")
Back to Journals » International Journal of Women's Health » Volume 14
The Association of Conflict-Related Trauma with Markers of Mental Health Among Syrian Refugee Women: The Role of Social Support and Post-Traumatic Growth
Authors Kheirallah KA , Al-Zureikat SH, Al-Mistarehi AH , Alsulaiman JW, AlQudah M , Khassawneh AH, Lorettu L, Bellizzi S, Mzayek F, Elbarazi I , Serlin IA
Received 29 January 2022
Accepted for publication 19 July 2022
Published 5 September 2022 Volume 2022:14 Pages 1251—1266
DOI https://doi.org/10.2147/IJWH.S360465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Khalid A Kheirallah,1 Sarah H Al-Zureikat,1 Abdel-Hameed Al-Mistarehi,1 Jomana W Alsulaiman,2 Mohammad AlQudah,1 Adi H Khassawneh,1 Liliana Lorettu,3 Saverio Bellizzi,4 Fawaz Mzayek,5 Iffat Elbarazi,6 Ilene A Serlin7
1Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Faculty of Medicine, Yarmouk University, Irbid, Jordan; 3Psychiatric Clinic, University of Sassari, Sassari, Italy; 4World Health Organization (WHO), Jordan Country Office, Amman, Jordan; 5School of Public Health, The University of Memphis, Memphis, TN, USA; 6Institute of Public Health, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 7International Institute for Advanced Training in Dance Movement Therapy, San Francisco, CA, USA
Correspondence: Khalid A Kheirallah, Department of Public Health, Community Medicine, and Family Medicine, Medical School of Jordan University of Science and Technology, P.O. Box: 3030, Irbid, 22110, Jordan, Tel +962 7 9611 9094, Email [email protected] Abdel-Hameed Al-Mistarehi, Department of Public Health, Community Medicine, and Family Medicine, Faculty of Medicine, Jordan University of Science and Technology, P.O.Box: 630001, Irbid, 22110, Jordan, Tel +962 7 9828 4360, Email [email protected]
Background: Syrian refugee women not only suffered the refuging journey but also faced the burden of being the heads of their households in a new community. We aimed to investigate the mental health status, traumatic history, social support, and post-traumatic growth (PTG) of Syrian refugee women.
Methods: A cross-sectional study was conducted using a structured interviewer-administered survey between August and November 2019. Syrian refugee women who head their households and live outside camps were eligible. The survey included items investigating socio-demographic characteristics and conflict-related physical trauma history. The Refugee Health Screener-15 (RHS-15) scale was used to screen for emotional distress symptoms of depression, anxiety, and post-traumatic stress disorder (PTSD), with a score range of 0− 4 and higher scores indicating emotional distress. The Multidimensional Scale of Perceived Social Support (MSPSS) was utilized to assess the perceived support from family, friends, and significant others (score range 1− 7), with scores of 3− 5 and 5.1− 7.0 representing moderate and high support, respectively. The PTG Inventory (PTGI) scale investigated the positive transformation following trauma; the score range was 0− 5, and the cutoff point of ≥ 3 defined moderate-to-high growth levels.
Results: Out of 140 invited refugee women, 95 were included, with a response rate of 67.9%. Their mean (SD) age was 41.30 (11.75) years, 50.5% were widowed, and 17.9% reported their husbands as missing persons. High levels of conflict-related traumatic exposure were found, including threats of personal death (94.7%), physical injury (92.6%), or both (92.6%); and a history of family member death (92.6%), missing (71.6%), or injury (53.7%). The mean (SD) RHS-15 score was above average (2.08 (0.46)), and most women (90.5%) were at high risk for depression, anxiety, and PTSD symptoms. The mean (SD) MSPSS score was 5.08 (0.71), representing moderate social support, with friends’ support being the highest (5.23 (0.85)). The mean (SD) PTGI score was 2.44 (0.48), indicating low growth, with only 12.6% of women experiencing moderate-to-high growth levels. Spiritual change and personal strength had the highest sub-scores, with moderate-to-high growth levels experienced by 97.9% and 84.2%, respectively. Most women were more optimistic and religious, had feelings of self-reliance and better difficulties adapting, and were stronger than they thought. Statistically significant correlations of MSPSS and its subscales with RHS-15 and PTGI were detected.
Conclusion: Significant but unspoken mental health problems were highly prevalent among Syrian refugee women and an imminent need for psychological support to overcome traumatic exposure. The role of social support seems to be prominent and needs further investigation.
Keywords: refugee, women, Syrian, mental health, social support, trauma growth, Jordan, MSPSS, RHS-15, PTGI
Introduction
Syrian Refuging Journey and Its Mental Health Effects
The ongoing conflict in Syria has caused the largest refugee crisis of our time. In early 2020, with Syria’s war heading into its tenth year, the United Nations High Commissioner for Refugees (UNHCR) identified 656,501 registered Syrian refugees residing in Jordan.1 Syrian refugees faced various traumatic events during their journey to Jordan and neighboring countries following the outbreak of the armed conflict around 2010. Exposure to atrocities of war, displacement, and the stress of resettling in a new hosting community were expected to affect the refugees’ mental health and well-being.2
Emotional disorders are the most common mental illnesses among Syrian refugees, as with many victims of conflicts and displacement.3,4 These disorders include depression, excessive sadness, post-traumatic stress disorder (PTSD), and anxiety disorders.5,6 The long-term mental health effects of conflict on Syrian refugees were estimated between 4.4% and 86% for PTSD, 20.3% and 88% for anxiety, and 2.3% and 80% for depression.7 In Turkey, 33.5% of Syrian refugees reported significant symptoms of PTSD.8 In Lebanon, postnatal depression symptoms were significantly higher among Syrian refugee mothers than in their Lebanese counterparts.9 Several traumatic events were associated with Syrian refugees, including physical torture, death threat, starvation,10 death threats to family members or friends,11 and war proximity.12 As a post-migration factor, living in a camp and not being satisfied with its conditions were also independently related to the high probability of developing depression.13 In Jordan, the prevalence of PTSD among Syrian refugee adults was estimated at 18.4%.14 In-depth interviews with 24 Syrian refugee women living in Jordan revealed several clinical and psychological symptoms attributed to war and displacement stressors, including weight loss, headaches, generalized pain, and other health problems.15
Post-Traumatic Growth (PTG)
Post-Traumatic Growth (PTG) is the positive psychological change after struggling with challenging life circumstances.16 PTG Inventory (PTGI) is an effective measure to assess positive life changes after a traumatic event experience.17 Female gender, low educational level, and trauma load were significant predictors for PTSD, while resilience and PTG were suggested to protect against PTSD.18 For refugees who lost their pre-conflict social life, relying on extended family support networks and communities is often regarded as the most important social support system.19 Strong ties with social networks were suggested to play a significant role in emotional well-being, provide support, and expand employment and education opportunities. Therefore, the lack of social support could be a crucial mental health risk factor among refugees, as the war is ongoing in the country of origin.5,20
Study Importance and Objectives
The sudden change in gender roles forced Syrian women to become heads of their households and created tremendous strains on refugees.21–23 Such change was not gradual in lifestyle, but relatively quick and sudden, caused by loss and displacement.24 The literature review of mental health assessments among Syrian refugees did not give sufficient attention to women who head their households or live outside camps within host communities.14,15 This vulnerable group represents a significant portion of refugees in Jordan. The UNHCR reported that around 80% of registered Syrian refugees in Jordan live outside refugee camps.1 Given the significant concerns regarding the effects of conflict and displacement on women, it is essential to understand better the mental health status resulting from the challenges refugees face to inform policymakers and improve psychosocial support services. This exploratory study aimed to screen for common mental health disorders and assess their correlation with the exposure to conflict-related traumatic events, perceived social support, and PTG among Syrian refugee women who were the primary head of their households and living outside camp settings in host communities in Jordan.
Materials and Methods
Study Design and Participants
This cross-sectional study collected data using a structured interviewer-administered questionnaire. Interviews were conducted between August and November 2019 by one female researcher who had advanced training in administering mental health screening questionnaires and was well known to most women included in the study as per the nature of her social work with refugee communities.
