")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Association Between Vitamin D and Type 2 Diabetes Mellitus Complicated with Non-Alcoholic Fatty Liver Disease: An Observational Cross-Sectional Study
Authors Xing Y, Cheng T, Zhou F , Ma H
Received 11 November 2021
Accepted for publication 14 January 2022
Published 2 February 2022 Volume 2022:15 Pages 269—280
DOI https://doi.org/10.2147/DMSO.S348870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Yuling Xing,1,2 Tiantian Cheng,1,3 Fei Zhou,1,2 Huijuan Ma1,4,5
1Department of Endocrinology, Hebei General Hospital, Shijiazhuang, 050017, People’s Republic of China; 2Graduate School of Hebei Medical University, Shijiazhuang, 050017, People’s Republic of China; 3Department of Internal Medicine, School of Clinical Medicine, North China University of Science and Technology, Tangshan, 063210, Hebei, People’s Republic of China; 4Hebei Key Laboratory of Metabolic Diseases, Hebei General Hospital Shijiazhuang, Hebei, 050051, People’s Republic of China; 5Department of Internal Medicine, Hebei Medical University, Shijiazhuang, Hebei, 050017, People’s Republic of China
Correspondence: Huijuan Ma, Email [email protected]
Objective: To investigate the association between vitamin D deficiency and NAFLD risk in patients with type 2 diabetes mellitus (T2DM).
Methods: Overall, 434 patients with T2DM admitted to Hebei General Hospital from January 2019 to December 2019 were selected as the study subjects. According to abdominal ultrasound findings, patients were divided into the NAFLD group and the non-NAFLD group. Participants were divided into two study groups according to the 25-hydroxyvitamin D [25(OH)D] level. 25(OH)D deficiency was defined if 25(OH)D vitamin levels were < 20 ng/mL. Chi-square test and one-way analysis of variance were used to compare groups. The relationship between 25(OH)D and NAFLD risk was analyzed using correlation and regression analyses. Furthermore, subgroup analyses were performed to verify the robustness of the results.
Results: The 25(OH)D level in patients with T2DM complicated by NAFLD was significantly lower than in patients with T2DM only. Vitamin D deficiency was highly prevalent among T2DM patients with NAFLD. This study suggested that vitamin D deficiency was an independent factor for developing NAFLD in patients with T2DM. T2DM patients with vitamin D deficiency had 2.045 times higher risk of developing NAFLD than those without vitamin D deficiency. Vitamin D deficiency was associated with high NAFLD preference in T2DM patients with BMI > 23kg/m2, but not those with BMI ≤ 23kg/m2. The significant correlation between vitamin D deficiency and NAFLD was found in participants with BMI > 23kg/m2, age ≤ 65 years, without hypertension, TG < 1.7mmol/l, HDL ≥ 1 mmol/l in men, ≥ 1.3 mmol/l in women, HBA1C ≤ 7%, or females.
Conclusion: This study suggests that T2DM people with BMI > 23kg/m2 were more susceptible to NAFLD by vitamin D deficiency and that it is necessary to maintain optimal serum vitamin D levels in this population.
Keywords: type 2 diabetes mellitus, non-alcoholic fatty liver disease, vitamin D
Introduction
Non-alcoholic fatty liver disease (NAFLD) was characterized by a spectrum of pathologies ranging from simple hepatocyte steatosis to non-alcoholic steatohepatitis (NASH). As the disease progresses, it can lead to liver cirrhosis and even the liver cancer.1 In a recent meta-analysis of 86 studies, the global prevalence of NAFLD was estimated to be 25.24% in the general population, while several meta-analyses indicated that in type 2 diabetes mellitus (T2DM) patients the prevalence was double (54–59.67%).2–4 The prevalence of NAFLD has reached as high as 90%, particularly in T2DM patients with obesity.5 However, accumulating evidence indicated that the effects of NAFLD extend beyond the liver and are negatively associated with a range of chronic diseases, most notably cardiovascular disease (CVD), T2DM and chronic kidney disease (CKD).6 However, there was no definitive treatment for NAFLD other than lifestyle intervention.7 Vitamin D was a lipid-soluble vitamin involved primarily in bone metabolism, calcium and phosphate homeostasis and skeletal development.8 25-Hydroxyvitamin D [25(OH)D] was the active form of vitamin D.9 The evaluation of vitamin D status usually relied on detection of the serum 25(OH)D concentration.10 Several epidemiologic studies show that low serum levels of 25(OH)D were associated with adverse health outcomes, such as metabolic syndrome, diabetes, chronic liver disease, cancer, cardiovascular disease and all-cause mortality.11–16 Worldwide, vitamin D deficiency was one of the most important public health issues and its prevalence in general populations is approximately 36% in the United States, 61% in Canada, 92% in Northern Europe, 45–98% in Asia, 31% in Australia and 56% in New Zealand.17 A meta-analysis concluded that vitamin D deficiency was common in Asia based on data from 472 studies with 746,564 participants.18 Epidemiological evidence indicated that low 25(OH)D level was an independent risk factor for NAFLD.14,19 A recent meta-analysis indicated a significant association between low 25(OH)D level and NAFLD.20 T2DM patients had multiple micro/macronutrient deficiencies, eg, magnesium deficiency.21 The risk of NAFLD was also linked with dietary components of the diet, eg, dietary insulinemic potential.22 NAFLD and T2DM interacted in a “cause or consequence” fashion such that the presence of one entity increases the predisposition and/or worsens the complications for the other disease.23–27 Based on the controversy over the relationship between vitamin D and NAFLD in patients with T2DM, so we aimed to explore the relationship between 25 (OH) D and NAFLD and to investigate whether there was any difference between different populations.
Methods
Patients and Study Design
The study was conducted following the Declaration of Helsinki and was approved by the Ethics Committee of Hebei General Hospital. Our study included 434 patients diagnosed with T2DM who were hospitalized in Hebei General Hospital of Shijiazhuang in China. All subjects had signed written informed consent. Studies were independently assessed by the two researchers and evaluated against inclusion and exclusion criteria by consensus.
Inclusion Criteria
1) Age ≥18 years. 2) The clinical diagnosis of T2DM was established according to the following criteria: 1) Patients who were under treatment with either oral antidiabetic agents or insulin, and who gave a history of diabetes, also were considered to have T2DM. 2) T2DM conformed to 1999 WHO Diagnostic Criteria: typical symptoms of diabetes (such as polyphagia, polydipsia, polyuria and weight loss) and random blood glucose ≥11.1 mmol/l or fasting blood glucose (FPG)≥7.0 mmol/l or glucose tolerance test two-hour blood glucose >11.1 mmol/l. Patients without typical symptoms of diabetes should be rechecked another day. 3) Fatty liver was diagnosed by the findings of ultrasound performed by trained technicians. The participants with liver contrast and liver brightness among the four known criteria (hepatorenal echo contrast, liver brightness, deep attenuation, and vascular blurring) were diagnosed as having fatty liver.28
Exclusion Criteria
1) Patients with type 1 diabetes mellitus, gestational diabetes and other particular types of diabetes were excluded. 2) Patients were excluded if they had a history of myocardial infarction, cerebral haemorrhage, severe dysfunction of liver and kidney, recent acute infection and stress within the last 3 months before enrollment. 3) IPatients were excluded if they had taken calcium, vitamin D supplements or any drugs affecting vitamin D metabolism in the past 6 months.4) Any participants currently using drugs that can increase NAFLD risk, such as amiodarone, corticosteroids, etc. 5) Patients were also excluded if they had a clear drinking history (≥30 grams/day in men and ≥20 grams/day in women). Subjects with positive for hepatitis B surface antigen (HBsAg) or anti-hepatitis C virus (HCV) antibody, autoimmune hepatitis, Wilson disease, primary biliary cirrhosis, primary sclerosing cholangitis, liver metabolic disorders, drug-induced hepatitis, hemochromatosis, malignancy, osteoporosis, thyroid disease or kidney disease were also excluded.
