Back to Journals » Infection and Drug Resistance » Volume 16
The Challenging Path to Diagnosing Extraintestinal Amoebiasis: A Case Report of an HIV-Infected Patient
Authors Li X, Chen C, Tong L, Gao Q, Chen W, Zhou G ![]() , Tong Z, Wang W
, Tong Z, Wang W ![]()
Received 19 October 2023
Accepted for publication 28 November 2023
Published 8 December 2023 Volume 2023:16 Pages 7569—7574
DOI https://doi.org/10.2147/IDR.S442075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaofeng Li,1,* Cha Chen,1,* Luyuan Tong,1 Qun Gao,1 Wenxian Chen,2 Guangde Zhou,3 Zhaowei Tong,1 Weihong Wang1,4
1Department of Infectious Diseases, Huzhou Central Hospital, Affiliated Central Hospital Huzhou University, Huzhou, Zhejiang Province, People’s Republic of China; 2Department of Ultrasonography, Huzhou Central Hospital, Affiliated Central Hospital Huzhou University, Huzhou, Zhejiang Province, People’s Republic of China; 3Department of Pathology, Affiliated Beijing You An Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Huzhou Key Laboratory of Precision Medicine Research and Translation for Infectious Diseases, Huzhou, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weihong Wang, Email [email protected]
Background: Amoebiasis, an infectious disease caused by the parasitic protozoan E. histolytica, is easily misdiagnosed due to its declining incidence and atypical symptoms.
Case Presentation: A 31-year-old male presented to the hospital with dyspnea and inability to lie flat. Imaging studies indicated a large amount of pleural effusion on the right side and multiple huge cysts in the liver. The patient underwent liver tumor resection surgery at another hospital due to suspected malignancy, but no evidence of relevant malignant tumors was found in the pathological examination. Subsequently, we performed metagenomic next-generation sequencing on the liver drainage fluid and obtained liver pathology slides from the hospital where the surgery was performed at that time. Both of them confirmed the diagnosis of amoebic infection. Empirical treatment with metronidazole was initiated before the diagnosis was confirmed, along with symptomatic treatments such as thoracic drainage and liver drainage. Eventually, the patient’s condition improved and he was discharged smoothly.
Conclusion: In order to avoid misdiagnosis of amoebiasis, thoroughly inquiring about the patient’s medical history, shifting perspectives and continuing investigating are necessary when one diagnostic approach proves ineffective. Besides, interdisciplinary collaboration and persistent efforts are crucial for accurate diagnosis.
Keywords: amebiasis, amoebic abscess, diagnosis, HIV, metagenomic next-generation sequencing, metronidazole
Background
Amoebiasis, an infectious disease caused by the parasitic protozoan Entamoeba histolytica (E. histolytica), is primarily transmitted through the oral ingestion of food or water contaminated with mature cysts.1 The etiological agent of this disease was first described by a Russian physician in 1975.2 The term “Entamoeba histolytica” was formally coined in 1903, reflecting its distinctive capacity to induce tissue dissolution.3 Amoebiasis exhibits a higher prevalence in developing countries, particularly those characterized by inadequate sanitation facilities, and is prominently endemic in regions of Asia, Africa, and Latin America. Conversely, in developed nations, the disease primarily affects individuals returning from or with a history of travel to endemic areas.2,4–6 Besides, traveler’s E. histolytica infection has also been frequently reported in MSM in developed nations.6
The majority of amoebiasis patients remain asymptomatic as the pathogenic E. histolytica colonizes the host’s intestines without producing noticeable symptoms.7 However, a small percentage of individuals may experience mild to severe diarrhea, accompanied by abdominal pain and watery or bloody stools.8 These clinical manifestations lack specificity, leading to potential misdiagnosis or missed diagnoses. Additionally, due to the ability of trophozoites to disseminate through the venous system, extra-intestinal amoebic diseases can occur, including amoebic liver abscess, amoebic lung abscess, and amoebic brain abscess.1,9–11 Amoebic liver abscess is the most frequent extraintestinal complication of E. histolytica.12 Approximately 2% to 5% of patients with intestinal amoebiasis develop liver abscesses.13 Patients with amoebic liver abscess will have fever and right upper abdominal pain after abscess formation. When there is pleuropulmonary involvement, amebic liver abscesses can be associated with cough, right lower lung dullness, or crackles in the right lung.14 Herein, we present a case of a human immunodeficiency virus (HIV)-positive patient with concurrent extraintestinal amoebiasis. The arduous and intricate diagnostic and therapeutic journey of this case deserves careful analysis and reflection.
