Back to Journals » Clinical Epidemiology » Volume 17
The Association Between Socioeconomic Position and Infection Risk After Hip Fracture Surgery: A Nationwide Cohort Study of 54,853 Patients
Authors Gadgaard NR ![]() , Varnum C
, Varnum C ![]() , Nelissen R
, Nelissen R ![]() , Vandenbroucke-Grauls C, Sørensen HT
, Vandenbroucke-Grauls C, Sørensen HT ![]() , Pedersen AB
, Pedersen AB ![]()
Received 16 May 2025
Accepted for publication 1 November 2025
Published 15 November 2025 Volume 2025:17 Pages 953—965
DOI https://doi.org/10.2147/CLEP.S540994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Ahern
Nadia Roldsgaard Gadgaard,1 Claus Varnum,2,3 Rob Nelissen,4 Christina Vandenbroucke-Grauls,1,5 Henrik Toft Sørensen,1 Alma Becic Pedersen1
1Department of Clinical Epidemiology, Center for Population Medicine, Aarhus University Hospital and Aarhus University, Aarhus, Denmark; 2Department of Orthopedic Surgery, Lillebaelt Hospital, Vejle, Denmark; 3Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 4Department of Orthopaedics, Leiden University Medical Center, Leiden, the Netherlands; 5Department of Medical Microbiology and Infection Control, Amsterdam University Medical Center, Amsterdam, the Netherlands
Correspondence: Nadia Roldsgaard Gadgaard, Department of Clinical Epidemiology, Center for Population Medicine, Aarhus University Hospital and Aarhus University, Olof Palmes Allé 43-45, Aarhus N, 8200, Denmark, Tel +45 8716 7212, Email [email protected]; [email protected]
Purpose: We examined the association between socioeconomic position (SEP) and risk of any infection after surgery for hip fracture, and whether markers of poor health modify this.
Methods: Individual-level data on SEP markers (education, liquid assets, marital status, and cohabitation) were obtained from Danish registries for hip fracture patients undergoing surgery (2010– 2018). We computed cumulative incidences of any hospital-treated infection within one month after surgery. Using Cox regression we estimated adjusted hazard ratios (aHRs) with 95% confidence intervals. Analyses were stratified by comorbidity clusters based on latent class analysis, body mass index (BMI), pre-fracture mobility, and residence type.
Results: The incidences of infection were: 17% for low vs 16% for high education (aHR 1.10, 1.02– 1.18), 19% for low vs 16% for high liquid assets (aHR 1.21, 1.15– 1.28), 18% for divorced vs 16% for married (aHR 1.24, 1.15– 1.32), and 18% for living alone vs 15% for cohabiting (aHR 1.16, 1.06– 1.28). The incidence of infection was highest among patients with diabetic-renal comorbidity, underweight, poor mobility, or nursing home residency. The magnitude and direction of associations were modified by comorbidity clusters, BMI, mobility, and residence type.
Conclusion: We observed socioeconomic inequalities in 30-day risk of infection after hip fracture surgery. Health modified the observed inequalities but could not fully explain them.
Keywords: (MeSH), Epidemiology, Hip fractures, Infections, Low Socioeconomic Status
Introduction
Infections are among the most frequent complications and causes of mortality after hip fracture surgery.1 Within 30 days after surgery 15% of patients are treated in hospital for infection.2 The 30-day mortality is 15% among patients who develop any type of infection, compared to 8% among patients without infection.3
Social inequalities persist in healthcare utilization and outcomes in welfare states, meaning health status or access to health differs dependent on the social conditions in which people live. To measure social conditions, social determinants such as education, income, or other markers of socioeconomic position are used. Low socioeconomic position (SEP) is associated with higher risk of hip fracture and subsequent elevated mortality.4,5 Furthermore, in recent study, a worryingly temporal trend of increase in social inequality in risk of infection after hip fracture surgery from 2012 to 2021 was observed.6 A better understanding of the interplay between mediating factors is needed to identify subgroups with the highest infection risk after hip fracture to guide targeted preventive measures and treatment of infection in these vulnerable patients.
Low SEP is associated with risk factors for infection such as comorbidity, frailty, and adverse lifestyle factors.7,8 Studies have reported that the effects of low SEP on outcome may be partially mediated through lifestyle factors and comorbidities9 and that an interaction effect between SEP and comorbidity on health outcomes exists.10 We therefore aimed to examine infection risk in the first month after hip fracture surgery in patients of different SEP and whether the risk is modified in subgroups of different health, as measured by comorbidity, body mass index (BMI), pre-fracture mobility, and type of residence.
Materials and Methods
Study Population
This cohort study utilized health registries in Denmark, a Scandinavian country with approximately 5.9 million residents as of 2023. Danish residents have access to tax-supported healthcare, including general practitioners and hospitals.
Patients aged ≥65 years who underwent surgery for a first unilateral hip fracture between 2010 and 2018 were identified in the Danish Multidisciplinary Hip Fracture Registry (DMHFR)11 The DMHFR contains information on patient- and surgery-related factors, in-hospital quality indicators, and outcomes.
All Danish residents are registered with a unique 10-digit personal identifier, enabling linkage of data across Danish health registries on the individual level.12
Markers of Socioeconomic Position
SEP can be estimated using several proxies. These proxies or markers are highly correlated but cannot be used interchangeably. It is therefore recommended to use several markers13 To investigate underlying effect of individual proxies, we utilized several data sources to obtain individual-level information on four SEP markers separately.
