")
Back to Journals » International Journal of General Medicine » Volume 16
The Association of Lipoprotein(a) and Neutrophil-to-Lymphocyte Ratio Combination with Atherosclerotic Cardiovascular Disease in Chinese Patients
Authors Wang X, Chen X, Wang Y, Peng S, Pi J, Yue J, Meng Q, Liu J, Zheng L, Chan P , Tomlinson B , Liu Z, Zhang Y
Received 10 March 2023
Accepted for publication 15 June 2023
Published 3 July 2023 Volume 2023:16 Pages 2805—2817
DOI https://doi.org/10.2147/IJGM.S410840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaoyu Wang,1 Xiaoli Chen,1 Yanfang Wang,1 Sheng Peng,2 Jingjiang Pi,3 Jinnan Yue,1 Qingshu Meng,1 Jie Liu,1 Liang Zheng,1,4 Paul Chan,5 Brian Tomlinson,6 Zhongmin Liu,1 Yuzhen Zhang1
1Key Laboratory of Arrhythmias of the Ministry of Education of China, Shanghai Heart Failure Research Center, Research Center for Translational Medicine, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Department of Trauma, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, 200120, People’s Republic of China; 3Department of Cardiology, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 4Jian hospital, Shanghai East Hospital, Tongji University School of Medicine, Jian, 343006, People’s Republic of China; 5Division of Cardiology, Department of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan; 6Faculty of Medicine, Macau University of Science and Technology, Macau, People’s Republic of China
Correspondence: Yuzhen Zhang; Zhongmin Liu, Key Laboratory of Arrhythmias of the Ministry of Education of China, Shanghai Heart Failure Research Center, Research Center for Translational Medicine, Shanghai East Hospital, School of Medicine, Tongji University, 150 Jimo Road, Pudong 15New District, Shanghai, 200092, People’s Republic of China, Tel +86-21-61569673, Email [email protected]; [email protected]
Objective: The association of lipoprotein(a) [Lp(a)] with atherosclerotic cardiovascular disease (ASCVD) risk can be modified by chronic systemic inflammation. The neutrophil-to-lymphocyte ratio (NLR) is a reliable and easily available marker of immune response to various infectious and non-infectious stimuli. The purpose of this study was to assess the combined effects of Lp(a) and NLR in predicting the ASCVD risk and coronary artery plaque traits.
Methods: This study included 1618 patients who had coronary computed tomography angiography (CTA) with risk assessment of ASCVD. CTA was used to evaluate the traits of coronary atherosclerotic plaques, and the association of ASCVD with Lp(a) and NLR was assessed by multivariate logistic regression models.
Results: Plasma Lp(a) and NLR were significantly increased in patients having plaques. High Lp(a) was defined as the plasma Lp(a) level > 75 nmol/L and high NLR as NLR > 1.686. The patients were grouped into four categories according to normal or high NLR and plasma Lp(a) as nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+ and hLp(a)/NLR+. The patients in the latter three groups had higher risk of ASCVD compared to the reference group nLp(a)/NLR-, with the highest ASCVD risk in the hLp(a)/NLR+ group (OR = 2.39, 95% CI = 1.49– 3.83, P = 0.000). The occurrence of unstable plaques was 29.94% in the hLp(a)/NLR+ group, which was significantly higher than groups nLp(a)/NLR+, hLp(a)/NLR- and nLp(a)/NLR- with 20.83%, 26.54% and 22.58%, respectively, and there was a significantly increased risk of unstable plaque in the hLp(a)/NLR+ group compared to the nLp(a)/NLR- group (OR = 1.67, 95% CI = 1.04– 2.68, P = 0.035). The risk of stable plaque was not significantly increased in the hLp(a)/NLR+ group compared to the nLp(a)/NLR- group (OR = 1.73, 95% CI = 0.96– 3.10, P = 0.066).
Conclusion: The concomitant presence of elevated Lp(a) and higher NLR is associated with increased unstable coronary artery plaques in patients with ASCVD.
Keywords: lipoprotein(a), neutrophil to lymphocyte ratio, ASCVD and coronary artery plaque
Introduction
Cardiovascular disease (CVD) is the main cause of death worldwide. The Report on Cardiovascular Health and Diseases in China 2021 stated that the prevalence of CVD is still increasing, although the predicted current prevalence is over 330,000,000, and the first rank CVD mortality has placed a significant burden on middle-aged and elderly people (age ≥ 45).1 The major cause of CVD is atherosclerosis, a chronic inflammatory condition with immune competent cells in lesions producing mainly pro-inflammatory cytokines contributing to buildup of plaque inside the artery walls.
There are many risk factors for CVD, some are not controllable, but others can be modified. One potential target is lipoprotein(a) [Lp(a)] that might be added as a therapeutic goal to enhance cardiovascular outcomes.2,3 Lp(a) is composed of an apolipoprotein (apo) B100 containing low-density lipoprotein (LDL)-like particle bound covalently to apo(a); therefore, Lp(a) has combined atherothrombotic traits from both apo (b) (from LDL) and apo(a) (thrombo-inflammatory aspects).4 Epidemiologic, experimental, and genetic studies suggested a robust and independent relationship between Lp(a) and an elevated risk of coronary heart disease, calcific aortic valve stenosis, and ischemic stroke.2,3,5–10 A study reported that Lp(a) was associated with accelerated progression of coronary low-attenuation plaque among patients with advanced stable coronary artery disease.11 In patients with higher LDL-cholesterol (LDL-C) levels, an elevated Lp(a) level was associated with a higher frequency of thin-cap fibroatheroma (TCFA).12 However, there is no study reporting the association of Lp(a) and plaque characteristics in patients with ASCVD in the Chinese Han population.
Atherosclerosis, the major cause of CVD, is a chronic inflammatory disease of the vascular wall. Recent large randomized controlled trials revealed that anti-inflammatory treatment reduced cardiovascular risk independent of effects on LDL-C.13 Growing evidence supported the role of neutrophils and lymphocytes in plaque instability and rupture as well as the development and evolution of atherosclerotic lesions.14,15
Therefore, the neutrophil-to-lymphocyte ratio (NLR), which is widely used as a reliable and easily available marker of immune response to various infectious and non-infectious stimuli, has recently gained attention as a potential novel biomarker that identifies individuals at risk for future CVD events.16–18 NLR reflects a dynamic relationship between innate (neutrophils) and adaptive cellular immune response (lymphocytes) during pathological states, and it was reported as an indicator for the prognosis of CVD patients.19 There are various inflammatory cells in atherosclerotic plaques of the carotid artery, and NLR was reported to predict carotid plaque vulnerability in acute ischemic stroke patients.20,21 However, the relationship between NLR and ASCVD morbidity with susceptible plaque traits has been poorly understood to date.
NLR symbolizes immune system activation, and sustained high levels of Lp(a) have a role in the development of atherosclerosis. However, few studies were published on the combined impact of Lp(a) and NLR on the risk of plaque condition and ASCVD occurrence among the Chinese Han population. It is unknown if the inflammation detected by NLR affects the Lp(a)-associated ASCVD risk. The purpose of the study was to examine the combined association between Lp(a) and NLR with ASCVD in Chinese subjects.