UNHCR-registered Syrian refugee women who lived in urban areas in the capital of Jordan, Amman, and were heads of their households were identified as potential candidates for participating in this study. A list of addresses was obtained from the Non-Governmental Organizations (NGOs) working with refugee women in Amman. However, NGOs working in mental health were not approached, and women receiving mental health services from these NGOs were excluded. These exclusion criteria were applied to preserve the homogeneity of the sample and achieve the study objectives of screening for mental health symptoms among Syrian refugee women as an exploratory study. Also, women younger than 18 years were excluded.
Study Instruments
The questionnaire consisted of five main sections. The researcher entered the answers to the questions directly into an iPad using the Google Forms tool. The questionnaire validity was tested in a pilot study that included 40 random participants, who assessed the questions’ clarity, and no significant modifications were required. The survey started with an introductory statement providing a piece of information about the study’s aims and consent to participate. Once the participant accepted participation, the questionnaire showed up to be filled out.
Section 1. Socio-Demographics
Participants first completed socio-demographic characteristics including age, marital status as a single, divorced, widowed, or married, having children living in the same household, highest education level, smoking status, and area of living in Syria before being a refugee. Also, questions about the refuging journey of participants were asked, including the number of years of being a refugee outside Syria, whether they were forced for displacement inside or outside Syria before arrival to Jordan, and whether their residency history in Jordan was within the camp settings, non-camp settings, or both. Further, the participants’ financial status was investigated, including whether being financially responsible or not and currently working in a job with a salary in Jordan.
Section 2. Conflict-Related Physical Trauma History
Participants were asked six yes-no questions about their personal or family-related physical trauma history and experience. During the Syrian conflict: “Have you been exposed to a death-like event?”, “Have you had a conflict-related incident that would expose you to physical injury?”, “Have you experienced a conflict-related physical injury?”, “Do you have any of your family members ‘missing’ due to the conflict in Syria?”, “Have you lost (death) a family member due to the conflict in Syria?”, “Was any of your family members physically injured due to the conflict in Syria?”.
One trauma index (Personal death and physical injury threats), consisting of the first two questions about the personal threat of death and the personal threat of injury, was created to indicate whether refugee women experienced either personal death threat, physical injury threat, or none (coded 0), or both personal death and physical injury threats (coded as 1). The Cronbach’s alpha coefficient of the one trauma index was 0.904, indicating high reliability. In contrast, the internal consistency reliability of the other conflict-related trauma questions was less than 0.300, indicating a rather reliability.
Section 3. Screening for PTSD, Depression, and Anxiety
Refugee Health Screener-15 (RHS-15) is a 15-item, efficient, and validated screening tool used to detect the distressing somatic symptoms of depression, anxiety, and PTSD among newly arrived refugees and has been validated in Arabic.25–27 This tool was developed in 2011 by the Pathways to Wellness: Integrating Community Health and Well-being project.26,27 The first 13 items include PTSD, anxiety, and depression symptoms. These symptoms are rated based on disturbing in the past month using a 5-point Likert scale (0 = “not at all” to 4 = “extremely”). Another item assesses the ability to handle stress (coping) on a 5-point Likert scale (0 = “Able to cope with anything” to 4 = “Able to cope with nothing”). The scores of the first 14 items of the RHS-15 scale, including the 13 symptom and one coping item responses, were added and then divided by 14 to obtain the RHS-15 score for each patient. Thus, the RHS-15 score ranges between 0 and 4, with higher scores indicating emotional distress. The last item is the Distress Thermometer (DT), with a response ranging from 0 at the bottom to 10 at the top. The zero-response means “No distress and things are good”, while the ten response means “Extreme distress and I feel as bad as I ever have”. A positive case with a high risk for depression, anxiety, and PTSD symptoms is defined as either a sum score of the first 14 items of the RHS-15 scale ≥12 or a score of ≥5 on the DT item.25,27,28 Hollifield et al, 2013 reported sensitivity values of 0.87, 0.96, and 0.98 for PTSD, anxiety, and depression, respectively, at the predetermined cutoff point.25
Section 4. Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) is a 12-item instrument used to assess perceived social support from three sources: family, friends, and significant other persons.29 Thus, the MSPSS includes three subscales (family, friends, and significant others), each consisting of four items, which are scored on a 7-point Likert scale (1 = “Strongly disagree” to 7 = “Strongly agree”). The scores of the total MSPSS scale and subscales were averaged over items. The sub-score of each subscale was calculated by summing its four items’ scores and then dividing by four; thus, the sub-score ranges between 1 and 7. The sum of sub-scores of the three subscales and dividing by three represents the total score for the full MSPSS scale; thus, it ranges from 1 to 7. The lower scores indicated lower levels of social support, with a mean score from 1 to 2.9 considered low support, while mean scores of 3−5 and 5.1−7.0 represented moderate and high support categories, respectively.29–32 The Arabic version of MSPSS was validated elsewhere.33–35
Section 5. Post-Traumatic Growth Inventory (PTGI)
It is essential to determine the tendency to perceive benefits arising from experiences with trauma. PTGI scale assessed perceived positive life changes following a traumatic experience.17,36,37 It is composed of 21 items included in five subscales: relating to others (7 items), new possibilities (5 items), personal strength (4 items), spiritual change (2 items), and appreciation of life (3 items). A 6-point Likert scale ranging from 0 (“I did not experience this change as a result of my crisis”) to 5 (“I experienced this change to a very great degree as a result of my crisis”) was used for each item. Similar to RHS-15 and MSPSS, the total PTGI scale and subscales were averaged over items by adding the scores of items for each patient, then dividing by the number of items. Thus, the total PTGI score ranges from 0 to 5.17,36,37 The higher total PTGI score indicates that the person has undergone a positive transformation and perceived the development of greater PTG resulting from their traumatic experience. The PTGI score or sub-scores of ≥ 3 was defined as the cutoff point for the moderate-to-high positive transformation and PTG.37–39 This scale was validated in Arabic elsewhere.40
Ethical Considerations
The eligible participants were informed about the study objectives and design before participation. Anonymity, and information confidentiality were assured. Written informed consent was obtained from each participant. Participants were informed that they could terminate the survey at any time desired. No monetary compensation or rewards were received for participation in this study. All participants were offered to be referred for psychosocial support services in collaboration with NGOs in Jordan. The Institutional Review Board (IRB) of Jordan University of Science and Technology approved this study (IRB number is 519/2019). This study was conducted following the 1975 Helsinki declaration, revised in 2008, and later amendments or comparable ethical standards. This study was funded by the Faculty of Research at Jordan University of Science and Technology, with a grant number of 20190473. Copyright permissions to utilize and reproduce the RHS-15 and PTGI scales were obtained.
Statistical Analysis
Data were analyzed using the IBM Statistical Package for the Social Sciences (SPSS) software for Windows, version 24.0 (IBM Corp., Armonk, NY, USA). Categorical variables, including socio-demographic characteristics and conflict-related physical trauma history estimates, were presented as frequencies and percentages. The continuous variables, including age and scale scores, were presented as means (SD) and medians after verifying the normality distribution of the datasets. The mean and median scores for the RHS-15, MSPSS, and PTGI were calculated and reported.
The independent Student’s t-test or one-way analysis of variance (ANOVA) was used to compare the mean scores of the used scales by conflict-related physical trauma events. Avoidance of the violation of the Student’s t-test and one-way ANOVA assumptions was checked.41 A Shapiro–Wilk test was conducted and demonstrated that the dataset was normally distributed with acceptable z-scores (−1.96 and +1.96) for the skewness and keratosis values.42–44 Also, based on the central limit theorem, our sample size is sufficient to conduct parametric statistical tests, including Student’s t-test and one-way ANOVA.45 Moreover, the observations within this study were collected and sampled randomly and independently of each other.
