Back to Journals » Clinical Ophthalmology » Volume 19
The Association Between the Retinal Sequelae of Myopia and Glaucoma in a Global Cohort
Authors Arnal LI, Mesfin Y, Ferreira G ![]() , Salvi A, Wai KM, Koo E, Kossler AL
, Salvi A, Wai KM, Koo E, Kossler AL ![]() , Koo E, Rahimy E, Mruthyunjaya P, Ludwig CA
, Koo E, Rahimy E, Mruthyunjaya P, Ludwig CA ![]()
Received 25 May 2025
Accepted for publication 7 October 2025
Published 11 October 2025 Volume 2025:19 Pages 3749—3760
DOI https://doi.org/10.2147/OPTH.S542692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yousef Fouad
Leo Itzel Arnal,1 Yeabsira Mesfin,2 Gabriel Ferreira,3 Anish Salvi,1 Karen M Wai,1 Eubee Koo,1 Andrea L Kossler,1 Euna Koo,1 Ehsan Rahimy,1,4 Prithvi Mruthyunjaya,1 Chase A Ludwig1
1Department of Ophthalmology, Byers Eye Institute, Stanford University School of Medicine, Palo Alto, CA, USA; 2Department of Ophthalmology, University of California San Francisco School of Medicine, San Francisco, CA, USA; 3Department of Medicine, Várzea Grande University Center (UNIVAG), Várzea Grande, Brazil; 4Department of Ophthalmology, Palo Alto Medical Foundation, Palo Alto, CA, USA
Correspondence: Chase A Ludwig, Department of Ophthalmology, Byers Eye Institute, 2370 Watson Court, Office 100D, Palo Alto, CA, 94303, USA, Tel +1 650 724 2722, Fax +1 650 853 6086, Email [email protected]
Purpose: Discerning glaucoma in myopic eyes with tilted optic nerve discs is challenging given the atypical appearance and segmentation on optical coherence tomography. This study aims to determine the association between retinal sequelae of myopia and primary open-angle glaucoma (POAG). We hypothesize that retinal sequelae of myopia may aid in identifying high-risk glaucoma patients.
Methods: An aggregated electronic health records research network was used to retrospectively identify 929,142 myopic patients. We evaluated the association of POAG with retinal sequelae of myopia, including choroidal neovascularization (CNV), myopic macular degeneration (MMD), foveoschisis, macular hole (MH), rhegmatogenous retinal detachment (RRD), and foveal retinal detachment (FRD). Logistic regressions estimated odds ratios (adjusted for age, sex, race, and ethnicity). Cox models estimated hazard ratios (additionally adjusted for pseudophakia).
Results: FRD exhibited the strongest association with POAG (AOR: 5.82; 95% CI: 3.44– 9.85), followed by foveoschisis (AOR: 3.10; 95% CI: 1.84– 5.21) and MMD (AOR: 2.87; 95% CI: 2.19– 3.75). Severe subtypes of POAG were also more highly associated with each retinal sequela than moderate and milder severity subtypes. Additionally, patients with each retinal sequela experienced a significantly faster progression from glaucoma suspect to POAG than those without these sequelae. Kaplan-Meier curves and adjusted Cox regression models suggested a faster progression from glaucoma suspect to POAG in those with foveoschisis (HR: 5.33; 95% CI: 2.21– 12.85; p< 0.005), CNV (HR: 1.73; 95% CI: 1.12– 2.67; p=0.01), MMD (HR: 2.74; 95% CI: 1.47– 5.10; p< 0.005), MH (HR: 1.73; 95% CI: 1.29– 2.31; p< 0.005), and RRD (HR: 1.54; 95% CI: 1.28– 1.86; p< 0.005), whereas FRD was not significantly associated with glaucoma progression (HR: 1.28; 95% CI: 0.18– 9.10; p=0.8).
Conclusion: The retinal sequelae of myopia are associated with the presence and progression of primary open-angle glaucoma. The presence of the retinal sequelae of myopia should cue ophthalmologists to refer such patients for glaucoma evaluation to encourage earlier detection and more targeted management.
Keywords: glaucoma, myopia, retinal sequelae, primary open-angle glaucoma
Introduction
The global prevalence of myopia is on the rise, with projections suggesting that nearly half of the world’s population will be affected by 2050.1 This trend indicates a surge not only in mild and moderate myopia but also in high myopia, which is often associated with severe ocular complications such as myopic macular degeneration (MMD), myopic traction maculopathy, and rhegmatogenous retinal detachments (RRD).2 The rising incidence of these conditions will contribute significantly to the overall global burden of visual impairment, emphasizing the need for targeted ocular health strategies and comprehensive understanding of myopia’s progression and impact.
Concurrently, glaucoma stands as a major global health issue and is one of the leading causes of irreversible blindness worldwide.3 This condition affects millions, with significant variations in prevalence across different regions and demographics, notably higher in populations of African and Asian descent.4 The burden of glaucoma extends beyond the loss of vision, impacting the quality of life and economic stability of individuals and communities.5 The disease’s asymptomatic progression often leads to late detection, making management and treatment more challenging and reinforcing the need for regular screening and advanced diagnostic approaches.6
Every millimeter increase in axial length is known to elevate the risk of myopia complications including both glaucoma and the retinal sequelae of myopia, yet the specific interactions between these complications of myopia have not been comprehensively studied.7 The study herein explores the intricate relationship between these two major causes of vision loss worldwide: myopia and glaucoma. By leveraging a large electronic health record (EHR) dataset, this paper aims to delineate the associations between retinal sequelae of myopia, such as choroidal neovascularization (CNV), MMD, foveoschisis, macular hole (MH), foveal retinal detachment (FRD), and RRD, and the progression of primary open-angle glaucoma (POAG), providing new insights into potential high-risk profiles and contributing to better clinical outcomes through targeted preventive care.
Methods
This research was conducted using data collection and analysis facilitated by TriNetX (Cambridge, MA, USA). The TriNetX Health Research Network aggregates anonymized EHR from over 124 million patients in nine countries, involving 60 healthcare organizations within the USA between January 1, 2003, and April 10, 2024. The network adheres to HIPAA regulations and is ISO 27001:2013 certified. The employment of anonymized and aggregated patient data meant that Institutional Review Board approval was not required for this study. The data, accessed from the TriNetX platform on April 10, 2024, offer a wide array of EHR information including patient diagnoses, treatment protocols, prescription details, laboratory results, and genetic information. This study was conducted in compliance with the STROBE guidelines, which are standards for reporting observational cohort studies.
Inclusion criteria included all patients who had an outpatient office visit and were diagnosed with myopia, as defined by International Classification of Diseases (ICD) codes and Current Procedural Terminology (CPT) codes (Table 1). The outcome of interest was POAG, with exposure to the following retinal sequelae of myopia: CNV, MMD, foveoschisis, MH, RRD, and FRD. Race categories included Asian, American Indian, Black or African American, Native Hawaiian, White, Unknown, or Other, sourced from TriNetX. Similarly, ethnicity categories encompassed Hispanic or Latino, Not Hispanic or Latino, and Unknown.