Methods and Materials
Study Population
This study included 1618 in-patients and outpatients of Tongji Medical School affiliated Shanghai East Hospital with typical and atypical chest pain, or cardiac assessment prior to surgery, who had coronary computed tomography angiography (CTA) during January 2012 to December 2013. Informed consent was obtained from each participant. This study was conducted according to the principles established in the Declaration of Helsinki of 1975, and the research protocol was approved by the Institutional Review Board of Shanghai East Hospital affiliated to Tongji Medical School with serial number 2013–011. The inclusion criteria were age ≥45 years old, had CTA during January 2012 to December 2013, and no previous history of malignancy or autoimmune disease. The exclusion criteria of the study population included patients with symptomatic hyperthyroidism, heart failure, severe renal hepatic dysfunction, and acute inflammation (WBC >10×10^9/L). Of the 2025 patients of the Shanghai East Hospital, 1618 patients were included (Figure 1).
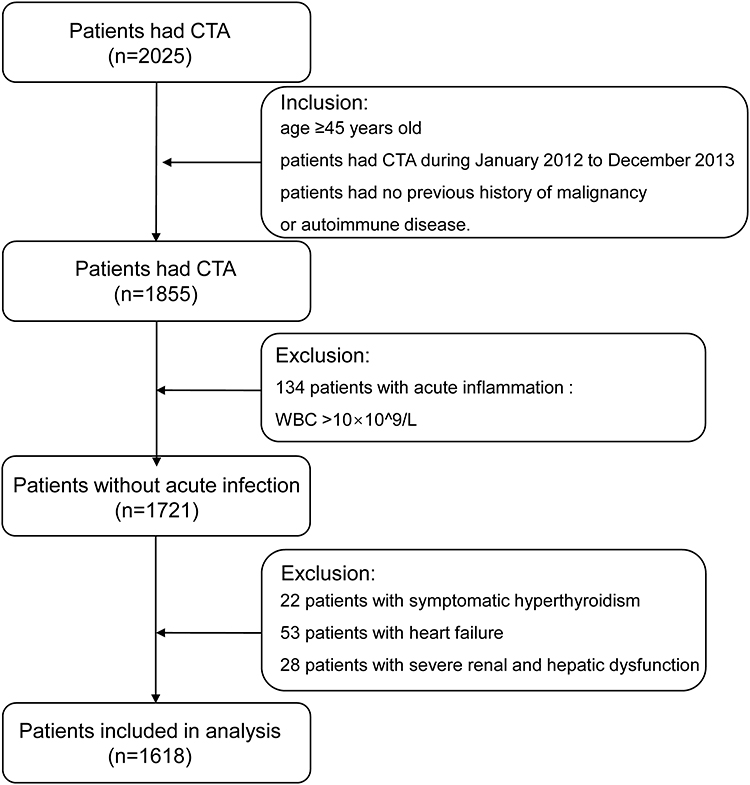 |
Figure 1 Flow chart for selection of study patients. Abbreviation: CTA, coronary computed tomography angiography. |
Demographics and Baseline Characteristics
Gender, age, smoking status, alcohol drinking status and detailed medical history were obtained from patients’ medical records of in-patients, and with a standard questionnaire by trained doctors for outpatients. Body mass index (BMI) was defined as weight divided by (height)2, with obesity defined as BMI ≥28 kg/m2. An automated oscillometric blood pressure device was used to measure resting blood pressure (BP) in the sitting position repeated 3 times after 5 minutes rest, and the average of the second and third readings was taken as the BP level. Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg, and/or use of antihypertensive medication. Fasting plasma glucose (FG) ≥7.0 mmol/l or normal FG with concurrent use of insulin or oral hypoglycemic medications was considered as diabetes. Atherosclerotic cardiovascular disease (ASCVD) was defined as one coronary artery and branches with plaques ≥70% stenosis or the left main coronary artery or 3-vessels with plaques ≥50% stenosis by CTA.22 Stable plaques were defined as density of plaques >350 HU, and unstable plaques were defined as density of plaques ≤350 HU.23 Lp(a) was analyzed as a categorical variable using established clinical cut points (75 nmol/dL).24
Laboratory Measurements
Blood samples were collected after at least 10 hours of overnight fasting and sent for measurement in the Blood Laboratory of Shanghai East Hospital.25 NLR was calculated based on the results of leukocyte counts and their various subtypes by using the automated blood cell counter following the manufacturer’s instructions. The latex-enhanced turbidimetric immunoassay (Denka Seiken) was used to measure plasma level of Lp(a), enzyme facilitating reaction (Roche Cobas 8000 C702 Biochemistry system) to measure fasting serum glucose, lipid profile and uric acid, and ion-exchange high-performance liquid chromatography (ToSoH G8 analyzer) to measure HbA1c.
Coronary CT Angiography for Assessment of Coronary Artery Atherosclerotic Plaques
In order to allow retrospective reconstruction of images in the proper cardiac phase (at 30–70% of the R–R interval) during a single breath hold, CTA scans were performed with an ECG gating system. The power injector was used to provide 70–90 mL of a nonionic contrast agent (Omnipaque, 350 mgI/mL; GE Healthcare, Princeton, NJ, USA) into an antecubital vein at a flow rate of 4–5 mL/s, followed by 30 mL of saline for contrast-enhanced scans. The delay time was calculated using a bolus tracking method. When the ascending aorta’s region of interest (ROI) crossed a threshold of 120 Hounsfield units (HU), the actual scan began. The image reconstruction used a medium-smooth convolution kernel (B26f).
The same 15-segment American Heart Association model was used to analyze the coronary artery calcium (CAC) scores and CTA datasets separately by two expert readers (J. Z. and Z. Y.). The calcifications in the coronary arteries of NCT images with a detection threshold of 130 HU were used to calculate CAC scores. The following types of coronary artery atherosclerotic plaques were determined using cardiac software (Circulation, Siemens Healthcare): stable plaque (≥130 HU); unstable plaque (<130 HU); and stable plaque and unstable plaque (comprising both non-calcified and calcified plaque components).26 CAC scores to risk-stratify patients for future CAD development were categorized into the following four groups as no-risk (CAC scores ≤10), mild-risk (10 < CAC scores ≤100), moderate-risk (100 < CAC scores ≤ 400), and severe-risk groups (CAC scores > 400).27
Statistical Analysis
The characteristics of the studied population as continuous normally distributed variables were reported as the mean (standard deviation, SD), categorical variables were presented as percentages and skewed distribution variables were presented as median (interquartile range). Continuous variables were compared using the Wilcoxon rank sum test and categorical variables using the Pearson χ2 test. A cut-off point to define the high NLR level of the patients was determined using receiver operating characteristic (ROC) curves. We investigated the association of Lp(a) and NLR with ASCVD using logistic regression. The confounders were chosen for inclusion in the adjusted models based on information from previous literature. Statistical analyses were performed using SPSS software (SPSS Inc., Chicago, IL). The statistical significance was determined at the level of 0.05, and all P values were based on 2-sided tests.
