")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
The Burden of a Multiple Myeloma Diagnosis on Patients and Caregivers in the First Year: Western European Findings
Authors Gatopoulou X , Iraqi W, Morgan K, Helme K, Spain VA , Redfearn J, Gardiner B
Received 27 April 2022
Accepted for publication 7 November 2022
Published 17 December 2022 Volume 2022:14 Pages 731—753
DOI https://doi.org/10.2147/CEOR.S367458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Xenia Gatopoulou,1 Wafae Iraqi,2 Kate Morgan,3 Kawitha Helme,4 Victoria A Spain,5 Jennifer Redfearn,5 Brett Gardiner5
1Health Economics, Market Access and Reimbursement EMEA, Janssen Pharmaceuticals, Athens, Greece; 2Patient Engagement, Janssen Pharmaceuticals, Issy-les-Moulineaux, France; 3Myeloma Patients Europe, Brussels, Belgium; 4Health Economics, Market Access and Reimbursement EMEA, Janssen Pharmaceuticals, High Wycombe, UK; 5The Research Partnership, London, UK
Correspondence: Wafae Iraqi, Janssen Pharmaceuticals, 1, Rue Camille Desmoulins, TSA 91003, Issy-les-Moulineaux, 92787, France, Email [email protected]
Background: This research aimed to quantify the burden of illness (BoI) in transplant eligible (TE) and transplant non-eligible (TNE) newly diagnosed multiple myeloma (NDMM) patients and their caregivers, in the first year after diagnosis: at months 0, 3, and 12.
Methods: Prospective, cross-sectional, observational NDMM study of TE and TNE patients and their caregivers from France, Germany, Italy, and Spain was conducted between May 2019 and January 2021. A structured, online questionnaire measuring disease burden, direct and costs, out-of-pocket expenses, and health-related quality of life (HRQoL) was used. Descriptive statistics were performed.
Results: A total of 164, 160, and 190 NDMM patients [> 65 years; self-described healthy; not working; living with caregiver] answered at months 0, 3, and 12. Patients lost independence to perform daily activities; mean pain intensity rose and opioid utilization increased, more significantly among TNE patients. Overall health status and HRQoL remained stable. Median 3-month direct medical costs peaked at month 3. Specialist consultations and hospital admissions were the greatest cost amongst TE and TNE patients. Home adaptations increased out-of-pocket expenditures amongst TNE patients. Patients describing themselves as working spent a median 0 hours in the office at all time points. A total of 131, 122, and 124 caregivers answered at months 0, 3, and 12. Mean self-rated burden score rose. By month 12, half of caregivers developed stress, anxiety or depression. Most employed caregivers continued working. Productivity was low at month 0 with a trend of recovering at month 12. Caregivers of TNE compared to TE patients reported greater time burden. Caregivers’ HRQoL was stable over time.
Conclusion: NDMM is burdensome for patients and caregivers in the first year after diagnosis. TNE patients are more dependent on caregivers and incur higher care costs than TE patients. Despite the financial, physical, and emotional burden, HRQoL remains stable possibly indicating resilience and illness adjustment amongst patients and caregivers.
Keywords: burden of illness, costs of disease, newly diagnosed multiple myeloma, health-related quality of life
Background
Multiple myeloma (MM) is a malignant clonal plasma cell proliferative disorder characterized by uncontrolled and progressive increase of monoclonal paraprotein leading to specific end-organ damage.1 The proliferating multiple myeloma cells displace the normal bone marrow, causing dysfunction in normal hematopoietic tissue and destruction of the normal bone marrow architecture.2 MM is an incurable disease associated with significant morbidity and mortality, especially among older adults. It is the second most common hematological malignancy after leukemia.3 Globally, its incidence increased by 126% between 1990 and 2016, and it was the cause of 2.1 million disability-adjusted life-years in 2016.4 Western Europe remains among the world regions with the highest age-standardized incidence rate.4
The daily life and wellbeing of patients with MM can be severely affected by a variety of progressing disease symptoms and treatment‐related adverse events (AEs), such as fatigue, bone pain, nausea, anemia, and diarrhea.5,6 Patients with NDMM experience a substantial reduction in health‐related quality of life (HRQoL) compared with the general population.7,8 There is also a parallel burden experienced by family caregivers of NDMM patients, due to a combination of both uncertainty about the future and a need to adapt to the disease.9,10
The number and type of therapeutic options for NDMM have increased dramatically in recent years and have been associated with large improvements in outcomes for both transplant eligible (TE) and transplant non-eligible (TNE) individuals.11 Despite this, treatment burden (defined as the effect of treatment on the individual patient’s workload and its subsequent impact on his or her well-being and functioning), is substantial, particularly within the first year after diagnosis.12 Additionally, both patients with NDMM and their caregivers face significant losses in productivity, alongside major challenges from disability, employment, health insurance and out-of-pocket costs for treatment for the individuals and their families.13,14
Despite the increasing evidence substantiating the considerable burden of NDMM, it remains unclear how the various aspects of the disease interrelate to the impact on the health and economic outcomes of patients and caregivers, particularly over the first year after diagnosis.15 This study aimed to quantify the burden of illness (BoI) in TE and TNE NDMM patients and their caregivers, at three time points: immediately after diagnosis and before treatment initiation, at 3 months and at 12 months post-diagnosis. The study calculated the direct and indirect costs that the disease and its co-morbidities may generate from the perspective of a large number of NDMM patients and caregivers.
This is the first published BoI study conducted in NDMM patients with a prospective cross-sectional design focused on the twelve months that immediately follow diagnosis. The measurement and analysis of the impact of NDMM on HRQoL and costs can be used to inform allocation of healthcare resources in the context of budget constraints in this MM patient population.
Methods
Design
This study took a prospective, cross-sectional, observational research approach, with findings based on a survey conducted amongst NDMM patients and their caregivers from France, Germany, Italy, and Spain. Qualitative research outputs were used to inform the quantitative questionnaire design used in the survey. The survey consisted of three data collection phases in order to establish the clinical, humanistic and financial burden of NDMM at different points in time after diagnosis, as follows:
- Month 0, as soon as possible after diagnosis and prior to treatment initiation.
- Month 3, three months after diagnosis.
- Month 12, twelve months after diagnosis.
Patients who had relapsed (therefore no longer receiving their first treatment regime) were no longer considered NDMM and were not deemed eligible to participate at remaining time points. A mix of Autologous Stem Cell Transplant (ASCT) eligible (TE) and transplant non-eligible (TNE) patients were included via natural fall-out.
Patients and caregivers were recruited through their hematologist/hemato-oncologist at Month 0 and followed up at 3 months and 12 months. Hematologists/hemato-oncologists who were willing to refer NDMM patients and/or their caregivers to the survey were recruited through an independent online database of validated physicians, who had previously given their permission to be contacted to participate in the research. Each hematologist/hemato-oncologist received a letter explaining the purpose and objectives of the study for themselves and a separate version to give to any potential eligible participant. Participants were given information on data protection and anonymization and on the voluntarily participation in the survey. All respondents signed a consent form. Recruitment was low in Germany, France and Spain due to HCPs being either prevented from participating by hospital policy or being unwilling to refer patients at the point of diagnosis.
The hematologists/hemato-oncologists recruited patients and caregivers until the target sample was reached. To ensure that a minimum number of patients completed all 3 time points and to compensate for any who chose not to continue or were no longer able to participate (for example through death, other health issues or no longer being considered NDMM due to a relapse), additional respondents were also recruited at Months 3 and 12. The survey took place between May 2019 and January 2021.
Criteria Selection
To participate in the survey, all participants met the following inclusion criteria (Table 1):
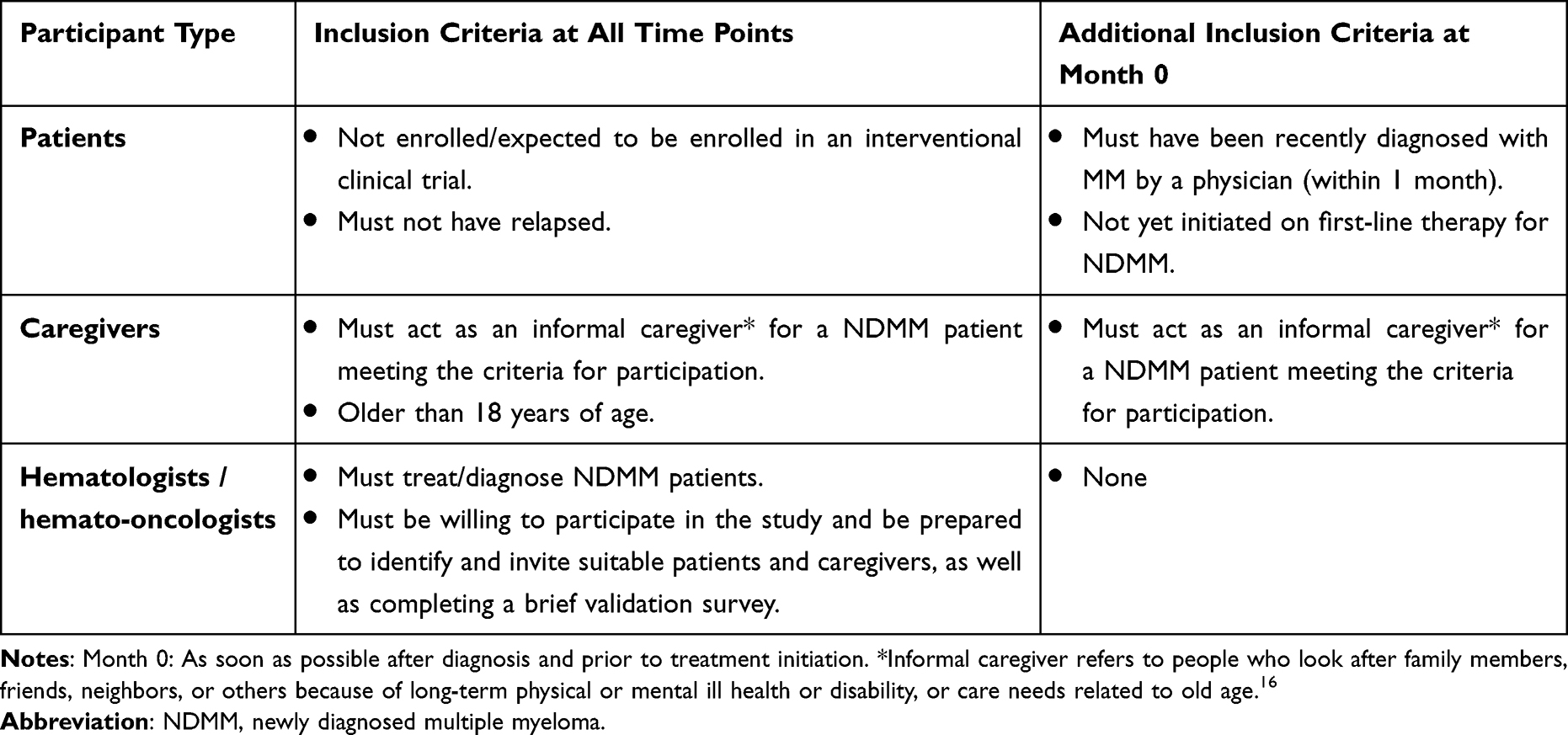 |
Table 1 Study Inclusion Criteria |
Data Collection
Prior to the quantitative research, a series of face-to-face interviews were conducted with 26 patients and 16 caregivers from across the 3 time points (using the same criteria and recruitment approach described above), to ensure the questionnaire approach and options were comprehensive. A semi-structured, online, self-completed questionnaire was then designed, incorporating feedback from the face-to-face interviews, to collect data from hematologists/hemato-oncologists, patients, and caregivers, respectively (Table 2).