- Educational level as of the surgery year, as recorded in the Population Education Registry.14 Educational level was categorized into low (elementary school), medium (more than elementary school but less than university), high (university), or none/unknown (persons who lacked records in the registry, which can either be due to not completing an education or due to a missing registration).
- Information on family liquid assets (ie, bank account holdings, property, stocks) was obtained from the Income Statistics Registry.15 For each patient, we calculated the mean liquid assets for the past 5 years. Subsequently, we categorized patients into low, medium, or high liquid asset groups, based on tertiles.
- Marital status as of the surgery year was ascertained from the Danish Civil Registration system.12 Patients were categorized as married, divorced, never married, or widowed.
- Living arrangement as of the surgery year was based on the combination of cohabitation status and type of residence obtained from the Danish Civil Registration System and the DMHFR. Living arrangement was categorized as: cohabiting (in own home), living alone (in own home), living in a nursing home, or other (ie, multiple-family cohabiting, homelessness, or missing values).
Infection
The primary outcome was any hospital-treated infection within 30 days following hip fracture surgery, defined according to International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes in the Danish National Patient Registry (DNPR).16
To capture less severe infections treated outside the hospital setting, a secondary outcome of community-treated infection was defined as redemption of a prescription for systemic antibiotics from a community pharmacy, using Anatomical Therapeutic Chemical Classification System (ATC) codes in the Danish National Prescription Registry.17
Potential Effect Measure Modifiers
Four variables, as markers of health, were investigated as potential effect modifiers.7,8
- Comorbidity clusters identified through latent class analysis using records of 27 selected comorbidity diagnoses with a prevalence >1% in the 10 years before the surgery date (See Supplementary Methods S1 and Supplementary Tables S1–S3). This enabled classification of patients into clusters to overcome limitations of the more commonly used comorbidity indices, for example, the individual comorbid diseases’ importance as predictors of infection.18,19 All patients were classified into one of six clusters labelled Healthy, Cardiac-Pulmonary, Cerebro-Vascular, Hepatic-Psychological-Neurological, Diabetic-Renal, and Malignancy.
- Body Mass Index (BMI) at the time of hospital admission was obtained from the DMHFR. BMI was categorized into underweight (BMI < 19 kg/m2), normal (BMI 19–24.9 kg/m2), overweight (including obese and extremely obese) (BMI ≥ 25 kg/m2), and outliers (BMI < 10 or >50 kg/m2).
- Pre-fracture mobility was ascertained from the DMHFR based on the cumulated ambulation score (CAS). Pre-fracture mobility was categorized as poor (CAS 0–4) or good (CAS 5–6) mobility.
- Type of residence was collected from the DMHFR and defined as living in nursing home or in own home.
Additional Variables
We captured information on the following variables:
- Patients’ sex and age on the surgery date, collected from the Danish Civil Registration System. We defined three age groups (65–74 years, 75–84 years, and ≥85 years).
- Surgery year, hip fracture type, surgery, mean surgery delay time (hours), and mean length of hospital stay (days) retrieved from the DMHFR.
- Retirement status in the year prior to surgery year was obtained from the Integrated Database for Labour Market Research.
Statistics
We analyzed any hospital-diagnosed infection and any community-treated infection separately. Patients were followed from the date of hip fracture surgery until outcome of interest, migration, death, end of study period (31 December 2018) or 30 days from the surgery date, whichever came first.
We used the Gray method for calculating crude cumulative incidences of infections taking account of the competing risk of death.
We used cause specific Cox proportional hazard regression to estimate crude and adjusted hazard ratios (HRs) of infections, comparing patients with lower SEP to those with high SEP, for example, comparing low educational level to high educational level. Competing risk was handled using censoring at outcome, death, emigration, end of study, end of follow up, or end of study. We choose this method over Fine & Grey regression due to causal rather than predictive nature of our study Assumption of proportionality was evaluated visually using log(-log) plots and found acceptable.
Directed Acyclic Graphs (DAGs) were used to identify possible confounders (Supplementary Figure S1). Variables included in the models for confounder adjustment were chosen for each marker of SEP separately taking topological ordering of the SEP markers into account to minimize overadjustment. Thus, variables included in the adjusted models had to fulfill all three properties of a confounding factor: 1) must be associated with the exposure, 2) must be associated with the outcome, and 3) must not be on the causal pathway from the exposure to the outcome.
To evaluate potential modified effects in subgroups of different health, we performed analyses stratified by comorbidity clusters, BMI, pre-fracture mobility, and residence for the primary outcome.
All estimates are presented with a 95% confidence interval (95% CI).
This paper follows guidelines for cohort studies as described in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). Analyses were performed using R software (version 4.3.1).
Diagnosis and prescription codes used in this study are provided in Supplementary Tables A1–A3.
Results
Patient Characteristics
Of the 54,853 patients with hip fracture, median age 83, the majority were women (70%). Many patients had low education (50%), were widowed (49%), and were living alone (39%). Liquid assets ranged from a mean of 7,878 USD in the lowest tertile group to a mean of 496,362 USD in the highest tertile group (Table 1).