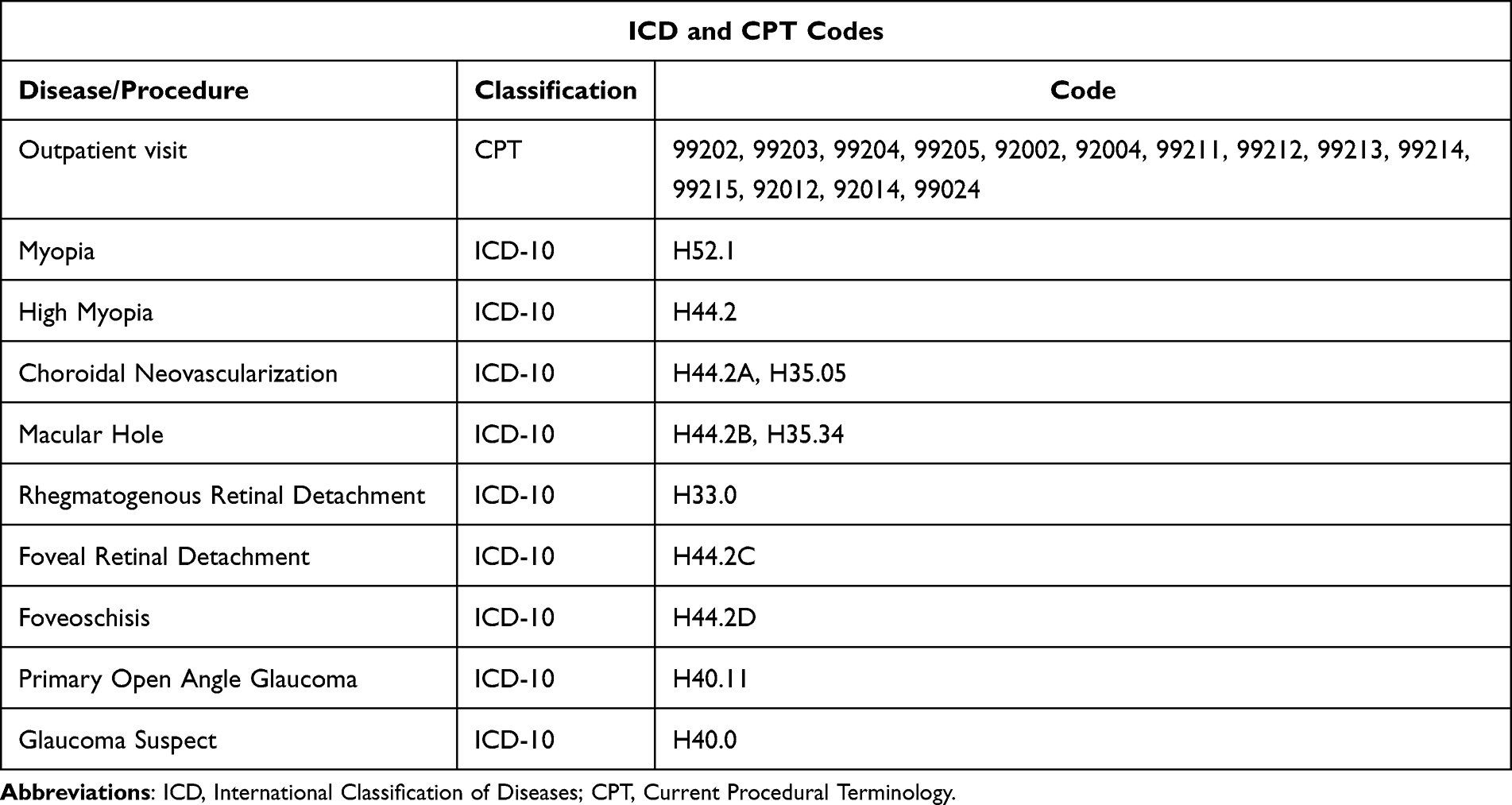 |
Table 1 ICD and CPT Codes Used to Extract Patient Data from the TriNetx Database |
We characterized patients with myopia (ICD-10 H52.1) and high myopia (ICD-10 H44.2) from TriNetX, stratified by age (0–19, 20–29, …, ≥90), sex, race, and ethnicity, and also characterized myopic patients with and without each retinal sequela. Chi-square tests were used to compare differences between myopes and high myopes. Two logistic regression models were run. Both compared those with each retinal sequela to those without. In the first model, we estimated crude odds ratios (OR) and adjusted odds ratios (AOR), adjusted for age, sex, race, ethnicity. The second model estimated the odds of POAG severity (mild, moderate, severe, other, none) among those with each retinal sequela versus those without, adjusted for the same covariates.
Lastly, a time-to-event analysis was conducted among myopic patients to examine the association between the diagnosis of any retinal sequela and the progression from a diagnosis of glaucoma suspect to POAG, using Cox regression analysis to yield hazard ratios (HR). The model was adjusted for age, sex, race, ethnicity, and the presence of pseudophakia. Kaplan-Meier curves were plotted to visualize the difference in survival, and the Log rank test was used to assess statistical significance. All statistical analyses were conducted using Python (dask, pandas, sklearn, lifelines).
Results
Table 1 outlines the ICD-10 and CPT codes utilized to extract patient data. Table 2 presents the baseline characteristics of myopic and highly myopic patients in TriNetX. Our cohort consisted of 929,142 patients, of which 12,567 patients were diagnosed with at least one of the retinal sequelae analyzed in this study. Overall, 550,760 (59.28%) patients identified as female. For race, 571,520 (61.5%) identified as White, 97,498 (10.49%) as unknown, 49,963 (5.38%) as Asian, 151,395 (16.29%) as Black or African American, 4205 (0.45%) as American Indian or Alaska Native, 2283 (0.25%) as Native Hawaiian or Other Pacific Islander, and 52,278 (5.63%) as other races. Regarding ethnicity, 103,693 (11.2%) identified as Hispanic or Latino, 666,498 (71.73%) as Not Hispanic or Latino, and 158,951 (17.11%) as unknown. Differences among each of these groups were found to be statistically significant (p<0.001). A statistically significant difference was observed when comparing myopes to high myopes across age, sex, race, and ethnicity (p<0.001). Demographic characteristics across each of the retinal sequelae are outlined in Supplemental Table 1.
