Back to Journals » Journal of Pain Research » Volume 16
The Association Between the Patient Self-Report Survey for the Assessment of Fibromyalgia with Pain Sensitivity and Psychological Factors in Individuals with Musculoskeletal Pain
Authors Wilson AT, Razzell C, Hanney WJ ![]()
Received 13 June 2023
Accepted for publication 16 September 2023
Published 28 September 2023 Volume 2023:16 Pages 3297—3308
DOI https://doi.org/10.2147/JPR.S425687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Abigail T Wilson,1,2 Charlotte Razzell,2 William J Hanney1,2
1University of Central Florida, School of Kinesiology and Rehabilitation Sciences, College of Health Professions and Sciences, Orlando, FL, USA; 2Musculoskeletal Research Lab, Institute of Exercise Physiology and Rehabilitation Science, University of Central Florida, Orlando, FL, USA
Correspondence: William J Hanney, University of Central Florida, College of Health Professions and Sciences, Division of Physical Therapy, Health Sciences Building I, 12805 Pegasus Drive, Orlando, FL, 32816, USA, Tel +1 407-823-0217, Fax +1 407-823-3464, Email [email protected]
Purpose: The Patient Self-Report Survey for the Assessment of Fibromyalgia may potentially be a method for subgrouping patients with musculoskeletal pain who have a nociplastic pain presentation. Limited research has explored the convergent validity of this questionnaire against psychophysical measures of pain sensitivity and psychological factors in individuals with musculoskeletal pain. Therefore, the purpose of this study is to examine the strength of the association between total scores on the Patient Self-Report Survey for the Assessment of Fibromyalgia with clinical, pain sensitivity, and psychological factors.
Patients and Methods: As a secondary analysis of a cross-sectional study, participants with shoulder (n = 20) or low back pain (n = 20) completed Quantitative Sensory Testing (QST), pain-related psychological questionnaires, and the Patient Self-Report Survey for the Assessment of Fibromyalgia. A Spearman correlation determined the association between total scores on the Patient Self Report Survey for the Assessment of Fibromyalgia with psychological factors and pain sensitivity behaviorally assessed with QST.
Results: Negative psychological factors demonstrate moderate to strong positive associations with the Patient Self-Report Survey for the Assessment of Fibromyalgia (rho range = 0.36– 0.80), suggesting greater negative psychological factors were observed in patients with higher severity of fibromyalgia symptoms. Pain sensitivity factors demonstrated weak to moderate negative associations with The Patient Self-Report Survey for the Assessment of Fibromyalgia (PPT rho range=− 0.36- − 0.41), suggesting that elevated pain sensitivity was observed in individuals with higher severity of nociplastic pain symptoms.
Conclusion: Collectively, this supports the convergent validity of the Patient Self-Report Survey for the Assessment of Fibromyalgia with psychological and pain sensitivity factors in patients with musculoskeletal pain.
Keywords: pain measurement, pain threshold, nociplastic pain, central sensitization
Introduction
Approximately 5–15% of the general population experiences nociplastic pain,1 a mechanistic classification for pain reflecting a change in nociception without a link to tissue damage.2 Consistent with the biopsychosocial model for pain, nociplastic pain is impacted by changes in the nervous system processing of noxious stimuli and psychological factors. In individuals with nociplastic pain, an amplification of nociceptive transmission3 and activity in parts of the brain responsible for processing pain and emotions are observed.4 Negative psychological factors are also heightened in this population, with greater levels of catastrophizing and depression reported.5,6 Heightened sensory and negative psychological factors are demonstrated in patients with nociplastic pain.7–10
Quantitative Sensory Testing (QST) is the systematic application of sensory stimuli for the purpose of behaviorally assessing somatosensory function or dysfunction.11 QST may be used to examine local and widespread hypersensitivity12–15 as well as modulatory capacity. Elevated pain sensitivity is demonstrated in individuals with nociplastic pain conditions compared to healthy controls.16–20 A similar pain sensitivity pattern is observed in subgroups of individuals experiencing musculoskeletal pain with a nociplastic presentation (mixed pain conditions) as hyperalgesia is observed in patients with moderate-to-severe chronic low back pain.21 Alterations in pain sensitivity behaviorally measured by QST may be one component that helps distinguish individuals with a nociplastic pain presentation. While QST is included in clinical criteria to identify patients with musculoskeletal pain and a nociplastic pain presentation,22 laboratory-based QST is often difficult to apply in clinical practice due to its expense and limitations in interpreting the results.11,23
Psychological factors, including emotional distress and depression, are predictors in the transition to persistent musculoskeletal pain7 and a risk factor for chronic widespread pain.24 In individuals with low back pain who have a nociplastic pain presentation, negative pain-related psychological factors25 and catastrophizing26 are significantly higher. Elevated negative pain-related psychological factors are also present in patients with nociplastic pain conditions, such as fibromyalgia. Higher rates of depression are observed in this population,5 and nociplastic pain is associated with higher levels of anxiety and negative mood.27 Collectively, elevated sensory-related and psychological factors are present in nociplastic pain conditions.16
A current challenge in clinical practice is the lack of a gold standard for identifying individuals with nociplastic pain (or central sensitization). Clinicians report being able to identify central sensitization in viewpoint articles and clinical practice28–30 based on a patient’s history of widespread pain and additional clinical symptoms.31 However, this approach lacks standardization in identifying central sensitization (or a nociplastic pain presentation). Self-report questionnaires including The Central Sensitization Index (CSI)32 are standardized approaches that may be efficiently administered in a clinical setting. The CSI helps reliably quantify central sensitization symptoms in patients with chronic pain.32–34 However, the CSI lacks validity against QST35,36 and high rates of false positives are observed in patients with negative psychological factors.34,35,37
The Patient Self-Report Survey for the Assessment of Fibromyalgia (also called the 2011 Fibromyalgia Survey) was originally developed as a method for identifying the prevalence of fibromyalgia in population-based studies38,39 and has been used to categorize a nociplastic pain presentation in musculoskeletal pain populations.13,25,40 The Patient Self-Report Survey for the Assessment of Fibromyalgia measures the severity of fibromyalgia-related symptoms and number of pain locations. Given that fibromyalgia is generally considered a primary example of a nociplastic pain condition, a questionnaire measuring the severity of fibromyalgia symptoms has the potential to serve as a proxy measure for identifying clinically important subgroups of patients with nociplastic pain affecting the musculoskeletal system. Twenty-two percent of patients receiving physical therapy for low back pain meet the threshold for fibromyalgia, and therefore a nociplastic pain presentation, based on the Patient Self-Report Survey for the Assessment of Fibromyalgia.25 When applying the threshold from this questionnaire to distinguish patients with low back pain with and without a nociplastic pain presentation, catastrophizing and depression are significantly higher in those with a nociplastic pain presentation.13,25,40
Collectively, the Patient Self-Report Survey for the Assessment of Fibromyalgia may be a promising questionnaire to assist in identifying a nociplastic pain presentation in patients with musculoskeletal pain. However, the validity of this questionnaire against pain sensitivity and psychological factors in individuals with musculoskeletal pain has been minimally investigated. Therefore, the purpose is to examine the strength of the association between total scores on the Patient Self-Report Survey for the Assessment of Fibromyalgia with clinical presentation, psychological factors, and pain sensitivity behaviorally assessed with QST. We aim to test the convergent validity of this questionnaire by examining whether the Patient Self-Report Survey for the Assessment of Fibromyalgia may be able to quantify pain sensitivity and psychological factors and, therefore, be a clinically useful measure to give insight into the presence of a nociplastic pain presentation in patients with musculoskeletal pain.