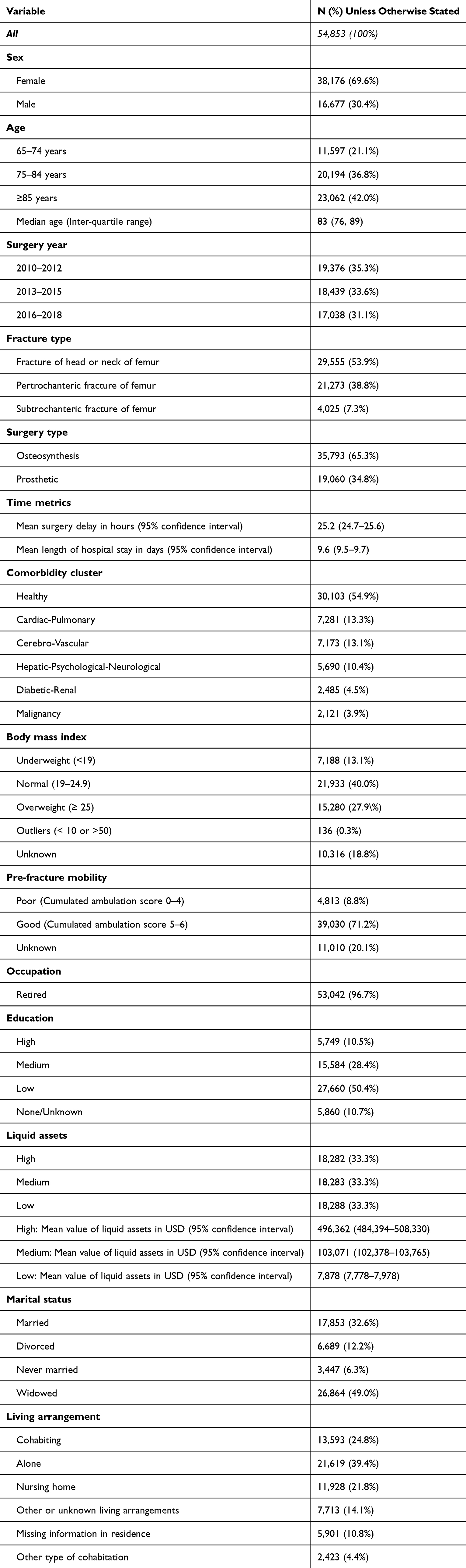 |
Table 1 Characteristics of the Total Cohort, Denmark, 2010–2017 |
Patients of lower SEP within each of the four markers had higher proportion of women, a higher median age, and higher level of comorbidity than those of high SEP, with those divorced being the only exception with lower median age (Figure 1).
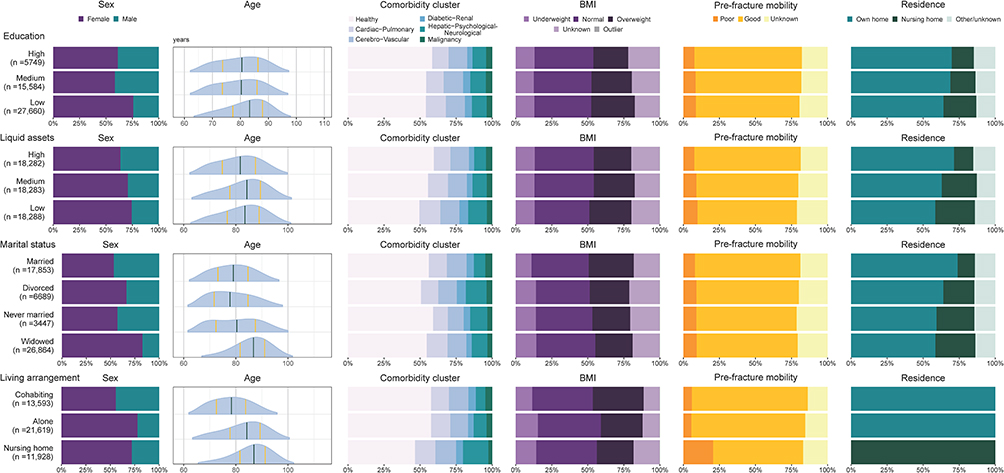 |
Figure 1 Age, sex, comorbidity-cluster, body mass index (BMI), pre-fracture mobility and residence distributions by markers of socioeconomic position. |
The proportion of patients living in nursing homes and the proportion of those with poor pre-fracture mobility was higher among patients with lower SEP compared to patients with high SEP. A higher BMI was more frequent among patients with lower education, fewer liquid assets, but also among patients with supportive marital status and living arrangement (Figure 1).
Any Hospital-Treated Infection
The highest 30-day cumulative incidences of any hospital-treated infection were observed among patients with a low education (17%), low liquid assets (19%), who were divorced (18%), and living in nursing homes (18%) (Figure 2 and Supplementary Table S4). Overall, of the 9,295 patients with an incident hospital-treated infection within 30 days after surgery, 38% had pneumonia, 38% had urinary tract infection, and 3% had a surgical site infection. Comparing SEP levels, there was minor variation in the distribution of infection types, but with no clear pattern.
