")
Back to Journals » International Journal of General Medicine » Volume 15
The Clinical Characteristics of 88 Patients with Total Anomalous Pulmonary Venous Connection and Risk Factors Associated with Early Postoperative Death
Authors Gui L, Wang AB, Zi J, Ai GY, Wang HH, Zhu M, Liang H
Received 30 June 2022
Accepted for publication 16 September 2022
Published 13 October 2022 Volume 2022:15 Pages 7809—7816
DOI https://doi.org/10.2147/IJGM.S380677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lin Gui,1 An-Biao Wang,2 Jie Zi,2 Ge-Yi Ai,3 Hui-Hui Wang,1 Mei Zhu,1 Hao Liang1
1Department of Ultrasound, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China; 2Department of Cardiovascular Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China; 3Department of Anesthesiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China
Correspondence: Mei Zhu; Hao Liang, Department of Ultrasound, Shandong Provincial Hospital Affiliated to Shandong First Medical University, No. 324, Jing Wu Road, Huai Yin District, Jinan, 250021, People’s Republic of China, Tel +86-15653101616 ; +86-13506411901, Email [email protected]; [email protected]
Objective: This study aimed to analyze the outcomes and risk factors of early postoperative death (within 30 days after surgery) in a single-center after repair of total anomalous pulmonary venous connection (TAPVC).
Methods: The clinical data of 88 children who had been diagnosed with TAPVC and underwent radical operation in the Shandong Provincial Hospital Affiliated with Shandong First Medical University (China) from January 2015 to July 2021 were retrospectively analyzed. All the patients were divided into the survival group (n = 81) and the death group (n = 7) for the analysis of preoperative and postoperative clinical data. The variables associated with early postoperative death were statistically analyzed to obtain the risk factors for early postoperative death of TAPVC.
Results: Of the 88 patients included in this study, 7 (7.95%) patients died early, including 4 supracardiac and 3 infracardiac cases. Recurrent pulmonary vein obstruction occurred in 2 patients after discharged from hospital, and both were intracardiac TAPVC. Delayed death occurred in 2 children, both of which were intracardiac TAPVC cases. According to univariate analysis, the risk factors statistically significantly associated with the early postoperative death included infracardiac type (P = 0.08), preoperative maximum pulmonary vein flow velocity (P = 0.031), preoperative mechanical ventilation (P = 0.043), preoperative maximum pulmonary artery pressure (P = 0.000), intraoperative cardiopulmonary bypass time (P = 0.003) and intraoperative aortic cross-clamp time (P = 0.000).
Conclusion: Infracardiac type of TAPVC, preoperative maximum pulmonary vein flow velocity, preoperative mechanical ventilation, preoperative maximum pulmonary artery pressure, intraoperative cardiopulmonary bypass time and aortic cross-clamp time are the risk factors for early postoperative death.
Keywords: congenital heart disease, TAPVC, cardiopulmonary bypass time, aortic cross-clamp time, risk factor, postoperative recurrent pulmonary venous obstruction
Total anomalous pulmonary venous connection (TAPVC) is a relatively rare congenital heart disease that accounts for approximately 1%–3% of congenital heart diseases.1 The anatomical feature of this disease is that the pulmonary veins, which typically flow into the left atrium, fail to connect to this part of the heart and instead, directly or indirectly flow into the right atrium. According to the classification by Darling et al in 1957,2 TAPVC can be divided into four types, ie, supracardiac, intracardiac, infracardiac, and mixed. Without treatment, the mortality rate of children with TAPVC in the first year of life is as high as 80%.3 With the accumulation of surgical experience and the enhancement of postoperative care, the surgical prognosis for children with TAPVC has continuously been improved, and the reported mortality rate has remained at <10%.4 The clinical characteristics and risk factors for early death among 88 children with TAPVC in the authors’ center were retrospectively analyzed in this study. Some echocardiography indicators were also considered in this study such as the velocity of preoperative pulmonary vein and preoperative pulmonary artery pressure to evaluate the relationship with early postoperative death.
Materials and Methods
Ethics Statement
The Ethics Committee of Shandong Provincial Hospital affiliated to Shandong First Medical University approved this study (approval number 2017458, date of approval 29 September 2017). This study was conducted in accordance with the declaration of Helsinki. The parent or legal guardian of patients under 18 years of age provided informed consent.
