")
Back to Journals » International Journal of General Medicine » Volume 16
The Association Between Nicotine Dependence and Mental Health in the General Population of Saudi Arabia: A Cross-Sectional Analytical Study
Authors Albarrak DA, Alotaibi AB , Alotaibi RF , Alramadhan SH , Bin Muhanna AI , Aldehan AM, Bin Abdulrahman KA
Received 8 July 2023
Accepted for publication 17 November 2023
Published 11 December 2023 Volume 2023:16 Pages 5801—5815
DOI https://doi.org/10.2147/IJGM.S429609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandul Yasobant
Danah Abdullah Albarrak,1 Abdulrahman Bandar Alotaibi,2 Roaa Faisal Alotaibi,3 Sara Hussain Alramadhan,3 Alhanouf Ibrahim Bin Muhanna,1 Abdulrahman Mohammed Aldehan,2 Khalid A Bin Abdulrahman4
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2Department of Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, 13317, Saudi Arabia; 3Department of Medicine, College of Medicine, AlMaarefa University, Ad Diriyah, 13713, Saudi Arabia; 4Department of Medical Education, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, 13317-4233, Saudi Arabia
Correspondence: Abdulrahman Bandar Alotaibi, Department of Medicine, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, 13317, Saudi Arabia, Email [email protected]
Background: High prevalence of mental disorders is associated with psychoactive substances, significantly contributing to morbidity, disability, and premature mortality. Worldwide, individuals who use electronic-cigarettes (EC) and have a mental health diagnosis are more likely to experience stress, depression, and drug use. This study aims to measure the prevalence of both EC use and mental health disorders namely, anxiety and depression additionally to investigate the association between EC use and mental health status among the general population of Saudi Arabia.
Methods: A cross-sectional analytical study was conducted across Saudi Arabia from November 2022 to May 2023. The survey was divided into three sections. The first section focuses on the demographics, while the second part asked about both conventional and EC smoking and their frequency. The third section assessed mental health status using a Patient Health Questionnaire with a 9-item depression scale (PHQ-9) and a 7-item Generalized Anxiety Disorder scale (GAD-7).
Results: The study revealed 21.1% reporting EC use in the past thirty days. While 19.8% reported smoking tobacco one or more days within the last thirty days. Regarding mental health, 36.6% of individuals had minimal anxiety, while 42.4% experienced mild anxiety. Moreover, most of the participant were considered to have mild followed by minimal depression accounting for 36.7% and 31.9%, respectively. The results indicated a positive and significant correlation between perceived depression scores and nicotine dependence among EC users. Additionally, there was a strong relationship between gender and nicotine dependence, with men being more inclined than women.
Conclusion: There is a correlation between nicotine use and mental health outcomes; people who use nicotine products are more likely to experience anxiety and depression.
Keywords: e-cigarettes, EC, mental health, anxiety, depression
Introduction
Over the past three decades, a global decline in tobacco smoking rates was observed with an inverse increase in the use of new tobacco products, namely electronic cigarettes (EC), a battery-powered device that delivers nicotine through a mouthpiece.1,2 This shift is mainly attributed to the fact that EC has been advertised as an effective method for smoking cessation with relatively less negative effect on health.2,3 However, EC has been confirmed to contain carcinogens in addition to nicotine; in fact, certain types of EC may contain tetrahydrocannabinol (THC) and vitamin E acetate, which can cause a new form of lung injury named EC or vaping product use associated lung injury (EVALI), identified back in 2019.4 The global tobacco control branch aimed to determine the global prevalence of EC by analyzing the data of 14 countries from 2015 to 2018. Results revealed the highest prevalence of EC in Russia, 14.2%, and Romania, 11.3%. In comparison, the remaining nine countries had a prevalence of less than 1% (Bangladesh, China, Ethiopia, India, Mexico, Philippines, Senegal, Uruguay, and Vietnam).5 In Canada, EC use prevalence was 16.1% back in 2014.6 Locally, in Saudi Arabia, EC prevalence was reported to be 26.3% in 2022.7
According to the World Health Organization (WHO), mental health is defined as a “state of well-being in which the individual realizes his or her abilities, can cope with the normal stresses of life, can work productively and fruitfully, and can contribute to his or her community”.8 Worldwide, there is a high prevalence of mental disorders associated with psychoactive substances, significantly contributing to morbidity, disability, and premature mortality. The most prevalent mental health issue is depression, which affects women twice as often as males.8 Research indicates that mental problems, such as depression and those linked to impulsivity (attention-deficit/hyperactivity disorder, oppositional defiant disorder, and conduct disorder), increase the likelihood of subsequent substance abuse, such as nicotine addiction.9 By looking at the statistics on tobacco product use among young adults, including e-cigarette usage, it is evident that individuals who use EC and have a mental health diagnosis are more likely to experience stress, depression, and drug use, especially marijuana.10,11 In other studies, smoking has been linked to an increased risk of developing depression over time, even after controlling for confounders;12 parallel connections may also exist for other mental health problems.13 Younger people tend to be more affected by cigarette smoking in terms of their chance of developing later mood and anxiety problems.14 According to a meta-analysis, quitting smoking is linked to lower levels of stress, anxiety, and depression, especially in people with mental health diagnoses.15
A systematic review by Becker TD et al illustrates that young adults with mental illnesses consume nicotine more frequently than their peers without such conditions.16 This might happen because of the following factors: (1) attempts to treat symptoms on their own, such as cognitive deficits in ADHD or low mood; (2) attempts to counteract sedative side effects of psychotropic medications; (3) prevalent underlying genetic or environmental risk factors for smoking and mental illness; or (4) neurotoxic effects of nicotine on mental health.16 There are probably other individual-specific elements involved.16 A study conducted in 2014 aimed to investigate the possible association between EC use and psychological distress in a repressive sample of United States adults, which revealed a significant association between increased levels of psychological distress and cigarette and EC use.17 Furthermore, a recent study examined the associations between youth substance use and psychological distress during 2019–2021. It concluded that EC had the strongest standardized association with psychological distress compared to other substances.18 Additionally, the association between EC and depressive symptoms intensified significantly from 2019 to 2021.18
Compared to other substances, the association between EC and mental health remains understudied. Therefore, there is an imminent need to investigate this association, especially considering the observed increase in the rates of EC use in Saudi Arabia.
Methods
Study Design
This is a cross-sectional analytical study that was conducted in Saudi Arabia from November 2022 to May 2023. The study population included the adult general population of Saudi Arabia who aged >18. For data collection, we used a convenience technique using an online self-administered survey; for all five regions, we enlisted volunteers to collect data by any means necessary, including face-to-face interviews and social media platforms through WhatsApp, Telegram, and other platforms. Sample size was calculated by the following formula: Sample Size = Z2p(1-p)/c2. Z = Z value or called confidence level = 1.96 for 95%. p = percentage picking a choice = 0.5. c = confidence interval = ±5% = 0.05. The minimum sample size needed to achieve a precision of ±5% with a 95% confidence interval is 385.
