Back to Journals » Infection and Drug Resistance » Volume 16
The Clinical Characteristics, Diagnostic Methods, Treatment, and Outcomes of Listeria monocytogenes Meningoencephalitis: A Case Series Study from China
Received 30 May 2023
Accepted for publication 14 September 2023
Published 27 September 2023 Volume 2023:16 Pages 6375—6383
DOI https://doi.org/10.2147/IDR.S423568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Dongrui Li,1 Hui Li2
1Department of Neurology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou City, People’s Republic of China; 2Department of Respiratory Medicine, The First Affiliated Hospital of Zhengzhou University, Zhengzhou City, People’s Republic of China
Correspondence: Hui Li, Tel +86 0371-66271332, Email [email protected]
Background: Listeria monocytogenes meningoencephalitis (LMM) is a rare but dangerous infection of the nervous system. This study intends to summarize and discuss the clinical features, diagnostic methods, treatment, and outcomes.
Methods: LMM patients treated in the First Affiliated Hospital of Zhengzhou University from June 2013 to December 2022 were retrospectively studied. The clinical data, magnetic resonance imaging (MRI), biochemical and hematological parameters, pathogen tests, treatments, and outcomes information were collected and summarized.
Results: Ten LMM patients were enrolled in this study. Three were female and seven were male, with a mean age of 54.5 years old. Seven (70%) of the patients had chronic conditions that either affected the liver (1 case), heart (1 case), or immune system (5 cases). The main clinical manifestations were fever (100%), headache, (60%), and disturbance of consciousness (60%). Out of the nine patients taken MRI, enhanced magnetic resonance imaging was observed with cerebral parenchyma and meningeal enhancement in 3 patients, whereas six patients showed non-specific abnormal signals and brain edema. Seven (70%) patients were positive for L. monocytogenes by bacterial culture and five patients were positive by further next-generation sequencing (NGS) test in CSF. All patients were treated with antibiotics based on antibiotic sensitivity tests or experience, with seven (70%) improved but three (30%) died within one month.
Conclusion: LMM patients have a high mortality rate. Considering the time and reliability of NGS reports, it would be better to identify L. monocytogenes infection in the CSF than bacterial culture. While, after diagnosis, giving timely and appropriate antibiotics would still be a challenge to achieve good outcomes.
Keywords: Listeria monocytogenes, meningoencephalitis, next-generation sequencing, antibiotics, outcome
Introduction
Listeria monocytogenes (L. monocytogenes) infection, also called Listeriosis, has been listed as one of the major foodborne diseases by the World Health Organization due to its high rate of hospitalization, intensive care unit (ICU) admission, and mortality.1 L. monocytogenes affects mostly old people with immunodeficiency, newborns, or pregnant women. The case-fatality risk ranges from 20% to 30%.2–4
Patients with underlying illnesses, immunotherapeutic medication use, or compromised cellular immunity are at risk for developing meningoencephalitis from L. monocytogenes, as so-called Listeria monocytogenes meningoencephalitis (LMM).5 The clinical manifestations of LMM are usually atypical, thus interfering with diagnosis6 and affecting the course of treatment.
Central nervous system infection may cause severe consequences. Timely and correct antibiotic medication is essential for an ideal therapeutic treatment. Empirically, Broad-spectrum antibiotics that can pass through the blood–brain barrier, such as vancomycin and meropenem, could be adequate for killing both gram-positive and negative bacteria.7 Cephalosporin is another type of broad-spectrum antibiotic that is commonly used for infections, especially when the meninges are affected. It is more important to choose or switch the antibiotics immediately after the pathogen and antimicrobial susceptibility test is known, especially when empiric treatment is ineffective. As gram-positive bacteria, Listeria monocytogenes exhibit natural resistance to most cephalosporin antibiotics. Thus, when treating infections induced by Listeria, the antibiotics commonly chosen are ampicillin or gentamicin, but not cephalosporin.
Miao et al compared mNGS and culture, using plasma, sputum and bronchoalveolar lavage fluid from patients with infectious diseases. The authors found that the sensitivity and specificity of mNGS for diagnosing infectious disease were 50.7% and 85.7%, respectively, and these values outperformed those of culture. Although many pathogens were detected, Lm was not detectable in this study.8 Yao et al reported 3 cases of Listeria encephalitis, relying on the detection of Lm in CSF by NGS, from whom the CSF yielded negative by culture.9 Similarly, other LMM cases were diagnosed with this approach.10,11 In all these studies, samples were collected for bacterial cultures directly, while the DNAs were extracted for NGS tests. Although small cases were included, these reports indicate a promising approach for a better way in LMM diagnosis.