Case Presentation
In early May, 2023, a 31-year-old male was brought to our hospital by an ambulance due to chest tightness and difficulty breathing. The patient had undergone liver surgery one month ago. He was an HIV-infected patient who had been on long-term oral antiviral therapy. Besides, he enjoyed eating raw food regularly.
Upon admission, the patient presented with shortness of breath, low-grade fever, and decreased blood oxygen saturation. Additionally, physical examination revealed his emaciated appearance, absence of breath sounds in the right lung, and tenderness in the liver area. The routine laboratory tests indicated an elevation in white blood cell count, neutrophil percentage, and high-sensitivity C-reactive protein. Additionally, the lymphocyte percentage and hemoglobin level were found to be low. The HIV-1 ribonucleic acid (RNA) quantity was less than 20 copies/mL, T and B lymphocyte subset analysis showed cluster of differentiation 4 (CD4) lymphocyte percentage of 18% [normal range, (27–510%)] and CD4/CD8 ratio of 0.42 [normal range, 0.63–3.49].
Additional examinations: Chest computed tomography (CT) showed a large amount of pleural effusion on the right side (Figure 1A). Closed thoracic drainage was performed and dark red turbid fluid was extracted. The pleural fluid was sent for different examinations, including polymerase chain reaction (PCR) for mycobacterium tuberculosis deoxyribonucleic acid (DNA) and metagenomic next-generation sequencing (mNGS), but no valuable results were found. Abdominal ultrasound showed a cystic mass measuring 19.3×16.5cm in the right lobe of the liver. Percutaneous drainage was performed for the liver abscess and a jam-like turbid fluid was extracted (Figure 1B). Bacterial and fungal cultures of the liver abscess fluid and pleural fluid were negative. We also performed bone marrow aspiration and biopsy, and no specific blood-related diseases were found.
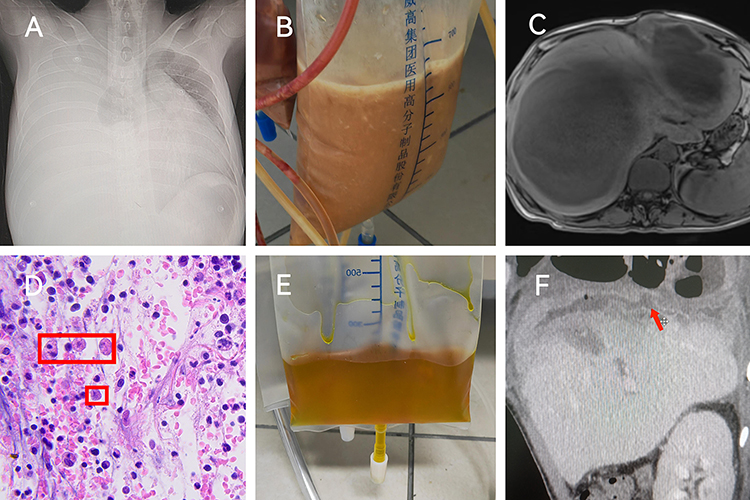 |
Figure 1 (A) Chest computed tomography (CT) showed a large amount of pleural effusion on the right side before treatment. (B) The features of the drainage fluid from liver abscess showing a milk-chocolate brown or a jam color before treatment. (C) Abdominal enhanced MRI showed a large solid cystic mass in the liver. (D) HE×200 Pathological section of liver tissue and in the red box is the amoeba trophozoite. (E) The drainage fluid from the liver abscess became clear and reduced after treatment. (F) Abdominal CT showed rupture of the right diaphragm, and the thoracic cavity was connected to the abdominal cavity as indicated by the red arrow. |
In September, 2022, the patient was admitted to Beijing You An Hospital due to massive lower gastrointestinal bleeding. At that time, the patient experienced acute diarrhea, starting with blood in the stool and eventually progressing to direct rectal bleeding, leading to a sharp decrease in hemoglobin levels to 30g/L. However, no significant abnormalities were found during gastrointestinal endoscopy examination. The patient was separated from the critical condition after receiving symptomatic support treatment such as blood transfusion and rehydration, but then he was in an anemia state. In March, 2023, the patient was hospitalized in the same hospital in Beijing due to abdominal enlargement. A contrast-enhanced abdominal magnetic resonance imaging (MRI) indicated solid cystic masses with tumor-like characteristics (Figure 1C). The positron emission tomography-computed tomography (PET-CT) scan indicated liver masses, possibly malignant. On March 28, 2023, a laparoscopic resection of the cystic mass in the left lobe of the liver was performed. However, the pathological examination did not reveal evidence of malignancy. Following discharge, the patient’s overall condition progressively deteriorated, progressing to a life-threatening state within a short span of one month.