Results
Demographic and Clinical Characteristics of Study Subjects
The demographic and clinical characteristics of the patient population are presented in Table 1. Among 1618 participants, the mean age was 65.15 years and 65.27% had coronary atherosclerotic plaque. There was a significantly higher plasma Lp(a) level (205 nmol/L vs 139.5 nmol/L, P = 0.000) in patients with plaque compared to the patients without plaque. Patients with atherosclerotic plaques had higher blood neutrophil counts (3.70 10^9/L vs 3.41 10^9/L, P = 0.000) and lower blood lymphocyte counts (1.74 10^9/L vs 1.83 10^9/L, P = 0.004) than those without plaque, and thus, the NLR of patients with plaques was significantly higher (2.06 vs 1.84, P = 0.000). In the whole cohort, the prevalence of diabetes was 23.79% with significantly higher prevalence in patients with plaques (30.11% vs 11.92%, P = 0.000) (Table 1). More statin treatment was observed in patients with plaques (10.89% vs 4.45%, P = 0.002). The patients having plaques had higher moderate and severe-risk CAC scores (>100) (35.32% vs 0%, P = 0.000).
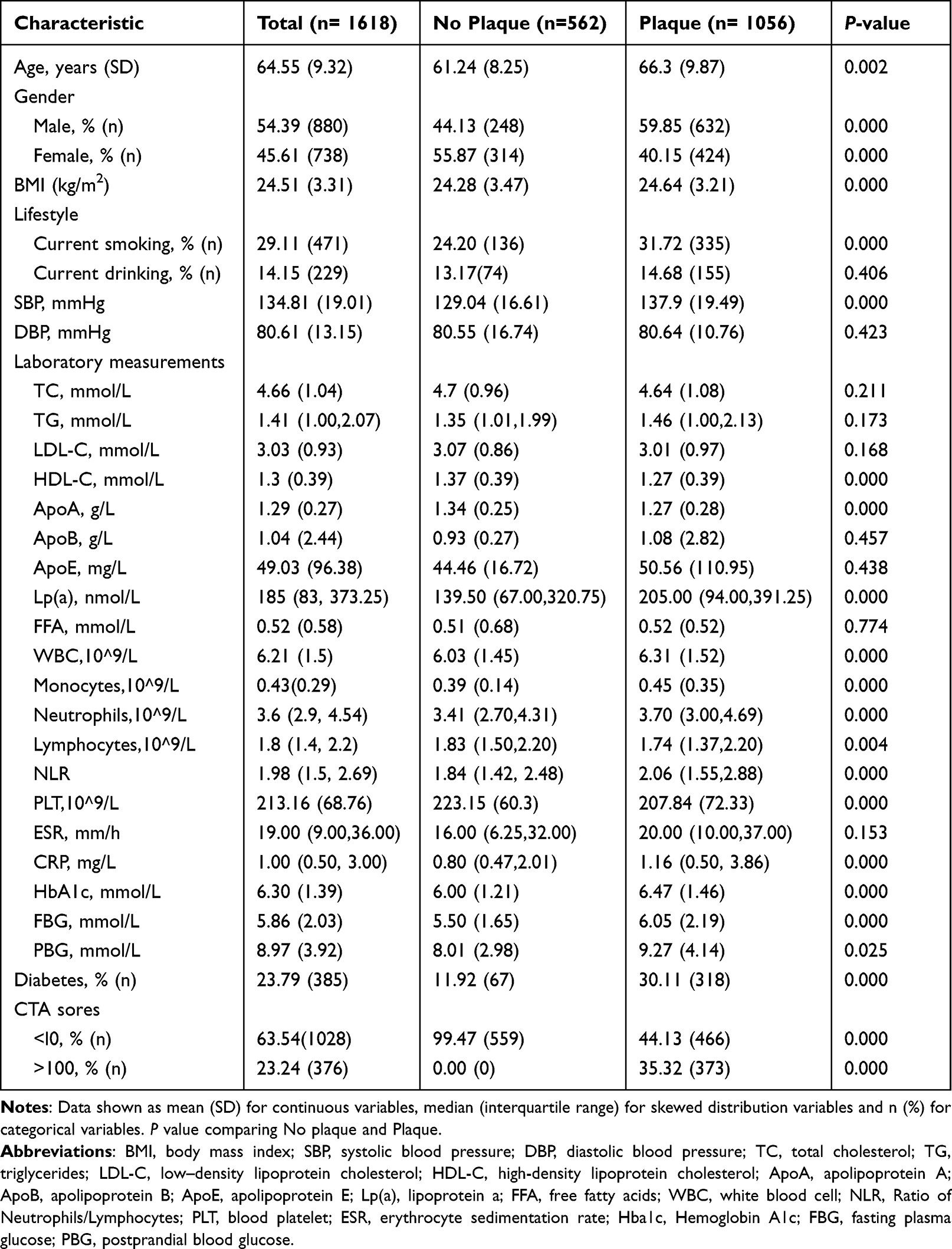 |
Table 1 Demographic and Laboratory Characteristics of the Study Population |
The Values of Demographic and Clinical Characteristics in the Study Groups Categorized by Lp(a) and NLR
In this study, we analyzed the combined effect of Lp(a) and the inflammatory marker NLR on the occurrence of ASCVD and the types of plaque in the patients. The cut-off value of NLR 1.686 was affirmed from the Youden index according to receiver operating characteristic (ROC) curves, and the high Lp(a) level was determined as >75 nmol/L according to the recommendation.24 Consequently, we separated the patients into four groups based on Lp(a) and NLR levels: normal Lp(a) and normal NLR (nLp(a)/NLR-); high Lp(a) and normal NLR (hLp(a)/NLR-); normal Lp(a) and high NLR (nLp(a)/NLR+); high Lp(a) and high NLR (hLp(a)/NLR+), and the values of clinical characteristics among various groups were examined. A total of 58 patients in the study population had a history of PCI. We found no difference in the incidence of in-stent restenosis between the groups by Fisher’s exact test (P > 0.05).
The majority of participants (51.0%) was in the hLp(a)/NLR+ group, followed by hLp(a)/NLR- (26.1%), nLp(a)/NLR+ (13.3%), and nLp(a)/NLR- (9.60%) groups. Compared to the other three groups, the hLp(a)/NLR+ group were older (65.7 vs 61.1, P < 0.05; 65.7 vs 62.3, P < 0.05; and 65.7 vs 63.3 years, P < 0.05; in nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+, respectively). A significant increase of total cholesterol (TC) and LDL-C was observed in patients with high Lp(a) level (Table 2). In comparison to the nLp(a)/NLR- group, the inflammatory markers including WBC counts were considerably higher in nLp(a)/NLR+ group (6.53 10^9/L vs 5.85 10^9/L, P < 0.05), and hLp(a)/NLR+ group had higher WBC counts than hLp(a)/NLR- group (6.46 10^9/L vs 5.70 10^9/L, P < 0.05). The three groups, hLp(a)/NLR-, nLp(a)/NLR+ and hLp(a)/NLR+, all had a significantly higher incidence of ASCVD than nLp(a)/NLR- group (34.12% vs 18.06%; 31.02% vs 18.06%; 66.30% vs 18.06%, P < 0.05) (Table 2). These results suggest that the hLp(a)/NLR+ group has the highest incidence of ASCVD.