Clinically, the diagnosis of LMM relies on detecting of L. monocytogenes in cerebrospinal fluid (CSF), with a bacteria culture test. However, the sensitivity of this test might be an issue, especially for the cases that are still in the early stage or have already received antibiotic treatment. Increased usage of the Next-generation sequencing (NGS) methodology has been observed for the identification of bacterial and viral infections in recent years, which theoretically is more sensitive for the early diagnosis of LMM. So far, only a few instances with distinct NGS diagnoses have been reported.8–11
Due to the rarity of the illness, few studies focused on the prognosis-predicting factors of LMM. Still, it has been reported that age, solid-organ malignancy, cardiovascular disease, liver disease, immunosuppression and sepsis were independent mortality risk factors for Listeriosis,12,13 which are highly linked with the risk factor of developing LMM. Furthermore, Lim et al reported that patients with delayed antibiotic therapy and fatal underlying disease were related to increased mortality of LMM.14
Here, we presented the demographic information, clinical characteristics, imaging findings, treatment and outcomes of 10 adult LMM patients from a single medical center. With a focus on the diagnosis approaches and antibiotics usage strategies.
Materials and Methods
Patient and Grouping
Patients with LMM were enrolled from June 2013 to December 2022 at the First Affiliated Hospital of Zhengzhou University (Figure 1) A bacterial culture or NGS detection of L. monocytogenes in cerebral fluid met the inclusion diagnostic criteria.5,10 Ten patients with complete baseline data were eventually included in the study. The study was approved by First Affiliated Hospital of Zhengzhou University’s Ethics Committee (approval no. 2021-KY-0951-002). All the participants provided written informed consent prior to enrollment.
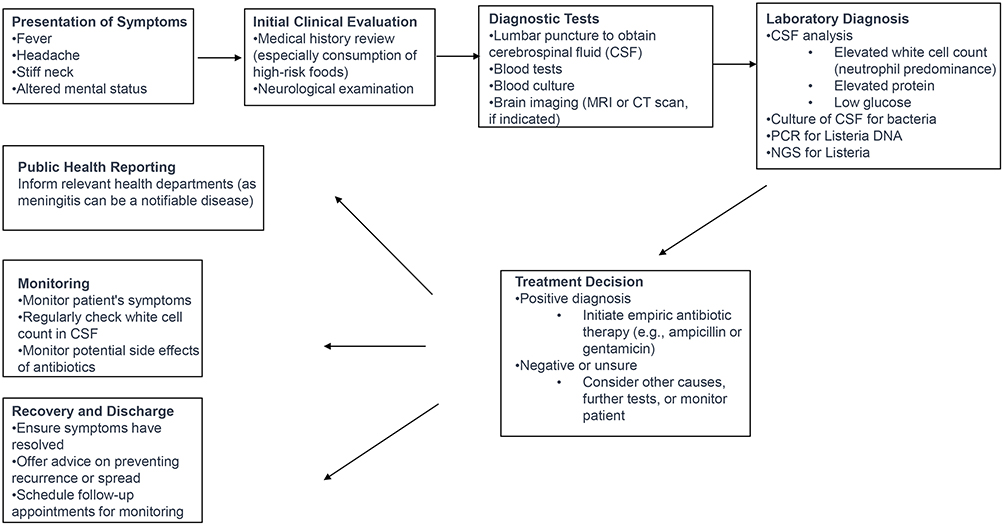 |
Figure 1 Flowchart for the diagnosis and treatment of Listeria meningitis. |
Data Collection
The medical record department of the First Affiliated Hospital of Zhengzhou University collected basic information, medical history, and examination information for each patient. The main statistical data included demographic information, clinic features, magnetic resonance imaging (MRI), laboratory tests (CSF bacteria culture and NGS, drug sensitivity test results), treatment, and outcome.