Methods
This is a secondary analysis of a cross-sectional observational study in individuals with shoulder (n = 20) or low back pain (n = 20). Participants attended one testing session in which they completed self-report questionnaires (pain-related psychological factors and the Patient Self-report Survey for the Assessment of Fibromyalgia) and underwent Quantitative Sensory Testing (QST). All study procedures were approved by the University of Central Florida’s Institutional Review Board and participants provided written informed consent. Additionally, this study complies with the Declaration of Helsinki.
Participants
Participants between 18 and 75 years old with shoulder or low back pain intensity rated at least a 3/10 (0 = no pain, 10 = worst pain imaginable) within the past 24 hours of testing were eligible to participate in the study. Participants were excluded if pain was due to fibromyalgia, surgery, or fracture within the past six months, or myelopathy. Participants were also excluded for safety during QST if they reported any medical conditions that affected sensation, blood clotting disorders, or contraindications to the application of ice.
Participants provided demographic information (age, sex, race, ethnicity) using a standard intake form. Shoulder or low back pain intensity was reported with the 101-point Numerical Pain Rating Scale (NPRS) in which 0 = no pain and 100 = worst pain imaginable. Participants provided their current, best, and worst pain intensity within the past 24 hours. These values were averaged, and the average pain intensity was analyzed. Pain-related disability was self-reported with the Oswestry Disability Index for individuals with low back pain41,42 and QuickDASH for individuals with shoulder pain.43,44
Patient Self-Report Survey for the Assessment of Fibromyalgia
The Patient Self-report Survey for the Assessment of Fibromyalgia (also called the 2011 Fibromyalgia Survey) is a five-item self-report questionnaire that measures widespread pain index and symptom severity.38 Participants check the number of locations of pain on a body diagram (up to 19 locations), rate the severity of three symptoms (fatigue, trouble thinking, and waking up tired), and report if they have experienced any of the following three somatic symptoms (pain/cramps abdomen, depression, headache) (up to 12 points for symptom severity and somatic symptoms). These items are scored according to the guidelines of the questionnaire with possible scores ranging from 0 to 31. A higher total score indicates greater widespread pain and severity of symptoms.38 A score of 13 or higher on this measure indicates fibromyalgia,38 but this threshold has been used to categorize a nociplastic pain presentation in musculoskeletal pain research.13,25,40 Participants also report if there is another disorder that could potentially explain these symptoms and if the symptoms have been present for over 3 months.
Psychological Factors
Participants completed several self-report questionnaires examining the following pain-related psychological factors: depression, fear of pain, pain catastrophizing, fear avoidance beliefs, kinesiophobia, pain-related anxiety, and pain self-efficacy.
Center for Epidemiologic Studies – Depression (CES-D)
The CES-D is a 20-item self-report measure in which participants rate the frequency of depression-related symptoms over the past week.45 The total score is the sum of the 20 questions. Scores may range from 0 to 60 with a higher score indicating a greater frequency of depression-related symptoms. Total scores were used in the analysis. The CES-D is a valid and reliable measure of depression.46
Fear of Pain Questionnaire-9 (FPQ-9)
The FPQ-9 is a shortened 9-item self-report measure in which participants rate the amount of fear associated with activities that would elicit pain, such as breaking your arm, from 1 = not at all to 5 = extreme. The total score ranges from 9 to 45 with higher scores indicating greater fear of pain.47 The FPQ-9 demonstrates concurrent, convergent, and divergent validity.47
Pain Catastrophizing Scale (PCS)
The PCS is a 13-item self-report measure in which participants rate the degree of catastrophic thinking during a painful episode from 0 = not at all to 4 = all the time. The total score ranges from 0 to 52 with higher scores indicating greater pain catastrophizing.48 The PCS demonstrates concurrent and predictive validity.49
Fear-Avoidance Beliefs Questionnaire (FABQ)
The FABQ is a 16-item self-report measure that includes a work (W) and physical activity (PA) sub-section. Participants rate how fear-avoidance beliefs may have contributed to their pain from 0 = completely disagree to 6 = completely agree. The FABQ-PA subscale ranges from 0 to 24 and FABQ-PA subscale ranges from 0 to 42. Higher scores indicate greater fear-avoidance beliefs.50 The FABQ is reliable and valid in patients with shoulder pain and low back pain.51
Tampa Scale of Kinesiophobia-11 (TSK-11)
The TSK-11 is a shortened version of the TSK that includes 11 items that measure the degree of fear of movement. Participants rate the degree to which they agree with statements relating to fear of movement from 1 = strongly disagree to 4 = strongly agree. Total scores range from 11 to 44 with higher scores indicating greater fear of movement.52 The TSK-11 has good reliability, responsiveness, and predictive validity.52
Pain Anxiety Symptoms Scale-20 (PASS-20)
The PASS-20 is a shortened, self-report measure of pain-related anxiety in which participants rate the frequency of anxiety during a painful episode from 0 = never to 5 = always. Total scores range from 0 to 100 with higher scores indicating greater anxiety related to pain.53 The PASS-20 has construct validity in a sample of patients receiving physical therapy for musculoskeletal pain.54
Pain Self-Efficacy Questionnaire (PSEQ)
The PSEQ is a 10-item self-report measure of confidence in doing activities despite pain (self-efficacy). Participants rate their confidence from 0 = not confident at all to 6 = completely confident. Total scores range from 0 to 60 with higher scores indicating greater self-efficacy.55
Quantitative Sensory Testing (QST)
QST was conducted in a laboratory setting with a standard temperature. Participants were trained on rating pain using the 101-point Numerical Pain Rating Scale (NPRS) in which 0 = no pain and 100 = worst pain imaginable and completed a familiarization task with each of the pain sensitivity tests. All QST (except temporal summation and conditioned pain modulation) were performed in three locations: 1) deltoid muscle belly, 2) medial to posterior superior iliac spine (PSIS), and 3) tibialis anterior muscle belly on the same side as the patient’s shoulder or low back pain. Two trials were performed at each site with the average threshold analyzed. Three sites were selected as a measure of local and widespread changes in pain sensitivity in individuals with shoulder or low back pain. QST was performed in the following order: Cold Pain Threshold (CPT), Heat Pain Threshold (HPT), Temporal Summation (TS), Pressure Pain Threshold (PPT), and Conditioned Pain Modulation (CPM).