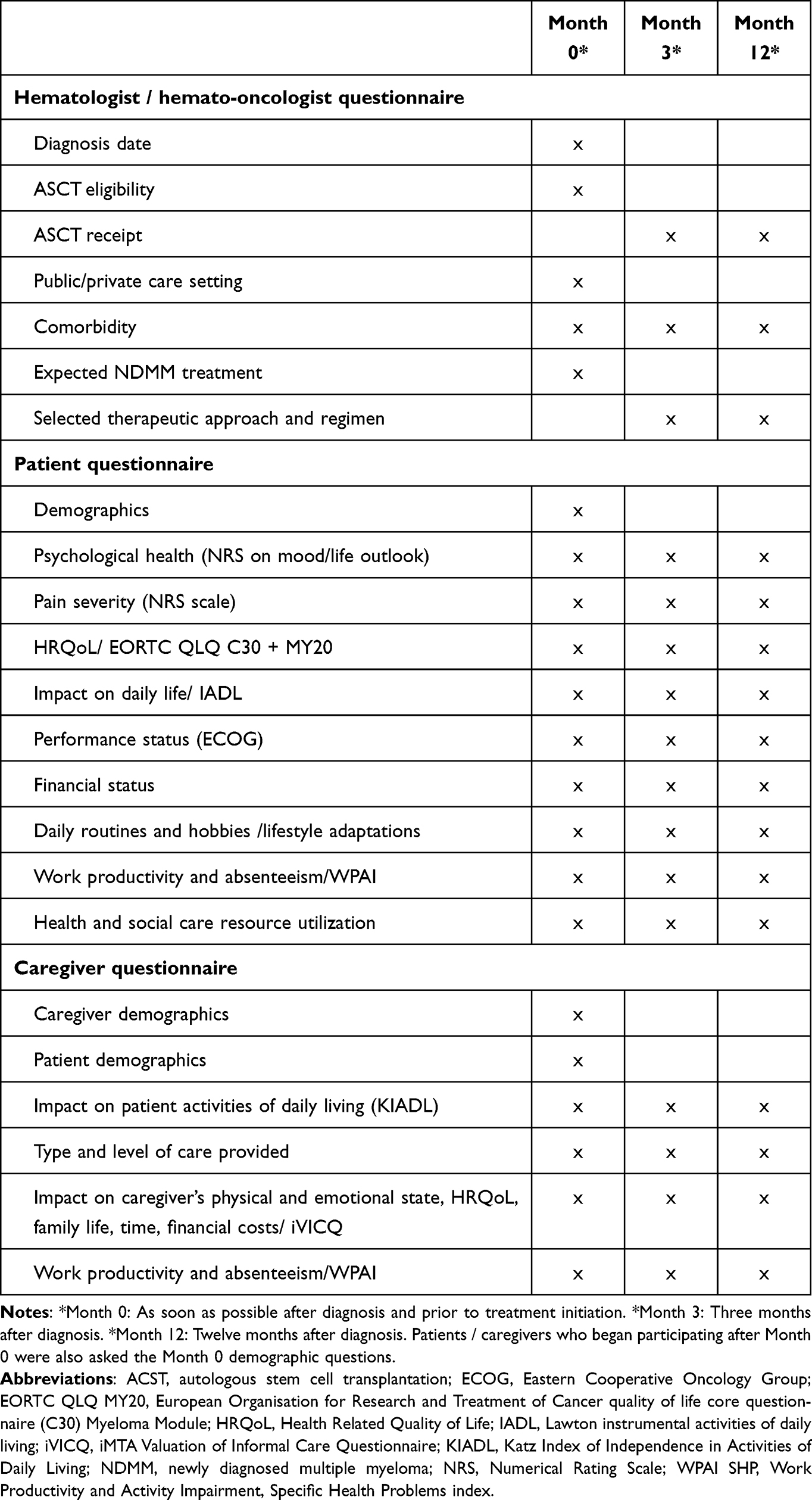 |
Table 2 Summary of Information Collected in the Questionnaire at Each Study Time Point |
The hematologist/hemato-oncologist questionnaire collected information on the date of diagnosis, transplant eligibility status, NDMM treatment (anticipated at Month 0, verified at subsequent time points) and comorbid conditions. The patient and caregiver questionnaires established demographic and financial status, as well as data to calculate direct costs to the healthcare system and community (use of health and social care resources, therapy costs); patient and caregiver out-of-pocket costs [attending appointments, lifestyle adaptations, extra support required (professional and informal)] and HRQoL changes arising from the disease. “Ad hoc” questions and rating scales derived from the face-to-face interviews were developed to collect data on these dimensions, alongside standardized assessments to establish validated outcomes, in order to achieve a comprehensive estimate of NDMM burden at each time point. For patients, the Eastern Cooperative Oncology Group (ECOG) scale of Performance Status,17 the Work Productivity and Activity Impairment: Specific Health Problems index (WPAI: SHP),18 the Lawton instrumental activities of daily living (IADL)19 and the European Organisation for Research and Treatment of Cancer quality of life core questionnaire (EORTC QLQ C30) including the additional Myeloma Module (EORTC QLQ MY20)20,21 were included. Additionally, patients also rated pain severity on a Numerical Rating Scale (NRS). Meanwhile for caregivers, the Katz Index of Independence in Activities of Daily Living,22 the iMTA Valuation of Informal Care Questionnaire,23 and the Work Productivity and Activity Impairment: Specific Health Problems index (WPAI: SHP)18 were included.
Each questionnaire was translated into the local language and proof-read to ensure consistency of meaning with the English-language version. Approved translations and programming checks were included for the EORTC. The questionnaire was self-completed online by NDMM patients and caregivers over 30 minutes at each of the three time points, with support offered via phone or e-mail if required. Respondents were given the opportunity to complete the questionnaire over the telephone or via a pen-and-paper format if preferred.
Patients and caregivers were asked to focus on their own views and opinions in their answers and to complete the questionnaire without any input from their caregivers (for patients), or from the patient they care for (for caregivers). The hematologists/hemato-oncologists were asked to consult the patient’s hospital records to complete the physician’s questionnaire to provide accurate data and were given a one-month period to complete each questionnaire.
All participants were requested to provide these details at each of Months 0, 3 and 12. At Months 3 and 12, hematologists/hemato-oncologists also confirmed the patient status and whether they were still eligible to participate based on the criteria selection defined for this study to track ongoing eligibility (Table 1). Any incomplete data sets were reviewed on a case-by-case basis, to ascertain whether sufficient data had been collected for inclusion in the research.
Data collection for Month 0 took place between May 2019 and March 2020; for Month 3, data was gathered from August 2019 to July 2020, and for Month 12, from June 2020 to January 2021. Part of Month 3 and all of Month 12 questionnaires were completed during the SARS-COV-2 pandemic.
Statistical Analysis
Raw data were aggregated, and descriptive statistics were applied. In order to achieve the research objectives, the study sample was divided into categorical subgroups of patients who were and were not eligible for ASCT (TE and TNE patients, respectively) at each time point. Findings at each time point, as well as differences between time points, were analyzed. Mean, median, mode, minimum and maximum ranges and standard deviation were calculated for numerical values. Mean percentage of patients and/or caregivers selecting each statement or option was calculated for non-numerical responses. Open-ended questions were analyzed qualitatively. “Do not know” or “Not applicable” were excluded and the database revised to include only answered questions. T-tests were used to look at observations from the same individuals [(dependent variables); T-tests (mean scores) or Z-tests (distributions) were used] as well as scores between different sub-groups (independent variables). For each test, the null hypothesis stated that the difference between the paired population means (or between the paired population proportions) was equal to zero. The tests looked at the 95% confidence level. If the p-value was small (<0.05), the null hypothesis was rejected and reported that, at the 95% confidence level, the observed difference was statistically significant. Data were analyzed with QPSMR CL 64 2020.
Calculation of Costs
Costs of NDMM were calculated in €, using publicly available data for each market dated as close to 2019 as possible. The median average cost was calculated per subgroup of patients, caregivers and the healthcare system in each studied country, respectively. Direct, out-of-pocket and indirect costs were established.
Estimates of direct costs were based on the use of the healthcare resource [as reported in the questionnaire by patients, including ambulance call outs; hospital visits (overnight stays, as a day patient, for tests); specialist consultations; consultations with other healthcare providers (such as radiologist, dietician); use of other medical services; use of community services (including professional caregivers, care facilities, social workers)], multiplied by the unit cost of that resource based on publicly available sources, as listed in Table S1. These costs included ambulance call outs, hospital visits (coving overnight stays, as a day patient, for tests), specialist consultations, consultations with other healthcare providers (eg radiologist, dietician), use of other medical services and use of community services (including professional caregivers, care facilities and social workers). The cost of the ASCT and treatments not purchased by the patient were not included in the cost calculations.
Out-of-pocket costs to patients per month were calculated via the median average from the estimates given in the questionnaire for each of a series of expenses, including concomitant medications taken, visiting a physician in private practice, adaptations to home/lifestyle, travel to medical appointments, accommodation close to hospital, family-related costs including unpaid leave and other costs completed via free text questions. Similarly, out-of-pocket costs to caregivers per month were calculated based on expenses reported in the questionnaire, including supporting the patient with household activities, personal care and practical needs, travel and accommodation costs, as well as any other logistical costs associated with supporting the patient (eg, requirement for a cleaner or babysitter within own household, taking unpaid leave).
The calculation of indirect costs was based on the human capital approach to loss of productivity. This validated method takes the patient’s perspective of time lost and does not assume employees are easily replaced.24 Thus, the cost of leaving paid-full time work due to NDMM was calculated for patients and caregivers based on average salary and hours worked per country. The human capital approach is considered particularly relevant in early disease stages, when patients are still working.25
The standardized WPAI: SHP was applied to assess patients’ and caregivers’ working patterns over the past week and to understand any absenteeism and presenteeism related to the condition or caring responsibilities, respectively. As part of this metric, question responses are allocated pre-set scores, to calculate an impairment percentage with higher numbers indicating greater impairment and less productivity.
Results
A total of 164 to 190 NDMM patients and 124 to 131 caregivers took part in the survey for at least one time point (patients: n = 164 at Month 0, n = 160 at Month 3, and n = 190 at Month 12; caregivers: n = 131 at Month 0, n = 122 at Month 3, and n = 124 at Month 12), and 91 NDMM patients and 72 caregivers completed questionnaires at all 3 study time points. Despite a relatively stable completion rate throughout the study, additional respondents were recruited at Month 3 and Month 12 to ensure data availability. Sample sizes vary at each study time point. Table S2 shows the distribution of the sample per participating country at each study time point.
Baseline Characteristics of Participants
The average NDMM patient profile in our study (Month 0) irrespective of transplant eligibility was that of a retired (73%) male (52%), over 65 years old (73%), with at least two co-occurring chronic conditions in addition to MM (70%), such as diabetes or chronic obstructive pulmonary disease; not working (73%); living with the caregiver (75%) and had no children or children were financially independent (89%). Patients self-described themselves as relatively healthy (55%) (Table 3).