All patients’ bacteria culture (ten patients) were tested in the microbiology laboratory following the Clinical and Laboratory Standards Institute guideline (Bacterial Culture and Identification: Once samples are collected, they are inoculated onto a nutrient-rich medium. After observing the growth of the bacteria, the VITEK 2 compact automatic microbiological identification instrument is employed for precise identification and antibiotic sensitivity testing). Under culture conditions at 37°C, Listeria monocytogenes typically forms visible colonies on blood agar or chocolate agar within 24–48 hours. However, in some instances, especially with clinical samples, a longer period, such as 72 hours or more, might be required to detect bacteria at low concentrations. For samples taken directly from patients, like cerebrospinal fluid or blood, especially if a Listeria infection is suspected, it is generally recommended to maintain the culture for at least 5 days to ensure sufficient time for bacterial growth.
The NGS results were tested by high-throughput Measurement platform of Henan Gene Hospital, the First Affiliated Hospital of Zhengzhou University. Cerebrospinal fluid (CSF) samples are collected using strict aseptic techniques while avoiding blood contamination. Specimens should be stored aseptically, free from disinfectants and preservatives, uncontaminated, well-sealed, and in transparent material, and transported under cold chain conditions. The mNGS testing process includes specimen handling, nucleic acid extraction, library preparation, sequencing, data processing, sequence alignment, removal of human sequences, microbial annotation, and reporting. The entire testing system has a comprehensive quality control scheme and parameters. The pathogenic microbial database used for alignment and annotation should be as complete, precise as possible, and regularly updated. It is essential to validate the analytical performance of the testing process to ensure the accuracy of the reported results.
Results
Demographic Data and Clinical Features
Ten LMM patients were included in this study (Table 1). Three were female and seven were males, with a mean age of 54.5 years old (ranging from 36 to 70 years old). Seven (70%) of the patients had chronic conditions that either affected the liver (1 case), heart (1 case), or immune system (5 cases). Three predominant clinical symptoms were fever (100%), headache (60%) and disturbance of consciousness (60%).
 |
Table 1 Demographic Data and Clinical Characteristics of Listeria Meningoencephalitis |
Imaging Features
Six patients have non-specific abnormal signals and brain edema in cranial MRI, which may be complicated with hydrocephalus. Three cases showed with cerebral parenchyma and meningeal enhancement on enhanced MRI. All imaging findings indicate intracranial infection; the representative results are shown in Figure 2.
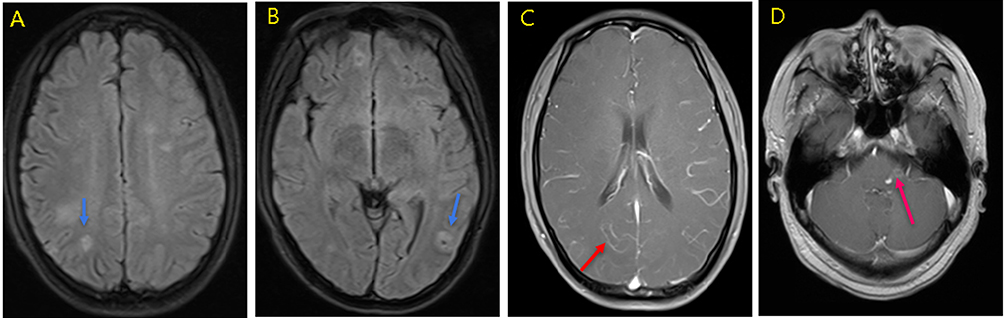 |
Figure 2 MRI results before treatment as representative of meningoencephalitis. (A and B) Blue arrow: Multiple abnormal signals can be seen in the brain of the same patient (Patient 6, T2 flair). (C) Red arrow (Patient 9, contrast-enhanced MRI brain imaging, T2 flair): Linear enhancement can be seen. (D) Red arrow (Patient 10, contrast-enhanced MRI brain imaging, T2 flair): Circular enhancement around the lesion. |
L. monocytogenes Detection in Blood and Cerebrospinal Fluid, Treatments, and Outcomes
All 10 patients underwent cerebrospinal fluid bacterial culture testing. Seven tested positive, and 3 tested negative. Those who tested negative underwent further examination, and the NGS (CSF) revealed positivity for Listeria monocytogenes. Among the 7 patients who tested positive, 2 also underwent NGS testing and the results were positive (Table 2 and Figure 3). Besides the CSF test, eight patients underwent blood bacteria culture test and one NGS. Three patients’ blood samples showed L. monocytogenes growth, of which two were negative by bacteria culture but positive by NGS in CSF.
