Back to Journals » Clinical Ophthalmology » Volume 19
Considerations for Glaucoma Evaluation and Management in Refractive Surgery Candidates
Authors Seresirikachorn K, Zhu AY ![]() , Chang TC
, Chang TC ![]()
Received 30 September 2025
Accepted for publication 23 December 2025
Published 30 December 2025 Volume 2025:19 Pages 4941—4950
DOI https://doi.org/10.2147/OPTH.S571303
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kasem Seresirikachorn,1– 3 Angela Y Zhu,1 Ta Chen Chang1
1Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 2Department of Ophthalmology, College of Medicine, Rangsit University, Rajavithi Hospital, Bangkok, Thailand; 3Department of Ophthalmology, Queen Sirikit National Institute of Child Health, Bangkok, Thailand
Correspondence: Ta Chen Chang, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th Street, Miami, FL, 33136, USA, Email [email protected]
Abstract: The popularity of refractive surgery has grown significantly in recent years, yet concerns about its effects on glaucoma evaluation and progression remain unclear. Various techniques in both corneal and lens-based refractive surgery have been developed, necessitating different strategies for monitoring glaucoma. With the advent of advanced technologies and instruments, our ability to detect and monitor glaucoma in patients undergoing refractive surgery has improved. This review provides comprehensive information on glaucoma risk assessment and monitoring from preoperative to postoperative stages for different types of refractive surgery, highlighting key considerations at each stage of care. We aim to raise awareness and confidence among refractive surgeons handling cases involving glaucoma suspects or patients with glaucoma at any stage of refractive surgery. Based on updated evidence, we provide key recommendations that include conducting a comprehensive glaucoma risk assessment, ensuring vigilant monitoring of high-risk cases, and selecting the most suitable tonometer for precise intraocular pressure measurement.
Keywords: glaucoma, intraocular pressure, refractive surgery, keratorefractive surgery, myopia
Introduction
Refractive surgery has seen a steady rise in popularity since its introduction over 25 years ago.1–3 Myopia accounts for 80% of refractive diagnoses among patients undergoing Laser Vision Correction, followed by hyperopia at 15%.4 Laser-assisted in situ keratomileusis (LASIK) is the predominant procedure, making up 85% of all refractive surgeries.3 The relationship between refractive surgery and the risk of glaucoma remains controversial, yet every stage of refractive surgery, from initial screening to long-term management, can be linked to glaucoma. Preoperative identification of glaucoma suspects or high-risk patients can inform surgical decisions, while perioperative factors may impact intraocular pressure (IOP) and corneal biomechanics, affecting glaucoma monitoring. Additionally, patients undergoing these procedures are typically quite young, making these considerations necessary long-term. This review provides insights into the impact of refractive surgery on glaucoma diagnosis and management, from preoperative stages up until the postoperative follow-up period. It addresses both laser corneal-based refractive surgeries, including photorefractive keratectomy (PRK), LASIK, and keratorefractive lenticule extraction (KLEx), as well as intraocular lens-based refractive surgeries, such as phakic intraocular lens implantation (PIOL) and refractive lens exchange (RLE).
Preoperative Considerations
A pre-existing glaucoma diagnosis is a relative contraindication for elective refractive surgery due to several factors,5 including challenges in accurately IOP, the potential for perioperative optic nerve damage secondary to acute IOP spikes during suction application, and challenges in tonometry associated with altered corneal biomechanics.
Clinical History & Exam
Several baseline factors that increase the risk of glaucoma, including age, family history, and comorbidities, should be reviewed. Key areas of focus include:
Type and Magnitude of Refractive Error
Most refractive surgery cases involve myopia, a known risk factor for all types of open-angle glaucoma.6,7 While all degrees of myopia are associated with an increased risk of glaucoma, the risk is particularly high in cases of severe myopia.7 A recent study has identified longer axial length as a significant risk factor for developing steroid-induced ocular hypertension following intravitreal dexamethasone injections.8 Additionally, high myopia, especially pathologic myopia with staphyloma, has been linked to greater optic nerve head deformation following acute IOP elevation.9 Therefore, special monitoring and evaluation are essential for patients with high myopia.
Pigment Dispersion Syndrome (PDS)
Pigment dispersion syndrome occurs when there is excessive pigment release from the iris, thought to be due to friction between the iris posterior pigmented epithelium and anterior zonules or lens. As the increased pigmentary dispersion can accumulate in the trabecular meshwork and reduce outflow, PDS is a risk factor for pigmentary glaucoma. This condition is usually asymptomatic and commonly seen in men under 40 years of age with myopia.10 Screening for this group of patients requires a careful evaluation, with slit lamp examination for the presence of Krukenberg spindles and performing gonioscopy. One single-site observational study has reported the prevalence of PDS in refractive surgery candidates to be about 26%.11 In PDS patients undergoing PRK, one study reported about 11% of patients to be steroid responders who required a single topical anti-glaucoma agent until completing the course of steroids.12
Angle Abnormalities
Several common conditions can be observed during gonioscopy, particularly in younger patients. These include angle recession, which is identified by a widening of the ciliary body band, often as a result of trauma; plateau iris, characterized by the “double hump” sign on indentation gonioscopy due to anteriorly positioned ciliary processes that push the peripheral iris forward; various primary or secondary angle closure conditions; and Axenfeld-Rieger phenotype, which may present with a prominent Schwalbe line, iris strands attached to the Schwalbe line, anterior insertion of the iris, and the presence of iris processes. Each of these findings may be asymptomatic and requires careful evaluation to assess the risk of glaucoma development or progression. If any of these abnormalities are noted, a baseline evaluation by a glaucoma specialist may be necessary.
Fundus Examination
Fundus examination is necessary to identify cases of pathologic myopia and staphyloma, as these conditions pose a higher risk for glaucoma development. Baseline evaluation of the optic disc is also critical. Differentiating between myopic discs and glaucomatous optic nerve head appearances can be challenging. For high-risk cases, it is recommended to obtain baseline disc photographs and monitor serially using the same camera to rule out changes over time, as written documentation alone may not be sufficient.