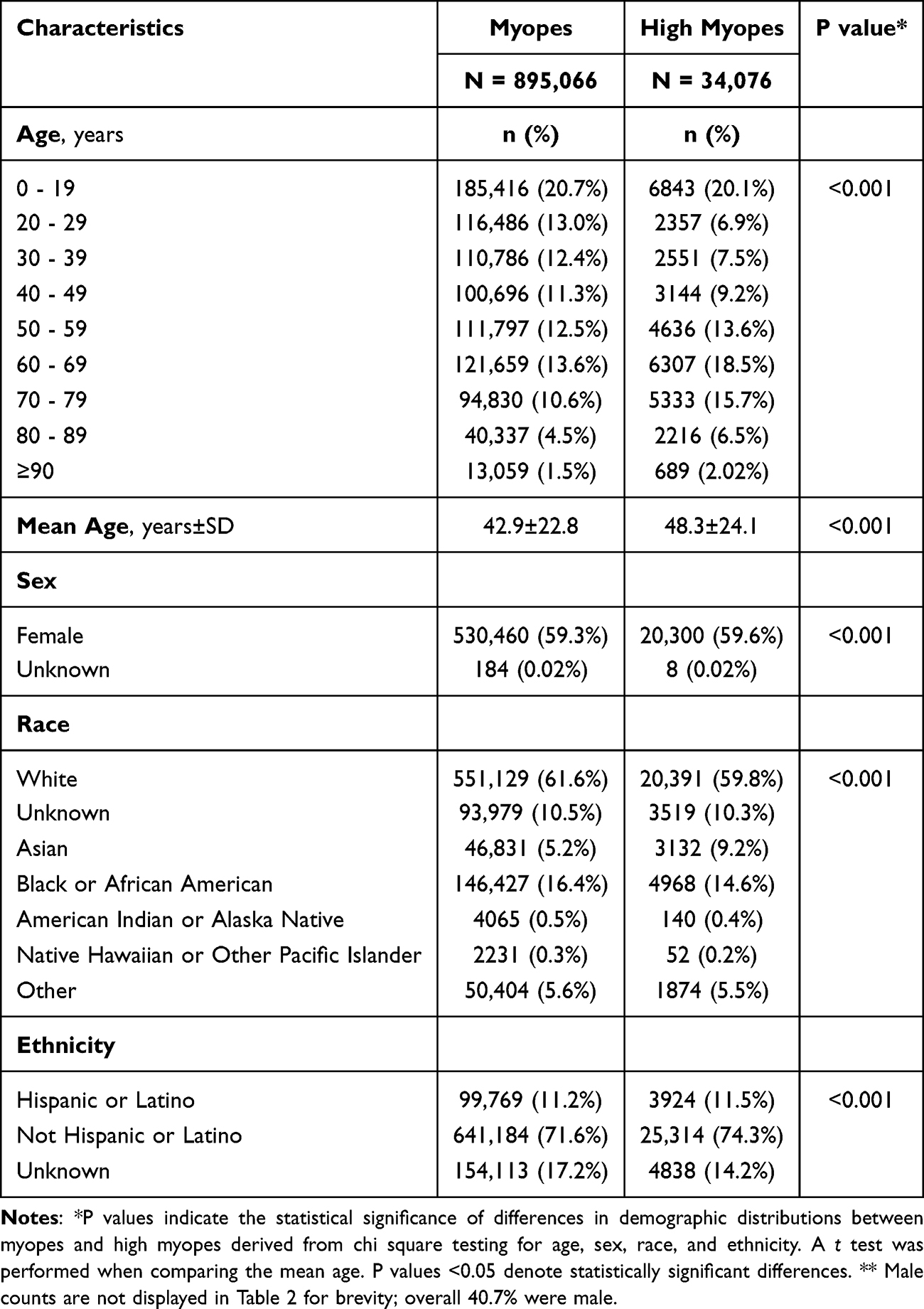 |
Table 2 Baseline Demographic Characteristics of Myopic Patients |
Table 3 illustrates the association between each of the retinal sequelae of myopia and POAG. The presence of any retinal sequelae significantly increased the risk of POAG (OR: 3.21, 95% CI: 3.02–3.41, 99% CI: 2.97–3.47; AOR: 1.75, 95% CI: 1.65–1.86, 99% CI: 1.61–1.90). FRD presented the highest odds among the specific sequelae (OR: 6.20, 95% CI: 3.83–10.03, 99% CI: 3.29–11.67), with odds remaining high after adjustment (AOR: 5.82, 95% CI: 3.44–9.85, 99% CI: 2.92–11.61). Foveoschisis also showed a substantial association with POAG, with an OR of 5.74 (95% CI: 3.51–9.39, 99% CI: 3.01–10.96) and an AOR of 3.10 (95% CI: 1.84–5.21, 99% CI: 1.57–6.13).
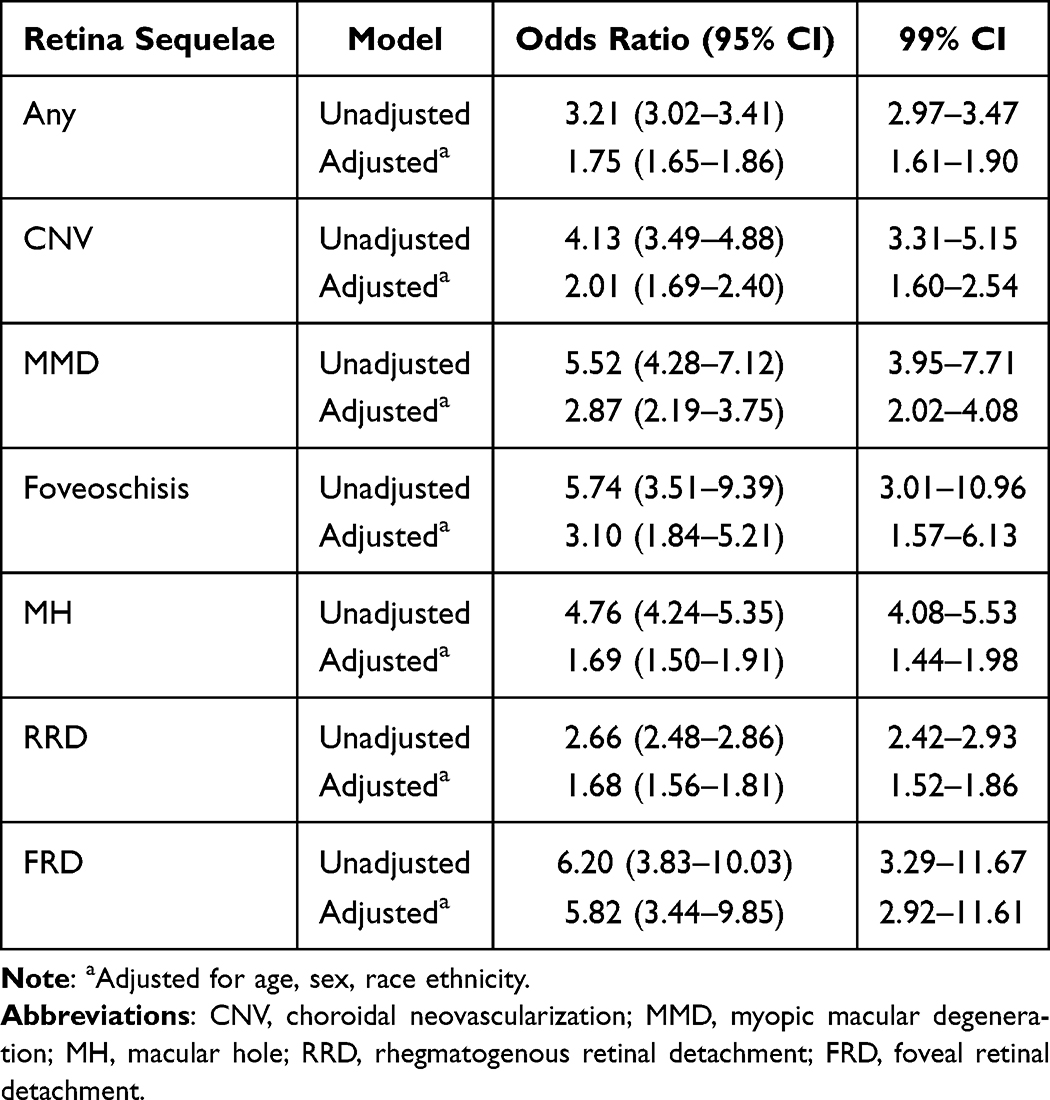 |
Table 3 Results of Logistical Regression, Demonstrating the Odds Ratio of Having a POAG Diagnosis in Those with Each Retinal Sequelae Compared to Those Without the Respective Sequelae |
Table 4 illustrates the association between each of the retinal sequelae of myopia and different severities of POAG. A significant association was observed between all retinal sequelae and each degree of POAG severity, with incrementally increasing ORs. FRD showed the most pronounced association with severe POAG (OR: 6.89, 95% CI: 2.94–16.13, 99% CI: 2.25–21.08), indicating a substantial risk increase with this sequela. Similarly, MMD showed high association with severe POAG (OR: 4.12, 95% CI: 2.71–6.28, 99% CI: 2.37–7.17).