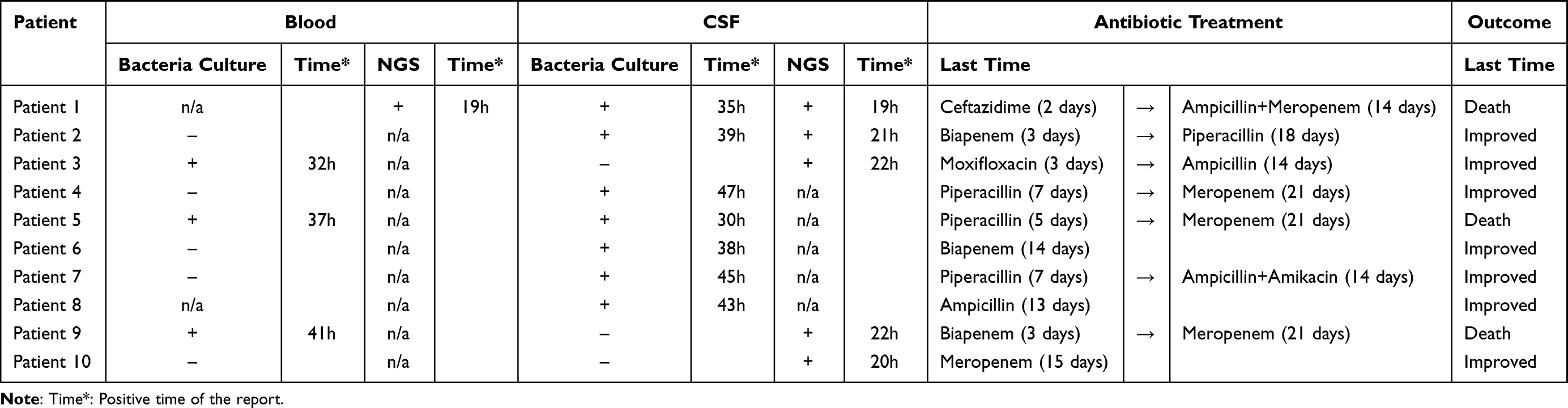 |
Table 2 Individual Patient’s Bacterial Culture and NGS Test Results, Antibiotic Treatment and Outcome |
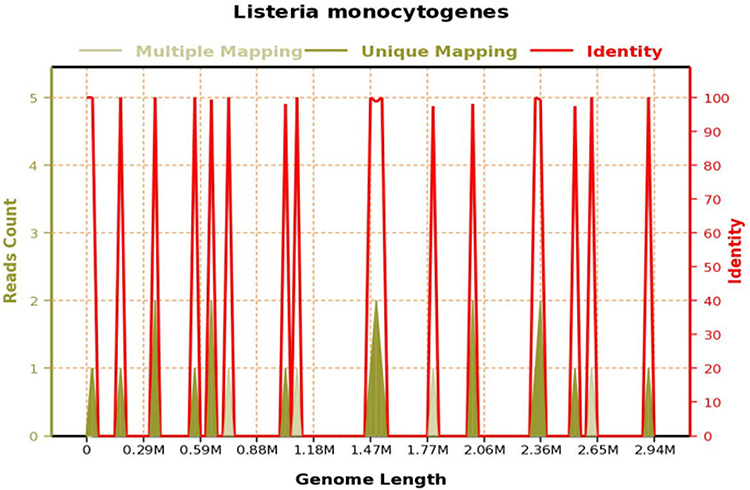 |
Figure 3 Genome coverage map of Listeria monocytogenes (patient 1): The total base number of this species sequence is 1725 (bp), and the total length of this species sequence is 1589 (bp). The coverage is 0.053965%, and the average depth is 1.090X. |
In terms of the report time, it can be seen that NGS (next-generation sequencing) detection methods are mostly completed within 24 hours (19h ~ 22h), in contrast to bacterial culture, which is typically concentrated around 48 hours (30h ~ 47h). This greatly reduces the detection time, and more conducive for patients to change their treatment plan. Moreover, in the cerebrospinal fluid test of the patient 1 and patient 2, Listeria monocytogenes was simultaneously detected by both NGS and bacterial culture, confirming the accuracy of each method.