Data Collection
A questionnaire was utilized to collect basic information from T2DM patients, including age, sex, course of diabetes, history of hypertension, and medication history. Height (m) and weight (kg) were measured to calculate body mass index [BMI = weight (kg)/height (m2)]. Venous blood samples were drawn from all subjects after an overnight fast of 8 hours. Blood measurements included glycosylated haemoglobin (HbA1c), FPG, albumin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transferase (GGT), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL), low-density lipoprotein cholesterol (LDL), very-low-density lipoprotein cholesterol (VLDL), 25(OH) D. The data and results will be entered into spreadsheets and cross-checked by two researchers. Serum 25(OH)D was determined by electrochemiluminescence immunoassays (ECLA) using Roche commercial kits (COBAS e 601, Roche, Germany).
Statistical Analysis
Statistical analyses were performed using SPSS software, version 25.0. Continuous variables were expressed as the mean ± standard deviation (SD) if normally distributed and as medians and interquartile range (P25, P75) if not normally distributed. Independent group t-test was used for a continuous variable when the data conformed to normal distribution; otherwise, the Kruskal–Wallis test was applied. The enumeration data were expressed in percentage [n/(%)], and the Chi-square test tested the comparison between the groups. Descriptive statistics were calculated and compared between T2DM patients with and without NAFLD or vitamin D deficiency. The variables with a p-value level of less than 0.1 were entered into the multiple logistic regression model. Differences were considered statistically significant for p values <0.05. Taking α = 0.05, β = 0.10, and bilateral testing, the PASS software (version 15.0) was used to calculate the sample size in this study.
Results
Comparison of Clinical Characteristics Between T2DM Patients with and without NAFLD
By comparing the clinical parameters of T2DM patients with NAFLD and those without NAFLD, there were no statistically differences in sex, the proportion of hypertension, the level of FPG and HbA1c between the two groups. Patients with NAFLD had a significantly shorter duration (p=0.049) and younger age (p=0.004) than patients without NAFLD. The levels of BMI (p<0.001), albumin (p=0.030), ALT (p<0.001), AST (p<0.001), GGT (p<0.001), TC (p=0.002), TG (p<0.001), LDL (p=0.004), VLDL (p<0.001) were higher among T2DM patients who had NAFLD compared to those without NAFLD. Patients with combined T2DM and NAFLD had decreased HDL levels compared with T2DM patients (Table 1).
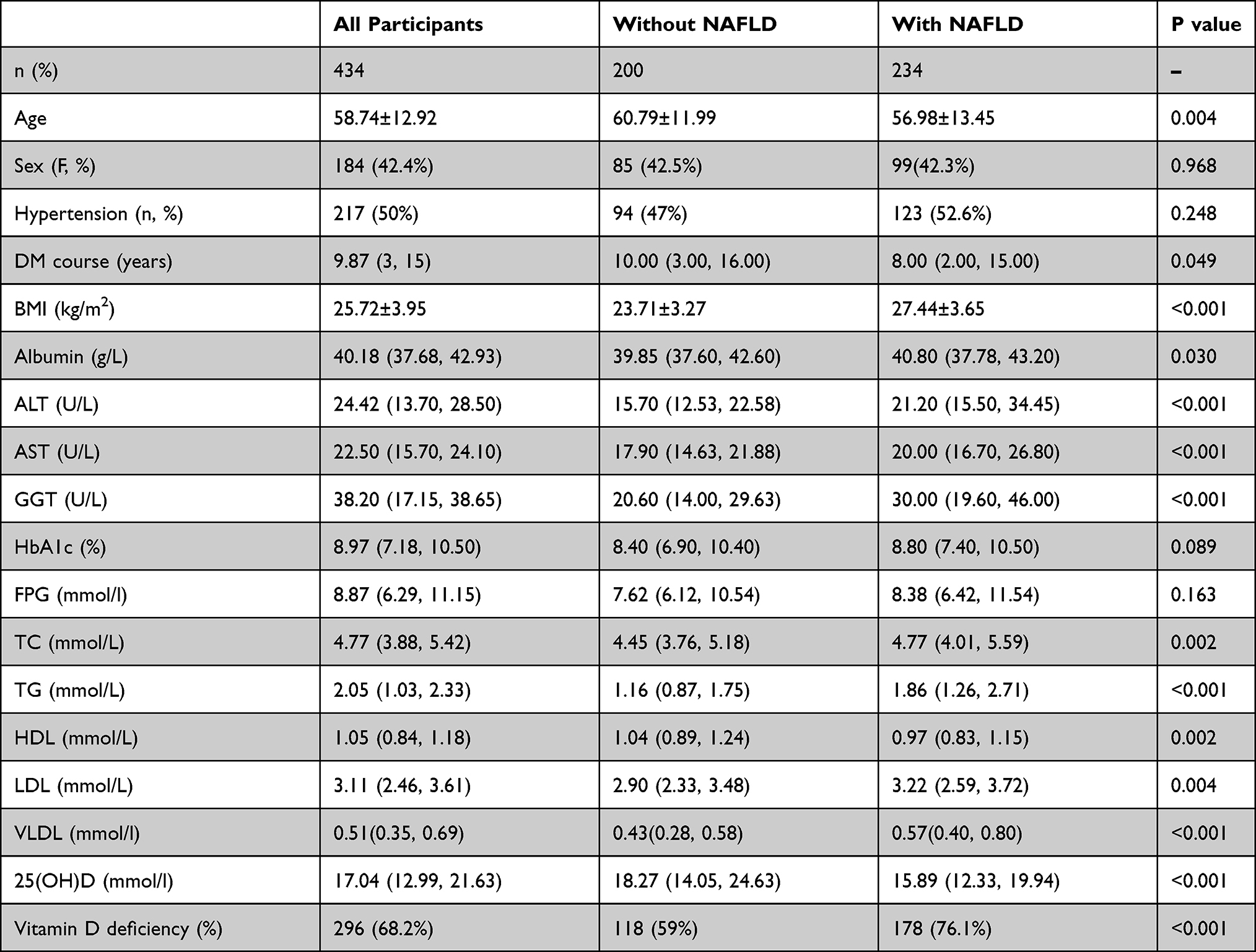 |
Table 1 Characteristics of Patients with and without NAFLD Included in This Study |
Comparison of Clinical Characteristics in T2DM Patients with VDD and VDND Groups
Patients were divided into two groups according to their 25(OH)D levels: vitamin D-deficient group (VDD) (<20 ng/mL), and vitamin D non-deficient group (VDND) (>20 ng/mL), with 296, 138 patients in each group, respectively. In the VDD group, BMI (p=0.03), HbA1c (p=0.002), TG (p<0.001), VLDL (p=0.009) levels and female proportion (p<0.001) were significantly higher compared with the VDND group, while the levels of albumin were lower than T2DM patients in the VDND group. However, there was no significant difference in age, T2DM course, ALT, AST, GGT, TC, HDL, LDL, FPG and hypertension proportion between the VDD and VDND groups (Table 2).