The Pearson Correlation (r) test was used to evaluate the association between the three scales, including PTGI, RHS-15, and MSPSS, as well as MSPSS subscales. A p-value of 0.05 or less was considered for statistical significance. Reliability analysis was conducted for the one trauma index and the other conflict-related physical trauma questions, and Cronbach’s Alpha was also reported.
Results
Out of 140 invited refugee women, 95 participated and were included in this study, with a response rate of 67.9%. Most dropouts were due to the inability to find time to participate in the study and concerns over privacy issues, as informed by the invited participants. The mean (SD) age of participants was 41.30 (11.75) years, and their median age was 39 years. Half of the participants (50.5%) were widowed, and 17.9% were married but reported lacking information about their husbands (missing persons). Most participating women (87.4%) reported having children who live with them. Table 1 shows the participants’ socio-demographics.
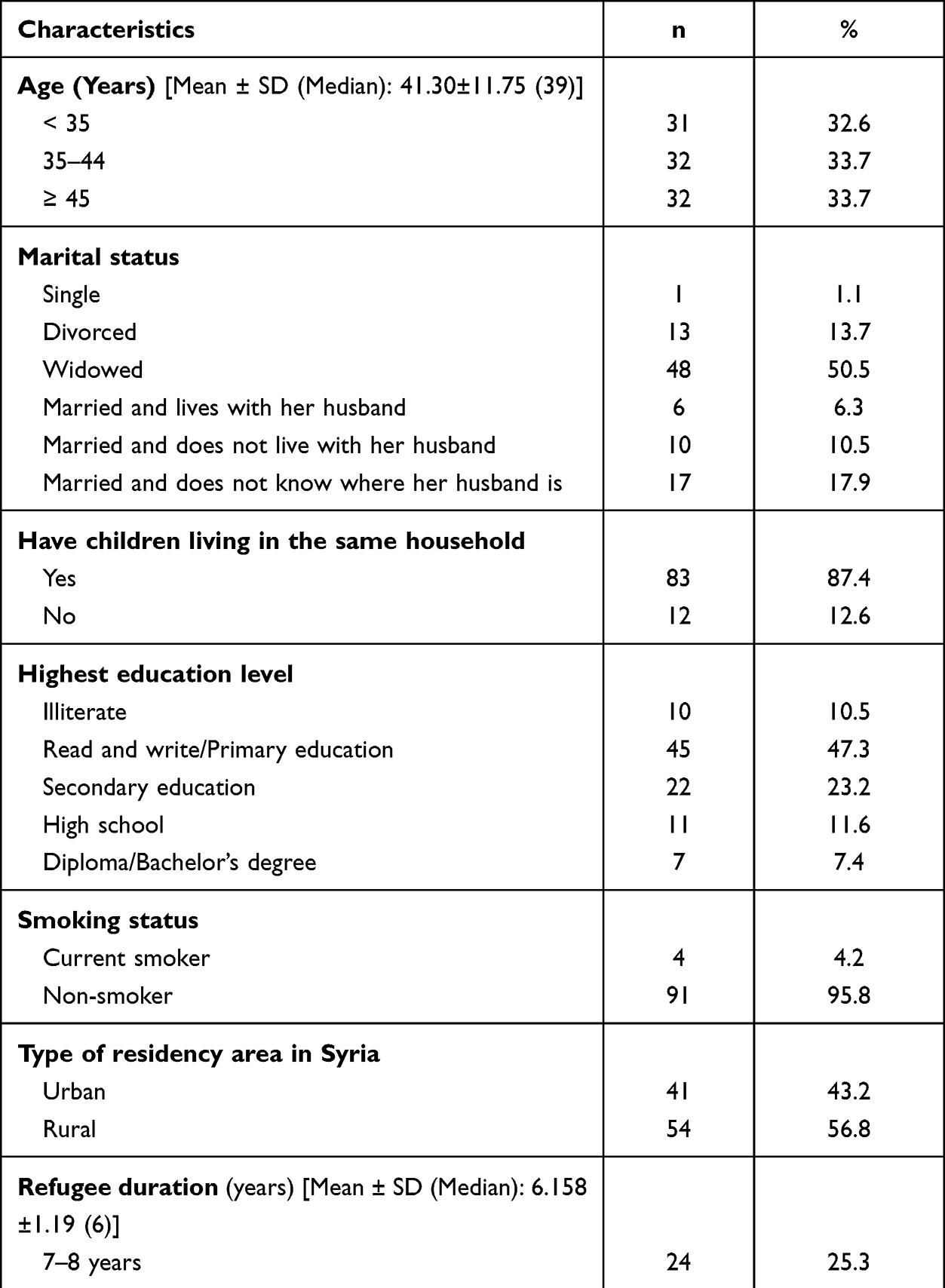 |
Table 1 Socio-Demographic Characteristics of the Participants (Total n=95) |
The median number of years since the participants have been a refugee in Jordan until the interview time was six years, ranging from two to nine years. About two-thirds of the participants (65.2%) fled to Jordan in 2013 or 2014, so they have been in the refuge for five to six years. Approximately 80% of women experienced forced displacement inside Syria before arriving in Jordan. After leaving Syria, 33.7% reported living in non-camp settings within host communities without a history of residency in camp settings.
Nearly all participants experienced a direct threat of death (94.7%) or physical injury (92.6%) due to war in Syria. The one trauma index representing the women who experienced both personal death and physical injury threats was 92.6%. However, six participants (6.3%) were physically injured during the conflict. Regarding family members, the prevalence of having a family member who died due to the conflict was 92.6%, having a missing family member was 71.6%, while 53.7% reported a physically injured family member (Table 2).
 |
Table 2 Estimates of Conflict-Related Physical Trauma History Among the Syrian Refugee (Total n=95) |
The distribution of participants’ responses for each item of the RHS-15 scale is presented in Supplementary File 1. Most participants reported experiencing the RHS-15 items moderately or quite a bit. Feeling down, sad, or blue most of the time, having too much thinking or too many thoughts, and feeling helpless were the most common three items reported by participants. The RHS-15 mean and median scores were above average, with a mean (SD) score of 2.08 (0.46), ranging from 0.64 to 3.00, and a median of 2.14. This high mean score of RHS-15 represents highly prevalent emotional distressing symptoms among Syrian refugee women. Approximately all Syrian refugee women (n=94, 98.9%) scored ≥12 on the sum of the first 14 items of the RHS-15 scale. Also, an extremely high percentage of women (n=86, 90.5%) scored the distress they felt ≥5 on the DT item, and 35 participants (36.8%) scored 10, which is the highest score on the DT item. Thus, most women (n=86, 90.5%) were at high risk for depression, anxiety, and PTSD symptoms.
The respondents’ distribution of the MSPSS by item is presented in Supplementary File 2. The mean (SD) total MSPSS score was 5.08 (0.71), ranging from 3.50 to 6.67, representing moderate perceived social support. The MSPSS subscale with the highest sub-score was perceived support from friends, with a mean (SD) of 5.23 (0.85) (range: 3.00−7.00). The friends support sub-score is higher than 5.1, indicating slightly high perceived support from friends. In contrast, the mean (SD) MSPSS sub-scores of family and significant others were 5.02 (1.01) (range: 1.75−7.00) and 4.99 (1.19) (range: 3.00−7.00), respectively, representing moderate perceived support.
Supplementary File 3 demonstrates the distribution of participants’ responses for each item of the PTGI Scale. Overall, the mean (SD) total PTGI score was 2.44 (0.48), ranging from 0.71 to 3.43, with a median score of 2.48. The mean (SD) total PTGI score was below a predetermined cutoff point of three, indicating low levels of positive transformation among Syrian refugee women following their traumatic experiences. Moderate-to-high levels of PTG were reported by 12 (12.6%) of the Syrian refugee women, while the rest (n=83, 87.4%) had a low positive transformation and growth.