Static Pain Sensitivity Tests
Cold Pain Threshold (CPT)
A 2 × 1 inch thermode attached to a Thermal Cutaneous Stimulator-II (TCS-II) (QST.Lab, Strasbourg, France) was applied to the skin. The thermode decreased from a baseline of 32°C at a rate of 1°C/second to a maximum of 0°C. Participants indicated when the temperature changed from a “comfortable cold to slightly unpleasant pain” by pressing a button. Participants then rated the pain intensity at threshold using the 101-point NPRS. CPT was recorded in °C and a higher CPT temperature indicated a higher pain sensitivity.
Heat Pain Threshold (HPT)
A 2 × 1 inch thermode attached to a TCS-II was applied to the skin. The thermode increased from a baseline of 32°C at a rate of 1°C/second to a maximum of 50°C. Participants indicated when the temperature changed from a “comfortable warmth to slightly unpleasant pain” by pressing a button. Participants then rated the pain intensity at threshold using the 101-point NPRS. HPT was recorded in °C and a lower HPT temperature indicated a higher pain sensitivity.
Pressure Pain Threshold (PPT)
A digital computerized pressure algometer (Algomed, Ramat Yishai, Israel) with a 1 cm rubber tip was applied at a constant rate. Participants indicated when the sensation changed from “comfortable pressure to slightly unpleasant pain” by pressing a button. Pain intensity was then rated at threshold using the 101-point NPRS. PPT was recorded in kilopascals (kPa) and a lower PPT indicated a higher pain sensitivity. PPT is reliable and able to distinguish between individuals with and without musculoskeletal pain.56–58
Dynamic Pain Sensitivity Tests
Temporal Summation (TS)
A 2 × 1 inch thermode attached to a Thermal Cutaneous Stimulator-II (TCS-II) (QST.Lab, Strasbourg, France) delivered a train of 10 heat pulses that increased from 41°C to 49°C at a rate to maintain the desired inter-stimulus interval. Individuals with persistent low back pain demonstrate significantly higher TS and aftersensations compared to healthy controls, suggesting this measure may distinguish these populations.59
Conditioned Pain Modulation (CPM)
CPM consisted of three steps.60 First, PPT was applied to the web space of the foot opposite the side of the patient’s shoulder or low back (testing stimulus #1). Second, participants immersed the hand on the same side as their shoulder or low back pain into a cold water bath set to a temperature of 8°C for men and 10°C for women for one minute (conditioning stimulus). Third, PPT was re-applied to the web space of the foot allowing for examination of immediate changes in testing stimulus after the application of a painful conditioning stimulus. CPM efficiency was calculated using the following formula: pre-testing stimulus – post-testing stimulus. A negative value indicates a pain inhibitory process (efficient CPM).60 A larger proportion of patients with a less efficient CPM are observed in individuals with persistent pain relative to healthy controls.61
Statistical Analysis
IBM SPSS software version 28 (Armonk, NY) was used for data analysis. Tests of normality indicated scores on the Patient Self Report Survey for the Assessment of Fibromyalgia (Kolmogorov–Smirnov p < 0.01 and Shapiro–Wilk p = 0.02) were not normally distributed. Visual inspection of the scatterplot indicated that a positive monotonic relationship was observed. Because bivariate normality assumptions were not met, Spearman correlation was used to determine the association between total scores on the Patient Self-report Survey for the Assessment of Fibromyalgia and clinical features, psychological factors, and pain sensitivity behaviorally assessed with QST. Magnitude of associations was interpreted with the following thresholds for the correlation coefficient: 0.3 = weak, 0.5 = moderate, and 0.8 = strong.62 A p-value less than 0.05 indicated statistical significance.
Clinical features associated with the Patient Self Report Survey for the Assessment of Fibromyalgia included pain duration (weeks), average pain intensity, QuickDASH for individuals with shoulder pain, and ODI total score for individuals with low back pain. Psychological factors associated with the Patient Self Report Survey for the Assessment of Fibromyalgia included CES-D, FPQ-9, PCS, FABQ, TSK-11, PASS-20, PSEQ. QST associated with the Patient Self Report Survey for the Assessment of Fibromyalgia included CPT, HPT, PPT applied to the deltoid, low back, and tibialis anterior, pain ratings during CPT, HPT, PPT, TS, and CPM efficiency.
Results
Demographic and Clinical Factors of Participants
Forty participants (n = 20 with low back pain, n = 20 with shoulder pain) were included in this analysis. Participants were mean ± standard deviation (SD) age = 26.00 ± 10.62 years old and 60.00% were female, 71.80% were white, 5.10% were African American, 12.80% were Asian, 10.20% indicated other for race and 35.00% were Hispanic.
Mean ± SD total scores on the Patient Self-report Survey for the Assessment of Fibromyalgia = 7.45 ± 4.13. Participants were experiencing low to moderate intensity of pain at the time of testing. For the total sample, mean ± SD pain intensity on the 101-point NPRS = 33.83 ± 19.84. Individuals with low back pain reported total ODI scores = 7.50 ± 5.82. Individuals with shoulder pain reported quickDASH scores = 55.00 ± 25.88. Average pain duration in weeks of the total sample = 92.79 ± 134.49.
The Patient Self-Report Survey for the Assessment of Fibromyalgia demonstrated a weak, non-significant association with the average pain intensity (rho = −0.03, p = 0.86) and pain duration (rho = −0.04, p = 0.82). A weak to moderate non-significant association was demonstrated for quickDASH scores (rho = 0.36, p = 0.12) and a moderate significant association was observed for ODI scores (rho = 0.57, p = 0.01). The Patient Self-Report Survey for the Assessment of Fibromyalgia was not associated with pain intensity or chronicity. However, the Patient Self-Report Survey for the Assessment of Fibromyalgia displayed a moderate positive association with pain-related disability in individuals with low back pain, suggesting that higher severity of fibromyalgia-related symptoms is associated with higher pain-related disability. Correlation coefficients by anatomical location of pain are presented in Table 1.
