Back to Journals » Journal of Inflammation Research » Volume 17
The Association Between S100A12 Protein and C-Reactive Protein with Malignant Ventricular Arrhythmias Following Acute Myocardial Infarction in the Elderly
Authors Song L, Lu YM, Zhang JC, Yuan YM, Li GR
Received 7 September 2023
Accepted for publication 9 January 2024
Published 23 January 2024 Volume 2024:17 Pages 461—468
DOI https://doi.org/10.2147/JIR.S439198
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Lei Song, Ying-Min Lu, Jin-Chun Zhang, Yu-Min Yuan, Gui-Ru Li
Department of Cardiology, Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences, Shanghai, 202150, People’s Republic of China
Correspondence: Ying-Min Lu, Department of Cardiology, Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences, No. 25 of Nanmen Street, Chengqiao Town, Chongming District, Shanghai, 202150, People’s Republic of China, Tel +86-18939929687, Email [email protected]
Objective: To investigate the association of S100A12 protein and C-reactive protein (CRP) with the onset of malignant ventricular arrhythmias (MVA) after acute myocardial infarction (AMI) in the elderly.
Methods: A total of 159 elderly AMI patients admitted to Chongming Hospital affiliated to Shanghai University of Medicine & Health Sciences from January 2018 to January 2023 were enrolled in the study. CRP levels were determined using an automatic biochemical analyzer, and S100A12 levels were measured using enzyme-linked immunosorbent assay (ELISA). Patients were categorized based on the Lown classification into groups without MVA and with MVA. Univariate analysis was initially performed to identify independent variables, followed by multivariate logistic regression to determine the risk factors for malignant ventricular arrhythmias post-AMI. The predictive value of S100A12 protein and CRP for malignant ventricular arrhythmias after acute myocardial infarction in the elderly was analyzed using the receiver operating characteristic (ROC) curve.
Results: Among the 159 patients with AMI, 27 (17%) had MVA. Multivariate logistic regression analysis indicated that both S100A12 protein and CRP could be independent risk factors for malignant ventricular arrhythmias following acute myocardial infarction in the elderly (p < 0.05). The area under the ROC curve showed the area under the curve (AUC) for S100A12 protein to be 0.7147, for CRP 0.7356, and for the combined diagnosis 0.8350 (p < 0.05).
Conclusion: S100A12 protein and CRP are independent risk factors for MVA after MI in the elderly. The combined application of S100A12 protein and CRP has higher diagnostic sensitivity and specificity.
Keywords: S100A12, C-reactive protein, acute myocardial infarction, malignant ventricular arrhythmias
Introduction
Acute myocardial infarction (AMI) stands as one of the leading causes of death among the elderly population. Complications arising from AMI often manifest in the form of ventricular or supraventricular arrhythmias. Of these, atrial fibrillation is the most frequently observed, yet malignant ventricular arrhythmias (MVA) remain the most lethal.1,2 MVAs primarily present as sustained ventricular tachycardia (VT), ventricular flutter, and ventricular fibrillation (VF), along with other life-threatening arrhythmias originating from the ventricles. MVAs account for one of the most common causes of death in AMI patients,3,4 with 25% to 50% of AMI patients succumbing to MVAs.5 Notably, MVAs frequently occur within 48 hours of the onset of AMI symptoms, with reports suggesting that 91% of AMI patients experience MVAs during this critical phase.6 Reperfusion therapies, especially percutaneous coronary intervention (PCI), have significantly reduced the incidence and mortality rates of myocardial infarction. However, the incidence rate of MVA post-AMI remains as high as 10%. Thus, an early assessment of MVA risk in AMI patients can assist clinicians in adopting proactive preventative and therapeutic measures, consequently reducing the risk of in-hospital mortality and improving prognosis.7 In this study, our objective is to explore the independent predictive factors for the occurrence of MVA in AMI patients during hospitalization.