Clinical Data and Definitions
Retrospective analysis was performed on the clinical data of 88 children diagnosed with TAPVC and treated with surgery in Shandong Provincial Hospital Affiliated to Shandong First Medical University (China) from January 2015 to July 2021, including the symptoms and signs on admission, preoperative transthoracic echocardiography (TTE) results, and intraoperative and postoperative follow-up TTE results. Children with complex congenital heart diseases, such as single ventricle and transposition of the great arteries, were excluded. There were 47 males (53.4%) and 41 females (46.6%), including 25 neonates (28.4%); the median age was 57.5 (28.5, 144.7) days, and the median weight was 4.05kg (3.58, 5.48) kg. There were 45 (51.1%) supracardiac, 32 (36.4%) intracardiac, 9 (10.2%) infracardiac, and 2 (2.3%) mixed-type cases; 29 (33%) cases were complicated with patent ductus arteriosus (PDA); 19 cases (20.5%) had preoperative pulmonary vein obstruction, and 11 cases (12.5%) of TAPVC that had been diagnosed in the fetal period with a diagnostic coincidence rate of 100% (Table 1). Early mortality was defined as death occurred 30 days after surgery during the hospital stay. The definition of preoperative pulmonary vein obstruction was made by the combination of oxygen saturation and the echocardiographic data, of which the flow velocity >1.8 m/s. The reintervention criteria were that a decline of the oxygen saturation and the flow velocity of the anastomotic >1.8 m/s. And the following strategy was surgical operation.
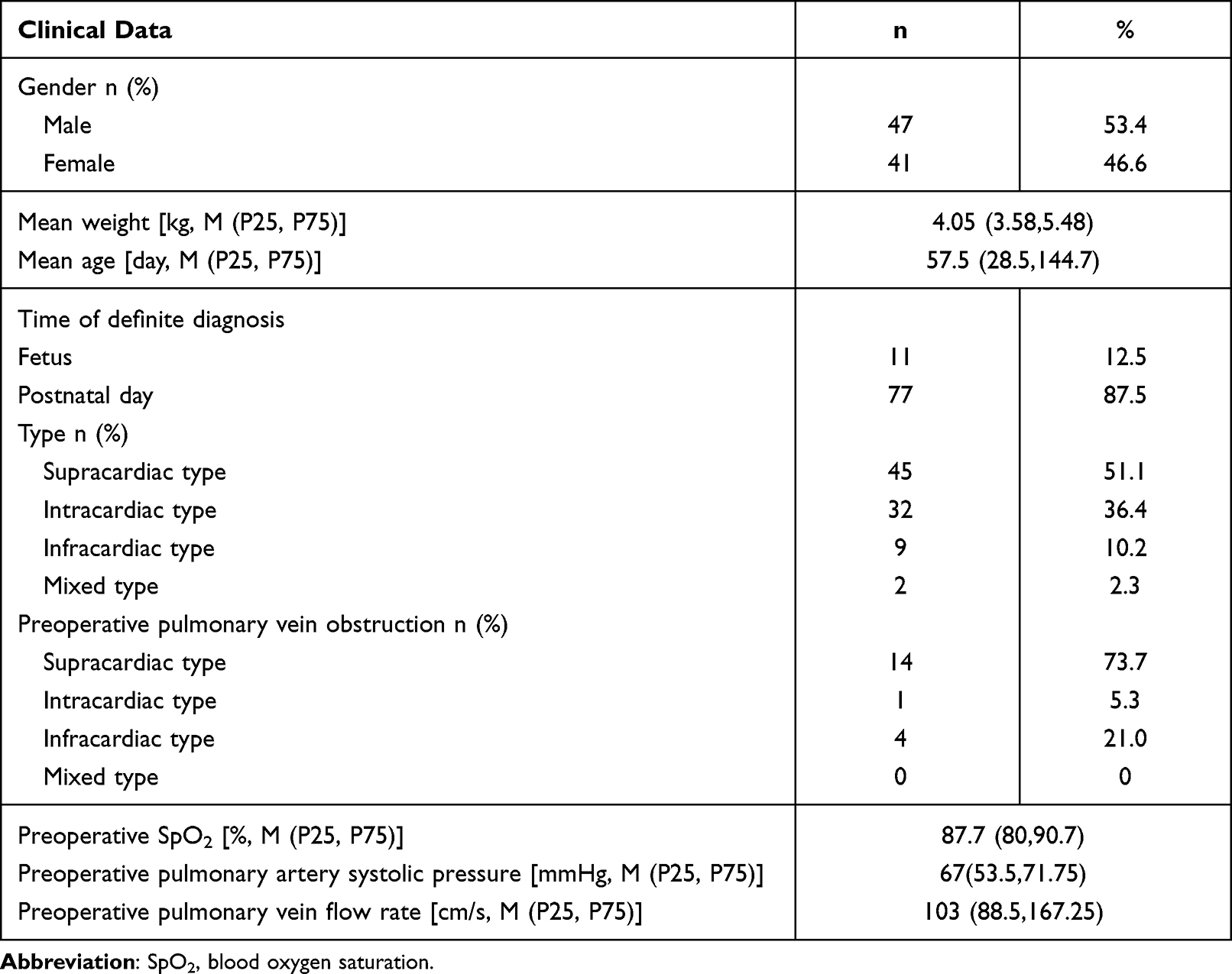 |
Table 1 Patient Data |
Grouping and Analysis
A total of 7 patients died early after surgery. All of the children who underwent TAPVC were divided into the survival (n = 81) and death groups (n = 7), respectively. The patients in the two groups were compared and analyzed for age, gender, weight, anatomical type, preoperative obstruction, preoperative pulmonary vein flow velocity, preoperative mechanical ventilation, preoperative oxygen saturation, preoperative pulmonary artery pressure, cardiopulmonary bypass (CPB) time, aortic cross-clamp (ACC) time, postoperative intensive care unit (ICU) stay, and other indexes.