Among the PTGI subscales, the spiritual change and personal strength subscales had the highest sub-scores. Approximately all participating women reported great to moderate positive outcomes in better understanding of spiritual matters and having stronger religious beliefs following traumatic exposure (97.9% and 96.9%, respectively). The mean and median sub-scores of the spiritual change subscale were 3.64 (0.61) and 4.00, respectively (range: 0.00−5.00), representing more optimistic and religious beliefs following conflict-related traumas. The second highest sub-score was for the personal strength subscale, with mean and median sub-scores of 3.32 (0.55) and 3.50, respectively (range 1.50−4.00). This personal strength sub-score indicated a positive change in the women’s recognition of their self-strength following their refuging journey. Most women reported a great perception of self-reliance (85.3%), positive outcomes of dealing with their difficulties (87.3%), better accepting the way things work out (87.3%), and feeling stronger than they thought (84.2%).
In contrast, most participants scored lower than three on the appreciation of life, relating to others, and new possibilities subscales indicating low growth in these aspects. Regarding the appreciation of life subscale, the mean (SD) sub-score was 2.74 (0.89), ranging between 0.00 and 4.33, and the median sub-score was 3.00, representing low appreciation for their own existence. Around half of the participants reported no to minor feelings about their values in life and the ability to appreciate the positives of every day (44.2% and 43.2%, respectively). In the PTGI subscale of relating to others, the mean (SD) sub-score was 1.98 (0.71), ranging from 0.29 to 3.29, with a median sub-score of 2.14. Thus, the participants reported low maturity levels in their relationships with others. Approximately two-thirds of women (68.4%) did not count on others in times of trouble, and 24.2% accounted on others to a small or less extent. Similarly, 71.5% of participants reported none or little experience in recognizing the wonderfulness of others. Also, 41.1% of participants reported no changes in disclosing their emotions to others. The recognition of new possibilities subscale had the lowest sub-score, with a mean (SD) of 1.70 (0.89), ranging from 0.00 to 3.60, and a median of 1.60, representing negative outcomes of conflict-related trauma on refugee perception of new possibilities. Approximately two-thirds of women (70.5%) reported a lack of new opportunities, and 71.5% reported a lack of attitude toward making new pathways in their life.
The vast majority of Syrian refugee women experienced moderate-to-high levels of PTG at spiritual change (n=93, 97.9%) and personal strength (n=80, 84.2%) dimensions. Followed by the appreciation of life dimension, with 54 (56.8%) participants reporting moderate-to-high growth levels. The least prevalence estimates of women with moderate-to-high PTG levels were observed in the dimensions of relating to others (n=8, 8.4%) and perception of new possibilities (n=7, 7.4%).
Table 3 shows the differences in the RHS-15, PTGI, and MSPSS mean scores by conflict-related physical trauma variables. Statistically significant differences in RHS-15 scores were detected with the experience of a family member’s physical injury. Women who reported having a family member injured due to the conflict in Syria had significantly higher mean (SD) RHS-15 scores (2.18 (0.45)) than those who did not report such an event (1.97 (0.45)) (p=0.020). In contrast, no statistically significant differences were in the PTGI and MSPSS scores by conflict-related physical trauma items (p>0.05).
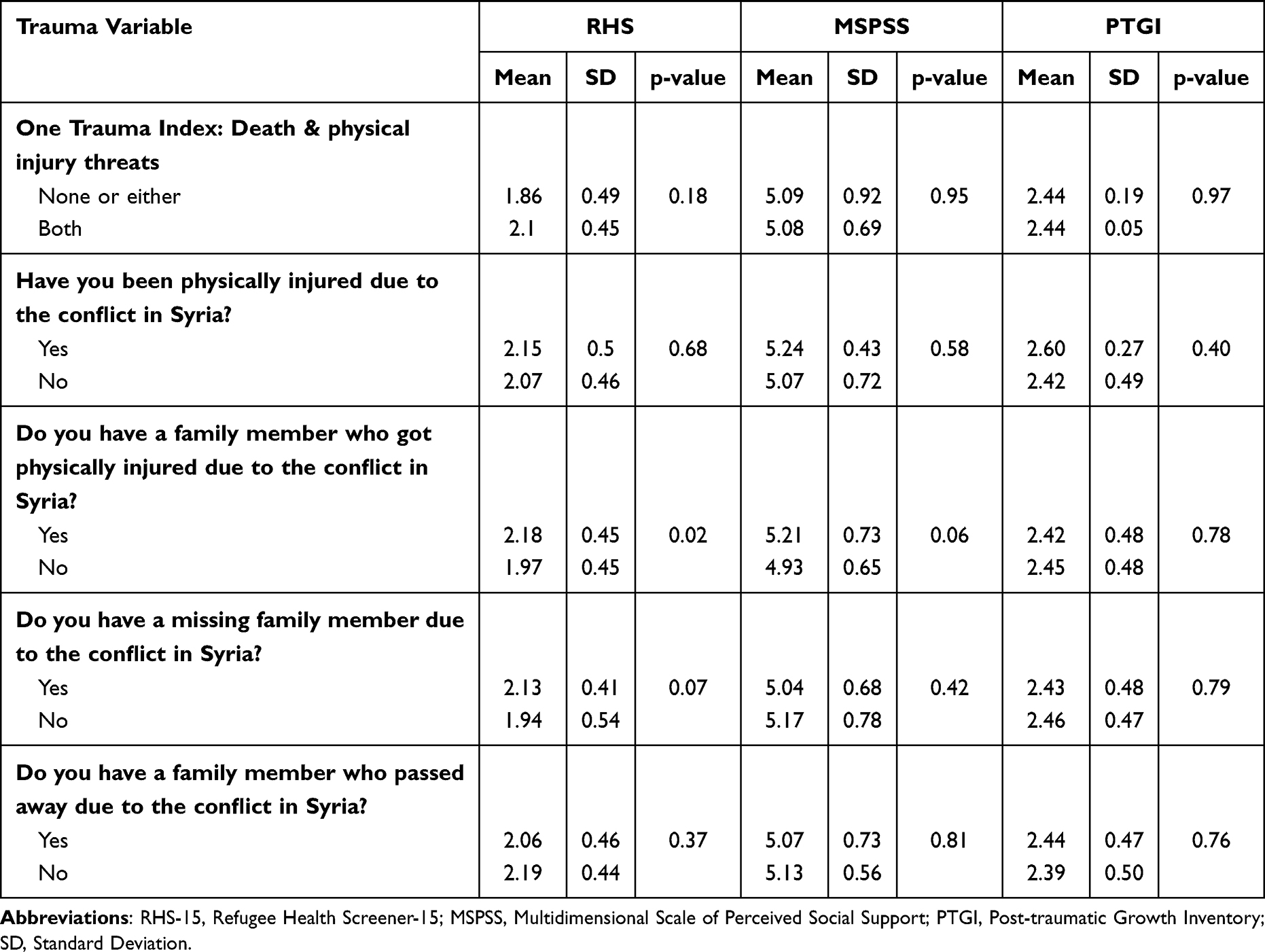 |
Table 3 Differences in Mean Score Values of the Refugee Health Screener-15 (RHS-15), the Multidimensional Scale of Perceived Social Support (MSPSS), and the Post-Traumatic Growth Inventory (PTGI) by Conflict-Related Physical Trauma History |
Differences in the mean scores of the MSPSS scale and subscales by conflict-related physical trauma variables showed that the mean (SD) sub-score of the friends support subscale was significantly higher among those who reported one trauma index (both personal death and physical injury threats) (5.28 (0.83)) than their counterparts who reported none or either threat (4.61 (0.84)) (p=0.04). Women with a physically injured family member had significantly higher mean (SD) MSPSS significant others and family sub-scores than those who did not have such. However, the difference of MSPSS significant others sub-score was statistically significant (p=0.05), while the difference in family sub-score was not statistically significant with a p-value of 0.06. Women who reported an experience of a family member’s death due to the conflict in Syria scored significantly higher on the friends’ subscale (5.29 (0.77)) than those with no such experience (4.75 (1.24)) (p=0.05). Other differences in the perceived social support subscales by conflict-related physical trauma were not statistically significant (Table 4).
