeguard patient rights.The study was conducted in accordance with the Declaration of Helsinki.
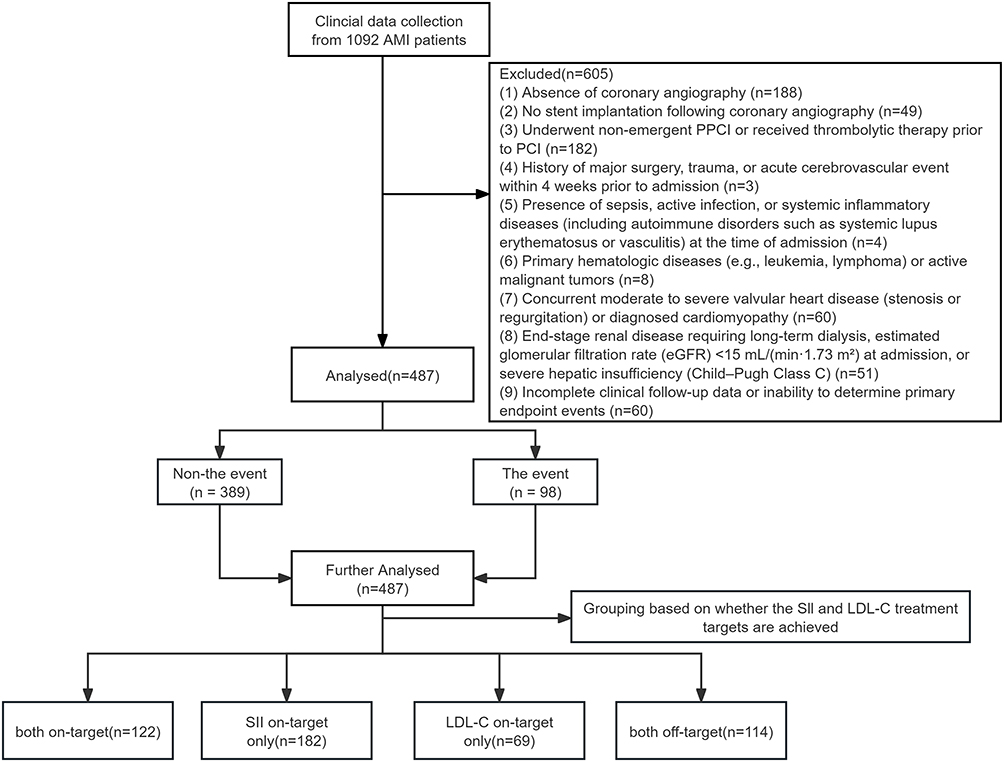 |
Figure 1 Flowchart illustrating the process of patient recruitment. Abbreviations: AMI, acute myocardial infarction; PPCI, primary percutaneous coronary intervention; PCI, percutaneous coronary intervention; eGFR, estimated glomerular filtration rate; SII, systemic immune-inflammation index; LDL-C, low-density lipoprotein cholesterol. |
Inclusion and Exclusion Criteria Inclusion Criteria
Inclusion criteria were as follows: (1) a clinical diagnosis of AMI according to the Fourth Universal Definition of Myocardial Infarction,23 requiring both (a) evidence of myocardial injury—defined as a rise and/or fall in high-sensitivity cardiac troponin (hs-cTn) with at least one value above the 99th-percentile upper reference limit (URL)—and (b) evidence of acute myocardial ischemia, indicated by at least one of the following: typical ischemic symptoms, new or presumed-new ischemic changes on electrocardiogram, imaging evidence of new loss of myocardial viability or new regional wall-motion abnormality, or angiographic demonstration of an intracoronary thrombus; (2) receipt of guideline-directed revascularization therapy: for STEMI, fulfillment of the 2017 Chinese guideline for STEMI and PPCI within 12 hours of symptom onset;24 for NSTEMI, fulfillment of the 2016 Chinese guideline for NSTEMI, a GRACE risk score >140, and an early invasive strategy within 24 hours of hospital admission;25 (3) age ≥18 years; and (4) availability of complete baseline clinical characteristics, laboratory results, and follow-up information.
Exclusion Criteria were as follows: (1) Absence of coronary angiography; (2) No stent implantation following coronary angiography; (3) Underwent non-emergent primary percutaneous coronary intervention (PCI) or received thrombolytic therapy prior to PCI; (4) History of major surgery, trauma, or acute cerebrovascular event within 4 weeks prior to admission; (5) Presence of sepsis, active infection, or systemic inflammatory diseases (including autoimmune disorders such as systemic lupus erythematosus or vasculitis) at the time of admission; (6) Primary hematologic diseases (eg, leukemia, lymphoma) or active malignant tumors; (7) Concurrent moderate to severe valvular heart disease (stenosis or regurgitation) or diagnosed cardiomyopathy; (8) End-stage renal disease requiring long-term dialysis, estimated glomerular filtration rate (eGFR) <15 mL/(min·1.73 m2) at admission, or severe hepatic insufficiency (Child–Pugh Class C); (9) Incomplete clinical follow-up data or inability to determine primary endpoint events.
Data Collection
Two investigators independently evaluated all patients with AMI according to prespecified inclusion and exclusion criteria. At admission, demographic, clinical, and laboratory data were collected. Patient information was abstracted from electronic and paper medical records and documented on a standardized case report form (CRF).
Baseline information included: (1) Baseline characteristics—sex, age, medical history (including hypertension, diabetes, and other comorbidities), smoking and alcohol use, systolic and diastolic blood pressure on admission, heart rate on admission, Killip class, and hospitalization day; (2) In-hospital medications—aspirin, P2Y12 receptor inhibitors, calcium channel blockers (CCBs), statins, beta-blockers, angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs), and diuretics; (3) Intraprocedural variables during PPCI—primary diseased coronary vessel, stent length, stent diameter, number of stents implanted, and whether intravascular ultrasound (IVUS) guidance was used; and (4) Discharge medications—aspirin, P2Y12 receptor inhibitors, diuretics, statins, beta-blockers, ACEIs or ARBs, and insulin.
Laboratory measurements included: (1) complete blood count—neutrophils, lymphocytes, and platelets; (2) lipid profile—low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), total cholesterol (TC), triglycerides (TG), and lipoprotein(a) [Lp(a)]; (3) biochemistry and cardiac biomarkers—hemoglobin (Hb), glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), estimated glomerular filtration rate (eGFR), serum creatinine (Scr), uric acid (UA), alanine aminotransferase (ALT), serum albumin (ALB), high-sensitivity cardiac troponin T (hs-TnT), N-terminal pro–B-type natriuretic peptide (NT-proBNP), creatine kinase-MB (CK-MB), and cardiac troponin I (cTnI); and (4) inflammatory index—the systemic immune-inflammation index (SII), calculated as platelet count × neutrophil count / lymphocyte count (SII = P × N / L). Blood samples were processed in the hospital central laboratory using an automated hematology analyzer (Sysmex XT-1800, Sysmex Inc., Kobe, Japan) and a clinical chemistry analyzer (Hitachi 747, Hitachi Ltd., Tokyo, Japan).
Lipid testing: To accommodate the time-critical nature of emergent PPCI, admission lipid measurements were obtained in the non-fasting state, consistent with ESC (2019) and AHA/ACC (2018) guidance.26,27 For the primary analyses, LDL-C measured 1 month after discharge under ≥8-hour fasting was used as the standardized, stable exposure variable.
Five prespecified SII time points were assessed: (1) 24h pre-procedure (baseline reflecting initial inflammatory and lipid status); (2) 24h post-procedure and (3) 48h post-procedure (capturing the acute inflammatory peak and early dynamics related to ischemia–reperfusion injury); (4) pre-discharge (assessing the cumulative in-hospital effect of inflammation control); and (5) 1 month post-discharge (chronic inflammatory burden after resolution of the acute phase, aligned with ESC/EAS27 recommendations for repeat LDL-C assessment).Because post-AMI inflammation evolves over days to weeks, serial SII measurements were collected to capture trajectory (resolution vs persistence).