Surgical Methods
A mid-sternal incision was made under general anesthesia. For supracardiac-type cases, the common trunk of the pulmonary vein was anastomosed with the left atrium, and the vertical vein was ligated. For the intracardiac-type cases, the atrial septal defect or oval foramen to the coronary sinus opening was enlarged, the atrial septal defect was repaired, and the pulmonary vein was isolated into the left atrium. For the infracardiac-type cases, the common trunk of the pulmonary vein was anastomosed with the left atrium, and the vertical vein ligated. For the mixed-type cases, the corresponding surgery mode was selected, based on the relevant anatomical morphology.
Sutureless technique was to incise the common trunk of the pulmonary vein and suture the pericardium around the common trunk of the pulmonary vein with the left atrium.
Statistical Analysis
The SPSS Statistics 26.0 software program was used to conduct the data analysis. All numerical variables were non-normally distributed data and presented as M (P25, P75), and a Cox regression model was used for evaluating the risk factors associated with early postoperative TAPVC death; P < 0.05 indicated a statistically significant difference. Multivariable analysis was not performed due to the limited sample size. The overall survival rate was analyzed by Kaplan–Meier curve.
Results
Ultrasonic Morphology Analysis
Among the 88 children with TAPVC, 11 were diagnosed with TAPVC by prenatal ultrasound, and all patients were diagnosed at 24–37 weeks of gestation. A total of 6 TAPVC cases were not detected during the fetal period, including 3 supracardiac and 2 intracardiac cases, as well as 1 mixed case, all of which were detected from 1 day to 1 month after birth.
The echocardiographic results of 88 children with TAPVC revealed 45 supracardiac cases, in which drained directly into the superior vena cava via vertical veins in 14 cases, and into the left innominate vein and then into the superior vena cava via vertical vein in 30 cases; 1 patient had double vertical veins, of which the left vertical vein drained into the left innominate vein, and the right vertical vein drained into the superior vena cava. There were 32 intracardiac-type cases, including 26 which draining into the coronary sinus via vertical veins and 6 cases which draining into the right atrium directly. There were 9 infracardiac cases, including 5 draining into the portal vein via the vertical vein, and 4 cases draining into the hepatic vein via vertical veins. The mixed type included 2 cases, both of which were the supracardiac + intracardiac type. A total of 19 patients were diagnosed with obstructive TAPVC preoperatively, including 14 supracardiac (31.1%), 4 infracardiac (44.4%), and 1 intracardiac (3.1%) cases; the infracardiac type was more likely to be associated with pulmonary vein obstruction than other types. There were 29 patients with PDA, 2 with a fine muscular ventricular septal defect, 1 with a bicuspid aortic valve, 1 with mild pulmonary valve stenosis, 1 with mild mitral valve prolapse, and 2 patients with congenital anal atresia.