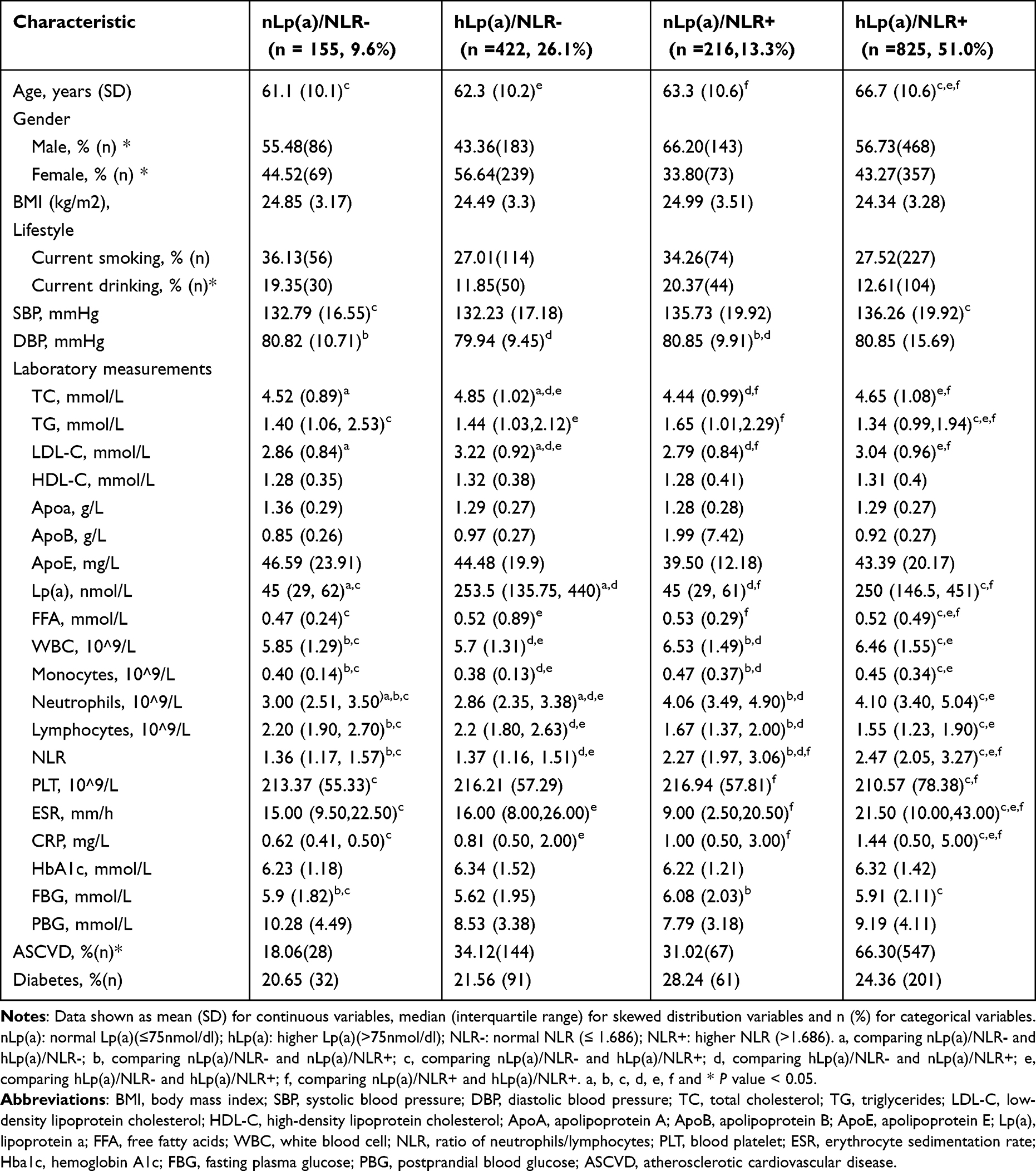 |
Table 2 The Clinical Characteristics of the Study Group Categorized by Lp(a) and NLR |
The Changes of Plaque Traits in the Study Groups Categorized by Lp(a) and NLR
According to a previous study, CTA-based plaque classification had enhanced risk stratification over coronary calcium score (CAC) in symptomatic patients with suspected CAD.22 Unstable plaques are easy to disrupt and then are prone to thrombosis. Therefore, we evaluated the different types of coronary artery plaques and the results are shown in Table 3.
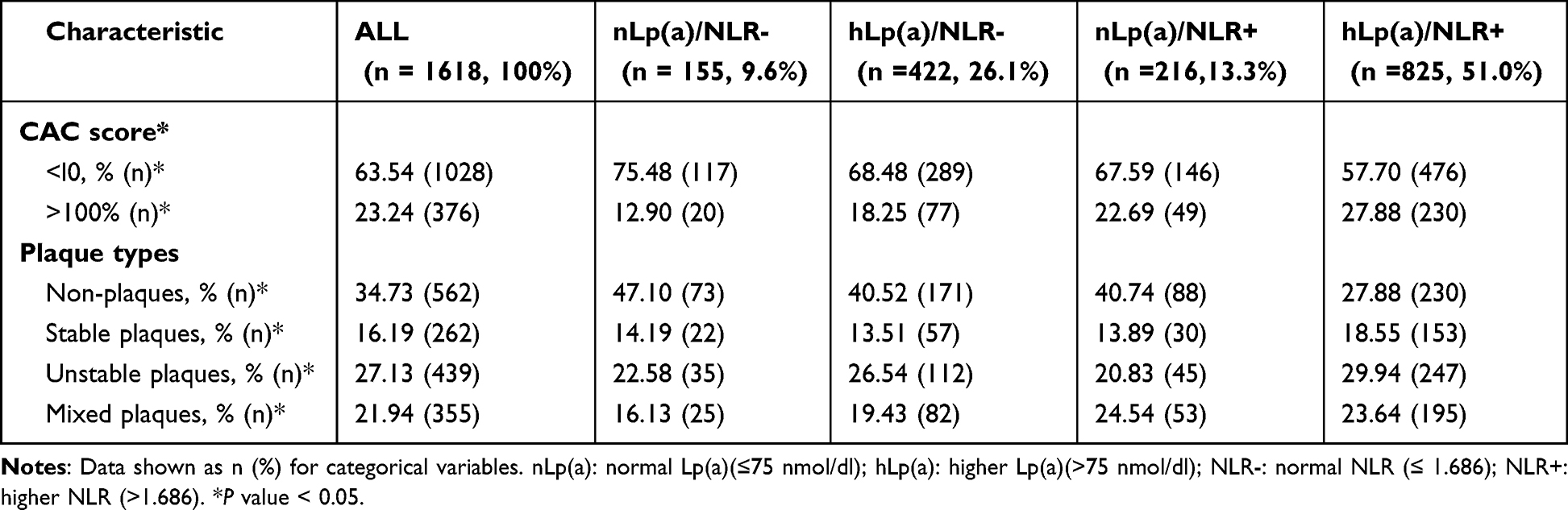 |
Table 3 Plaque Analysis in Coronary Arteries and Branches |
Compared to the other three groups, the hLp(a)/NLR+ group had less percentage of non-plaque (27.88% vs 47.10%, 40.52% and 40.74% in nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+, P < 0.05). We found the highest proportion of unstable plaques in the hLp(a)/NLR+ group compared with the other three groups (29.94% vs 22.58%, 26.54% and 20.83% in nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+, respectively, P < 0.05). The hLp(a)/NLR+ group had the highest percentage of patients with moderate and severe-risk CAC scores and the lowest percentage of patients with none-risk CAC score, which was statistically significant (CAC scores >100: 27.88% vs 12.90%, 27.88% vs 18.25%, 27.88% vs 22.69% in nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+, respectively, P < 0.05;CAC scores <l0: 57.70% vs 75.48%, 57.70% vs 68.48%, 57.70% vs 67.59% in nLp(a)/NLR-, hLp(a)/NLR-, nLp(a)/NLR+, respectively, P < 0.05). These results suggest that the hLp(a)/NLR+ group has the highest risk of moderate and severe CAC and unstable plaque scores than other groups.