Penicillin G, amikacin, ampicillin, Meropenem, and sulfamethoxazole were all shown to be effective against L. monocytogenes in vitro drug sensitivity tests in 5 patients. In the actual clinical practice, different antibiotics were applied empirically first, and the treatments were adapted to sensitive antibiotics when no improved observed after the drug sensitivity tests (Table 2, Patients 2–4, Patient 9) or switched to other antibiotics based on experience if not sensitivity test available (Table 2, Patient 1, Patient 5, and Patient 7). During the medical treatment process, patients who passed away had complex conditions. In the early stages of treatment, bacterial meningitis was suspected, and empirical drug treatment was applied. After receiving the bacterial culture results for cases 2, 3, 4, 8, and 9, cases 2 and 3 switched to penicillin-based medications. Case 8 was empirically treated with penicillin-based medication, so no change in medication was made. Patients in cases 4 and 9 had infections in other organs, thus carbapenem drugs were chosen for treatment.7 patients improved after the treatment while 3 patients passed away within 4 weeks after the admission. Respiratory failure was the ultimate factor in the deaths of all patients.
Discussion
Listeria monocytogenes infection is thought to be the most severe food infection illness because of high pathogenicity, and high fatality.15 In this current study, we reported 10 patients with LMM, 70% of them had chronic conditions linked with the risk factors previously reported.12–14 Only 30% of the patients showed abnormality in MRI. Notably, 50% cases were diagnosed based on the NGS, which might be missed by traditional bacteria culture. Although with antibiotics usage according to the antimicrobial susceptibility test, 30% cases passed away within one month of admission.
L. monocytogenes is an intracellular conditional pathogen that once individuals infected, the clearance of the bacteria mostly relies on T-cell-based cellular immunity.16 So patients with cellular immunodeficiency have high risk to get infected.17 About 68% of adult patients with LMM have immune system-related disease,18 similar findings were showed in the current study. This study identified no pregnant cases, which was in conformity with the previous results that pregnancy-related LMM is uncommon.5
Bacterial culture is the gold standard for diagnosing L. monocytogenes infection. However, this approach is time-consuming and insensitive, especially when applying to CSF culture.19,20 Particular polymerase chain reaction (PCR) has been recommended to identify viral encephalitis.21 However, the application of PCR for detecting L. monocytogenes in the central nervous system has not gained widespread acceptance in China.22 Sample-to-answer turnaround time for PCR is usually less than twelve hours, and it depends on the causative agent’s identity. In order to test different uncommon infections, Specific PCR poses challenges.23 In order to identify microorganisms and get beyond the constraints of focused molecular diagnostic techniques, NGS has been developed.8 A prospective multicenter study has shown that NGS is more effective and precise in detecting central nervous system infections than conventional bacterial cultures.20 Additionally, with the advancement of technology, the time it takes for NGS to produce findings can be cut in half to just two days.23 In theory, many types of central nervous system infections can be identified, which can be applied to diagnose patients with critical and complex infections.24–26 In this study, L. monocytogenes infection was considered to be intracranial because L. monocytogenes was discovered following application based on NGS but was not detected in the bacterial culture of cerebral fluid in three patients. Regardless of the great sensitivity, NGS also has certain limits that clinicians should interpret the results cautiously.
In practical sample testing, especially in complex samples, the purification and enrichment of target bacterial DNA is crucial for enhancing detection sensitivity, even when constrained by the number of bacteria present in the original sample. Due to variations in sequencing platforms, library preparation methods, and sample complexity, more starting material might sometimes be required. When employing metagenomic methods, particular attention must be given to its sensitivity, specificity, and reproducibility of measurement, as these elements restrict its application range. Standardization of the metagenomic workflow, including bioinformatics processing, is essential and requires validation. This not only contributes to the accuracy of microbial monitoring models but also ensures their consistency in a globalized context.27
Timely and correct antibiotic usage is essential to cure the disease.28 Mostly, treatments are selected based on antibiotic sensitivity tests or experience. Cephalosporins are naturally resistant by L. monocytogenes, the first therapeutic option is either ampicillin or penicillin.29 Vancomycin and sulfonamides are options for patients who are allergic to penicillin.30,31 Meropenem was chosen empirically or when the patients did not respond to the other antibiotics used at the beginning. However, all the 3 patients who passed away switched to meropenem in the last stage. It was consistent with other studies, which may indicate an inadequate empiric antibiotic therapy and the definitive therapy with meropenem could not reverse the course of the disease anymore.32
This study has several limitations: 1) As a retrospective study, descriptive data was ported and discussed as the core of the current study, a strict methods comparison is needed in detecting L. monocytogenes to reveal the sensitivity and specificity of NGS.