Inflammation plays a pivotal role in the onset and progression of AMI.8 C-reactive protein (CRP) is a quintessential protein of the acute inflammatory phase and serves as a significant molecular exacerbator in AMI patients. A recent study has shown that CRP is not only a marker of inflammation, but also promotes inflammation and subsequent myocardial fibrosis through the TLR4/NF-κB/TGF-β pathway.9 Previous studies have shown that elevated CRP is significantly associated with the occurrence and recurrence of AF in the structural heart disease population10,11 and with an increased risk of malignant ventricular arrhythmias.12 The elevated frequency of arrhythmias post-AMI, along with the prolongation of its onset, positively correlates with elevated peripheral blood CRP expression levels.13,14
S100A12, a member of the S100 calcium-binding protein family secreted by leukocytes, belongs to the largest subfamily of EF-hand calcium-binding proteins.15 Many current studies have focused on the role and influence of S100A12 in various diseases. S100A12 are crucial for the activation of natural killer (NK) cells, neutrophil chemotaxis and inflammation regulation.16 Reports suggest that S100A12 is implicated in chronic inflammatory diseases such as rheumatoid arthritis and inflammatory bowel syndrome.15 Literature has also highlighted S100A12 as a novel atherosclerotic molecule associated with cardiovascular events in atherosclerotic diseases.17 By activating cells involved in inflammation through various mechanisms, it partakes in the chronic inflammatory pathology of atherosclerosis. This positions S100A12 as a valuable biomarker and tracer in atherosclerotic diseases and various other inflammatory conditions.18 Research conducted by Zhiqiang et al19 also indicates that elevated S100A12 levels pose as risk factors that negatively impact the prognosis of coronary heart disease (CHD), underscoring the profound significance of S100A12 levels in predicting CHD outcomes. Although S100A12 has been regarded as one of inflammatory biomarkers in cardiovascular disease, no literature has yet elucidated the relevance of S100A12 in arrhythmias following AMI.20
Although there is growing evidence for the role of inflammatory dysregulation in AF, these studies often use a single biomarker and the results are inconsistent.21,22 This study se eks to explore the association of S100A12 protein and CRP in elderly AMI patients developing MVA and assess the potential of these two molecules as novel predictive biomarkers, which has important clinical significance for further prevention and diagnosis of arrhythmia.
Materials and Methods
Study Subjects
From January 2018 to January 2023, a convenience sample of 159 elderly AMI patients treated at Chongming Hospital affiliated with Shanghai University of Medicine & Health Sciences was selected for this study. All patients were admitted to the hospital within 1 to 6 hours after the onset of AMI and underwent primary PCI immediately after admission. There were no complications such as heart failure, bleeding, and re-infarction within 7 days after operation, suggesting that the operation was effective. The mortality rate was 0(no subjects died during the study period).
Inclusion criteria: (1) Age ≥ 65 years; (2) Meets the diagnostic criteria for ST-segment elevation myocardial infarction;23 (2) Has not recently taken anti-arrhythmic drugs; (3) Clinical data is comprehensive and authentic. Exclusion criteria: (1) Patients with severe heart, liver, or kidney dysfunction; (2) Patients concurrently diagnosed with malignant tumors; (3) Patients with acute cerebrovascular diseases; (4) Patients with a history of arrhythmias or those on long-term oral β-blockers or other anti-arrhythmic drugs; (5) Patients diagnosed with diabetes. This study was approved by the Medical Ethics Committee of Chongming Hospital affiliated with Shanghai University of Medicine & Health Sciences. All participants provided informed consent.
Collection of Relevant Indicators and Grouping
Upon operation, patients underwent 5-lead 24-hour bedside cardiac monitoring. General patient data (gender, age, body mass index, blood pressure, heart rate, basic medical history, smoking history, etc.) were collected. Blood samples were collected as follows: On the second day after PCI, peripheral blood was collected for the detection of various indicators. Using an automated biochemistry analyzer, the following parameters were measured: fasting blood glucose (FBG), serum creatinine (Scr), C-reactive protein (CRP), and lipid profile markers [triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C)]. An automatic hematology analyzer was employed to measure white blood cells (WBC), hemoglobin (Hb), and blood platelets (PLT). An automated coagulation analyzer was used to determine D-dimer (D-D) levels. The enzyme-linked immunosorbent assay (ELISA) was employed to measure S100A12 levels. Echocardiography was used to measure the left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVDD), and left ventricular end-systolic diameter (LVSD). Diagnostic criteria for MVA: Immediately upon admission, patients underwent 5-lead cardiac monitoring for a duration of 72 hours. The occurrence of ventricular arrhythmias was observed, and based on the results of the 24-hour dynamic electrocardiogram monitoring, they were graded using the Lown classification (also known as Ventricular Premature Beat Degree classification),24 ranging from Grades I to V: Grade 0, no ventricular premature beat; Grade I, occasional ventricular premature beats (<30 beats / hour); Grade II, multiple premature ventricular beats (>30 beats / hour); Grade IVa, successive ventricular premature beats; Grade IVb, short runs of ventricular tachycardia (short bursts of ventricular tachycardia, more than 3 times in a row, no more than 7 times at most); Grade V: early-onset ventricular premature beats (R - on - t), with 3 or more R - on - t phenomena in 1 hour during the 24-hour monitoring period. Lown Grades ≥ IVb were defined as MVA, encompassing primary and non-primary ventricular fibrillation and sustained ventricular tachycardia. Observational indicators were divided based on Lown grading into non-MVA and MVA groups. The incidence of MVA was statistically measured, and differences in general data between the two groups were compared to analyze potential influencing factors for MVA.