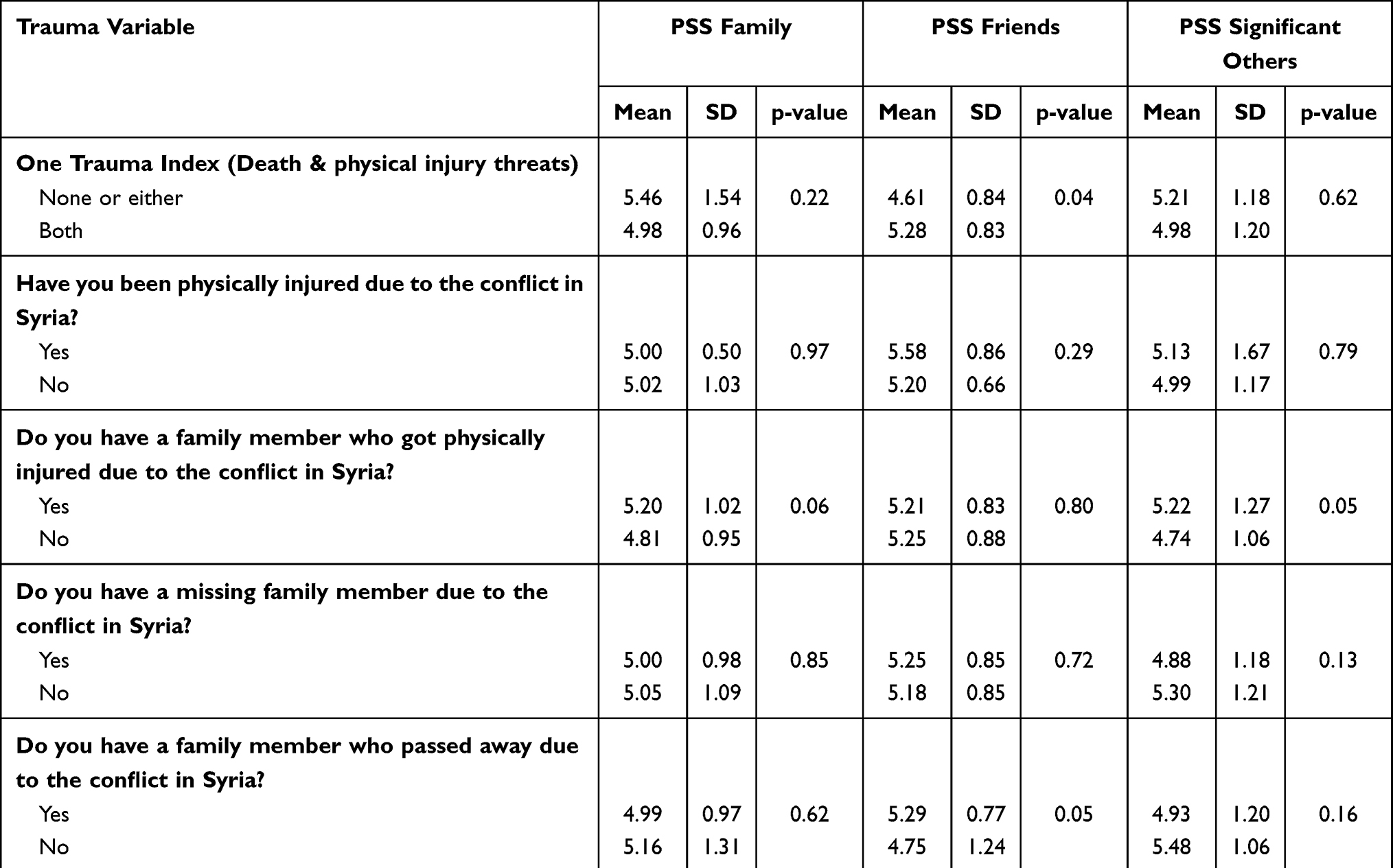 |
Table 4 Differences in the Mean Sub-Scores of Subscales of the Perceived Social Support (PSS) by Conflict-Related Physical Trauma History |
A negative correlation was detected between the PTGI and RHS-15 scores (r=−0.192). This relationship, however, was not statistically significant (p=0.06). On the other hand, as PTGI scores increased, the MSPSS scores significantly increased (r=0.568, p<0.001). For MSPSS subscales, there was a statistically significant positive association between PTGI and MSPSS-family sub-scores. As the mean PTGI score increased, the MSPSS-family sub-scores significantly increased (r=0.514, p<0.001). Similarly, statistically significant positive correlations were observed between PTGI scores and MSPSS-friends sub-scores (r=0.518, p<0.001) and MSPSS significant others sub-scores (r=0.207, p=0.046). Statistically significant inverse associations were observed between the RHS-15 scores and the overall MSPSS score (r=−0.206, p=0.045), and the sub-score of the MSPSS-significant others subscale (r =−0.206, p=0.045) (Table 5).
 |
Table 5 Correlations Between the Scores of the Refugee Health Screener-15 (RHS-15), the Multidimensional Scale of Perceived Social Support (MSPSS) and Its Subscales, and the Post-Traumatic Growth Inventory (PTGI) |
Discussion
Most Syrian refugee women experienced significant traumatic events due to the conflict in Syria, including both personal death and physical injury threats and having a dead, missing, or injured family member. These traumatic events resulted in distressing mental health symptoms, such as depression, anxiety, and PTSD, among the vast majority of Syrian refugee women, with a prevalence estimate of 90.5%. This may reflect a loss of pre-conflict life, as the Syrian crisis tore families and communities apart and forced women into a new, unprecedented reality. Despite experiencing traumatic events due to the conflict in Syria, refugees could be protected from emotionally distressing symptoms of depression, anxiety, and PTSD by increased social support, which was also linked with developing PTG. The participants reported moderate levels of perceived social support, with friends being the highest support resource for women. Most participants (87.4%) developed low levels of PTG. Moreover, significant negative relationships between RHS-15 and MSPSS and significant social support from significant others were detected. Also, statistically significant positive correlations of PTGI with MSPSS and its subscales were observed. Thus, substantial psychological interventions are recommended to mitigate the distressing mental health symptoms among Syrian refugees, considering the positive role of social support.
A survey study about the mental health of Syrian refugees in Sweden showed that mental ill-health was generally more common among refugee women who were older, divorced, or widowed.12 This finding is concordant with our reporting of mental health distressing symptoms among our cohort of refugee women who were heads of their households. However, the prevalence estimate of emotional distress symptoms in our cohort was extremely high (90.5%), which could be attributable, at least partially, to the sudden change in gender roles and exposure to traumatic events.5,24,35,46–49 The loss of the head of household in conservative societies exposes women to plenty of new life stressors that are not common. Also, experiencing conflict-related traumatic events by the majority of participants is another possible reason for the high levels of distressing emotional symptoms among the study participants, including a refuge journey, personal injury threats, personal death threats, losing one’s home, and having a family member(s) death, missing, or injury. This vulnerable group is in critical need of psychosocial support services that will empower them to mitigate traumatic events’ effects and potential mental health conditions. Concern over personal safety within a new community is another critical attribute in such societies. Previous reports reported a lack of safety to the degree that Syrian refugee women rarely leave their households due to fear.5,50 This finding is concordant with our findings of potentially high anxiety levels among Syrian refugee women in Jordan.