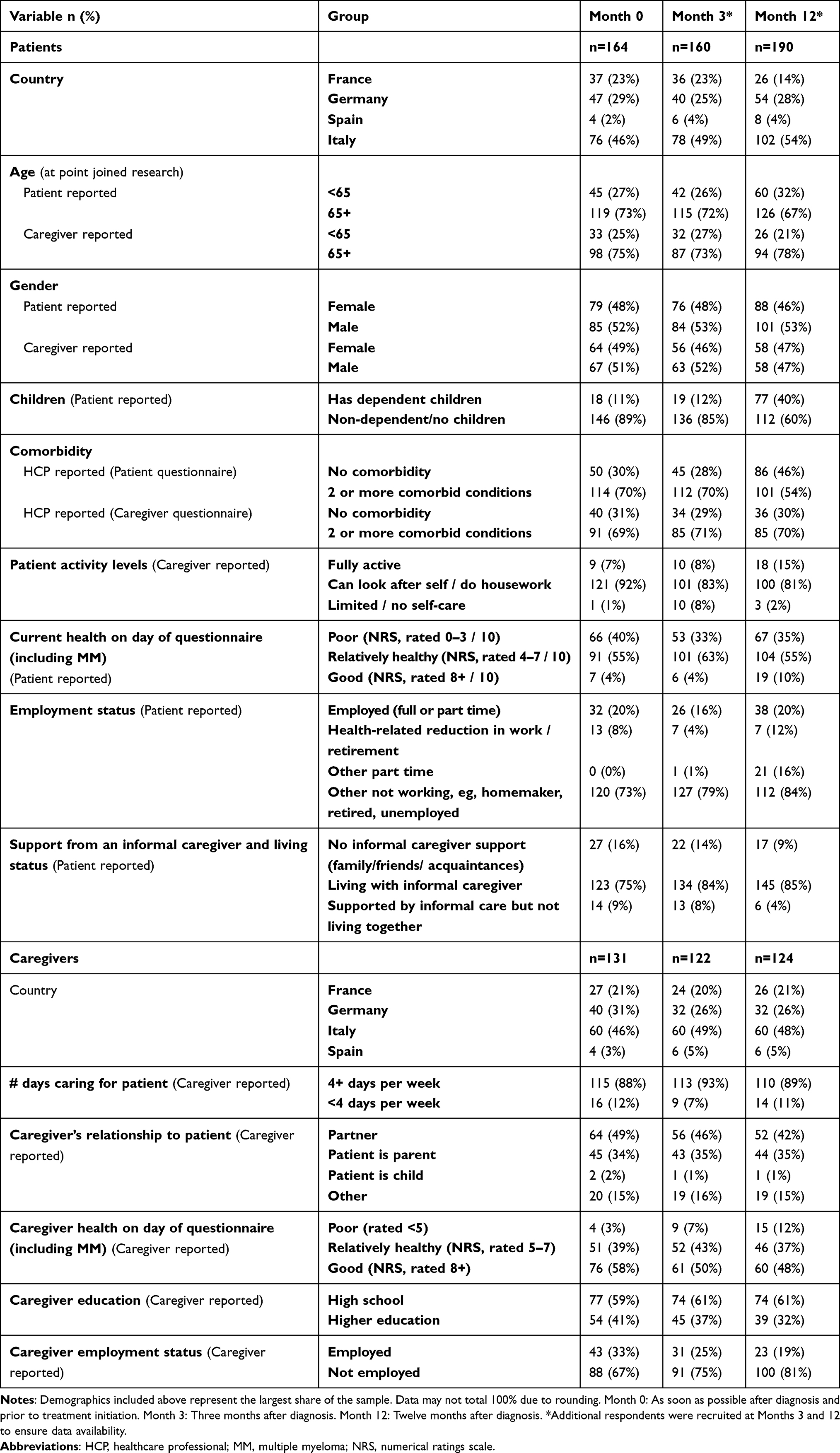 |
Table 3 Baseline Demographic Characteristics of Patients and Caregivers |
Likewise, the average profile of the caregiver in our study was that of a woman (51%) who was either married to the male patient (49%) or was the patient’s adult child (34%). Eighty-two percent shared a household with him or her. Fifty-nine percent had gone to high school and (67%) were not employed. Eighty-eight percent cared for the NDMM patient more than 4 days a week (Table 3).
Treatment Regimes
No quotas were set on transplant eligibility and an equal number of patients in the sample were TE or TNE. Amongst TE patients, bortezomib, cyclophosphamide and dexamethasone (VCd) and bortezomib, lenalidomide and dexamethasone (VRd) were used for induction in 53% and 20% of cases (n = 59), respectively. VCd was the regimen most frequently used in Germany (81%; n = 35), whereas VRd was common in France (44%; n = 9), Italy (44%; n = 9), and Spain (51%; n = 6). Amongst TNE patients, bortezomib, melphalan and prednisolone (VMP) were the regimen most commonly used, accounting for 44%–47% (Month 3, n = 92 and Month 12, n = 98, respectively), particularly in France and Italy. In Germany, VRd and daratumumab, lenalidomide and dexamethasone (DRd) were more frequently used compared to other regimens (Figure S1).
Clinical and Humanistic Burden of NDMM on Patients During the First Year After Diagnosis
Pain and Treatment-Related Symptoms
Overall self-reported mean pain intensity (NRS scale: 0 no pain −10 worst possible pain) was moderate immediately after diagnosis (5.2, Month 0), with a significant improvement at three months (4.7, Month 3) followed by a significant decline at twelve months after diagnosis (5.4, Month 12), though they still considered themselves to be middling on the scale on average. TNE individuals rated their pain higher than TE patients at all study time points (5.3, 4.7 and 5.7 vs 5.0, 4.6, 5.1, respectively) but the trend for improvement at Month 3 was maintained irrespective of transplant eligibility status (Figure 1).
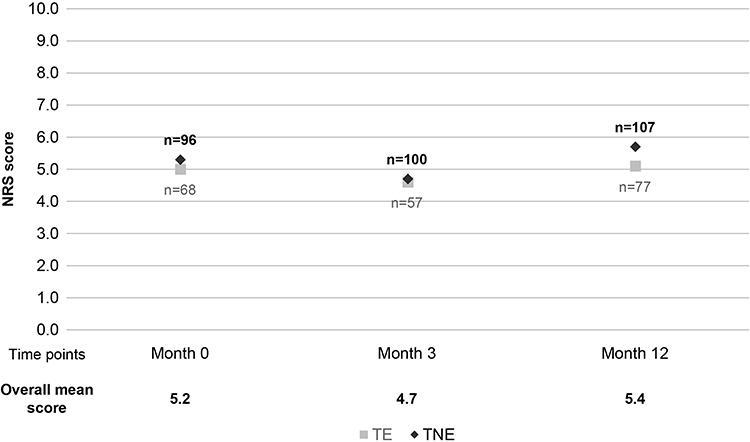 |
Figure 1 Mean self-reported pain intensity in a NRS by TE and TNE NDMM patients at three study time-points. Month 0: As soon as possible after diagnosis and prior to treatment initiation. Month 3: Three months after diagnosis. Month 12: Twelve months after diagnosis. Numeric rating scale (NRS) for pain: Scale of 0 (no pain) to 10 (worst pain imaginable). Patients were asked to select a whole number (0–10 integers) that best reflects the intensity of their pain, with “0” representing no pain and “10” representing worst pain imaginable. The timeframe used was “in the last 24 hours” to capture the pain intensity felt presently by the patient. Patients self-score themselves based on pain extremities experienced. A higher score indicates greater pain intensity. Abbreviations: NRS, numeric rating scale; TNE, transplant non-eligible; TE, transplant eligible. |
In line with changes in pain intensity, NDMM patients were increasingly taking opioids to help manage the pain due to MM as the year progressed. Amongst TE patients, 16% needed opioids at Month 0, tripling to 52% at Month 12. Use of other medications to alleviate pain (including corticosteroids and bisphosphonates) peaked at Month 3 but tailed off by Month 12 when opioid use became more widespread. Amongst TNE patients, 58% required opioids at Month 0, increasing to 78% at Month 12 (Table 4).
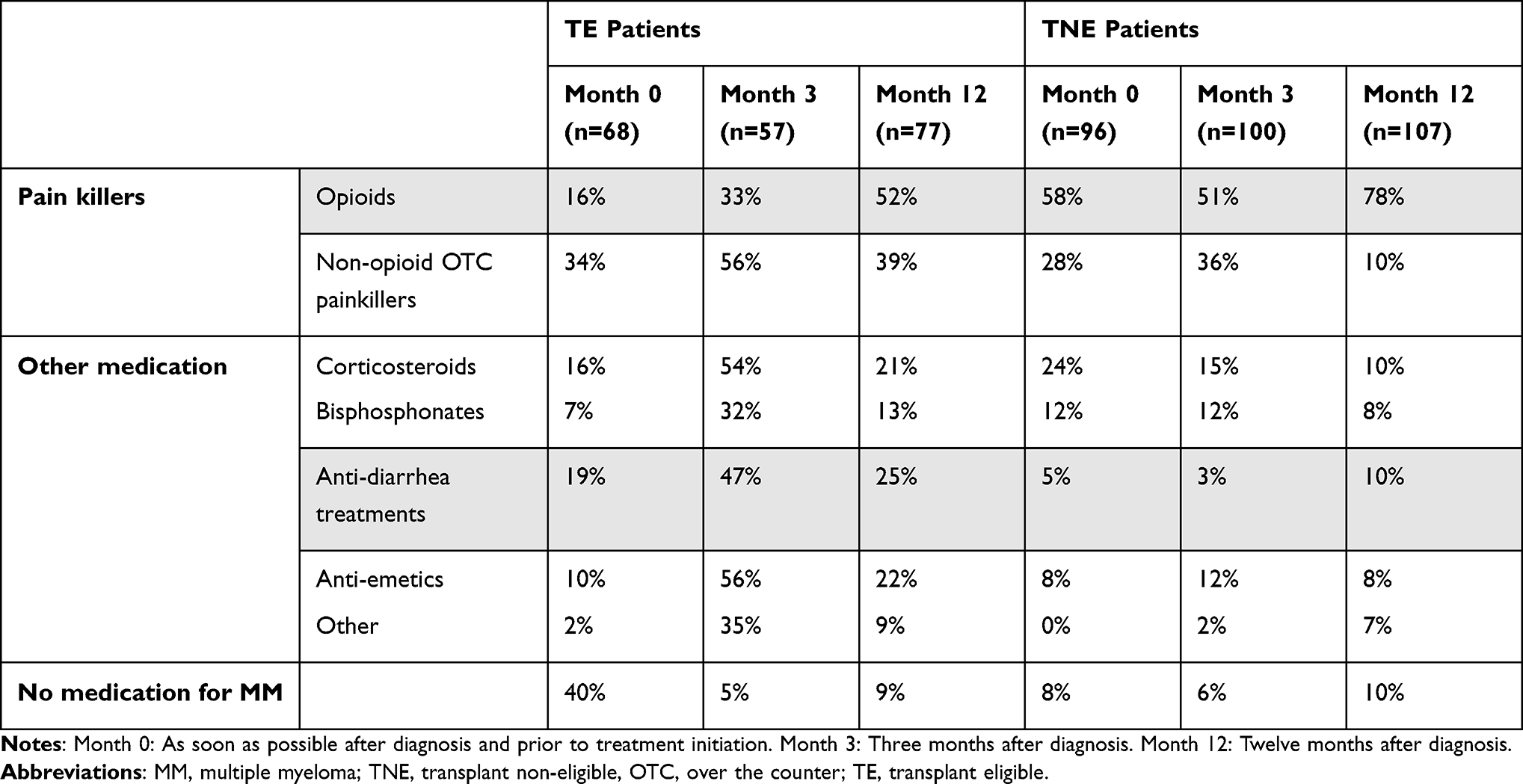 |
Table 4 Medications Taken for Symptoms Management by TE and TNE NDMM Patients at Three Study Time Points |
Consistent with the appearance of treatment-related side-effects, use of anti-diarrhea and anti-emetic medications increased amongst TE patients three months after diagnosis (study Month 3) while use was low amongst TNE individuals at all study time points (Table 4).