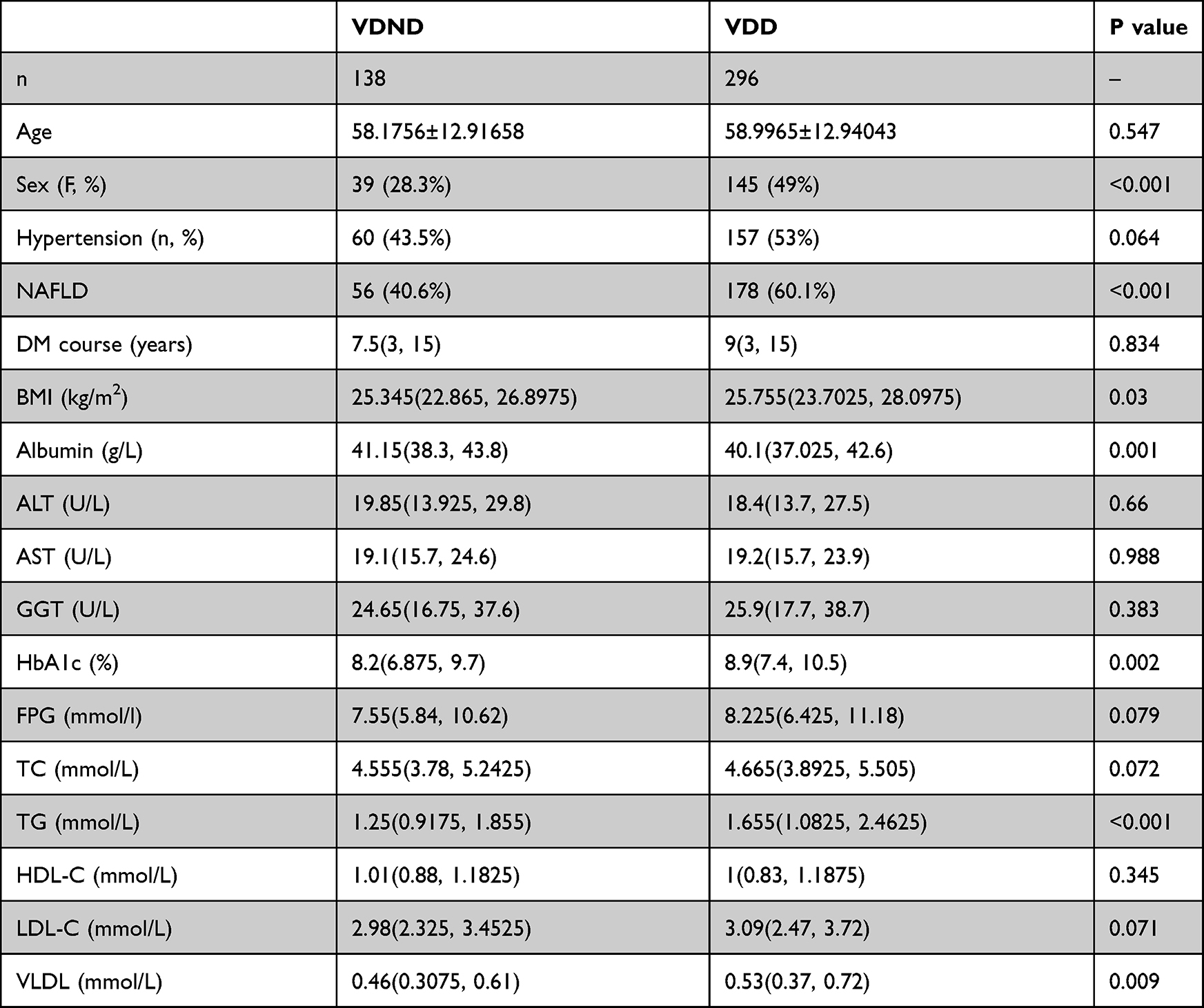 |
Table 2 Characteristics of Patients with and without Vitamin D Deficiency Included in This Study |
Comparison of 25(OH)D Levels and Prevalence of NAFLD in T2DM Patients with Different Levels of BMI
Patients who underwent combined NAFLD still conferred a statistically significant lower level of 25(OH)D [15.89 (12.33, 19.94) vs 18.27 (14.05, 24.63), p<0.001] (Figure 1A) and a higher proportion of patients with vitamin D deficiency (76.1% vs 59%, P<0.001) compared with T2DM patients without NAFLD (Table 1). NAFLD prevalence in T2DM patients with 25 (OH) D deficiency was higher than in those without 25 (OH) D deficiency, and the difference was statistically significant (60.1% vs 40.6%, P<0.001) (Figure 2A).
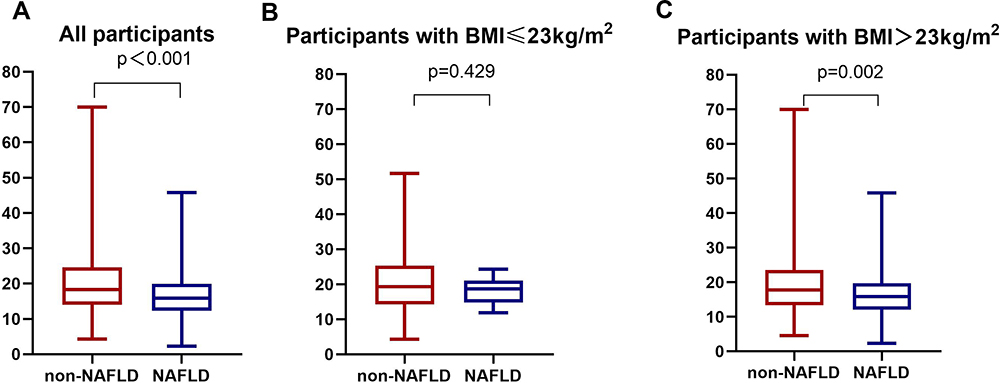 |
Figure 1 Comparison of 25(OH)D between the NAFLD group and the non-NAFLD group in participants with T2DM: (A) all participants; (B) participants with BMI >23kg/m2; (C) participants with BMI ≤23kg/m2. |
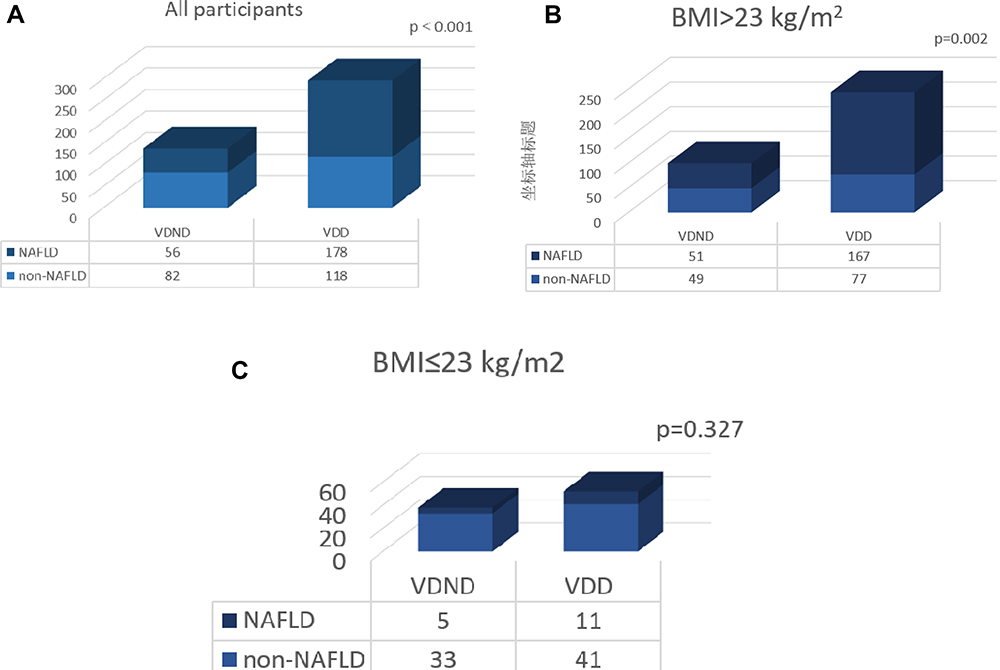 |
Figure 2 Comparison of the prevalence of NAFLD in T2DM patients with and without vitamin D deficiency: (A) all participants; (B) participants with BMI >23kg/m2; (C) participants with BMI ≤23kg/m2. |
BMI was categorized as BMI ≤23kg/m2 and BMI ≥23 kg/m2. We also carried out separate analyses for these two subgroups. In T2DM patients with BMI >23kg/m2, the level of 25(OH)D was significantly lower in T2DM patients with NAFLD compared with those without NAFLD [15.80 (12.04, 19.73) vs 17.72 (13.36, 23.57), P=0.002] (Figure 1B). The NAFLD prevalence in patients with 25 (OH) D deficiency was higher than in those without 25 (OH) D deficiency, and the difference was statistically significant (68.4% vs 51%, P=0.002) in T2DM patients with BMI>23kg/m2 (Figure 2B). However, no difference was observed in the levels of 25 (OH) D between NAFLD and non-NAFLD groups in T2DM patients with BMI ≤23kg/m2 (Figure 1C). There was no difference in the prevalence of NAFLD between VDND and VDD groups in T2DM patients with BMI ≤23kg/m2 (Figure 2C).