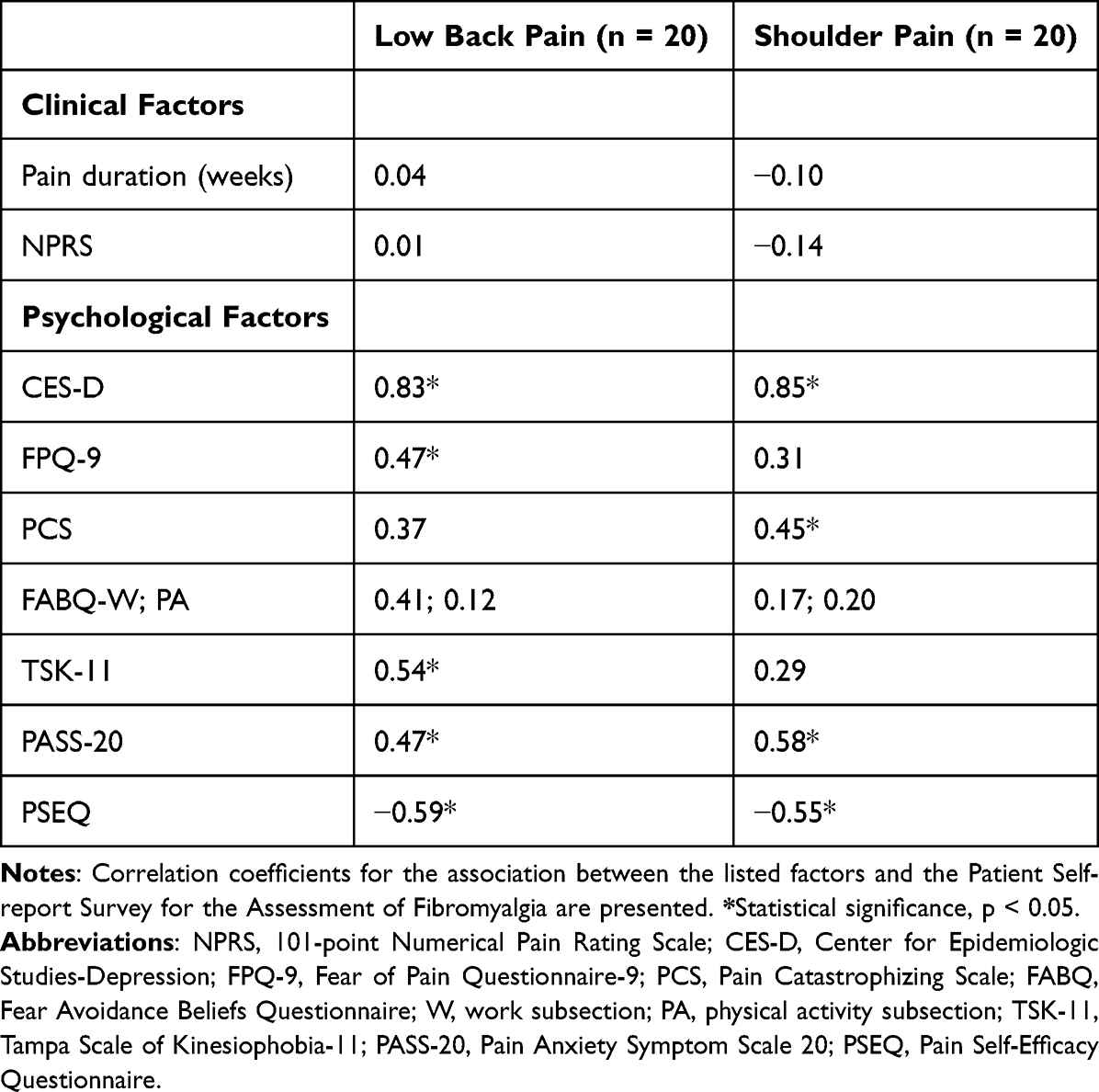 |
Table 1 Spearman Correlation Coefficients for Clinical and Psychological Factors by Anatomic Location of Pain |
Psychological Factors
For the total sample, the Patient Self-report Survey for the Assessment of Fibromyalgia demonstrated a significant, strong positive association with depression (rho = 0.80, p < 0.01). A significant, moderate to strong negative association was observed with self-efficacy (rho = −0.58, p < 0.01). Pain anxiety (rho = 0.57, p < 0.01) demonstrated a moderate to large significant association with the Patient Self-Report Survey for the Assessment of Fibromyalgia. Collectively, this suggests higher depressionand lower self-efficacy are strongly associated with the Patient Self-Report Survey for the Assessment of Fibromyalgia. Pain-related anxiety is moderately to strongly associated with the Patient Self-Report Survey for the Assessment of Fibromyalgia.
Kinesiophobia (rho = 0.47, p < 0.01), fear of pain (rho = 0.36, p = 0.02), and catastrophizing (rho = 0.41, p < 0.01) demonstrated moderate associations with The Patient Self-Report Survey for the Assessment of Fibromyalgia. This suggests that higher kinesiophobia, fear of pain, and catastrophizing were positively associated with The Patient Self-Report Survey for the Assessment of Fibromyalgia scores with a moderate to strong correlation.
Fear-avoidance beliefs were not associated with The Patient Self-report Survey for the Assessment of Fibromyalgia (work subsection rho = 0.32, p = 0.06; physical activity rho = 0.13, p = 0.43).
Correlation coefficients by anatomical location are presented in Table 1.
Pain Sensitivity
Static Pain Sensitivity
Thermal Pain Sensitivity
HPT applied to the low back trended toward being significantly associated with the Patient Self-Report Survey for the Assessment of Fibromyalgia (rho = −0.29, p = 0.06). HPT applied to deltoid (rho = −0.24, p = 0.14) and tibialis anterior (rho = −0.24, p = 0.13) displayed a weak to moderate non-significant correlation. Pain ratings at HPT were significantly associated with The Patient Self-Report Survey for the Assessment of Fibromyalgia (low back: rho = −0.40, p = 0.01; deltoid rho = −0.41, p = 0.01; tibialis anterior rho = −0.35, p = 0.03). A negative weak to moderate association was observed, suggesting individuals with higher severity of fibromyalgia symptoms provided lower pain ratings at threshold. Collectively, individuals with higher severity of fibromyalgia symptoms appear to demonstrate significantly lower pain ratings.
CPT was also applied to the shoulder, low back, and leg. CPT was not associated with The Patient Self-report Survey for the Assessment of Fibromyalgia with the exception of pain ratings during CPT at the back (weak to moderate association, rho = −0.43, p = 0.02). Correlations ranged from 0.17 to 0.27.
Pressure Pain Sensitivity
PPT applied to the low back was significant, and a small to moderate negative association was observed (rho = −0.36, p = 0.03), indicating people with higher severity of fibromyalgia symptoms have lower PPT. PPT applied to the deltoid (rho = −0.49, p < 0.01) and tibialis anterior (rho = −0.41, p = 0.01) displayed a weak to moderate negative association with The Patient Self-Report Survey for the Assessment of Fibromyalgia. Pain ratings at threshold were significantly associated with scores on the Patient Self-report Survey for the Assessment of Fibromyalgia (low back rho = −0.45, p = 0.01; deltoid rho = −0.40, p = 0.01; tibialis anterior rho = −0.39, p = 0.01) with a weak to moderate effect. Collectively, individuals with higher severity of fibromyalgia symptoms appear to demonstrate significantly lower PPT applied to the extremities with lower pain ratings.
Dynamic Pain Sensitivity
Thermal temporal summation was not associated with the Patient Self-Report Survey for the Assessment of Fibromyalgia (rho = −0.03, p = 0.87). CPM efficiency was not associated with the Patient Self-Report Survey for the Assessment of Fibromyalgia (rho = −0.13, p = 0.43).
