Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
The Association Between Neighborhood Socioeconomic Disadvantage and Chronic Obstructive Pulmonary Disease
Authors Galiatsatos P, Woo H, Paulin LM, Kind A, Putcha N, Gassett AJ ![]() , Cooper CB
, Cooper CB ![]() , Dransfield MT, Parekh TM, Oates GR, Barr RG, Comellas AP
, Dransfield MT, Parekh TM, Oates GR, Barr RG, Comellas AP ![]() , Han MK, Peters SP
, Han MK, Peters SP ![]() , Krishnan JA
, Krishnan JA ![]() , Labaki WW
, Labaki WW ![]() , McCormack MC
, McCormack MC ![]() , Kaufman JD
, Kaufman JD ![]() , Hansel NN
, Hansel NN
Received 17 November 2019
Accepted for publication 20 April 2020
Published 5 May 2020 Volume 2020:15 Pages 981—993
DOI https://doi.org/10.2147/COPD.S238933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Panagis Galiatsatos,1 Han Woo,1 Laura M Paulin,2 Amy Kind,3,4 Nirupama Putcha,1 Amanda J Gassett,5 Christopher B Cooper,6 Mark T Dransfield,7 Trisha M Parekh,7 Gabriela R Oates,8 R Graham Barr,9 Alejandro P Comellas,10 Meilan K Han,11 Stephen P Peters,12 Jerry A Krishnan,13 Wassim W Labaki,11 Meredith C McCormack,1 Joel D Kaufman,14 Nadia N Hansel1
1Division of Pulmonary and Critical Care Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Pulmonary and Critical Care, Dartmouth Hitchcock Medical Center, Lebanon, NH, USA; 3University of Wisconsin School of Medicine and Public Health, Department of Medicine Health Services and Care Research Program and Division of Geriatrics, Madison, WI, USA; 4Geriatric Research Education and Clinical Center, Wm. S. Middleton Veterans Hospital, Madison, WI, USA; 5Internal Medicine, University of Washington, Seattle, WA, USA; 6Department of Medicine, University of California Los Angeles School of Medicine, Los Angeles, CA, USA; 7Department of Medicine, University of Alabama Birmingham and Birmingham Veterans Affairs Medical Center, Birmingham, AL, USA; 8Department of Medicine, University of Alabama Birmingham, Birmingham, AL, USA; 9Presbyterian Hospital, Columbia University Medical Center, New York, NY, USA; 10Internal Medicine and Pulmonary, University of Iowa, Iowa City, IA, USA; 11Pulmonary and Critical Care Medicine, University of Michigan, Ann Arbor, MI, USA; 12Department of Medicine, Wake Forest University Health Sciences, Winston-Salem, NC, USA; 13Department of Medicine, University of Illinois, Chicago, IL, USA; 14Office of the Dean, University of Washington School of Public Health, Seattle, WA, USA
Correspondence: Panagis Galiatsatos
Johns Hopkins University School of Medicine, 4940 Eastern Avenue, Asthma and Allergy Building, 4th Floor, Baltimore, MD 21224, USA
Tel +1410 550-0522
Fax +1410 550-1094
Email [email protected]
Rationale: Individual socioeconomic status has been shown to influence the outcomes of patients with chronic obstructive pulmonary disease (COPD). However, contextual factors may also play a role. The objective of this study is to evaluate the association between neighborhood socioeconomic disadvantage measured by the area deprivation index (ADI) and COPD-related outcomes.
Methods: Residential addresses of SubPopulations and InteRmediate Outcome Measures in COPD Study (SPIROMICS) subjects with COPD (FEV1/FVC < 0.70) at baseline were geocoded and linked to their respective ADI national ranking score at the census block group level. The associations between the ADI and COPD-related outcomes were evaluated by examining the contrast between participants living in the most-disadvantaged (top quintile) to the least-disadvantaged (bottom quintile) neighborhood. Regression models included adjustment for individual-level demographics, socioeconomic variables (personal income, education), exposures (smoking status, packs per year, occupational exposures), clinical characteristics (FEV1% predicted, body mass index) and neighborhood rural status.
Results: A total of 1800 participants were included in the analysis. Participants residing in the most-disadvantaged neighborhoods had 56% higher rate of COPD exacerbation (P< 0.001), 98% higher rate of severe COPD exacerbation (P=0.001), a 1.6 point higher CAT score (P< 0.001), 3.1 points higher SGRQ (P< 0.001), and 24.6 meters less six-minute walk distance (P=0.008) compared with participants who resided in the least disadvantaged neighborhoods.
Conclusion: Participants with COPD who reside in more-disadvantaged neighborhoods had worse COPD outcomes compared to those residing in less-disadvantaged neighborhoods. Neighborhood effects were independent of individual-level socioeconomic factors, suggesting that contextual factors could be used to inform intervention strategies targeting high-risk persons with COPD.
Keywords: health disparities, COPD, area deprivation index
Introduction
Lower individual socioeconomic status (SES) has widely been accepted to be linked to chronic disease morbidity;1,2 however, contextual-level (specifically, neighborhood) socioeconomic risk factors can influence health outcomes independently of commonly measured patient-level factors.3–5 For example, individuals who live in both poor households and poor neighborhoods may have worse chronic health outcomes compared to poor individuals who live in less disadvantaged neighborhoods in the United States (US).6,7 Further, when moving to less disadvantaged neighborhoods, without changing individual socioeconomic factors, low-income families have shown positive health benefits,8,9 highlighting that neighborhood disadvantage is an additional risk factor beyond personal disadvantage. However, the effect of neighborhood disadvantage on chronic obstructive pulmonary disease (COPD) outcomes in the US is unknown. While COPD affects a significant portion of persons in the US, is a substantial cause of morbidity and mortality, and has known disparities in regards to disease incidence and prevalence,10,11 the dearth of insight into understanding the relationship between neighborhoods of the US and COPD-related outcomes warrants investigation.
We explored whether neighborhood disadvantage is associated with COPD-related health outcomes, and whether this relationship is independent of individual-level SES factors. We used information captured in the SubPopulations and InteRmediate Outcome Measures in COPD Study (SPIROMICS)12 and the SPIROMICS AIR13 study. Neighborhood disadvantage was measured by the Area Deprivation Index (ADI), a validated, publicly available geospatial index of socioeconomic disadvantage constructed from US Census data and updated to incorporate 2013 American Community Survey data.14,15 A well-established composite measure of socioeconomic disadvantage for all areas of the United States, it reliably drills down to the highly discrete geographic units (block groups) and has been associated with several chronic health outcomes.3,15-17
We hypothesized that participants from more disadvantaged neighborhoods within the United States have worse COPD-related outcomes than patients from more affluent areas.
Methods
Study Population
SPIROMICS is a multicenter prospective cohort study that has enrolled geographically diverse patients with COPD, along with smokers without COPD and non-smokers, across 12 US sites.12 Participants were aged 40 to 80 years old at enrollment and provided current home addresses. The study design and inclusion and exclusion criteria have been previously detailed.12 The research protocol for SPIROMICS was approved by the institutional review boards at all participating institutions (Supplemental File), and written informed consents were obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki. We analyzed data from the baseline visit of participants with COPD, defined as post-bronchodilator FEV1/FVC less than 0.70.