Statistical Analysis
Data were analyzed using SPSS 26.0 statistical software. Continuous variables with a normal distribution were expressed as  and were compared using paired T-tests between groups. Non-normally distributed continuous data were represented by the median and interquartile range and were compared using non-parametric tests. Comparisons among multiple groups were conducted using the Kruskal–Wallis H-test, with pairwise comparisons corrected using the Bonferroni method. Categorical data were represented as frequencies and percentages and were compared using the χ²-test or Fisher’s exact test. Multivariate logistic regression was utilized to analyze risk factors for MVA, with P<0.05 indicating statistical significance.
and were compared using paired T-tests between groups. Non-normally distributed continuous data were represented by the median and interquartile range and were compared using non-parametric tests. Comparisons among multiple groups were conducted using the Kruskal–Wallis H-test, with pairwise comparisons corrected using the Bonferroni method. Categorical data were represented as frequencies and percentages and were compared using the χ²-test or Fisher’s exact test. Multivariate logistic regression was utilized to analyze risk factors for MVA, with P<0.05 indicating statistical significance.
Results
General Clinical Data
Of the 159 patients, 27 experienced MVA, with an incidence rate of 17%. As observed from baseline data, patients who developed MVA after AMI had elevated levels of both C-reactive protein (CRP) and S100A12, which were statistically significant (p < 0.05). Additionally, a decline in lymphocyte count was also statistically significant (p < 0.05). Other indicators did not show any statistical significance (p > 0.05). Further details are presented in Table 1.
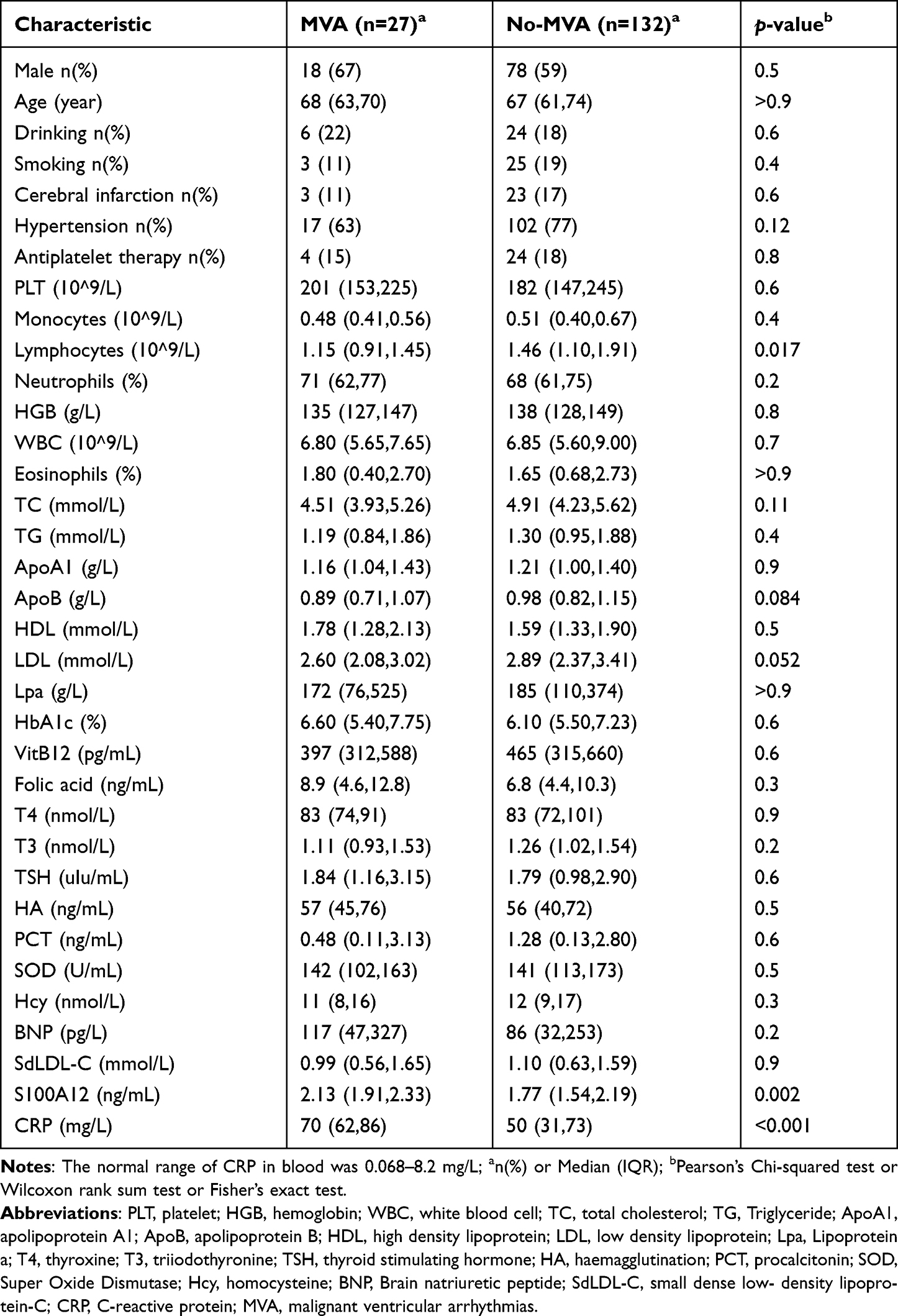 |
Table 1 Baseline Characteristics of the Patients |
Multivariate Logistic Regression Analysis Results
Utilizing multivariate logistic regression analysis and considering LDL, APoB, TC, CRP, S100A12, and lymphocyte count as independent variables, and the occurrence of MVA as the dependent variable, the results indicated that CRP and S100A12 are independent risk factors for MVA with statistical significance (OR=0.95, 0.006; 95% CI 0.93–0.98, 0.01–0.24; p < 0.05). More details are available in Table 2.
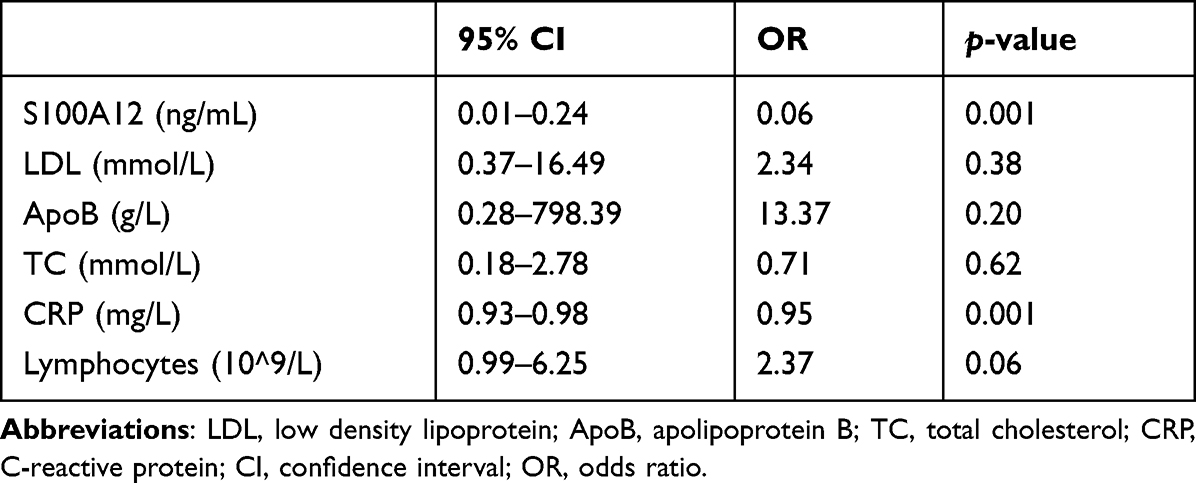 |
Table 2 Results of the Multivariate Logistic Regression Analysis |
2.3 Predictive Value of S100A12 Protein and C-reactive Protein for Malignant Arrhythmias in Elderly Acute Myocardial Infarction.