Definitions and Endpoints
- Hypertension: systolic blood pressure (SBP) > 140 mmHg and/or diastolic blood pressure (DBP) > 90 mmHg, a documented history of hypertension, or current use of antihypertensive medication.28
- Diabetes: fasting plasma glucose (FPG) > 7.0 mmol/L, random plasma glucose > 11.1 mmol/L, glycated hemoglobin (HbA1c) ≥ 6.5%, or current use of glucose-lowering therapy.28
- Smoking status: current smoking or cessation within the previous 12 months.28
- Alcohol use: current drinking or cessation within the previous 12 months.28
- Major adverse cardiovascular events (MACEs): a composite endpoint including all-cause mortality, recurrent myocardial infarction, repeat revascularization (percutaneous coronary intervention or coronary artery bypass grafting), and ventricular arrhythmias. Events were adjudicated according to prespecified criteria using source clinical documentation (eg, coronary angiography reports, electrocardiograms, and laboratory results).29 Although adjudicators were not fully blinded to biomarker data, all determinations required objective evidence to reduce the risk of bias.
- LDL-C treatment target: prespecified per the 2019 ESC/EAS dyslipidaemia guideline27—defined as < 1.4 mmol/L at 1 month post-discharge or a ≥ 50% reduction from baseline—for very-high-risk patients, including those with acute myocardial infarction.
- SII cutoff derivation: no guideline-endorsed threshold; SII measured at five prespecified time points; receiver-operating characteristic (ROC) analyses for 1-year outcomes compared discrimination; the Youden index identified the optimal cutoff. The 1-month post-discharge SII showed the highest predictive performance (AUC = 0.76; 95% CI 0.71–0.82; P < 0.001), yielding a threshold of 676.6 × 109 /L; subsequent analyses dichotomized SII at this value.
Intervention Procedure
All patients included in the study received chewable aspirin (300 mg), ticagrelor (180 mg), and intravenous unfractionated heparin at a dose of 70–100 U/kg prior to undergoing PPCI. The procedure was performed by an experienced interventional cardiologist using a standard radial artery approach with either a 6-French or 7-French catheter.The selection of stent type—either bare-metal or drug-eluting—and the decision to perform thrombus aspiration were made at the operator’s discretion. A glycoprotein IIb/IIIa receptor inhibitor, chosen by the operator, was administered via the intracoronary route at a bolus dose of 10 µg/kg, followed by continuous intravenous infusion at 0.15 µg/kg/min. Coronary lesions were treated using standard PPCI techniques.Selective coronary angiography was conducted using the standard Judkins technique (Expo; Boston Scientific, Natick, MA, USA) with the Siemens Axiom Sensis XP system (Siemens Healthcare, Munich, Germany). In accordance with the European Society of Cardiology (ESC) guidelines, recommended pharmacological therapies were administered during hospitalisation and continued post-discharge.
Statistical Analysis
The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data were presented as mean ± standard deviation (SD), non-normal data as median (interquartile range, IQR), and categorical variables as counts (percentages). Between-group comparisons were performed using Student’s t-test or the Mann–Whitney U-test for continuous variables and the chi-square (χ2) test or Fisher’s exact test for categorical variables.Two-sided P < 0.05 was considered statistically significant.Variable selection followed a two-stage approach: first, least absolute shrinkage and selection operator (LASSO) regression was used for preliminary screening of predictors; second, retained variables together with prespecified clinically relevant covariates were entered into multivariable Cox proportional hazards models to identify independent factors associated with 1-year outcomes among AMI patients treated with PPCI. Adjusted covariates included demographics (age, sex), lifestyle factors (smoking, alcohol use), medical history (hypertension, stroke/transient ischemic attack [TIA]), and prior medications (glucose-lowering and lipid-lowering therapies).The predictive performance of the SII for adverse events was evaluated using receiver operating characteristic (ROC) analysis, and the optimal cutoff was determined by the Youden index; SII was then dichotomized accordingly. Patients were further stratified by attainment of SII and LDL-C targets. One-year survival was depicted using Kaplan–Meier curves, group differences were compared with the Log rank test, and an SII×LDL-C interaction term was tested within Cox models. The proportional hazards assumption was assessed using Schoenfeld residuals (assumed satisfied if P > 0.05). Internal validation and sensitivity analyses were conducted via bootstrap resampling (B = 300). In primary endpoint analyses, participants lost to follow-up were right-censored; secondary endpoints were analyzed using a complete-case dataset. The missing rate for baseline and clinical variables was <0.5% and was reconciled using the hospital information system. Analyses were performed with SPSS 26.0, R 4.5.0, and GraphPad Prism 10.3.