Measures
Area Deprivation Index (ADI)
Participants’ addresses were used to identify their respective US Census block group, and block groups were matched to their respective national-level ADI ranking. The ADI reports a value from 1 (least disadvantaged) to 100 (most disadvantaged) and is freely available at www.neighborhoodatlas.medicine.wisc.edu. The ADI is a composite score constructed from 17 indicators in the domains of income, education, housing, employment, home and vehicle ownership, and family structure weighted by factor score coefficients for each indicator.15,16
Individual Socioeconomic Status (SES)
Education (more than high school vs. high school or less), income (≤$49,000, ≥$50,000, or Decline to answer), and marital status (married vs. not married) were assessed by questionnaire at baseline.
Other Covariates
Additional covariates included age, gender (female vs. male), race (white vs. non-white), body mass index, FEV1% predicted,18,19 smoking status (current vs. former), pack years, and self-report of occupational exposure to vapor, dust, gas or fumes in the longest held job (ever exposed vs. never exposed).20 For about 10% of the sample who answered “don’t know” to the occupational exposure question, we grouped them together with those who answered “yes” to the question. The rural/non-rural status of one’s residence was also determined.21
Outcome Measures
Functional status was measured by 6MWD.22 Respiratory symptoms were obtained through the COPD Assessment Test (CAT),23 and dyspnea was measured by the modified Medical Research Council (mMRC) dyspnea score.24 Cough and sputum were measured using the total score from the Ease of Cough and Sputum questionnaire.25 Respiratory-specific quality of life was measured by the St. George’s Respiratory Questionnaire (SGRQ).26 Anxiety and depression were measured using the Hospital Anxiety and Depression Scale (HADS).27 Inspiratory and expiratory chest CT were used to determine percentage of gas trapping (percent −856 Hounsfield units on expiration), airway wall thickness by the square root of wall area for a theoretical airway with 10mm lumen (pi10), and percentage of emphysema (percent below −950 Hounsfield units at inspiration).28–30
COPD exacerbations following enrollment were collected by quarterly phone calls and annual clinical visits for up to 3 years. Exacerbations were self-reported by participants based on oral antibiotic or steroid use for worsening respiratory symptoms; severe exacerbations were defined as worsening in respiratory symptoms leading to emergency department (ED) visit or hospitalization. We used the total count of exacerbation (and severe exacerbation), measured prospectively from the start of the study, as our outcome measures.
Statistical Analysis
Variable distributions were examined and measures of central tendency were assessed using descriptive analyses. Participants were dichotomized into below- and above-median for ADI national ranking. Participant characteristics, ADI, and COPD outcomes were compared by t-tests for continuous variables and chi-squared test for categorical variables. To assess the associations between ADI national ranking score and COPD outcomes, ADI was modeled continuously and in quintiles. We ran multivariable regression analyses adjusting for age, sex, race, education, income, marital status, rural status, BMI, FEV1% predicted, smoking status, pack years, and occupational exposure. We used generalized linear mixed model (GLMM) with robust standard error estimator, employing link functions for continuous and count outcomes as appropriate, and specified clinical centers as random intercept to account for clustering of observations within study sites. For continuous ADI, we estimated the predicted difference in outcome for one standard deviation increase in ADI adjusting for covariates; for quintiles, we estimated the predicted difference in outcome between the highest quintile (the most-disadvantaged neighborhood) and the lowest quintile (the least-disadvantaged neighborhood) adjusting for covariates, and tested the linear trends by modeling quintiles as an ordinal variable. As a sensitivity analysis, we performed all our regression analyses using study sites as fixed effect instead of random effect.
We additionally assessed—based on a priori hypothesis—whether residing in rural areas (vs. non-rural areas) modified the association between the continuous ADI and COPD-outcomes. We ran two-way interaction regression analyses with the multiplicative interaction term between ADI and rural status specified. We evaluated the direction and statistical significance of the interaction term, and obtained the effect estimates of the continuous ADI at rural and non-rural areas using linear combination tests. As a sensitivity analysis, we ran stratified analysis by rural status, and tested the constant covariate effect assumption across rural status.
Standard regression diagnostics were performed, including testing of linearity assumption by fractional polynomial model approach, normality assumption by Q–Q plots of residuals, heteroscedasticity with Breusch–Pagan test, and model fit by log-likelihood ratio tests and Akaike and Bayesian Information Criteria. All analyses were completed using STATA version 15.1 (College Station, TX). Statistical significance was defined as P<0.05 for main effects and P<0.10 for interactions. Missing values were not imputed.
Results
Participant Characteristics
Of the 1829 subjects with COPD, 30 participants had a missing ADI, resulting in 1799 participants included in this cohort for analysis. The mean (standard deviation, ±SD) ADI national ranking was 41.0 ± 29.4 (range, 1 to 100), and the median was 37 (interquartile range 47). Across different levels of our covariates, ADI showed its full range of distribution (Figure 1). Cohort characteristics are further broken down by ADI quintile (Table 1). Participants residing in more disadvantaged neighborhoods had lower education, less income, and were less likely to be married compared to those residing in less disadvantaged neighborhood; they were also younger, and more likely to be females, non-white, current smokers, and live in urban areas. There was no ADI difference for BMI or pack years.