Patient Level of Functioning (Performance Status, ECOG)
The share of patients managing without any help declined from 17% at Month 0 to 9% at Month 12 (Table 3). In line with this, there was a decline in patient performance status and activity levels over the course of 12 months, with the share of patients able to work and do light housework but unable to take part in strenuous activity decreasing from 57% (Month 0, ECOG scale) to 43% at Month 12 (Figure 2). This was reflected in a concurrent increase in those who remain active but were now unable to work or to do light activities by the end of the 12 months (34% at Month 0, 45% at Month 12). Deterioration of activity levels was more significant amongst TNE patients compared to TE individuals twelve months after diagnosis (Figure 2A). Caregivers’ judgements of overall health and activity levels were aligned with the patients’ self-assessment (Figure 2B).
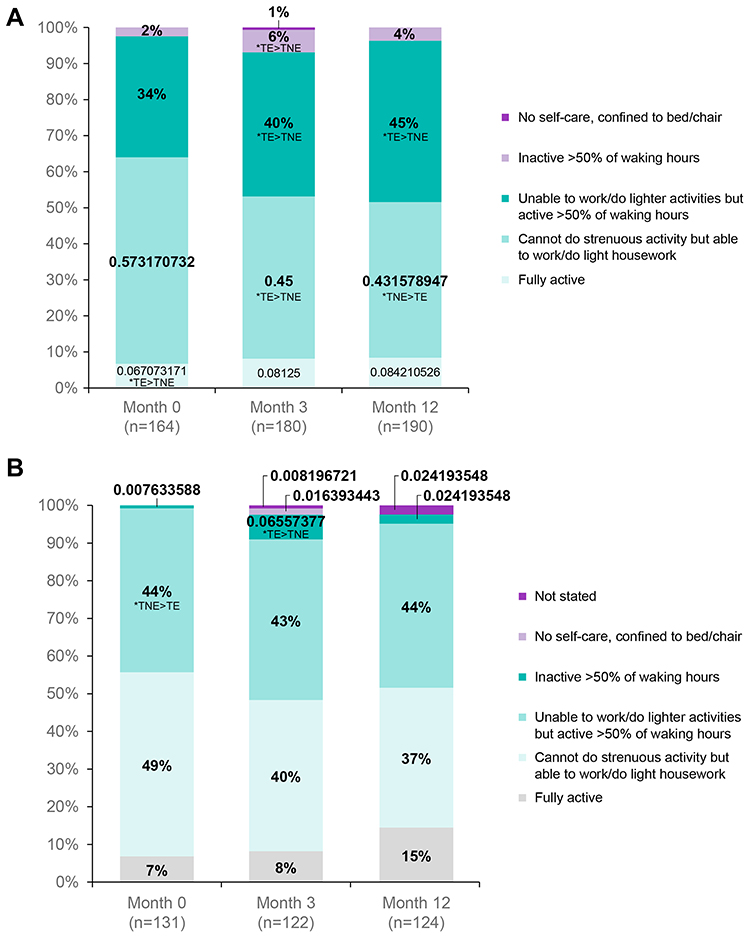 |
Figure 2 Patients (A) and caregivers (B) perspective on TE and TNE NDMM patient performance status at three study time points. Month 0: As soon as possible after diagnosis and prior to treatment initiation. Month 3: Three months after diagnosis. Month 12: Twelve months after diagnosis. How would you describe your (patient questionnaire) / his/her (caregiver questionnaire) current activity levels / ability to carry out day to day activities? 1. Fully active, not restricted in day-to-day activities at all. 2. Cannot do physically strenuous activity but able to work or conduct light housework. 3. Unable to work or conduct any lighter activities, such as housework, but can look after self and active for more than 50% of waking hours. 4. Capable of limited self-care; confined to bed or chair more than half of all waking hours. 5. Cannot carry out any self-care; confined to bed or chair all the time. Statistically significant differences*. |
Overall Health of Patients (Visual Analog Scale – VAS)
Despite this decline in activity, when considering their overall health, the majority of patients maintained a perception of average health status at all study time points (VAS scale of 0 worst possible health to 10 best possible health. “Average” considered to be a rating between 4 and 7, selected by 87%, 88% and 77% at Months 0, 3, and 12 respectively) (Figure 3). Ten percent of patients felt their overall health was good, while 13% considered it poor 12 months after the MM diagnosis.
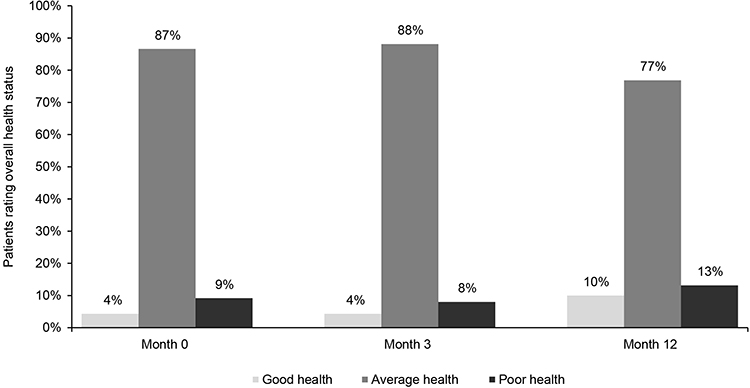 |
Figure 3 TE and TNE NDMM patients self-rating of overall health status at three study time points. Month 0: As soon as possible after diagnosis and prior to treatment initiation. Month 3: Three months after diagnosis. Month 12: Twelve months after diagnosis. Bases unless otherwise stated: Month 0 n=164; Month 3, n=160; Month 12 n=190. We would like to understand how good or bad your health is TODAY? Please place the marker on the scale below, to indicate how your health is TODAY. The “0” means the worst health you could imagine. The “10” means the best health you could imagine. |
Independent Living Ability (IADL)
In line with this decrease in health, ability to live independently also significantly decreased over the 12-month period after diagnosis (determined by the Lawton IADL index), declining from 4.3 at Month 0 to 3.6 at Month 12 [scale 0 (low function, dependent) to 8 (high function, independent)]; (P<0.001). TE patients scored higher than TNE patients on level of independence at all study time points (mean score: 5.4, 4.4 and 4.2 vs 3.5, 3.3 and 3.0, respectively) (Table 5). Unsurprisingly, the share of patients living with their informal caregiver similarly increased from 75% at Month 0 to 85% at Month 12 (Table 3).
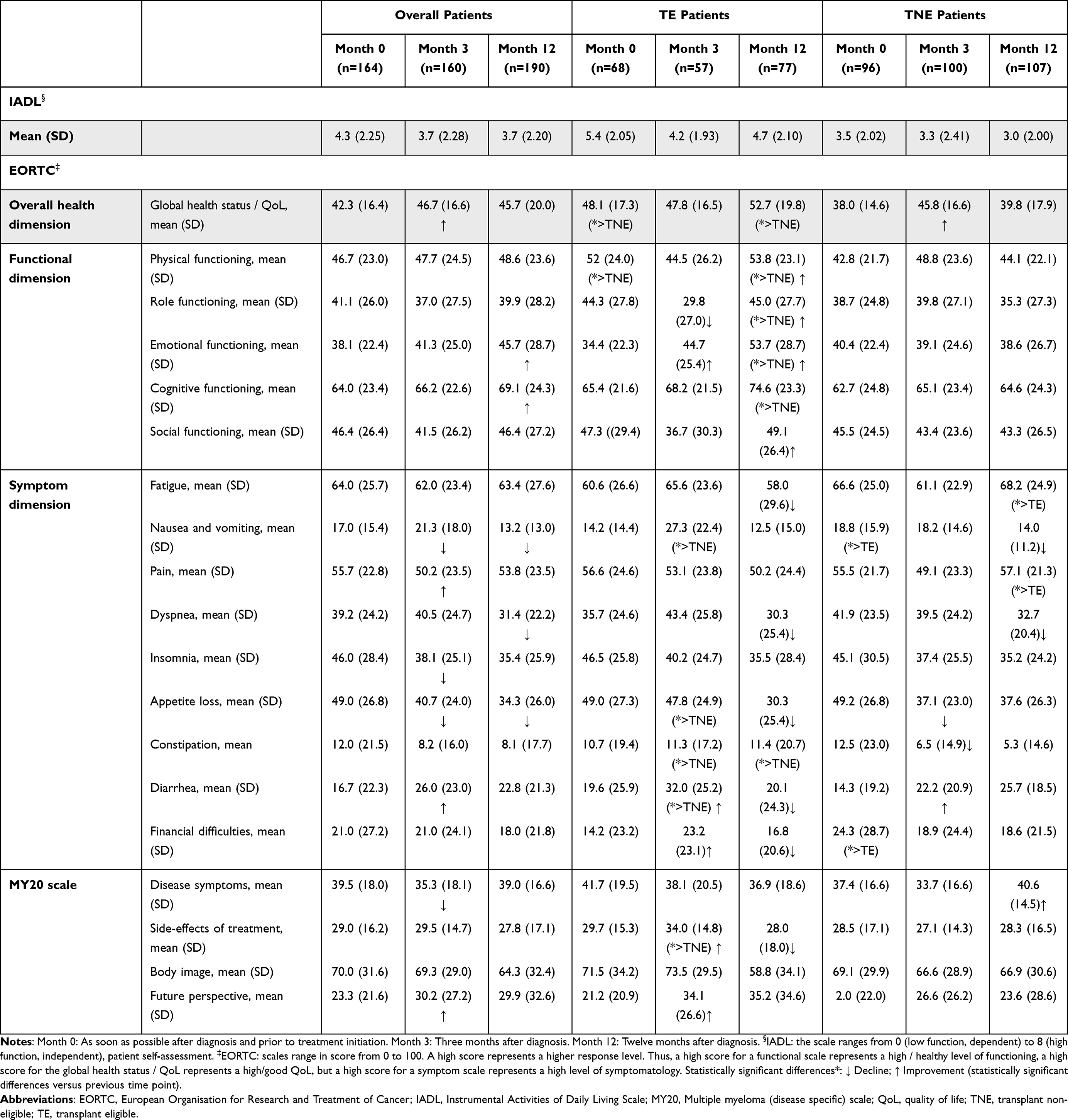 |
Table 5 IADL and QoL Mean Scores Amongst TE and TNE NDMM Patients at Three Study Time Points |
Health-Related Quality of Life (EORTC)
Overall, mean scores for global health, functioning and disease-specific symptoms in the EORTC HRQoL questionnaire were moderate across all 3 time points for both TE and TNE NDMM patients (0 = poor QoL, 100 = good QoL). There was a significant improvement in overall HRQoL by Month 3 which was maintained at Month 12, though still just below the middle score of 50. This is concurrent with an improved future perspective 3 months after diagnosis vs Month 0, supported by lower pain, insomnia, and appetite loss scores (though increased nausea and vomiting and diarrhea are also seen at Month 3). As seen with other scores, TE patients had a significantly higher functioning at Month 12 vs TNE patients. Across all participants, fatigue scores remained stable from Month 0 to Month 12 with an average score of 64 (at Month 0) and 63 (Months 3 and 12, on a score ranging from 0 (good) to 100 (poor)). However, TE patients reported a significant improvement in the level of fatigue they experienced at Month 12 vs Month 3 (mean score: 58 vs 67 respectively) compared with increased fatigue felt by TNE patients at Month 12 (mean score: 68 at Month 12, 62 at Month 3). By Month 12 there was also a significant improvement in patients’ emotional and cognitive functioning vs Month 3. This was driven by changes for TE patients, with few differences perceived by TNE patients at all study time points (Table 5).
Hobbies and Leisure Time
Patients were asked how they spent their leisure time prior to their diagnosis, then what they were still able to do over the twelve months after diagnosis. At Month 12, the majority of NDMM patients had stopped spending time with family, dining with friends or going away on trips (71%, 83% and 90% for Months 0, 3 and 12 respectively). Similarly, patients undertaking cultural and physical leisure activities also declined at Month 3 (Figure 4). However, given the timing of the research, some of the hobbies and interactions may have been restricted due to the SARS-CoV-2 pandemic.