Results
Baseline Characteristics
A total of 487 patients with AMI treated with PPCI were enrolled. Primary endpoint events (MACEs) occurred in 98 patients (20.1%; event group), whereas 389 patients (79.9%) had no events (non-event group). As shown in Table 1, the two groups did not differ significantly in baseline demographic characteristics such as age and sex (P > 0.05). By contrast, the event group had larger stent diameter and length and higher use of CCBs and β-blockers (all P < 0.05). On laboratory testing, the event group exhibited significantly higher levels of the SII, LDL-C, HDL-C, and cardiac injury biomarkers (hs-TnT, NT-proBNP, cTnI, CK-MB) than the non-event group (all P < 0.05; Table 2). Overall, baseline medical therapy was highly consistent across groups: dual antiplatelet therapy, statins, and β-blockers were used in nearly all patients, and >80% received an ACE inhibitor or an angiotensin receptor blocker (ACEI/ARB), in line with current guideline recommendations.
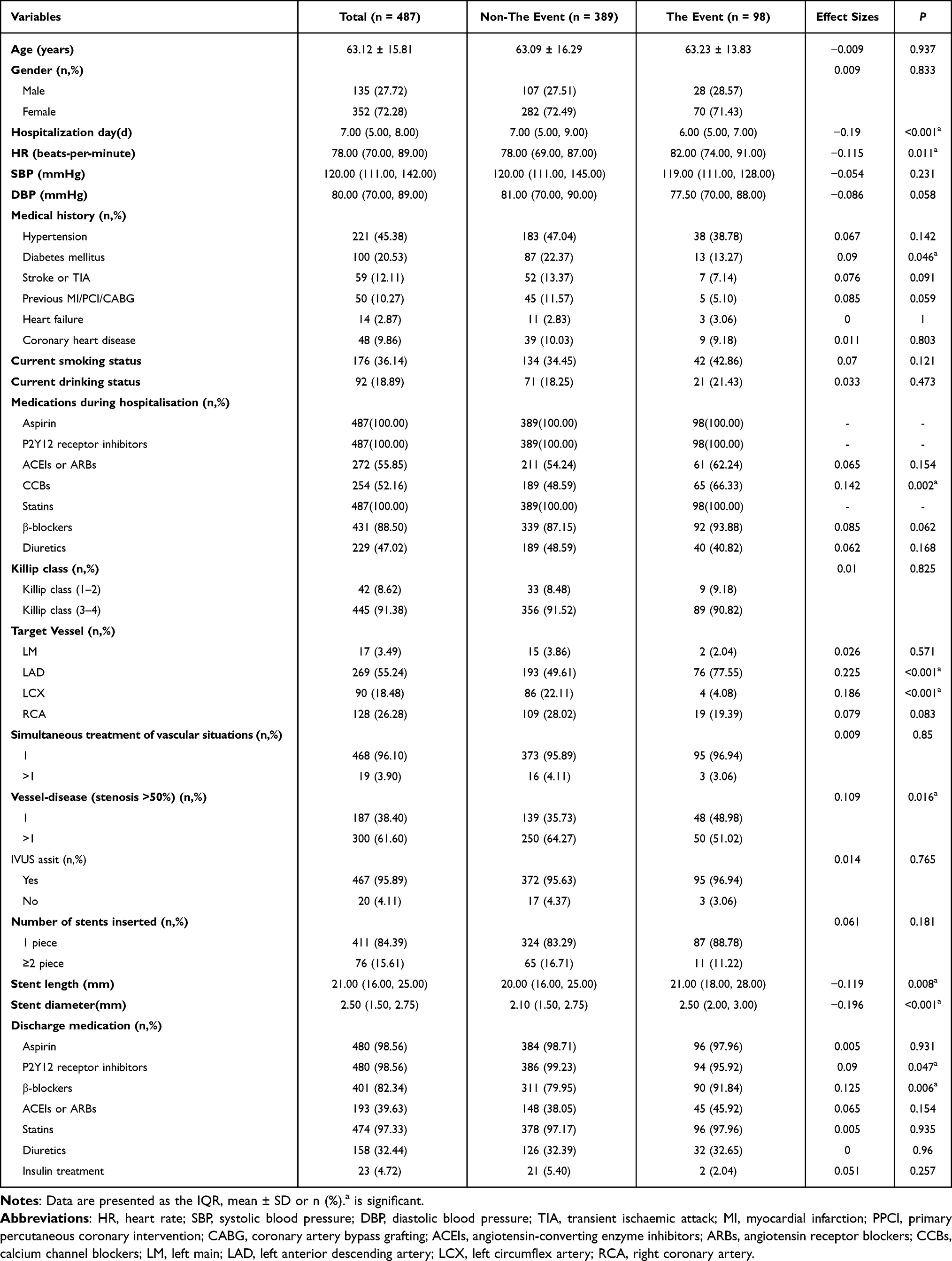 |
Table 1 Comparison of Clinical Characteristics Between the Event and Non-Event Groups |
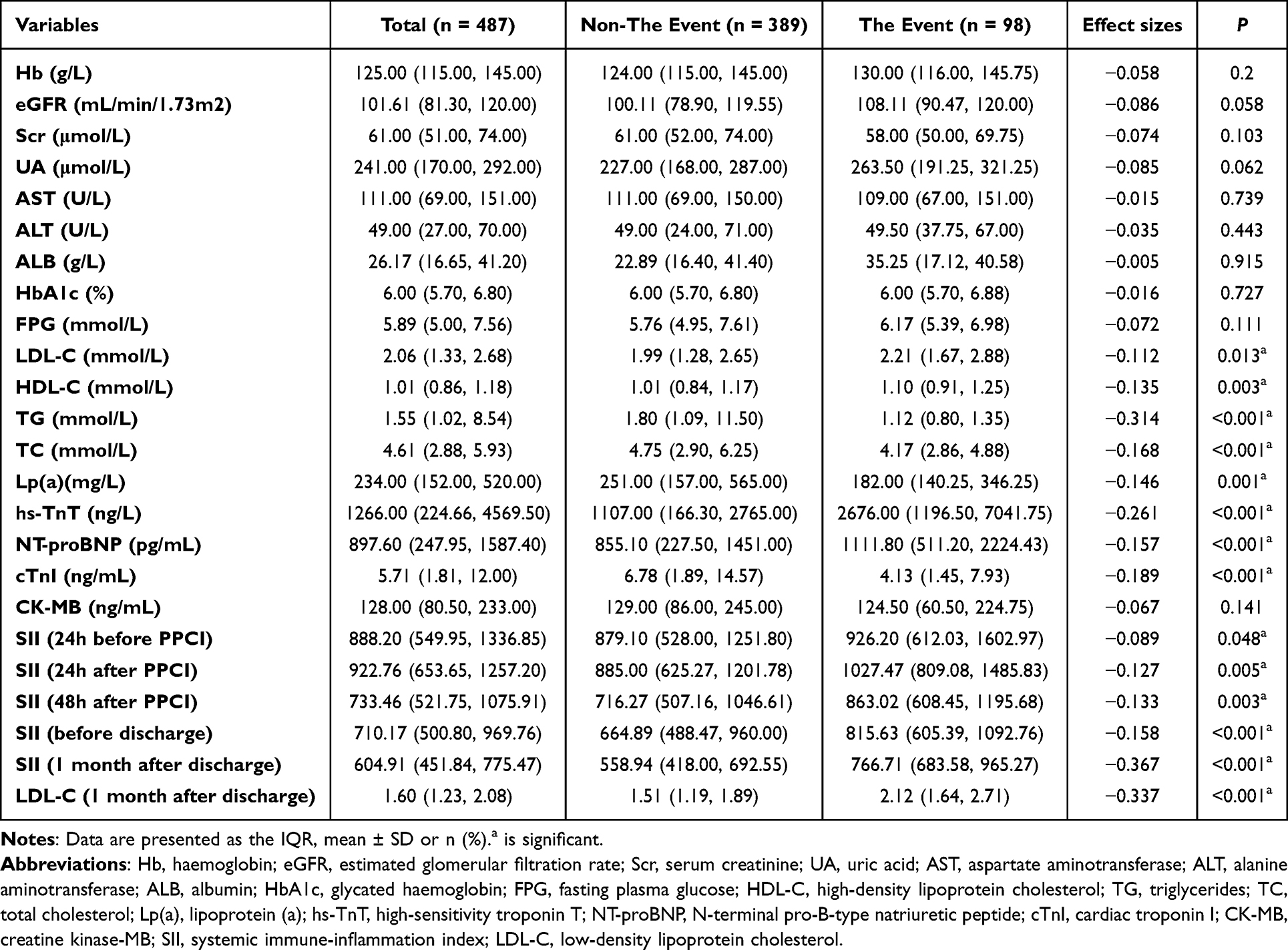 |
Table 2 Comparison of Biochemical Characteristics Between the Event and Non- the Event Groups |
Identification of Distinct Predictors for Early and Late Risk
We first used univariable Cox regression to screen 25 variables significantly associated with the primary endpoint (P < 0.05; Supplementary Table S1). To reduce dimensionality and address multicollinearity while accommodating potential time-varying predictor effects, we applied a time-segmented LASSO Cox regression, partitioning follow-up at the median event time (7 months) into an early window (t ≤ 7 months) and a late window (t > 7 months), with variable selection by 10-fold cross-validation.No significant predictors were identified in the early window (t ≤ 7 months) (Supplementary Figure S1).In the late window (t > 7 months), LASSO pre-screening indicated eight variables with predictive value (Supplementary Table S2), and applying the 1-SE rule yielded five core predictors (Figure 2): TG, hs-TnT, NT-proBNP, SII (1 month after discharge), and LDL-C (1 month after discharge).For model robustness and clinical interpretability, these five variables were carried forward into the subsequent multivariable Cox regression.
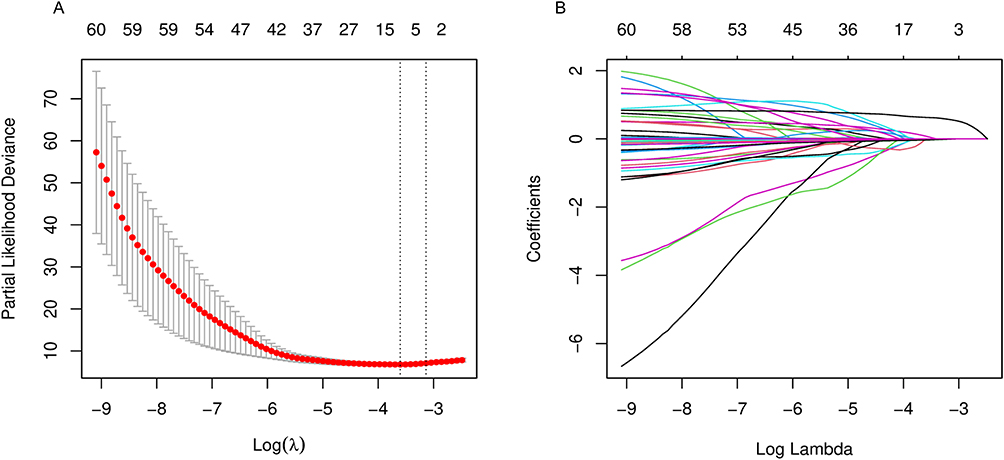 |
Figure 2 Variable selection using time-segmented LASSO-Cox regression in the late window (t > 7 months). Abbreviations: λ, penalty parameter; SE, standard error. Notes: (A) Ten-fold cross-validated partial-likelihood deviance versus log(λ). Red dots indicate the mean deviance; gray bars, ±1 SE. Vertical dotted lines mark λ_min and λ_1-SE. Numbers above the curve indicate the number of non-zero coefficients at each λ. (B) Coefficient paths for candidate predictors as a function of log(λ); coefficients shrink toward zero as the penalty increases. |
Assessment of the Proportional Hazards Assumption and Landmark Analysis
Given the potential for time-varying effects among LASSO-selected covariates, we tested the Cox proportional hazards (PH) assumption using the Schoenfeld residuals test. The global test indicated a violation of the PH assumption (χ2=12.86, P=0.025), driven primarily by 1-month post-discharge LDL-C (χ2=8.95, P=0.003), whereas other covariates showed no significant departures (all P>0.05; Supplementary Figure S2). To mitigate early-event heterogeneity and immortal-time bias, we implemented a 1-month post-discharge landmark, restricted the cohort to patients alive and event-free at that time, and restarted follow-up from the landmark. Findings were consistent in the landmark cohort: the PH assumption was again violated (χ2=12.86, df=5, P=0.025), predominantly due to LDL-C (χ2=8.95, P=0.003), while the remaining covariates met the PH requirement (Figure 3). Accordingly, the final model specified an interaction between 1-month LDL-C and log(time) to capture the increasing hazard associated with LDL-C over time and to avoid bias from assuming a constant hazard ratio.