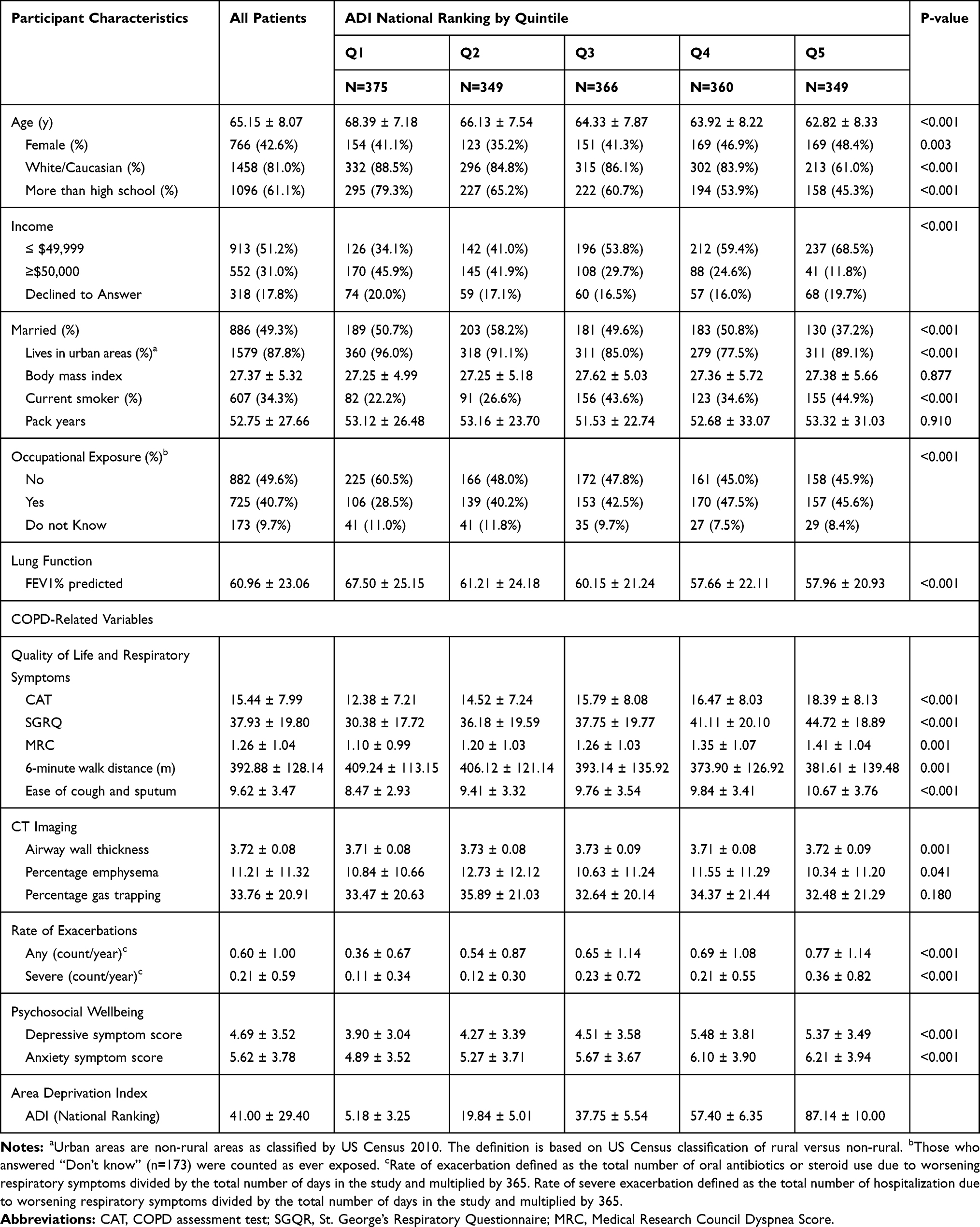 |
Table 1 Patient Characteristics by ADI Quintile |
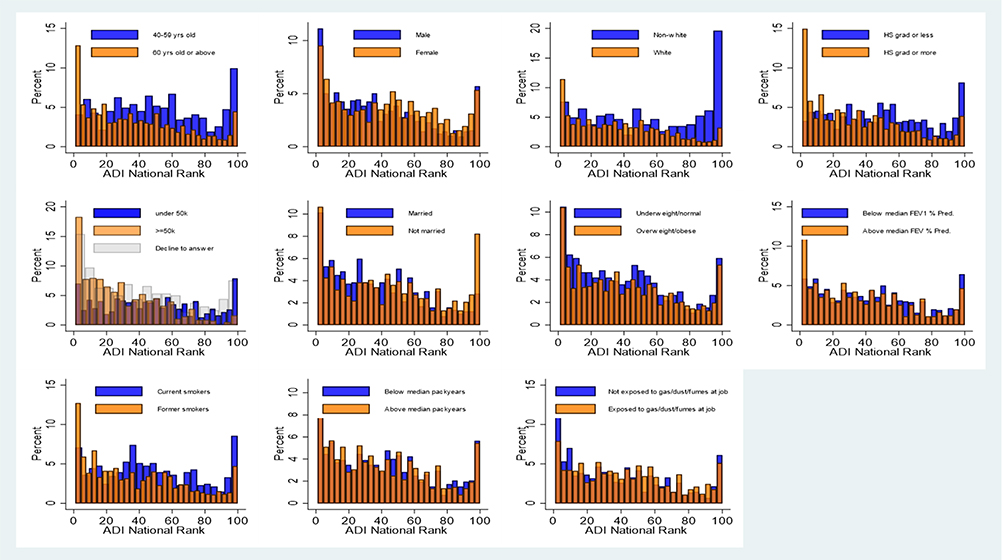 |
Figure 1 Distribution of ADI national rank by covariate levels. For continuous covariates (age, BMI, FEV1% predicted, pack years), the variables were dichotomized in the way it is described in the legends. |
Multivariable Regression
Quintiles ADI
In multivariable regression analyses (adjusting for age, sex, race, education, income, marital status, rural status, BMI, FEV1% Predicted, smoking status, pack years, and occupational exposure to gas/dust/fumes) (Table 2), those residing in the highest quintiles ADI (the most-disadvantaged neighborhoods) had 56% higher rate of COPD exacerbation (P<0.001, P<0.001 for linear trend) and 98% higher rate of severe COPD exacerbation (P=0.001, P<0.001 for linear trend) than those living in the lowest quintiles ADI (the least-disadvantaged neighborhoods) (Figure 2).
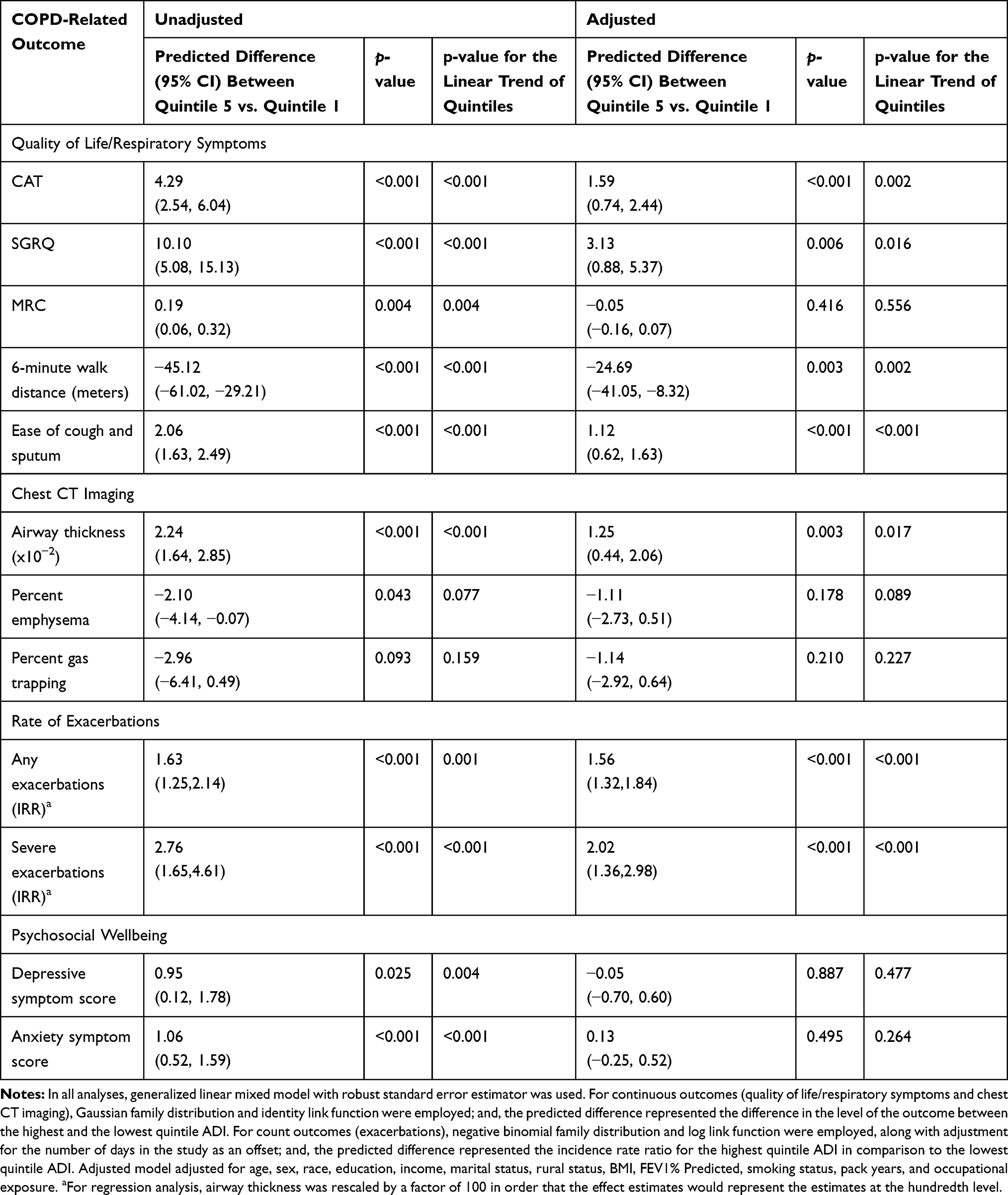 |
Table 2 Regression of COPD-Related Outcomes on Quintile ADI |
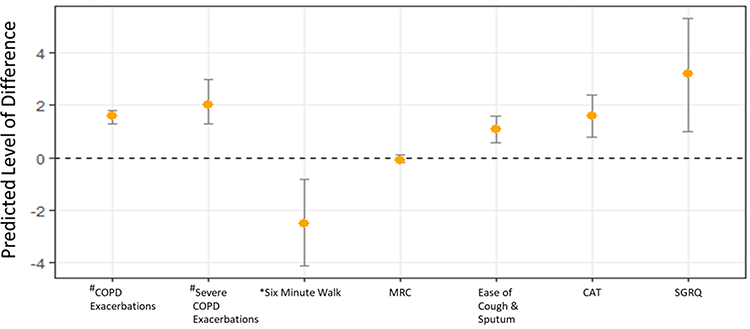 |
Figure 2 Average predicted difference between top and bottom quantile ADI national rank: the most-disadvantaged vs the least-disadvantaged neighborhoods. *Six-minute walk was rescaled by a factor of one-tenth (e.g., the value −2 meters indicates −20 meters). #For exacerbation variables only, Y-axis indicates the rate ratio (e.g., the value of 2 would indicate the rate of exacerbation that is twice as great for the most disadvantaged neighborhood than that for the least disadvantaged). Notes: Y-axis represents the regression coefficient for the most-disadvantaged 20th percentile (with the least-disadvantaged 20th percentile as the reference category) in the fully adjusted regression of outcomes on quintile ADI. |
After adjusting for covariates, similar results of worse COPD outcomes among those residing in disadvantaged neighborhoods were shown with respect to quality of life, respiratory symptoms, and exercise capacity (e.g., 6MWD). Further, health differences between the highest quintile compared to the lowest quintile neighborhoods