The Unstable Plaque Risk in the Study Groups Categorized by Lp(a) and NLR
Using patients of the nLp(a)/NLR- as the reference group, the hLp(a)/NLR+ group had the highest risk of stable plaque (OR = 2.21; 95% CI = 1.31–3.71, P = 0.003). However, no statistically significant difference of increased stable plaque risk was found in the hLp(a)/NLR+ group (OR = 1.73, 95% CI = 0.96–3.10, P = 0.066) after adjusting for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC and Statins. The hLp(a)/NLR+ group also had the highest risk of unstable plaque compared to patients of the nLp(a)/NLR- group as the reference group (OR = 2.24; 95% CI = 1.44–3.48, P = 0.000). Moreover, the hLp(a)/NLR+ group still had the highest risk of unstable plaque with OR = 1.67 (95% CI = 1.04–2.68, P = 0.035) after adjusting for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC and Statins (Figure 2). These results demonstrate that the higher level of combined Lp(a) and NLR is related to the enhanced risk of unstable plaques. In this study, we also analyzed the combined effect of Lp(a) and another inflammatory marker C-Reactive Protein (CRP) on the occurrence of ASCVD and the types of plaque in the patients. The high CRP level was determined as ≥2mg/L according to the previous study.28 The hLp(a)/CRP+ group had the highest risk of stable and unstable plaque with OR = 2.92 (95% CI = 1.64–5.22, P = 0.000) and OR = 2.13 (95% CI = 1.34–3.39, P = 0.001) after adjusting for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC and Statins (Supplement Figure 1). These results suggest that elevated levels of Lp(a) and CRP associated with both stable and unstable plaque.
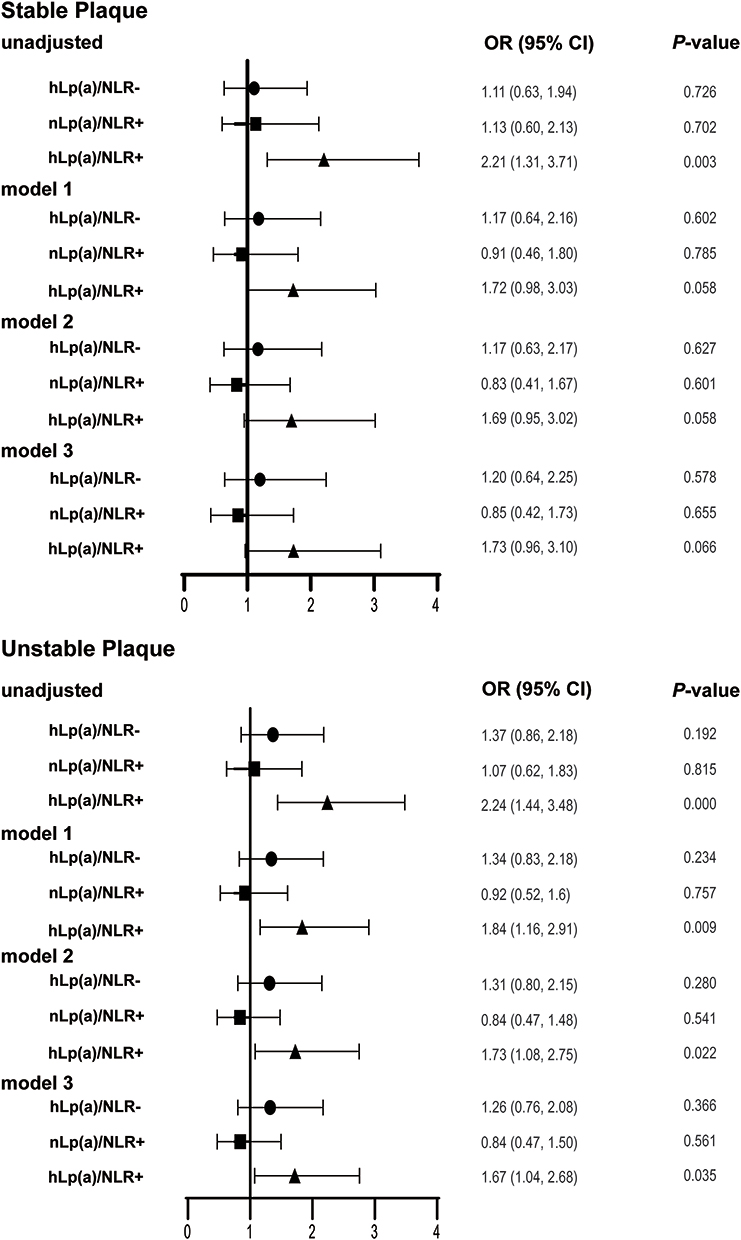 |
Figure 2 Odds ratios (ORs) of plaque traits of the study groups categorized by Lp(a) and NLR. Notes: nLp(a): normal Lp(a) (≤75 nmol/dl); hLp(a): higher Lp(a) (>75 nmol/dl); NLR-: normal NLR (≤1.686); NLR+: higher NLR (>1.686). nLp(a)/NLR- group used as reference. Model 1: Data adjusted for age, sex. Model 2: Data adjusted for age, sex, smoking status, hypertension, diabetes. Model 3: Data adjusted for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC, Statins. |
The ASCVD Risk in the Study Groups Categorized by Lp(a) and NLR
The concomitant presence of elevated Lp(a) and higher NLR were significantly related to moderate and severe-risk CAC scores and ASCVD (Figure 3). These results indicated only a statistically significant difference of enhanced risk of moderate and severe-risk CAC scores (CAC scores >100) with the hLp(a)/NLR+ group with OR = 1.73 (95% CI = 1.02–2.94, P = 0.042) after adjusting for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC and Statins in logistic regression models (Figure 3, Model 3). The crude and adjusted combined association of Lp(a) and NLR for the prevalence of ASCVD are illustrated in Figure 3. Using the nLp(a)/NLR- group as the reference group, the patients in hLp(a)/NLR-, nLp(a)/NLR+, and hLp(a)/NLR+ groups had increased incidence of ASCVD with OR = 1.68 (95% CI = 1.06–2.67, P = 0.028), OR = 2.04 (95% CI = 1.24–3.36, P = 0.005), and OR = 3.15 (95% CI = 2.04–4.85, P = 0.000), respectively. The hLp(a)/NLR+ group also had the highest ASCVD with OR = 2.39 (95% CI = 1.49–3.83, P = 0.000) after adjusting for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC and Statins in model 3 (Figure 3). These results suggest that elevated levels of Lp(a) and NLR are significantly associated with an increased incidence of ASCVD. In this study, we also found that the higher level of combined Lp(a) and CRP is related to the enhanced risk of moderate and severe-risk CAC scores and increased incidence of ASCVD (Supplement Figure 2).