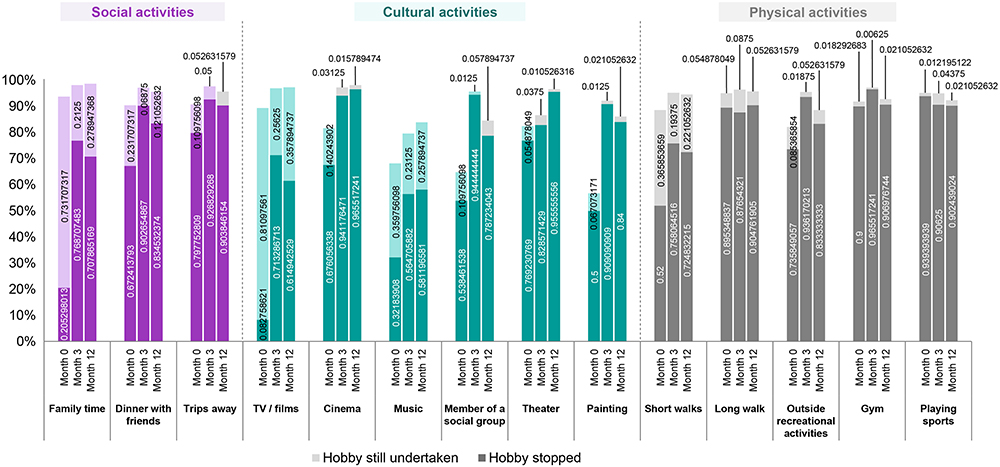 |
Figure 4 NDMM patients’ leisure activities maintained and stopped at three study time points§. Month 0: As soon as possible after diagnosis and prior to treatment initiation. Month 3: Three months after diagnosis. Month 12: Twelve months after diagnosis. Bases unless otherwise stated: Month 0 n=164; Month 3, n=160; Month 12, n=190. §Many hobbies may have been restricted at Month 12 due to SARS-CoV-2 pandemic. |
The Burden of NDMM on Caregivers During the First Year After Diagnosis
At diagnosis, the bulk of patients were cared for only by an informal caregiver: 97% were cared for by family or friends only, while 3% of patients also had a professional caregiver. Twelve months after diagnosis, 10% of patients received additional care from a professional caregiver and 2% visited a day care facility or nursing home. At all study time points, about 10% of caregivers perceived that the patients they cared for needed more professional care than that currently received. Meanwhile, a greater proportion of caregivers received additional support from patient and charity organizations, friends, and family at Month 0 (28%) than twelve months after diagnosis (11%).
Burden of the Caring Role
Using a numeric scale from 0 (burden is not at all straining) to 10 (burden is much too straining), caregivers self-rated their caring burden as moderate, with a mean of 5.3 at Month 0, 6.1 at Month 3 and 5.6 at Month 12, indicating a peak in the burden three months after diagnosis and a potential recovery at twelve months after diagnosis. Caregivers of TNE patients consistently feel more burdened than those caring for TE patients, as measured by the self-rated burden scale, the Carer Strain Index and the CarerQoL 7D scale. Caregivers of a partner reported a higher burden and a worse caregiving situation than their counterparts caring for a parent (Table 6). Though caregivers felt that the caring role was having an impact on their ability to do regular daily activities, family life and social activities, the effect remained consistent over the three time points. In terms of working patterns, many fewer were working by Month 12 vs Month 0 (81% vs 67%), but those who were still able to work were more productive twelve months after diagnosis than at the start of their journey (mean score: 5.0 at Month 0 and Month 3, and 3.0 at Month 12). The majority of caregivers felt that they could continue caring for the patient for a year or more with the level of burden experienced at that time point if no changes to the situation occurred (83% at Month 0–84% at Month 12).
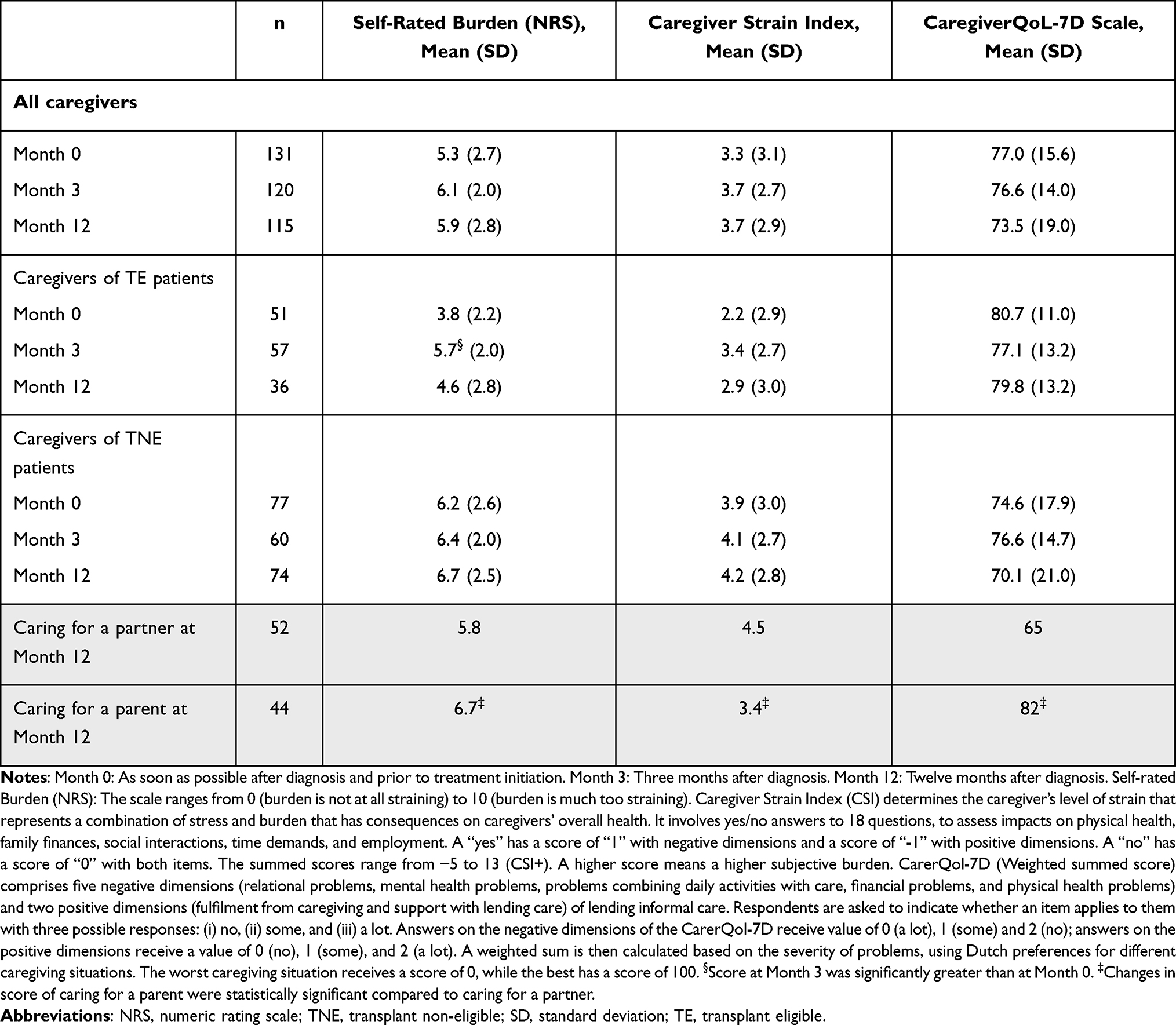 |
Table 6 Self-Rated Burden, Strain, and QoL of Caregivers of TE and TNE NDMM Patients |
Overall Health of Caregivers
Emotional support, general housework, meal preparation and attending hospital visits were the types of care provided most frequently by caregivers (to more than 60% of patients), which remained constant across the three time points. Meanwhile, help with personal care was less frequent (50% Month 0) and declined to 30% of patients by Month 12, particularly reducing among those caring for a partner rather than a parent.
Overall, caregivers felt their own overall health status was average to good with an NRS mean score of 7.7 at Month 0 (scale of 0 (worst possible) to 10 (best possible)) and 7.3 at Month 12. Fifty-eight percent considered themselves in good health at Month 0, compared with 48% at Month 12. However, over one-third (38%) reported being diagnosed with one of stress, anxiety, or depression due to their caring role at Month 0, increasing to almost half (48%) one year after the MM diagnosis (Table 7).
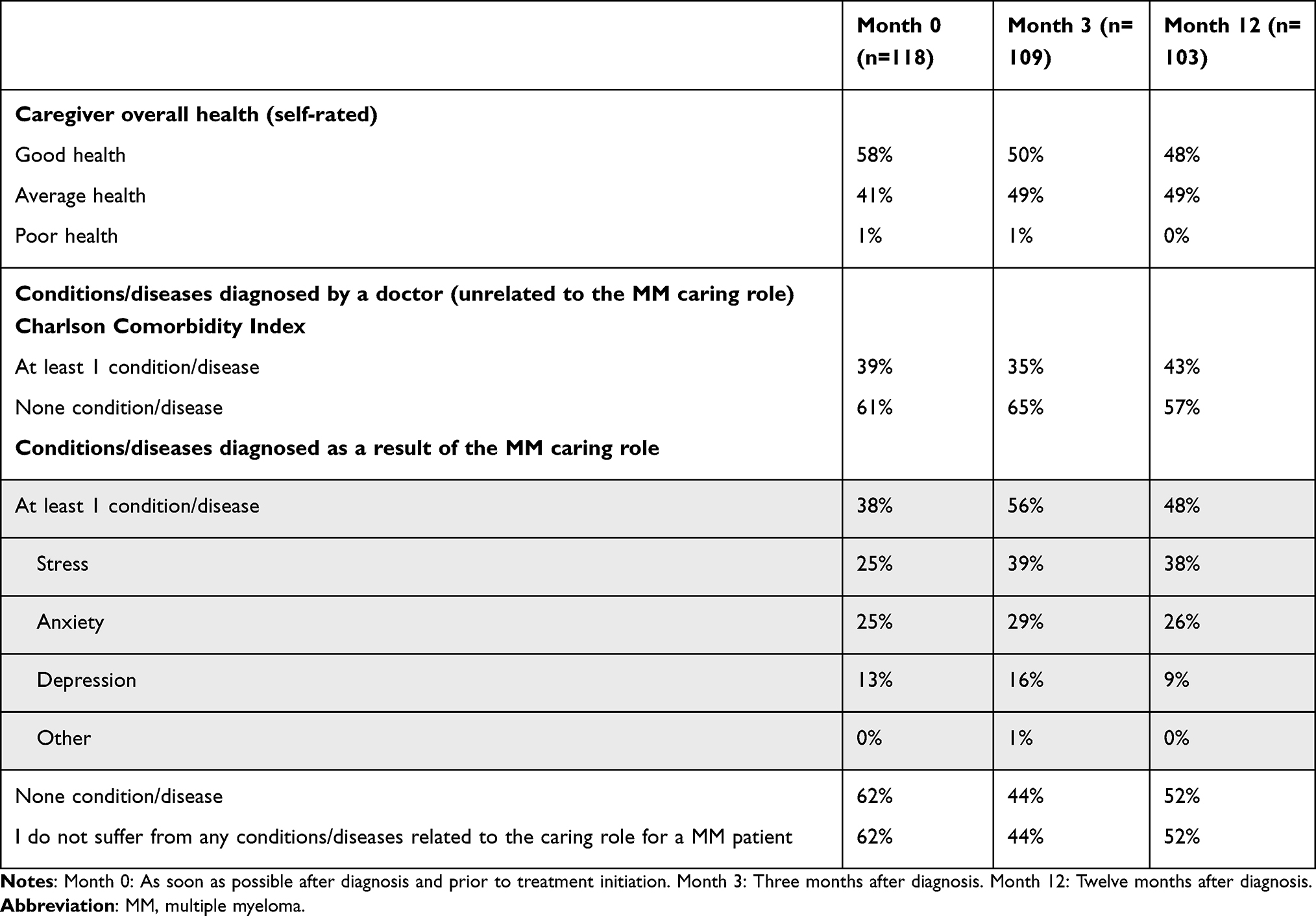 |
Table 7 Caregivers’ Self-Assessment of Their Own Overall Health as a Result of the NDMM Caring Role |
Economic Burden of NDMM During the First Year After Diagnosis
Costs of Care
The direct medical cost to the community per TE patient was similar to the cost per TNE patient during the period covered. Over the three time points (each covering the previous 3 months, to a total of 9 months), the median total cost was €18,430 for TE patients, compared with €17,218 for TNE patients. These direct medical costs relate to the use of healthcare resources in the healthcare system. Specialist consultations and hospital visits accounted for about 90% of the direct medical costs per patient at all study time points. The cost of treatments, tests and transplants to the healthcare system are not included in these costs, beyond the time spent in hospital.