Early Mortality Analysis
The median CPB and AAC time of 88 children who underwent surgery was 76.5 (65,105) min and 46 (35.25, 62.75) min, respectively. The median time of postoperative ICU stay was 7 (5, 10) days, and the median time of postoperative mechanical ventilation was 3 (2, 5) days. A total of 7 patients (7.95%) died, including 4 supracardiac and 3 infracardiac cases, among which 3 were neonates; 4 cases had PDA, and all 6 patients presented respiratory failure and severe pulmonary hypertension preceding surgery. Delayed sternal closure occurred in 3 children postoperatively, and circulatory failure was the main cause of death (Table 2). Delayed death occurred in 2 children, one of whom died 40 days after surgery, and one died of heart failure 35 days after surgery. The analysis of the factors associated with death and survival showed statistically significant differences between the death and survival groups, respectively, in terms of infracardiac type (P = 0.008), preoperative maximum pulmonary vein flow rate (P = 0.031), preoperative mechanical ventilation (P = 0.043), preoperative maximum pulmonary artery pressure (P = 0.000), intraoperative CPB time (P = 0.003) and ACC time (P = 0.000) (Table 3).
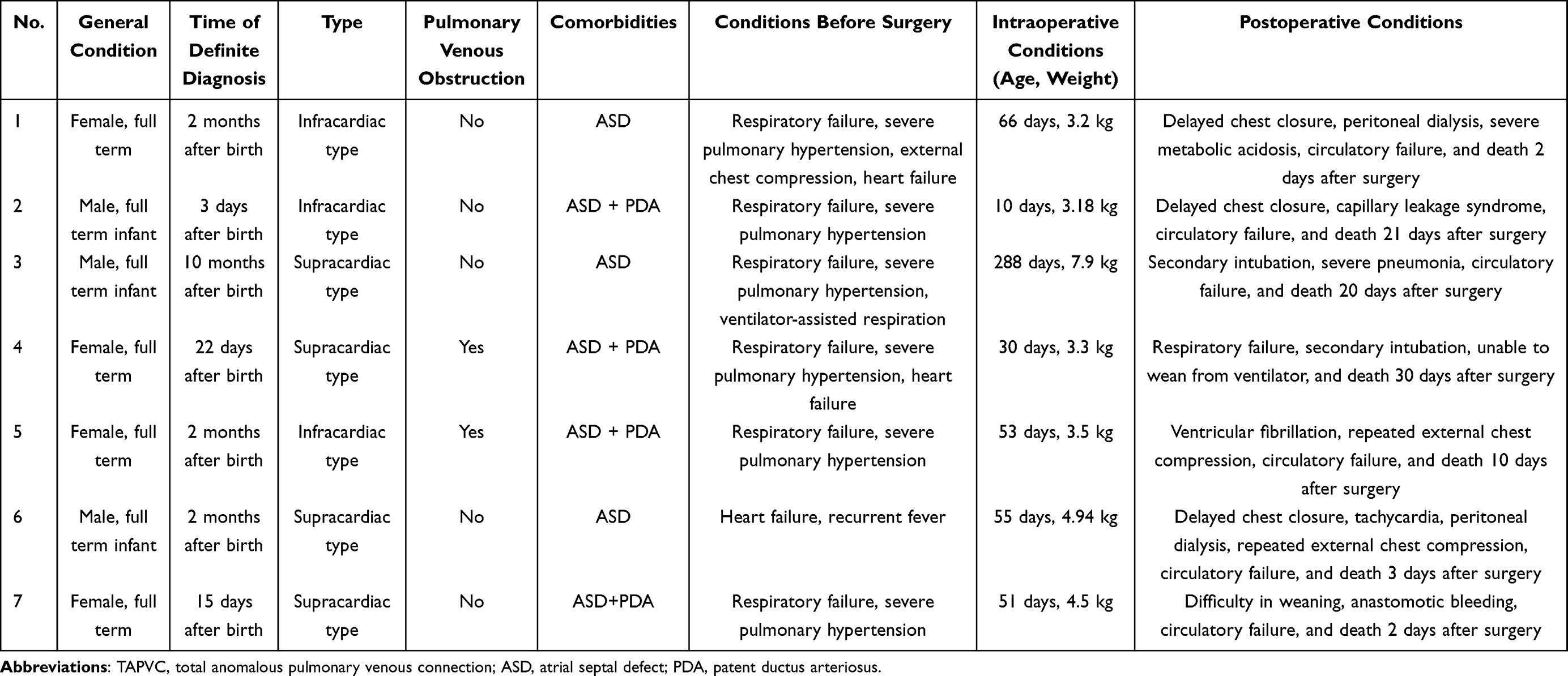 |
Table 2 Seven Cases of Early Postoperative Death After TAPVC |
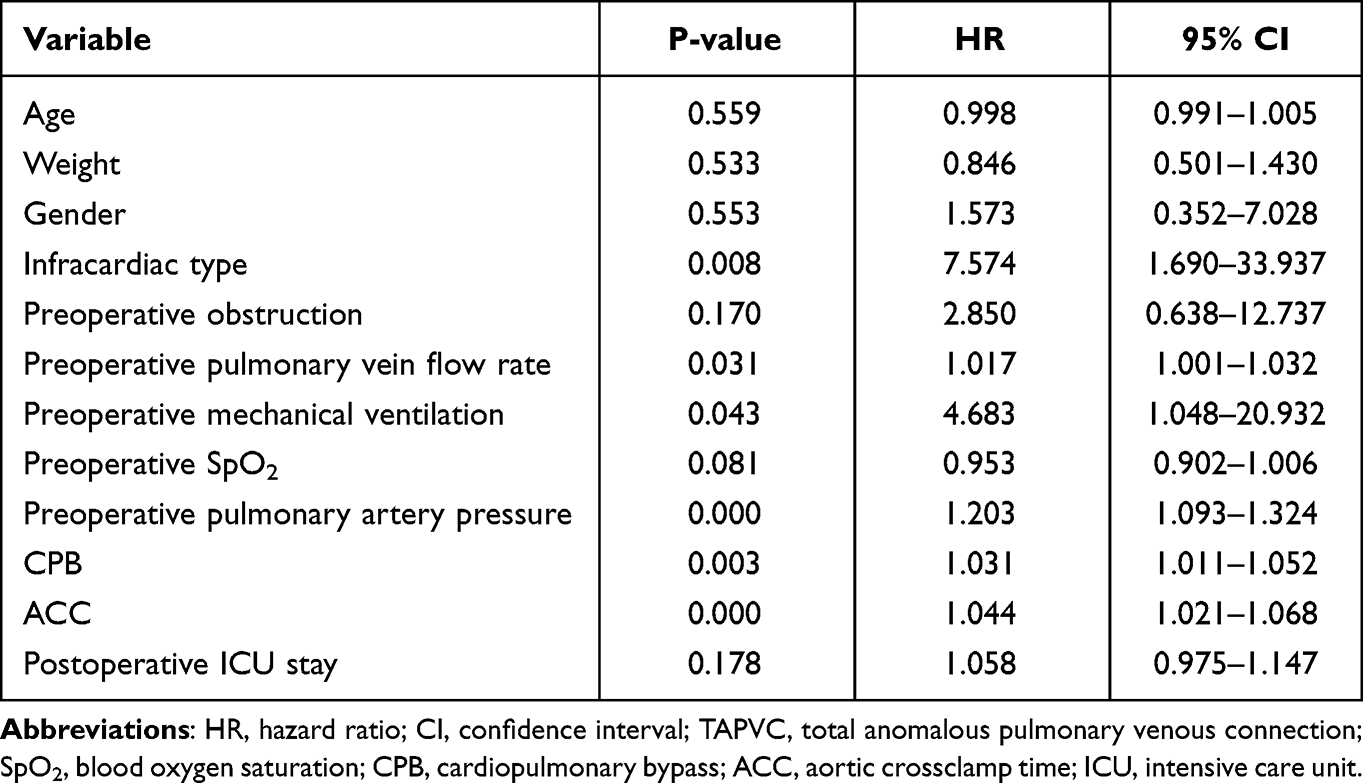 |
Table 3 Variables in the Univariate Cox Proportional Hazard Model Associated with Early Postoperative Death of TAPVC |
Analysis of Postoperative Recurrent Obstruction
Recurrent post-surgery obstruction occurred in 2 children with TAPVC. Both of them were intracardiac TAPVC, and no pulmonary vein obstruction were observed before surgery. The first child had anastomotic stenosis occurred 3 months after surgery. After the reintervention, the child’s condition improved and was discharged after the second surgery but died 40 days after discharged for unknown causes.
The second child had recurrent pulmonary vein obstruction 9 months after surgery, the child was discharged after reintervention, and was normal at a 6-month follow-up.
Follow-Up
Of the 81 patients who were discharged from hospital, 75 patients were followed up for a period from 1 to 84 months, 2 of them had delayed death, 2 of them had postoperative recurrent PVO, and the overall survival rate is displayed in Figure 1.