Based on the above analyses, ROC curve analyses were performed separately for CRP and S100A12. The area under the ROC curve demonstrated an AUC of 0.7356 for CRP (p < 0.05) and 0.7147 for S100A12 (p < 0.05). The combined diagnostic AUC was 0.8350 (p < 0.05). This suggests that the combined diagnosis of CRP and S100A12 offers greater sensitivity and specificity in predicting malignant arrhythmias following acute myocardial infarction in the elderly, providing meaningful insights for clinical practice. Refer to Figure 1.
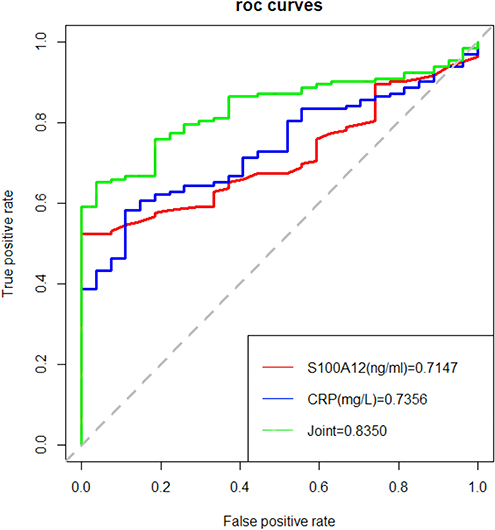 |
Figure 1 Predictive value of S100A12, CRP, and their combined application for MVA. Abbreviations: CRP, C-reactive protein; MVA, malignant ventricular arrhythmias. |
Discussion
Studies have shown that the proportion of AMI patients developing MVA is approximately 20.0%, and the mortality risk for patients with MVA is 4–7 times higher than those without MVA.25 Our research found that, out of 235 elderly AMI patients, 89 developed MVA, leading to an incidence rate of 37.87%. Among these, 14 patients succumbed, resulting in a mortality rate of 15.73%.26,27 This underlines that the occurrence rate of MVA in elderly AMI patients is notably high, and so is the mortality rate, warranting significant clinical attention.
In this study, it was observed that the expression levels of CRP were notably elevated in elderly AMI patients who developed MVA compared to those without MVA. Regression analysis identified CRP as an independent risk factor for the onset of MVA in AMI patients, suggesting its potential as a predictive marker. The influence of CRP on myocardial tissue is primarily related to inflammatory responses. Inflammation plays a pivotal role in the progression of AMI, being intimately associated with atheromatous plaque formation and recognized as an independent risk factor that exacerbates the vulnerability of coronary atherosclerotic plaques, thereby increasing the likelihood of MVA in AMI patients.28 CRP is an acutely sensitive albeit less specific inflammatory product. Proteomic-based risk models have found that CRP is a major risk predictor for coronary atherosclerosis.29 It significantly contributes to the pathogenesis of coronary artery disease and AMI, mainly by promoting atherosclerosis and instigating inflammatory processes. CRP also exerts detrimental effects on myocardial metabolism, leading to cardiac functional impairment due to its cardiotoxic properties.30 In AMI patients, the larger the area of myocardial necrosis, the higher the internal CRP content. Circulating CRP can be recognized as a potential biomarker for diagnosis and severity assessment of disease in AMI.31 Some scholars have found that reducing peripheral blood CRP levels can mitigate myocardial damage from AMI.32–34 Furthermore, numerous studies have indicated that increased circulating CRP concentrations post-AMI can destabilize myocardial electrical activity, alter inherent cardiac membrane potentials, and precipitate lethal arrhythmias such as malignant ventricular arrhythmias.35
In this study, we observed that the expression levels of S100A12 were significantly elevated in elderly AMI patients who developed MVA compared to those without MVA. Regression analysis pinpointed S100A12 as an independent risk factor for the onset of MVA in AMI patients, suggesting its viability as a prognostic indicator. The impact mechanism of S100A12 on myocardial tissue is intrinsically tied to inflammatory responses. Expressed in granulocytes and activated monocytes/macrophages, S100A12, when bound to the Receptor for Advanced Glycation End products (RAGE), induces the upregulation of nuclear factor κB (NFκB), intensifying the inflammatory response. This binding of S100A12 to RAGE mediates the secretion of cytokines.36,37 Previous research has indicated that S100A12 may serve as a distinct biomarker for cardiovascular pathological processes and has a close association with MVA,38,39 mirroring our findings and further supporting the potential of S100A12 as a predictor for MVA in AMI patients.