Correlation coefficients by anatomical location of pain are presented in Table 2.
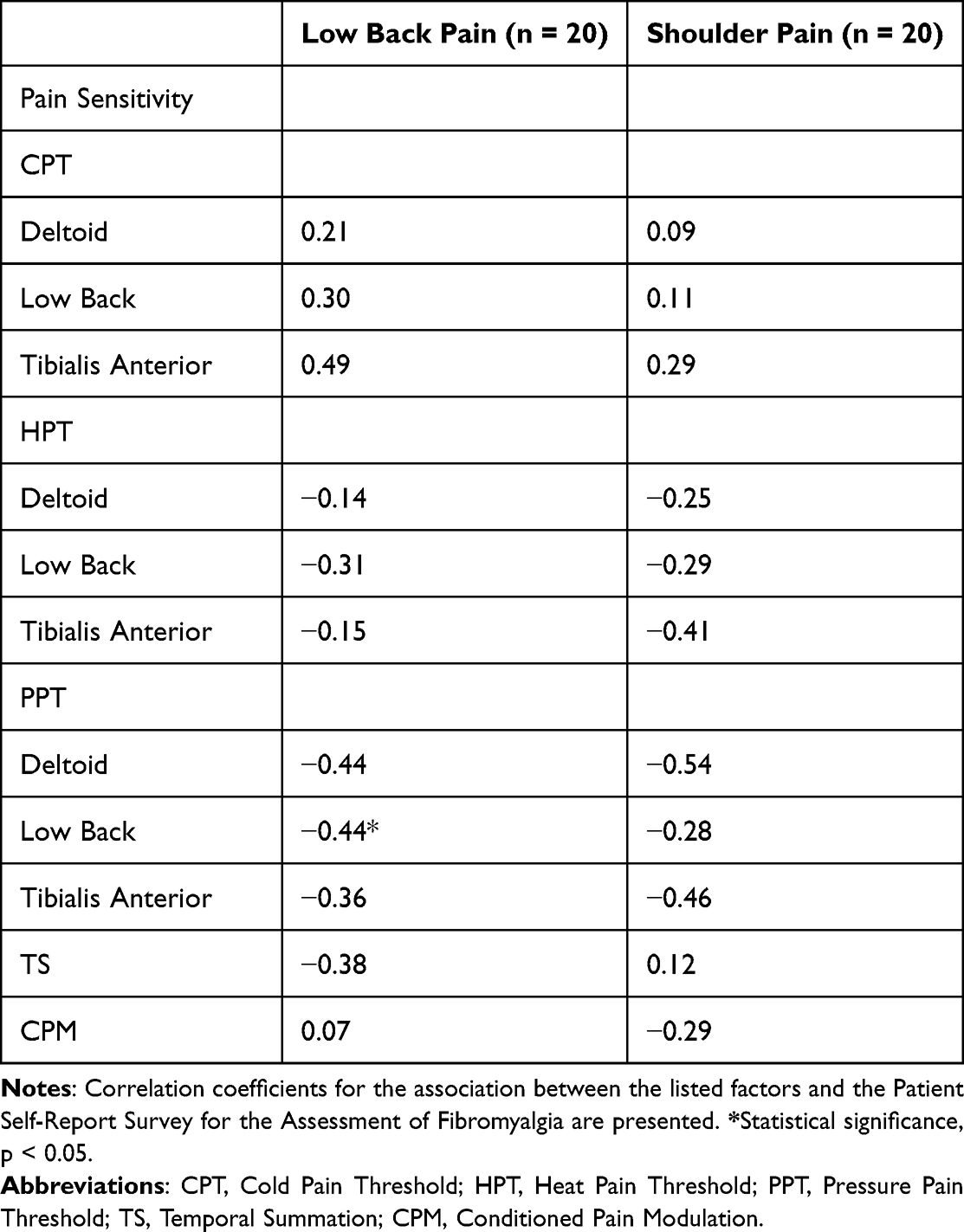 |
Table 2 Correlation Coefficients for Pain Sensitivity Factors by Anatomic Location of Pain |
Discussion
This study aimed to examine the convergent validity of the Patient Self-Report Survey for the Assessment of Fibromyalgia in patients with shoulder and low back pain by correlating the total score of this questionnaire with measures of pain sensitivity and psychological factors. Psychological factors demonstrate moderate to strong positive associations with the Patient Self-Report Survey for the Assessment of Fibromyalgia, suggesting greater negative psychological factors are observed in patients with higher severity of fibromyalgia symptoms. Pain sensitivity factors demonstrate weak to moderate negative associations with The Patient Self-Report Survey for the Assessment of Fibromyalgia, suggesting that elevated pain sensitivity may be observed in individuals with higher severity of nociplastic pain symptoms. Collectively, this supports the convergent validity of the Patient Self-Report Survey for the Assessment of Fibromyalgia with psychological and pain sensitivity factors important to the development of nociplastic pain in patients with musculoskeletal pain. These findings are clinically significant because they suggest the Patient Self-Report Survey for the Assessment of Fibromyalgia may be useful in providing insight into the presence of nociplastic pain in patients with shoulder or low back pain.
Psychological Factors
Higher depression, anger, anxiety, kinesiophobia, fear of pain, and catastrophizing were associated with higher scores on the Patient Self-Report Survey for the Assessment of Fibromyalgia and, therefore, severity of nociplastic pain symptoms. A lower self-efficacy was associated with higher scores on the Patient Self-Report Survey for the Assessment of Fibromyalgia. A preliminary study from our research group found patients receiving physical therapy for low back pain categorized as having symptoms consistent with fibromyalgia (and therefore a nociplastic pain presentation) based on this questionnaire had significantly higher depression, catastrophizing, and anxiety.25 The results from these separate studies from our group are consistent. The results of this study are further supported in the work by Brummett et al40 and Aoyagi et al.13 Patients with spine pain who have a fibromyalgia-like phenotype have significantly higher levels of depression,13,40 anxiety,13,40 and catastrophizing.13 Assessment of multiple pain-related psychological domains can be important to separate clinical depression that requires medical treatment from overlapping frustration of having chronic pain for long periods of time. We add to this body of literature by now demonstrating that higher kinesiophobia and fear of pain are moderately to strongly associated with greater severity of nociplastic pain symptoms.
Pain Sensitivity Factors
Associations between pain sensitivity and the Patient Self-report Survey for the Assessment of Fibromyalgia are weak to moderate and appear to be modality dependent. The Patient Self-report Survey for the Assessment of Fibromyalgia was significantly correlated with PPT at all sites. This result is corroborated by prior research in patients with knee osteoarthritis demonstrating the 2011 fibromyalgia survey criteria (Widespread Pain Index and Symptom Severity Score) were significantly correlated with pressure pain sensitivity in women.63 Widespread hyperalgesia was observed in patients with higher fibromyalgia survey criteria scores, suggesting these questionnaires may help identify patients with central sensitization.63 The results of our study confirm these findings and provide support for the convergent validity of the Patient Self-Report Survey for the Assessment of Fibromyalgia questionnaire as a self-report measure of widespread sensitization. The Patient Self-Report Survey for the Assessment of Fibromyalgia is clinically feasible to administer, and emerging evidence supports that this questionnaire may be capable of identifying nociplastic pain in a subgroup of patients with musculoskeletal pain.