IOP Evaluation
For all patients requiring refractive surgery, documenting a baseline IOP is essential, with Goldmann applanation tonometry (GAT) being the consensus gold standard. Having multiple preoperative IOP measurements, preferably on different dates, helps establish a baseline range for future follow-up, especially if glaucoma-related concerns arise. Following any corneal laser-ablative refractive procedures, GAT often underestimates IOP.13 Therefore, for baseline documentation, measuring IOP concurrently using GAT and other instruments less affected by refractive surgery is recommended, especially in high-risk eyes. These instruments include dynamic contour tonometry (DCT), the ocular response analyzer (ORA), and corneal visualization Scheimpflug technology.
When using portable devices, it is advised that measurements be obtained from both the central cornea and peripheral cornea outside of the refractive surgery treatment zone. The location of the cornea where the measurement is taken can impact the results. It is important to document the specific location of the measurements to ensure comparability after refractive surgery.
Another consideration is the central corneal thickness (CCT), which may cause IOP to be over- or underestimated. Recording CCT along with baseline IOP before refractive surgery is essential, as postoperative measurements may differ. This information helps assess glaucoma risk and adjust the target IOP if glaucoma treatment becomes necessary.
Ancillary Glaucoma Testing
Currently, imaging and perimetry play major roles in diagnosing and detecting the progression of glaucoma, especially in high-risk cases where clinical evaluation alone is insufficient. A multimodal approach combining structural and functional assessments is recommended for detecting and monitoring glaucoma.14 Baseline preoperative optic disc imaging would allow future comparisons and adjudicate whether the optic disc has changed sufficiently to warrant a glaucoma diagnosis and subsequent treatment postoperatively. Ideally, the same instruments should be used before and after refractive surgery to ensure consistency.
While keratorefractive surgery may alter the cornea and IOP measurements, the optic disc structural and functional assessments should remain unchanged post-surgery. Optical coherence tomography is a valuable tool for assessing the peripapillary retinal nerve fiber layer (RNFL) and the macular ganglion cell-inner plexiform layer (GCIPL), both of which should remain unaffected by refractive surgery.15,16 All patients with confirmed or suspected glaucoma should have OCT data collected preoperatively to serve as a reference for post-surgical surveillance. Myopia can cause RNFL thinning and artifacts that may suggest glaucoma. Any progressive changes following surgery should raise concern for the possibility of an active glaucoma process.
Perimetry is crucial for all patients, as nearly 80% of individuals with myopia and suspected glaucomatous optic neuropathy, despite not having confirmed glaucoma, exhibit various types of visual field (VF) defects.17 Documenting a baseline VF before surgery can be very valuable for future monitoring.
An alternative tool for evaluating glaucoma risk is the novel, free, desktop-based glaucoma calculator. This tool combines age, IOP, and central corneal thickness (CCT) into a composite score,18,19 providing an optional method for preoperative and postoperative risk stratification in refractive surgery patients.
Intraoperative Considerations for Laser Ablative Procedures
Experimental and clinical studies have reported that LASIK patients experience IOP increases of 100 mmHg or more during the application of suction.20 A previous study by Shyam et al monitored IOP in rabbit eyes during LASIK and found that IOP increased to 81.78 mmHg during globe suction and 62.25 mmHg during femtosecond laser cutting. In the group using a microkeratome, IOP increased even more.21
Newer technologies, such as the WaveLight FS200 FS laser platform (Alcon Laboratories Inc., Fort Worth, TX, USA), have demonstrated reduced IOP elevations, with increases of 32.33 mmHg and 38.22 mmHg above baseline during the suctioning and cutting phases, respectively.22 In contrast, KLEx procedures have less effect on IOP spikes during surgery.23 PRK also reports less IOP rise and fluctuation during surgery; however, due to the often increased duration of topical steroids post-surgery compared to LASIK and KLEx, there may be a higher risk of steroid-induced ocular hypertension.
Concerns have been raised about the effects of increased IOP on structural and functional changes in the eye. Most studies suggest that keratorefractive surgeries have minimal effects on optic disc structural changes. Some recent studies indicate that femtosecond LASIK does not alter macular measurements, such as peripapillary RNFL, retinal ganglion cell thickness, and central macular thickness (MT), as measured by spectral domain OCT.24 Similarly, studies on KLEx technology report no changes in MT, RNFL, choroidal thickness, macular vessel density, and peripapillary vessel density, as measured by Cirrus HD OCT 5000 (Carl Zeiss Meditec, Inc., Dublin, CA, USA).25
However, some reports indicate that femtosecond LASIK may induce microvascular changes in the optic nerve head, potentially leading to non-arteritic anterior ischemic optic neuropathy.26 Cases of optic neuropathy following LASIK have been reported, but they are considered rare. The optic nerve damage induced by LASIK could be ischemic, resulting from a temporary disruption of blood flow in the central retinal artery and short posterior ciliary arteries when the IOP exceeds the arterial perfusion pressure.26,27 Based on this evidence and theoretical considerations, KLEx or PRK may pose the least long-term risk for patients at high risk of developing glaucoma. However, further studies are needed to substantiate the potential benefits of KLEx.
Anterior chamber parameters, including anterior chamber depth (ACD), angle, and volume (ACV), may appear to change after femtosecond LASIK and KLEx in patients with myopia or hyperopia. However, these changes are likely attributable to a corneal magnification effect rather than actual anatomical alterations.25,28 A case report of bilateral acute angle-closure glaucoma following hyperopic LASIK emphasizes the need for thorough preoperative assessment. Prophylactic laser iridotomy may be required for patients with narrow angles if refractive laser surgery is being considered.29
Postoperative Considerations After Laser Ablative Procedures
Corneal Biomechanics
The effects of refractive surgery extend beyond central corneal thickness to include alterations in the biomechanical properties of the cornea. These changes influence post-operative IOP measurements, necessitating different methods and strategies for at-risk patients. Previous reports indicate that ablative procedures cause corneal thinning, which decreases mechanical stiffness and increases sensitivity to IOP variations.30 Central corneal thickness has a minor effect on post-LASIK IOP, suggesting that corneal biomechanics may have a greater impact on IOP measurement.31
Preoperative central corneal thickness (CCT) and flap thickness are key predictors of postoperative IOP after femtosecond LASIK. Some studies suggest that KLEx causes fewer biomechanical changes postoperatively compared to LASIK.32
Post-refractive surgery, measuring IOP can be challenging, as changes in corneal biomechanical properties may compromise the accuracy of these measurements. Refractive surgeons might consider procedures like KLEx or femtosecond LASIK, which have a lesser impact on corneal biomechanics compared to other ablative techniques, such as PRK or microkeratome LASIK, particularly for patients at high risk of glaucoma.