S100A12 acts as a mediator that amplifies inflammation and tumorigenesis. Studies have demonstrated a correlation between plasma S100A12 levels and hs-CRP levels, suggesting a relationship between S100A12 and the inflammation levels in CAD patients.40 Through ROC curve analysis in our study, we discerned that the combined diagnostic AUC of CRP and S100A12 was 0.8350, surpassing the value of each marker used in isolation. This indicates a heightened sensitivity and specificity of the combined diagnosis of CRP and S100A12 in predicting malignant arrhythmias following acute myocardial infarction in the elderly. Additionally, it suggests that the combined application of both markers augments predictive and diagnostic accuracy. Research by Xiaotong et al40 revealed that, in AMI patients, serum S100A12 levels increase with the escalation in the number of lesions and severity of the condition. Hence, it can be inferred that serum S100A12 levels, in conjunction with hsCRP, CK-MB, and the Gensini score, can gauge the severity of AMI patients. Moreover, it can serve as a novel biomarker to guide clinical severity classification and treatment. Our findings are consistent with this research, further corroborating that in AMI patients, the combined application of S100A12 and CRP can more effectively predict the onset of MVA. The potential of this novel prognostic biomarkers of inflammation and thrombosis will be a valuable clinical tool for evaluating risk stratification and progression of AF after AMI.
This study possesses certain limitations. Firstly, the sample size is relatively limited. Secondly, given that the observed outcomes were manually assessed and cannot guarantee consistent evaluation by the same individual, there might be subjective variances leading to biases. Lastly, considering that all patients hail from the same region and belong to the middle-aged and elderly demographic, the study boasts robust internal validity, yet its external validity is compromised. Further multicenter prospective studies with a larger sample size are planned to evaluate the clinical relevance of the combination of CPR and S100A12.
Conclusion
The expression levels of CRP and S100A12 may serve as independent risk factors in forecasting MVA following AMI. Their combined assessment holds paramount significance in evaluating patient condition fluctuations and prognosis.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Chongming Hospital Affiliated to Shanghai University of Medicine and Health Sciences. Written informed consent was obtained from all participants.
Funding
This study did not receive any funding in any form.
Disclosure
The authors declare that they have no competing interests.
References
1. Zhou Z, Liu C, Xu S, et al. Metabolism regulator adiponectin prevents cardiac remodeling and ventricular arrhythmias via sympathetic modulation in a myocardial infarction model. Basic Res Cardiol. 2022;117(1):34. doi:10.1007/s00395-022-00939-2
2. Zeymer U. Hat der Patient einen Herzinfarkt? [Diagnosis and initial management of acute myocardial infarction]. MMW Fortschr Med. 2019;161(4):34–36. Gernman.
3. Pollard TJ. The acute myocardial infarction. Prim Care. 2000;27(3):
4. Wang CG, Qin XC, Nie SP, Wang CM, Ai H, Que B. C-reactive protein as a predictor of malignant ventricular arrhythmias in non-ST elevation myocardial infarction. J Geriatr Cardiol. 2019;16(8):614–620. doi:10.11909/j.issn.1671-5411.2019.08.007
5. Bui AH, Waks JW. Risk stratification of sudden cardiac death after acute myocardial infarction. J Innov Card Rhythm Manag. 2018;9(2):3035–3049. doi:10.19102/icrm.2018.090201
6. Compiling Group of China’s Cardiovascular Health and Disease Report, Hu Shengshou. Annual report on cardiovascular health and diseases in China (2020). Chin Circ J. 2021;36(06):521–545.