Taking into account the patient’s medical history, we began to search for alternative explanations. Later, we sent the liver abscess fluid for mNGS detection. It reported sequence reads of amoeba trophozoites (specific sequence reads: 81). Simultaneously, we actively cooperated with Beijing You An Hospital where the patient had undergone liver cystic mass resection, recommending additional testing on the liver tissue. The final pathological feedback confirmed the presence of amoeba trophozoites in the tissue (Figure 1D). As a result, the patient’s diagnosis was determined as amoebic liver abscess, amoebic pulmonary abscess, and concurrent HIV infection.
Due to the severity of the patient’s condition, although the diagnosis was not yet confirmed, we empirically administered intravenous infusion of metronidazole sodium chloride injection at a dose of 0.5g q8h, which was adjusted to 0.5g q6h two days later. Gradually, the drainage fluid from the chest and liver became clear and reduced (Figure 1E). And chest CT showed that the amount of pleural effusion was significantly lower than before. After 32 days of hospitalization, the patient’s condition stabilized. He was discharged with instructions for regular outpatient follow-up visits and medication to consolidate the treatment.
Discussion
In recent years, with the development of the Chinese economy and improvements in healthcare conditions, amoebiasis has shown sporadic outbreaks and a gradual decrease in incidence.15 This is the first reported case of amoebiasis in the past 15 years in Huzhou City, Zhejiang Province. However, on a global scale, the incidence of invasive amoebic infection has been increasing among HIV/acquired immune deficiency syndrome (AIDS) patients.6,16 HIV infection leads to immune dysfunction, which is a significant risk factor for acquiring invasive amoebic infection.16–18 Additionally, several studies have indicated a higher proportion of invasive amoebic infection among men who have sex with men, suggesting that sexual transmission and increased fecal-oral contact in this population contribute to the spread of invasive amoebiasis.19,20 The patient we reported had a history of HIV infection for three years and had been on long-term antiviral therapy. Although the viral replication level was not high, the CD4 lymphocyte count remained low, indicating immune deficiency in the patient and making them susceptible to amoebic infection. Detailed questioning revealed that the patient was not a male homosexual and had not engaged in unsafe sexual activities since being diagnosed with HIV infection. The patient’s preference for consuming raw seafood may be the primary cause of their invasive amoebic infection.
The most common manifestations of amoebic colitis include abdominal pain, watery or bloody diarrhea, with severe rectal bleeding being uncommon.21–23 However, there have been reported cases with complaints of diarrhea and rectal bleeding.24,25 Our patient experienced acute lower gastrointestinal bleeding in September, 2022. Considering the patient’s current condition, we suspect that the episode at that time could have been a case of amoebic colitis with concurrent acute lower gastrointestinal bleeding. However, the patient sought initial treatment at another hospital and did not undergo further examinations. Therefore, it remains merely a reasonable conjecture.