IOP Measurement
Most studies indicate that IOP is generally measured lower after corneal refractive surgery compared to preoperative levels.13,33 The reduction in IOP is more pronounced following myopic procedures than hyperopic ones, likely due to the combined effect of central corneal tissue removal along with peripheral corneal ablation in myopic corrections, compared to the impact of only peripheral corneal tissue ablation in hyperopic corrections.34 Regardless of the type of refractive error being corrected, the creation of a lamellar flap in LASIK alone was associated with a decrease in IOP of approximately 0.94 mmHg compared to patients undergoing PRK.34 Given this evidence, we recommend conducting a series of IOP measurements both before and after surgery, particularly for high-risk patients to firmly correlate the pre- and post-operative baseline IOP levels. In high-risk glaucoma patients, prolonged steroid use or periods of IOP elevation following refractive surgery should be closely monitored, with regular IOP measurements until levels return to normal and remain stable If IOP remains uncontrolled or clinical signs of glaucoma are detected, referral to a glaucoma specialist with detailed clinical data is strongly recommended.
Numerous established methods and devices are available for clinical IOP measurement. Several techniques have been proposed as potentially superior for post-refractive surgery cases; however, no gold standard has been identified to date. Each method has its own advantages and limitations, which are outlined below and summarized in Table 1.
- Goldmann applanation tonometry (GAT): While GAT is the gold standard for measuring IOP preoperatively, most studies report that it often underestimates true IOP following refractive surgery.33,35,36 This discrepancy is influenced not only by changes in CCT, but also by alterations in corneal biomechanics. Postoperative IOP measurements corrected for CCT are often unreliable. Various techniques have been developed to enhance the accuracy of GAT, including the Corrective Applanation Tonometer Surface (CATS) and the new Goldman Convex Prism.35,37 However, these methods still lack precision and require further evaluation to confirm their accuracy. We do not recommend relying solely on GAT for monitoring postoperative IOP.
- Rebound tonometry (RT): Some evidence suggests that the iCare IC100 (Icare Finland Oy, Vantaa, Finland) is more reliable compared to GAT for measuring IOP following myopic LASIK and PRK procedures.33,36 Additionally, the iCare Home (Icare HOME tonometer; TIOLATOY, Cor., Finland) has proven to be a reliable method for IOP measurement after implantable collamer lens implantation.38 This machine offers an alternative option for postoperative IOP measurement and is user-friendly.
- Ocular response analyzer (ORA): Most reports suggest that this method (ORA, Reichert, USA) is more reliable than GAT because it is less influenced by CCT.33 The ORA offers the advantage of measuring corneal biomechanical properties, including corneal hysteresis (CH) and corneal resistance factor (CRF). Lower CH values are linked to faster glaucoma progression and greater visual field loss,39 making CH a strong predictor beyond central corneal thickness or IOP. LASIK generally causes greater reductions than KLEx,40 underscoring the need for careful postoperative monitoring. Consequently, it may be a viable alternative for patients who have undergone refractive surgery.
- Dynamic contour tonometry (DCT): Previous studies have shown that this method (DCT, Pascale, Switzerland) is more reliable for measuring IOP after PRK, LASIK, and photorefractive keratectomy compared to GAT.33,41–43 Based on previous studies, this technique is recommended for measuring IOP after refractive surgery. However, its routine use in post-refractive care may be limited due to restricted office availability.
- New generation noncontact tonometer: The new generation of noncontact tonometer, Corvis ST (CVS, Oculus, Germany), which measures biomechanically corrected IOP, has been reported to show the smallest changes between preoperative and postoperative IOP measurements compared to other tonometers following refractive surgery.37,44–46 This new noncontact tonometer is a good choice for patients who have undergone refractive surgery.
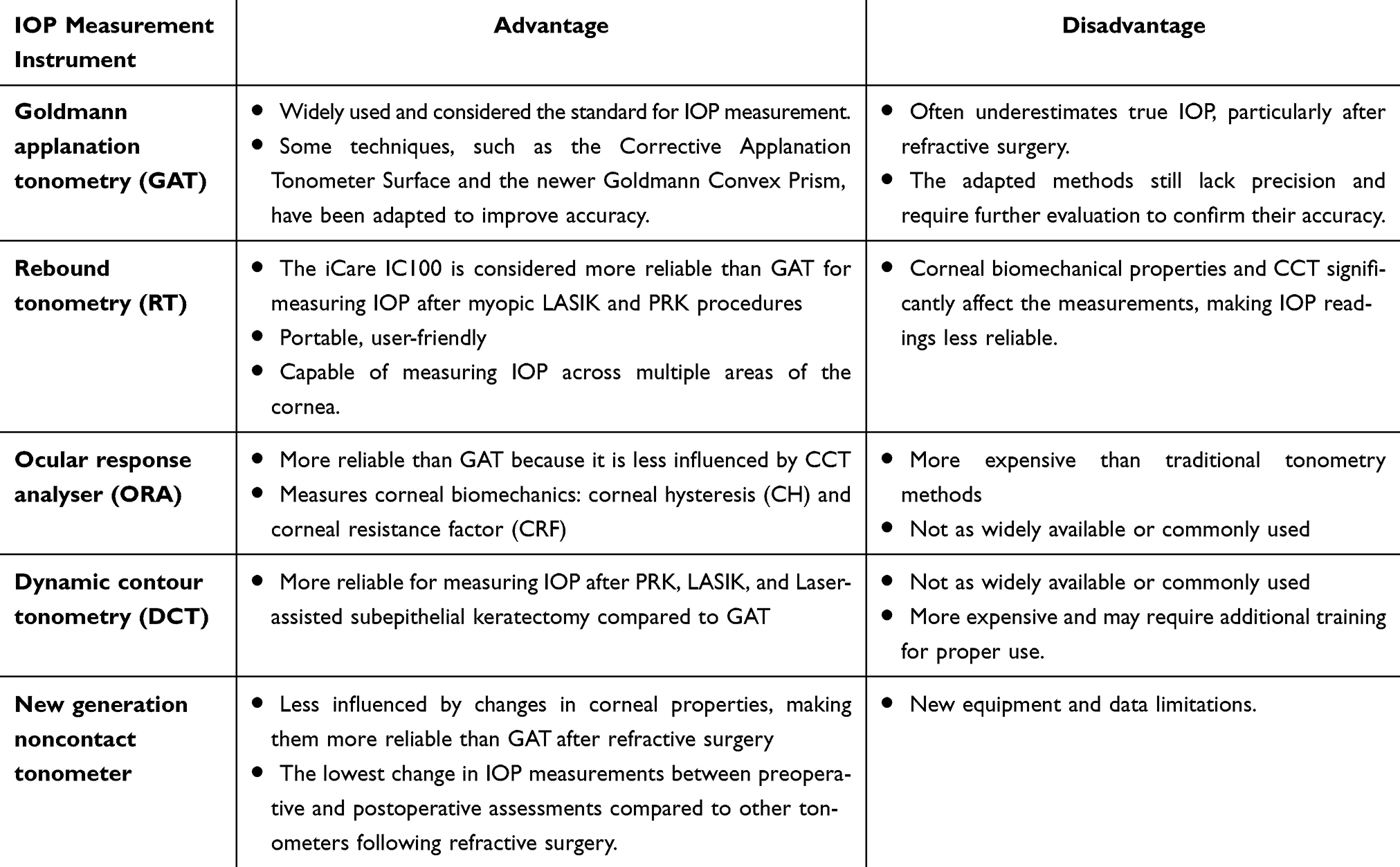 |
Table 1 Advantages and Disadvantages of Various IOP Measurement Instruments |
Structural and Functional Monitoring