Spearman Correlation of 25(OH)D with Potential NAFLD Factors
Correlation analysis demonstrated that 25(OH)D level was positively correlated with albumin (r=0.214, p<0.001) and negatively correlated with BMI (r=−0.138, p=0.004), FPG (r=−0.112, p=0.019), HbA1c (r=−0.190, p<0.001), TG (r=−0.231, p<0.001), LDL (r=−0.103, p=0.032), VLDL (r=−0.151, p=0.002) in all study subjects. Figure 3 demonstrates the results of Spearman correlation analysis.
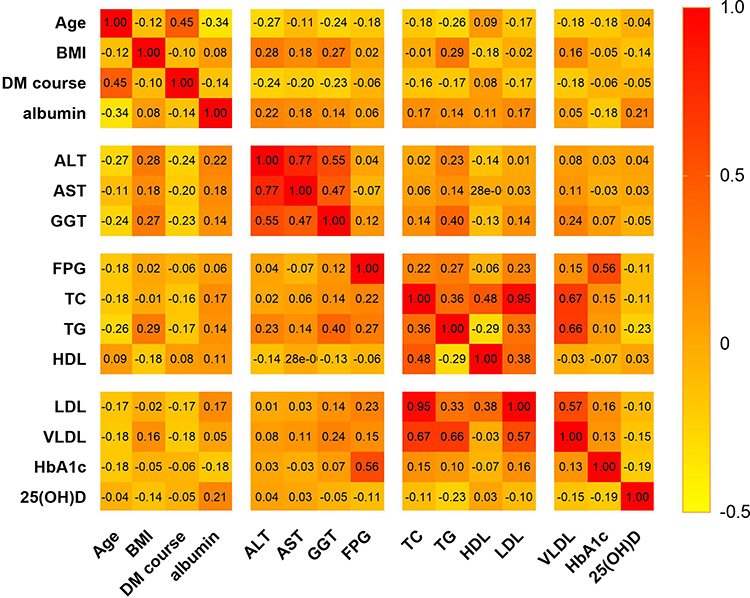 |
Figure 3 Spearman correlation analysis of 25(OH)D with potential risk factors for NAFLD. |
Multivariate Logistic Regression Analyses of NAFLD and Associated Factors
Multiple logistic regression analysis was employed to examine whether vitamin D deficiency was independently and significantly associated with the presence of NAFLD in T2DM patients. For all T2DM patients, vitamin D deficiency was significantly associated with a higher prevalence of NAFLD. Specifically, T2DM patients with vitamin D deficiency had a 2.045 (95% CI: 1.167, 3.583) times higher risk of developing NAFLD than those without vitamin D deficiency (Table 3).
 |
Table 3 Logistic Regression Analysis of Vitamin D Deficiency for NAFLD in Patients with T2DM |
Vitamin D deficiency was not associated with high NAFLD preference in T2DM patients with BMI ≤23 kg/m2, (P = 0.216 for model 1, P = 0.754 for model 2, and P = 0.838 for model 3) (Table 4). Vitamin D deficiency was associated with high NAFLD preference in T2DM patients with BMI >23kg/m2, regardless of whether an unadjusted or adjusted model was used (P = 0.004 for model 1, P = 0.003 for model 2, and P = 0.016 for model 3) (Table 5).
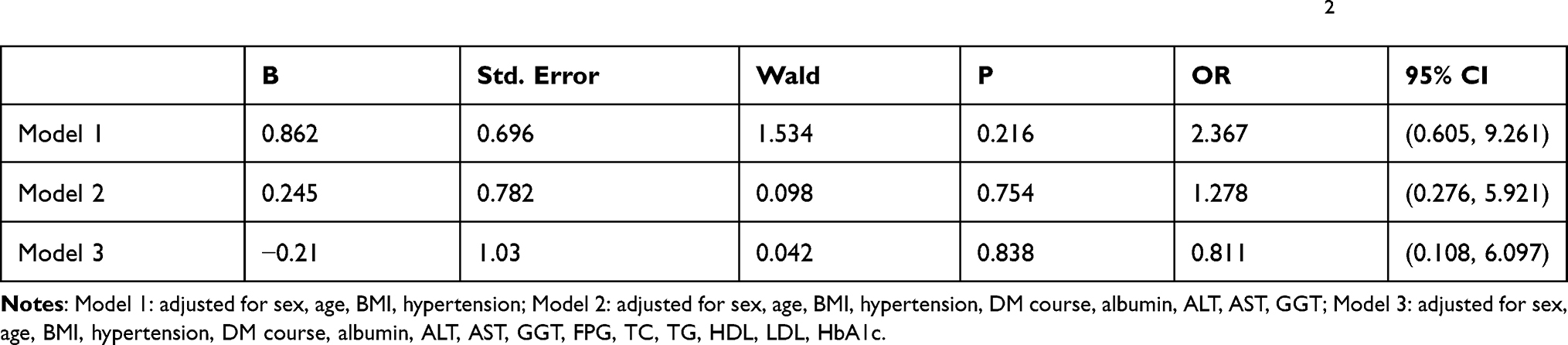 |
Table 4 Logistic Regression Analysis of Vitamin D Deficiency for NAFLD in T2DM Patients with BMI ≤23kg/m2 |
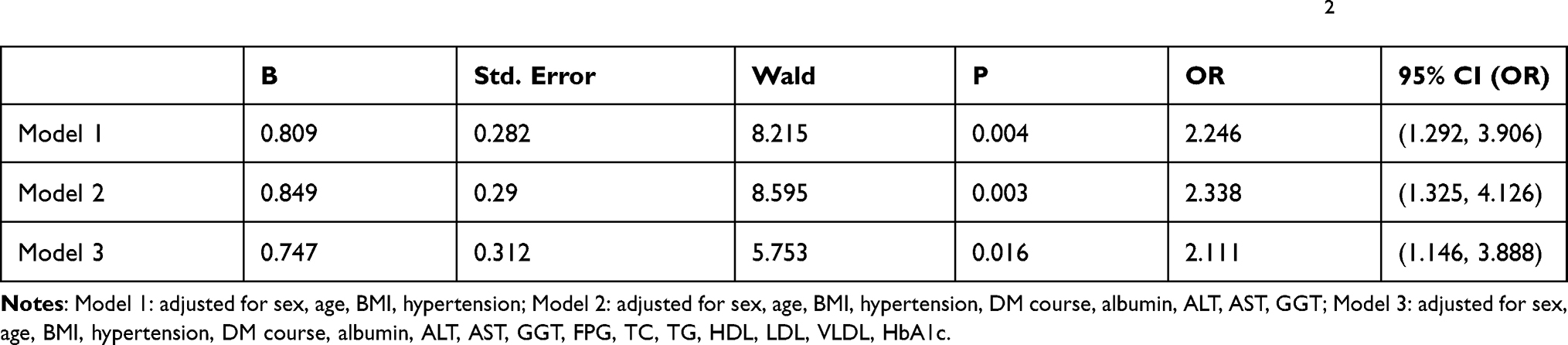 |
Table 5 Logistic Regression Analysis of Vitamin D Deficiency for NAFLD in T2DM Patients with BMI >23kg/m2 |
Subgroup Analysis
To further investigate the impact of other risk factors on the correlation of vitamin D deficiency with NAFLD risk in T2DM patients with BMI >23 kg/m2, subgroup analyses were carried according to sex, age, history of hypertension, TG, HDL and HbA1c. Table 6 has summarized the results of subgroup analysis results. The significant correlation between vitamin D deficiency and NAFLD was found in participants with age≤65 years, without hypertension, TG<1.7mmol/l, HDL≥1 mmol/l in men, ≥1.3 mmol/l in women, HBA1C ≤7%, or females.