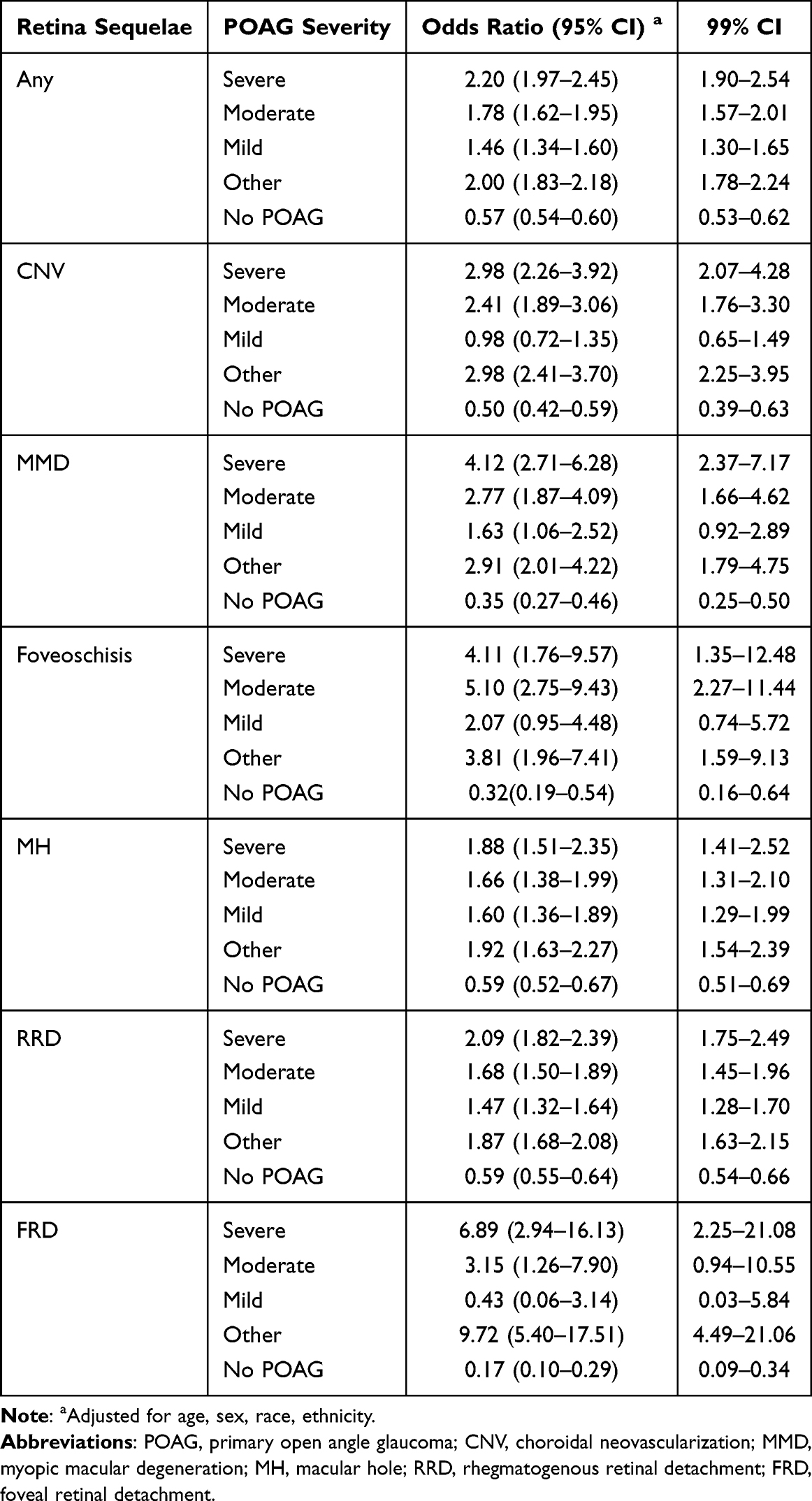 |
Table 4 Results of Logistical Regression, Demonstrating the Likelihood of Each Severity Subtype of POAG When Comparing Those with and without Each Retinal Sequela |
Figure 1 and Table 5 reveal the results from the Cox proportional hazards model. All results were significant except for FRD (p=0.8). Each of the remaining retinal sequelae was associated with an increased risk of progressing from glaucoma suspect to POAG. The strongest association was found among patients with foveoschisis (HR: 5.33, 95% CI: 2.21–12.85, p<0.005), followed by those with MMD (HR: 2.74; 95% CI: 1.47–5.10; p<0.005), CNV (HR: 1.73; 95% CI: 1.12–2.67; p=0.01), MH (HR:1.73; 95% CI: 1.29–2.31; p<0.005), and RRD (HR: 1.54; 95% CI: 1.28–1.86; p<0.005). Finally, Figure 2 visualizes all Kaplan-Meier curves, demonstrating how patients with each retinal sequela experienced a significantly faster progression from glaucoma suspect to POAG for all sequelae (log-rank p<0.05) except FRD.