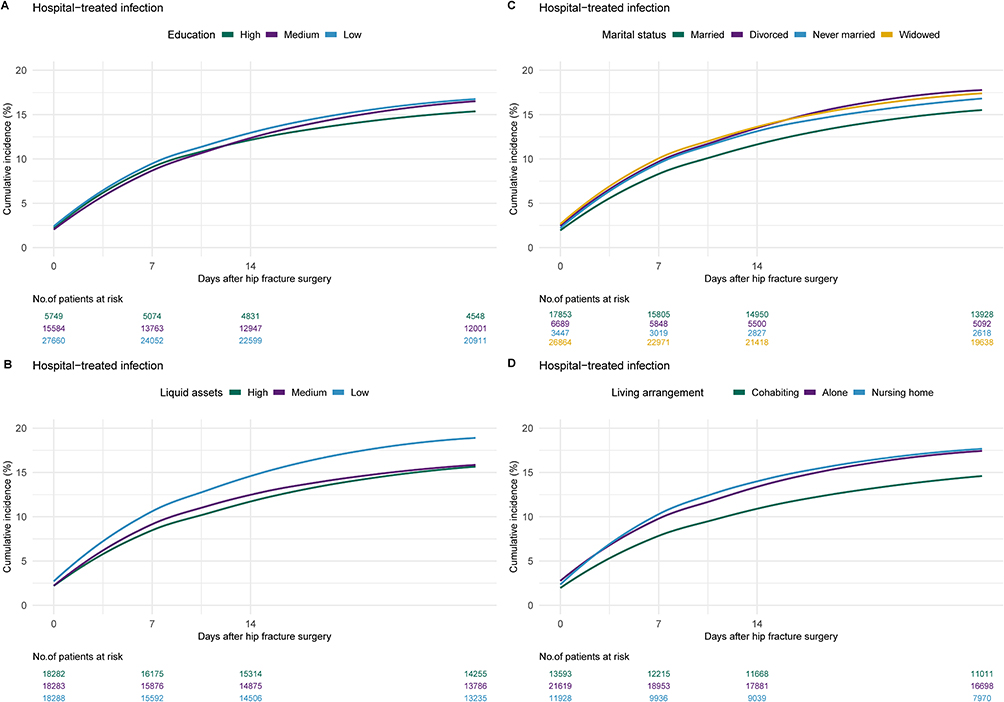 |
Figure 2 Plots of cumulative incidences of hospital-treated infection over time up to 30 days after date of surgery by (A) education, (B) liquid assets, (C) marital status, and (D) living arrangement. |
We observed an association between all four markers of low SEP and risk of any hospital-treated infection within 30 days of surgery. The highest adjusted HRs were 1.10 (95% CI: 1.02–1.18) for low education versus high, 1.21 (95% CI: 1.15–1.28) for low liquid assets versus high assets, 1.24 (95% CI 1.15–1.32) for divorced compared to married, and 1.18 (95% CI: 1.06–1.30) for living alone compared to cohabiting (Figure 3 and Supplementary Table S4).
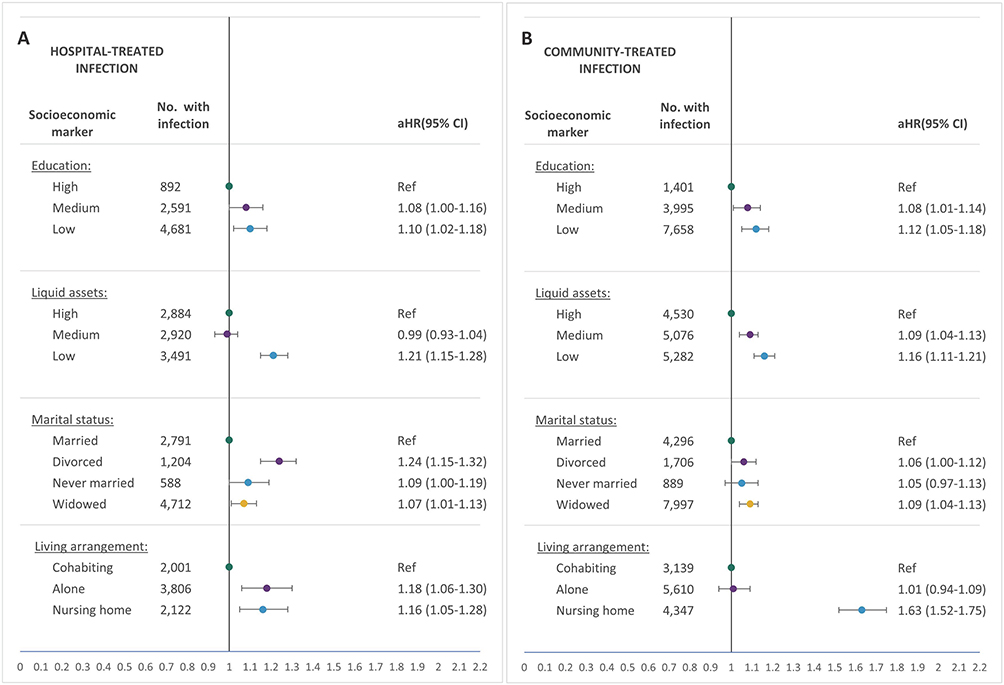 |
Figure 3 Forest plots of adjusted hazard ratios (aHRs) for (A) hospital-treated infection or (B) community-treated infection by socioeconomic markers: Education adjusted by age, sex, and surgery year. Liquid assets adjusted by age, sex, surgery year, education, marital status, and comorbidity cluster. Marital status adjusted by age, sex, surgery year, and education. Living arrangements adjusted by age, sex, surgery year, education, marital status, comorbidity cluster, liquid assets, body mass index, and pre-fracture mobility. |
Community-Treated Infection
The 30-day cumulative incidences of community-treated infection were higher than those for hospital-treated infection. The highest cumulative incidences of community-treated infection were observed for patients with a low educational level (28%), low liquid assets (29%), those who were widowed (30%), and in particular among those in nursing homes (36%) (Supplementary Table S5).
We observed an association between all four markers of low SEP and risk of community-treated infection within 30 days of surgery. The highest adjusted HRs were 1.12 (95% CI: 1.05–1.18) for low education versus high, 1.16 (95% CI: 1.11–1.21) for low liquid assets versus high, 1.09 (95% CI 1.04–1.13) for widowed compared married, and 1.63 (95% CI: 1.52–1.75) for living in nursing homes compared to cohabiting (Figure 3 and Supplementary Table S5).