Study Questionnaire
The survey was divided into three sections. The first section focuses on the demographic and personal information of the participants, including gender, age, nationality, place of residence, and body mass index (BMI). The BMI was calculated as the body mass divided by the square of the body height and expressed as kg/m2, resulting from weight in kilograms and height in meters.
The second part of the questionnaire assessed aspects of EC use and conventional smoking. EC use was assessed by asking, “Have you ever used an EC in your life?” (yes/no). Answering no was classified as “never use.” Respondents who answered in the affirmative were asked, “Have you used ECs in the past 30 days?” (yes/no). Answering yes was classified as a “current user”, and answering no was classified as a “former user.” Those who said “yes” were asked an additional question to assess the frequency: “How many puffs do you smoke daily?”
Similarly, cigarette smoking was assessed by asking, “Have you ever smoked even one puff in your life?” (yes/no). Answering no was classified as “never smoker”. Respondents who answered in the affirmative were asked, “In the past 30 days, how many days did you smoke?” Answering ‘one or more days’ was classified as “current smoker”, and answering “none” was classified as “former smoker”. Those who said “yes” were asked an additional question to assess the frequency: “How many packets do you smoke daily?”
Lastly, Mental health functioning was determined by assessing for anxiety and depression using the following tools. The Patient Health Questionnaire (PHQ-9) included nine items on a 4 Likert scale (0–3). The total scores range from 0 to 27; the collective score is then interpreted at cut-off points at 4, 5, 10, 15, and 20 as none/minimal, mild, moderate, moderately severe, and severe, respectively. In addition, the Generalized Anxiety Disorder scale (GAD-7) included seven items on a 4 Likert scale (0–3), total scores ranging from 0 to 21, and the collective score is interpreted at cut-off points at 4, 5, 10, and 15 as none/minimal, mild, moderate, and severe, respectively.
Statistical Data Analysis
The mean and standard deviation were used to describe the continuous variables. The median and the interquartile range ranges were used to define variables that showed statistical normality assumption violations. The categorical variables were described with frequencies and percentages. The categorical exploratory Factor Analysis (FA) was used to reduce the indicators of nicotine dependence (smoking, smoked days, and number of cigarettes per day and the like measured e-cigarettes use factors) into a standardized one metric score that characterized nicotine dependence factor-based (z-score), the resulted factor solution was evaluated for reliability, and salient item-factor loadings were considered when loadings were ≥0.32. The resulting factor analysis based on Nicotine dependence Z-score was transformed into a normed T-score by multiplying the z-score by ten and then adding the resulting product to 50 points. The Spearman’s (Rho) correlation test assessed the bivariate correlations between metric-measured perceptions. The Generalized Linear Multivariable Modelling was used to determine the statistical significance of predictors for each measured concept (depression, anxiety, and nicotine dependence scores) using the Gamma Regression due to skewness in the error modeling using the other conventional regression methods. The association between the predictor variables with their dependent outcome variables was expressed as multivariate-adjusted Risk Rates (RR) with a 95% confidence interval. The SPSS IBM software version 21 was used for statistical data analysis. Alpha significance level was considered at 0.050 level. The Cronbach’s alpha internal consistency test was applied to the measured questionnaires (Table 1). The resulting findings showed that the Patients Health Questionnaire was measured with sufficient internal consistency, Cronbach’s alpha = 0.885, likewise the Generalized Anxiety Disorder seven-item questionnaire was internally consistent, Cronbach’s alpha = 0.888, but also the six categorical questions that characterized people’s nicotine dependence and consumption had great internal consistency according to the categorical Cronbach’s alpha (=0.79) test. This indicates that the measured indicators of depression, anxiety, and nicotine consumption were read and understood equally reliably by people.
 |
Table 1 Internal Consistency/ Reliability Analysis of the Measured Questionnaires |
Results
A total of 2293 people residing in Saudi Arabia enrolled in the study and completed the questionnaire. Table 2 displays the resulting descriptive analysis of people’s sociodemographic characteristics; findings showed that 50.8% of people were females. The distribution of people’s age groups is shown in Figure 1; most were aged between 18 and 28 years accounting for 46.6%. Considering the body mass index levels of the respondents, the majority were considered to have normal BMI 36.8%, followed by overweight and obesity class I accounting for 28.8%, 20% respectively.
 |
Table 2 Descriptive Analysis of People’s Sociodemographic Characteristics. N=2293 |
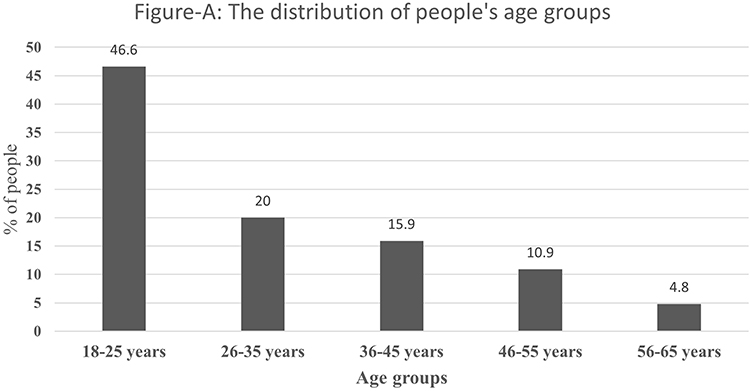 |
Figure 1 The distribution of People’s age groups. |
Regarding nationality, 95.3% of participants were Saudis. The majority of respondents educational level was a university degree 64.6%, followed by high school degree 21.2%.
Additionally, the employment state of people showed that 39.9% were still students, 26.6% were government employed, but 11.7% of them were private-sector employed. However, 7% of them were retired, 12.4% of them were unemployed. Concerning the residence of people, the majority lived in the central or eastern region of the kingdom accounting for 25.1% and 22.5%, respectively.
Table 3 displays the results of the descriptive analysis of people’s nicotine dependence indicators; 31.6% of respondents confirmed using EC at least once in their lifetime, while 21.1% have used EC in the last thirty days. Regarding the frequency of EC use, 13.2% smoked EC less than ten times in the last month, and 6.3% smoked EC 10–20 times in the previous thirty days.
 |
Table 3 Descriptive Analysis of People’s Smoking Habits |
Additionally, 46.8% of the respondents were found to have smoked tobacco in their lifetime, whereas 19.8% reported smoking tobacco one or more days within the last thirty days. However, people were asked to indicate how many cigarettes they smoked daily. The resulting findings showed 10.1% smoked <10 cigarettes/day, another 6.3% smoked between 10 and 20 cigarettes per day.