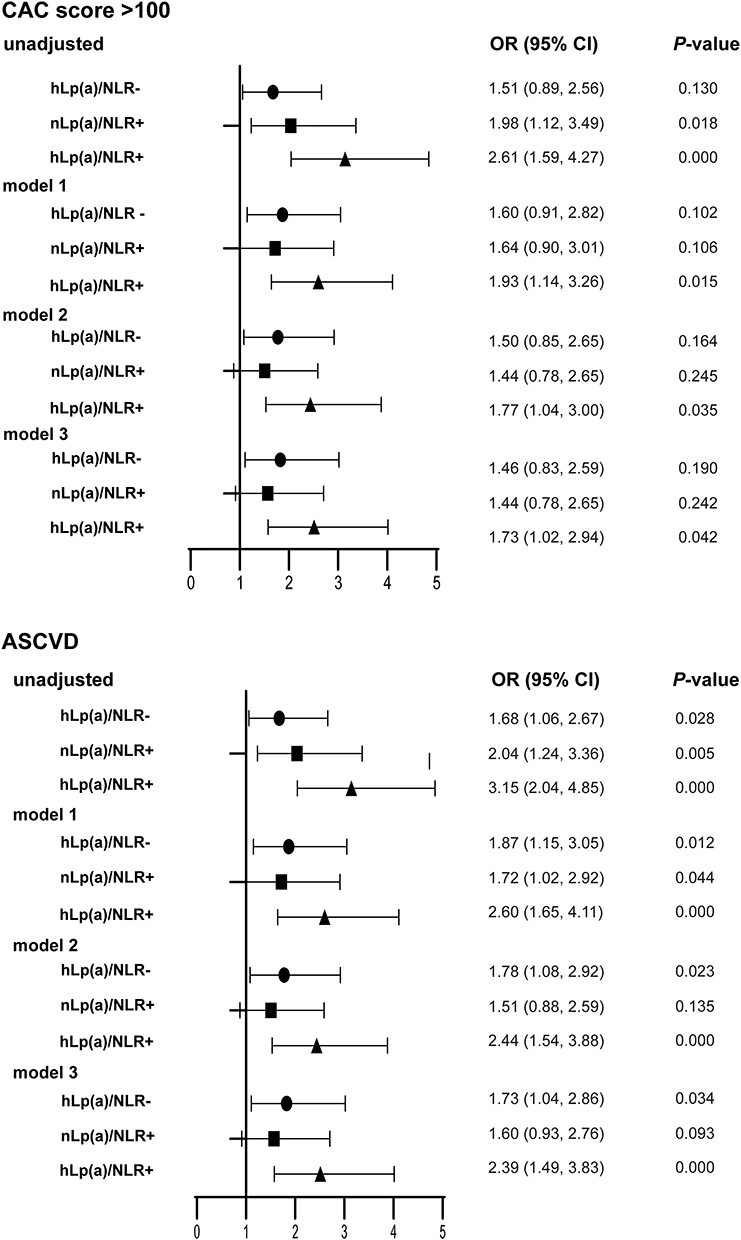 |
Figure 3 Odds ratios (ORs) of moderate and severe-CAC scores and ASCVD of the study groups categorized by Lp(a) and NLR. Abbreviation: ASCVD, atherosclerotic cardiovascular disease. Notes: nLp(a): normal Lp(a) (≤75 nmol/dl); hLp(a): higher Lp(a) (>75 nmol/dl); NLR-: normal NLR (≤1.686); NLR+: higher NLR (>1.686). nLp(a)/NLR- group used as reference. Model 1: Data adjusted for age, sex. Model 2: Data adjusted for age, sex, smoking status, hypertension, diabetes. Model 3: Data adjusted for age, sex, smoking status, hypertension, diabetes, HDL-C, TG, TC, Statins. |
Greater Association of Elevated Lp(a) and NLR with ASCVD
As accurate diagnosis of ASCVD is important for guiding future treatment, we attempted to use the combination of Lp(a) and NLR to identify the patients with greater ASCVD. We found that 4 variables, age, HbA1c, Lp(a), NLR, had the greater area under receiver operating characteristic curve (AUC) in the validation sets for ASCVD association, with the greatest AUC for the variables combination (Figure 4). The predictive value of combination for patients with ASCVD was AUC = 0.733 (95% CI = 0.705–0.760, P = 0.014), which had a better predictive value than Lp(a) AUC = 0.572 (95% CI = 0.543–0.601, P = 0.015), NLR AUC = 0.593 (95% CI = 0.564–0.622, P = 0.015), age (AUC = 0.679, 95% CI = 0.651–0.706, P = 0.014) and HbA1c (AUC = 0.642, 95% CI = 0.611–0.673, P = 0.016). These results indicate that the combined Lp(a) and NLR might improve ASCVD risk evaluation.