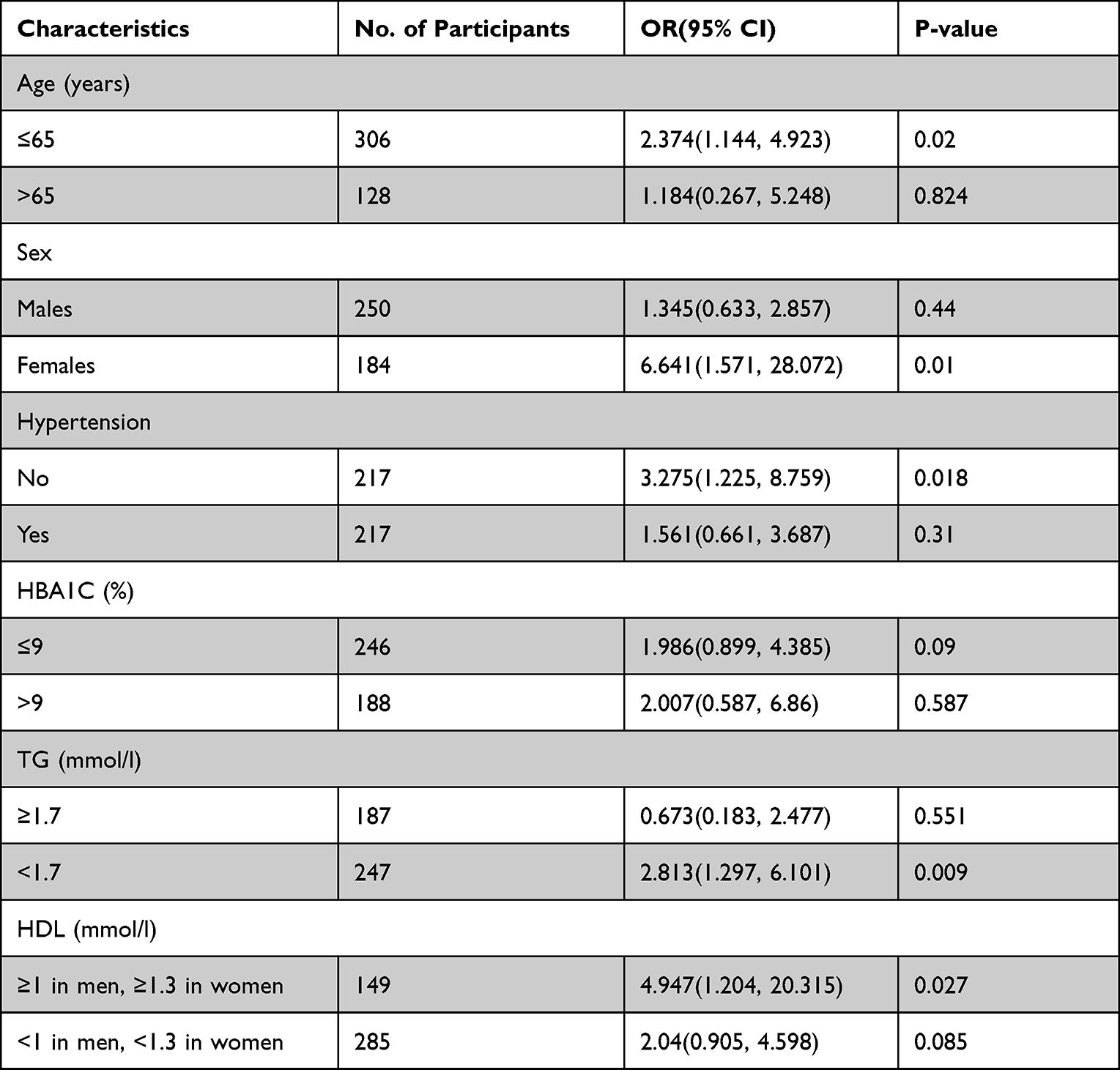 |
Table 6 Effect of Vitamin D Deficiency on NAFLD Risk Stratified by Subgroups |
Discussion
The results of this study revealed that the 25(OH)D level in patients with T2DM complicated by NAFLD was significantly lower than that in patients with T2DM only. It was consistent with the result of Xiu et al.29 Recently, it was shown that bariatric surgery could also influence vitamin D levels in obese patients.30 No patients in this study underwent bariatric surgery. A meta-analysis of 10 RCTs (randomized controlled trials) showed that Sodium-Glucose Transporter 2 (SGLT2) inhibitors could remarkably reduce hepatic enzymes and hepatic fat.31 Another meta-analysis found that pioglitazone could significantly improve the histological performance of the liver and insulin sensitivity.32 Moreover, this study demonstrated that none of the T2DM patients used SGLT2 inhibitors or pioglitazone.
Our results indicated that vitamin D deficiency was highly prevalent among T2DM patients with NAFLD. It was demonstrated that the relation between vitamin D deficiency and NAFLD was bidirectional. On the one hand, vitamin D (either synthesized in the skin – cholecalciferol – or obtained from dietary – ergocalciferol) was metabolized within the liver to 25(OH) D and within the kidneys to the biologically active (1,25- dihydroxy vitamin D).33 On the other hand, insulin resistance was at the root of both T2DM and NAFLD, and vitamin D may significantly impact insulin sensibilization through its anti-inflammatory effects and its role in regulating insulin secretion.34
Because obesity was a confounding factor,35 we measured BMI, a surrogate measure of obesity, and it had also mainly been demonstrated.36 Several recent studies recommend that BMI may be best maintained within 23kg/m2.37–41 Therefore, we performed multiple regression analysis in all T2DM subjects and T2DM patients with BMI>23kg/m2 and BMI ≤23kg/m2, respectively. We observed that vitamin D deficiency was an independent risk factor for NAFLD in T2DM patients, especially in those with BMI >23kg/m2.