The results of this study indicate that individuals with greater severity of nociplastic pain symptoms display greater sensitivity to pressure stimuli at all sites and heat stimuli along the spine. Given that our sample was in individuals with shoulder or low back pain, this suggests widespread elevations in pain sensitivity were observed in patients with higher scores on this questionnaire. Consistent with our findings, total scores on the 2011 Fibromyalgia criteria were significantly associated with PPT in individuals with low back pain13 and knee osteoarthritis.63 However, we add to the body of literature by demonstrating that there may be site-specific and modality-specific considerations in individuals with nociplastic pain presentation, as indicated on The Patient Self-Report Survey for the Assessment of Fibromyalgia. Consistent with prior research, patients with fibromyalgia are more sensitive to heat but not pressure stimuli.19 Pressure stimuli activate deep mechanoreceptors responsive to noxious stimuli and heat stimuli activate cutaneous thermal receptors responsive to noxious stimuli. The results of this study also concur with prior systematic reviews that patients with chronic low back pain demonstrate significantly lower PPT.12 Pain ratings at threshold were significantly associated with scores on The Patient Self-Report Survey for the Assessment of Fibromyalgia with a weak to moderate effect, suggesting patients with a nociplastic pain presentation are more sensitive to experimentally induced stimuli compared to other pain conditions.21 The results of our study indicate weak, non-significant associations are demonstrated between self-report measures of central sensitization and dynamic measures of pain sensitivity (temporal summation, conditioned pain modulation). The CSI and Pain Sensitivity Questionnaire also show weak or no correlations with temporal summation and conditioned pain modulation.64
Symptoms of persistent pain conditions may overlap even though the pathoanatomical location of pain differs. Prior studies have viewed musculoskeletal pain symptoms along a continuum rather than as a discrete condition and applied measures of sensitization, such as the CSI or Patient Self-Report Survey for the Assessment of Fibromyalgia, to measure severity of nociplastic pain symptoms.13,40 Widespread pain occurs in a subgroup of individuals with musculoskeletal pain.13 However, a challenge in clinical practice is identifying subgroups of patients with mixed pain conditions or those with musculoskeletal pain who also have a nociplastic pain presentation. Biopsychosocial factors may represent neurophysiological mechanisms contributing to a nociplastic pain presentation. The Patient Self-report Survey for the Assessment of Fibromyalgia has the potential to be used in research as a surrogate measure for nociplastic pain presentation in other chronic pain conditions. The results of this study are clinically relevant as they support the convergent validity of this questionnaire with the underlying biopsychosocial mechanisms of nociplastic pain in patients with musculoskeletal pain.
There are important considerations when applying this questionnaire to individuals with musculoskeletal pain. The 2011 American College of Rheumatology authors caution that the use of modified criteria based on self-report symptoms should only be used for research and not for a clinical diagnosis of fibromyalgia.38,39,65 In 2010, the tender point criteria was removed due to difficulty in performing the examination.65 The 2010 criteria moved to counting the number of painful regions, the widespread pain index, and symptom severity scale.65 In 2011, the criteria then introduced the fibromyalgia severity score to reflect fibromyalgia can be along a continuum of symptoms similar to other nociplastic pain conditions.38 Therefore, the fibromyalgia symptom severity score may be useful to determine the severity of fibromyalgia symptoms and may serve as a measure of the level of fibromyalgia type symptoms.39 More recently, the 2016 criteria introduced a generalized pain criterion based on pain in at least 4 of 5 regions.39 The 2016 criteria also support the use of the fibromyalgia symptom scale when fibromyalgia is viewed as a continuum of symptoms and recommend reporting this as a measure of symptom severity.39
Limitations
As a secondary analysis, the limitation of our study is the small sample size and that we did not specifically recruit for patients with a nociplastic pain presentation. Future trials may aim to recruit a larger sample of individuals with chronic pain. Our intent was to examine if this questionnaire was capable of potentially being used to screen for a nociplastic pain presentation. As a result, we did not specifically recruit a sample of individuals with chronic pain. Additionally, we did not administer any additional self-report measures of central sensitization including the CSI. As a result, it is unknown if pain sensitivity and psychological factors would be associated with the CSI in this sample. Future studies may aim to apply this questionnaire in a larger sample of individuals with nociplastic pain.
Conclusion
The Patient Self-Report Survey for the Assessment of Fibromyalgia demonstrates convergent validity with pain sensitivity and psychological factors in patients with shoulder or low back pain. Moderate to strong correlations between negative psychological factors and severity of nociplastic pain symptoms were observed. Weak to moderate correlations between pain sensitivity and severity of nociplastic pain symptoms were observed. As a result, this questionnaire may have future application in clinical research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dydyk AM, Givler A. Central Pain Syndrome. StatPearls Publishing; 2022. Available from: http://www.ncbi.nlm.nih.gov/books/NBK553027/.
2. International Association for the Study of Pain. IASP Terminology. Available from: https://www.iasp-pain.org/resources/terminology/.