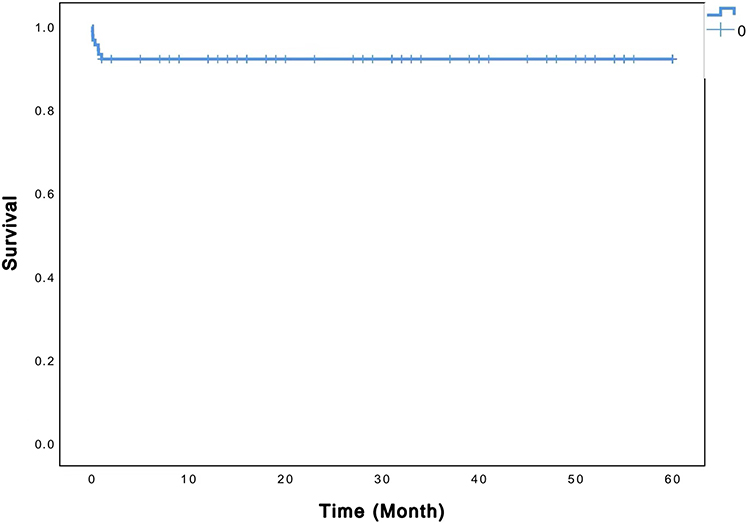 |
Figure 1 Kaplan–Meier curves for all survival. |
Discussion
Based on the continued improvement of surgical methods and clinical management, studies have shown that the early postoperative mortality of TAPVC ranged from 2.7% to 9.8%.5–8 The current study revealed that the early postoperative mortality of TAPVC in the authors’ center was approximately 7.9%, and univariate analysis showed that TAPVC anatomical type, increased preoperative pulmonary vein flow velocity, increased pulmonary artery pressure, mechanical ventilation, and a longer CPB time were all associated with early postoperative death.
Total anomalous pulmonary venous connection can be divided into four types, with a low incidence of mixed type, and the infracardiac type is more likely to be complicated by pulmonary vein obstruction.9,10 In this study, the obstruction rate of the infracardiac TAPVC was higher compared with other types. Infracardiac TAPVC pulmonary vein was generally channeled into the right chamber via the portal vein and the inferior vena cava, with a long return path and a raised risk of external compression; moreover, hepatic and portal vein systems were prone to fibrosis and occlusion; therefore, pulmonary vein obstruction was more likely to occur.
This study showed that the infracardiac type of TAPVC was associated with early death. Infracardiac TAPVC was prone to being complicated by obstruction, leading to severe pulmonary edema and an increased mortality rate.6,9 Some studies showed that the prognosis of mixed TAPVC was poor, likely due to the lack of a single common convergence area and the uncertain and complex morphology of pulmonary venous return, which will increase the risk of death.9 In this study, the 2 cases of mixed type were both supracardiac + intracardiac type, the drainage pathway of pulmonary vein was not that complicated, no preoperative pulmonary vein obstructions were observed, and the prognosis was good. The amount of this type of TAPVC was small, so they cannot reflect the characteristics of the mixed type of TAPVC.
Most of the children who received mechanical ventilation before surgery evidenced unstable conditions, with low oxygen partial pressure, high pulmonary artery pressure, pulmonary vein obstruction, and were complicated with respiratory failure, cardiac insufficiency, and other symptoms. The risk of postoperative death increased due to the poor overall conditions of these children.
This study indicated mechanical ventilation before surgery as being associated with postoperative mortality. Due to the complexity of TAPVC surgery and the unstable condition of patients during the operation, a long CPB time or ACC time is always required, resulting in an increased risk of death.6 Multiple studies indicated a too-long CPB time or ACC time as being risk factors for death.11 Furthermore, an extended CPB time or ACC time also tended to aggravate the destruction of blood-cell components, caused severe hemolysis, and increased the burden on the kidneys, resulting in the increased accumulation of lactic acid, aggravated acidosis, and abnormal coagulation function, thereby increasing the risk of bleeding in important organs. Moreover, a long CPB time or ACC time was also more likely to cause lung tissue reperfusion injury,12 and was thus more likely to lead to longer postoperative ventilator support times, a longer ICU stay, an increased risk of lung infection, and increased mortality. In this study, we found that the CPB time and the ACC time were the risk factors of operative early death.
Multiple studies have indicated preoperative obstruction to be associated with postoperative mortality and a recurrent obstruction rate.6,9,13 In the current study, however, the statistical analysis showed no significant relationship between preoperative obstruction and early postoperative death; instead, preoperative maximum pulmonary vein flow rate and maximal pulmonary artery systolic pressure were associated with early postoperative death, ie, the higher the pulmonary vein flow rate, the more obvious the obstruction, the higher the pulmonary artery pressure, and the greater risk of death. Generally, preoperative pulmonary vein obstruction is defined as a maximum pulmonary vein flow rate >1.8 m/s, measured by echocardiography.14 However, studies have shown that even a minor preoperative obstruction, ie, a preoperative pulmonary vein flow rate ≥1.2 m/s, was associated with postoperative recurrent obstruction, even when there was no anatomical stenosis; as such, a pulmonary vein flow rate ≥1.2 m/s can also be used as a predictor for postoperative recurrent obstruction.15 However, according to our study, due to the small number of recurrent postoperative pulmonary vein obstruction (PVO), we cannot explore the relationship between the preoperative pulmonary vein flow velocity with the PVO.