For TE patients, median 3-months costs of healthcare services usage peaked at Month 3 [€ 4792 at diagnosis (Month 0), €10,026 three months after diagnosis (Month 3) and €4012 twelve months after diagnosis (Month 12)]. TE patients almost all spent time in hospital for blood tests at Month 0 and made more specialist visits at Month 0 and Month 3 compared to TNE patients. Contrastingly, the peak median TNE patient cost to the community was at Month 0 (€10,983 at Month 0, €3447 at Month 3 and €2846 at Month 12). TNE patients received more consultations with non-specialized HCPs than TE patients throughout the first year after diagnosis while TE patients used community services more often than TNE patients.
Other Direct Costs
Median patient spend on MM was €0. At Month 0, 15% of patients reported a spend on MM >€0, 6% at Months 3 and 12. However, the majority did not keep track of the costs for over the counter (OTC) medication, any treatment fees, house adaptations, travel to appointments or other costs, being either unable or unwilling to give an answer. Of the minority of patients providing an answer (including those answering €0), the mean patient spend on MM was €590 at Month 0 (n = 40, range: €0-€4000), €139 at Month 3 (n = 21, range €0-€500), €1121 at Month 12 (n = 36, range: €0-€5280). The largest spend was on home adaptations, being particularly expensive for TNE patients (median €325 at Month 12, vs €150 for TE patients). Caregivers were able to estimate their spend on support in the home as increasing from a median €0 in the three months prior to Month 3 (50% reported spending >€0), to €720 in the three months prior to Month 12. At Month 0, 15% of patients reported a spend on MM >€0, 6% at Months 3 and 12. As with patients, the majority of caregivers did not keep track of travel and accommodation costs or other logistical costs (Table 8).
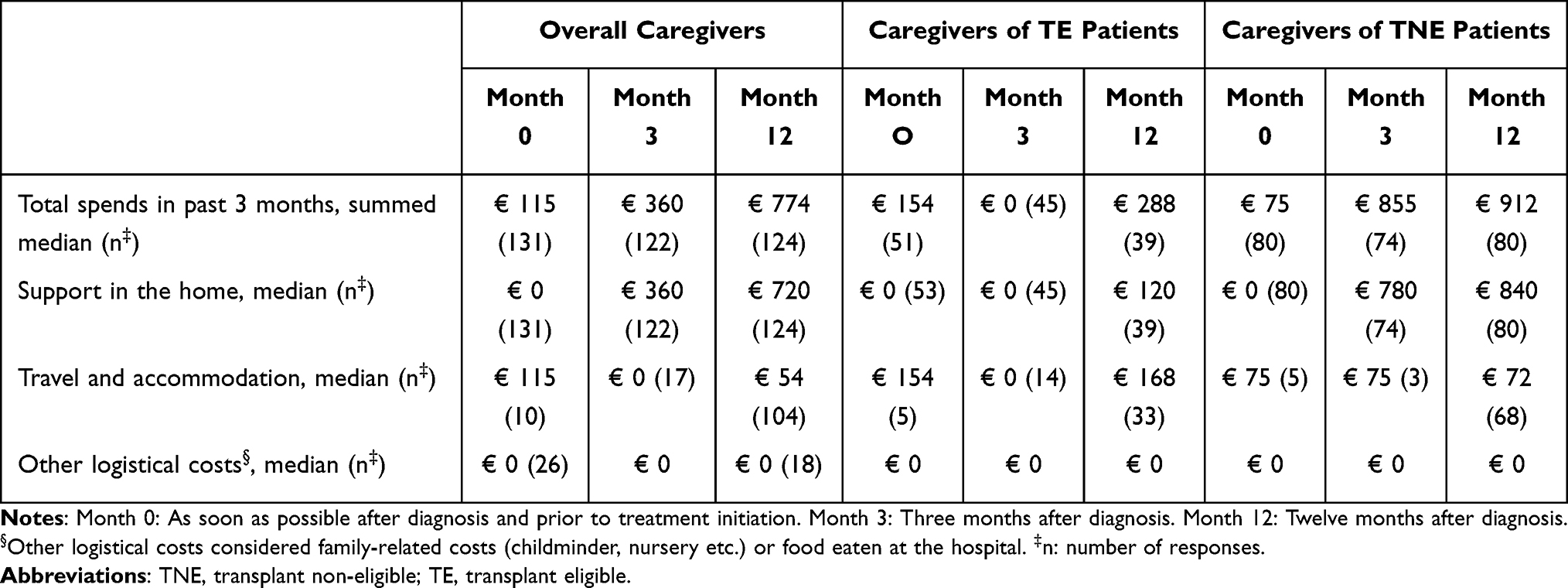 |
Table 8 Direct Costs to Caregivers of TE and TNE NDMM Patients at Three Study Time Points |
Costs of Productivity Loss
Productivity Loss Amongst Patients
More than 70% of the participating NDMM patients were retired at study entry and employment further decreased throughout the study. Among the sample tracked over time, employment dropped from 21% at Month 0 to 13% by Month 12. The share of employed patients who had to stop working/reduce their hours due to their condition increased over the year, affecting 5% of patients at Month 0, rising to 20% at Month 12. Those still describing themselves as working spent a median zero hours at work at all time points. Of the patients who were working 16%, 13%, and 18% reported spending >0 hours working in the past 7 days at 0 months, 3 months, and 12 months, respectively.
Amongst employed patients, the median number of days of work missed during the previous 3 months was 57.9 at Month 0, 57.5 at Month 3 and 50.1 at Month 12 (Table 9). TE patients had slightly less time off work than TNE patients at diagnosis (mean number of days of work missed per 3 months: 54.5 vs 60.9 respectively) and twelve months after diagnosis (47.3 vs 55.4).
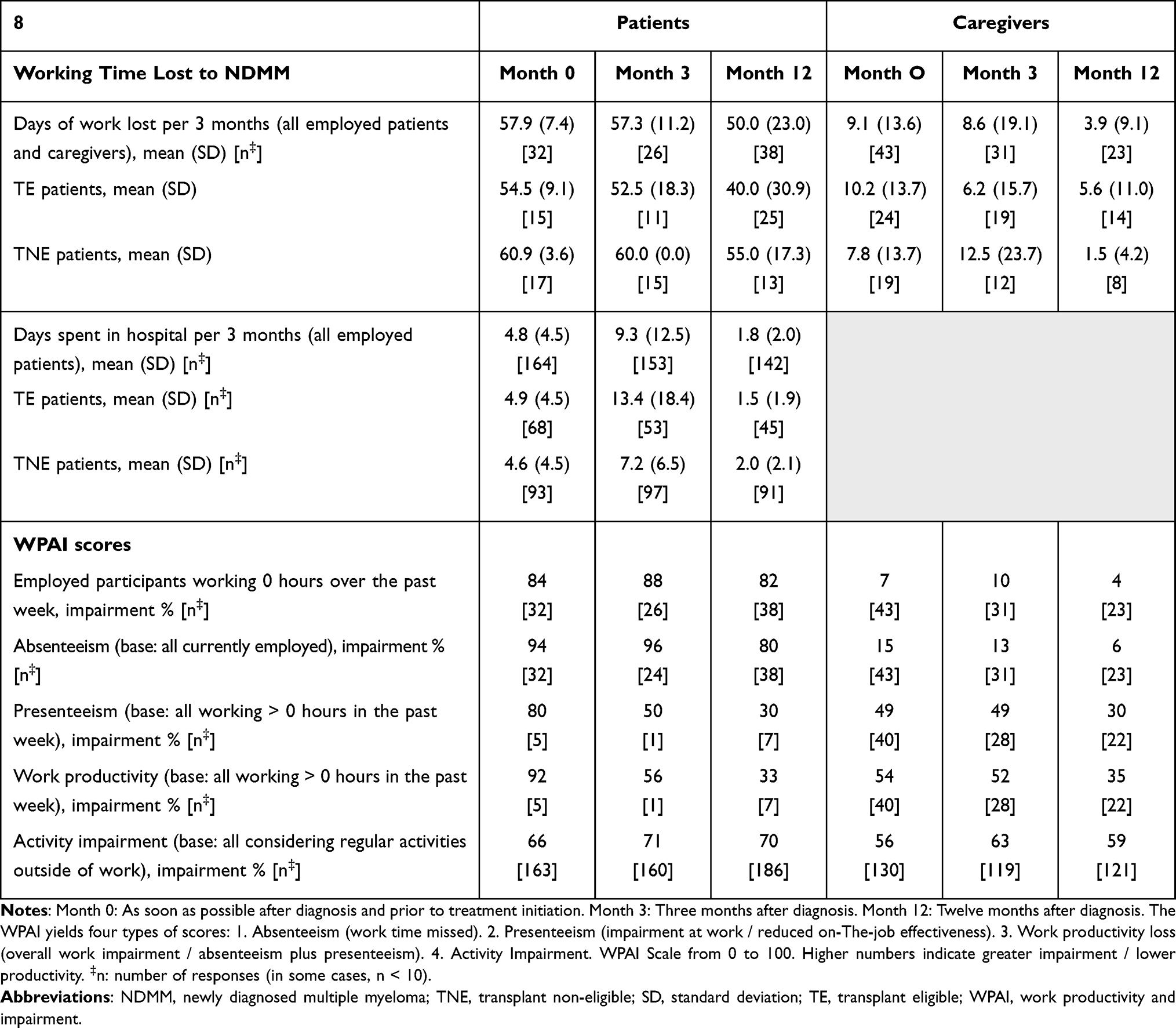 |
Table 9 Productivity Loss Amongst NDMM Patients and Caregivers at Three Study Time Points |
The WPAI questionnaire was used to measure impairments in both paid work and unpaid work, as well as absenteeism, presenteeism and the impairments in unpaid activity because of MM during the seven days prior to completing the questionnaire. Absenteeism (absence from work) and presenteeism (staying at work despite being ill) both indicate a loss of productivity. To quantify this, an impairment score between 0 and 100 is calculated, with higher numbers indicating greater impairment and less productivity. Absenteeism scores of NDMM patients were 94, 96 and 80 points at Months 0, 3 and 12, respectively, showing that absenteeism was very high. Based on the average gross wage of each market, the costs of absenteeism per employed patient per 3 months was calculated as €8769.60 at Month 0, €8640.60 at study Month 3 and €7101.68 at Month 12 with an estimated consistent median cost to employers of €8770.00 across all study time points, per 3 months. Due to the limited time spent working by most patients, the sample size for presenteeism and overall work productivity scores were very low, conclusions cannot be drawn. However, directionally the impairment for those working decreased across time points. The authors hypothesize that this may relate to fewer “less able” patients continuing to work overtime, or an impact of treatment, however interpretation is beyond the scope of this study.