Amoebic lung abscess often occurs as a complication of amoebic liver abscess and can occur through various pathways such as diaphragmatic penetration, hepatic-bronchial fistula, lymphatic spread, and hematogenous dissemination. The most common route of transmission is when an amoebic liver abscess ruptures, allowing direct entry into the pleural space through the diaphragm, resulting in secondary amoebic lung abscess and possibly concurrent diaphragmatic rupture.26–29 Toshinobu Yokoyama et al reported a case of a dyspneic patient in whom an amoebic liver abscess directly invaded the thoracic cavity through the diaphragm.30 Tomohiro Yazawa et al reported a case of a right basal bronchial fistula caused by amoebic infection.31 Our patient was primarily admitted to our hospital due to respiratory distress. Upon confirming the presence of a significant amount of pleural effusion, we promptly performed thoracentesis for drainage. Surprisingly, a few days after the thoracic drainage, we observed through ultrasound that the size of the right hepatic abscess had reduced compared to admission. This gave us a hint that diaphragmatic rupture might have occurred. After the right hepatic abscess ruptured, the pus drained into the pleural cavity through the ruptured diaphragm. As the patient’s overall condition slightly improved, we also performed percutaneous aspiration of the liver abscess. During the aspiration, gas was extracted, suggesting a possible communication between the abdominal and thoracic cavities. Subsequently, this hypothesis was confirmed by contrast-enhanced abdominal CT scan (Figure 1F), indicating the presence of diaphragmatic rupture. Combined with the purulent drainage fluid from the liver abscess, these details further strengthened our suspicion of amoebic infection in the patient, providing additional support for the empirical use of metronidazole before the definitive diagnosis.
Due to the atypical symptoms of amoebic disease, misdiagnosis and missed diagnosis are common occurrences. Fu et al reported a case of an amoebic lung and pleural patient who was misdiagnosed with tuberculous pleurisy and unfortunately passed away due to delayed treatment.32 The severity of our patient’s condition upon admission to the hospital was primarily due to the lack of a definitive diagnosis. From the initial gastrointestinal bleeding to the subsequent presence of a massive liver abscess, the true underlying cause of the patient’s condition remained unidentified. Even after the patient underwent liver abscess resection surgery, the histopathological examination only revealed the presence of significant acute and chronic inflammatory cells and tissue aggregation. The delay in the patient’s diagnosis was attributed to multiple factors. On one hand, auxiliary examinations such as PET-CT and contrast-enhanced abdominal MRI indicated the possibility of a malignant tumor, leading the medical team to focus their efforts in that direction. On the other hand, without obtaining a definitive diagnosis, there was a failure to shift the approach and continue the search for the underlying cause, resulting in the patient’s condition deteriorating day by day. Within 10 days of the patient’s admission to our hospital, empirical treatment was initiated. We persistently searched for the cause and confirmed the diagnosis of amoeba infection after two weeks of hospitalization, which saved the patient’s life and bought a chance for his subsequent recovery.
Cases involving amoebic infection affecting multiple organs simultaneously are relatively rare in recent years. However, due to the compromised immune system in HIV-positive patients, the incidence of amoebic infection is higher. Clinicians should consider the possibility of amoebic infection and conduct targeted investigations when encountering such patients to avoid treatment delays.
Conclusion
Due to the atypical symptoms of amoebic disease, misdiagnosis and missed diagnosis are common occurrences. It is crucial to thoroughly inquire about the patient’s medical history. If a patient has immunocompromised diseases, we should consider the possibility of infection with parasites such as amoeba and try to identify it. When one diagnostic approach proves ineffective, it is necessary to shift perspectives and continue investigating. Besides, interdisciplinary collaboration and persistent efforts are crucial for accurate diagnosis.
Data Sharing Statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of Huzhou Central Hospital (Approval No: 202307011-01).