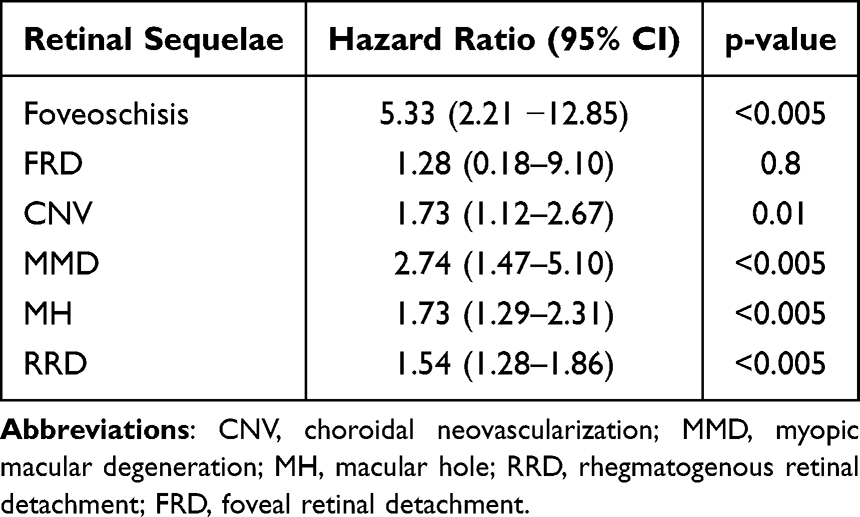 |
Table 5 Risk of Progression from Glaucoma Suspect to POAG for Each Retinal Sequelae |
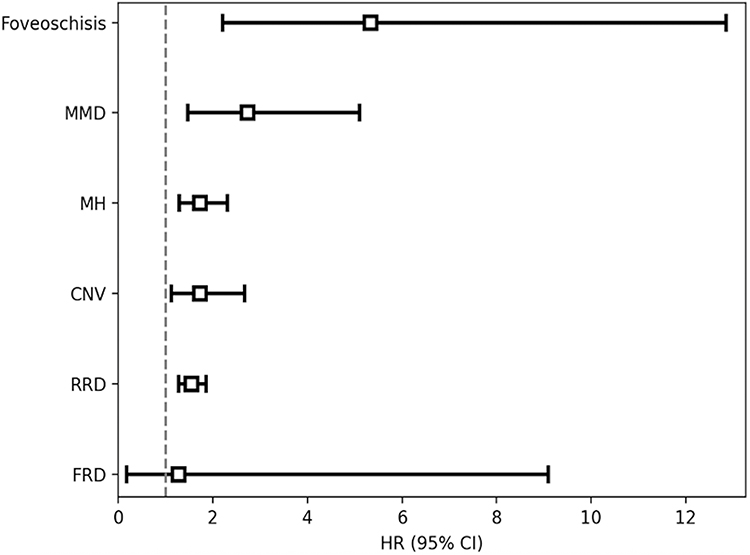 |
Figure 1 Risk of glaucoma progression by retina sequelae of myopia. Cox proportional hazards models of risk of progression from glaucoma suspect to POAG in myopes stratified by retina sequelae: choroidal neovascularization (CNV), myopic macular degeneration (MMD), foveoschisis, macular hole (MH), foveal retinal detachment (FRD), rhegmatogenous retinal detachment (RRD). All models adjusted for age, sex, race, ethnicity, and presence of pseudophakia. |
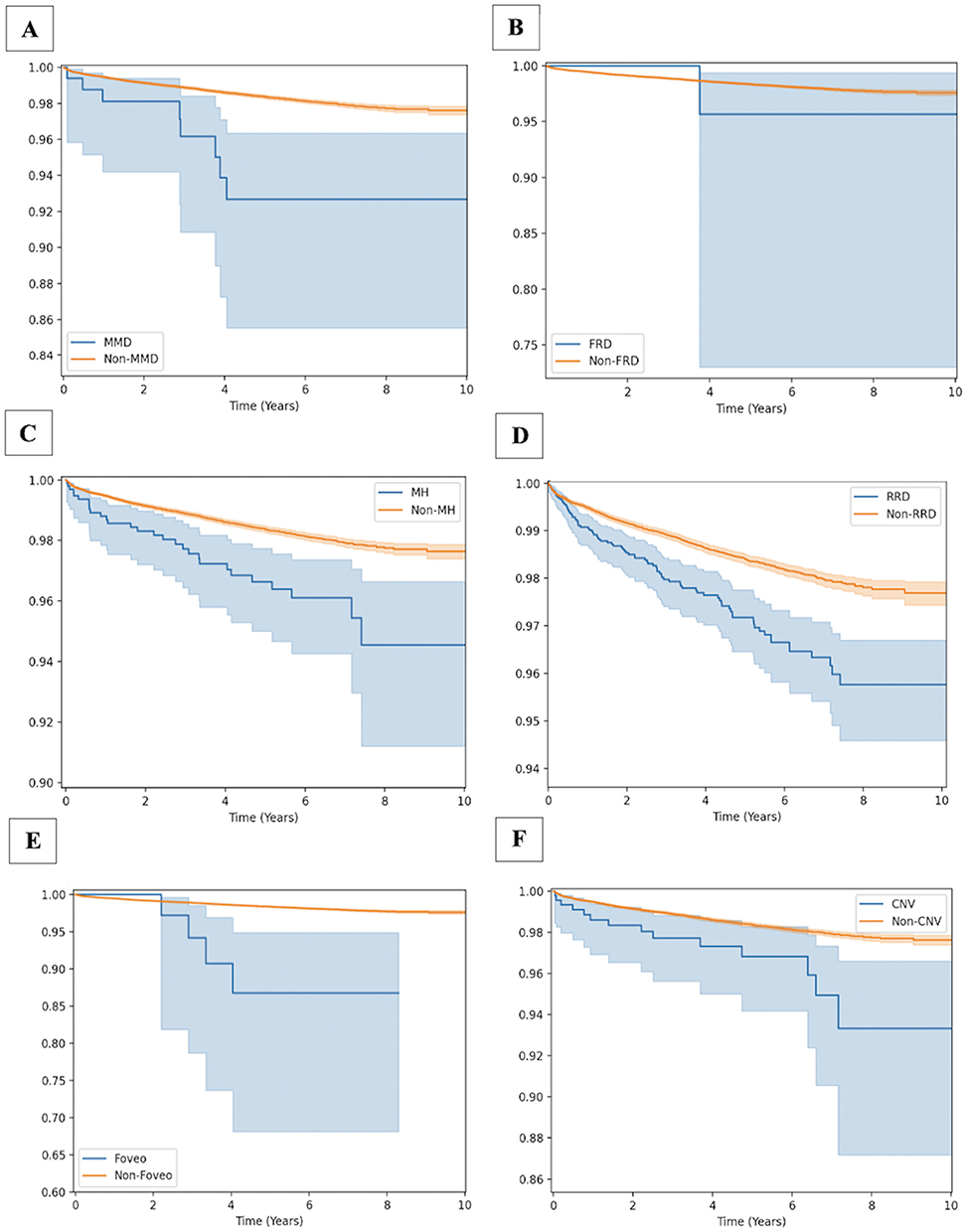 |
Figure 2 Survival curves showing time from diagnosis of borderline primary open-angle glaucoma (POAG) to diagnosis of severe POAG in myopes stratified by retina sequelae: myopic macular degeneration (MMD, A), foveal retinal detachment (FRD, B), macular hole (MH, C), rhegmatogenous retinal detachment (RRD, D), foveoschisis (E), and choroidal neovascularization (CNV, F). |
Discussion
Respectively, 4.8 billion and 111.8 million people are expected to be affected by myopia and glaucoma over the coming decades.1,4 The concurrently surging prevalence of these disorders and their ocular complications warrants a better understanding of their interrelationship. Our study suggests that the odds of POAG are markedly elevated in the presence of each retinal sequela of myopia, but especially among patients diagnosed with FRD. Furthermore, the different degrees of POAG severity were found to be linked to each myopic sequela as well.