Postoperative pulmonary vein obstruction (PVO) is a serious complication that can occur after TAPVC; typically, this happens within a few months after TAPVC repair and rapidly progresses into pulmonary vein wall-thickening and fibrosis, affecting the long-term survival rate of children.16 Some studies have shown that preoperative pulmonary vein obstruction and mixed TAPVC were associated with the occurrence of postoperative pulmonary vein obstruction.13,17,18 In the present study, there were only two cases of postoperative pulmonary vein obstruction (both were intracardiac types), with an incidence rate of approximately 2.5%.
Due to the small number of cases included in this study, it was impossible to perform statistical analysis of related factors that may have caused postoperative pulmonary vein obstruction. In addition, no obstructions were observed in preoperative ultrasound diagnoses, and one child died of unknown causes after reoperation.
The pathogenesis of PVO remains unclear. Studies have shown that traumatic surgery and micro-obstruction changes will cause cardiac pulmonary vein vasoconstriction, which may cause PVO; furthermore, some patients often evidence postoperative PVO, starting from the anastomotic stoma and extending to the opening of individual pulmonary vein branches, and anastomotic obstruction will subsequently cause pulmonary vein stenosis.19 Pulmonary vein obstruction is closely associated with TAPVC mortality; therefore, preventing the occurrence of PVO can effectively reduce the mortality rate.5 If there are no obvious symptoms of postoperative PVO, progress can be observed through short-term close follow-up. Considering the potential risks of radiation, CT is rarely used in the postoperative follow-up examination of children with TAPVC in the authors’ center. Echocardiography is of diagnostic significance for severe PVO, but the evaluation of progressive pulmonary vein stenosis is often limited using this method. Because multidetector computed tomography can provide three-dimensional images applying multi-angle reconstruction, allowing for good visualization of the pulmonary vein’s anatomy, it can be used as a favorable tool for the diagnosis of PVO.20
Based on recent studies, sutureless surgery can reduce the incidence of PVO compared with traditional surgery.6,18,21 The surgery method was to incise the common trunk of the pulmonary vein and suture the pericardium around the common trunk of the pulmonary vein with the left atrium, thereby avoiding suturing the edge of the pulmonary vein incision. Compared with the irregular suture line at the incision of the common trunk of the pulmonary vein, a single suture surgical method can avoid deformation and reduce the occurrence of PVO.22 In this study, only 2 cases were done by the sutureless surgery, most of the surgeons used a traditional TAPVC repair approach and, as such, it was not possible to compare the effect of a sutureless repair.
The primary limitations of this study are its single-center nature and small sample size. Additionally, the included surgeries were performed by different surgeons; as such, there may have been small deviations in the results.
In conclusion, the infracardiac type of TAPVC, preoperative mechanical ventilation, preoperative maximum pulmonary vein flow velocity, pulmonary arterial pressure, intraoperative cardiopulmonary bypass time and aortic cross-clamp time were all associated with early postoperative death.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Shandong Provincial Hospital affiliated to Shandong First Medical University. This study was conducted in accordance with the declaration of Helsinki. The parent or legal guardian of patients under 18 years of age provided informed consent.
Funding
This study was funded by Key Research and Development Program of Shandong Province (2018GSF118112). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Herlong JR, Jaggers JJ, Ungerleider RM. Congenital Heart Surgery Nomenclature and Database Project: pulmonary venous anomalies. Ann Thorac Surg. 2000;69(4 Suppl):S56–69. doi:10.1016/S0003-4975(99)01237-0
2. Craig JM, Darling RC, Rothney WB. Total pulmonary venous drainage into the right side of the heart; report of 17 autopsied cases not associated with other major cardiovascular anomalies. Lab Invest. 1957;6(1):44–64.