approached the minimal clinical important difference (MCID) for the respective outcomes. Specifically, individuals with COPD residing in the highest quintile ADI had a 1.6 higher CAT score (P<0.001, P=0.001 for linear trend), 3.1 points higher SGRQ (P=0.005, P=0.014 for linear trend), 24.6 meters less six-minute walk distance (P=0.003, P=0.002 for linear trend), and 1.1 worse Ease of Cough and Sputum score (P<0.001, P<0.001 for linear trend) compared with participants who resided in the lowest quintile ADI. For dyspnea, there was significant association with quantile ADI in the unadjusted model, but when adjusting for covariates, there was no longer a significant association.
In terms of chest CT measures, participants residing in the highest quintile ADI showed higher airway wall thickness (pi10) (β=1.24 x10−2 in multivariate models; P=0.003) than those residing in the lowest quantile. There were no significant differences in gas trapping and emphysema across the quintiles of ADI in both unadjusted and adjusted models.
Continuous ADI
In the multivariable regression analyses in which ADI was modeled as continuous, results were consistent with the quintile analysis, in that, a higher ADI national ranking was associated with higher rate of prospective exacerbations, adjusting for covariates. Specifically, a one SD increase in ADI was associated with a 15% higher rate of COPD exacerbations (IRR=1.15, P=0.002) and 26% higher rate of severe COPD exacerbations (IRR=1.26, P<0.001) (Supplemental Figure 1; Table 3). Similarly, one standard deviation (SD) increase in ADI national ranking score was associated with higher CAT (β=0.6, P<0.001), higher SGRQ (β=0.9, P=0.031), a lower 6MWD (β=−11.0 meters, P<0.001) and worse Ease of Cough and Sputum score (β=0.4, P<0.001). In terms of chest CT metric, a higher ADI was associated with higher airway wall thickness (β=3.3x10−3, P=0.03). ADI was not statistically significantly associated with dyspnea after adjustment with covariates but was associated with the unadjusted model. ADI was not associated with either gas trapping or emphysema in both unadjusted and adjusted models.