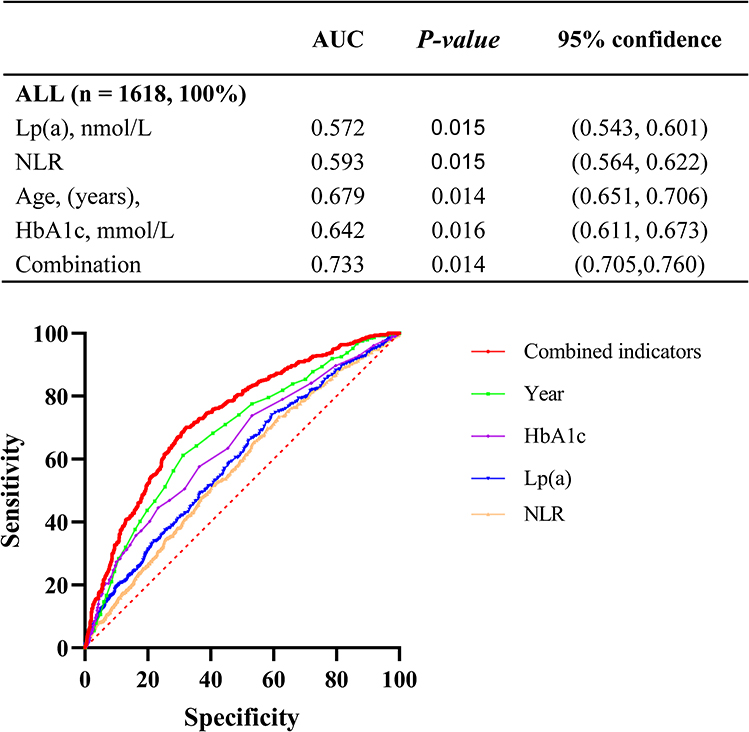 |
Figure 4 ROC curve analysis for predicting ASCVD. Abbreviations: AUC, area under the curve; Lp(a), lipoprotein(a); Hba1c, hemoglobin A1c; Combined indicators, the combined indicators of Lp(a), Neutrophils/Lymphocytes, age and HbA1c. |
Discussion
According to the 2018 AHA/ACC cholesterol guideline and the 2019 ACC/AHA guideline on primary prevention of cardiovascular disease, Lp(a) and hsCRP were used as biomarkers aiding in ASCVD risk evaluation for primary prevention.29,30 In this study, we recruited the middle-aged and elderly patients who had CTA for quantification of coronary atherosclerotic plaques and the level of Lp(a) and NLR were measured in the patients. The hLp(a)/NLR+ group had the highest risk of unstable plaque and increased incidence of ASCVD compared with other three groups. Therefore, we conclude that Lp(a) and NLR are strongly associated with ASCVD and the occurrence of unstable plaques in the patients.
Lp(a) is reported to be related to the development of MI, stroke, and calcific aortic valve stenosis, according to epidemiologic and genetic studies, and post hoc analysis of the clinical trials.2,4,5,8 There is a linear relationship between high Lp(a) levels and ASCVD, according to a meta-analysis of various statin trials with 95,576 person-years at risk and 5751 occurrences.8 We discovered that the patients with atherosclerotic plaques at Shanghai East Hospital between 2012 and 2013 had elevated plasma level of Lp(a) and NLR. Regarding Lp(a)’s effects, plasminogen activation inhibition in the context of fibrin clots has received the majority of attention.31,32 Lp(a) might accelerate the coagulation cascade, activate platelets to aggregate, or change the structure of fibrin clots to be more resistant to lysis.33–36 Further, we may investigate the effects of Lp(a) on various forms of atherosclerotic plaques and the specific mechanisms of Lp(a) affecting atherosclerotic plaque traits.
Chronic systemic inflammation has been identified as a key factor in residual cardiovascular risk. It is frequently observed as a pathophysiological characteristic of metabolic syndrome.4,37 The neutrophil-to-lymphocyte ratio (NLR) is an inflammatory biomarker that correlates with mortality rates due to congestive heart failure and can predict the likelihood of death in patients with acute coronary syndromes and the incidence of cardiac arrhythmias.38–40 The higher NLR indicates an increased risk of atherosclerotic disease when the WBC counts are within the usual range.16 The NLR, in contrast to many other inflammatory indicators, is easily accessible and affordable, and it offers additional risk classification beyond traditional markers.41
Atherosclerosis has a complicated etiology, with vascular wall inflammation, lipid buildup, intimal thickening and fibrosis, arterial stiffness, remodeling, and the plaque rupture or erosion being the main risk for myocardial infarction.42 The term “vulnerable plaque” describes a plaque that is more likely to rupture, which would then cause a distal embolization.43 A thin or torn fibrous cap, a necrotic core rich in lipids, intraplaque bleeding, and intraplaque active inflammation are pathological features of susceptible plaque.5 There was no association between CRP and plaque type by CTA, although CRP was the most common inflammatory marker.44 Studies have demonstrated that NLR could be used to predict the existence of susceptible carotid plaque as determined by carotid ultrasonography in patients with acute ischemic stroke among Chinese patients.26 In this study of the Chinese subjects, we confirmed the significant association of high Lp(a) and NLR with unstable plaques and elevated levels of Lp(a) and CRP without association with plaque type after adjustment for age, gender and clinical risk factor. NLR was regarded to be a more accurate indication of unstable plaque than CRP in this study.
There are several limitations in this study which deserve comment. The study is an observational, retrospective and single-center study, and further randomized controlled trials are required to prove that Lp(a) or NLR is a causative risk factor for ASCVD. Second, as neutrophil and lymphocyte numbers alter over time, NLR is a dynamic and time-varying marker. Therefore, further continuously monitoring the NLR is required. In this study, we employed CT angiography to assess ASCVD by measuring the atherosclerotic plaques in the coronary arteries. In the present study, other forms of plaque characteristics pertaining to the CTA patient were not taken into consideration. Therefore, our objective is to persist in the process of enrolling patients who have undergone CTA, in order to procure additional forms of plaque characteristics and update the database. The study had advantages, including a relatively wide age range of participants examined that has not been studied in this depth before, and the general equality of the number of male and female participants makes it easier to examine gender disparities that are obviously present.
In conclusion, we found that Lp(a) and NLR were significantly associated with ASCVD and unstable plaques in these Chinese patients in Shanghai. The high level of Lp(a) was a risk factor for ASCVD, and a stronger association with risk was found by combining high Lp(a) with a high-level NLR. This study may suggest a future recommendation to measure Lp(a) and NLR for coronary atherosclerosis risk estimation in clinical practice, particularly for unstable plaques.
Funding
This study is supported by the National Natural Science Foundation of China (82130016, 81970232, 81970233, 81970234, 82170257), Shanghai Rising-Star Program (20QA1408100, 21QA1401400), Research program of Shenzhen Science and Technology Innovation Committee (JCYJ20190807102605515, JCYJ20220530163601003) and Science and Technology Plan Project of Jiangxi Provincial Health commission (SKJP220227143).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li -J-J, Ma C-S, Zhao D, Yan X-W. Lipoprotein(a) and Cardiovascular Disease in Chinese Population: a Beijing Heart Society Expert Scientific Statement. JACC: Asia. 2022;2(6):653–665. doi:10.1016/j.jacasi.2022.08.015
2. Erqou S, Kaptoge S, Perry PL, et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302(4):412–423.
3. Kamstrup PR, Benn M, Tybjaerg-Hansen A, Nordestgaard BG. Extreme lipoprotein(a) levels and risk of myocardial infarction in the general population: the Copenhagen City Heart Study. Circulation. 2008;117(2):176–184. doi:10.1161/CIRCULATIONAHA.107.715698
4. Ellis KL, Boffa MB, Sahebkar A, Koschinsky ML, Watts GF. The renaissance of lipoprotein(a): brave new world for preventive cardiology. Prog Lipid Res. 2017;68:57–82.
5. Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301(22):2331–2339.
6. Thanassoulis G, Campbell CY, Owens DS, et al. Genetic associations with valvular calcification and aortic stenosis. N Engl J Med. 2013;368(6):503–512.
7. Clarke R, Peden JF, Hopewell JC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361(26):2518–2528.
8. Willeit P, Ridker PM, Nestel PJ, et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: individual patient-data meta-analysis of statin outcome trials. Lancet. 2018;392(10155):1311–1320.