Table 4 displays the descriptive analysis of people’s perceptions of the indicators of generalized anxiety and depression. The results revealed that people’s top perceived indicator of anxiety was feeling nervous, anxious, and on edge; followed by becoming easily annoyed and having trouble relaxing. Whereas people’s top perceived indicator of depression was Feeling tired or having little energy; followed by trouble falling or staying asleep, then losing appetite or overeating and feeling down and depressed, followed by having little interest/pleasure in doing things.
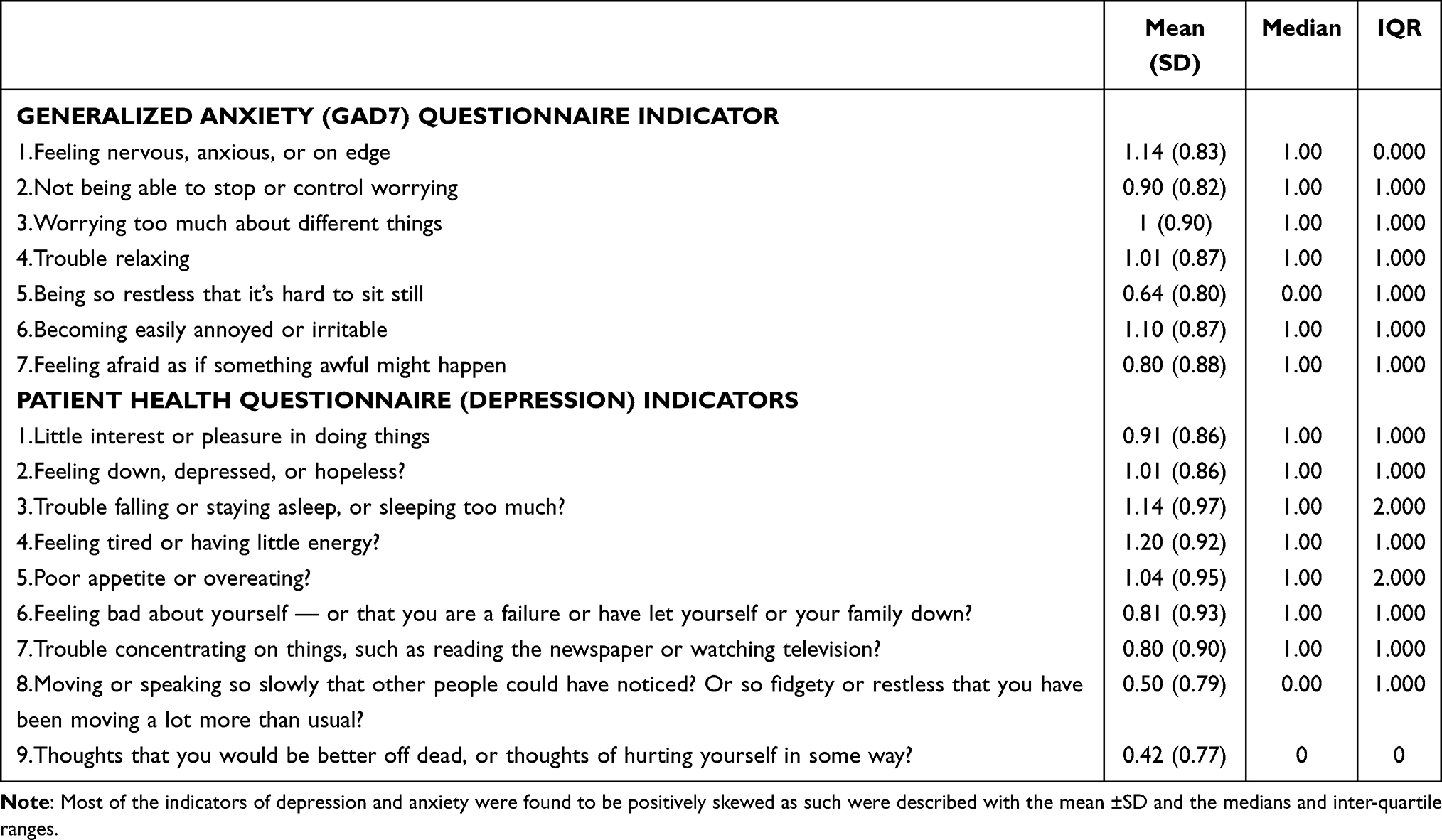 |
Table 4 Descriptive Analysis of People’s Perceptions of the Indicators of Anxiety and Depression |
Most of the indicators of depression and anxiety were found to be positively skewed as such, were described with the mean ±SD and the medians and inter-quartile ranges.
Table 5 displays the findings for the descriptive analysis of people’s overall perceptions of anxiety and depression. The yielded results showed that people’s overall mean perceived Generalized Anxiety (GAD7) score was 6.48 (4.62), also considering the anxiety levels, note Figure 2, it was found that 36.6% of people were considered to have low anxiety, while 42.4% were considered to have mild anxiety. Moreover, people’s perceived depression was rated with a mean collective score of 7.82 (5.76). Most were considered to have mild followed by minimal depression accounting for 36.7%, 31.9% respectively, whereas only 4.8% reported severe depression level Figure 3.
 |
Table 5 Descriptive Analysis of People’s Overall Perceptions of Anxiety and Depression |
 |
Figure 2 The percentage of people with different anxiety perceived levels. |
 |
Figure 3 The percentage of people with different perceived depression levels. |
The Non-Linear Factor Analysis was applied to people’s measured EC and tobacco cigarette consumption indicators to reduce them into a single latent continuous factor that can characterize their nicotine dependence. The resulting analysis finding displayed in Table 6, showed that the six indicators had loaded saliently and positively (well ≥0.690) to a single latent factor that explained 66.7% of the variability between people on their nicotine dependence and consumption types. Therefore, people who scored higher on the latent nicotine dependence factor score tended to consume more tobacco and EC and were inclined to more daily consumption of both types and vice versa. According to the Categorical Cronbach’s alpha test, the six indicators were internally consistent, denoting that people had read and understood them equally reliably. The analysis program computed the nicotine factor score and expressed it as a Z-score with a mean = zero and an SD = 1. However, we converted it into a T-score to analyze it using the multivariable regression analysis.