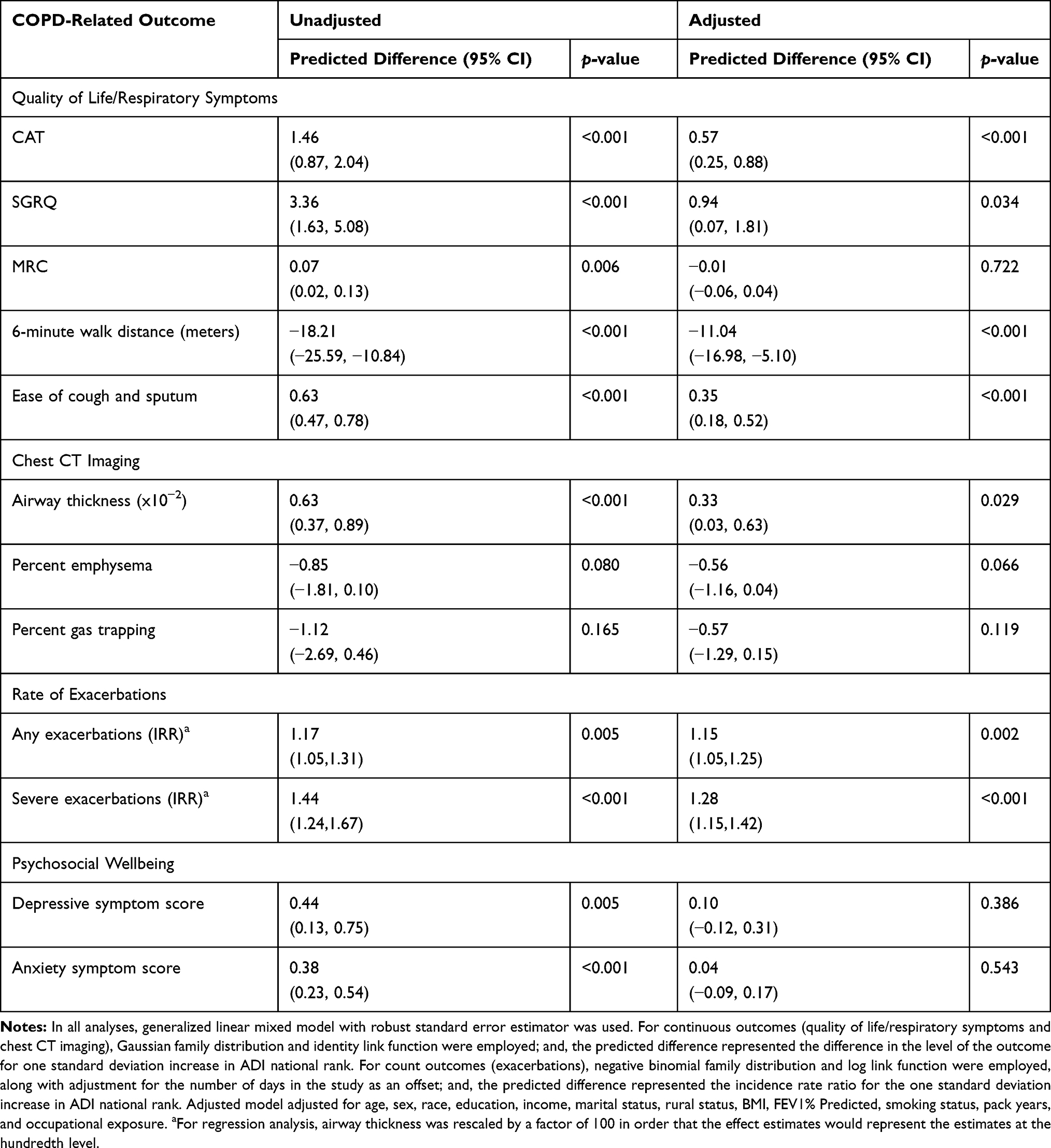 |
Table 3 Regression of COPD-Related Outcomes on Continuous ADI |
ADI Associations by Rural Status
Adjusting for covariates, the continuous ADI’s association with COPD-outcomes varied by rural status for SGRQ (Pint=0.055), dyspnea (Pint=0.038), and 6-minute walk distance (Pint=0.012). In all three outcomes, the association between ADI and outcomes was more adverse for those who reside in rural areas than those residing in non-rural areas (Figure 3). For example, one SD increase in ADI was associated with 36.2 fewer meters walked in 6MWD for those residing in rural areas (β=−36.2, P=0.001) while only 8.8 fewer meters walked for those residing in non-rural areas (β=−8.8, P=0.008). A one standard deviation increase in ADI was associated with a 3.8 increase of the SGRQ score (P=0.014) among hose residing in rural areas, but no association was shown for those residing in non-rural areas (β=0.7, P=0.125). In the case of dyspnea, the difference in the association by rural status (i.e., interaction) was significant with a trend towards worse dyspnea with increasing ADI (β=0.159, p=0.060) only among those in rural areas. There was no significant ADI-rural status interaction for CAT, Ease of Cough and Sputum, chest CT outcomes, and exacerbation outcomes.
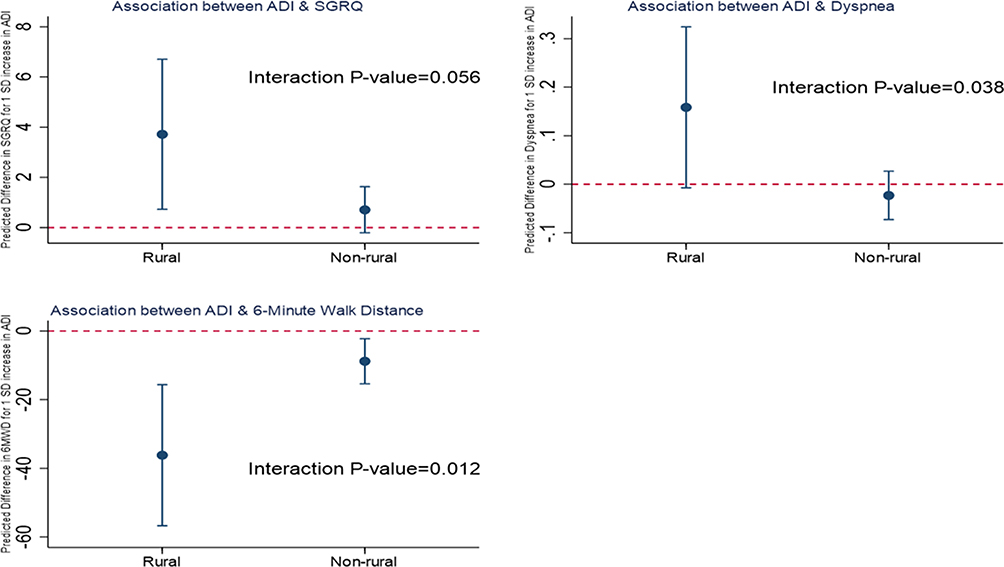 |
Figure 3 Association of continuous ADI and COPD-related outcomes by rural status. The charts illustrate the interactions between continuous ADI and rural status on their associations with SGRQ, dyspnea, and 6-minute walk distance. The y-axis represents the predicted difference in outcome for one SD increase in ADI based on the fully adjusted regression model adjusting for age, sex, education, income, marital status, BMI, FEV1% predicted, smoking status, pack years, and occupational exposure. |
Discussion
Neighborhood disadvantage has been linked with health disparities in other diseases,31,32 but studies in pulmonary disease, specifically COPD, have been limited. Our results show that living in a disadvantaged neighborhood—as measured by the Area Deprivation Index (ADI), a neighborhood-level composite socioeconomic score—is associated with worse COPD-related outcomes, including exacerbation risk in addition to respiratory symptoms, functional capacity, quality of life, and airway wall thickness on CT imaging. This effect is retained after accounting for measured individual socioeconomic variables, tobacco use, and occupational exposure to vapor, dust, gas or fumes. Our findings suggest the need for interventions that target neighborhood-level socioeconomic factors in addition to individual-level efforts designed to promote health equity in people with COPD.
Despite an increased scientific interest in the role of socio-environmental factors for COPD outcomes, few studies have investigated the role of neighborhood level factors on respiratory disease outcomes. Kind et al showed that persons in the United States living in the most disadvantaged neighborhoods, measured by ADI, had higher rates of chronic pulmonary disease when compared to persons living in less disadvantaged neighborhoods;16 however, whether individuals with COPD in the US living in disadvantaged neighborhoods have worse respiratory outcomes are unknown. Previous results in the United Kingdom (UK) suggest that the socioeconomic gradient of communities has adverse consequences on patients with COPD.33–35 Specifically, persons with COPD who lived in disadvantaged communities, measured using the English Index of Multiple Deprivation (IMD) score, had greater health care use (e.g. admissions to the emergency department and/or hospital), costs, and 1-year mortality compared to persons residing in more affluent neighborhoods.36 To our knowledge, our study is the first to investigate the association of neighborhood disadvantage (the ADI) and COPD outcomes for persons living in the United States and our findings extend existing knowledge by exploring the association of neighborhood disadvantage with several measures of COPD morbidity, including respiratory symptoms, functional status, respiratory-specific quality of life and exacerbation risk.
