Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
The Barthel index-dyspnea a tool for respiratory rehabilitation: reply to the letter by Chuang [Letter of clarification]
Authors Carone M, Vitacca M ![]() , Paneroni M
, Paneroni M ![]() , Baiardi P, Spanevello A
, Baiardi P, Spanevello A ![]() , Bertolotti G
, Bertolotti G ![]()
Received 23 December 2016
Accepted for publication 19 January 2017
Published 8 March 2017 Volume 2017:12 Pages 813—815
DOI https://doi.org/10.2147/COPD.S130991
Checked for plagiarism Yes
Editor who approved publication: Prof. Dr. Richard Russell
Mauro Carone,1 Michele Vitacca,2 Mara Paneroni,2 Paola Baiardi,3 Antonio Spanevello,4,5 Giorgio Bertolotti6
1Respiratory Division, ICS MAUGERI SPA SB, Institute of Cassano Murge (BA) IRCCS, Italy; 2Respiratory Rehabilitation Division, ICS MAUGERI SPA SB, Institute of Lumezzane (BS) IRCCS, Italy; 3Scientific Direction, ICS MAUGERI SPA SB, Institute of Pavia, IRCCS, Italy; 4Respiratory Rehabilitation Division, ICS MAUGERI SPA SB, Institute of Tradate (VA) IRCCS, Italy; 5Respiratory Diseases Unit, University of Insubria, Varese; 6Psychology Unit, ICS MAUGERI SPA SB, Institute of Tradate (VA) IRCCS, Italy
We read the remarkable letter by Chuang.1 We thank him for his valid suggestions on our paper. Interestingly, he focused on the two dimensions of the Barthel index-dyspnea (BI-d), which was exactly our goal. As rehabilitators, our goal is to provide patients with physical therapy depending on their health status and to improve their respiratory function. We need to verify and demonstrate the efficacy and the outcomes of respiratory rehabilitation, supported by physical therapy. For these reasons, we need an assessment device that measures respiratory improvement during daily motor activities that should be monitored.The modified Barthel index2 is a well-consolidated and widely used instrument to assess the performance of a person in a predetermined and fixed set of activities of daily living (ADLs). By proposing BI-d,3 we aimed to develop a scale to measure how dyspnea precludes or reduces the same ADLs, with the ultimate goal of globally assessing the effectiveness of rehabilitation. Hence, an assessment method that measures the impact of dyspnea on activities monitored by a rehabilitation program is of utmost importance for rehabilitators. Large part of Chuang’s letter is based on the Chronic Respiratory Questionnaire-dyspnea (CRQ-d). The CRQ-d is a health-related quality of life (health status) questionnaire, with a dyspnea “domain”.4 However, for our purposes, the CRQ-d is too individualized as each subject selects five activity items – “the most important” – out of 26 listed activities. Therefore, each subject may choose different items from other subjects in the same study group. Due to this significant methodology, CRQ was standardized recently into a version that contains a total of only five items with a dyspnea domain, all of which have to be responded.5
View the original paper by Vitacca et al
View the original letter by Chuang
Dear editor
We read the remarkable letter by Chuang.1 We thank him for his valid suggestions on our paper. Interestingly, he focused on the two dimensions of the Barthel index-dyspnea (BI-d), which was exactly our goal. As rehabilitators, our goal is to provide patients with physical therapy depending on their health status and to improve their respiratory function.
We need to verify and demonstrate the efficacy and the outcomes of respiratory rehabilitation, supported by physical therapy. For these reasons, we need an assessment device that measures respiratory improvement during daily motor activities that should be monitored.
The modified Barthel index2 is a well-consolidated and widely used instrument to assess the performance of a person in a predetermined and fixed set of activities of daily living (ADLs). By proposing BI-d,3 we aimed to develop a scale to measure how dyspnea precludes or reduces the same ADLs, with the ultimate goal of globally assessing the effectiveness of rehabilitation. Hence, an assessment method that measures the impact of dyspnea on activities monitored by a rehabilitation program is of utmost importance for rehabilitators.
Large part of Chuang’s letter is based on the Chronic Respiratory Questionnaire-dyspnea (CRQ-d). The CRQ-d is a health-related quality of life (health status) questionnaire, with a dyspnea “domain”.4 However, for our purposes, the CRQ-d is too individualized as each subject selects five activity items – “the most important” – out of 26 listed activities. Therefore, each subject may choose different items from other subjects in the same study group. Due to this significant methodology, CRQ was standardized recently into a version that contains a total of only five items with a dyspnea domain, all of which have to be responded.5
Conversely, the modified Barthel index2 includes a predetermined and fixed set of ADLs. This allows better comparison between subjects or group of subjects, before and after a treatment, a significant criterion in rehabilitation, and a specific field for which we mainly developed the scale. Moreover, CRQ-d is dyspnea centered, whereas BI-d is activity centered.
This first paper on BI-d validation is auspicious. The metric qualities are good and the variability is acceptable, with 95% confidence intervals of correlation coefficient of BI-d versus 6-minute walking test being −0.609 and −0.352, respectively.