It is crucial to understand that after corneal ablative refractive surgery, the structural and functional aspects of the eye remain mostly unchanged, except for the cornea. A markedly high or low axial length accompanying the preoperative myopia or hyperopia is not altered despite improved refractive error, and the long-term risks of associated ocular comorbidities, such as retinal detachment and glaucoma, are similarly unchanged. It is essential to inform patients about these underlying risks based on their refractive status.
Parameters such as disc appearance, RNFL thickness, ganglion cell analysis, and VF appearance should remain stable after surgery, as reported by numerous studies.25,47 Structural and functional assessments are particularly important for high-risk patients due to potentially unreliable IOP readings post-surgery. The frequency of monitoring should be determined based on the patient’s risk level and the likelihood of developing glaucoma. For high-risk patients, prompt referral to a glaucoma specialist may be beneficial.
Postoperative Glaucoma Complications After Laser Ablative Procedures
Interface Fluid Syndrome (IFS)
Also known as pressure-induced stromal keratitis (PISK) and pressure-induced interface keratitis (PIRK), IFS can occur at any time postoperatively, with the longest reported case being 16 years after surgery.48–50 It can affect any type of corneal-ablative refractive surgery that involves the creation of a corneal interface, including KLEx.51 This condition arises due to two main factors: increased IOP triggered by postoperative steroid use and corneal endothelial dysfunction. The elevated IOP causes fluid to shift from areas of high pressure through the endothelium to areas of lower pressure, such as the interface space in post-surgical patients.
Typically, patients with IFS present with prolonged steroid use, elevated IOP, and corneal edema. It is crucial to note that IOP readings from GAT may be falsely low due to the compressibility of the fluid-filled interface.52 Therefore, if IFS is suspected, it is recommended to measure IOP at the peripheral cornea using a different tonometer. Anterior segment OCT can be valuable in detecting fluid accumulation in the interface and monitoring the clinical course.
The primary differential diagnosis for IFS is often diffuse lamellar keratitis (DLK), a rare, non-infectious complication of refractive surgery that generally occurs during the early postoperative period. DLK is characterized by inflammatory infiltrates beneath the corneal flap interface.53 Patients with DLK typically present within one week after surgery with symptoms such as photophobia and blurry vision, often having normal IOP. Due to its inflammatory nature, DLK generally responds well to corticosteroid therapy, in contrast to IFS, where corticosteroids are often a triggering factor.
Treatment for IFS involves immediate cessation of steroids and lowering IOP. Previous reports indicate that 33.3% of IFS patients required glaucoma surgery. Over 50% of patients see resolution within one month and achieve a final corrected distance visual acuity of 20/25 or better. Patients with a history of corneal endothelial dysfunction have an 18-fold increased risk of needing surgical intervention.54
Steroid-Induced Ocular Hypertension
Postoperative refractive surgery regimens generally require the use of steroids, often aggressively, especially post-PRK. Reports indicate that 40% of eyes undergoing PRK develop ocular hypertension (OHT) within 12 weeks postoperatively.55 Treatment for this condition includes topical and systemic anti-glaucoma agents to lower IOP. Prompt discontinuation or minimization of steroid therapy is essential and should be initiated as early as possible.56,57 It is recommended to closely monitor IOP in PRK patients, with measurements taken within 1–2 weeks after surgery.
For other refractive surgeries, such as LASIK and KLEx, topical steroids are generally used for shorter durations, but IOP still needs to be monitored. However, the risk of IFS should be considered, particularly in cases of prolonged steroid use.
Glaucoma Progression
There is no strong evidence to suggest that refractive surgery is a risk factor for glaucoma or glaucoma progression. Previous studies have indicated that glaucoma progression in newly diagnosed patients with a history of refractive surgery is not significantly different from those without such a history.58 However, if glaucoma is suspected at any stage of the surgical process, prompt referral to a glaucoma specialist is recommended.