9. Tsimikas S, Hall JL. Lipoprotein(a) as a potential causal genetic risk factor of cardiovascular disease: a rationale for increased efforts to understand its pathophysiology and develop targeted therapies. J Am Coll Cardiol. 2012;60(8):716–721.
10. Liu HH, Cao YX, Jin JL, et al. Association of lipoprotein(a) levels with recurrent events in patients with coronary artery disease. Heart. 2020;106(16):1228–1235.
11. Kaiser Y, Daghem M, Tzolos E, et al. Association of Lipoprotein(a) With Atherosclerotic Plaque Progression. J Am Coll Cardiol. 2022;79(3):223–233.
12. Muramatsu Y, Minami Y, Kato A, et al. Lipoprotein (a) level is associated with plaque vulnerability in patients with coronary artery disease: an optical coherence tomography study. Int J Cardiol Heart Vasc. 2019;24:100382.
13. Tardif JC, Kouz S, Waters DD, et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019;381(26):2497–2505.
14. Araos P, Figueroa S, Amador CA. The role of neutrophils in hypertension. Int J Mol Sci. 2020;21(22):654.
15. Sesti-Costa R, de Moraes-Vieira P, Cervantes-Barragan L. Dendritic cells: immune response in infectious diseases and autoimmunity. Mediators Inflamm. 2020;2020:2948525.
16. Duffy BK, Gurm HS, Rajagopal V, Gupta R, Ellis SG, Bhatt DL. Usefulness of an elevated neutrophil to lymphocyte ratio in predicting long-term mortality after percutaneous coronary intervention. Am J Cardiol. 2006;97(7):993–996.
17. Uthamalingam S, Patvardhan EA, Subramanian S, et al. Utility of the neutrophil to lymphocyte ratio in predicting long-term outcomes in acute decompensated heart failure. Am J Cardiol. 2011;107(3):433–438.
18. Kalay N, Dogdu O, Koc F, et al. Hematologic parameters and angiographic progression of coronary atherosclerosis. Angiology. 2012;63(3):213–217.
19. Lee CD, Folsom AR, Nieto FJ, Chambless LE, Shahar E, Wolfe DA. White blood cell count and incidence of coronary heart disease and ischemic stroke and mortality from cardiovascular disease in African-American and White men and women: atherosclerosis risk in communities study. Am J Epidemiol. 2001;154(8):758–764.
20. Chalela JA. Evaluating the carotid plaque: going beyond stenosis. Cerebrovasc Dis. 2009;27(Suppl 1):19–24.
21. Li X, Li J, Wu G. Relationship of Neutrophil-to-Lymphocyte Ratio with Carotid Plaque Vulnerability and Occurrence of Vulnerable Carotid Plaque in Patients with Acute Ischemic Stroke. Biomed Res Int. 2021;2021:6894623.
22. Cury RC, Abbara S, Achenbach S, et al. CAD-RADS(TM) Coronary Artery Disease - Reporting and Data System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016;10(4):269–281.
23. Chinese Association of Radiologists. Chinese Association of Radiologists. Chin J Radiol. 2022;56(6):595–607.
24. Beijing Heart Association. Expert Statement on the Relationship Between Lipoprotein(a) and Cardiovascular Disease Risk and Clinical Management. Chin Circulation J. 2021;36(12):1158–1167.
25. Peng S, Shen T, Liu J, et al. Uncontrolled Hypertension Increases with Age in an Older Community-Dwelling Chinese Population in Shanghai. Aging Dis. 2017;8(5):558–569.
26. Austen WG, Edwards JE, Frye RL, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975;51(4 Suppl):5–40.
27. Goff DC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2935–2959.
28. Zhang W, Speiser JL, Ye F, et al. High-Sensitivity C-Reactive Protein Modifies the Cardiovascular Risk of Lipoprotein(a): multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol. 2021;78(11):1083–1094.
29. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1046–e1081.
30. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596–e646.
31. Hancock MA, Boffa MB, Marcovina SM, Nesheim ME, Koschinsky ML. Inhibition of plasminogen activation by lipoprotein(a): critical domains in apolipoprotein(a) and mechanism of inhibition on fibrin and degraded fibrin surfaces. J Biol Chem. 2003;278(26):23260–23269.
32. Romagnuolo R, Marcovina SM, Boffa MB, Koschinsky ML. Inhibition of plasminogen activation by apo(a): role of carboxyl-terminal lysines and identification of inhibitory domains in apo(a). J Lipid Res. 2014;55(4):625–634.
33. Undas A, Plicner D, Stepień E, Drwiła R, Sadowski J. Altered fibrin clot structure in patients with advanced coronary artery disease: a role of C-reactive protein, lipoprotein(a) and homocysteine. J Thromb Haemost. 2007;5(9):1988–1990.
34. Undas A, Slowik A, Wolkow P, Szczudlik A, Tracz W. Fibrin clot properties in acute ischemic stroke: relation to neurological deficit. Thromb Res. 2010;125(4):357–361.
35. Undas A, Cieśla-Dul M, Drążkiewicz T, Sadowski J. Altered fibrin clot properties are associated with residual vein obstruction: effects of lipoprotein(a) and apolipoprotein(a) isoform. Thromb Res. 2012;130(3):e184–7.
36. Skuza AA, Polak M, Undas A. Elevated lipoprotein(a) as a new risk factor of cerebral venous sinus thrombosis: association with fibrin clot properties. J Thromb Thrombolysis. 2019;47(1):8–15.
37. Dandona P, Aljada A, Chaudhuri A, Mohanty P, Garg R. Metabolic syndrome: a comprehensive perspective based on interactions between obesity, diabetes, and inflammation. Circulation. 2005;111(11):1448–1454.
38. Curran FM, Bhalraam U, Mohan M, et al. Neutrophil-to-lymphocyte ratio and outcomes in patients with new-onset or worsening heart failure with reduced and preserved ejection fraction. ESC Heart Fail. 2021;8(4):3168–3179.
39. Li S, Chen H, Zhou L, Cui H, Liang S, Li H. Neutrophil-to-lymphocyte ratio predicts coronary artery lesion severity and long-term cardiovascular mortality in patients with unstable angina pectoris. Acta Cardiol. 2022;77(8):708–715.
40. Silberman S, Fink D. Neutrophil to Lymphocyte Ratio and Risk of Atrial Fibrillation. Am J Cardiol. 2019;123(11):1889.
41. Wang R, Chen PJ, Chen WH. Diet and exercise improve neutrophil to lymphocyte ratio in overweight adolescents. Int J Sports Med. 2011;32(12):982–986.
42. Fairweather D. Sex differences in inflammation during atherosclerosis. Clin Med Insights Cardiol. 2014;8(Suppl 3):49–59.
43. Tomaniak M, Katagiri Y, Modolo R, et al. Vulnerable plaques and patients: state-of-The-art. Eur Heart J. 2020;41(31):2997–3004.
44. Navaravong L, Steenson C, Sigurdsson G. Coronary plaque type and burden by computed tomography angiography without association to C-reactive protein. N Am J Med Sci. 2014;6(6):260–265.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.