7. Çitaku H, Miftari R, Stubljar D, Krasniqi X. Size of acute myocardial infarction correlates with earlier time of initiation of reperfusion therapy with cardiac perfusion scintigraphy: a national single-center study. Med Sci Monit Basic Res. 2021;27:e933214. doi:10.12659/MSMBR.933214
8. Cai S, Zhao M, Zhou B, et al. Mitochondrial dysfunction in macrophages promotes inflammation and suppresses repair after myocardial infarction. J Clin Invest. 2023;133(4):e159498. doi:10.1172/JCI159498
9. Sun W, Wu Y, Gao M, et al. C-reactive protein promotes inflammation through TLR4/NF-κB/TGF-β pathway in HL-1 cells. Biosci Rep. 2019;39(8):BSR20190888. doi:10.1042/BSR20190888
10. Wang Z, Wang B, Li X, Zhang S, Wu S, Xia Y. Metabolic syndrome, high-sensitivity C-reactive protein levels and the risk of new-onset atrial fibrillation: results from the Kailuan study. Nutr Metab Cardiovasc Dis. 2021;31(1):102–109. doi:10.1016/j.numecd.2020.06.026
11. Xie JY, Noeman M, Pimenta D, Little C. C-reactive protein as a predictor for developing post-operative atrial fibrillation. Europace. 2021;23(1):159. doi:10.1093/europace/euaa303
12. Kalinskaya A, Dukhin O, Lebedeva A, et al. Circulating cytokines in myocardial infarction are associated with coronary blood flow. Front Immunol. 2022;13:837642. doi:10.3389/fimmu.2022.837642
13. Wang L, Peng Y, Song L, et al. Colchicine-containing nanoparticles attenuates acute myocardial infarction injury by inhibiting inflammation. Cardiovasc Drugs Ther. 2022;36(6):1075–1089. doi:10.1007/s10557-021-07239-2
14. Alkouri A, Cybularz M, Mierke J, et al. The predictive role of early CRP values for one-year mortality in the first 2 d after acute myocardial infarction. Biomarkers. 2022;27(3):293–298. doi:10.1080/1354750X.2022.2040591
15. Li Y, He Y, Chen S, et al. S100A12 as biomarker of disease severity and prognosis in patients with idiopathic pulmonary fibrosis. Front Immunol. 2022;13:810338. doi:10.3389/fimmu.2022.810338
16. Kazakov AS, Zemskova MY, Rystsov GK, et al. Specific S100 proteins bind tumor necrosis factor and inhibit its activity. Int J Mol Sci. 2022;23(24):15956. doi:10.3390/ijms232415956
17. Xie J, Luo C, Mo B, et al. Inflammation and oxidative stress role of S100A12 as a potential diagnostic and therapeutic biomarker in acute myocardial infarction. Oxid Med Cell Longev. 2022;2022:2633123. doi:10.1155/2022/2633123
18. Xinglan C, Shengnan L, Shaofeng C, Deng F, Peiyi Z. Research progress on the relationship between S100A8/A9 and S100A12 with atherosclerosis. Hainan Med J. 2020;31(05):647–652.
19. Zhiqiang N, Hongyan J, Guokang Y, Han L, Bin X. Expression and prognostic value of S100A12, ABI, and non-HDL-C in coronary atherosclerotic heart disease. Med Pharm J Chin People’s Lib Army. 2021;33(08):
20. Singh H, Rai V, Agrawal DK. LPS and oxLDL-induced S100A12 and RAGE expression in carotid arteries of atherosclerotic Yucatan microswine. Mol Biol Rep. 2022;49(9):8663–8672. doi:10.1007/s11033-022-07703-8
21. Selcuk M, Cinar T, Saylik F, Dogan S, Selcuk I, Orhan AL. Predictive value of systemic immune inflammation index for postoperative atrial fibrillation in patients undergoing isolated coronary artery bypass grafting. Meden Med J. 2021;36(4):318–324. doi:10.4274/MMJ.galenos.2021.37998
22. Bağcı A, Aksoy F. Systemic immune-inflammation index predicts new-onset atrial fibrillation after ST elevation myocardial infarction. Biomarker Med. 2021;15(10):731–739. doi:10.2217/bmm-2020-0838
23. Stengaard C, Sørensen JT, Rasmussen MB, Bøtker MT, Pedersen CK, Terkelsen CJ. Prehospital diagnosis of patients with acute myocardial infarction. Diagnosis. 2016;3(4):155–166. doi:10.1515/dx-2016-0021
24. Wu W, He J, Zhang S, Zeng C, Wang Q. Basic demographic characteristics and prevalence of comorbidities in acute mesenteric ischemia: a systematic review and proportional meta-analysis. Scand J Gastroenterol. 2023;58(6):605–618. doi:10.1080/00365521.2022.2152289
25. Takada T, Shishido K, Hayashi T, et al. Impact of late ventricular arrhythmias on cardiac mortality in patients with acute myocardial infarction. J Interv Cardiol. 2019;2019:5345178. doi:10.1155/2019/5345178
26. Oikawa J, Fukaya H, Ako J, et al; on behalf the J-MINUET Investigators. Risk factors of in-hospital lethal arrhythmia following acute myocardial infarction in patients undergoing primary percutaneous coronary intervention- insight from the J-MINUET study. Circ Rep. 2019;2(1):17–23. doi:10.1253/circrep.CR-19-0081
27. Ren L, Guo J, Zhao W, et al. Serum homocysteine relates to elevated lipid level, inflammation and major adverse cardiac event risk in acute myocardial infarction patients. Biomarker Med. 2023;17(6):297–306. doi:10.2217/bmm-2023-0096
28. Zhang N, Shi F, Liang H, Wang H. The feasibility of using Hcy, CRP, and Cys-C to analyze AMI patients’ disease conditions and prognoses. Am J Transl Res. 2021;13(4):2724–2730.