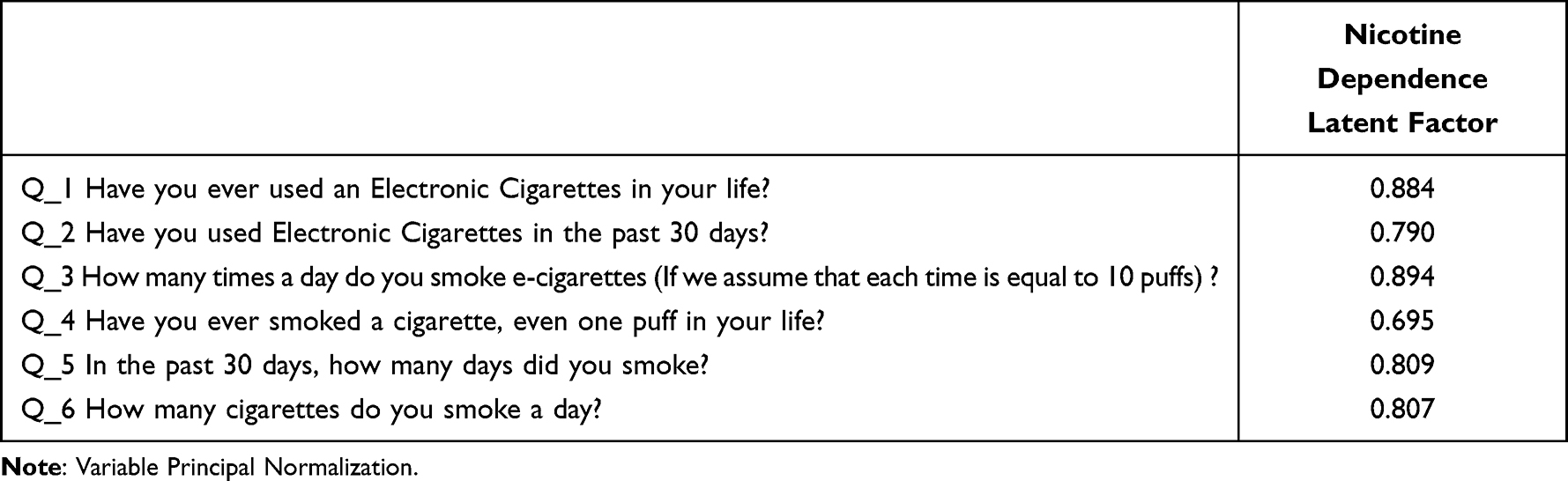 |
Table 6 Categorical Factor Analysis Component Analysis Yielded Item-Factor Loadings |
The Bivariate Spearman’s (Rho) test analysis, Table 7, showed that the people’s mean perceived anxiety and depression scores had correlated positively and significantly with each other’s, rho = 0.724, p <=0.010, denoting that as people’s anxiety score tended to rise their mean perceived depression score tended to rise significantly accordingly and vice versa. Also, the resulting factor analysis-based nicotine dependence score had correlated positively and significantly but very weakly with people’s depression mean perceived (PHQ9) score, rho = 0.10, p-value < =0.010, denoting that people who consume more nicotine products tended to perceive greater depression in general. From another hand, people’s perceived mean anxiety score and their nicotine dependence score did not correlate significantly.
 |
Table 7 Bivariate Spearman Correlations Between the Measured Perceptions |
The Multivariable Generalized Linear Models with Gamma Regression was applied to people’s mean perceived Nicotine dependence factor based score, the resulted findings, shown in Table 8, males were found to be significantly more inclined to nicotine dependence (1.157 times more, or 15.7% times higher) compared to females, p-value < 0.001. Also, the resulted analysis model showed that people’s sex had correlated significantly and negatively with their nicotine dependence factor score, people aged ≥66 years were found to be significantly less predicted to nicotine dependence (9.57% times less) compared to those aged 18–25 years old, p-value=0.001, also people aged between 56–65 years were found to be significantly less inclined to nicotine dependence (5.3% times less) compared to people aged 18–25 years, p-value=0.019, and people aged between 46 and 55 years were found to be significantly less predicted to nicotine dependence (5.2% times less) compared to people aged 18–25 years, p-value=0.001, but also people aged between 36 and 45 years were found to be significantly less predicted to nicotine dependence (4.6% times less) compared to people aged between 18 and 25 years, p-value = 0.001. People aged between 26 and 35 years did not differ significantly from those aged between 18 and 25 years with respect to their mean perceived nicotine dependence, p-value=0.273. Also, people’s nationality did not converge significantly on their perceived nicotine dependence score.
 |
Table 8 Generalized Multivariate Linear Gamma Regression Analysis for People’s Perceived Nicotine Dependence T-Score. N=2293 |
The resulted analysis findings also showed that people residing in different KSA provinces differed significantly with respect to their mean perceived nicotine dependence, people residing in Southern, northern, Eastern and western provinces) measured significantly lower mean perceived nicotine dependence when compared to people residing in the central regions on average, p-value < 0.001 each respectively, note Figure 4. Also, people’s education had correlated negatively with their perceived nicotine dependence score, people educated with a PhD level were found to be significantly less predicted (5.7% times less) to nicotine dependence compared to people with primary and intermediate education level on average, p-value = 0.0200, also people educated with Master’s degree were found to be significantly less predicted (6.2% times less) to nicotine dependence compared to those with primary and intermediate educational levels, p-value=0.003, but people with university degree and those with high school educational levels did not differ significantly with respect to their nicotine dependence compared to those with primary and intermediate educational levels, p > 0.050 each, respectively. People’s employment state levels did not differ significantly with respect to their nicotine dependence except people employed in the private sector were found to be significantly more predicted to nicotine dependence (8.2% times more) when compared to the students, p-value < 0.001. Moreover, people’s mean Body mass index (BMI) and their perceived anxiety scores did not correlate significantly with their mean nicotine dependence score, but people’s mean perceived depression (PHQ9) score had converged positively and significantly on their mean perceived nicotine dependence factor score, for each additional one points rise in people’s perceived PHQ9 depression score their mean predicted nicotine factor score tended to rise by a factor equal to 0.4% times higher on average, p-value < 0.001, depression predicted more nicotine use and consumption as such.
 |
Figure 4 The association between people’s residence and their perceived Nicotine dependence T-score. |
Also, the resulted analysis model showed that people’s sex had correlated significantly and negatively with their nicotine dependence factor score, people aged ≥66 years were found to be significantly less predicted to nicotine dependence (9.57% times less) compared to those aged 18–25 years old, p-value=0.001, also people aged between 56 and 65 years were found to be significantly less inclined to nicotine dependence (5.3% times less) compared to people aged 18–25 years, p-value=0.019, and people aged between 46 and 55 years were found to be significantly less predicted to nicotine dependence (5.2% times less) compared to people aged 18–25 years, p-value=0.001, but also people aged between 36 and 45 years were found to be significantly less predicted to nicotine dependence (4.6% times less) compared to people aged between 18 and 25 years, p-value = 0.001.