The Retinal Sequelae of Myopia Increase the Likelihood of POAG
We found that all retinal sequelae analyzed in this study were associated with higher odds of developing POAG. Specifically, CNV, MMD, foveoschisis, MH, RRD, and FRD were shown to be associated with higher likelihood of developing POAG, with the severe and “Other” subtypes of POAG exhibiting the strongest association across each sequela. Additionally, aside from FRD, such patients were also found to be at higher risk of progressing from glaucoma suspect to POAG over time.
Previous studies have linked myopia with glaucoma. Mitchell et al, found that different degrees of myopia were associated with higher odds of open-angle glaucoma, noting that even low myopia increases one’s likelihood by 2.3-fold. Moderate-to-high myopia was associated with an even higher likelihood of open-angle glaucoma (OR=3.3).8 When pooling data from eleven cross-sectional studies, Marcus et al, furthered these findings in their meta-analysis, substantiating how higher degrees of myopia are associated with higher odds of open-angle glaucoma as well.9 Through their respective studies, Mitchell et al, and Marcus et al, underscore not only how myopia predisposes patients to open-angle glaucoma, but also the dose-dependent pattern of this predisposition. This suggests that the probability of developing open-angle glaucoma in myopic patients may directly correlate with one’s refractive error.
Similarly, each of the retinal sequelae in this study have also been independently linked with myopia. Pathologic myopia is characterized as the presence of high myopia and degenerative retinal changes, such as CNV, MMD, foveoschisis, MH, RRD, and FRD.10 In their retrospective study, Cohen et al, found that 62% of patients developed CNV due to high myopia.11 Additionally, Haarman et al, demonstrated that low, moderate, and high degrees of myopia were associated with 13.57-, 72.74-, and 845.08-times higher odds of developing MMD, respectively. They also demonstrated that such patients had a 3.15-, 8.74-, and 12.62-times higher likelihood of developing RRD as well, respectively.2 Meanwhile, Wu et al demonstrated that axial elongation in high myopia was associated with a 17.7 times higher odds of foveoschisis and foveal detachment.12 Lastly, the work of Singh et al, postulated that patients with macular holes on average have axial lengths that are 0.531 mm longer than control groups, establishing axial length as a risk factor for macular hole.13
Ultimately, by demonstrating that the retinal complications of myopia are associated with glaucoma, our findings support prior studies by indirectly correlating myopia with POAG. Thus, we can infer a similar relationship between these two ocular pathologies as previously documented.8,9,14,15 Furthermore, our findings expand on the understood relationship between these two ocular pathologies by demonstrating how specific subgroups of myopic patients with these retinal complications are predisposed towards POAG. Retinal sequelae of myopia were associated with an increased risk of POAG, and across each subclass of POAG, severe manifestations were the most likely to develop. Given that CNV, MMD, foveoschisis, MH, RRD, and FRD are characteristic of pathologic myopia, our results highlight how higher degrees of myopia are associated with a higher probability of POAG.2 This study pushes forward by providing additional clinical clues for physicians towards identifying high-risk demographics of myopic patients who are likely to develop POAG.
Pathophysiologic Explanations
Axial elongation is assumed to be implicated in both the retinal sequelae of myopia and POAG. For instance, axial elongation is thought to disproportionately upregulate angiogenic factors, leading to choroidal neovascularization, while also exerting tractional forces that lead to retinal tears and macular holes.16,17 The disruption of retinal blood flow autoregulation among patients with longer axial lengths has been proposed to play a role in the retina’s susceptibility to intraocular pressure changes.18 Thus, the vascular dysfunction observed in CNV may exacerbate the ischemic changes to the optic nerve in myopic eyes, predisposing them to glaucoma. Similarly, axial elongation also imposes mechanical stress along the posterior wall of the sclera, commonly forming posterior staphylomas. These scleral outpouchings distort the macula and encourage the separation of its retinal layers, contributing to foveoschisis, foveal retinal detachment, and macular degeneration.12 Such stretching may be associated with a decreased vessel density in the macula. This disruption of the macula’s vascular supply has been associated with longer axial lengths and increasing severities of glaucoma, highlighting how macular degenerative changes may contribute towards glaucoma risk by similarly inducing ischemia of the ganglion cells.19
RRD, FRD, and foveoschisis can be managed with vitrectomies, though such surgeries are also linked with the development of open-angle glaucoma as well.20,21 For example, chronic intraocular pressure elevations have been observed in 8% of cases following the use of silicone oil during pars plana vitrectomies.22 While some cases are attributed to secondary angle closure due to pupillary block, silicone oil can cause secondary open-angle glaucoma by overfilling the anterior chamber or through the emulsification of microdroplets into the trabecular network.22 Similarly, following a scleral buckle, the subsequent indentations to the orbit lead to a significant increase in the axial length, which can degenerate the lamina cribrosa.23 Additionally, though corticosteroids such as dexamethasone can mitigate inflammation and decrease risk of proliferative vitreoretinopathy following retinal surgeries, the administration of these medications is also linked with acute rises in intraocular pressures.24,25 Thus, the stretched deformations in high myopia contribute towards how these retinal complications may predispose patients to POAG.