Similar to the study in the UK,36 we found higher odds of reporting COPD exacerbations requiring antibiotics or steroids as well as higher odds of reporting severe COPD exacerbations requiring acute health care utilization occurring in patients living in more disadvantaged areas in the US. Specifically, those residing in the most disadvantaged neighborhoods had 98% higher rate of severe COPD exacerbation compared to those in the most affluent neighborhood quintile, even after adjusting for individual socioeconomic variables, tobacco use, and occupational exposure. COPD exacerbations are costly to persons with COPD and to the healthcare system.37 Given the clinical and economic significance of exacerbations, identifying factors associated with exacerbation risk is vital for allocation of adequate resources for prevention and treatment. In addition, our results extend current knowledge, by highlighting that neighborhood disadvantage is associated with several COPD morbidity measures. For instance, we show that higher neighborhood disadvantage by ADI is linked with worse respiratory-specific quality of life, worse health status as measured by higher CAT score, increased cough and sputum production, and lower functional status as measured by 6WMD. Given these findings, our data underscore the importance of neighborhood socioeconomic environment for COPD outcomes across several domains that impact the daily life of individuals with COPD.
While our findings emphasize the association between neighborhood socioeconomic status through the area deprivation index and COPD-related outcomes, it is notable that the impact of neighborhood deprivation on some COPD outcomes is worse for rural areas versus non-rural. Though Raju et al recently showed that residing in rural areas is a risk factor for developing COPD,21 a finding that is consistent in other studies,1 it is unclear as to why neighborhood socioeconomic status may have greater adverse associations in rural areas. We do not have available information on several factors, such as distance to health care, which may help further clarify this difference by urban/rural status, but deserves further consideration. For example, it is possible that higher cigarette exposure and lack of resources, such as for smoking cessation initiatives, are more pronounced in low-income rural areas compared to urban areas.10 Overall, assessing the feasibility of prioritizing high-risk rural populations for COPD-related morbidity for allocation of healthcare resources may attenuate such disparities and should be a public health priority.
There are several plausible explanations for the observed association between neighborhood disadvantage and COPD outcomes. First, neighborhood disadvantage may be a surrogate for the hardships and struggles of everyday life that affect disease management.38 For instance, ADI may reflect the prevalence of stressors (e.g. violence) that negatively impact COPD health in the same manner reported in other diseases.39,40 Conversely, the positive impact of community resources41 and social support42 may be attenuated in more disadvantaged neighborhoods,43 leading to worse COPD outcomes. Second, disadvantaged neighborhoods may have a clustering of risk factors that worsen COPD morbidity, such as tobacco smoke exposure, indoor and outdoor air quality, substandard housing, limited access to nutritious foods, and promotion of healthy diet.44–47 For example, access to tobacco is greater in low-income neighborhoods, and high density of tobacco stores is associated with worse general health outcomes.44,45 In addition, neighborhood disadvantage may impact access to care, including transportation challenges48 and fewer health care specialists.49
Importantly, our results show that neighborhood factors, independent of individual SES factors, which have previously been linked to worse quality of life and functional status50,51 are associated with COPD outcomes. Therefore, our conclusions underscore the relevance of neighborhoods for COPD and suggest that attempts to solely change socioeconomic variables at the individual level may not be adequate. The results of our study suggest that strategies to promote health equity in COPD may be more effective if they address both individual and contextual socioeconomic factors. Area-level measures may be a clinically useful tool for identifying high-risk COPD patients and expanding health records to include spatial data may be considered to drive targeted prevention and treatment strategies for COPD.
Some limitations must be noted. The SPIROMICS data were linked to the ADI from residential addresses recorded at the baseline visit without taking into account the duration of residence at that location or subsequent changes in residence. Therefore, we cannot determine if length of time in a specific ADI impacts a person’s outcome, and whether a relocation to a neighborhood with a different ADI ranking impacts COPD outcomes. Health benefits have been noted when persons move from disadvantaged to more affluent neighborhoods.8,9 An additional exploration, a limitation of this study, is to see if there is an impact on survival on patients with COPD and their respective ADI. Given that the ADI is a composite score,15 we cannot identify which component is the predominant driver of COPD-related outcomes. However, all components that make up the index are intertwined, and policy efforts targeting one (i.e. unemployment) will likely impact others (i.e. housing). Additional research is needed to understand the role of these non-biological factors for COPD disease progression and morbidity. It should be noted that the mean/median ADI scores of our sample were below the mean/median ADI scores for the general US population, suggesting that a portion of our cohort resides in more affluent neighborhoods than the general US population. Therefore, our findings may be conservative estimates of the true population effects of neighborhood disadvantage for COPD contextual relationship between neighborhood and persons with COPD. Finally, there was significant missing data regarding individual income in the SPIROMICS dataset, which likely limits the effectiveness of the adjustment.
For the first time in a US population, we report that persons with COPD who reside in disadvantaged neighborhoods have worse outcomes related to COPD clinical status, quality of life, exacerbation risk, and airway wall thickness on CT, independent of individual SES factors. Understanding how COPD disease severity and outcomes aggregate geographically is warranted in order to identify proximal socioeconomic exposures and risk factors that can be addressed in an effort to improve COPD morbidity. Finally, further research is warranted to understand how the identification of the ADI in a person with COPD can be utilized for creating and targeting novel and equitable health strategies in the clinical setting.