Pre-Fracture Comorbidity, BMI, Mobility, and Residence as Effect Measure Modifiers
Cumulative incidences of hospital-treated infection were highest among patients who were in the Diabetes-Renal cluster, were underweight, had poor mobility, and were living in nursing homes (Supplementary Tables S6 and S7).
Comparing cumulative incidences, risk differences were higher between strata of poor vs good health than between SEP levels within each stratum. Additionally, risk differences between high and low SEP marker were similar across all strata (Supplementary Tables S6 and S7).
The degree of association between the four SEP markers and risk of hospital-treated infection varied by strata, indicating effect modification. An association between low SEP and increased risk of was observed among patients in the “Healthy” cluster, whereas no clear pattern of association was observed for patients in the 5 other comorbidity clusters.
For example, an association was observed between non-married status and increased risk of hospital-treated infection in the Cerebro-Vascular cluster but the inverse association was observed in the Hepatic-Psychological-Neurological cluster (Figure 4 and Supplementary Table S8).
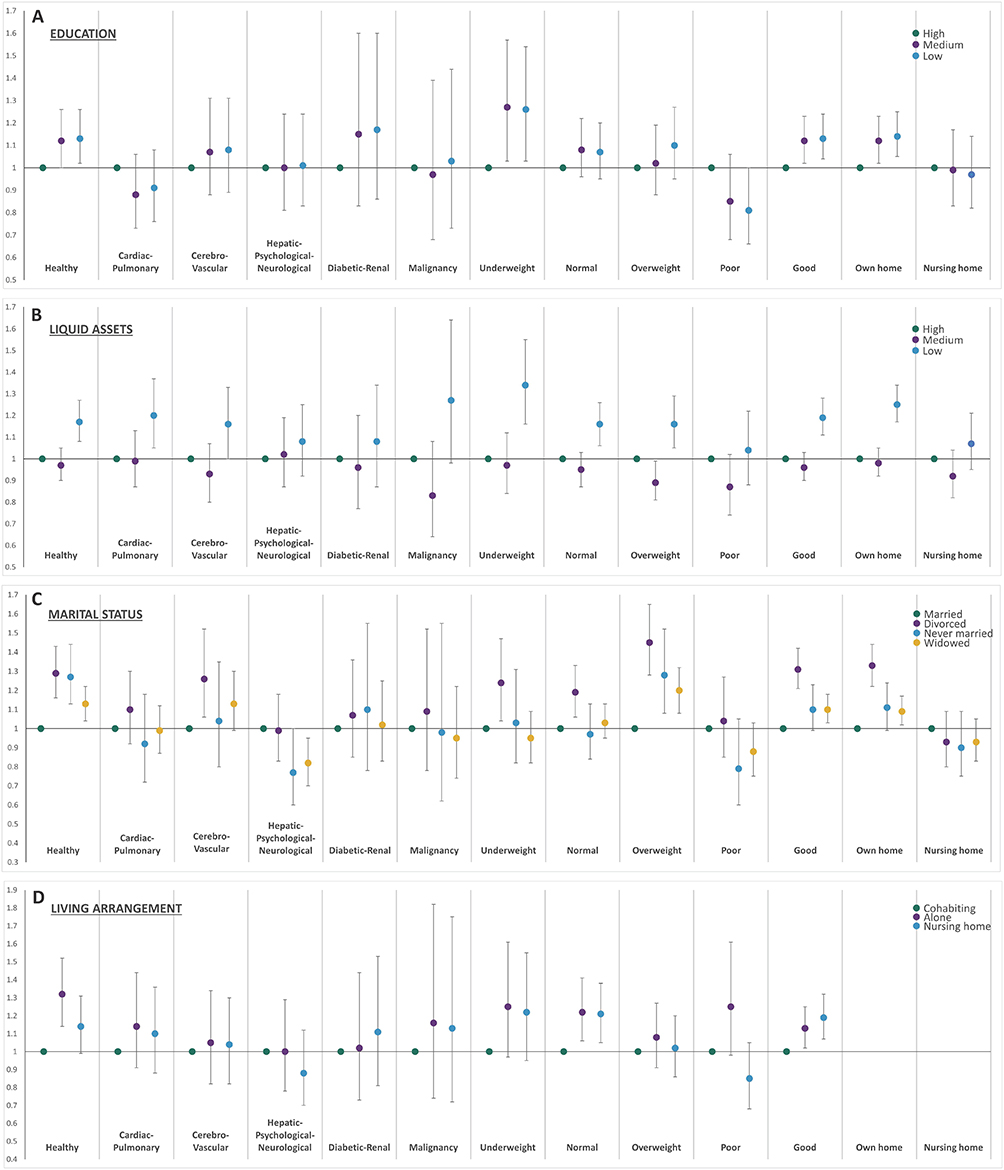 |
Figure 4 Plots of adjusted hazard ratios for hospital-treated infection stratified by comorbidity clusters, body mass index, pre-fracture mobility, and residence type. According to (A) education adjusted by age, sex, and surgery year; (B) liquid assets adjusted by age, sex, surgery year, education, marital status, and comorbidity cluster; (C) marital status adjusted by age, sex, surgery year, and education; and (D) living arrangement adjusted by age, sex, surgery year, education, marital status, comorbidity cluster, liquid assets, body mass index, and pre-fracture mobility. |
Pre-fracture mobility, and to a lesser degree BMI, appeared to modify the association between all four SEP markers and risk of hospital-treated infection. Residence appeared to especially modify the association between marital status and hospital-treated infection (Figure 4 and Supplementary Table S9).