Conclusion
LMM patients have a high mortality rate. Considering the time and reliability of NGS reports, it would be better to identify L. monocytogenes infection in the CSF than bacterial culture. While, after diagnosis, giving timely and appropriate antibiotics would still be a challenge to achieve good outcomes.
Data Sharing Statement
Raw genome sequences have been uploaded into EMBL database with accession number is PRJEB61774.
Acknowledgments
The authors would like to thank the microbiology laboratory in the First Affiliated Hospital of Zhengzhou University and the High-throughput Measurement platform of Henan Gene Hospital for their laboratory technical assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Rebagliati V, Philippi R, Rossi M, Troncoso A. Prevention of foodborne listeriosis. Indian J Pathol Microbiol. 2009;52(2):145–149. doi:10.4103/0377-4929.48903
2. Kashish Soni DK, Mishra SK, Prakash R, Dubey SK, Dubey SK. Label-free impedimetric detection of Listeria monocytogenes based on poly-5-carboxy indole modified ssDNA probe. J Biotechnol. 2015;200:70–76. doi:10.1016/j.jbiotec.2015.02.025
3. Mateus T, Silva J, Maia RL, Teixeira P. Listeriosis during pregnancy: a public health concern. ISRN Obstet Gynecol. 2013;2013:851712. doi:10.1155/2013/851712
4. Soni DK, Singh KM, Ghosh A, Chikara SK, Joshi CG, Dubey SK. Whole-genome sequence of listeria monocytogenes strains from clinical and environmental samples from Varanasi, India. Genome Announc. 2015;3(1). doi:10.1128/genomeA.01496-14
5. Clauss HE, Lorber B. Central nervous system infection with Listeria monocytogenes. Curr Infect Dis Rep. 2008;10(4):300–306. doi:10.1007/s11908-008-0049-0
6. Fan Z, Xie J, Li Y, Wang H. Listeriosis in mainland China: a systematic review. Int J Infect Dis. 2019;81:17–24. doi:10.1016/j.ijid.2019.01.007
7. Schneider F, Gessner A, El-Najjar N. Efficacy of vancomycin and meropenem in central nervous system infections in children and adults: current update. Antibiotics. 2022;11:2.
8. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
9. Yao M, Zhou J, Zhu Y, et al. Detection of listeria monocytogenes in CSF from three patients with meningoencephalitis by next-generation sequencing. J Clin Neurol. 2016;12(4):446–451. doi:10.3988/jcn.2016.12.4.446
10. Lan ZW, Xiao MJ, Guan YL, Zhan YJ, Tang XQ. Detection of Listeria monocytogenes in a patient with meningoencephalitis using next-generation sequencing: a case report. BMC Infect Dis. 2020;20(1):721. doi:10.1186/s12879-020-05447-z
11. Zhang X, Wang R, Luo J, Xia D, Zhou C. Detection of meningoencephalitis caused by Listeria monocytogenes with ischemic stroke-like onset using metagenomics next-generation sequencing: a case report. Medicine. 2021;100(31):e26802. doi:10.1097/MD.0000000000026802
12. Maertens De Noordhout C, Devleesschauwer B, Maertens De Noordhout A, et al. Comorbidities and factors associated with central nervous system infections and death in non-perinatal listeriosis: a clinical case series. BMC Infect Dis. 2016;16:256. doi:10.1186/s12879-016-1602-3
13. Scobie A, Kanagarajah S, Harris RJ, et al. Mortality risk factors for listeriosis - A 10 year review of non-pregnancy associated cases in England 2006–2015. J Infect. 2019;78(3):208–214. doi:10.1016/j.jinf.2018.11.007
14. Lim S, Chung DR, Kim YS, et al. Predictive risk factors for Listeria monocytogenes meningitis compared to pneumococcal meningitis: a multicenter case-control study. Infection. 2017;45(1):67–74. doi:10.1007/s15010-016-0939-2
15. Poulsen KP, Czuprynski CJ. Pathogenesis of listeriosis during pregnancy. Anim Health Res Rev. 2013;14(1):30–39. doi:10.1017/S1466252312000242
16. Aguilar-Bultet L, Nicholson P, Rychener L, et al. Genetic separation of listeria monocytogenes causing central nervous system infections in animals. Front Cell Infect Microbiol. 2018;8:20. doi:10.3389/fcimb.2018.00020
17. Pagliano P, Arslan F, Ascione T. Epidemiology and treatment of the commonest form of listeriosis: meningitis and bacteraemia. Infez Med. 2017;25(3):210–216.