Considerations for Intraocular Refractive Surgery
Intraocular refractive surgery can be categorized into refractive lens exchange and phakic intraocular lens (IOL) implants. Refractive lens exchange carries surgical risks similar to elective cataract surgery, while phakic IOLs present higher associated risks. Phakic IOLs are further divided into anterior chamber and posterior chamber types. Currently, phakic IOLs are primarily indicated for correcting high myopia. All cases require an adequate anterior chamber depth, and a peripheral iridotomy (PI)6 is necessary to prevent pupillary block glaucoma before or during phakic IOL surgery, except when using newer generation phakic IOLs, such as the EVO ICL (Staar Surgical, Monrovia, CA). Preoperative evaluation for intraocular refractive surgery closely resembles that of cornea-based procedures. However, certain conditions warrant special attention. For instance, small eyes carry a higher risk of ciliary block glaucoma, and nanophthalmic eyes are prone to uveal effusion, which may necessitate posterior sclerotomies during surgery. Postoperative IOP measurement is generally more straightforward, as intraocular refractive surgery does not alter corneal biomechanics.
Anterior Chamber Phakic IOL
In anterior chamber phakic IOL procedures, only 1.6% of 1140 eyes experienced IOP > 30 mmHg, most of which occurred one day postoperatively and did not persist beyond 20 days. Most cases were attributed to retained viscoelastic material and/or a steroid response. One eye, in which a peripheral iridotomy was not performed, developed a pupillary block.59 A long-term study on anterior chamber phakic IOL demonstrated that mean IOP remained stable over 10 years.60 Although earlier reports noted occasional cases of IOP elevation, no instances of visual field loss or optic nerve damage were observed.61
Posterior Chamber Phakic IOL
The posterior chamber phakic IOL or implantable collamer lens is positioned in the posterior chamber and can lift the iris into the anterior chamber, which may reduce the anterior chamber angle, affecting the flow of aqueous humor.62 An improperly sized phakic IOL that results in a high vault is associated with a narrow anterior chamber angle. Preoperative screening should include assessing the anterior chamber angle (at least Shaffer grade 3 or 4) and anterior chamber depth, along with selecting the appropriate size of the phakic IOL. A study by Lingling in 2019 found no increase in IOP in cases with shallow anterior chambers (ACD < 2.8 mm) before surgery.63 Previous studies have published reliable algorithms using anterior segment metrics to predict postoperative anterior chamber angles (ACAs) for ICL surgery.64 This approach helps prevent overlooked risks of ACA narrowing, enhancing surgical accuracy and safety, but long-term safety and stability still require further investigation.
The increase in IOP after ICL procedures ranges from 0.8% to 26.2%.65 An early transient rise in postoperative IOP is now believed to be more related to steroid use or retained viscoelastic than to the surgery itself and usually resolves with temporary topical medication.66,67 However, some cases report long-term increases in IOP caused by pupillary block despite the presence of a patent PI, as well as pigment dispersion from iris chafing by the IOL.68,69 These complications may require additional iridectomies, glaucoma surgery, and lens explantation.68,70,71 To decrease the risk of these potential issues, adequate iridotomies should be performed, and excessive ICL vault should be avoided (usually by preventing overestimation of the ICL size). Recent studies on new-generation posterior chamber phakic IOLs with a central port, such as the EVO/EVO+ ICL (Staar Surgical, Monrollia, CA), have shown promising results, with no significant increase in IOP and no new cases of glaucoma in a study of 225 eyes.72 Postoperative monitoring should include IOP measurement, gonioscopy, and anterior segment evaluation to detect and manage any complications.
Conclusions
A thorough preoperative evaluation is essential when considering refractive surgery in patients at risk for glaucoma. This includes a detailed history, comprehensive ophthalmic examination, and gonioscopy to identify high-risk individuals and guide the selection of the most appropriate surgical approach. Baseline IOP measurements, along with both anatomical and functional assessments, are crucial in patients suspected of having glaucoma. While intraoperative IOP spikes are unlikely to cause significant structural or functional damage, postoperative IOP measurement may be complicated by changes in central corneal thickness and corneal biomechanics in laser ablative procedures. In these cases, alternative tonometry methods are recommended over GAT. Surgeons should also be aware of potential glaucoma-related post-refractive surgery complications such as IFS and steroid-induced ocular hypertension. Close monitoring of IOP and potential complications is essential, and prompt referral to a glaucoma specialist is advised if glaucoma is suspected at any stage of the surgical process.
Funding
The project was supported by NIH Center Core Grant P30EY014801, Research to Prevent Blindness- Unrestricted Grant (GR004596-1), and the 2024 American Glaucoma Society Mid-Career Physician Scientist Award Grant. Its contents are solely the authors’ responsibility and do not necessarily represent the official views of the NIH.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
References
1. Council TRS. RSC reports 32% YTD increase in LVC procedure volume over 2020. RSD. Available from: https://americanrefractivesurgerycouncil.org/press-room/refractive-surgery-council-reports-32-ytd-increase-in-laser-vision-correction-procedure-volume-over-2020/.
2. Lee Y, Kim JS, Park UC, Lim J, Garza León M. Recent trends of refractive surgery rate and detailed analysis of subjects with refractive surgery: the 2008-2015 Korean national health and nutrition examination survey. PLoS One. 2021;16(12):e0261347. doi:10.1371/journal.pone.0261347
3. Joffe SN. The 25th Anniversary of laser vision correction in the United States. Clin Ophthalmol. 2021;15:1163–1172. doi:10.2147/OPTH.S299752