Syrian refugee women in our study were exposed to multiple conflict-related traumatic events, given that 80% of them were forcefully displaced from their homes inside Syria, and about all of them reported exposure to traumatic events related to experiencing the threat of death or injury not only to themselves but also to their family members. There may have been a plateau effect of conflict-related trauma exposure in our sample, as most women reported exposure to all six items of traumas. Also, during the interview, many women stated that their experiences within refugee camp settings were “humiliating” and “depressive” and that they still remember their previous living conditions. Accordingly, these traumatic events may explain why 90.5% of women had high scores on the DT even years after displacement and 90.5% had high risks of depression, anxiety, and PTD. This may reflect deep suffering, sorrow, frustration, and estrangement, given the accumulating stressors from the initial stages of the Syrian crisis to the day the study was conducted. Also, utilizing the RHS-15 scale as a screening tool for evaluating emotional distress symptoms of depression, anxiety, and PTSD could be another reason for overestimating such symptoms among the studied refugees despite the excellent sensitivity and specificity rates of the RHS-15.25,51
Most women in our study complained of physical symptoms (muscle, bone, or joint pain) along with those related to emotional distress, such as breaking out in a sweat and heartbeats fast. Such symptoms could be related to emotional suffering, which was reported elsewhere. For example, fatigue, loss of appetite, sleeping difficulty, gastrointestinal symptoms, and other medically unexplained physical symptoms were commonly associated with psychological distress.3 The cultural stigma associated with mental illnesses increases their incidence and prevalence rates in our societies and may be a barrier to help-seeking behaviors.52 Consequently, the patients would rather reach family and friends for social support than seek professional mental health or psychosocial services to avoid people’s negative attitudes toward accessing such services.53,54
The study findings indicated low positive growth and transformation levels among most Syrian refugee women (87.4%) following their traumatic experience, with a mean PTGI score of less than three. The leading attributes for the low PTG were the appreciation of life, relating to others, and new possibilities dimensions of the PTGI scale. The low appreciation of Syrian refugee women for their lives could be mainly attributed to the adjustment challenges, instability, economic insecurity, being unemployed, host community attitudes and stigma toward refugees, pre-and post-migration psychological and physical traumatic events, and loss of their loved people.55 Regarding relation to others dimension, the Syrian refugee women could have several issues resulting in a substantial reduction of their social interactions, including bad experiences with others, not knowing people well in the new host community, social tension, being besieged by suspicion, being mistrusted by others, and fears of building new relationships with the host community members. These factors could explain the low positive change in the PTGI dimension of relation to others. This is true for our cohort as they live in the host communities, not in camp settings where their friends and families live. In our cohort, the positive development of social relations with others came from the increased compassion and efforts toward building and improving relationships with others, heightened benefits of closeness with others, and raised sensitivity to other people’s needs.
Among the PTGI subscales, the lowest sub-score was recorded for the new possibilities dimension. This finding indicated the negative outcomes of conflict-related trauma on refugees’ perception of new possibilities. Most women reported the lack of new opportunities and attitudes to take new pathways in their life. The host country, Jordan, is a middle-income country suffering from economic challenges, high unemployment, job competition, and limited national resources, which enhance the perception of no opportunities or new life paths among Syrian refugee women in Jordan. As well as, the lack of a near solution for the conflict in their homeland exaggregated the refugees’ feelings of no opportunities.
The positive growth outcomes were reported for spiritual change and personal strength dimensions of the PTGI. Several studies reported the levels of spirituality and religiosity as positive predictors of PTG.56–59 Our cohort of Syrian refugee women scored high on the spiritual change dimension, as they had more optimistic, religious, and extroverted beliefs following conflict-related trauma. This finding suggests that Syrian refugee women relied on religious beliefs to cope with stress and strengthen themselves in this area. The conflict in Syria significantly altered the ordinary life of Syrian refugee women; thus, it reflected on their spiritual matters as spirituality became their approach to coping with stressful events. In our study, during the interview process, most women reported they turned to coping with their suffering by praying and reading Quran. Growing evidence indicated significant positive relationships between religiosity, spirituality, and mental and physical well-being.60 In an International Medical Corps (IMC) assessment report of coping mechanisms and help-seeking behaviors among Syrian refugees, most participants reported faith and spiritual beliefs as the most common primary coping mechanism.61
With the new economic and legal conditions and the abrupt alteration in gender roles in the host communities after being refugees, Syrian refugee women were compelled to take on responsibilities that were once a man’s domain, including, for example, finding a job.21–23,62 These changes explain the high levels of growth in the personal strength dimension, considering that women in our study felt more self-assured, better adapted to changes, and stronger than before. Thus, living through conflict-related traumas provided refugees with information about self-reliance and their ability to handle difficulties more assertively than they previously thought. Refugee women coping with traumatic events conclude their knowledge that they are self-confident and stronger, which may generalize to future traumas.
A growing body of evidence confirmed the potential protective role of social support for mental health.63–66 This study found a statistically significant positive correlation between PTGI and perceived social support from family, friends, and significant others. Women in our study seem to have built moderate support networks with their neighbors in a similar situation and within their local community. Cheng and Chan suggested that women would benefit more from the social support of friends than men because they engaged in more self-disclosure to others.67 On the other hand, not being united with one’s family could be considered a loss of vital social support, resulting in mental health illness.62,68 The potential buffering role of social support on the mental health status among Syrian women refugees was evident with the negative correlations of RHS-15 with MSPSS and the MSPSS from significant others. This finding reinforced the protective role of close relationships, which was reported among Syrian refugee youth.34 The lack of statistically significant relationships between conflict-related trauma events and other scales may be due to the plateau effect of trauma variables and related scales.
Strengths and Limitations of the Study
The study findings add to the literature by investigating the emotional distress and somatic symptoms of common mental health problems among Syrian refugee women in Jordan, with the assessment of conflict-related traumatic events history, perceived social support, and PTG. The novelty of this study is in its population, as targeting refugee women who head their households and live outside camps within host communities. However, several limitations should be reported. First, the study included a small sample size of Syrian refugee women; thus, the sample’s representativeness for the population was low, and the selection bias in the process of participants’ recruitment could not be ruled out. The limited sample could be attributed to the study approach of the face-to-face interview rather than a self-reported survey. However, the in-depth interview approach had several advantages, including achieving a high response rate and collecting high-quality data with good reliability. The response rate in our study was relatively good (67.9%); however, monetary incentives are suggested to achieve a better response rate. Second, the interviews were single-session and conducted by one person. This approach could be associated with several biases, including a tendency of participants toward safe, flattening complexity, and downplaying socio-political conflict, as well as the hardness of the interviewer to build trust and familiarity. However, in our study, the interviewer was a well-trained female familiar with refugee women, which minimizes these biases. Third, the lack of data on nonrespondents and the cross-sectional design of the study are other limitations limiting the generalizability of the study findings beyond the people who responded. Fourth, this study did not include a control group to compare with, and the conducted statistical analysis was not advanced, with no potential confounding factors being considered. Thus, we could not provide evidence for causal relationships between the symptoms of mental health illnesses and traumatic events, social support, and PTG. Future qualitative and case-control studies with a larger and more representative sample are recommended to comprehensively evaluate the effects of trauma experience, social support, and PTG on mental health symptoms. Finally, the RHS-15 tool is a sensitive screening tool rather than a diagnostic; thus, it might result in over-estimation of mental health problems among the participants. However, the RHS-15 is an effective tool with the high influx of refugees and limited health resources that can be administered within minutes, but the positive case with a high risk for emotional distress symptoms should be referred for clinical psychological health assessment by diagnostic interviews.25,51
Conclusions
High levels of exposure to traumatic events were found among Syrian refugee women. The study findings also demonstrated a significantly high but unspoken burden of mental health problems among Syrian refugee women living outside camps. Despite the challenges in detecting mental disorders among refugee women, effective screening would identify those who would benefit from further mental health evaluation and treatment. Psychosocial support services and professional assessment of needs and strengths to overcome traumatic exposures should be considered. This research supports preliminary evidence for the supposed role of social support in minimizing trauma effects and mental health symptoms. Thus, culturally tailored interventions that consider social support within networks of family and friends may be beneficial. Sustainable interdisciplinary models of psychosocial support plans, community outreach activities, awareness campaigns, and educational programs are necessary to promote mental health education, disperse myths, and reduce mental health stigma.
Data Sharing Statement
The datasets generated and analyzed during the current study are available with the corresponding authors.
Compliance with Ethical Consideration
The Institutional Review Board (IRB) of Jordan University of Science and Technology approved this study, with the IRB number of 519/2019. This study was conducted following the 1975 Helsinki declaration, revised in 2008, and its later amendments or comparable ethical standards.
Informed Consent
Written informed consent was obtained from each participant.