 |
Figure 3 Proportional-hazards diagnostics using scaled Schoenfeld residuals (Landmark cohort at 1 month after discharge). Abbreviations: PH, proportional hazards; TG, triglycerides; hs-TnT, high-sensitivity troponin-T; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SII, systemic immune-inflammation index; LDL-C, low-density lipoprotein cholesterol. Notes: For each LASSO-selected covariate, scaled Schoenfeld residuals are plotted against transformed time (points) with a LOESS smoother (solid line) and 95% CI (shaded band); the horizontal dashed line denotes the zero slope expected under the PH assumption. The global PH test is shown in the header. |
Multivariable Cox Modelling and Validation of Time-Dependent Effects
As prior testing indicated that LDL-C violated the PH assumption, we employed a multivariable Cox model incorporating a time-dependent term for subsequent analyses.We introduced an interaction term, 1-month post-discharge LDL-C ×log(time), into the baseline model to capture its time-amplifying risk.To assess independent effects and control confounding, we applied sequential adjustments: Model 1 (baseline), Model 2 (Model 1 plus age and sex), and Model 3 (additionally including smoking status, drinking status, history of hypertension, history of stroke or TIA, and the use of antidiabetic and antilipidemic medications).In the fully adjusted model, the LDL-C × time interaction was significant (aHR = 1.443, 95% CI 1.301–1.600; P < 0.001; Table 3); accordingly, the HR per +1 mmol/L increase in LDL-C was 1.496, 1.928, and 2.485 at 3, 6, and 12 months, respectively, and for an IQR increase of 0.855 mmol/L, the HRs were 1.411, 1.753, and 2.178 (Table 4).Beyond LDL-C, SII remained an independent risk factor (per +1 unit: HR = 1.001, 95% CI 1.000–1.001; P < 0.001; scaled to +100 × 10^9/L, HR ≈ 1.105; other covariates in Table 3).In terms of discrimination, the C-index increased from 0.830 (SE 0.017) without the time term to 0.835 (SE 0.016) after including the interaction, and further reached 0.837 (SE 0.016) and 0.847 (SE 0.017) after adjustment for age/sex and for all confounders, respectively (Table 5).Detailed results for the baseline model without time terms and for the PH tests are provided in Supplementary Tables S3 and S4.
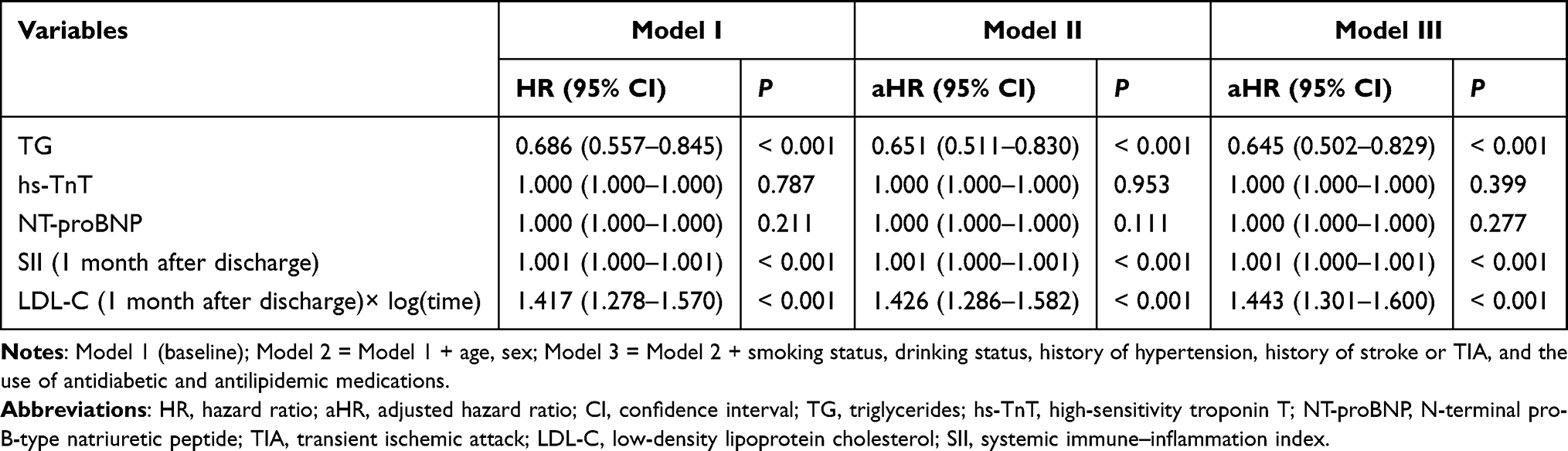 |
Table 3 Multivariable Time-Dependent Cox Analysis: Associations with the Primary Outcome |
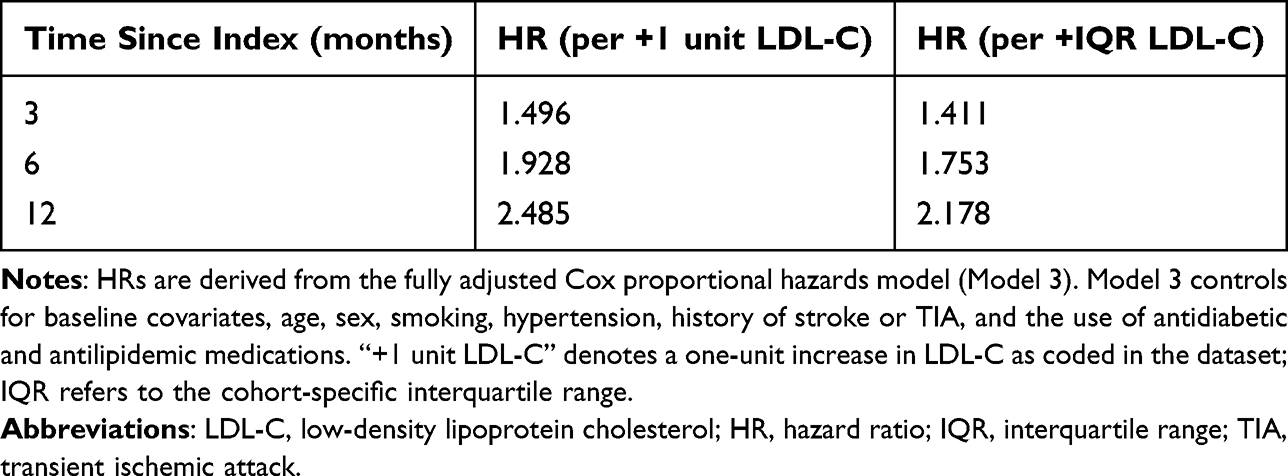 |
Table 4 Time-Specific Hazard Ratios for LDL-C From a Fully Adjusted Cox Model with an LDL-C × Log(Time) Interaction |
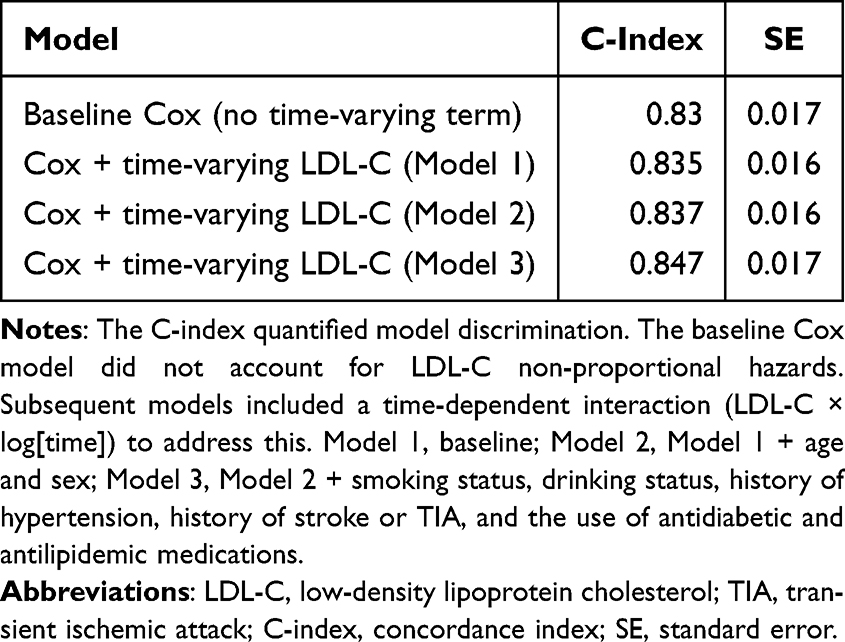 |
Table 5 C-Index Gains with Time-Dependent LDL-C and Adjustments |
Although the per-unit hazard ratio (HR) for SII appears close to 1.00, its clinical relevance lies in the large dynamic range of this biomarker. SII, calculated as (platelet count × neutrophil count) / lymphocyte count using counts in ×109/L, typically spans several hundred to several thousand. For example, with an HR of 1.001 per unit, a 500-unit increase corresponds to 1.001500 ≈ 1.65, and a 1,000-unit increase to 1.0011000 ≈ 2.72. This exponential relationship means that even small unit-level effects can translate into meaningful risk differences across realistic SII ranges. Despite a modest per-unit effect, SII remains a clinically informative and dynamic risk marker.