The explanation for why obese and lean individuals have inconsistent correlations between vitamin D and NAFLD remains unclear, although several possibilities exist.42 First, obesity could be a contributing factor to low vitamin D levels. Second, patients with vitamin D deficiency have higher serum levels of proinflammatory cytokines, which promote NAFLD development. Third, under vitamin D deficiency conditions, the flow of free fatty acids (FFAs) in the blood increases, and fat deposition into hepatocytes is accelerated, contributing to the progress of NAFLD.
It was recognised that a strong association between a low level of 25(OH)D and NAFLD existed in patients with T2DM.43 Another study conducted in Korea has also reported similar results indicating a negative association between 25(OH)D and NAFLD after adjustment for potential confounders.44 Recently, Nelson et al45 reported that 25(OH)D deficiency was commonly associated with the increased risk of NAFLD diagnosed by liver biopsy. In a meta-analysis by Eliades et al,20 25(OH)D level was lower in patients diagnosed with NAFLD. In addition, several studies have demonstrated that vitamin D status was associated with dyslipidemia, inflammation, insulin resistance, oxidative stress and obesity.11,46–49 Vitamin D levels can be modulated by consuming other drugs/supplements, eg, omega-3 fatty acids.50 Thus, there have been recommendations that taking vitamin supplements may potentially contribute to NAFLD treatment. However, the results are inconsistent. Findings by Talaei et al51 suggested that a 2-month course of vitamin D supplementation improved insulin resistance in patients with T2DM. A study by Papapostoli et al52 had demonstrated that vitamin D supplementation reduced the severity of hepatic steatosis in patients with NAFLD. The results of Barchetta et al7 revealed that hepatic steatosis was not able to improve after 24 weeks of supplementation of vitamin D. As pointed out by Heaney,53 a central bias behind the inconsistent results from trials on the effects of vitamin D supplementation may be represented by the well-known physiology of nutrients, which do not show the dose–response relation observed for most drugs. Results from a recent meta-analysis that included 16 RCTs indicated that Vitamin D supplementation could be considered an effective strategy in managing patients with NAFLD.54 Patients with NAFLD were also prone to develop liver fibrosis and even liver cancer if they were associated with vitamin D deficiency.55,56
Vitamin D deficiency may play a role in the pathogenesis of NAFLD by decreasing the expression of the glucose transporter, reducing hepatic glucose output, and stimulating intrahepatic lipid synthesis.57 Thus, a low serum vitamin D level was potentially prone to intrahepatic lipid accumulation, leading to NAFLD. The first “two hits” theory of NAFLD pathogenesis mainly involved insulin resistance and excessive free fatty acids in the circulation.58 Vitamin D decreased insulin resistance induced by free fatty acids in peripheral tissues and hepatocytes.59 In addition, Thais et al’s study60 also showed insulin resistance could be improved in vitamin D-supplemented animals. Moreover, they proved vitamin D deficiency had a particularly adverse impact on metabolism, hepatic steatosis, and changes caused by hepatic stellate cell activation (liver fibrosis, β-oxidation, lipogenesis, and liver inflammation). Animals appeared to improve all these data after vitamin D supplementation.
Oxidative stress was considered the second hit of the “two hits” theory of NAFLD pathogenesis. Some studies have demonstrated higher oxidative stress biomarkers in people with a low 25(OH)D level. Intake of vitamin D also decreased oxidative stress.61,62 Indeed, Eftekhari et al63 found that the intake of calcitriol (1,25(OH)2D3) significantly reduced TC, LDL, TG, and malondialdehyde levels in patients with T2DM. They concluded that 1, 25(OH)2D3 could reduce oxidative stress and improve lipid profiles. Nakano et al64 recently found that sunlight therapy ameliorated hepatocyte inflammation and fibrosis by regulating lipid transfer/metabolic. Inflammation could also lead to the development and progression of NAFLD.65 Vitamin D was also known to exhibit anti-inflammatory effects on macrophages.66 The study also demonstrated that vitamin D deficiency was associated with impaired T lymphocyte immune function and increased inflammation through elevated levels of proinflammatory cytokines.67 A potentially novel insight was provided into the interactions of the liver and intestine in the progression and pathogenesis of NAFLD.68 Vitamin D deficiency facilitated non-alcoholic steatohepatitis progression by impaired enterohepatic circulation in animal models.69 Hamed et al showed that the NAFLD patients with T2DM were characterized by different gut compositions,70 which supported the role of gut microbiota in the pathogenesis of T2DM and NAFLD. The findings from this study suggest intake of vitamin D should be emphasized in order to prevent NAFLD in obese T2DM populations.
The present study had a few limitations. Firstly, a causal relationship cannot be established due to the cross-sectional study design. Further studies are required to evaluate the causative relationships between 25(OH)D and NAFLD, the effect of vitamin D supplementation on NAFLD, and patients with T2DM. Secondly, the diagnosis of NAFLD was based on ultrasonography and the exclusion of other known causes of liver disease but was not confirmed by liver biopsy. Third, the BMI classification criteria applied in this study are limited to Asian people, so our findings may not be generalizable to other ethnic populations.
Conclusion
This study suggests that T2DM peope with BMI >23kg/m2 were more susceptible to NAFLD by vitamin D deficiency and that it is necessary to maintain optimal serum vitamin D levels in this population.
Data Sharing Statement
The original data can be available by email request at any time (Yuling Xing:[email protected]).
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Farrell GC, Larter CZ. Nonalcoholic fatty liver disease: from steatosis to cirrhosis. Hepatology. 2006;43(2 Suppl 1):S99–s112. doi:10.1002/hep.20973
2. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
3. Amiri Dash Atan N, Koushki M, Motedayen M, et al. Type 2 diabetes mellitus and non-alcoholic fatty liver disease: a systematic review and meta-analysis. Gastroenterol Hepatol Bed Bench. 2017;10(Suppl1):S1–s7.