Acknowledgment
The authors would like to thank the Faculty of Research at Jordan University of Science and Technology for supporting the conduct of this study under the grant number of 20190473.
Funding
This study was funded by the faculty of Research at Jordan University of Science and Technology (JUST), Irbid, Jordan, with the grant number of 20190473.
Disclosure
The authors declare that they have no competing interests.
References
1. UNHCR. UNHCR - Jordan. (2021). Available from: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://reporting.unhcr.org/sites/default/files/Jordan.country.factsheet-February.2021.pdf.
2. Derose KP, Varda DM. Social capital and health care access: a systematic review. Med Care Res Rev. 2009;66(3):272–306. doi:10.1177/1077558708330428
3. Hassan G, Kirmayer L, Mekki-Berrada A, El-Chammay R. Culture, context and the mental health and psychosocial wellbeing of Syrians. Unhcr. 2015;25(September):1–50.
4. Yonis OB, Khader Y, Al-Mistarehi AH, Khudair SA, Dawoud M. Behavioural and emotional symptoms among schoolchildren: a comparison between Jordanians and Syrian refugees. East Mediterr Health J. 2021;27(12):1162–1172. doi:10.26719/emhj.21.072
5. Hassan G, Ventevogel P, Jefee-Bahloul H, Barkil-Oteo A, Kirmayer LJ. Mental health and psychosocial wellbeing of Syrians affected by armed conflict. Epidemiol Psychiatr Sci. 2016;25(2):129–141. doi:10.1017/S2045796016000044
6. Hijazi Z, Weissbecker I. Syria crisis: addressing regional mental health needs and gaps in the context of the Syria crisis. Available from: https://reliefweb.int/report/syrian-arab-republic/syria-crisis-addressing-regional-mental-health-needs-and-gaps-context.
7. Bogic M, Njoku A, Priebe S. Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights. 2015;15:29. doi:10.1186/s12914-015-0064-9
8. Alpak G, Unal A, Bulbul F, et al. Post-traumatic stress disorder among Syrian refugees in Turkey: a cross-sectional study. Int J Psychiatry Clin Pract. 2015;19(1):45–50. doi:10.3109/13651501.2014.961930
9. Stevenson K, Alameddine R, Rukbi G, et al. High rates of maternal depression amongst Syrian refugees in Lebanon - a pilot study. Sci Rep. 2019;9(1). doi:10.1038/s41598-019-48247-5
10. Fazel M, Wheeler J, Danesh J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet. 2005;365(9467):1309–1314. doi:10.1016/S0140-6736(05)61027-6
11. Chung MC, AlQarni N, Al Muhairi S, Mitchell B. The relationship between trauma centrality, self-efficacy, posttraumatic stress and psychiatric co-morbidity among Syrian refugees: is gender a moderator? J Psychiatr Res. 2017;94:107–115. doi:10.1016/j.jpsychires.2017.07.001
12. Tinghög P, Malm A, Arwidson C, Sigvardsdotter E, Lundin A, Saboonchi F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: a population-based survey. BMJ Open. 2017;7(12):e018899. doi:10.1136/bmjopen-2017-018899
13. Acarturk C, Cetinkaya M, Senay I, Gulen B, Aker T, Hinton D. Prevalence and predictors of posttraumatic stress and depression symptoms among Syrian refugees in a refugee camp. J Nerv Ment Dis. 2018;206(1):40–45. doi:10.1097/NMD.0000000000000693
14. Al-Smadi AM, Halaseh HJ, Gammoh OS, Ashour AF, Gharaibeh B, Khoury LS. Do chronic diseases and availability of medications predict post-traumatic stress disorder (PTSD) among Syrian refugees in Jordan? Pakistan J Nutr. 2016;15(10):936–941. doi:10.3923/pjn.2016.936.941
15. Rizkalla N, Arafa R, Mallat NK, Soudi L, Adi S, Segal SP. Women in refuge: Syrian women voicing health sequelae due to war traumatic experiences and displacement challenges. J Psychosom Res. 2020;129(109909):109909. doi:10.1016/j.jpsychores.2019.109909
16. Taku K, Cann A, Calhoun LG, Tedeschi RG. The factor structure of the posttraumatic growth inventory: a comparison of five models using confirmatory factor analysis. J Trauma Stress. 2008;21(2):158–164. doi:10.1002/jts.20305
17. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress. 1996;9(3):455–471. doi:10.1002/jts.2490090305
18. Ssenyonga J, Owens V, Olema DK. Posttraumatic growth, resilience, and Posttraumatic Stress Disorder (PTSD) among refugees. Procedia - Soc Behav Sci. 2013;82:144–148. doi:10.1016/j.sbspro.2013.06.238
19. Boswall K, Akash R. Personal perspectives of protracted displacement: an ethnographic insight into the isolation and coping mechanisms of Syrian women and girls living as urban refugees in northern Jordan. Interv - Eur J Econ Econ Policies. 2015;13(3):203–215.
20. de Haas H. Migration and Development: a Theoretical Perspective. Int Migr Rev. 2010;44(1):227–264. doi:10.1111/j.1747-7379.2009.00804.x
21. Haddad Z How the crisis is altering women’s roles in Syria | forced migration review. (2014). Available from: https://www.fmreview.org/syria/haddad.
22. Doocy S, Lyles E. Humanitarian needs among displaced and female-headed households in government-controlled areas of Syria. Am J Public Health. 2017;107(6):950. doi:10.2105/AJPH.2017.303710
23. Center for International Private Enterprise. Women head more than a quarter of refugee households. what’s next for them? Available from: https://www.cipe.org/blog/2017/03/08/women-head-more-than-a-quarter-of-refugee-households-whats-next-for-them/.
24. Kisilu A, Darras L. Highlighting the gender disparities in mental health among Syrian refugees in Jordan. Intervention. 2018;16(2):140–146. doi:10.4103/INTV.INTV_18_18
25. Hollifield M, Verbillis-Kolp S, Farmer B, et al. The Refugee Health Screener-15 (RHS-15): development and validation of an instrument for anxiety, depression, and PTSD in refugees. Gen Hosp Psychiatry. 2013;35(2):202–209. doi:10.1016/j.genhosppsych.2012.12.002
26. Johnson-Agbakwu CE, Allen J, Nizigiyimana JF, Ramirez G, Hollifield M. Mental health screening among newly arrived refugees seeking routine obstetric and gynecologic care. Psychol Serv. 2014;11(4):470–476. doi:10.1037/a0036400
27. Pathways to Wellness. Refugee health screener-15: development and use of the RHS-15. Integrating refugee health and well-being creating pathways for refugee survivors to heal; (2011). Available from: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://refugeehealthta.org/wp-content/uploads/2012/09/RHS15_Packet_PathwaysToWellness-1.pdf.
28. Hollifield M, Toolson EC, Verbillis-Kolp S, et al. Effective screening for emotional distress in refugees: the refugee health screener. J Nerv Ment Dis. 2016;204(4):247–253. doi:10.1097/NMD.0000000000000469
29. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
30. Perceived Social Support | MSPSS. Greenspace mental health knowledge base. Available from: https://help.greenspacehealth.com/article/92-perceived-social-support-mspss.
31. Alshraifeen A, Al-Rawashdeh S, Alnuaimi K, et al. Social support predicted quality of life in people receiving haemodialysis treatment: a cross-sectional survey. Nurs Open. 2020;7(5):1517–1525. doi:10.1002/nop2.533
32. Zimet G. Multidimensional Scale of Perceived Social Support (MSPSS) - scale items and scoring information; (2016). Available from: https://www.researchgate.net/publication/311534896_Multidimensional_Scale_of_Perceived_Social_Support_MSPSS_-_Scale_Items_and_Scoring_Information.