Acknowledgments
The authors thank the SPIROMICS participants and participating physicians, investigators and staff for making this research possible. More information about the study and how to access SPIROMICS data is at www.spiromics.org. We would like to acknowledge the following current and former investigators of the SPIROMICS sites and reading centers: Neil E Alexis, MD; Wayne H Anderson, PhD; Mehrdad Arjomandi, MD; Igor Barjaktarevic, MD, PhD; R Graham Barr, MD, DrPH; Lori A Bateman, MSc; Surya P Bhatt, MD; Eugene R Bleecker, MD; Richard C Boucher, MD; Russell P Bowler, MD, PhD; Stephanie A Christenson, MD; Alejandro P Comellas, MD; Christopher B Cooper, MD, PhD; David J Couper, PhD; Gerard J Criner, MD; Ronald G Crystal, MD; Jeffrey L Curtis, MD; Claire M Doerschuk, MD; Mark T Dransfield, MD; Brad Drummond, MD; Christine M Freeman, PhD; Craig Galban, PhD; MeiLan K Han, MD, MS; Nadia N Hansel, MD, MPH; Annette T Hastie, PhD; Eric A Hoffman, PhD; Yvonne Huang, MD; Robert J Kaner, MD; Richard E Kanner, MD; Eric C Kleerup, MD; Jerry A Krishnan, MD, PhD; Lisa M LaVange, PhD; Stephen C Lazarus, MD; Fernando J Martinez, MD, MS; Deborah A Meyers, PhD; Wendy C Moore, MD; John D Newell Jr, MD; Robert Paine, III, MD; Laura Paulin, MD, MHS; Stephen P Peters, MD, PhD; Cheryl Pirozzi, MD; Nirupama Putcha, MD, MHS; Elizabeth C Oelsner, MD, MPH; Wanda K O’Neal, PhD; Victor E Ortega, MD, PhD; Sanjeev Raman, MBBS, MD; Stephen I. Rennard, MD; Donald P Tashkin, MD; J Michael Wells, MD; Robert A Wise, MD; and Prescott G Woodruff, MD, MPH. The project officers from the Lung Division of the National Heart, Lung, and Blood Institute were Lisa Postow, PhD, and Lisa Viviano, BSN; SPIROMICS was supported by contracts from the NIH/NHLBI (HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN268200900019C, HHSN268200900020C), and a grant from the NIH/NHLBI (U01 HL137880, and supplemented by contributions made through the Foundation for the NIH and the COPD Foundation from AstraZeneca/MedImmune; Bayer; Bellerophon Therapeutics; BoehringerIngelheim Pharmaceuticals, Inc.; Chiesi Farmaceutici S.p.A.; Forest Research Institute, Inc.; GlaxoSmithKline; Grifols Therapeutics, Inc.; Ikaria, Inc.; Novartis Pharmaceuticals Corporation; Nycomed GmbH; ProterixBio; Regeneron Pharmaceuticals, Inc.; Sanofi; Sunovion; Takeda Pharmaceutical Company; and Theravance Biopharma and Mylan. The abstract of this paper was presented at the American Thoracic Society International Conference in May 2019 as a poster presentation and conference talk with interim findings. The poster’s abstract was published in “Abstracts” in the American Journal of Respiratory and Critical Care Medicine (https://www.atsjournals.org/doi/book/10.1164/ajrccm-conference.2019.A26).
Author Contributions
PG, NNH, HW were responsible for the concept, design, data analysis, and initial writing of the manuscript. AK contributed to analyzing the area deprivation index methodology and outcomes. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The Area Deprivation Index variable was supported by National Institutes of Health-National Institute on Minority Health and Health Disparities Award (R01MD010243 [PI Kind]). This material is the result of work also supported with the resources and the use of facilities at the William S Middleton Memorial Veterans Hospital Geriatric Research, Education and Clinical Center in Madison, WI and the University of Wisconsin Department of Medicine Health Services and Care Research Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the US Department of Veterans Affairs.
Disclosure
Dr Laura Paulin reports grants from NIEHS, during the conduct of the study. Dr Nirupama Putcha reports grants from NIH, outside the submitted work. Dr Christopher Cooper reports personal fees from GlaxoSmithKline, outside the submitted work. Dr Mark Dransfield reports grants from NIH, during the conduct of the study. Dr R Graham Barr reports grants from NIH, Foundation for the NIH, grants, non-financial support from COPD Foundation, during the conduct of the study. Dr Alejandro Comellas reports grants from NIH, during the conduct of the study; non-financial support from VIDA, outside the submitted work. Dr Meilan Han reports personal fees from GSK, AZ, BI, Merck, and Mylan, non-financial support from Novartis, grants from Sunovion, outside the submitted work. Professor Stephen Peters reports grants from NIH and NHLBI, outside the submitted work. Dr Jerry Krishnan reports grants from NIH and ResMed, during the conduct of the study. Dr Wassim Labaki reports non-financial support from Pulmonx, outside the submitted work. Dr Meredith McCormack reports grants from NIH/NIMHD and Environmental Protection Agency, during the conduct of the study; personal fees from Celgene, Glaxo Smith Kline, and UpToDate, outside the submitted work. Dr Nadia Hansel reports grants, personal fees from AstraZeneca and GSK, grants from Boehringer Ingelheim and COPD Foundation, and NIH; personal fees from Mylan, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Beckfield J, Olafsdottir S, Bakhtiari E. Health inequalities in global context. Am Behav Sci. 2013;57(8):1014–1039. doi:10.1177/0002764213487343
2. Prescott E, Lange P, Vestbo J. Socioeconomic status, lung function and admission to hospital for COPD: results from the Copenhagen City heart study. Eur Respir J. 1999;13(5):1109–1114. doi:10.1034/j.1399-3003.1999.13e28.x
3. Durfey SNM, Kind AJH, Buckingham WR, DuGoff EH, Trivedi AN. Neighborhood disadvantage and chronic disease management. Health Serv Res. 2019;54(Suppl 1):206–216. doi:10.1111/1475-6773.13092
4. Sheets L, Petroski GF, Jaddoo J, et al. The effect of neighborhood disadvantage on diabetes prevalence. AMIA Annu Symp Proc. 2017;2017:1547–1553.
5. Jung D, Kind A, Robert S, Buckingham W, DuGoff E. Linking neighborhood context and health in community-dwelling older adults in the medicare advantage program. J Am Geriatr Soc. 2018;66(6):1158–1164. doi:10.1111/jgs.15366
6. Ludwig J, Duncan GJ, Gennetian LA, et al. Neighborhood effects on the long-term well-being of low-income adults. Science. 2012;337(6101):1505–1510. doi:10.1126/science.1224648
7. Acevedo-Garcia D, Osypuk TL, McArdle N, Williams DR. Toward a policy-relevant analysis of geographic and racial/ethnic disparities in child health. Health Aff (Millwood). 2008;27(2):321–333. doi:10.1377/hlthaff.27.2.321
8. Leventhal T, Dupere V. Moving to opportunity: does long-term exposure to ‘low-poverty’ neighborhoods make a difference for adolescents? Soc Sci Med. 1999;13(5):737–743. doi:10.1016/j.socscimed.2011.06.042
9. Sciandra M, Sanbonmatsu L, Duncan GJ, et al. Long-term effects of the moving to opportunity residential mobility experiment on crime and delinquency. J Exp Criminol. 2013;9(4):451–489. doi:10.1007/s11292-013-9189-9
10. Croft JB, Wheaton AG, Liu Y, et al. Urban-Rural County and state differences in chronic obstructive pulmonary disease - United States, 2015. MMWR Morb Mortal Wkly Rep. 2018;67(7):205–211. doi:10.15585/mmwr.mm6707a1
11. Ford ES. Trends in mortality from COPD among adults in the United States. Chest. 2015;148(4):962–970. doi:10.1378/chest.14-2311
12. Couper D, LaVange LM, Han M, et al. Design of the Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS). Thorax. 2014;69(5):491–494. doi:10.1136/thoraxjnl-2013-203897
13. Hansel NN, Paulin LM, Gassett AJ, et al. Design of the Subpopulations and Intermediate Outcome Measures in COPD (SPIROMICS) AIR Study. BMJ Open Respir Res. 2017;4(1):e000186. doi:10.1136/bmjresp-2017-000186
14. Kind AJH, Buckingham WR. Making neighborhood-disadvantage metrics accessible - the neighborhood atlas. N Engl J Med. 2018;378(26):2456–2458. doi:10.1056/NEJMp1802313
15. Singh GK. Area deprivation and widening inequalities in US mortality, 1969–1998. Am J Public Health. 2003;93(7):1137–1143. doi:10.2105/AJPH.93.7.1137
16. Kind AJ, Jencks S, Brock J, et al. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: a retrospective cohort study. Ann Intern Med. 2014;161(11):765–774. doi:10.7326/M13-2946
17. Singh GK, Azuine RE, Siahpush M, Kogan MD. All-cause and cause-specific mortality among US youth: socioeconomic and rural-urban disparities and international patterns. J Urban Health. 2013;90(3):388–405. doi:10.1007/s11524-012-9744-0
18. Miller MR, Crapo R, Hankinson J, et al. General considerations for lung function testing. Eur Respir J. 2005;26(1):153–161. doi:10.1183/09031936.05.00034505
19. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
20. Paulin LM, Diette GB, Blanc PD, et al. Occupational exposures are associated with worse morbidity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;191(5):557–565. doi:10.1164/rccm.201408-1407OC
21. Raju S, Keet CA, Paulin LM, et al. Rural Residence and Poverty are Independent Risk Factors for COPD in the United States. Am J Respir Crit Care Med. 2019;199(8):961–969.