Discussion
In this nationwide cohort study, markers of lower SEP (education, liquid assets, marital status, and living arrangements) were associated with increased risk of infection within 30 days of surgery for hip fracture, with comorbidity, BMI, pre-fracture mobility, and nursing home residence modifying the associations.
Interpretation
Low health literacy, associated to low educational level, may partly explain the observed inverse association between education and infection risk through reduced compliance and abilities to comprehend, communicate, and navigate within health-related settings.20 Hip fracture patients may be particularly vulnerable to health illiteracy due to advanced age and added stressors.20 Of further explanation, previous studies report associations between markers of SEP, such as education, and comorbidity and adverse health behaviours.9,21 As educational level usually is established by early adulthood, the cumulative effects of education over a lifespan could introduce survival bias, which could explain the lack of association, for example, in the Cardiac-Pulmonary cluster.
Patients with low assets may struggle to afford transportation to healthcare providers, medications, proper housing, rehabilitation, or social services, contributing to infection risk. Not all healthcare in Denmark is covered by the public sector and additional healthcare may be provided privately. Low liquid assets was not a risk factor among those living in nursing homes, which could be due to higher public sector coverage of healthcare and social services in these patients compared to those living in their own home.
Both cohabitation and marital status could be considered proxies for social support or informal caregiving. Although all patients in Denmark are eligible to receive formal care after hip fracture surgery both inside and outside the hospital setting, most patients rely heavily on informal care from family members or friends.22
In orthopedic and geriatric patients, lower social support is associated with impeded recovery, failure to regain pre-surgical physical function, and outcomes such as infection.23,24 Non-cohabiting or unmarried status could lead to increased risk of severe infections due to delays in contacting healthcare providers. An association between unmarried status and delay in diagnosing community-acquired infection has been observed in other patient groups.25,26 However, unmarried patients could have an increased likelihood of hospital admission if healthcare personnel consider social support when deciding between hospital or community treatment.
Social support may also be provided by a non-married partner or children but we were unable to account for these situations.
Although the presence of comorbidity, poor pre-fracture mobility, underweight BMI, and living in a nursing home could indicate a higher dependence on informal care, these factors might also be associated with receiving more formal care. This may explain why the association between marital status and any hospital-treated infection was clearer among those healthy, overweight, with good mobility, and living in their own home.
Although studies suggest an association between lack of social support and nursing home residency, we considered nursing home residency mostly a marker of vulnerability.27 Risk factors for developing infection such as dysphagia, compromised immune response, or close living quarters are common among nursing home populations, which would explain the high cumulative incidence of infection we observed.28 The competing risk of death and clinical decisions on level of care might have impacted these results, particularly, as the subpopulation living in nursing homes was elderly and comorbid.29 Such competing risks may also explain the negative association observed in some strata, for example, as observed for nursing home residents with poor mobility.
Perspectives
Though the examined markers of SEP are non-modifiable, knowledge about their association with infection may help to identify vulnerable patient subgroups, indicate effective early interventions, or aid the prevention of severe infection. The aHRs ranging from 1.10 to 1.24 with small absolute differences between SEP groups are statistically significant but may raise questions of clinical relevance of our results. However, patients with lower SEP combined with poorer health should be considered a particular vulnerable subgroup with highest absolute risks of infection after hip fracture and thereby possible highest risk of mortality.1,3 Thus, clinical practice and future studies on the benefits of interventions to reduce high risk of infection after hip fracture surgery could be focused on multidisciplinary and individualised care, including support from the primary medical and social sectors among patients with lower SEP. For example, an intervention with patient-tailored programs where infection preventive measures are combined with high-quality information and caregiver involvement30 or an intervention with oral nutritional supplementation31 might be considered in patients with lower education. Meanwhile, additional focus on transitional and home care could be considered for patients with no informal caregivers, as early transitional care has been shown to lower readmission risk in geriatric patients. However, the preferrable type, effectiveness, and cost-benefit of transitional care remain under debate.32 Previous studies reported no association between SEP and in-hospital care of hip fracture patients in Denmark.4 However, we found modest inequality between SEP and infection risk. This gap between care and patient outcome should be addressed, especially considering the increase in inequality of infection risk previously reported.6 The potential preventive and treatment interventions in-hospital and in the transition between the hospital and home settings after hip fracture surgery should be taking patient health into account, as well as differences in healthcare systems and healthcare accessibility.
Methodological Considerations
We analyzed separate markers representing different aspects of SEP to capture independent effects.13 While a composite SEP score considers interactions between markers, it can be challenging to interpret due to equal weighting of markers with varying effects. As a result, many patients have medium composite SEP scores, combining different low and high SEP markers.
It is unknown whether we capture all patients surgically treated for hip fracture. Hospitals have legal and economic incentives to report hip fracture patients to the DNPR, source for the DMHFR, therefore the completeness of the DMHFR is considered very high.
We excluded 11% of cohort members due to missing data on education, most likely missing because patients never finished primary school. Because the data was not missing at random, we did not perform multiple imputations.
A positive predictive value (PPV) of 100% has been reported for hip fracture in the DMHFR. Misclassification is considered low for data on marital status, cohabitation, and liquid assets, as these data are maintained by major government registries and used by civil agencies. The PPV for residence as reported in the DMHFR is unknown.
Education is expected to be misclassified for minimum 3% of the observations.14 In the DNPR, a PPV of 98% for any infection was reported for a sample of cancer patients,33 while a PPV of 78% was reported for infection diagnoses in the emergency room.34 PPVs ranging from 82% to 100% have been reported for a majority of the diagnoses used in the cluster analysis.