Bootstrap-Based Internal Validation: Calibration and Discrimination
To further assess the robustness of the primary model, we performed internal validation using bootstrap resampling (B=300) and evaluated performance at τ=11.5 months (event times truncated at 11.50 months; administrative censoring at 12.00 months). Before calibration, the Kaplan–Meier estimate of overall event risk was 19.9%, whereas the model’s mean predicted risk was 29.7%, indicating overestimation (E/O=1.49; Supplementary Figure S3). Linear recalibration substantially improved agreement (E/O=1.00; calibration slope=1.04; Figure 4A). After bootstrap validation with optimism correction (B=300), the model remained well calibrated (E/O=1.03; calibration slope=0.96; Figure 4B). For discrimination, Harrell’s C was 0.829 (95% CI 0.797–0.862), and Uno’s C at τ=11.5 months was 0.831 (Figure 4C); the optimism-corrected estimates were 0.822 (95% CI 0.810–0.841) and 0.824 (95% CI 0.811–0.843), respectively. Overall, the model exhibited good calibration and discriminative ability at the fixed time horizon and preserved stability after internal validation (Figure 4D).
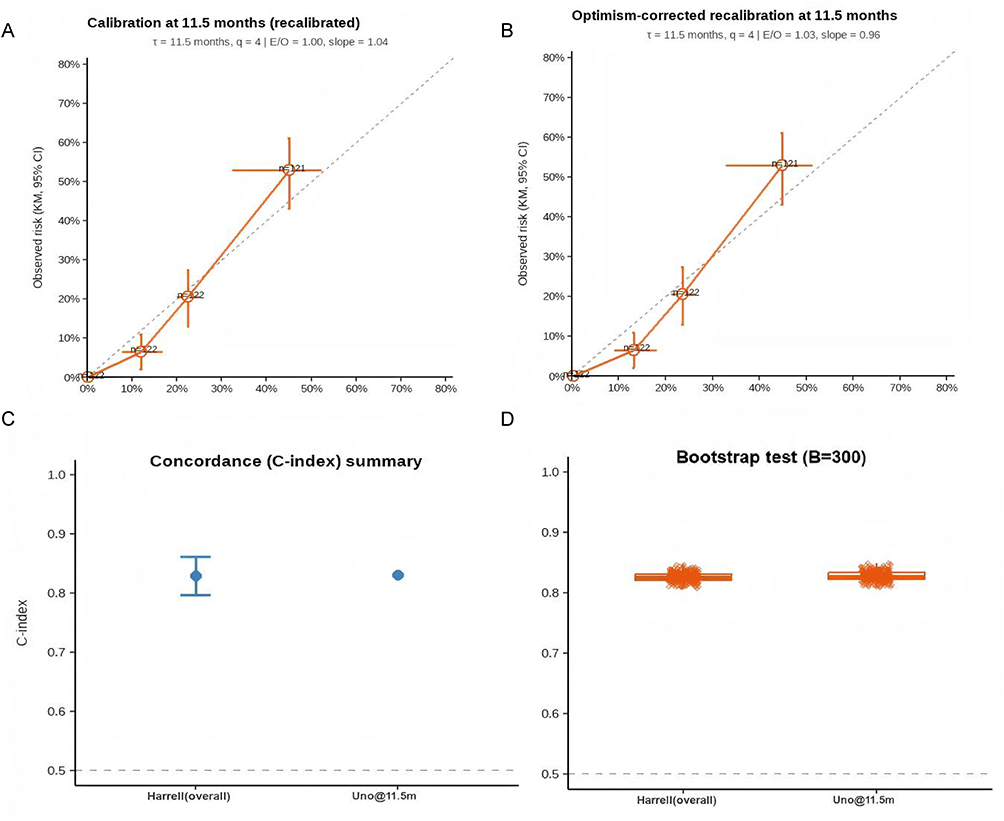 |
Figure 4 Internal validation and performance assessment at τ = 11.5 months. Abbreviations: τ, evaluation time horizon; B, number of bootstrap resamples; KM, Kaplan–Meier; CI, confidence interval. Notes: (A) Calibration plot after linear recalibration: observed Kaplan–Meier risk versus mean predicted risk across risk groups, with 95% CI. (B) Optimism-corrected calibration after bootstrap validation (B = 300). (C) Discrimination summary showing Harrell’s C and Uno’s C at τ = 11.5 months. (D) Bootstrap distributions of C-indices (B = 300). Event times were truncated at 11.5 months with administrative censoring at 12.0 months. |
Association Between the Temporal Trajectory of SII and Adverse Event Risk
To assess how temporal variation in the SII relates to the risk of MACE, we examined SII at multiple prespecified time points from the periprocedural period through post-discharge. We found that across all five time points—24h pre-PPCI, 24h post-PPCI, 48h post-PPCI, pre-discharge, and 1 month post-discharge—the event group consistently exhibited higher SII than the non-event group (all P < 0.05; Figure 5A–E). Despite an overall downward trend in both groups, the event group maintained consistently higher SII throughout follow-up (Figure 5F), indicating that persistently elevated SII is associated with adverse outcomes.
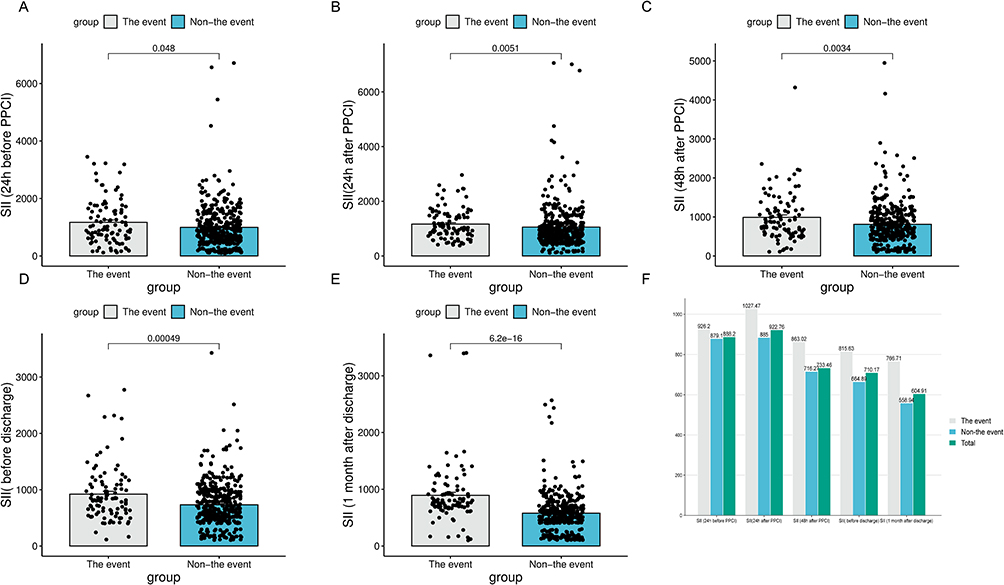 |
Figure 5 Dynamic changes in SII during the PPCI process and its association with adverse events. Abbreviations: SII, systemic immune-inflammation index; PPCI, primary percutaneous coronary intervention. Notes: (A) SII (24 h before PPCI) in event vs non-event groups; (B) SII (24 h after PPCI) in event vs non-event groups; (C) SII (48 h after PPCI) in event vs non-event groups; (D) SII (before discharge) in event vs non-event groups; (E) SII (1 month after discharge) in event vs non-event groups; (F) SII (longitudinal trajectory across all time points) in event vs non-event groups. |
Two-Dimensional Risk Stratification Based on LDL-C Target Attainment and the SII Cutoff
To construct a clinically actionable risk-stratification framework, we combined the 1-month post-discharge LDL-C target from the 2019 ESC/EAS dyslipidemia guidelines27 (attainment defined as LDL-C <1.4 mmol/L or ≥50% reduction from baseline) with the optimal SII cutoff determined by ROC analysis. Across five SII measurement time points from the peri-procedural period to 1 month post-discharge, the 1-month SII provided the highest discrimination (AUC=0.76; 95% CI, 0.71–0.82; P<0.001; Figure 6A), and the Youden index identified an optimal cutoff of 676.6×109/L. Patients were first stratified by this SII cutoff (≤676.6×109/L: n=304; >676.6×109/L: n=183) and then by 1-month LDL-C target attainment, yielding four groups: both on-target (n=122), SII on-target only (n=182), LDL-C on-target only (n=69), and both off-target (n=114) (Figure 6B). This two-dimensional scheme offers a concise, clinically actionable, and easy-to-apply basis for subsequent prognostic comparisons and risk assessment.