18. Amaya-Villar R, Garcia-Cabrera E, Sulleiro-Igual E, et al. Three-year multicenter surveillance of community-acquired Listeria monocytogenes meningitis in adults. BMC Infect Dis. 2010;10:324. doi:10.1186/1471-2334-10-324
19. Acewicz A, Witkowski G, Rola R, Ryglewicz D, Sienkiewicz-Jarosz H. An unusual presentation of Listeria monocytogenes rhombencephalitis. Neurol Neurochir Pol. 2017;51(2):180–183. doi:10.1016/j.pjnns.2016.12.004
20. Xing XW, Zhang JT, Ma YB, et al. Metagenomic next-generation sequencing for diagnosis of infectious encephalitis and meningitis: a large, prospective case series of 213 patients. Front Cell Infect Microbiol. 2020;10:88. doi:10.3389/fcimb.2020.00088
21. Tunkel AR, Glaser CA, Bloch KC, et al. The management of encephalitis: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. 2008;47(3):303–327. doi:10.1086/589747
22. Infante-Urrios A, Bunuel-Adan F, Gazquez-Gomez G, Ortiz de la Tabla-Ducasse V. Meningitis por Listeria monocytogenes: diagnostico mediante PCR multiplex. Enferm Infecc Microbiol Clin. 2018;36(1):61–62. doi:10.1016/j.eimc.2017.03.007
23. Brown JR, Bharucha T, Breuer J. Encephalitis diagnosis using metagenomics: application of next generation sequencing for undiagnosed cases. J Infect. 2018;76(3):225–240. doi:10.1016/j.jinf.2017.12.014
24. Goldberg B, Sichtig H, Geyer C, Ledeboer N, Weinstock GM. Making the leap from research laboratory to clinic: challenges and opportunities for next-generation sequencing in infectious disease diagnostics. mBio. 2015;6(6):e01888–15. doi:10.1128/mBio.01888-15
25. Westblade LF, van Belkum A, Grundhoff A, et al. Role of clinicogenomics in infectious disease diagnostics and public health microbiology. J Clin Microbiol. 2016;54(7):1686–1693. doi:10.1128/JCM.02664-15
26. Lusk RW. Diverse and widespread contamination evident in the unmapped depths of high throughput sequencing data. PLoS One. 2014;9(10):e110808. doi:10.1371/journal.pone.0110808
27. Ko K, Chng KR, Nagarajan N. Metagenomics-enabled microbial surveillance. Nat Microbiol. 2022;7(4):486–496. doi:10.1038/s41564-022-01089-w
28. Karakitsos D, Samonis G, Georgountzos V, Karabinis A. Fulminant listerial infection of the central nervous system in an otherwise healthy patient: a case report. J Med Case Rep. 2009;3:7383. doi:10.4076/1752-1947-3-7383
29. Lorber B. Listeriosis. Clin Infect Dis. 1997;24(1):1–9; quiz 10–1. doi:10.1093/clinids/24.1.1
30. Prieto M, Martinez C, Aguerre L, Rocca MF, Cipolla L, Callejo R. Antibiotic susceptibility of Listeria monocytogenes in Argentina. Enferm Infecc Microbiol Clin. 2016;34(2):91–95. doi:10.1016/j.eimc.2015.03.007
31. Obaidat MM, Bani Salman AE, Lafi SQ, Al-Abboodi AR. Characterization of Listeria monocytogenes from three countries and antibiotic resistance differences among countries and Listeria monocytogenes serogroups. Lett Appl Microbiol. 2015;60(6):609–614. doi:10.1111/lam.12420
32. Thonnings S, Knudsen JD, Schonheyder HC, et al. Antibiotic treatment and mortality in patients with Listeria monocytogenes meningitis or bacteraemia. Clin Microbiol Infect. 2016;22(8):725–730. doi:10.1016/j.cmi.2016.06.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.