Lastly, axial elongation is also directly associated with the development of POAG as well. The elongation of the globe in myopic eyes is thought to weaken the lamina cribrosa, predisposing the optic nerve head to biomechanical and barometric injury.26 Prior studies have demonstrated how such defects in the lamina cribrosa are strongly associated with POAG in patients with high myopia.27 Furthermore, the larger optic disc tilt angles and smaller ovality index that accompanies scleral stretching was also found to be associated with lamina cribrosa defects in these patients.27 Axial elongation is also associated with degenerative changes in the peripapillary region, a marker of progressive glaucomatous damage.28,29 It also weakens the retinal pigment epithelium layer and induces lacquer cracks within the Bruch’s membrane, compromising the delivery of nutrients from the choroid to the retina and furthering its susceptibility to glaucoma.30,31
Clinical Implications
Importantly, this study can provide significant insights for clinical judgment by ophthalmologists. The clinical features of high myopia can often resemble those of glaucoma, representing a diagnostic challenge that can lead to misdiagnoses of patients with normal-range intraocular pressures. For example, high myopia has been documented to reduce the biomechanical properties of the cornea.32 This can directly influence tonometry measurements in myopic patients suspected to also have glaucoma. Similarly, myopia and glaucoma are both associated with a thinning of the retinal nerve fiber layer (RNFL), which can lead to a misinterpretation of optical coherence tomography (OCT) reports.33,34 Myopic optic disc tilt is also associated with RNFL changes, which can be mistaken for glaucomatous defects on OCT imaging.35,36 Furthermore, the vision loss that accompanies glaucoma often occurs insidiously in its early stages, and because of its indolent progression, many patients are unaware of their visual deterioration until its later stages.37 In their population study, for example, Hennis et al, found that as many as 53% of patients with open-angle glaucoma were unaware of their diagnosis, leading to few eye care visits.38 Given its insidious progression, the early detection of glaucoma can substantially change its prognosis and visual outcomes. Pattern electrophysiology and OCT parameters derived from the Bruch’s membrane opening have shown promise in detecting early retinal ganglion cell dysfunction in the absence of detectable vision loss.39,40 Thus, building off the conclusions of our analysis, the detection of these retinal complications when examining myopic patients can further flag physicians towards considering a glaucoma diagnosis in their differential. This can potentially reshape referral patterns to glaucoma specialists and lead to improved outcomes in patients with POAG.
Strengths and Limitations
The strengths of our study include a large population of over 124 million patients across nine countries, including 60 healthcare organizations in the USA. Another point to consider is the study period from January 1, 2003, to April 10, 2024, which supports the currency and reliability of the dataset. However, our study also has its limitations. First, the retrospective design of our study implies an association between the retinal sequelae of myopia and glaucoma rather than establishing causality between the two. Despite the large population of our cohort, non-Hispanic white patients consisted of the majority of our population, which may also limit the generalizability of our results towards patients from underrepresented populations. Additionally, our reliance on electronic health record data and ICD codes may have subjected our analysis to misclassification bias, given the diversity of diagnostic and coding practices between institutions. For example, given the challenges associated with distinguishing the structural changes of glaucoma from those of myopia on ocular examination, certain diagnoses may have been misclassified. Our analysis also did not account for the presence of multiple sequelae in one patient, limiting our understanding of the individual contributions of each retinal disorder. Similarly, our analysis is weakened by a lack of clinical data, such as intraocular pressures, axial lengths, refractive errors, visual field tests, and imaging results, which limited our capacity to differentiate retinal and glaucoma diagnoses from true ocular pathologies. Lastly, patients with FRD represented the smallest proportion of patients with retinal sequelae. This may have influenced the directionality of our results, potentially accounting for why a significant relationship was not observed between FRD and glaucoma progression. Ultimately, future studies that address these issues may offer clearer insights. For instance, including a more diverse and proportional patient population and bolstering analysis with pertinent clinical measurements can expand the generalizability and accuracy of our findings.
Conclusion
In conclusion, retinal sequelae of myopia were associated with a greater likelihood of POAG. Not only were these retinal pathologies found to increase the odds of severe POAG, but they also elevated the risk of progressing from glaucoma suspect to a POAG diagnosis. These findings build off the established relationship between myopia and glaucoma by demonstrating a direct link between the retinal complications of myopia and glaucoma. Patients with myopia should be monitored for glaucoma, and the presence of these retinal sequelae should strongly raise suspicion for glaucoma and encourage ophthalmologists to refer their patients to glaucoma specialists. Given how indolently glaucoma progresses, this change in referral patterns can lead to early detection, preventing permanent blindness from glaucoma.
Data Sharing Statement
The data that support the findings of this study are available from the TriNetX registry. Restrictions apply to the availability of these data, which were used under license for this study. Data are available from the authors with the permission of TriNetX.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Eye Institute K23 Grant, K23EY035741, E. Matilda Ziegler Foundation for the Blind for Chase A. Ludwig, MD, MS, as well as the P30 Vision Research Core Grant, NEI P30-EY026877, Research to Prevent Blindness, Inc. for Karen M. Wai, MD; Eubee Koo, MD; Andrea L. Kossler, MD, FACS; Euna Koo, MD; Ehsan Rahimy, MD; Prithvi Mruthyunjaya, MD, MHS; and Chase A. Ludwig, MD, MS.
Disclosure
The authors report no relevant financial disclosures or proprietary interests in the materials described in the article.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
2. Haarman AEG, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49. doi:10.1167/iovs.61.4.49
3. Steinmetz JD, Bourne RRA, Briant PS. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the global burden of disease study. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/s2214-109x(20)30489-7
4. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
5. Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011;152(4):515–522. doi:10.1016/j.ajo.2011.06.004
6. Prior M, Francis JJ, Azuara-Blanco A, Anand N, Burr JM. Why do people present late with advanced glaucoma? A qualitative interview study. Br J Ophthalmol. 2013;97(12):1574–1578. doi:10.1136/bjophthalmol-2013-303813
7. Du R, Xie S, Igarashi-Yokoi T, et al. Continued increase of axial length and its risk factors in adults with high myopia. JAMA Ophthalmol. 2021;139(10):1096–1103. doi:10.1001/jamaophthalmol.2021.3303
8. Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: the blue mountains eye study. Ophthalmology. 1999;106(10):2010–2015. doi:10.1016/s0161-6420(99)90416-5
9. Marcus MW, de Vries MM, Junoy Montolio FG, Jansonius NM. Myopia as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. Ophthalmology. 2011;118(10):1989–1994.e2. doi:10.1016/j.ophtha.2011.03.012
10. Morgan IG, Ohno-Matsui K, Saw S-M. Myopia. Lancet. 2012;379(9827):1739–1748. doi:10.1016/S0140-6736(12)60272-4
11. Cohen SY, Laroche A, Leguen Y, Soubrane G, Coscas GJ. Etiology of choroidal neovascularization in young patients. Ophthalmology. 1996;103(8):1241–1244. doi:10.1016/s0161-6420(96)30515-0
12. Wu PC, Chen YJ, Chen YH, et al. Factors associated with foveoschisis and foveal detachment without macular hole in high myopia. Eye. 2009;23(2):356–361. doi:10.1038/sj.eye.6703038
13. Singh AJ, Muqit MM, Woon WH. Is axial length a risk factor for idiopathic macular hole formation? Int Ophthalmol. 2012;32(4):393–396. doi:10.1007/s10792-012-9568-7
14. Wu J, Hao J, Du Y, et al. The association between myopia and primary open-angle glaucoma: a systematic review and meta-analysis. Ophthalmic Res. 2022;65(4):387–397. doi:10.1159/000520468
15. Shim SH, Sung KR, Kim JM, et al. The prevalence of open-angle glaucoma by age in myopia: the Korea national health and nutrition examination survey. Curr Eye Res. 2017;42(1):65–71. doi:10.3109/02713683.2016.1151053
16. Seko Y, Seko Y, Fujikura H, Pang J, Tokoro T, Shimokawa H. Induction of vascular endothelial growth factor after application of mechanical stress to retinal pigment epithelium of the rat in vitro. Invest Ophthalmol Vis Sci. 1999;40(13):3287–3291.