Consent for Publication
Written informed consent was provided by the patient for the publication of the case details and images. Details of the case can be published without institutional approval.
Acknowledgments
Many thanks for works by the staffs in the infectious ward from the Huzhou Central Hospital and the support of the public welfare application research project of Zhejiang Science and Technology Department (No. LGF22H190006). In addition, the pathological section of the liver in this paper was from the Department of Pathology, Beijing You An Hospital. We sincerely thank them for the assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the public welfare application research project of Zhejiang Science and Technology Department (No. LGF22H190006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kantor M, Abrantes A, Estevez A, et al. Entamoeba histolytica: updates in clinical manifestation, pathogenesis, and vaccine development. Can J Gastroenterol Hepatol. 2018;2018:4601420. doi:10.1155/2018/4601420
2. Carrero JC, Reyes-López M, Serrano-Luna J, et al. Intestinal amoebiasis: 160 years of its first detection and still remains as a health problem in developing countries. Int J Med Microbiol. 2020;310(1):151358. doi:10.1016/j.ijmm.2019.151358
3. Pinilla AE, López MC, Viasus DF. History of the Entamoeba histolytica protozoan. Rev Med Chil. 2008;136(1):118–124. doi:10.4067/S0034-98872008000100015
4. Li J, Cui Z, Li X, Zhang L. Review of zoonotic amebiasis: epidemiology, clinical signs, diagnosis, treatment, prevention and control. Res Vet Sci. 2021;136:174–181. doi:10.1016/j.rvsc.2021.02.021
5. Ximénez C, Morán P, Rojas L, Valadez A, Gómez A. Reassessment of the epidemiology of amebiasis: state of the art. Infect Genet Evol. 2009;9(6):1023–1032. doi:10.1016/j.meegid.2009.06.008
6. Shirley D-AT, Farr L, Watanabe K, Moonah S. A review of the global burden, new diagnostics, and current therapeutics for amebiasis. Open Forum Infect Dis. 2018;5(7):ofy161. doi:10.1093/ofid/ofy161
7. Haque R, Huston CD, Hughes M, Houpt E, Petri WA. Amebiasis. N Engl J Med. 2003;348(16):1565–1573. doi:10.1056/NEJMra022710
8. Nagaraja S, Ankri S. Target identification and intervention strategies against amebiasis. Drug Resist Updat. 2019;44:1–14. doi:10.1016/j.drup.2019.04.003
9. Roediger R, Lisker-Melman M. Pyogenic and amebic infections of the liver. Gastroenterol Clin North Am. 2020;49(2):361–377. doi:10.1016/j.gtc.2020.01.013
10. Cheepsattayakorn A, Cheepsattayakorn R. Parasitic pneumonia and lung involvement. Biomed Res Int. 2014;2014:874021. doi:10.1155/2014/874021
11. Victoria-Hernández JA, Ventura-Saucedo A, López-Morones A, et al. Case report: multiple and atypical amoebic cerebral abscesses resistant to treatment. BMC Infect Dis. 2020;20(1):669. doi:10.1186/s12879-020-05391-y
12. Stanley SL. Amoebiasis. Lancet. 2003;361(9362):1025–1034. doi:10.1016/S0140-6736(03)12830-9
13. Arellano-Aguilar G, Marín-Santillán E, Castilla-Barajas JA, Bribiesca-Juárez MC, Domínguez-Carrillo LG. A brief history of amoebic liver abscess with an illustrative case. Rev Gastroenterol Mex. 2017;82(4):344–348. doi:10.1016/j.rgmx.2016.05.007
14. Lübbert C, Wiegand J, Karlas T. Therapy of Liver Abscesses. Viszeralmedizin. 2014;30(5):334–341. doi:10.1159/000366579