4. Jones C. Refractive surgery market report. MarketScope. 2020;1–283.
5. Jacobs DS, Lee JK, Shen TT, et al. Refractive surgery preferred practice pattern. Ophthalmology. 2023;130(3):PP61–p135. doi:10.1016/j.ophtha.2022.10.032
6. Xu L, Wang Y, Wang S, Wang Y, Jonas JB. High myopia and glaucoma susceptibility the Beijing Eye Study. Ophthalmology. 2007;114(2):216–220. doi:10.1016/j.ophtha.2006.06.050
7. Shen L, Melles RB, Metlapally R, et al. The association of refractive error with glaucoma in a multiethnic population. Ophthalmology. 2016;123(1):92–101. doi:10.1016/j.ophtha.2015.07.002
8. Choi W, Kim JD, Bae HW, Kim CY, Seong GJ, Kim M. Axial length as a risk factor for steroid-induced ocular hypertension. Yonsei Med J. 2022;63(9):850–855. doi:10.3349/ymj.2022.63.9.850
9. Chuangsuwanich T, Tun TA, Braeu FA, et al. How myopia and glaucoma influence the biomechanical susceptibility of the optic nerve head. Invest Ophthalmol Vis Sci. 2023;64(11):12. doi:10.1167/iovs.64.11.12
10. Farrar SM, Shields MB, Miller KN, Stoup CM. Risk factors for the development and severity of glaucoma in the pigment dispersion syndrome. Am J Ophthalmol. 1989;108(3):223–229. doi:10.1016/0002-9394(89)90110-4
11. Doane JF, Rickstrew JJ, Tuckfield JQ, Cauble JE. Prevalence of pigment dispersion syndrome in patients seeking refractive surgery. J Glaucoma. 2019;28(5):423–426. doi:10.1097/IJG.0000000000001193
12. Bower KS, Sia RK, Ryan DS, et al. Visual and IOP outcomes after PRK in pigment dispersion syndrome. J Refract Surg. 2011;27(9):686–690. doi:10.3928/1081597X-20110324-01
13. Fan Q, Zhang J, Zheng L, Feng H, Wang H. Intraocular pressure change after myopic laser in situ keratomileusis as measured on the central and peripheral cornea. Clin Exp Optom. 2012;95(4):421–426. doi:10.1111/j.1444-0938.2011.00703.x
14. Shan M, Dong Y, Chen J, Su Q, Wang Y. Global tendency and frontiers of research on myopia from 1900 to 2020: a bibliometrics analysis. Front Public Health. 2022;10:846601.
15. Zivkovic M, Jaksic V, Giarmoukakis A, et al. The effect of LASIK procedure on peripapillary retinal nerve fiber layer and macular ganglion cell-inner plexiform layer thickness in myopic eyes. Biomed Res Int. 2017;2017:8923819. doi:10.1155/2017/8923819
16. Katsanos A, Arranz-Marquez E, Cañones R, Lauzirika G, Rodríguez-Perez I, Teus MA. Retinal nerve fiber layer thickness after laser-assisted subepithelial keratomileusis and femtosecond LASIK: a prospective observational cohort study. Clin Ophthalmol. 2018;12:1213–1218. doi:10.2147/OPTH.S168033
17. Kumar RS, Baskaran M, Singh K, Aung T. Clinical characterization of young Chinese myopes with optic nerve and visual field changes resembling glaucoma. J Glaucoma. 2012;21(5):281–286. doi:10.1097/IJG.0b013e318218253b
18. Laroche D, Rickford K, Mike EV, et al. A novel, low-cost glaucoma calculator to identify glaucoma patients and stratify management. J Ophthalmol. 2022;2022:5288726. doi:10.1155/2022/5288726
19. Grimes K, Madu CT, Carrington C, Laroche D. Validation of a novel low-cost glaucoma risk calculator for community-based screening in high-risk populations. Clin Ophthalmol. 2025;19:357–369. doi:10.2147/OPTH.S500509
20. Krueger RR, Seiler T, Gruchman T, Mrochen M, Berlin MS. Stress wave amplitudes during laser surgery of the cornea. Ophthalmology. 2001;108(6):1070–1074. doi:10.1016/S0161-6420(01)00570-X
21. Chaurasia SS, Luengo Gimeno F, Tan K, et al. In vivo real-time intraocular pressure variations during LASIK flap creation. Invest Ophthalmol Vis Sci. 2010;51(9):4641–4645. doi:10.1167/iovs.10-5228
22. Lauzirika G, Garcia-Gonzalez M, Bolivar G, et al. Measurement of the intraocular pressure elevation during laser-assisted in situ keratomileusis flap creation using a femtosecond laser platform. Transl Vis Sci Technol. 2021;10(3):9. doi:10.1167/tvst.10.3.9
23. Zhao Z, Michée S, Faure J-F, Baudouin C, Labbé A, Thomas BB. Effects of SMILE surgery on intraocular pressure, central corneal thickness, axial length, peripapillary retinal nerve fiber layer, and macular ganglion cell complex thickness. Journal of Ophthalmology. 2020;2020(1):4934196. doi:10.1155/2020/4934196
24. Özülken K, Ilhan Ç. Evaluation of retinal ganglion cell layer thickness in the early period after femtosecond LASIK surgery. Turk J Ophthalmol. 2020;50(4):211–215. doi:10.4274/tjo.galenos.2020.29939
25. Chen Y, Liao H, Sun Y, Shen X. Short-term changes in the anterior segment and retina after small incision lenticule extraction. BMC Ophthalmology. 2020;20(1):397. doi:10.1186/s12886-020-01668-7
26. Maden A, Yilmaz S, Yurdakul NS. Nonarteritic ischemic optic neuropathy after LASIK with femtosecond laser flap creation. J Neuroophthalmol. 2008;28(3):242–243. doi:10.1097/WNO.0b013e3181772452
27. Cameron BD, Saffra NA, Strominger MB. Laser in situ keratomileusis–induced optic neuropathy. Ophthalmology. 2001;108(4):660–665. doi:10.1016/S0161-6420(00)00577-7
28. Wang Z, Ma H, Zhang Y, Yuan Y, Liu Y, Chen Y. Changes in anterior chamber after myopic and hyperopic FS-LASIK. Ophthalmol Therapy. 2022;11(6):2243–2257. doi:10.1007/s40123-022-00579-8
29. Osman EA, Alsaleh AA, Al Turki T, Al Obeidan SA. Bilateral acute angle closure glaucoma after hyperopic LASIK correction. Saudi J Ophthalmol. 2009;23(3–4):215–217. doi:10.1016/j.sjopt.2009.10.006
30. Sánchez P, Moutsouris K, Pandolfi A. Biomechanical and optical behavior of human corneas before and after photorefractive keratectomy. J Cataract Refract Surg. 2014;40(6):905–917. doi:10.1016/j.jcrs.2014.03.020
31. Liu J, Roberts CJ. Influence of corneal biomechanical properties on intraocular pressure measurement: quantitative analysis. J Cataract Refract Surg. 2005;31(1):146–155. doi:10.1016/j.jcrs.2004.09.031