 |
Figure 6 Prognostic stratification and temporal predictive value of SII in AMI after PPCI. Abbreviations: AMI, acute myocardial infarction; PPCI, primary percutaneous coronary intervention; SII, systemic immune-inflammation index; LDL-C, low-density lipoprotein cholesterol; AUC, area under the curve. Notes: (A) ROC curves of SII measured at different time points for predicting 1-year adverse events. (B) Flowchart for patient stratification based on 1-month post-discharge SII and LDL-C target attainment. |
Interaction Between SII and LDL-C
Building on the stratified analyses, we evaluated SII–LDL-C interaction on both the multiplicative and additive scales to ascertain whether synergy exists. A dose–response gradient in primary‐outcome incidence was observed: dual target attainment 1.6% (2/122), LDL-C only not at target 9.9% (18/182), SII only not at target 20.3% (14/69), and both not at target 56.1% (64/114) (Supplementary Table S5). Schoenfeld residuals supported that the proportional hazards assumption held for the overall model (χ2 = 11.38, df = 6, P = 0.077; Supplementary Table S6). In multivariable Cox regression, the multiplicative interaction term was not significant (HR = 0.527, 95% CI 0.11–2.54; P = 0.425; Supplementary Table S7); likelihood ratio test χ2 = 0.718; P = 0.397. Nevertheless, adjusted hazards increased stepwise relative to the dual-attainment reference: SII on-target only, HR = 7.19 (1.67–31.0; P = 0.008); LDL-C on-target only, HR = 18.3 (4.14–80.6; P < 0.001); both off-target, HR = 69.2 (16.8–285.0; P < 0.0001; Figure 7). Although the limited events in the reference group widened some confidence intervals, both hazard ratios and crude rates increased monotonically, indicating a substantial cumulative risk effect of inadequate inflammation and lipid control. Consistent with this, additive‐scale indices indicated significant synergy: RERI = 44.79 (95% CI 9.94–201.22), AP = 0.65 (95% CI 0.38–0.78), and SI = 2.91 (95% CI 1.64–5.09)(Table 6). At 12 months, estimated absolute risks were 14.3% for the dual‐attainment group, 69.7% for SII only not at target, 55.8% for LDL-C only not at target, and 75.3% for both not at target (Supplementary Table S8), supporting synergistically amplified prognostic risk when both targets are unmet.
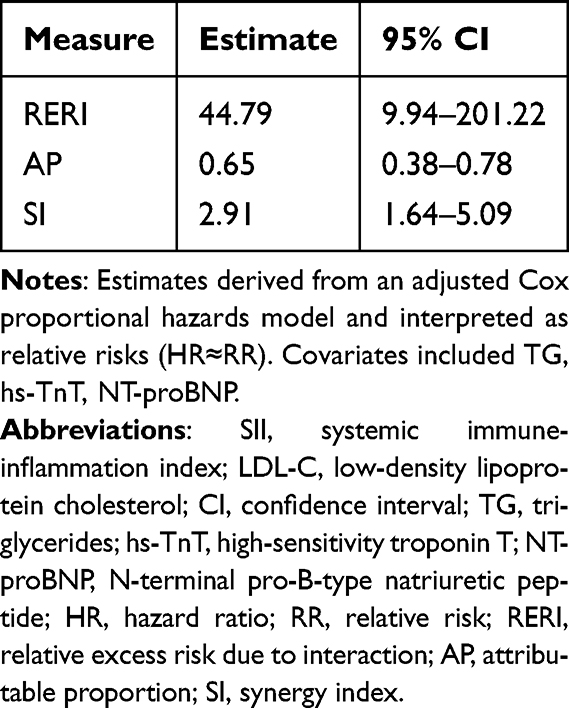 |
Table 6 Additive Interaction Between SII and LDL-C on the Relative-Risk Scale |
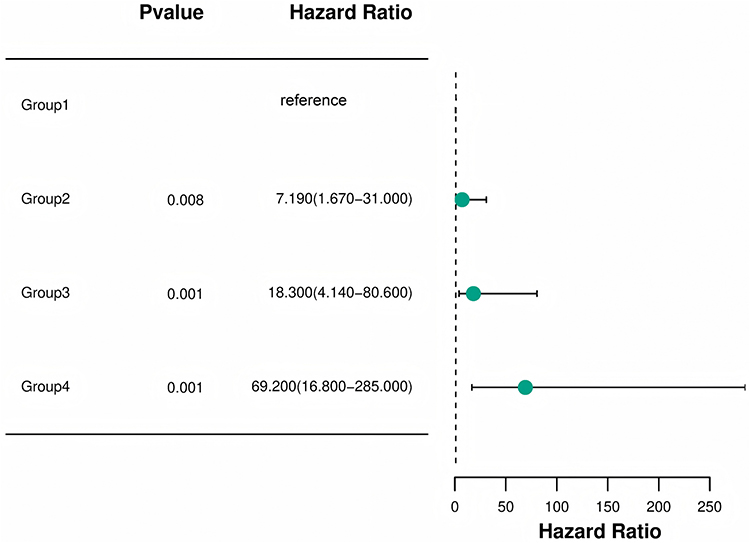 |
Figure 7 Forest plot of hazard ratios by dual-target stratification. Abbreviations: SII, systemic immune-inflammation index; LDL-C, low-density lipoprotein cholesterol; HR, hazard ratio; CI, confidence interval. Notes: Group definitions: Group 1, both on-target; Group 2, SII on-target only; Group 3, LDL-C on-target only; Group 4, both off-target. Points show hazard ratios from a multivariable Cox mo horizontal bars indicate 95% confidence intervals; the vertical dashed line marks HR = 1. P values are from Wald tests. |
Clinical and Biochemical Characteristics Stratified by SII and LDL-C Target-Attainment Status
When stratified by SII and LDL-C target attainment, there were no significant between-group differences in baseline age, sex, length of stay, heart rate, or blood pressure (all P>0.05). Diabetes prevalence differed across groups (P=0.046), whereas hypertension and heart failure did not. Regarding medications, only CCBs use varied between groups (P=0.002); use of ACEIs, ARBs, and β-blockers showed no significant differences. For biochemical indices, UA, ALB, LDL-C, HDL-C, and SII all differed across groups (all P<0.05; Supplementary Table S9). Notably, the both off-target (Group 4) displayed the most adverse inflammatory–metabolic profile—highest SII and LDL-C together with the lowest HDL-C—and also the highest diabetes prevalence and CCBs use (all P<0.05;Supplementary Table S9), indicating an accumulation of systemic inflammatory and metabolic burden and a more unfavorable cardiovascular risk profile.