Parameter Estimates
To understand better what may explain people’s perceived Generalized Anxiety (GAD7 score) the multivariable Generalized Linear Models with Gamma Regression was applied to people’s mean perceived generalized anxiety score regressing it against people’s sociodemographic and nicotine dependence-related factors. The yielded multivariable findings, Table 9 showed that male people were found to be significantly less predicted (9.8% times less) to anxiety compared to females on average, p-value < 0.001. People’s age groups also differ significantly with respect to their mean perceived GAD7 score, people aged between 46 and 55 years were found to be significantly more inclined to anxiety (12.1% times more) on average compared to people aged between 18 and 25 years, p-value = 0.002, also people aged between 36 and 45 years measured significantly higher mean perceived GAD score (12.3% times higher) on average compared to those people aged between 18 and 25 years, p-value < 0.001, and people aged between 26 and 35 years were also found to be significantly more inclined to anxiety (7.5% times more) compared to those aged between 18 and 25 years on average, p-value = 0.013. Nonetheless, people’s educational level and body mass index (BMI) and occupation did not correlate significantly with their mean perceived generalized anxiety score. Not unexpectedly, people’s mean perceived depression score had correlated positively and significantly statistically with their mean perceived anxiety score, for each additional one points rise in people’s perceived PHQ9 depression score their mean perceived anxiety score tended to rise by a factor equal to 8.2% times higher on average, p-value < 0.001. People’s days of smoking cigarettes did not correlate significantly with their mean perceived anxiety score, but their number of daily smoked cigarettes had loaded significantly and positively on their mean perceived anxiety score, those people who smoked ≥31 cigarettes per day were found to be significantly more predicted to anxiety (5.7% times more) compared to those who smoked <30 cigarettes per day or those who do not smoke cigarettes at all. In background iterative analysis models the nicotine dependence factor score and other e-cigarettes use and consumption factors did not correlate with people’s mean perceived anxiety, as such those factors were dismissed from the analysis model shown in this paper.
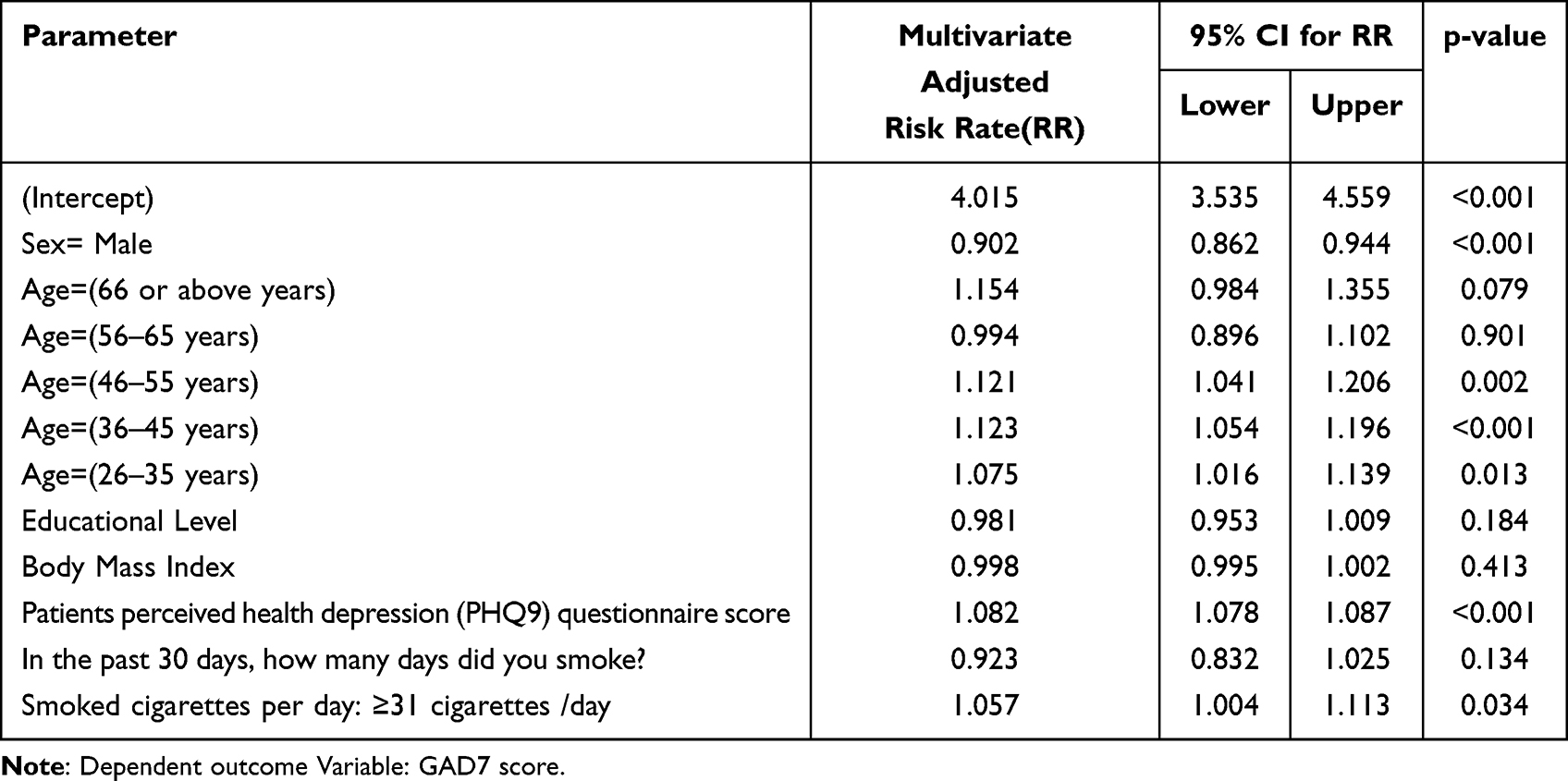 |
Table 9 Generalized Multivariate Linear Gamma Regression Analysis for People’s Perceived Generalized Anxiety (GAD7) Score |
Table 10 displays the resulted multivariable Generalized Linear Models analysis with Gamma regression for people’s mean perceived depression score. The resulted findings showed that males were found to be significantly less inclined to depression (15.2% times less) compared to females on average, p-value < 0.001. Also, people in different age groups had differed significantly with respect to their mean perceived PHQ9 depression score, people aged 66 years and above were found to be significantly less predicted to depression (33.6% times less) compared to people aged 18–25 years on average, p-value < 0.001, also people aged between 56 and 65 years were found to be significantly less inclined to depression (16.9% times less) compared to those aged between 18 and 25 years, p-value = 0.017, but also people aged between 46 and 55 years were found to be significantly less predicted (17% times less) compared to those aged between 18 and 25 years, p-value = <0.001. Not only so but also people aged between 36 and 45 years were found to be significantly less inclined to depression (13.7% times less) compared to those aged between 18 and 25 years on average, p-value = 0.001. People’s employment state had correlated significantly with their mean perceived depression score, the retired people indeed were found to be significantly less inclined to depression (14.7% times less) compared to students, p-value = 0.027, also people in governmental jobs were found to be significantly less predicted to depression (8.4% times less) on average compared to students, p-value = 0.036. People's educational level and residence location did not correlate significantly with their depression levels. However, people’s mean perceived generalized anxiety (GAD7) score had correlated positively with their mean perceived Depression score, for each additional one points rise in people’s perceived anxiety score their mean predicted PHQ depression score tended to rise by a factor equal to 11.4% times higher on average by considering the other predictors in the analysis model as accounted for nevertheless, p-value < 0.001. Too, the analysis model showed that people’s body mass index (BMI) had converged positively on their mean perceived depression score, for each additional one points rise in people’s BMI score their mean perceived depression score tended to rise by a factor equal to 10.4% times higher on average, p-value = 0.038. Not only that but also people’s mean Nicotine dependence factor score had correlated significantly positively with their mean perceived depression score, as their nicotine dependence factor score tended to rise by one standard points on average their mean predicted depression score tended to rise by a factor equal to 10.6% times higher on average, p-value < 0.001. People’s other measured sociodemographic factors and variables did not correlate significantly with their mean perceived depression score.