32. Li H, Wang Y, Dou R, et al. Intraocular pressure changes and relationship with corneal biomechanics after SMILE and FS-LASIK. Invest Ophthalmol Vis Sci. 2016;57(10):4180–4186. doi:10.1167/iovs.16-19615
33. Lanza M, Sbordone S, Tortori A, Gironi Carnevale UA, Melillo P, Simonelli F. Evaluating intraocular pressure after myopic photorefractive keratectomy: a comparison of different tonometers. J Glaucoma. 2022;31(6):406–412. doi:10.1097/IJG.0000000000002023
34. Schallhorn JM, Schallhorn SC, Ou Y. Factors that influence intraocular pressure changes after myopic and hyperopic LASIK and photorefractive keratectomy: a large population study. Ophthalmology. 2015;122(3):471–479. doi:10.1016/j.ophtha.2014.09.033
35. Iglesias M, Kudsieh B, Laiseca A, et al. Intraocular pressure after myopic laser refractive surgery measured with a new Goldmann convex prism: correlations with GAT and ORA. BMC Ophthalmology. 2022;22(1):79. doi:10.1186/s12886-022-02309-x
36. Gómez-Gómez A, Talens-Estarelles C, Alcocer-Yuste P, Nieto JC. Reliability of iCare ic100 rebound tonometry and agreement with goldmann applanation tonometry in healthy and post-myopic LASIK patients. J Glaucoma. 2021;30(8):634–642. doi:10.1097/IJG.0000000000001878
37. Ang RET, Bargas NVR, Martinez GHA, Sosuan GMN, Nabor-Umali MI. Comparison of three tonometers in measuring intraocular pressure in eyes that underwent myopic laser in situ keratomileusis and photorefractive keratectomy. Clin Ophthalmol. 2022;16:1623–1637. doi:10.2147/OPTH.S362344
38. Ye Y, Yang F, Ding L, et al. Comparison of Icare HOME and non-contact tonometer in intraocular pressure measurement in the early stage after ICL V4c implantation. Eur J Ophthalmol. 2022;32(6):3303–3311. doi:10.1177/11206721221093990
39. Medeiros FA, Meira-Freitas D, Lisboa R, Kuang T-M, Zangwill LM, Weinreb RN. Corneal hysteresis as a risk factor for glaucoma progression: a prospective longitudinal study. Ophthalmology. 2013;120(8):1533–1540. doi:10.1016/j.ophtha.2013.01.032
40. Guo H, Hosseini-Moghaddam SM, Hodge W. Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: a systematic review and meta-analysis. BMC Ophthalmology. 2019;19(1):167. doi:10.1186/s12886-019-1165-3
41. Arango AF, Tello A, Parra JC, Galvis V. Photorefractive surgery with excimer laser and its impact on the diagnosis and follow-up of glaucoma. a review. Ceska a slovenska oftalmologie. 2021;77(6):276–283. doi:10.31348/2021/8
42. Han KE, Kim H, Kim NR, Jun I, Kim EK, Kim T-I. Comparison of intraocular pressures after myopic laser-assisted subepithelial keratectomy: tonometry-pachymetry, Goldmann applanation tonometry, dynamic contour tonometry, and noncontact tonometry. J Cataract Refract Surg. 2013;39(6):888–897. doi:10.1016/j.jcrs.2013.01.035
43. Sadigh AL, Fouladi RF, Hashemi H, Beheshtnejad AH. A comparison between Goldmann applanation tonometry and dynamic contour tonometry after photorefractive keratectomy. Graefes Arch Clin Exp Ophthalmol. 2013;251(2):603–608. doi:10.1007/s00417-012-2142-1
44. Chen S, Lopes BT, Huang W, et al. Effectiveness of 4 tonometers in measuring IOP after femtosecond laser–assisted LASIK, SMILE, and transepithelial photorefractive keratectomy. J Cataract Refract Surg. 2020;46(7):967–974. doi:10.1097/j.jcrs.0000000000000204
45. Salouti R, Azimi A, Meshksar A, et al. Intraocular pressure before and after corneal refractive surgery: a prospective comparison of corvis ST and ocular response analyzer. J Glaucoma. 2024;33(10):780–784. doi:10.1097/IJG.0000000000002434
46. Hong J, Yu Z, Jiang C, et al. Corvis ST tonometer for measuring postoperative IOP in LASIK patients. Optometry and Vision Science. 2015;92(5):589–595. doi:10.1097/OPX.0000000000000575
47. Hosny M, Zaki RM, Ahmed RA, Khalil N, Mostafa HM. Changes in retinal nerve fiber layer thickness following mechanical microkeratome-assisted versus femtosecond laser-assisted LASIK. Clin Ophthalmol. 2013;7:1919–1922. doi:10.2147/OPTH.S51774
48. Koronis S, Diafas A, Tzamalis A, Samouilidou M, Mataftsi A, Ziakas N. Late-onset interface fluid syndrome: a case report and literature review. Semin Ophthalmol. 2022;37(7–8):839–848. doi:10.1080/08820538.2022.2102928
49. Lee V, Sulewski ME, Zaidi A, Nichols CW, Bunya VY. Elevated intraocular pressure–induced interlamellar stromal keratitis occurring 9 years after laser in situ keratomileusis. Cornea. 2012;31(1):87–89. doi:10.1097/ICO.0b013e31821140fa
50. Jia Z, Zhao S, Wei R, Huang Y, Zhang C, Yang R. Interface fluid syndrome: a potential lifelong complication after LASIK. A case report. Am J Ophthalmol Case Rep. 2018;11:23–25. doi:10.1016/j.ajoc.2018.04.020
51. Zheng K, Han T, Li M, et al. Corneal densitometry changes in a patient with interface fluid syndrome after small incision lenticule extraction. BMC Ophthalmol. 2017;17(1):34. doi:10.1186/s12886-017-0428-0
52. Senthil S, Rathi V, Garudadri C. Misleading Goldmann applanation tonometry in a post-LASIK eye with interface fluid syndrome. Indian J Ophthalmol. 2010;58(4):333–335. doi:10.4103/0301-4738.64133
53. Smith RJ. Diffuse lamellar keratitis A new syndrome in lamellar refractive surgery. Ophthalmology. 1998;105(9):1721–1726. doi:10.1016/S0161-6420(98)99044-3
54. Ravipati A, Pradeep T, Donaldson KE. Interface fluid syndrome after LASIK surgery: retrospective pooled analysis and systematic review. J Cataract Refract Surg. 2023;49(8):885–889. doi:10.1097/j.jcrs.0000000000001214
55. Javadi M-A, Mirbabaei-Ghafghazi F, Mirzade M, Yazdani S, Yaseri M. Steroid induced ocular hypertension following myopic photorefractive keratectomy. J Ophthalmic Vis Res. 2008;3(1):42–46.