Kaplan–Meier Survival Analysis Stratified by SII and LDL-C Target Attainment
Kaplan–Meier event-free survival curves stratified by SII and LDL-C target attainment showed significant separation across the four groups (log-rank P < 0.0001): the dual target-attainment group had the highest 12-month event-free survival, the dual non-attainment group had the poorest prognosis, and single-target attainment groups were intermediate. These findings indicate that concomitant control of inflammatory status and lipid levels is associated with substantially improved survival, underscoring the importance of integrated risk-management strategies in patients with acute myocardial infarction (Figure 8).
 |
Figure 8 Kaplan–Meier survival curves comparing four patient groups according to combined attainment of SII and LDL-C targets. Abbreviations: SII, systemic immune-inflammation index; LDL-C, low-density lipoprotein cholesterol. Notes: Group definitions: Group 1, both on-target; Group 2, SII on-target only; Group 3, LDL-C on-target only; Group 4, both off-target. |
Discussion
Among patients with AMI undergoing PPCI, we observed that at the 1-month post-discharge reassessment, strata defined by the combined control of the SII and LDL-C exhibited a clear absolute-risk gradient for 12-month clinical outcomes. Relative to either marker alone, the combined stratification yielded additional, clinically interpretable prognostic information—both on the additive scale (RERI, AP, and SI) and in between-group absolute-risk differences; the lack of statistical significance for interaction on the multiplicative scale does not preclude clinically meaningful joint effects. At 1 month, SII showed favorable discrimination (AUC ≈ 0.76), whereas the LDL-C–related risk appeared to increase over time, suggesting that subacute residual inflammation and medium- to long-term lipid burden may predominate in different temporal windows of risk. In view of the observational nature of this study, causal inferences should not be drawn from these associations.
Compared with prior studies, this work advances the literature on inflammatory markers and outcomes after AMI by proposing and validating a dual-target (“inflammation + lipids”) risk assessment strategy. Existing publications have widely reported associations between inflammatory indices—such as the SII and the neutrophil-to-lymphocyte ratio (NLR)—and adverse AMI outcomes; some have assessed SII at ≥6-month follow-up or compared multiple inflammatory markers within a common analytic framework.30–32 We did not conduct a head-to-head longitudinal comparison across multiple inflammatory indices (eg, SII, NLR, PLR); such comparative trajectory analyses will be addressed in future prospective work.Rather than repeating these baseline analyses, we contribute three innovations. First, we move beyond single-marker paradigms by introducing a four-quadrant dual-target stratification model, quantifying cumulative harm with additive interaction and absolute risk difference to enhance interpretability and clinical actionability. Second, we demonstrate temporal complementarity between SII and LDL-C: SII shows higher discriminative performance at 1 month post-discharge, whereas the prognostic value of LDL-C strengthens with longer follow-up, thereby informing dynamic surveillance and prioritization of interventions.27,33 Third, we promote translation from discrimination to clinical decision-making by incorporating SII and LDL-C as continuous variables in follow-up templates and applying bootstrap resampling for internal validation to evaluate model performance and stability,thereby laying the groundwork for net-benefit assessments—including net reclassification improvement (NRI), integrated discrimination improvement (IDI), and decision-curve analysis (DCA)—to support stepwise clinical implementation.34–36 We note that heterogeneity and potential bias in endpoint definitions, threshold selection, and covariate adjustment persist across existing studies; therefore, external validation and model calibration remain prerequisites for broader adoption of this strategy.Our study profiles SII longitudinally at prespecified time points and integrates SII with LDL-C for risk stratification.
Mechanistically, our findings align with a pathophysiological framework of reciprocal amplification between immunity and lipids:17,37 inflammatory activation promotes LDL oxidation and phagocytic uptake by macrophages,38 augments platelet reactivity,39 and worsens endothelial dysfunction,40 whereas cholesterol burden within the vascular wall sustains inflammation and a prothrombotic milieu,40 together fostering an adverse immunothrombotic microenvironment.41 Despite the rapid reperfusion afforded by PPCI, inflammatory resolution may follow a nonlinear trajectory;41 early post-discharge inflammatory burden and subsequent lipid-driven atherosclerotic activity may sequentially dominate risk trajectories, providing biological plausibility for temporally distinct risk phenotypes (requiring further confirmation in mechanistic studies and interventional trials).
Clinical application: a two-pronged strategy.(1) Set dichotomized targets (on-target vs off-target) for SII and LDL-C at the 1-month post-discharge visit. If only LDL-C is off-target, intensify lipid-lowering therapy and strengthen adherence support. If only SII is off-target, perform a systematic work-up for inflammatory sources (eg, infection, periodontitis, obesity-related metabolic inflammation, smoking) and evaluate the appropriateness and safety of anti-inflammatory options. If both are off-target, assign the patient to a high-risk management pathway with medication optimization, lifestyle modification, inflammatory source control, and prioritized multidisciplinary care.(2) Continuous-variable pathway embedded in the EHR. Integrate SII and LDL-C as continuous variables into EHR-based follow-up templates with periodic reassessment; quantify net clinical benefit over current workflows using net reclassification improvement (NRI), integrated discrimination improvement (IDI), decision-curve analysis (DCA), and clinical impact curves (CIC); thresholds and models warrant external recalibration in independent cohorts.Note on the SII threshold. The SII cut-off used in this study (≤ 676.6 × 109/L) was derived from an internal ROC analysis and intended primarily for within-cohort stratification; its external generalizability and the optimal cut-point require validation in independent populations.
This study neither prespecified nor conducted sex-stratified analyses or sex-by-marker (SII, LDL-C) interaction analyses; accordingly, the estimates reflect sex-combined averages and should not be assumed to apply equally to men and women. Future studies and external validations should prospectively register prespecified sex-stratified and sex-by-marker interaction analyses, use event-driven power calculations, and report sex-specific absolute risks and net clinical benefit to define the sex-specific applicability of this strategy.
This study anchors a clinically meaningful 1-month reassessment window, delineates longitudinal trajectories of the SII, applies LASSO for variable selection while explicitly modeling time-varying effects, and quantifies interaction on the additive scale together with absolute risk differences to enhance clinical interpretability. Model robustness is further supported by bootstrap resampling. Nevertheless, several limitations merit consideration. First, the single-center, retrospective design and the small number of events in the reference group constrain external validity and preclude causal inference. Second, Residual confounding may persist due to incomplete adjustment for treatment adherence and high-risk phenotypes (eg, cardiogenic shock). Third, approximating risk ratios with hazard ratios on the additive scale may bias estimates when events are not rare. Fourth, the SII cut point was derived from internal data, and the model— including LASSO-based selection—lacks external validation and recalibration, raising concern for overfitting. Fifth, the absence of repeated longitudinal measurements of SII and LDL-C and limited long-term follow-up precluded evaluation of long-term outcomes and cost-effectiveness. Looking ahead, multicenter prospective studies with richer longitudinal profiling, external validation and recalibration of thresholds/models, and extended follow-up are needed to establish long-term outcomes and health-economic benefits.
Future work should proceed along three complementary axes: (1) in multicenter prospective cohorts, externally validate the four-quadrant risk-stratification strategy and perform threshold/model recalibration; (2) integrate treatment trajectories and repeated-measures data, applying joint and multi-state models together with time-dependent covariates to characterize the longitudinal coupling between SII and LDL-C, and quantify net clinical benefit using net NRI, IDI, and DCA; (3) in the dual non-attainment population, evaluate a structured, multi-component intervention (pharmacotherapy, lifestyle modification, control of inflammatory sources, adherence support) with embedded cost-effectiveness analysis and sex-stratified evaluation. Overall, the evidence chain is transitioning from association discovery to validation of actionable strategies; closing the loop will require both external validation and interventional trials.
Conclusions
Among AMI patients undergoing PPCI, combined control of the SII and LDL-C was associated with improved 12-month outcomes. Control of inflammation provided prognostic information incremental to lipid-lowering therapy, underscoring the importance of addressing residual inflammatory risk. These findings support integrating a dual-target strategy (inflammation and lipids) into secondary prevention, while prospective—ideally randomized—validation is needed before routine clinical implementation.
Data Sharing Statement
Data for the current study are available from the corresponding author upon reasonable request.
Ethics Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Xuzhou Medical University Affiliated Hospital (Approval No. XYFY2022-KL420-01).
Consent for Publication
All the authors approved to publication.
Patient Consent Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Xuzhou Medical University Affiliated Hospital (Approval No. XYFY2022-KL420-01). Given the retrospective nature of the study, the requirement for informed consent was waived by the ethics committee. All patient data were anonymized and handled with strict confidentiality to ensure the protection of personal privacy and rights.