3. Woolf CJ, Thompson SW. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain. 1991;44(3):293–299. doi:10.1016/0304-3959(91)90100-C
4. Gracely RH, Petzke F, Wolf JM, Clauw DJ. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46(5):1333–1343. doi:10.1002/art.10225
5. Munipalli B, Allman ME, Chauhan M, et al. Depression: a Modifiable Risk Factor for Poor Outcomes in Fibromyalgia. J Prim Care Community Health. 2022;13:21501319221120736. doi:10.1177/21501319221120738
6. Gracely RH, Geisser ME, Giesecke T, et al. Pain catastrophizing and neural responses to pain among persons with fibromyalgia. Brain. 2004;127(Pt 4):835–843. doi:10.1093/brain/awh098
7. Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine. 2002;27(5):E109–20. doi:10.1097/00007632-200203010-00017
8. Clark J, Nijs J, Yeowell G, Goodwin PC. What Are the Predictors of Altered Central Pain Modulation in Chronic Musculoskeletal Pain Populations? A Systematic Review. Pain Phys. 2017;20(6):487–500. doi:10.36076/ppj.2017.20.5.487
9. Gupta A, Silman AJ, Ray D, et al. The role of psychosocial factors in predicting the onset of chronic widespread pain: results from a prospective population-based study. Rheumatology. 2007;46(4):666–671. doi:10.1093/rheumatology/kel363
10. Treede RD. The role of quantitative sensory testing in the prediction of chronic pain. Pain. 2019;160:S66–S69. doi:10.1097/j.pain.0000000000001544
11. Cruz-Almeida Y, Fillingim RB. Can quantitative sensory testing move us closer to mechanism-based pain management? Pain Med. 2014;15(1):61–72. doi:10.1111/pme.12230
12. Amiri M, Alavinia M, Singh M, Kumbhare D. Pressure Pain Threshold in Patients With Chronic Pain: a Systematic Review and Meta-Analysis. Am J Phys Med Rehabil. 2021;100(7):656–674. doi:10.1097/PHM.0000000000001603
13. Aoyagi K, He J, Nicol AL, et al. A Subgroup of Chronic Low Back Pain Patients With Central Sensitization. Clin J Pain. 2019;35(11):869–879. doi:10.1097/AJP.0000000000000755
14. Arendt-Nielsen L, Skou ST, Nielsen TA, Petersen KK. Altered Central Sensitization and Pain Modulation in the CNS in Chronic Joint Pain. Curr Osteoporos Rep. 2015;13(4):225–234. doi:10.1007/s11914-015-0276-x
15. Starkweather AR, Heineman A, Storey S, et al. Methods to measure peripheral and central sensitization using quantitative sensory testing: a focus on individuals with low back pain. Appl Nursing Res. 2016;29:237–241. doi:10.1016/j.apnr.2015.03.013
16. Varol U, Úbeda-D’Ocasar E, Cigarán-Méndez M, et al. Understanding the Psychophysiological and Sensitization Mechanisms behind Fibromyalgia Syndrome: a Network Analysis Approach. Pain Med. 2022. doi:10.1093/pm/pnac121
17. Potvin S, Marchand S. Pain facilitation and pain inhibition during conditioned pain modulation in fibromyalgia and in healthy controls. Pain. 2016;157(8):1704–1710. doi:10.1097/j.pain.0000000000000573
18. O’Brien AT, Deitos A, Trinanes Pego Y, Fregni F, Carrillo-de-la-Pena MT. Defective Endogenous Pain Modulation in Fibromyalgia: a Meta-Analysis of Temporal Summation and Conditioned Pain Modulation Paradigms. j Pain. 2018;19(8):819–836. doi:10.1016/j.jpain.2018.01.010
19. Geisser ME, Casey KL, Brucksch CB, Ribbens CM, Appleton BB, Crofford LJ. Perception of noxious and innocuous heat stimulation among healthy women and women with fibromyalgia: association with mood, somatic focus, and catastrophizing. Pain. 2003;102(3):243–250. doi:10.1016/s0304-3959(02)00417-7
20. Zanette SA, Dussan-Sania JA, Souza A, Deitos A, Torres ILS, Caumo W. Higher serum S100B and BDNF levels are correlated with a lower pressure-pain threshold in fibromyalgia. Mol Pain. 2014;10:46. doi:10.1186/1744-8069-10-46
21. Goubert D, Danneels L, Graven-Nielsen T, Descheemaeker F, Meeus M. Differences in Pain Processing Between Patients with Chronic Low Back Pain, Recurrent Low Back Pain, and Fibromyalgia. Pain Physician. 2017;20(4):307–318.
22. Kosek E, Clauw D, Nijs J, et al. Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system. Pain. 2021;162(11):2629–2634. doi:10.1097/j.pain.0000000000002324
23. Uddin Z, MacDermid JC. Quantitative Sensory Testing in Chronic Musculoskeletal Pain. Pain Med. 2016;17(9):1694–1703. doi:10.1093/pm/pnv105
24. Zhao SS, Holmes MV, Alam U. Disentangling the relationship between depression and chronic widespread pain: a Mendelian randomisation study. Semin Arthritis Rheum. 2023;60:152188. doi:10.1016/j.semarthrit.2023.152188
25. Wilson AT, Riley JL, Bishop MD, Beneciuk JM, Cruz-Almeida Y, Bialosky JE. Characteristics and Outcomes of Patients Receiving Physical Therapy for Low Back Pain with a Nociplastic Pain Presentation: a Secondary Analysis. Pain Res Manag. 2023;2023:5326261. doi:10.1155/2023/5326261
26. Miki T, Nishigami T, Takebayashi T, Yamauchi T. Association between central sensitivity syndrome and psychological factors in people with presurgical low back pain: a cross-sectional study. J Orthopaedic Sci. 2021;26(3):337–342. doi:10.1016/j.jos.2020.03.017
27. Demori I, Molinari E, Rapallo F, et al. Online Questionnaire with Fibromyalgia Patients Reveals Correlations among Type of Pain, Psychological Alterations, and Effectiveness of Non-Pharmacological Therapies. Healthcare. 2022;10(10):1975. doi:10.3390/healthcare10101975
28. Nijs J, Van Houdenhove B, Oostendorp RAB. Recognition of central sensitization in patients with musculoskeletal pain: application of pain neurophysiology in manual therapy practice. Man Ther. 2010;15(2):135–141. doi:10.1016/j.math.2009.12.001
29. Cayrol T, Draper-Rodi J, Fabre L, Pitance L, van den Broeke EN. Stuck in the Middle With You: why a Broad-Brush Approach to Defining Central Sensitization Does Not Help Clinicians and Patients. J Orthop Sports Phys Ther. 2021;51(5):204–206. doi:10.2519/jospt.2021.10340
30. van Griensven H, Schmid A, Trendafilova T, Low M. Central Sensitization in Musculoskeletal Pain: lost in Translation? J Orthop Sports Phys Ther. 2020;50(11):592–596. doi:10.2519/jospt.2020.0610
31. Shraim MA, Massé-Alarie H, Hodges PW. Methods to discriminate between mechanism-based categories of pain experienced in the musculoskeletal system: a systematic review. Pain. 2021;162(4):1007–1037. doi:10.1097/j.pain.0000000000002113
32. Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the central sensitization inventory. Pain Practice. 2012;12(4):276–285. doi:10.1111/j.1533-2500.2011.00493.x
33. Scerbo T, Colasurdo J, Dunn S, Unger J, Nijs J, Cook C. Measurement Properties of the Central Sensitization Inventory: a Systematic Review. Pain Pract. 2018;18(4):544–554. doi:10.1111/papr.12636
34. Neblett R, Cohen H, Choi Y, et al. The Central Sensitization Inventory (CSI): establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. j Pain. 2013;14(5):438–445. doi:10.1016/j.jpain.2012.11.012
35. Coronado RA, George SZ. The Central Sensitization Inventory and Pain Sensitivity Questionnaire: an exploration of construct validity and associations with widespread pain sensitivity among individuals with shoulder pain. Musculoskeletal Sci Practice. 2018;36:61–67. doi:10.1016/j.msksp.2018.04.009
36. Hendriks E, Voogt L, Lenoir D, Coppieters I, Ickmans K. Convergent Validity of the Central Sensitization Inventory in Chronic Whiplash-Associated Disorders; Associations with Quantitative Sensory Testing, Pain Intensity, Fatigue, and Psychosocial Factors. Pain Med. 2020;21(12):3401–3412. doi:10.1093/pm/pnaa276
37. Shigetoh H, Tanaka Y, Koga M, Osumi M, Morioka S. The Mediating Effect of Central Sensitization on the Relation between Pain Intensity and Psychological Factors: a Cross-Sectional Study with Mediation Analysis. Pain Res Manag. 2019;2019:3916135. doi:10.1155/2019/3916135
38. Wolfe F, Clauw DJ, Fitzcharles MA, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol. 2011;38(6):1113–1122. doi:10.3899/jrheum.100594
39. Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
40. Brummett CM, Goesling J, Tsodikov A, et al. Prevalence of the fibromyalgia phenotype in patients with spine pain presenting to a tertiary care pain clinic and the potential treatment implications. Arthritis Rheum. 2013;65(12):3285–3292. doi:10.1002/art.38178
41. Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940–2952. doi:10.1097/00007632-200011150-00017