SEP and health status change over a life course, and reciprocal relationships exist between these factors.35 We considered this and time of measurement for possible confounders. For example, education is usually established by early adulthood and therefore was considered a confounder for the remaining SEP markers. However, it is difficult to assess which was established first: a person’s accumulated poor health or accumulated liquid assets. Therefore, the variables included in the final models were chosen based on current literature and expert knowledge of the authors but also relies on some assumptions.
We did not have data on lifestyle factors such as smoking, alcohol use, nutrition, and functional status beyond pre-fracture mobility that might play a role in terms of sustaining infection postoperatively. However, while this data is important, they are not fulfilling the confounding criteria; thus, they are mediators (on the clinical pathway from exposure to outcome) and as such, should not be included in regression model.
Conclusion
Living alone or in a home, being unmarried, having low liquid assets, and low education were associated with a higher infection risk in the first month after hip fracture surgery. Pre-fracture comorbidity, mobility, BMI, and type of residence modified the magnitude of effect, in particular of marital status and living arrangement.
Abbreviations
ATC, Anatomical Therapeutic Chemical classification System; BMI, Body mass index; CI, Confidence interval; DAGs, Directed acyclic graphs; DMHFR, The Danish Multidisciplinary Hip Fracture Registry; DNPR, The Danish National Patient Registry; HR, Hazard ratio; ICD-10, International Classification of Diseases Tenth Revision; PPV, Positive predictive value; SEP, Socioeconomic position; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; USD, US dollars.
Data Sharing Statement
To protect the privacy of patients, it is by Danish law prohibited to make individual-level data publicly available.
Ethics and Registration
The study was reported to the Danish Data Protection Agency through registration at Aarhus University (record number: AU-2016-051-000001, sequential number 880). Patient consent is not required by Danish law for registry-based studies.
Acknowledgments
The Department of Clinical Epidemiology, Aarhus University, receives funding for other studies from companies in the form of research grants to (and administered by) Aarhus University. None of those studies have any relation to the present study.
The abstract of this paper was presented at the 6th Annual Research Meeting at the Dept. of Clinical Medicine Aarhus University 2023 and at the Danish Orthopedic Society Congress 2024, both as a conference talks with interim findings. The abstract was published in “DOS Abstracts” on the website of the Danish Orthopedic Society.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Helsefonden (grant number 20-B-0140); Helga og Peter Kornings Fond; Frimodt-Heineke Fonden; and the Department of Clinical Medicine at Aarhus University, Denmark. The sponsors had no role in the design, data collection, analysis, interpretation, or submission of the study.
Disclosure
CV received travel expenses from Stryker with no relevance to the present study. The authors report no other conflicts of interest in this work.
References
1. Rohold CK, Lauritzen JB, Jørgensen HL. Causes of death among 93.637 Hip fracture patients- data based on the Danish National Registry of causes of death. Eur J Trauma Emerg Surg. 2021;48:1861–1870. doi:10.1007/s00068-021-01791-0
2. Gadgaard NR, Varnum C, Nelissen R, Vandenbroucke-Grauls C, Sørensen HT, Pedersen AB. Comorbidity and risk of infection among patients with Hip fracture: a Danish population-based cohort study. Osteoporos Int. 2023;34:1739–1749. doi:10.1007/s00198-023-06823-6
3. Kjørholt KE, Kristensen NR, Prieto-Alhambra D, Johnsen SP, Pedersen AB. Increased risk of mortality after postoperative infection in hip fracture patients. Bone. 2019;127:563–570. doi:10.1016/j.bone.2019.07.023
4. Kristensen PK, Thillemann TM, Pedersen AB, Søballe K, Johnsen SP. Socioeconomic inequality in clinical outcome among hip fracture patients: a nationwide cohort study. Osteoporos Int. 2017;28(4):1233–1243. doi:10.1007/s00198-016-3853-7
5. Valentin G, Ravn MB, Jensen EK, et al. Socio-economic inequalities in fragility fracture incidence: a systematic review and meta-analysis of 61 observational studies. Osteoporos Int. 2021;32(12):2433–2448. doi:10.1007/s00198-021-06038-7
6. Gadgaard NR, Varnum C, Nelissen R, Vandenbroucke-Grauls C, Pedersen AB. Temporal trends in socioeconomic inequalities and risk of infection after hip fracture surgery: a nationwide cohort study, 2010–2021. Osteoporos Int. 2025. doi:10.1007/s00198-025-07576-0
7. Trevisan C, Noale M, Amidei CB, et al. Frailty and the risk of infection-related hospitalizations in older age: differences by sex. Maturitas. 2023;168:1–6. doi:10.1016/j.maturitas.2022.10.009
8. Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. 2018;42(2):186–194. doi:10.1111/1753-6405.12762
9. Petrovic D, de Mestral C, Bochud M, et al. The contribution of health behaviors to socioeconomic inequalities in health: a systematic review. Prev Med. 2018;113:15–31. doi:10.1016/j.ypmed.2018.05.003
10. Chen YH, Karimi M, Mölken M R-V. The disease burden of multimorbidity and its interaction with educational level. PLoS One. 2020;15(12):e0243275. doi:10.1371/journal.pone.0243275
11. Hjelholt TJ, Edwards NM, Vesterager JD, Kristensen PK, Pedersen AB. The positive predictive value of hip fracture diagnoses and surgical procedure codes in the Danish multidisciplinary hip fracture registry and the Danish National Patient Registry. Clin Epidemiol. 2020;12:123–131. doi:10.2147/clep.S238722
12. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
13. Geyer S, Hemström O, Peter R, Vågerö D. Education, income, and occupational class cannot be used interchangeably in social epidemiology. Empirical evidence against a common practice. J Epidemiol Community Health. 2006;60(9):804–810. doi:10.1136/jech.2005.041319
14. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–94. doi:10.1177/1403494810394715
15. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. doi:10.1177/1403494811405098
16. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/clep.S91125
17. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798–798f. doi:10.1093/ije/dyw213
18. Storbjerg DK, Gadgaard NR, Pedersen AB. Any infection among patients with hip fracture: predictive ability of Charlson, Elixhauser, Rx-Risk, and Nordic comorbidity indices. Surgeon. 2024;22(1):e61–e68. doi:10.1016/j.surge.2023.11.004
19. Gadgaard NR, Varnum C, Nelissen R, Vandenbroucke-Grauls C, Sørensen HT, Pedersen AB. Major comorbid diseases as predictors of infection in the first month after Hip fracture surgery: a population-based cohort study in 92,239 patients. Eur Geriatr Med. 2024;15:1069–1080. doi:10.1007/s41999-024-00989-w
20. Holmes M, Bacon TJ, Dobson LA, et al. Addressing health literacy through improved patient-practitioner communication. N C Med J. 2007;68(5):319–326.