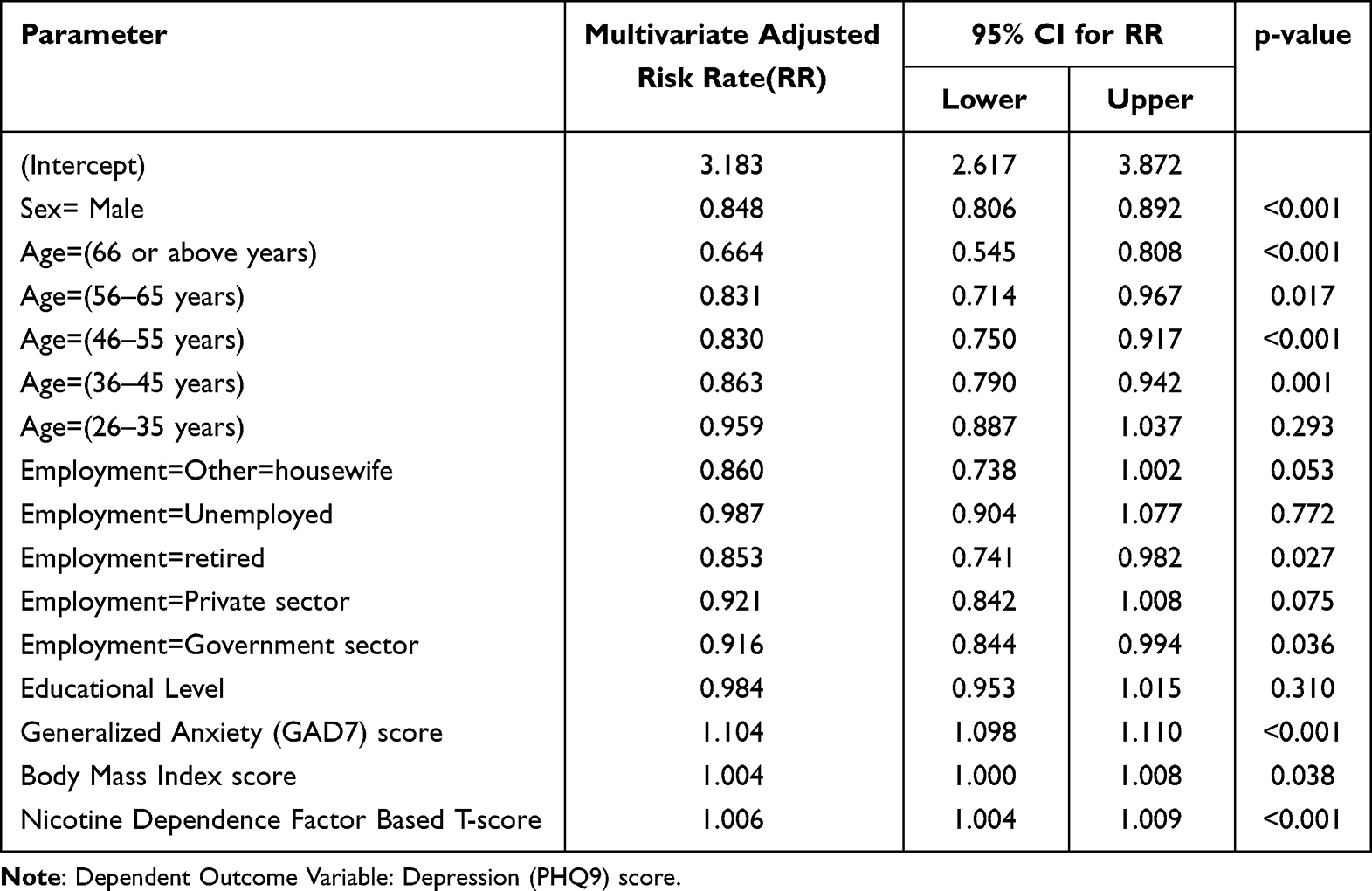 |
Table 10 Generalized Multivariate Linear Gamma Regression Analysis for People’s Perceived Depression (PHQ9) Score |
Discussion
In this nationally representative sample of the general population in Saudi Arabia, poorer mental health functioning was found to be associated with tobacco and EC use. The prevalence of tobacco smoking and EC use in the last 30 days, “current smokers” was 21.6% and 21.1%, respectively. Our findings regarding tobacco smoking prevalence are consistent with recently published papers.19–24 In terms of cigarette smoking prevalence among the general population 34.4% was the highest prevalence reported in the literature while 12.2% was the lowest.25,26 Aljoharah M et al investigated the prevalence of cigarette smoking among the general population and found it to be 21.4%, similar to our findings.27 Few studies have investigated the impact of gender variation on the association between EC use and mental health. Female EC users were found to have higher adverse mental health than males, which supports the findings of our study.28,29 Sung B reported that women were more likely to develop depression than men.30 A recent survey among EC users revealed that depression was positively associated with EC use. Additionally, depressive episodes were reported to be approximately 15% and 25% in males and females, respectively.30 Lee J and Oh M found a strong association between vaping and gender.31 Unlike males, females were less likely to used vape.31,32 However, another study showed greater EC use among women than men.33 Furthermore, the lifetime prevalence of anxiety was reported to be higher in females than males, which is consistent with the current study.34 Higher odds of vaping were found among high school graduates, those with some college education, and college grads than among those with only a high school diploma.31 In this study, unemployed participants showed a positive correlation between using EC and self-reported depression; this finding is supported by a recent study that revealed that EC use was associated with depression and unemployment in adults, even after adjusting for potential confounders.35 Evidence shows that people without jobs experience depression or other depressive symptoms more frequently than employed people.36 As nicotine smoking dysregulates coping mechanisms for depression, external stressors as unemployment might further impact the mental health of individuals.37
In the current study, the mean nicotine dependence score correlated significantly with perceived depression which was assessed using the PHQ-9 scale. Similar results were reported in a study published in 2023 that investigated EC nicotine dependence and depressive symptoms among adolescents, revealing that 88% who reported depressive symptoms on screening with PHQ-9 also suffered from EC nicotine dependence.38 Additionally, it has been reported that exposure to EC, whether current or former use, is associated with an increased risk for depression compared to those who never used EC.30 Moreover, a study published in 2017 among college students concluded that depressive symptoms could predict EC use and not vice versa.39 However, recent scientific evidence suggest that EC use is associated with mental health status.40 A recent study assessing the association between EC use and depressive symptoms in adolescents found that adolescents with depressive symptoms had increased odds of EC use.40 Furthermore, another study revealed that over 60% of smokers with mental health conditions were more susceptible to using EC than smokers without psychiatric disorders.30 EC use was associated with depression, suicidal ideation, and suicidal attempts, which were significantly higher compared to non-EC users.41
Additionally, higher rates of depressive and anxiety symptoms were significantly associated with EC use.42 Furthermore, higher rates of anxiety were observed in EC users compared to non-users.42 The current study found that people’s smoking days did not correlate significantly with the mean perceived anxiety score. However, the daily smoking frequency greatly affected their mean perceived anxiety score. Lastly, in the current study, the perceived anxiety score positively impacted the perceived depression score and vice versa. This finding is consistent with the literature, which found that anxiety and depression commonly coexist with an approximate prevalence of 41%.43,44