Productivity Loss Amongst Caregivers
At study Month 0, 19% of caregivers were employed, of whom 67% were full-time and 33% were part-time workers. Employment figures rose amongst caregivers by 12 months post-diagnosis, when 33% were employed. Absenteeism amongst caregivers was relatively low at diagnosis (WPAI score 15 out of 100) and both absenteeism and costs to employers of absenteeism decreased over time. Higher levels of presenteeism than absenteeism were reported amongst caregivers across all time points, although this also decreased over time (49 at Months 0 and 3, and 30 at Month 12) (Table 9).
Altogether, the overall cost of absenteeism of NDMM patients and caregivers to employers for each NDMM patient for the previous 3 months is €10,474.80 at Month 0, €10,219.22 at Month 3 and €7979.13 at Month 12 (Figure 5).
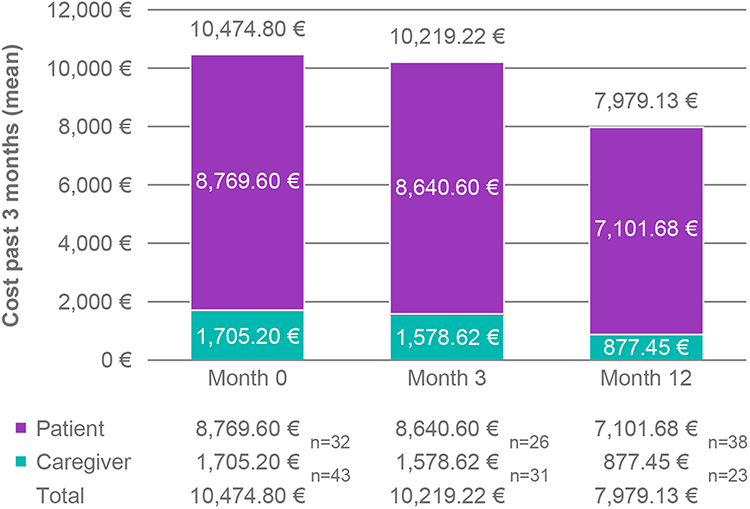 |
Figure 5 Costs of absenteeism for all employed NDMM patients and caregivers at three study time points. Month 0: As soon as possible after diagnosis and prior to treatment initiation. Month 3: Three months after diagnosis. Month 12: Twelve months after diagnosis. Costs were calculated in €, based on the average salary (OECD 2018 for Month 0 and 2019 for Month 3/Month 12) and average number of hours worked annually per country. |
The Impact of SARS-COV-2 Pandemic on Study Development and Results
The SARS-COV-2 pandemic spread across Europe during Q1 2020, coinciding with collection of data for Months 3 and 12.
The pandemic had a detrimental effect on patients. Twenty-three percent of patients and 15% of caregivers were confirmed to have SARS-COV-2 infection during the study. TE patients reported delays in the initiation of their therapy and ASCT, most significantly in Italy. Using an impact scale of 1 (no impact) to 7 (very high), patients and caregivers rated the impact of the pandemic as consistently high; impact on their social life 6.0 and 6.3, their emotional well-being 6.3 and 6.2, their physical well-being 5.8 and 5.5 and their concern attending hospital visits 5.4 and 5.3, respectively. This was reflected in their mood/outlook on life, where they assigned a below average score of 4.0 and 4.6 (patients and caregivers respectively) to their overall mood and outlook on life on a rating scale of 0 (worst possible) to 10 (best possible).
Discussion
This is the first published study to explore the views of NDMM patients and their caregivers on the burden of the illness in the twelve months after diagnosis. The study applied a combination of standardized assessment tools to understand the journey taken by NDMM patients and their caregivers from four European countries, providing a snapshot of their situations at the time of diagnosis, three months later and a full year post-diagnosis. It also depicts differences between TE and TNE NDMM patients. The study findings show that the diagnosis of MM has a significant clinical, humanistic, and financial impact on patients, caregivers, and society.
We demonstrated that patients progressively lose independence and the ability to perform daily activities throughout those first 12 months after diagnosis. Consequently, reliance on caregivers increased. Also identifying the need to understand the burden on NDMM patients, Cenzer et al 2020,26 and Larsen et al 2020,27 similarly observed a functional decline in several MM patient-reported functional measures after diagnosis. Although decline in these functional domains is commonly considered part of ageing, the authors found that the functional decline in MM patients was considerably higher than the decline in participants of similar age without an MM diagnosis29 but similar to other cancer populations.30
In this study, pain burden was particularly significant amongst TNE patients who reported higher use of opioid medications than TE patients. TNE patients were also more fatigued than TE individuals. In this sense, Mian et al 2020,8 reported that symptoms, such as tiredness, pain, drowsiness, loss of appetite and depression significantly compromised TNE patients’ well-being. Furthermore, in this study, other symptoms mostly derived from medication side-effects, such as vomiting and diarrhea, were more common amongst TE patients 3 months after diagnosis. These results are comparable to those of Mian et al 2020,12 who found a substantial burden of treatment within the first year of diagnosis, which was highest during the first 3 months, particularly amongst those patients who underwent ASCT.7
Despite these findings, overall self-reported health status and HRQoL remained stable amongst NDMM patients with average scores over time, possibly suggesting they become accustomed to their illness. This is consistent with other research conducted in cancer survivors showing that HRQoL tends to improve over time through completion of treatment, and remains stable afterwards.28,29 In our research, TNE patients reported worse HRQoL outcomes and were more concerned about the future compared to TE patients. This finding may be explained by TNE patients in our study being more dependent on caregivers, struggling more with pain and being significantly less able to work than TE patients. Other research in TNE NDMM patients found that overall HRQoL recovers after 6 to 12 months of therapy management.30,31
As reliance of patients on caregivers increased during the first year after diagnosis, caregiver burden also rose with a peak three months after diagnosis. Those caring for TNE NDMM patients reported greater burden and time dedicated to caring compared to TE individuals. Caregivers developed stress, anxiety or depression related to the NDMM throughout the year, particularly those caring for their partner. Separately, it has been observed that about 70% of caregivers of patients with a hematological malignancy had difficulty in fulfilling their responsibilities and had decisional conflicts related to the diagnosis and treatment process after the diagnosis of cancer.32 The uncertainty about the future after diagnosis and alteration of family dynamics had the greatest emotional burden on caregivers.33 Financial problems and changes in their professional life were the greatest determinants of emotional and social distress32 as well as lower HRQoL.34 This study found the strain was also significantly greater for those caring for a partner (compared to those caring for a parent) who felt unappreciated and confined. Spousal relationship has consistently been associated with greater degrees of depression and stress and low ratings of subjective well-being in caregivers.35
However, as seen with patients, caregivers also perceived themselves in relatively good health, with average HRQoL sustained over time. Other research suggests that the stress appraisals of patients and caregivers mutually influence each other’s perceptions of their HRQoL.36 Adapting to the disease and commitment to the patient have also been described in the coping experience of family caregivers.9
This study further shows that the economic burden of NDMM is also significant for the healthcare system and society, though direct costs are usually not monitored by the individuals themselves. Consultations with specialists and hospital visits or admissions explained most direct medical costs during the first year after diagnosis in this study, though the cost of treatments and medications were beyond the study scope. In the burden of illness study conducted by Neves et al 202137 in Portugal, pharmacological costs represented more than 60% of the direct medical costs, while hospital admissions that included a 9% transplant related in-hospital stays were the second largest component. The Portuguese authors calculated an average yearly direct costs per patients with MM of €31,449 (year 2018 values) with total direct costs amounting €61 million per year. Likewise, Antunes et al 201938 reported that main cost drivers in Portuguese MM patients were medications, transplantations and hospitalizations, with older patients having lower health resources use costs and fewer stem cell transplantations compared to younger patients. Robert and Miroslava 2017,39 and Petrucci et al 201340 also found drug costs to be the most important component of MM during the first 12 months after diagnosis, followed by special medical procedures and hospitalizations. This difference in the cost components between this study and previous publications is mostly explained by the differing methodology used in each case. While other authors objectively analyzed different patients and hospital datasets to estimate the costs of MM based on the prevalence of the disease, in this study the cost calculations were based on data from survey responses by patients and caregivers at three specific time points. Thus, this study relied on participants’ recall and captured their subjective perception of healthcare resources usage and expenses, without incorporating costs beyond the patient’s awareness.
Compared to TE patients, TNE patients’ direct medical costs were slightly lower, but depended more heavily on their caregivers who increased their outlays to support home adaptations and care. Other authors found that out-of-pocket expenses may correspond to 3.1% of the total costs of illness,40 while MM treatment-related overheads, including co-payments for physician visits, medications, treatments, diagnostic tests, and procedures may represent about 36% of patients’ income during the first year of treatment of NDMM.14 Furthermore, MM patients may need to apply for financial assistance (36%), use their savings to pay for myeloma treatment (46%), or borrow money to pay for medications (21%) as other studies found.41
This study found that patients and caregivers did not routinely keep a record of their travel and accommodation expenditure. The type of therapy, the geographical distance to tertiary hospitals, travel time, and relocation needs of patients and caregivers can significantly influence travel and accommodation costs.42
Less than one-fourth of NDMM patients were employed at the time of the MM diagnosis (mean age at diagnosis of 69 in our study), as could reasonably be expected for a disease of patients of advanced age (our data are in line with other findings showing an average diagnosis age of 69).43 The small share of working patients at study entry reduced further across the 12 months. Those patients still describing themselves as working reported a high level of productivity loss, absenteeism and presenteeism. Likewise, a significant increase in missed work days per month following the initial diagnosis of MM has been found in other studies.13 According to other published estimates, productivity loss represents 13.1% of the total burden of NDMM. Symptoms burden and ASCT are strong determinants of work-related losses and costs for informal care.40 Jackson et al 201944 estimated average total productivity losses per ASCT NDMM patient at €290,601 over a 20‐year period. According to these authors, more than half of patients changed from full-time employment to retirement after ASCT and during maintenance therapy. Amongst those keeping their jobs, worked hours dropped considerably due to reduced working hours and to absenteeism associated with disease impact. Need for administration of their MM treatment in the hospital may also magnify high losses in productive working hours for patients and caregivers alike.13,42 Research conducted in the outpatient setting in breast cancer survivors receiving chemotherapy similarly showed that absenteeism and presenteeism due to treatment side effects are associated with large and significant productivity losses.45
In our study, the decline in share of employed caregivers in the tracked sample and increase in mental health issues highlighted some of the strains on caregivers. Informal caregivers of cancer survivors need to make extended employment changes to accommodate their caring role.46 Productivity of caregivers in our sample was low immediately after diagnosis with a trend towards improving (less presenteeism) after 1 year of caring among those keeping their job. This aligns with the findings of others, where changes in employment are more likely closer to diagnosis or end of treatment; amongst caregivers of patients treated with transplant and who experienced functional limitations.46
These findings, though providing valuable insight, need to be interpreted within the limitations of the research. The status of a patient as either TE or TNE was as identified by their physician without any additional clinical context. Results rely on the accurate answer of participants. Costs derived from using health- and social care resources, and productivity loss relied on patients’ and caregivers’ recollection of usage and should be interpreted as such. In addition, the costs of treatment to the patients were not recorded. As mentioned, only a small number of NDMM patients were employed at each time point, predominantly due to the age of participants. Results relating to productivity loss must be read in the light of this small sample.
Despite these limitations, this study provides real-world information on an area little researched and underpins patients’ and caregivers’ notion of the clinical, emotional and financial burden of NDMM during the first year after diagnosis. These findings will support resource allocation decision-making and broader treatment value decisions.