17. Stirpe M, Michels RG. Retinal detachment in highly myopic eyes due to macular holes and epiretinal traction. Retina. 1990;10(2):113–114. doi:10.1097/00006982-199004000-00004
18. Juliano J, Burkemper B, Lee J, et al. Longer axial length potentiates relationship of intraocular pressure and peripapillary vessel density in glaucoma patients. Invest Ophthalmol Visual Sci. 2021;62(9):37. doi:10.1167/iovs.62.9.37
19. Rezapour J, Bowd C, Dohleman J, et al. Macula structural and vascular differences in glaucoma eyes with and without high axial myopia. Br J Ophthalmol. 2023;107(9):1286–1294. doi:10.1136/bjophthalmol-2021-320430
20. Wakatsuki Y, Nakashizuka H, Tanaka K, Mori R, Shimada H. Outcomes of vitrectomy with fovea-sparing and inverted ILM flap technique for myopic foveoschisis. J Clin Med. 2022;11(5):1274. doi:10.3390/jcm11051274
21. Sultan ZN, Agorogiannis EI, Iannetta D, Steel D, Sandinha T. Rhegmatogenous retinal detachment: a review of current practice in diagnosis and management. BMJ Open Ophthalmol. 2020;5(1):e000474. doi:10.1136/bmjophth-2020-000474
22. Barr CC, Lai MY, Lean JS, et al. Postoperative intraocular pressure abnormalities in the silicone study: silicone study report 4. Ophthalmology. 1993;100(11):1629–1635. doi:10.1016/S0161-6420(93)31425-9
23. Goezinne F, La Heij EC, Berendschot TT, et al. Anterior chamber depth is significantly decreased after scleral buckling surgery. Ophthalmology. 2010;117(1):79–85. doi:10.1016/j.ophtha.2009.06.052
24. Bonfiglio V, Reibaldi M, Macchi I, et al. Preoperative, intraoperative and postoperative corticosteroid use as an adjunctive treatment for rhegmatogenous retinal detachment. J Clin Med. 2020;9(5):1556. doi:10.3390/jcm9051556
25. Weinreb R, Polansky J, Kramer S, Baxter J. Acute effects of dexamethasone on intraocular pressure in glaucoma. Invest Ophthalmol Visual Sci. 1985;26(2):170–175.
26. Jonas JB, Wang YX, Dong L, Panda-Jonas S. High myopia and glaucoma-like optic neuropathy. Asia-Pac J Ophthalmol. 2020;9(3):234–238. doi:10.1097/APO.0000000000000288
27. Kimura Y, Akagi T, Hangai M, et al. Lamina cribrosa defects and optic disc morphology in primary open angle glaucoma with high myopia. PLoS One. 2014;9(12):e115313. doi:10.1371/journal.pone.0115313
28. Uchida H, Ugurlu S, Caprioli J. Increasing peripapillary atrophy is associated with progressive glaucoma. Ophthalmology. 1998;105(8):1541–1545. doi:10.1016/S0161-6420(98)98044-7
29. Kim M, Kim T-W, Weinreb RN, Lee EJ. Differentiation of parapapillary atrophy using spectral-domain optical coherence tomography. Ophthalmology. 2013;120(9):1790–1797. doi:10.1016/j.ophtha.2013.02.011
30. Dong L, Shi XH, Kang YK, et al. Bruch’s membrane thickness and retinal pigment epithelium cell density in experimental axial elongation. Sci Rep. 2019;9(1):6621. doi:10.1038/s41598-019-43212-8
31. Neelam K, Ng SM, Ho EL, Au eong K-G. Lacquer cracks in pathological myopia: a clinical review. Eye. 2024;38(15):2859–2873. doi:10.1038/s41433-024-03183-1
32. Wu W, Dou R, Wang Y. Comparison of corneal biomechanics between low and high myopic eyes—a meta-analysis. Am J Ophthalmol. 2019;207:419–425. doi:10.1016/j.ajo.2019.07.007
33. Leung CK-S, Mohamed S, Leung KS, et al. Retinal nerve fiber layer measurements in myopia: an optical coherence tomography study. Invest Ophthalmol Visual Sci. 2006;47(12):5171–5176. doi:10.1167/iovs.06-0545
34. Kanamori A, Nakamura M, Escano MF, Seya R, Maeda H, Negi A. Evaluation of the glaucomatous damage on retinal nerve fiber layer thickness measured by optical coherence tomography. Am J Ophthalmol. 2003;135(4):513–520. doi:10.1016/S0002-9394(02)02003-2
35. Shin H-Y, Park H-YL, Park CK. The effect of myopic optic disc tilt on measurement of spectral-domain optical coherence tomography parameters. Br J Ophthalmol. 2015;99(1):69–74. doi:10.1136/bjophthalmol-2014-305259
36. Lee JE, Sung KR, Park JM, et al. Optic disc and peripapillary retinal nerve fiber layer characteristics associated with glaucomatous optic disc in young myopia. Graefes Arch Clin Exp Ophthalmol. 2017;255(3):591–598. doi:10.1007/s00417-016-3542-4
37. Tatham AJ, Medeiros FA, Zangwill LM, Weinreb RN. Strategies to improve early diagnosis in glaucoma. Prog Brain Res. 2015;221:103–133.
38. Hennis A, Wu S-Y, Nemesure B, Honkanen R, Leske MC, Group BES. Awareness of incident open-angle glaucoma in a population study: the Barbados Eye Studies. Ophthalmology. 2007;114(10):1816–1821. doi:10.1016/j.ophtha.2007.06.013
39. Alhagaa AA, Mahmoud Badawi N, Abd Allah El-Morsy O. Primary open angle glaucoma diagnosis using pattern electroretinogram parameters. Clin Ophthalmol. 2023;Volume 17:3281–3293. doi:10.2147/OPTH.S424323
40. Gmeiner JM, Schrems WA, Mardin CY, Laemmer R, Kruse FE, Schrems-Hoesl LM. Comparison of Bruch’s membrane opening minimum rim width and peripapillary retinal nerve fiber layer thickness in early glaucoma assessment. Invest Ophthalmol Visual Sci. 2016;57(9):OCT575–OCT584. doi:10.1167/iovs.15-18906
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Considerations for Glaucoma Evaluation and Management in Refractive Surgery Candidates
Seresirikachorn K, Zhu AY, Chang TC
Clinical Ophthalmology 2025, 19:4941-4950
Published Date: 30 December 2025