42. Fairbank JC, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;66(8):271–273.
43. Beaton DE, Wright JG, Katz JN. Development of the QuickDASH: comparison of three item-reduction approaches. J Bone Joint Surg Am. 2005;87(5):1038–1046. doi:10.2106/jbjs.d.02060
44. Kennedy CA, Beaton DE, Smith P, et al. Measurement properties of the QuickDASH (disabilities of the arm, shoulder and hand) outcome measure and cross-cultural adaptations of the QuickDASH: a systematic review. Quality Life Res. 2013;22(9):2509–2547. doi:10.1007/s11136-013-0362-4
45. Radloff LS. The CES-D scale: a self report depression scale for research in the general population. Appl Psychol Measurements. 1977;1(3):385–401. doi:10.1177/014662167700100306
46. Thombs BD, Hudson M, Schieir O, Taillefer SS, Baron M; Canadian Scleroderma Research Group. Reliability and validity of the center for epidemiologic studies depression scale in patients with systemic sclerosis. Arthritis Rheum. 2008;59(3):438–443. doi:10.1002/art.23329
47. McNeil DW, Kennedy SG, Randall CL, et al. Fear of Pain Questionnaire-9: brief assessment of pain-related fear and anxiety. Eur J Pain. 2018;22(1):39–48. doi:10.1002/ejp.1074
48. Bishop SMJ, Pivik SR. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
49. Osman A, Barrios FX, Kopper BA, Hauptmann W, Jones J, O’Neill E. Factor structure, reliability, and validity of the Pain Catastrophizing Scale. J Behav Med. 1997;20(6):589–605. doi:10.1023/A:1025570508954
50. Waddell G, Newton M, Henderson I, Somerville D, Main CJ. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52(2):157–168. doi:10.1016/0304-3959(93)90127-B
51. Mintken PE, Cleland JA, Whitman JM, George SZ. Psychometric properties of the Fear-Avoidance Beliefs Questionnaire and Tampa Scale of Kinesiophobia in patients with shoulder pain. Arch Phys Med Rehabil. 2010;91(7):1128–1136. doi:10.1016/j.apmr.2010.04.009
52. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the Tampa Scale for Kinesiophobia. Pain. 2005;117(1–2):137–144. doi:10.1016/j.pain.2005.05.029
53. McCracken LM, Dhingra L. A short version of the Pain Anxiety Symptoms Scale (PASS-20): preliminary development and validity. Pain Res Manag. 2002;7(1):45–50. doi:10.1155/2002/517163
54. Coons MJ, Hadjistavropoulos HD, Asmundson GJG. Factor structure and psychometric properties of the Pain Anxiety Symptoms Scale-20 in a community physiotherapy clinic sample. Eur J Pain. 2004;8(6):511–516. doi:10.1016/j.ejpain.2003.11.018
55. Nicholas MK. The pain self-efficacy questionnaire: taking pain into account. Eur j Pain. 2007;11(2):153–163. doi:10.1016/j.ejpain.2005.12.008
56. Zicarelli CAM, Santos JPM, Poli-Frederico RC, et al. Reliability of pressure pain threshold to discriminate individuals with neck and low back pain. J Back Musculoskelet Rehabil. 2020. doi:10.3233/BMR-181208
57. Waller R, Straker L, O’Sullivan P, Sterling M, Smith A. Reliability of pressure pain threshold testing in healthy pain free young adults. Scand J Pain. 2015;9(1):38–41. doi:10.1016/j.sjpain.2015.05.004
58. Tabatabaiee A, Takamjani IE, Sarrafzadeh J, Salehi R, Ahmadi M. Pressure Pain Threshold in Subjects With Piriformis Syndrome: test-Retest, Intrarater, and Interrater Reliability, and Minimal Detectable Changes. Arch Phys Med Rehabil. 2020;101(5):781–788. doi:10.1016/j.apmr.2019.10.194
59. Simon CB, Lentz TA, Ellis L, et al. Static and Dynamic Pain Sensitivity in Adults With Persistent Low Back Pain: comparison to Healthy Controls and Associations With Movement-evoked Pain Versus Traditional Clinical Pain Measures. Clin J Pain. 2021;37(7):494–503. doi:10.1097/ajp.0000000000000945
60. Yarnitsky D, Bouhassira D, Drewes AM, et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Eur J Pain. 2015;19(6):805–806. doi:10.1002/ejp.605
61. Rabey M, Kendell M, Koren S, et al. Do chronic low back pain subgroups derived from dynamic quantitative sensory testing exhibit differing multidimensional profiles? Scandinavian j Pain. 2021;21(3):474–484. doi:10.1515/sjpain-2020-0126
62. C J. Statistical Power Analysis for the Behavioral Sciences.
63. Neville SJ, Clauw AD, Moser SE, et al. Association Between the 2011 Fibromyalgia Survey Criteria and Multisite Pain Sensitivity in Knee Osteoarthritis. Clin J Pain. 2018;34(10):909–917. doi:10.1097/AJP.0000000000000619
64. Adams GR, Gandhi W, Harrison R, et al. Do “central sensitization” questionnaires reflect measures of nociceptive sensitization or psychological constructs? A systematic review and meta-analyses. Pain. 2023;164(6):1222–1239. doi:10.1097/j.pain.0000000000002830
65. Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010;62(5):600–610. doi:10.1002/acr.20140
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Central Sensitization and Nociplastic Pain: Shared Mechanisms in Fibromyalgia, Osteoarthritis, and Inflammatory Arthritis
Hladkykh FV, Liadova TI, Matvieienko MS, Komorovsky R, Smiyan S, Student V
Journal of Pain Research 2026, 19:571311
Published Date: 26 March 2026
The Emotional Allodynia Questionnaire: Preliminary Validation and Clinical Phenotyping in Fibromyalgia
Corriero A, Giglio M, Pilolla A, Galdini F, Mucci O, Vurro M, Fornarelli F, Di Venosa C, Trerotoli P, Puntillo F
Journal of Pain Research 2026, 19:607309
Published Date: 3 June 2026