Conclusions
NDMM is highly burdensome for patients and caregivers in the first year after treatment initiation. In this study, TNE patients experience greater pain and are more dependent on caregivers than TE patients. Despite the financial, physical and emotional burden, HRQoL remains stable, possibly indicating resilience and illness adjustment amongst patients and caregivers.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical review and approval and patient consent were not necessary for this study, due to its exploratory and descriptive nature based on an anonymous survey on patients’ and caregivers’ recalls of their care experience. Patients received an information sheet informing about the name of study, objectives, sponsors, data anonymization and processing, and voluntarily participation.
Acknowledgments
We thank the patients, caregivers and healthcare professionals for their contribution to this study. We also thank Anunciacion Seco, Jacob Collins, Hannah Marshall, Will Spencer and Kieran Chudasama at Research Partnership for their support with the fieldwork and analysis and Silvia Paz Ruiz, at SmartWorking4U, for medical writing assistance and editorial support in manuscript preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Janssen Pharmaceuticals provided financial support for this study.
Disclosure
XG and WI are employees at Janssen Pharmaceuticals; BG, JR and VS work at Research Partnership, a consultancy company that received financial support from Janssen Pharmaceuticals to conduct the study. KK reports grants from AbbVie, Sanofi, Janssen, Sandoz, BMS, Takeda, GSK, Oncopeptides, Mundipharma, Gilead, Amgen, Roche, Karyopharm, and Pfizer, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Al-Farsi K. Multiple myeloma: an update. Oman Med J. 2013;28(1):3–11. doi:10.5001/omj.2013.02
2. Noll JE, Williams SA, Purton LE, Zannettino ACW. Tug of war in the haematopoietic stem cell niche: do myeloma plasma cells compete for the HSC niche? Blood Cancer J. 2012;2(9):e91. doi:10.1038/bcj.2012.38
3. Dimopoulos MA, Moreau P, Terpos E, et al. Multiple myeloma: EHA-ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2021;32(3):309–322. doi:10.1016/j.annonc.2020.11.014
4. Cowan A, Allen C, Barac A, et al. Global burden of multiple myeloma - A systematic analysis for the global burden of disease study 2016. JAMA Oncol. 2018;4(9):1221–1227. doi:10.1001/jamaoncol.2018.2128
5. Cornell RF, Kassim AA. Evolving paradigms in the treatment of relapsed/refractory multiple myeloma: increased options and increased complexity. Bone Marrow Transplant. 2016;51(4):479–491. doi:10.1038/bmt.2015.307
6. Robinson D, Orlowski R, Stokes M, et al. Economic burden of relapsed or refractory multiple myeloma: results from an international trial. Eur J Hematol. 2017;99(2):119–132. doi:10.1111/ejh.12876
7. He J, Duenas A, Collacott H, et al. Patient perceptions regarding multiple myeloma and its treatment: qualitative evidence from interviews with patients in the United Kingdom, France, and Germany. Patient. 2021;14(5):613–623. doi:10.1007/s40271-021-00501-7
8. Mian HS, Pond GR, Wildes TM, Sivapathasundaram B, Sussman J, Seow H. Symptom burden in transplant ineligible patients with newly diagnosed multiple myeloma: a population-based cohort study. Haematologica. 2020;106(7):1991–1994. doi:10.3324/haematol.2020.267757
9. Quiñoa-Salanova C, Porta-Sales J, Monforte-Royo C, Edo-Gual M. The experiences and needs of primary family caregivers of patients with multiple myeloma: a qualitative analysis. Palliat Med. 2019;33(5):500–509. doi:10.1177/0269216319830017
10. Morris M, Marshall-Lucette S. The experience of myeloma caregivers during home-based oral chemotherapy treatment: a qualitative study. Semin Oncol Nurs. 2017;33(3):362–371. doi:10.1016/j.soncn.2017.05.010
11. Joo CW, Quach H, Raje N. Perspectives in the rapidly evolving treatment landscape of multiple myeloma: expert review of new data presentations from ASH 2019. Clin Lymphoma Myeloma Leuk. 2020;20(11):724–735. doi:10.1016/j.clml.2020.06.015
12. Mian HS, Fiala MA, Wildes TM. Burden of treatment among older adults with newly diagnosed multiple myeloma. Clin Lymphoma Myeloma Leuk. 2020;21(2):e152–9. doi:10.1016/j.clml.2020.09.010
13. Merola D, Yong C, Noga S, Shermock K. Costs associated with productivity loss among U.S. patients newly diagnosed with multiple myeloma receiving oral versus injectable chemotherapy. J Manag Care Spec Pharm. 2018;24(10):1019–1026. doi:10.18553/jmcp.2018.24.10.1019
14. Goodwin JA, Coleman EA, Sullivan E, et al. Personal financial effects of multiple myeloma and its treatment. Cancer Nurs. 2013;36(4):301–308. doi:10.1097/NCC.0b013e3182693522
15. Jo C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. 2014;20(4):327–337. doi:10.3350/cmh.2014.20.4.327
16. House of Commons Library. Informal Carers [Internet]. Briefing paper; 2021 [cited April 8, 2021]. Available from: https://researchbriefings.files.parliament.uk/documents/CBP-7756/CBP-7756.pdf.
17. Oken MM, Creech RH, Davis TE. Toxicology and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol Cancer Clin Trials. 1982;5(6):649–655.
18. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
19. Graf C. The Lawton instrumental activities of daily living scale. Am J Nurs. 2008;108(4):52–62. doi:10.1097/01.NAJ.0000314810.46029.74
20. Quality of Life - EORTC: EORTC [Internet]; [cited March 18, 2021]. Available from: https://www.eortc.org/research_field/quality-of-life/.
21. Proskorovsky I, Lewis P, Williams CD, et al. Mapping EORTC QLQ-C30 and QLQ-MY20 to EQ-5D in patients with multiple myeloma. Health Qual Life Outcomes. 2014;12(1):35. doi:10.1186/1477-7525-12-35
22. Shelkey M, Wallace M. Katz index of independence in activities of daily living. J Gerontol Nurs. 1999;25(3):8–9. doi:10.3928/0098-9134-19990301-05
23. Hoefman RJ, van Exel J, Brouwer WBF. Measuring the impact of caregiving on informal carers: a construct validation study of the CarerQol instrument. Health Qual Life Outcomes. 2013;11(1):173. doi:10.1186/1477-7525-11-173
24. Van Den Hout WB. The value of productivity: human-capital versus friction-cost method. Ann Rheum Dis. 2010;69(Suppl 1):i89–91. doi:10.1136/ard.2009.117150
25. Gol-Montserrat J, Del Burgo MLM, Quecedo L, Del Llano JE. Analysis of productivity costs in cancer: a systematic review. Glob Reg Heal Technol Assess Ital North Eur Spanish. 2017;4(1):5000262.
26. Cenzer I, Berger K, Rodriguez AM, Ostermann H, Covinsky KE. Patient-reported measures of well-being in older multiple myeloma patients: use of secondary data source. Aging Clin Exp Res. 2020;32(6):1153–1160. doi:10.1007/s40520-019-01465-3
27. Larsen RF, Jarden M, Minet LR, Frølund UC, Möller S, Abildgaard N. Physical function in patients newly diagnosed with multiple myeloma; A Danish cohort study. BMC Cancer. 2020;20(1):1–11. doi:10.1186/s12885-020-6637-6
28. Pearman T. Health and quality of life outcomes quality of life and psychosocial adjustment in gynecologic cancer survivors. Health Qual Life Outcomes. 2003;1(1):33. doi:10.1186/1477-7525-1-33
29. Chakraborty R, Hamilton BK, Hashmi SK, Kumar SK, Majhail NS. Health-related quality of life after autologous stem cell transplantation for multiple myeloma. Biol Blood Marrow Transplant. 2018;24(8):1546–1553. doi:10.1016/j.bbmt.2018.03.027
30. Nielsen LK, Stege C, Lissenberg-Witte B, et al. Health-related quality of life in transplant ineligible newly diagnosed multiple myeloma patients treated with either thalidomide or lenalidomide-based regimen until progression: a prospective, open-label, multicenter, randomized, Phase 3 study. Haematologica. 2020;105(6):1650–1659. doi:10.3324/haematol.2019.222299
31. Perrot A, Facon T, Plesner T, et al. Health-related quality of life in transplant-ineligible patients with newly diagnosed multiple myeloma: findings from the Phase III MAIA trial. J Clin Oncol. 2021;39(3):227–237. doi:10.1200/JCO.20.01370
32. Karacan Y, Akkus Y, Ozcelik ET, Ali R. Identification of psychological and social problems in caregivers of individuals diagnosed with hematologic malignancy. Asia-Pacific J Oncol Nurs. 2021;8(2):204–210. doi:10.4103/apjon.apjon_53_20
33. Myeloma UK. A life in Limbo 2016 A Myeloma UK research report on the experiences of myeloma carers in the UK [Internet]; 2016 [cited July 26, 2021]. cited July 26, 2021: www.myeloma.org.uk.
34. Pereira MG, Vilaça M, Pinheiro M, et al. Quality of life in caregivers of patients with multiple myeloma. Aging Ment Health. 2020;24(9):1402–1410. doi:10.1080/13607863.2019.1617240
35. Schulz R, Sherwood PR. Physical and mental health effects of family caregiving. Am J Nurs. 2008;108(9):23–27. doi:10.1097/01.NAJ.0000336406.45248.4c
36. La IS, Yun EK. Effects of stress appraisal on the quality of life of adult patients with multiple myeloma and their primary family caregivers in Korea. Psychooncology. 2017;26(10):1640–1646. doi:10.1002/pon.4348
37. Neves M, Trigo F,Rui B, et al. Multiple myeloma in Portugal: burden of disease and cost of illness. Pharmacoeconomics. 2021;39(5):579–587. doi:10.1007/s40273-020-00993-5
38. Antunes L, Rocha-Gonçalves F, Chacim S, et al. Real-world treatment patterns, resource use and cost burden of multiple myeloma in Portugal. Eur J Cancer Care (Engl). 2019;28(4):e13026. doi:10.1111/ecc.13026
39. Robert B, Miroslava R. Direct and indirect costs associated with multiple myeloma: a case study from the Slovak Republic. Int Healthc J. 2017;1:11–16.
40. Petrucci MT, Calabrese E, Levi A, et al. Cost of illness in patients with multiple myeloma in Italy: the CoMiM study. Tumori. 2013;99(4):e193–e202. doi:10.1177/030089161309900434
41. Huntington SF, Weiss BM, Vogl DT, et al. Financial toxicity in insured patients with multiple myeloma: a cross-sectional pilot study. Lancet Haematol. 2015;2(10):e408–16. doi:10.1016/S2352-3026(15)00151-9
42. Mankinen P, Vihervaara V, Torvinen S, Martikainen J, Soini E. Costs of administration, travelling, and productivity losses associated with hospital administration of multiple myeloma drugs in Finland. J Med Econ. 2019;22(4):328–335. doi:10.1080/13696998.2019.1569457
43. Anand Padala S, Barsouk A, Barsouk A, et al. Epidemiology, staging, and management of multiple myeloma. Med Sci. 2021;9(3). doi:10.3390/medsci9010003
44. Jackson G, Galinsky J, Alderson DEC, et al. Productivity losses in patients with newly diagnosed multiple myeloma following stem cell transplantation and the impact of maintenance therapy. Eur J Haematol. 2019;103(4):393–401.
45. Tachi T, Teramachi H, Tanaka K, et al. The impact of side effects from outpatient chemotherapy on presenteeism in breast cancer patients: a prospective analysis. Springerplus. 2016;5(1):32.
46. de Moor JS, Dowling EC, Ekwueme DU, et al. Employment implications of informal cancer caregiving. J Cancer Surviv. 2017;11(1):48–57. doi:10.1007/s11764-016-0560-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.