Despite the comprehensiveness of this research in reporting the prevalence of EC use and its association with mental health status, namely depression, and anxiety, among the adult general population of Saudi Arabia, there are certain limitations. The study design is cross-sectional, which limits the ability to demonstrate causation. Additionally, the mode of data collection was based on self-reported electronic surveys, which increases the possibility for bias, specifically non-response bias and social desirability bias which might have affected the results. However, this study has multiple strengths, including the validity of the scales used to assess mental health status and a large representative sample that reflects the five main residential areas of Saudi Arabia, which positively impacts the generalizability of this study.
Conclusion
In conclusion, the finding of the current study supports the international literature. Most of the participants were females, in the age group 18–25 residing with a university educational level residing in either the central or eastern regions of Saudi Arabia. 31.6% of the participants reported trying EC use in their lifetime, while 21.1% confirmed continuous EC use in the past 30 days. 36.6% of people were found to have low anxiety, while 42.4% had mild anxiety. Furthermore, 36.7% were considered to have mild and minimal depression accounting for 36.7% and 31.9%, respectively. The results revealed that people’s top perceived indicator of anxiety was feeling nervous, anxious, and on edge; followed by becoming easily annoyed and having trouble relaxing. Whereas people’s top perceived indicator of depression was feeling tired or having little energy; followed by trouble falling or staying asleep, losing appetite, or overeating and feeling down and depressed, followed by having little interest/pleasure in doing things. The Mean nicotine dependence factor score correlated significantly with the mean perceived depression score.
Institutional Review Board Statement
The study was approved by the IMSIU Research Ethics Committee (project number: 407/2023, approval date: 20/01/2023) All writing was done in accordance with the ethical principles of the Declaration of Helsinki. The survey link included a brief study description and a more detailed explanation on the front page. Participants were told that completion of the survey constituted consent. All participant consent and data were collected in complete confidence throughout the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that there is no conflict of interest concerning the publication of this article.
References
1. CDCTobaccoFree. 2016 SGR: e-Cigarette Use Among Youth and Young Adults. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/tobacco/sgr/e-cigarettes/index.htm.
2. National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Population Health and Public Health Practice, Committee on the Review of the Health Effects of Electronic Nicotine Delivery Systems. Public Health Consequences of E-Cigarettes. Eaton DL, Kwan LY, Stratton K, editors. Washington, D.C., DC: National Academies Press; 2018. doi:10.17226/24952
3. Alsanosy RM. Smokeless tobacco (shammah) in Saudi Arabia: a review of its pattern of use, prevalence, and potential role in oral cancer. Asian Pac J Cancer Prev. 2014;15(16):6477–6483. doi:10.7314/apjcp.2014.15.16.6477
4. CDCTobaccoFree. Electronic cigarettes. Centers for Disease Control and Prevention. 2022. Available from: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/index.htm.
5. Pan L, Morton J, Mbulo L, Dean A, Ahluwalia IB. Electronic cigarette use among adults in 14 countries: a cross-sectional study. EClinicalMedicine. 2022;47(101401):101401. doi:10.1016/j.eclinm.2022.101401
6. Czoli CD, Hammond D, White CM. Electronic cigarettes in Canada: prevalence of use and perceptions among youth and young adults. Can J Public Health. 2014;105(2):e97–102. doi:10.17269/cjph.105.4119
7. Althobaiti NK, Mahfouz MEM. Prevalence of electronic cigarette use in Saudi Arabia. Cureus. 2022;14(6):e25731.
8. World Health Organization.Promoting Mental Health: Concepts, Emerging Evidence, Practice: Summary Report / a Report from the World Health Organization, Department of Mental Health and Substance Abuse in Collaboration with the Victorian Health Promotion Foundation and the University of Melbourne. World Health Organization; 2004. https://apps.who.int/iris/handle/10665/42940.