33. Aroian K, Templin TN, Ramaswamy V. Adaptation and psychometric evaluation of the multidimensional scale of perceived social support for Arab immigrant women. Health Care Women Int. 2010;31(2):153–169. doi:10.1080/07399330903052145
34. Kliewer W, Kheirallah KA, Cobb CO, Alsulaiman JW, Mzayek F, Jaddou H. Trauma exposure and post-traumatic stress symptoms among Syrian refugee youth in Jordan: social support and gender as moderators. Int J Psychol. 2021;56(2):199–207. doi:10.1002/ijop.12695
35. Kheirallah KA, Cobb CO, Alsulaiman JW, et al. Trauma exposure, mental health and tobacco use among vulnerable Syrian refugee youth in Jordan. J Public Health. 2020;42(3):e343–e351. doi:10.1093/pubmed/fdz128
36. Zoellner T, Maercker A. Posttraumatic growth in clinical psychology - a critical review and introduction of a two component model. Clin Psychol Rev. 2006;26(5):626–653. doi:10.1016/j.cpr.2006.01.008
37. Jansen L, Hoffmeister M, Chang-Claude J, Brenner H, Arndt V. Benefit finding and post-traumatic growth in long-term colorectal cancer survivors: prevalence, determinants, and associations with quality of life. Br J Cancer. 2011;105(8):1158–1165. doi:10.1038/bjc.2011.335
38. Pollari CD, Brite J, Brackbill RM, et al. World trade center exposure and posttraumatic growth: assessing positive psychological change 15 years after 9/11. Int J Environ Res Public Health. 2020;18(1):1–12. doi:10.3390/ijerph18010104
39. Holtmaat K, van der Spek N, Cuijpers P, Leemans CR, Verdonck-de Leeuw IM. Posttraumatic growth among head and neck cancer survivors with psychological distress. Psychooncology. 2017;26(1):96–101. doi:10.1002/pon.4106
40. Kira I, Abou-Median S, Ashby J, Lewandowski L, Mohanesh J, Odenat L. Post-traumatic growth inventory: psychometric properties of the Arabic version in Palestinian adults. Int J Educ Psychol Assess. 2012;11(2):120–137.
41. Hoekstra R, Kiers HAL, Johnson A. Are assumptions of well-known statistical techniques checked, and why (not)? Front Psychol. 2012;3(MAY). doi:10.3389/fpsyg.2012.00137
42. Doane DP, Seward LE. Measuring skewness: a forgotten statistic? J Stat Educ. 2017;19(2). doi:10.1080/10691898.2011.11889611
43. Razali NM, Wah YB. Power comparisons of shapiro-wilk, kolmogorov-smirnov, lilliefors and anderson-darling tests. J Stat Model Analyt. 2011;2(1):21–33.
44. Shapiro SS, Wilk MB. An analysis of variance test for normality (complete samples). Biometrika. 1965;52(3–4):591–611. doi:10.1093/biomet/52.3-4.591
45. Kwak SG, Kim JH. Central limit theorem: the cornerstone of modern statistics. Korean J Anesthesiol. 2017;70(2):144–156. doi:10.4097/kjae.2017.70.2.144
46. UNHCR UNICEF, IOM, CARITAS and CRS WFP. Joint assessment for Syrian refugees in Alexandria, Egypt; (2013).
47. Mahmood HN, Ibrahim H, Goessmann K, Ismail AA, Neuner F. Post-Traumatic stress disorder and depression among Syrian refugees residing in the Kurdistan region of Iraq. Confl Health. 2019;13(1):1–11. doi:10.1186/s13031-019-0238-5
48. Dehnel R, Dalky H, Sudarsan S, Al-Delaimy WK. Resilience and mental health among Syrian refugee children in Jordan. J Immigr Minor Heal. 2022;24(2):420. doi:10.1007/s10903-021-01180-0
49. Renner A, Jäckle D, Nagl M, et al. Predictors of psychological distress in Syrian refugees with posttraumatic stress in Germany. PLoS One. 2021;16(8):e0254406. doi:10.1371/journal.pone.0254406
50. Al Akash R, Boswall K. Listening to the voices of Syrian women refugees in Jordan: ethnographies of displacement and emplacement. Intervention. 2015;13(3):203–215.
51. Fellmeth G, Plugge E, Fazel M, et al. Validation of the refugee health screener-15 for the assessment of perinatal depression among Karen and Burmese women on the Thai-Myanmar border. PLoS One. 2018;13(5):e0197403. doi:10.1371/journal.pone.0197403
52. Rohlof HG, Knipscheer JW, Kleber RJ. Somatization in refugees: a review. Soc Psychiatry Psychiatr Epidemiol. 2014;49(11):1793–1804. doi:10.1007/s00127-014-0877-1
53. Abu-Ras W. Barriers to services for Arab immigrant battered women in a detroit suburb. J Soc Work Res Eval. 2003;4(1):49–66.
54. Al-Shdayfat N, Hatamleh R. Syrian refugee women’s reasons for not reporting violence an exploratory study. Int J Nurs Educ. 2017;9(96):4.
55. Factors impacting life satisfaction of refugees in Australia: a mixed method study - UQ eSpace. Available from: https://espace.library.uq.edu.au/view/UQ:2e134c7.
56. Tedeschi RG, Cann A, Taku K, Senol-Durak E, Calhoun LG. The posttraumatic growth inventory: a revision integrating existential and spiritual change. J Trauma Stress. 2017;30(1):11–18. doi:10.1002/jts.22155
57. Taku K, Cann A. Cross-national and religious relationships with posttraumatic growth: the role of individual differences and perceptions of the triggering event. J Cross Cult Psychol. 2014;45(4):601–617. doi:10.1177/0022022113520074
58. Gerber MM, Boals A, Schuettler D. The unique contributions of positive and negative religious coping to posttraumatic growth and PTSD. Psycholog Relig Spiritual. 2011;3(4):298–307. doi:10.1037/a0023016
59. Sörensen J, Rzeszutek M, Gasik R. Social support and post-traumatic growth among a sample of arthritis patients: analysis in light of conservation of resources theory. Curr Psychol. 2021;40(4):2017–2025. doi:10.1007/s12144-019-0131-9
60. Koenig HG. Religion, spirituality, and medicine: research findings and implications for clinical practice. South Med J. 2004;97(12):1194–1200. doi:10.1097/01.SMJ.0000146489.21837.CE
61. International Medical Corps. Utilization of mental health and psychosocial support services among Syrian refugees and Jordanians; (2020):1–36. Available from: https://reliefweb.int/report/jordan/utilization-mental-health-and-psychosocial-support-services-among-syrian-refugees-and.
62. Shalaby M, Marnicio A. Women in Conflict. J Women Hum. 2015;2015(2):1–37.
63. Loayza-Rivas J, Fernández-Castro J. Perceived stress and well-being: the role of social support as a protective factor among Peruvian immigrants in Spain. Ansiedad y Estrés. 2020;26(2):67–72. doi:10.1016/j.anyes.2020.03.002
64. Oppedal B, Idsoe T. The role of social support in the acculturation and mental health of unaccompanied minor asylum seekers. Scand J Psychol. 2015;56(2):203–211. doi:10.1111/sjop.12194
65. Sim A, Bowes L, Gardner F. The promotive effects of social support for parental resilience in a refugee context: a cross-sectional study with Syrian mothers in Lebanon. Prev Sci. 2019;20(5):674. doi:10.1007/s11121-019-0983-0
66. Gottvall M, Vaez M, Saboonchi F. Social support attenuates the link between torture exposure and post-traumatic stress disorder among male and female Syrian refugees in Sweden. BMC Int Health Hum Rights. 2019;19(1):28. doi:10.1186/s12914-019-0214-6
67. Cheng S-T, Chan ACM. The multidimensional scale of perceived social support: dimensionality and age and gender differences in adolescents. Pers Individ Dif. 2004;37(7):1359–1369. doi:10.1016/j.paid.2004.01.006
68. Schweitzer R, Melville F, Steel Z, Lacherez P. Trauma, post-migration living difficulties, and social support as predictors of psychological adjustment in resettled Sudanese refugees. Aust N Z J Psychiatry. 2006;40(2):179–187. doi:10.1080/j.1440-1614.2006.01766.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.