21. Siepmann M. Health behavior. In: Kirch W, editor. Encyclopedia of Public Health. Springer Netherlands; 2008:515–521.
22. Ipsen JA, Viberg B, Pedersen LT, Draborg E, Bruun IH. Informal care after Hip fracture: prospective cohort. BMC Geriatr. 2024;24(1):436. doi:10.1186/s12877-024-05040-y
23. Zhu Y, Xu BY, Low SG, Low LL. Association of social support with rehabilitation outcome among older adults with hip fracture surgery: a prospective cohort study at post-acute care facility in Asia. J Am Med Dir Assoc. 2023;24:1490–1496. doi:10.1016/j.jamda.2023.03.034
24. Edwards NM, Varnum C, Nelissen R, Overgaard S, Pedersen AB. The association between socioeconomic status and the 30- and 90-day risk of infection after total Hip arthroplasty: a registry-based cohort study of 103,901 patients with osteoarthritis. Bone Joint J. 2022;104-b(2):221–226. doi:10.1302/0301-620x.104b2.Bjj-2021-1030.R1
25. Austin D, Yan AT, Jamieson S, Zaman AG, Kunadian V, Bagnall AJ. Treatment delay in primary PCI in relation to marital status and distance from acute medical care. Eur Heart J. 2013;34(suppl_1):P469–P469. doi:10.1093/eurheartj/eht307.P469
26. Yuan R, Zhang C, Li Q, Ji M, He N. The impact of marital status on stage at diagnosis and survival of female patients with breast and gynecologic cancers: a meta-analysis. Gynecol Oncol. 2021;162(3):778–787. doi:10.1016/j.ygyno.2021.06.008
27. Shah SJ, Fang MC, Wannier SR, Steinman MA, Covinsky KE. Association of social support with functional outcomes in older adults who live alone. JAMA Intern Med. 2022;182(1):26–32. doi:10.1001/jamainternmed.2021.6588
28. Juthani-Mehta M, Quagliarello VJ. Infectious diseases in the nursing home setting: challenges and opportunities for clinical investigation. Clin Infect Dis. 2010;51(8):931–936. doi:10.1086/656411
29. Vesterager JD, Madsen M, Hjelholt TJ, Kristensen PK, Pedersen AB. Prediction ability of Charlson, elixhauser, and Rx-risk comorbidity indices for mortality in patients with hip fracture. A Danish population-based cohort study from 2014–2018. Clin Epidemiol. 2022;14:275–287. doi:10.2147/clep.S346745
30. Cassidy MR, Rosenkranz P, McCabe K, Rosen JE, McAneny D. I COUGH: reducing postoperative pulmonary complications with a multidisciplinary patient care program. JAMA Surg. 2013;148(8):740–745. doi:10.1001/jamasurg.2013.358
31. Chen B, Zhang JH, Duckworth AD, Clement ND. Effect of oral nutritional supplementation on outcomes in older adults with Hip fractures and factors influencing compliance. Bone Joint J. 2023;105–b(11):1149–1158. doi:10.1302/0301-620x.105b11.Bjj-2023-0139.R1
32. Sezgin D, O’Caoimh R, Liew A, et al. The effectiveness of intermediate care including transitional care interventions on function, healthcare utilisation and costs: a scoping review. Eur Geriatric Med. 2020;11(6):961–974. doi:10.1007/s41999-020-00365-4
33. Holland-Bill L, Xu H, Sørensen HT, et al. Positive predictive value of primary inpatient discharge diagnoses of infection among cancer patients in the Danish National Registry of Patients. Ann Epidemiol. 2014;24(8):593–7,597.e1–18. doi:10.1016/j.annepidem.2014.05.011
34. Henriksen DP, Nielsen SL, Laursen CB, Hallas J, Pedersen C, Lassen AT. How well do discharge diagnoses identify hospitalised patients with community-acquired infections?--a validation study. PLoS One. 2014;9(3):e92891. doi:10.1371/journal.pone.0092891
35. Hoffmann R, Kröger H, Geyer S. Social causation versus health selection in the life course: does their relative importance differ by dimension of SES? Soc Indic Res. 2019;141(3):1341–1367. doi:10.1007/s11205-018-1871-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.