4. Dai W, Ye L, Liu A, et al. Prevalence of nonalcoholic fatty liver disease in patients with type 2 diabetes mellitus: a meta-analysis. Medicine. 2017;96(39):e8179. doi:10.1097/MD.0000000000008179
5. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am J Gastroenterol. 2012;107(6):811–826. doi:10.1038/ajg.2012.128
6. Mikolasevic I, Milic S, Turk Wensveen T, et al. Nonalcoholic fatty liver disease - A multisystem disease? World J Gastroenterol. 2016;22(43):9488–9505. doi:10.3748/wjg.v22.i43.9488
7. Barchetta I, Del Ben M, Angelico F, et al. No effects of oral vitamin D supplementation on non-alcoholic fatty liver disease in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled trial. BMC Med. 2016;14:92. doi:10.1186/s12916-016-0638-y
8. Christakos S, Dhawan P, Verstuyf A, Verlinden L, Carmeliet G. Vitamin D: metabolism, molecular mechanism of action, and pleiotropic effects. Physiol Rev. 2016;96(1):365–408. doi:10.1152/physrev.00014.2015
9. Tsuprykov O, Chen X, Hocher CF, Skoblo R, Lianghong Y, Hocher B. Why should we measure free 25(OH) vitamin D? J Steroid Biochem Mol Biol. 2018;180:87–104. doi:10.1016/j.jsbmb.2017.11.014
10. Pham H, Waterhouse M, Baxter C, et al. The effect of vitamin D supplementation on acute respiratory tract infection in older Australian adults: an analysis of data from the D-Health Trial. Lancet Diabetes Endocrinol. 2021;9(2):69–81. doi:10.1016/S2213-8587(20)30380-6
11. Gagnon C, Lu ZX, Magliano DJ, et al. Low serum 25-hydroxyvitamin D is associated with increased risk of the development of the metabolic syndrome at five years: results from a national, population-based prospective study (The Australian Diabetes, Obesity and Lifestyle Study: ausDiab). J Clin Endocrinol Metab. 2012;97(6):1953–1961. doi:10.1210/jc.2011-3187
12. Lips P, Eekhoff M, van Schoor N, et al. Vitamin D and type 2 diabetes. J Steroid Biochem Mol Biol. 2017;173:280–285. doi:10.1016/j.jsbmb.2016.11.021
13. Sacerdote A, Dave P, Lokshin V, Bahtiyar G. Type 2 diabetes mellitus, insulin resistance, and Vitamin D. Curr Diab Rep. 2019;19(10):101. doi:10.1007/s11892-019-1201-y
14. Rhee EJ, Kim MK, Park SE, et al. High serum vitamin D levels reduce the risk for nonalcoholic fatty liver disease in healthy men independent of metabolic syndrome. Endocr J. 2013;60(6):743–752. doi:10.1507/endocrj.EJ12-0387
15. Manson JE, Cook NR, Lee IM, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33–44. doi:10.1056/NEJMoa1809944
16. Pollock RD, Duggal NA, Lazarus NR, Lord JM, Harridge SDR. Cardiorespiratory fitness not sedentary time or physical activity is associated with cardiometabolic risk in active older adults. Scand J Med Sci Sports. 2018;28(6):1653–1660. doi:10.1111/sms.13071
17. Holick MF. The vitamin D deficiency pandemic: approaches for diagnosis, treatment and prevention. Rev Endocr Metab Disord. 2017;18(2):153–165. doi:10.1007/s11154-017-9424-1
18. Jiang Z, Pu R, Li N, et al. High prevalence of vitamin D deficiency in Asia: a systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2021;1–10. doi:10.1080/10408398.2021.1990850
19. Dasarathy J, Periyalwar P, Allampati S, et al. Hypovitaminosis D is associated with increased whole body fat mass and greater severity of non-alcoholic fatty liver disease. Liver Int. 2014;34(6):e118–127. doi:10.1111/liv.12312
20. Eliades M, Spyrou E, Agrawal N, et al. Meta-analysis: vitamin D and non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2013;38(3):246–254. doi:10.1111/apt.12377
21. Găman MA, Dobrică EC, Cozma MA, et al. Crosstalk of magnesium and serum lipids in dyslipidemia and associated disorders: a systematic review. Nutrients. 2021;13(5):1411. doi:10.3390/nu13051411
22. Sohouli MH, Sayyari AA, Lari A, et al. Association of dietary insulinaemic potential and odds of non-alcoholic fatty liver disease among adults: a case-control study. J Hum Nutr Diet. 2021;34(5):901–909. doi:10.1111/jhn.12865
23. Lonardo A, Nascimbeni F, Mantovani A, Targher G. Hypertension, diabetes, atherosclerosis and NASH: cause or consequence? J Hepatol. 2018;68(2):335–352. doi:10.1016/j.jhep.2017.09.021
24. Loomba R, Abraham M, Unalp A, et al. Association between diabetes, family history of diabetes, and risk of nonalcoholic steatohepatitis and fibrosis. Hepatology. 2012;56(3):943–951. doi:10.1002/hep.25772
25. Li Y, Wang J, Tang Y, et al. Bidirectional association between nonalcoholic fatty liver disease and type 2 diabetes in Chinese population: evidence from the Dongfeng-Tongji cohort study. PLoS One. 2017;12(3):e0174291. doi:10.1371/journal.pone.0174291
26. Bril F, Cusi K. Nonalcoholic fatty liver disease: the new complication of type 2 diabetes mellitus. Endocrinol Metab Clin North Am. 2016;45(4):765–781. doi:10.1016/j.ecl.2016.06.005
27. Fukuda T, Hamaguchi M, Kojima T, et al. Transient remission of nonalcoholic fatty liver disease decreases the risk of incident type 2 diabetes mellitus in Japanese men. Eur J Gastroenterol Hepatol. 2016;28(12):1443–1449. doi:10.1097/MEG.0000000000000736
28. Hamaguchi M, Kojima T, Itoh Y, et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am J Gastroenterol. 2007;102(12):2708–2715. doi:10.1111/j.1572-0241.2007.01526.x
29. Xiu L, Jiang T, Yao XA, Wen Z. Correlation between 25 Hydroxyvitamin D levels and nonalcoholic fatty liver disease in Chinese patients with type 2 diabetes mellitus: a cross-sectional study. Int J Gen Med. 2021;14:3099–3107. doi:10.2147/IJGM.S319449
30. Bourbour F, Kabir A, Pazouki A, et al. Trends in serum Vitamin D levels within 12 months after One Anastomosis Gastric Bypass (OAGB). Obes Surg. 2021;31(9):3956–3965. doi:10.1007/s11695-021-05434-6
31. Wei Q, Xu X, Guo L, Li J, Li L. Effect of SGLT2 inhibitors on type 2 diabetes mellitus with non-alcoholic fatty liver disease: a meta-analysis of randomized controlled trials. Front Endocrinol. 2021;12:635556. doi:10.3389/fendo.2021.635556
32. Lian J, Fu J. Pioglitazone for NAFLD patients with prediabetes or type 2 diabetes mellitus: a meta-analysis. Front Endocrinol. 2021;12:615409. doi:10.3389/fendo.2021.615409
33. Bjelakovic G, Nikolova D, Bjelakovic M, Gluud C. Vitamin D supplementation for chronic liver diseases in adults. Cochrane Database Syst Rev. 2017;11(11):Cd011564. doi:10.1002/14651858.CD011564.pub2
34. Hosny SS, Ali HM, Mohammed WA, El Ghannam MH. Study of relationship between total vitamin D level and NAFLD in a sample of Egyptian patients with and without T2DM. Diabetes Metab Syndr. 2019;13(3):1769–1771. doi:10.1016/j.dsx.2019.04.002
35. Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72(3):690–693. doi:10.1093/ajcn/72.3.690
36. Flegal KM, Shepherd JA, Looker AC, et al. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am J Clin Nutr. 2009;89(2):500–508. doi:10.3945/ajcn.2008.26847
37. Caleyachetty R, Barber TM, Mohammed NI, et al. Ethnicity-specific BMI cutoffs for obesity based on type 2 diabetes risk in England: a population-based cohort study. Lancet Diabetes Endocrinol. 2021;9(7):419–426. doi:10.1016/S2213-8587(21)00088-7