3. Burroughs JT, Edwards JE. Total anomalous pulmonary venous connection. Am Heart J. 1960;59(6):913–931. doi:10.1016/0002-8703(60)90414-2
4. Kogon B, Fernandez J, Shashidharan S, et al. A 30-year experience with mixed-type total anomalous pulmonary venous connection: a word of caution. Cardiol Young. 2017;27(5):870–876. doi:10.1017/S1047951116001414
5. Harada T, Nakano T, Oda S, et al. Surgical results of total anomalous pulmonary venous connection repair in 256 patients. Interact Cardiovasc Thorac Surg. 2019;28(3):421–426. doi:10.1093/icvts/ivy267
6. Shi G, Zhu Z, Chen J, et al. Total anomalous pulmonary venous connection: the current management strategies in a pediatric cohort of 768 patients. Circulation. 2017;135(1):48–58. doi:10.1161/CIRCULATIONAHA.116.023889
7. Lo Rito M, Gazzaz T, Wilder T, et al. Repair type influences mode of pulmonary vein stenosis in total anomalous pulmonary venous drainage. Ann Thorac Surg. 2015;100(2):654–662. doi:10.1016/j.athoracsur.2015.04.121
8. Husain SA, Maldonado E, Rasch D, et al. Total anomalous pulmonary venous connection: factors associated with mortality and recurrent pulmonary venous obstruction. Ann Thorac Surg. 2012;94(3):825–831. doi:10.1016/j.athoracsur.2012.04.026
9. Karamlou T, Gurofsky R, Al Sukhni E, et al. Factors associated with mortality and reoperation in 377 children with total anomalous pulmonary venous connection. Circulation. 2007;115(12):1591–1598. doi:10.1161/CIRCULATIONAHA.106.635441
10. Ross FJ, Joffe D, Latham GJ. Perioperative and anesthetic considerations in total anomalous pulmonary venous connection. Semin Cardiothorac Vasc Anesth. 2017;21(2):138–144. doi:10.1177/1089253216672012
11. Wu Y, Fan X, Chen L, et al. Emergency surgical treatment of total anomalous pulmonary venous connection. J Card Surg. 2022;37(1):47–52. doi:10.1111/jocs.16079
12. Curran RD, Mavroudis C, Backer CL, et al. Inhaled nitric oxide for children with congenital heart disease and pulmonary hypertension. Ann Thorac Surg. 1995;60(6):1765–1771. doi:10.1016/0003-4975(95)00812-8
13. Seale AN, Uemura H, Webber SA, et al. Total anomalous pulmonary venous connection: morphology and outcome from an international population-based study. Circulation. 2010;122(25):2718–2726. doi:10.1161/CIRCULATIONAHA.110.940825
14. Ricci M, Elliott M, Cohen GA, et al. Management of pulmonary venous obstruction after correction of TAPVC: risk factors for adverse outcome. Eur J Cardiothorac Surg. 2003;24(1):28–36. doi:10.1016/S1010-7940(03)00180-5
15. White BR, Ho DY, Faerber JA, et al. Repair of total anomalous pulmonary venous connection: risk factors for postoperative obstruction. Ann Thorac Surg. 2019;108(1):122–129. doi:10.1016/j.athoracsur.2019.02.017
16. Hickey EJ, Caldarone CA. Surgical management of post-repair pulmonary vein stenosis. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2011;14(1):101–108. doi:10.1053/j.pcsu.2011.01.007
17. Mueller C, Dave H, Prêtre R. Primary correction of total anomalous pulmonary venous return with a modified sutureless technique. Eur J Cardiothorac Surg. 2013;43(3):635–640. doi:10.1093/ejcts/ezs376
18. Honjo O, Atlin CR, Hamilton BCS, et al. Primary sutureless repair for infants with mixed total anomalous pulmonary venous drainage. Ann Thorac Surg. 2010;90(3):862–868. doi:10.1016/j.athoracsur.2010.05.007
19. Kato H, Fu YY, Zhu J, et al. Pulmonary vein stenosis and the pathophysiology of ”upstream” pulmonary veins. J Thorac Cardiovasc Surg. 2014;148(1):245–253. doi:10.1016/j.jtcvs.2013.08.046
20. Yoshimura N, Fukahara K, Yamashita A, et al. Current topics in surgery for isolated total anomalous pulmonary venous connection. Surg Today. 2014;44(12):2221–2226. doi:10.1007/s00595-014-0877-5
21. Azakie A, Lavrsen MJ, Johnson NC, et al. Early outcomes of primary sutureless repair of the pulmonary veins. Ann Thorac Surg. 2011;92(2):666–671. doi:10.1016/j.athoracsur.2011.04.024
22. Yanagawa B, Alghamdi AA, Dragulescu A, et al. Primary sutureless repair for ”simple” total anomalous pulmonary venous connection: midterm results in a single institution. J Thorac Cardiovasc Surg. 2011;141(6):1346–1354. doi:10.1016/j.jtcvs.2010.10.056
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.