29. Nurmohamed NS, Belo Pereira JP, Hoogeveen RM, et al. Targeted proteomics improves cardiovascular risk prediction in secondary prevention. Eur Heart J. 2022;43(16):1569–1577. doi:10.1093/eurheartj/ehac055
30. Sheriff A, Kayser S, Brunner P, Vogt B. C-reactive protein triggers cell death in ischemic cells. Front Immunol. 2021;12:630430. doi:10.3389/fimmu.2021.630430
31. Maier W, Altwegg LA, Corti R, et al. Inflammatory markers at the site of ruptured plaque in acute myocardial infarction: locally increased interleukin-6 and serum amyloid A but decreased C-reactive protein. Circulation. 2005;111(11):1355–1361. doi:10.1161/01.CIR.0000158479.58589.0A
32. Oprescu N, Micheu MM, Scafa-Udriste A, Popa-Fotea NM, Dorobantu M. Inflammatory markers in acute myocardial infarction and the correlation with the severity of coronary heart disease. Ann Med. 2021;53(1):1041–1047. doi:10.1080/07853890.2021.1916070
33. Akbarzadeh Najar R, Ghaderian SM, Tabatabaei Panah AS. C-reactive protein (CRP) gene polymorphisms: implication in CRP plasma levels and susceptibility to acute myocardial infarction. Mol Biol Rep. 2012;39(4):3705–3712. doi:10.1007/s11033-011-1145-z
34. Chung MK, Martin DO, Sprecher D, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. 2001;104(24):2886–2891. doi:10.1161/hc4901.101760
35. Asadikaram G, Noroozi S, Ebrahimi Meimand HA, et al. Interferon-β 1a modulates expression of RAGE but not S100A12 and nuclear factor-κB in multiple sclerosis patients. Neuroimmunomodulation. 2016;23(5–6):345–351. doi:10.1159/000464136
36. Kim K, Kim HJ, Binas B, Kang JH, Chung IY. Inflammatory mediators ATP and S100A12 activate the NLRP3 inflammasome to induce MUC5AC production in airway epithelial cells. Biochem Biophys Res Commun. 2018;503(2):657–664. doi:10.1016/j.bbrc.2018.06.057
37. He YY, Yan W, Liu CL, et al. Usefulness of S100A12 as a prognostic biomarker for adverse events in patients with heart failure. Clin Biochem. 2015;48(4–5):329–333. doi:10.1016/j.clinbiochem.2014.11.016
38. Tong X, Zhao X, Dang X, Kou Y, Kou J. Predicting diagnostic gene biomarkers associated with immune checkpoints, N6-methyladenosine, and ferroptosis in patients with acute myocardial infarction. Front Cardiovasc Med. 2022;9:836067. doi:10.3389/fcvm.2022.836067
39. Gellen B, Thorin-Trescases N, Thorin E, et al; SURDIAGENE Study group. Increased serum S100A12 levels are associated with higher risk of acute heart failure in patients with type 2 diabetes. ESC Heart Fail. 2022;9(6):3909–3919. doi:10.1002/ehf2.14036
40. Xiaotong L, Xin L, Xue W, Wei S, Shanshan X, Laichuan L. Relationship between serum S100A12 levels and severity of coronary artery lesions in AMI patients. J Clin Cardiol. 2018;34(06):588–592.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.