As pointed out in our paper, additional studies in respiratory rehabilitation programs are required to further assess the applicability of the scale in a broadest context. Mild COPD patients are among those populations who are potential candidates of BI-d. Dr Chuang showed accurately that only 8.1% of our study population had mild COPD. This is obvious as COPD is largely underestimated, and patients usually consult a specialist only when they are diagnosed with GOLD 26 stage disease.7–9 Table 1 and Figure 1 show a few outcomes of four subjects based on the four GOLD stages. They also show that the less obstructed the patient, the lower the BI-d was. Conversely, the more obstructed the patient, the higher the BI-d was. After pulmonary rehabilitation, the BI-d improved in all patients. The best results were observed in GOLD 4 stage as they received a more intensive health care and rehabilitation program. On the other hand, the smallest limitation was assessed at the baseline, and the smallest differences in outcome were observed in subjects at GOLD 1 stage.
 | Table 1 Four clinical cases according to GOLD severity criteria of obstruction: stages 1–4 |
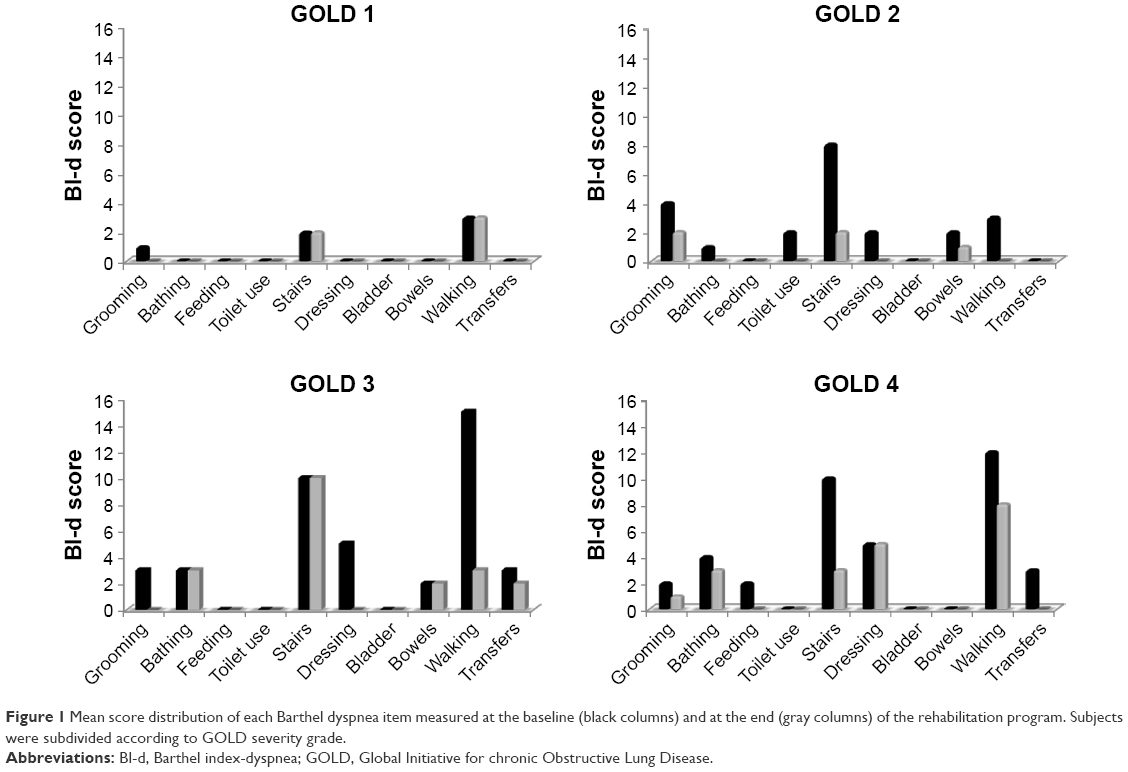 | Figure 1 Mean score distribution of each Barthel dyspnea item measured at the baseline (black columns) and at the end (gray columns) of the rehabilitation program. Subjects were subdivided according to GOLD severity grade. |
Conclusion
In conclusion, we consider it appropriate to uphold all items of both the modified Barthel index score (because they collect important information from a physical rehabilitation point of view) and of the Barthel dyspnea index (because they allow the estimate of the outcome of a specifically tailored respiratory rehabilitation program).
Disclosure
The authors report no conflicts of interest in this communication.
References
Chuang ML. The Barthel index-dyspnea: a new two-dimensional dyspnea scale. Int J Chron Obstruct Pulmon Dis. 2016;11:1843–1844. | ||
Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. | ||
Vitacca M, Paneroni M, Baiardi P, et al. Development of a Barthel index based on dyspnea for patients with respiratory diseases. Int J Chron Obstruct Pulmon Dis. 2016;11:1199–1206. | ||
Lacasse I, Wong E, Guyatt GH. Individualising questionnaires. In: Joyce CRB, O’Boyle CA Mc Gee H, editors. Individual Quality of Life. Amsterdam: Harwood Academic Publishers; 1999:87–104. | ||
Schünemann HJ, Griffith L, Jaeschke R, et al. A comparison of the original chronic respiratory questionnaire with a standardized version. Chest. 2003;124(4):1421–1429. | ||
Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6): 532–555. | ||
Buist AS, McBurnie MA, Vollmer WM, et al; BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. | ||
Guerriero M, Caminati M, Viegi G, Senna G, Cesana G, Pomari C. COPD prevalence in a north-eastern Italian general population. Respir Med. 2015;109(8):1040–1047. | ||
Kim V, Criner GJ. The chronic bronchitis phenotype in chronic obstructive pulmonary disease: features and implications. Curr Opin Pulm Med. 2015;21(2):133–141. | ||
Dove Medical Press encourages responsible, free and frank academic debate. The content of the International Journal of Chronic Obstructive Pulmonary Disease 'letters to the editor' section does not necessarily represent the views of Dove Medical Press, its officers, agents, employees, related entities or the International Journal of Chronic Obstructive Pulmonary Disease editors. While all reasonable steps have been taken to confirm the content of each letter, Dove Medical Press accepts no liability in respect of the content of any letter, nor is it responsible for the content and accuracy of any letter to the editor. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.