38. Teufel F, Seiglie JA, Geldsetzer P, et al. Body-mass index and diabetes risk in 57 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 685 616 adults. Lancet. 2021;398(10296):238–248. doi:10.1016/S0140-6736(21)00844-8
39. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
40. Wang L, Zhou B, Zhao Z, et al. Body-mass index and obesity in urban and rural China: findings from consecutive nationally representative surveys during 2004–18. Lancet. 2021;398(10294):53–63. doi:10.1016/S0140-6736(21)00798-4
41. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9(6):373–392. doi:10.1016/S2213-8587(21)00045-0
42. Wang Q, Shi X, Wang J, Zhang J, Xu C. Low serum vitamin D concentrations are associated with obese but not lean NAFLD: a cross-sectional study. Nutr J. 2021;20(1):30. doi:10.1186/s12937-021-00690-9
43. Barchetta I, Angelico F, Del Ben M, et al. Strong association between non alcoholic fatty liver disease (NAFLD) and low 25(OH) vitamin D levels in an adult population with normal serum liver enzymes. BMC Med. 2011;9:85. doi:10.1186/1741-7015-9-85
44. Seo JA, Eun CR, Cho H, et al. Low vitamin D status is associated with nonalcoholic Fatty liver disease independent of visceral obesity in Korean adults. PLoS One. 2013;8(10):e75197. doi:10.1371/journal.pone.0075197
45. Nelson JE, Roth CL, Wilson LA, et al. Vitamin D deficiency is associated with increased risk of non-alcoholic steatohepatitis in adults with non-alcoholic fatty liver disease: possible role for MAPK and NF-κB? Am J Gastroenterol. 2016;111(6):852–863. doi:10.1038/ajg.2016.51
46. Farhangi MA, Mesgari-Abbasi M, Hajiluian G, Nameni G, Shahabi P. Adipose tissue inflammation and oxidative stress: the ameliorative effects of Vitamin D. Inflammation. 2017;40(5):1688–1697. doi:10.1007/s10753-017-0610-9
47. Asemi Z, Hashemi T, Karamali M, Samimi M, Esmaillzadeh A. Effects of vitamin D supplementation on glucose metabolism, lipid concentrations, inflammation, and oxidative stress in gestational diabetes: a double-blind randomized controlled clinical trial. Am J Clin Nutr. 2013;98(6):1425–1432. doi:10.3945/ajcn.113.072785
48. Mohammadi SM, Eghbali SA, Soheilikhah S, et al. The effects of vitamin D supplementation on adiponectin level and insulin resistance in first-degree relatives of subjects with type 2 diabetes: a randomized double-blinded controlled trial. Electron Phy. 2016;8(9):2849–2854. doi:10.19082/2849
49. Mutt SJ, Hyppönen E, Saarnio J, Järvelin MR, Herzig KH. Vitamin D and adipose tissue-more than storage. Front Physiol. 2014;5:228. doi:10.3389/fphys.2014.00228
50. Alhabeeb H, Kord-Varkaneh H, Tan SC, et al. The influence of omega-3 supplementation on vitamin D levels in humans: a systematic review and dose-response meta-analysis of randomized controlled trials. Crit Rev Food Sci Nutr. 2020;1–8. doi:10.1080/10408398.2020.1863905
51. Talaei A, Mohamadi M, Adgi Z. The effect of vitamin D on insulin resistance in patients with type 2 diabetes. Diabetol Metab Syndr. 2013;5(1):8. doi:10.1186/1758-5996-5-8
52. Papapostoli I, Lammert F, Stokes CS. Effect of short-term Vitamin D correction on hepatic steatosis as quantified by controlled attenuation parameter (CAP). J Gastrointestin Liver Dis. 2016;25(2):175–181. doi:10.15403/jgld.2014.1121.252.cap
53. Heaney RP. Vitamin D–baseline status and effective dose. N Engl J Med. 2012;367(1):77–78. doi:10.1056/NEJMe1206858
54. Rezaei S, Tabrizi R, Nowrouzi-Sohrabi P, et al. The effects of Vitamin D supplementation on anthropometric and biochemical indices in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Front Pharmacol. 2021;12:732496. doi:10.3389/fphar.2021.732496
55. Gheorghe G, Bungău S, Ceobanu G, et al. The non-invasive assessment of hepatic fibrosis. J Formos Med Assoc. 2021;120(2):794–803. doi:10.1016/j.jfma.2020.08.019
56. Zhang Y, Jiang X, Li X, et al. Serum Vitamin D levels and risk of liver cancer: a systematic review and dose-response meta-analysis of cohort studies. Nutr Cancer. 2021;73(8):1–9. doi:10.1080/01635581.2020.1797127
57. Benedict M, Zhang X. Non-alcoholic fatty liver disease: an expanded review. World J Hepatol. 2017;9(16):715–732. doi:10.4254/wjh.v9.i16.715
58. Day CP, James OF. Steatohepatitis: a tale of two “hits”? Gastroenterology. 1998;114(4):842–845. doi:10.1016/S0016-5085(98)70599-2
59. Zhou QG, Hou FF, Guo ZJ, Liang M, Wang GB, Zhang X. 1,25-Dihydroxyvitamin D improved the free fatty-acid-induced insulin resistance in cultured C2C12 cells. Diabetes Metab Res Rev. 2008;24(6):459–464. doi:10.1002/dmrr.873
60. Maia-Ceciliano TC, Dutra RR, Aguila MB, Mandarim-de-lacerda CA. The deficiency and the supplementation of vitamin D and liver: lessons of chronic fructose-rich diet in mice. J Steroid Biochem Mol Biol. 2019;192:105399. doi:10.1016/j.jsbmb.2019.105399
61. Tamadon MR, Soleimani A, Keneshlou F, et al. Clinical trial on the effects of Vitamin D supplementation on metabolic profiles in diabetic hemodialysis. Horm Metab Res. 2018;50(1):50–55. doi:10.1055/s-0043-119221
62. Tarcin O, Yavuz DG, Ozben B, et al. Effect of vitamin D deficiency and replacement on endothelial function in asymptomatic subjects. J Clin Endocrinol Metab. 2009;94(10):4023–4030. doi:10.1210/jc.2008-1212
63. Eftekhari MH, Akbarzadeh M, Dabbaghmanesh MH, Hassanzadeh J. The effect of calcitriol on lipid profile and oxidative stress in hyperlipidemic patients with type 2 diabetes mellitus. ARYA Atheroscler. 2014;10(2):82–88.
64. Nakano T, Cheng YF, Lai CY, et al. Impact of artificial sunlight therapy on the progress of non-alcoholic fatty liver disease in rats. J Hepatol. 2011;55(2):415–425. doi:10.1016/j.jhep.2010.11.028
65. Caldwell SH, Argo CK. Divergent effects of peroxisome proliferator-activated receptor-gamma ligands in human and mouse nonalcoholic steatohepatitis. Hepatology. 2007;46(2):285–287. doi:10.1002/hep.21881
66. Haussler MR, Haussler CA, Bartik L, et al. Vitamin D receptor: molecular signaling and actions of nutritional ligands in disease prevention. Nutr Rev. 2008;66(10 Suppl 2):S98–112. doi:10.1111/j.1753-4887.2008.00093.x
67. Ford ES, Ajani UA, McGuire LC, Liu S. Concentrations of serum vitamin D and the metabolic syndrome among U.S. adults. Diabetes Care. 2005;28(5):1228–1230. doi:10.2337/diacare.28.5.1228
68. Abenavoli L, Milic N, Di Renzo L, Preveden T, Medić-Stojanoska M, De Lorenzo A. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. World j Gastroenterol. 2016;22(31):7006–7016. doi:10.3748/wjg.v22.i31.7006
69. Kong M, Zhu L, Bai L, et al. Vitamin D deficiency promotes nonalcoholic steatohepatitis through impaired enterohepatic circulation in animal model. Am J Physiol Gastrointest Liver Physiol. 2014;307(9):G883–893. doi:10.1152/ajpgi.00427.2013
70. Ebrahimzadeh Leylabadlo H, Samadi Kafil H, Farajnia S, et al. Gut microbiota in nonalcoholic fatty liver diseases with and without type-2 diabetes mellitus. Eur J Gastroenterol Hepatol. 2021;33:e548–e554. doi:10.1097/MEG.0000000000002140
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.