56. Nagy ZZ, Szabó A, Krueger RR, Süveges I. Treatment of intraocular pressure elevation after photorefractive keratectomy. J Cataract Refract Surg. 2001;27(7):1018–1024. doi:10.1016/S0886-3350(01)00889-6
57. Vetrugno M, Maino A, Quaranta GM, Cardia L. A randomized, comparative open-label study on the efficacy of latanoprost and timolol in steroid induced ocular hypertension after photorefractive keratectomy. Eur J Ophthalmol. 2000;10(3):205–211. doi:10.1177/112067210001000303
58. Kim YJ, Yun S-C, Na JH, Tchah HW, Jung JJ, Sung KR. Glaucoma progression in eyes with a history of refractive corneal surgery. Invest Ophthalmol Visual Sci. 2012;53(8):4485–4489. doi:10.1167/iovs.12-9862
59. Stulting RD, John ME, Maloney RK, Assil KK, Arrowsmith PN, Thompson VM. Three-year results of artisan/verisyse phakic intraocular lens Implantation: results of the United States food and drug administration clinical trial. Ophthalmology. 2008;115(3):464–472.e461. doi:10.1016/j.ophtha.2007.08.039
60. Tahzib NG, Nuijts RM, Wu WY, Budo CJ. Long-term study of Artisan phakic intraocular lens implantation for the correction of moderate to high myopia: ten-year follow-up results. Ophthalmology. 2007;114(6):1133–1142. doi:10.1016/j.ophtha.2006.09.029
61. Huang D, Schallhorn SC, Sugar A, et al. Phakic intraocular lens implantation for the correction of MyopiaA report by the American academy of ophthalmology. Ophthalmology. 2009;116(11):2244–2258. doi:10.1016/j.ophtha.2009.08.018
62. Pineda R, Chauhan T. Phakic intraocular lenses and their special indications. J Ophthalmic Vis Res. 2016;11(4):422–428. doi:10.4103/2008-322X.194140
63. Niu L, Miao H, Han T, Ding L, Wang X, Zhou X. Visual outcomes of Visian ICL implantation for high myopia in patients with shallow anterior chamber depth. BMC Ophthalmology. 2019;19(1):121. doi:10.1186/s12886-019-1132-z
64. Choi H, Kim T, Kim SJ, et al. Predicting postoperative anterior chamber angle for phakic intraocular lens implantation using preoperative anterior segment metrics. Transl Vis Sci Technol. 2023;12(1):10. doi:10.1167/tvst.12.1.10
65. Fernandes P, González-Méijome JM, Madrid-Costa D, Ferrer-Blasco T, Jorge J, Montés-Micó R. Implantable collamer posterior chamber intraocular lenses: a review of potential complications. J Refract Surg. 2011;27(10):765–776. doi:10.3928/1081597X-20110617-01
66. Senthil S, Choudhari NS, Vaddavalli PK, Murthy S, Reddy JC, Garudadri CS. Etiology and management of raised intraocular pressure following posterior chamber phakic intraocular lens implantation in myopic eyes. PLoS One. 2016;11(11):e0165469. doi:10.1371/journal.pone.0165469
67. Almalki S, Abubaker A, Alsabaani NA, Edward DP. Causes of elevated intraocular pressure following implantation of phakic intraocular lenses for myopia. Int Ophthalmol. 2016;36(2):259–265. doi:10.1007/s10792-015-0112-4
68. Mimouni M, Alió Del Barrio JL, Alió JL. Occlusion of AquaPORT flow in a case of toxic anterior segment syndrome following implantable collamer lens surgery causing severe pupillary block. J Refract Surg. 2020;36(12):856–859. doi:10.3928/1081597X-20201015-01
69. Frost A, Ritter DJ, Trotter A, Pulia MS. Acute angle-closure glaucoma secondary to a phakic intraocular lens, an ophthalmic emergency. Clin Prac Cases Emerg Med. 2019;3(2):137–139. doi:10.5811/cpcem.2019.1.41399
70. Sánchez-Galeana CA, Zadok D, Montes M, Cortés MA, Chayet AS. Refractory intraocular pressure increase after phakic posterior chamber intraocular lens implantation. Am J Ophthalmol. 2002;134(1):121–123. doi:10.1016/S0002-9394(02)01414-9
71. Park IK, Lee JM, Chun YS. Recurrent occlusion of laser iridotomy sites after posterior chamber phakic IOL implantation. Korean J Ophthalmol. 2008;22(2):130–132. doi:10.3341/kjo.2008.22.2.130
72. Albo C, Nasser T, Szynkarski DT, et al. A comprehensive retrospective analysis of EVO/EVO+ implantable collamer lens: evaluating refractive outcomes in the largest single center study of ICL patients in the United States. Clin Ophthalmol. 2024;18:69–78. doi:10.2147/OPTH.S440578
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Photorefractive Keratectomy Enhancement (PRK) After Small-Incision Lenticule Extraction (SMILE)
Moshirfar M, Parsons MT, Chartrand NA, Lau CK, Stapley S, Bundogji N, Ronquillo YC, Hoopes PC
Clinical Ophthalmology 2022, 16:3033-3042
Published Date: 12 September 2022
A Comprehensive Retrospective Analysis of EVO/EVO+ Implantable Collamer Lens: Evaluating Refractive Outcomes in the Largest Single Center Study of ICL Patients in the United States
Albo C, Nasser T, Szynkarski DT, Nguyen N, Mueller B, Libfraind L, Parkhurst G
Clinical Ophthalmology 2024, 18:69-78
Published Date: 9 January 2024