15. Zheng J, Zhang N, Shen G, et al. Spatiotemporal and seasonal trends of class A and B notifiable infectious diseases in china: retrospective analysis. JMIR Public Health Surveill. 2023;9:e42820. doi:10.2196/42820
16. Huang SH, Tsai MS, Lee CY, et al. Ongoing transmission of Entamoeba histolytica among newly diagnosed people living with HIV in Taiwan, 2009–2018. PLoS Negl Trop Dis. 2020;14(6):e0008400. doi:10.1371/journal.pntd.0008400
17. Watanabe K, Nagata N, Sekine K, et al. Asymptomatic intestinal amebiasis in Japanese HIV-1-infected individuals. Am J Trop Med Hyg. 2014;91(4):816–820. doi:10.4269/ajtmh.14-0278
18. Lin P, Ko WC, Lin WC, Li MC. Liver abscess caused by coexisting Salmonella enteritidis and Entamoeba histolytica in a HIV-infected patient. J Microbiol Immunol Infect. 2019;52(5):836–837. doi:10.1016/j.jmii.2018.05.006
19. Salit IE, Khairnar K, Gough K, Pillai DR. A possible cluster of sexually transmitted Entamoeba histolytica: genetic analysis of a highly virulent strain. Clin Infect Dis. 2009;49(3):346–353. doi:10.1086/600298
20. Hung CC, Chang SY, Ji DD. Entamoeba histolytica infection in men who have sex with men. Lancet Infect Dis. 2012;12(9):729–736. doi:10.1016/S1473-3099(12)70147-0
21. Cooper CJ, Fleming R, Boman DA, Zuckerman MJ. Varied clinical manifestations of amebic colitis. South Med J. 2015;108(11):676–681. doi:10.14423/SMJ.0000000000000370
22. Pehrson PO. Amoebiasis in a non-endemic country. Epidemiology, presenting symptoms and diagnostic methods. Scand J Infect Dis. 1983;15(2):207–214. doi:10.3109/inf.1983.15.issue-2.14
23. Takahashi T, Gamboa-Dominguez A, Gomez-Mendez TJ, et al. Fulminant amebic colitis: analysis of 55 cases. Dis Colon Rectum. 1997;40(11):1362–1367. doi:10.1007/BF02050824
24. Pittman FE, el-Hashimi WK, Pittman JC. Studies of human amebiasis. I. Clinical and laboratory findings in eight cases of acute amebic colitis. Gastroenterology. 1973;65(4):581–587. doi:10.1016/S0016-5085(19)33037-9
25. Rozen P, Baratz M, Rattan J. Rectal bleeding due to amebic colitis diagnosed by multiple endoscopic biopsies: report of two cases. Dis Colon Rectum. 1981;24(2):127–129. doi:10.1007/BF02604301
26. Ackers JP, Mirelman D. Progress in research on Entamoeba histolytica pathogenesis. Curr Opin Microbiol. 2006;9(4):367–373. doi:10.1016/j.mib.2006.06.014
27. Kubitschek KR, Peters J, Nickeson D, Musher DM. Amebiasis presenting as pleuropulmonary disease. West J Med. 1985;142(2):203–207.
28. Ragheb MI, Ramadan AA, Khalil MA. Intrathoracic presentation of amebic liver abscess. Ann Thorac Surg. 1976;22(5):483–489. doi:10.1016/s0003-4975(10)64458-x
29. Shamsuzzaman SM, Hashiguchi Y. Thoracic amebiasis. Clin Chest Med. 2002;23(2):479–492. doi:10.1016/s0272-5231(01)00008-9
30. Yokoyama T, Hirokawa M, Imamura Y, Aizawa H. Respiratory failure caused by intrathoracic amoebiasis. Infect Drug Resist. 2010;3:1–4. doi:10.2147/idr.s8647
31. Yazawa T, Igai H, Kamiyoshihara M, Shirabe K. Right basal bronchial fistula due to amebic infection: a case report. BMC Pulm Med. 2023;23(1):117. doi:10.1186/s12890-023-02412-9
32. Fu B, Wang J, Fu X. A rare case of extraintestinal amebiasis. BMC Infect Dis. 2022;22(1):364. doi:10.1186/s12879-022-07348-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.