9. Groenman AP, Janssen TWP, Oosterlaan J. Childhood psychiatric disorders as a risk factor for subsequent substance abuse: a meta-analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(7):556–569. doi:10.1016/j.jaac.2017.05.004
10. King JL, Reboussin BA, Spangler J, Cornacchione Ross J, Sutfin EL. Tobacco product use and mental health status among young adults. Addict Behav. 2018;77:67–72. doi:10.1016/j.addbeh.2017.09.012
11. Conway KP, Green VR, Kasza KA, et al. Co-occurrence of tobacco product use, substance use, and mental health problems among youth: findings from wave 1 (2013-2014) of the population assessment of tobacco and health (PATH) study. Addict Behav. 2018;76:208–217. doi:10.1016/j.addbeh.2017.08.009
12. Chaiton M, Cohen JE, Rehm J, Abdulle M, O’Loughlin J. Confounders or intermediate variables? Testing mechanisms for the relationship between depression and smoking in a longitudinal cohort study. Addict Behav. 2015;42:154–161. doi:10.1016/j.addbeh.2014.11.026
13. Smith TC, LeardMann CA, Smith B, et al. Longitudinal assessment of mental disorders, smoking, and hazardous drinking among a population-based cohort of US service members. J Addict Med. 2014;8(4):271–281. doi:10.1097/adm.0000000000000050
14. Mojtabai R, Crum RM. Cigarette smoking and onset of mood and anxiety disorders. Am J Public Health. 2013;103(9):1656–1665. doi:10.2105/AJPH.2012.300911
15. Taylor G, McNeill A, Girling A, Farley A, Lindson-Hawley N, Aveyard P. Change in mental health after smoking cessation: a systematic review and meta-analysis. BMJ. 2014;348(feb13 1):g1151. doi:10.1136/bmj.g1151
16. Becker TD, Arnold MK, Ro V, Martin L, Rice TR. A systematic review of electronic cigarette use (vaping) and mental health comorbidity among adolescents and young adults. Nicotine Tob Res. 2021;23(3):415–425. doi:10.1093/ntr/ntaa171
17. Park SH, Lee L, Shearston JA, Weitzman M. Patterns of electronic cigarette use and level of psychological distress. PLoS One. 2017;12(3):e0173625. doi:10.1371/journal.pone.0173625
18. Cambron C. E-cigarette use is associated with increased psychological distress among youth: a pooled cross-sectional analysis of state-level data from 2019 and 2021. Int J Environ Res Public Health. 2022;19(18). doi:10.3390/ijerph191811726
19. Alasqah I, Mahmud I, East L, Usher K. A systematic review of the prevalence and risk factors of smoking among Saudi adolescents. Saudi Med J. 2019;40(9):867–878. doi:10.15537/smj.2019.9.24477
20. Alotaibi SA, Alsuliman MA, Durgampudi PK. Smoking tobacco prevalence among college students in the Kingdom of Saudi Arabia: systematic review and meta-analysis. Tob Induc Dis. 2019;17(April):35. doi:10.18332/tid/105843
21. Bin Abdulrahman KA, Alghamdi HA, Alfaleh RS, et al. Smoking habits among college students at a public university in Riyadh, Saudi Arabia. Int J Environ Res Public Health. 2022;19(18):11557. doi:10.3390/ijerph191811557
22. Al-Mohamed HI, Amin TT. Pattern and prevalence of smoking among students at King Faisal University, Al Hassa, Saudi Arabia. East Mediterr Health J. 2010;16(1):56–64.
23. Jarallah JS, al-Rubeaan KA, al-Nuaim AR, al-Ruhaily AA, Kalantan KA. Prevalence and determinants of smoking in three regions of Saudi Arabia. Tob Control. 1999;8(1):53–56. doi:10.1136/tc.8.1.53
24. Tahir M. Smoking and its risks in Saudi Arabia: a literature review. Hamdan Med J. 2019;12(4):152.
25. Siddiqui S, Ogbeide DO, Al Khalifa I. Smoking in a Saudi community: prevalence, influencing factors, and risk perception. Fam Med. 2001;33(5):367–370.
26. Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: findings from a national survey. BMC Public Health. 2015;15(1):611. doi:10.1186/s12889-015-1902-3
27. Algabbani AM, Almubark R, Althumiri N, Alqahtani A, BinDhim N. The prevalence of cigarette smoking in Saudi Arabia in 2018. Food Drug Regulatory Sci J. 2018;1(1):1.
28. Smith CA, Shahab L, McNeill A, Jackson SE, Brown J, Brose L. Harm perceptions of E-cigarettes among smokers with and without mental health conditions in England: a cross-sectional population survey. Nicotine Tob Res. 2021;23(3):511–517. doi:10.1093/ntr/ntaa020
29. Pham T, Williams JVA, Bhattarai A, Dores AK, Isherwood LJ, Patten SB. Electronic cigarette use and mental health: a Canadian population-based study. J Affect Disord. 2020;260:646–652. doi:10.1016/j.jad.2019.09.026
30. Sung B. Gender difference in the association between E-cigarette use and depression among US adults. Osong Public Health Res Perspect. 2021;12(1):13–19. doi:10.24171/j.phrp.2021.12.1.03
31. Lee J, Oh M. The moderating effect of gender on the association between E-cigarette use and smoking status: a cross-sectional study. Addict Behav. 2019;93:108–114. doi:10.1016/j.addbeh.2019.01.038
32. Schoenborn CA, Gindi RM. Electronic cigarette use among adults: United States, 2014. NCHS Data Brief. 2015;217:1–8.
33. Levy DT, Yuan Z, Li Y. The prevalence and characteristics of E-cigarette users in the U.s. Int J Environ Res Public Health. 2017;14(10):1200. doi:10.3390/ijerph14101200
34. Faravelli C, Alessandra Scarpato M, Castellini G, Lo Sauro C. Gender differences in depression and anxiety: the role of age. Psychiatry Res. 2013;210(3):1301–1303. doi:10.1016/j.psychres.2013.09.027
35. Saeed OB, Chavan B, Haile ZT. Association between E-cigarette use and depression in US adults. J Addict Med. 2020;14(5):393–400. doi:10.1097/adm.0000000000000604
36. Paul KI, Moser K. Unemployment impairs mental health: meta-analyses. J Vocat Behav. 2009;74(3):264–282. doi:10.1016/j.jvb.2009.01.001
37. Leventhal AM, Zvolensky MJ. Anxiety, depression, and cigarette smoking: a transdiagnostic vulnerability framework to understanding emotion-smoking comorbidity. Psychol Bull. 2015;141(1):176–212. doi:10.1037/bul0000003
38. Winburn C, Ofei-Dodoo S. Nicotine dependence from electronic cigarette use and depressive symptoms among adolescents. Kans J Med. 2023;16(1):1–4. doi:10.17161/kjm.vol16.18723
39. Bandiera FC, Loukas A, Li X, Wilkinson AV, Perry CL. Depressive symptoms predict current E-cigarette use among college students in Texas. Nicotine Tob Res. 2017;19(9):1102–1106. doi:10.1093/ntr/ntx014
40. Gorfinkel L, Hasin D, Miech R, Keyes KM. The link between depressive symptoms and vaping nicotine in U.s. adolescents, 2017-2019. J Adolesc Health. 2022;70(1):133–139. doi:10.1016/j.jadohealth.2021.07.003
41. Javed S, Usmani S, Sarfraz Z, et al. A scoping review of vaping, E-cigarettes, and mental health impact: depression and suicidality. J Community Hosp Intern Med Perspect. 2022;12(3):33–39. doi:10.55729/2000-9666.1053
42. Masaki K, Taketa RM, Nakama MK, Kawamoto CT, Pokhrel P. Relationships between depressive symptoms, anxiety, impulsivity and cigarette and E-cigarette use among young adults. Hawaii J Health Soc Welf. 2022;81(3):51–57.
43. Dunner DL. Management of anxiety disorders: the added challenge of comorbidity. Depress Anxiety. 2001;13(2):57–71. doi:10.1002/da.1018
44. McLaughlin TP, Khandker RK, Kruzikas DT, Tummala R. Overlap of anxiety and depression in a managed care population: prevalence and association with resource utilization. J Clin Psychiatry. 2006;67(8):1187–1193. doi:10.4088/jcp.v67n0803
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.