Acknowledgments
We appreciate the support of all study participants and thank Mingjie Chen (Shanghai NewCore Biotechnology Co., Ltd.) for assistance with data analysis and visualization. This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-6674609/v1.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Defeng Pan’s Applied Basic Research Project of Xuzhou.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hudzik B, Błachut A, Lesiak M, et al. Summary of the European Society of Cardiology guidelines on dual antiplatelet therapy in patients after percutaneous coronary interventions. Kardiol Pol. 2022;80(10):974–989. doi:10.33963/KP.a2022.0198
2. Räber L, Mintz GS, Koskinas KC, et al. Clinical use of intracoronary imaging. Part 1: guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J. 2018;39(35):3281–3300. doi:10.1093/eurheartj/ehy285
3. Thrane PG, Olesen KKW, Thim T, et al. Mortality trends after primary percutaneous coronary intervention for st-segment elevation myocardial infarction. J Am Coll Cardiol. 2023;82(10):999–1010. doi:10.1016/j.jacc.2023.06.025
4. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
5. Guedeney P, Giustino G, Sorrentino S, et al. Efficacy and safety of alirocumab and evolocumab: a systematic review and meta-analysis of randomized controlled trials. Eur Heart J. 2022;43(7):e17–e25. doi:10.1093/eurheartj/ehz430
6. Libby P. Inflammation in atherosclerosis-no longer a theory. Clin Chem. 2021;67(1):131–142. doi:10.1093/clinchem/hvaa275
7. Frantz S, Hundertmark MJ, Schulz-Menger J, Bengel FM, Bauersachs J. Left ventricular remodelling post-myocardial infarction: pathophysiology, imaging, and novel therapies. Eur Heart J. 2022;43(27):2549–2561. doi:10.1093/eurheartj/ehac223
8. Kawai K, Kawakami R, Finn AV, Virmani R. Differences in stable and unstable atherosclerotic plaque. Arterioscler Thromb Vasc Biol. 2024;44(7):1474–1484. doi:10.1161/atvbaha.124.319396
9. Hu B, Yang X-R, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.Ccr-14-0442
10. Esenboğa K, Kurtul A, Yamantürk YY, Tan TS, Tutar DE. Systemic immune-inflammation index predicts no-reflow phenomenon after primary percutaneous coronary intervention. Acta Cardiol. 2022;77(1):59–65. doi:10.1080/00015385.2021.1884786
11. Luo J, Qin X, Zhang X, et al. Prognostic implications of systemic immune-inflammation index in myocardial infarction patients with and without diabetes: insights from the NOAFCAMI-SH registry. Cardiovasc Diabetol. 2024;23(1):41. doi:10.1186/s12933-024-02129-x
12. Zhang C, Li M, Liu L, et al. Systemic immune-inflammation index as a novel predictor of major adverse cardiovascular events in patients undergoing percutaneous coronary intervention: a meta-analysis of cohort studies. BMC Cardiovasc Disord. 2024;24(1):189. doi:10.1186/s12872-024-03849-4
13. Bilgin M, Akkaya E, Dokuyucu R. Evaluation of inflammatory markers in predicting coronary complexity: insights from the SYNTAX II Score in NSTEMI patients. J Clin Med. 2024;13(19):5940. doi:10.3390/jcm13195940
14. Li X, Chen Y, Yuan Q, et al. Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio associated with 28-day all-cause mortality in septic patients with coronary artery disease: a retrospective analysis of MIMIC-IV database. BMC Infect Dis. 2024;24(1):749. doi:10.1186/s12879-024-09516-5
15. Li X, Yu C, Liu X, et al. A prediction model based on systemic immune-inflammatory index combined with other predictors for major adverse cardiovascular events in acute myocardial infarction patients. J Inflamm Res. 2024;17:1211–1225. doi:10.2147/jir.S443153
16. Yang YL, Wu C-H, Hsu P-F, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
17. Libby P. Inflammation during the life cycle of the atherosclerotic plaque. Cardiovasc Res. 2021;117(13):2525–2536. doi:10.1093/cvr/cvab303
18. Dri E, Lampas E, Lazaros G, et al. Inflammatory mediators of endothelial dysfunction. Life. 2023;13(6). doi:10.3390/life13061420
19. Tall AR, Yvan-Charvet L. Cholesterol, inflammation and innate immunity. Nat Rev Immunol. 2015;15(2):104–116. doi:10.1038/nri3793
20. Inoue T, Croce K, Morooka T, et al. Vascular inflammation and repair: implications for re-endothelialization, restenosis, and stent thrombosis. JACC. 2011;4(10):1057–1066. doi:10.1016/j.jcin.2011.05.025
21. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
22. Tercan H, van Broekhoven A, Bahrar H, et al. The effect of low-dose colchicine on the phenotype and function of neutrophils and monocytes in patients with chronic coronary artery disease: a double-blind randomized placebo-controlled cross-over study. Clin Pharmacol Ther. 2024;116(5):1325–1333. doi:10.1002/cpt.3394
23. Thygesen K, Alpert JS, Jaffe AS. Fourth universal definition of myocardial infarction (2018). Rev Esp Cardiol. 2019;72. doi:10.1016/j.rec.2018.11.011
24. Ibánez B, James S, Agewall S, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Rev Esp Cardiol. 2017;70(12):1082. doi:10.1016/j.rec.2017.11.010
25. Guideline and consensus for the management of patients with non-ST-elevation acute coronary syndrome (2016). Zhonghua Xin Xue Guan Bing Za Zhi. 2017;45(5):359–376. doi:10.3760/cma.j.issn.0253-3758.2017.05.003
26. Grundy SM, Stone NJ, Bailey AL, et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation. 2019;139(25):e1046–e1081. doi:10.1161/cir.0000000000000624
27. Mach F, Baigent C, Catapano AL, et al. ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
28. Öcal L, Keskin M, Cerşit S, et al. Systemic immune-inflammation index predicts in-hospital and long-term outcomes in patients with ST-segment elevation myocardial infarction. Coron Artery Dis. 2022;33(4):251–260. doi:10.1097/mca.0000000000001117
29. Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovascular studies: the story of major adverse cardiac events and percutaneous coronary intervention. J Am Coll Cardiol. 2008;51(7):701–707. doi:10.1016/j.jacc.2007.10.034
30. Ul Hussain H, Kumar KA, Zahid M, et al. Neutrophil to lymphocyte ratio as a prognostic marker for cardiovascular outcomes in patients with ST-segment elevation myocardial infarction after percutaneous coronary intervention: a systematic review and meta-analysis. Medicine. 2024;103(26):e38692. doi:10.1097/md.0000000000038692
31. Wei X, Zhang Z, Wei J, Luo C. Association of systemic immune inflammation index and system inflammation response index with clinical risk of acute myocardial infarction. Front Cardiovasc Med. 2023;10:1248655. doi:10.3389/fcvm.2023.1248655
32. Zhu Y, He H, Qiu H, et al. Prognostic value of systemic immune-inflammation index and nt-probnp in patients with acute st-elevation myocardial infarction. Clin Interv Aging. 2023;18:397–407. doi:10.2147/cia.S397614
33. Banach M, Surma S, Toth PP. 2023:The year in cardiovascular disease - the year of new and prospective lipid lowering therapies. Can we render dyslipidemia a rare disease by 2024? Arch Med Sci. 2023;19(6):1602–1615. doi:10.5114/aoms/174743
34. Pencina MJ, D’Agostino RB, Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30(1):11–21. doi:10.1002/sim.4085
35. Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. 2008;8(53). doi:10.1186/1472-6947-8-53
36. Iba K, Shinozaki T, Maruo K, Noma H. Re-evaluation of the comparative effectiveness of bootstrap-based optimism correction methods in the development of multivariable clinical prediction models. BMC Med Res Methodol. 2021;21(9). doi:10.1186/s12874-020-01201-w
37. Soehnlein O, Libby P. Targeting inflammation in atherosclerosis - from experimental insights to the clinic. Nat Rev Drug Discov. 2021;20(8):589–610. doi:10.1038/s41573-021-00198-1
38. Binder CJ, Papac-Milicevic N, Witztum JL. Innate sensing of oxidation-specific epitopes in health and disease. Nat Rev Immunol. 2016;16(8):485–497. doi:10.1038/nri.2016.63
39. Koupenova M, Clancy L, Corkrey HA, Freedman JE. Circulating platelets as mediators of immunity, inflammation, and thrombosis. Circ Res. 2018;122(2):337–351. doi:10.1161/circresaha.117.310795
40. Gimbrone MA Jr, García-Cardeña G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. 2016;118(4):620–636. doi:10.1161/circresaha.115.306301
41. Engelmann B, Massberg S. Thrombosis as an intravascular effector of innate immunity. Nat Rev Immunol. 2013;13(1):34–45. doi:10.1038/nri3345
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.