22. Laboratories ATSCoPSfCPF. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
23. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
24. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
25. Rubin BK, Ramirez O, Ohar JA. Iodinated glycerol has no effect on pulmonary function, symptom score, or sputum properties in patients with stable chronic bronchitis. Chest. 1996;109(2):348–352. doi:10.1378/chest.109.2.348
26. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. The St. george’s respiratory questionnaire. Am Rev Respir Dis. 1992;145(6):1321–1327. doi:10.1164/ajrccm/145.6.1321
27. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
28. Grydeland TB, Dirksen A, Coxson HO, et al. Quantitative computed tomography measures of emphysema and airway wall thickness are related to respiratory symptoms. Am J Respir Crit Care Med. 2010;181(4):353–359. doi:10.1164/rccm.200907-1008OC
29. Kim WJ, Silverman EK, Hoffman E, et al. CT metrics of airway disease and emphysema in severe COPD. Chest. 2009;136(2):396–404. doi:10.1378/chest.08-2858
30. Sieren JP, Newell JD
31. Lantos PM, Hoffman K, Permar SR, et al. Neighborhood disadvantage is associated with high cytomegalovirus seroprevalence in pregnancy. J Racial Ethn Health Disparities. 2018;5(4):782–786. doi:10.1007/s40615-017-0423-4
32. Singh GK, Siahpush M, Azuine RE, Williams SD. Increasing area deprivation and socioeconomic inequalities in heart disease, stroke, and cardiovascular disease mortality among working age populations, United States, 1969–2011. Int J MCH AIDS. 2015;3(2):119–133.
33. Eisner MD, Blanc PD, Omachi TA, et al. Socioeconomic status, race and COPD health outcomes. J Epidemiol Community Health. 2011;65(1):26–34. doi:10.1136/jech.2009.089722
34. British Lung Foundation. Invisible Lives: Chronic Obstructive Pulmonary Disease (COPD) - Finding the MIssing Millions. London: COPD; 2007.
35. Noble M, McLennan D, Wilkinson K, Whitworth A, Barnes H, Dibden C. The English Indices of Deprivation 2007. London: Communities and Local Government; 2008.
36. Collins PF, Stratton RJ, Kurukulaaratchy RJ, Elia M. Influence of deprivation on health care use, health care costs, and mortality in COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:1289–1296. doi:10.2147/COPD.S157594
37. Toy EL, Gallagher KF, Stanley EL, Swensen AR, Duh MS. The economic impact of exacerbations of chronic obstructive pulmonary disease and exacerbation definition: a review. COPD. 2010;7(3):214–228. doi:10.3109/15412555.2010.481697
38. Disler RT, Gallagher RD, Davidson PM. Factors influencing self-management in chronic obstructive pulmonary disease: an integrative review. Int J Nurs Stud. 2012;49(2):230–242. doi:10.1016/j.ijnurstu.2011.11.005
39. Steptoe A, Feldman PJ. Neighborhood problems as sources of chronic stress: development of a measure of neighborhood problems, and associations with socioeconomic status and health. Ann Behav Med. 2001;23(3):177–185. doi:10.1207/S15324796ABM2303_5
40. Sundquist K, Theobald H, Yang M, Li X, Johansson SE, Sundquist J. Neighborhood violent crime and unemployment increase the risk of coronary heart disease: a multilevel study in an urban setting. Soc Sci Med. 2006;62(8):2061–2071. doi:10.1016/j.socscimed.2005.08.051
41. Effing TW, Bourbeau J, Vercoulen J, et al. Self-management programmes for COPD: moving forward. Chron Respir Dis. 2012;9(1):27–35. doi:10.1177/1479972311433574
42. Chen Z, Fan VS, Belza B, Pike K, Nguyen HQ. Association between social support and self-care behaviors in adults with chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2017;14(9):1419–1427. doi:10.1513/AnnalsATS.201701-026OC
43. Moskowitz D, Vittinghoff E, Schmidt L. Reconsidering the effects of poverty and social support on health: a 5-year longitudinal test of the stress-buffering hypothesis. J Urban Health. 2013;90(1):175–184. doi:10.1007/s11524-012-9757-8
44. Galiatsatos P, Kineza C, Hwang S, et al. Neighbourhood characteristics and health outcomes: evaluating the association between socioeconomic status, tobacco store density and health outcomes in Baltimore City. Tob Control. 2018;27(e1):e19–e24. doi:10.1136/tobaccocontrol-2017-053945
45. Fakunle DO, Milam AJ, Furr-Holden CD, Butler J
46. Osman LM, Douglas JG, Garden C, et al. Indoor air quality in homes of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;176(5):465–472. doi:10.1164/rccm.200605-589OC
47. Hanson C, Rutten EP, Wouters EF, Rennard S. Influence of diet and obesity on COPD development and outcomes. Int J Chron Obstruct Pulmon Dis. 2014;9:723–733. doi:10.2147/COPD.S50111
48. Sahin H, Naz I. Why are COPD patients unable to complete the outpatient pulmonary rehabilitation program? Chron Respir Dis. 2018;15(4):411–418. doi:10.1177/1479972318767206
49. Kim M, Ren J, Tillis W, Asche CV, Kim IK, Kirkness CS. Explaining the link between access-to-care factors and health care resource utilization among individuals with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:357–367. doi:10.2147/COPD.S95717
50. Jones PW, Gelhorn H, Wilson H, et al. Socioeconomic status as a determinant of Health Status Treatment Response in COPD trials. Chronic Obstr Pulm Dis. 2017;4(2):150–158. doi:10.15326/jcopdf.4.2.2017.0132
51. Medina PG, Mancilla ES, Munoz RC, Escobar MC. Effects of gender and socioeconomic status of older people on the execution of the 6 minute walk test. Rev Med Chil. 2015;143(4):484–492. doi:10.4067/S0034-98872015000400010
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.