Back to Journals » Nature and Science of Sleep » Volume 14
The Association Between Insomnia and Atherosclerosis: A Brief Report
Authors Pan XL, Nie L ![]() , Zhao SY, Zhang XB, Zhang S, Su ZF
, Zhao SY, Zhang XB, Zhang S, Su ZF
Received 27 August 2021
Accepted for publication 1 March 2022
Published 15 March 2022 Volume 2022:14 Pages 443—448
DOI https://doi.org/10.2147/NSS.S336318
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Video abstract of "Study on the relationship between insomnia and atherosclerosis" [ID 336318].
Views: 402
Xian-Li Pan,1 Li Nie,1 Shu-Yi Zhao,1 Xiao-Bao Zhang,2 Shan Zhang,2 Zeng-Feng Su2
1Chaohu Hospital Affiliated with Anhui Medical University, Chaohu City, People’s Republic of China; 2Department of General Medicine, Chaohu Hospital Affiliated with Anhui Medical University, Chaohu City, People’s Republic of China
Correspondence: Zeng-Feng Su, Tel +86 0551-82321572, Email [email protected]
Aim: The objective of the study was to clarify the occurrence of atherosclerosis in patients with insomnia.
Methods: A total of 60 patients with insomnia and 58 patients in a control group were selected to measure blood glucose, blood lipids and other biochemical and physiological indicators. Brachial-ankle pulse wave velocity (baPWV) was measured to assess arterial stiffness, and color Doppler ultrasound was used to examine carotid artery intima-media thickness (CIMT) and plaque incidence. These indicators were used to determine the occurrence and degree of carotid atherosclerosis, and to compare the differences between the two groups.
Results: While there was no significant difference in biochemical or physiological indicators between the two groups (P > 0.05), the baPWV, CIMT, and incidence of carotid plaque in the insomnia group were higher than the control group. In addition, the baPWV, CIMT, and incidence of carotid plaque in the chronic insomnia group were higher than that in the short-term insomnia group. Multiple linear regression analysis was carried out to analyze the effects of insomnia, systolic blood pressure, blood glucose, triglycerides, cholesterol, BMI, age and low-density lipoprotein on atherosclerosis. The results showed that increased CIMT was significantly correlated with insomnia in atherosclerosis group (R2=0.27 on the left, R2=0.37 on the right, P < 0.001).
Conclusion: Insomnia correlated with increased arterial stiffness and carotid atherosclerosis, and as the duration of insomnia prolongs, the correlation between them became more obvious.
Keywords: insomnia, brachial-ankle pulse wave velocity, carotid intima-media thickness, carotid plaque
Introduction
In recent years, behavioral and psychosocial factors have received more and more attention in the occurrence, prevention, and treatment of atherosclerosis and cardiovascular disease (CVD). Sleep disorder is an important behavioral factor in the occurrence of CVD.1–3 Common sleep disorders include insomnia, obstructive sleep apnea syndrome, and narcolepsy. Among these, insomnia is the most common. Its main symptoms are difficulty in falling asleep, difficulty in maintaining sleep, early awakening, decreased sleep quality, and reduced total sleep time, accompanied by daytime dysfunction.4 Common chronic insomnia can cause a series of health problems such as obesity, hypertension, diabetes, and mental and psychological diseases.5–7 Some studies have found that short sleep time and low sleep quality are associated with increased carotid intima-media thickness (CIMT) and brachial-ankle pulse wave velocity (baPWV).8 The latter is a clinical detection index of atherosclerosis and can be used as a predictor of cardiovascular events.9 In order to fully understand the occurrence of atherosclerosis in patients with insomnia to provide the possibility of early diagnosis and intervention, this study examined CIMT, carotid plaque incidence and baPWV in patients with insomnia.
Materials and Methods
Study Population
A continuous collection of patients with insomnia who were diagnosed and treated in the General Medicine Department of Chaohu Hospital affiliated with Anhui Medical University from January 2020 to December 2020 were studied. The inclusion criteria were: (1) meeting the diagnostic criteria for insomnia in the Third Edition of the International Classification of Sleep Disorders;4 Pittsburgh Sleep Quality Index (PSQI) score > 7; Insomnia severity index (ISI) score > 14; (2) 60–85 years of age; (3) education level of elementary school or above to prevent barriers to understanding; (4) lack of coronary heart disease, cerebral infarction, or other atherosclerotic diseases. Exclusion criteria included: (1) use of antidepressants, sedatives, or hypnotic drugs in the past 2 weeks; (2) alcoholism, serious endocrine diseases (such as liver disease, hyperthyroidism, pituitary tumors), or other diseases affecting the secretion of amylase (such as chronic pancreatitis, salivary gland disease); (3) pregnancy or breastfeeding; (4) visual or hearing impairment such that the patient cannot complete the test; (5) polysomnography (PSG) apnea-hypopnea index>15 times/hr. In the end, 60 patients with insomnia were included and divided into short-term insomnia (disease course <3 months, 22 cases) and chronic insomnia (disease course ≥ 3 months, 38 cases). Fifty-eight subjects with normal sleep during the same period were selected as a control group. There were no significant differences between the two groups in terms of age, gender, body mass index (BMI), blood pressure (BP), fasting blood glucose (FBG), blood lipids, homocysteine (Hcy), or smoking history. This study was a cross-sectional study and was reviewed and approved by the Ethics Committee of Chaohu Hospital affiliated with Anhui Medical University. All subjects signed an informed consent form. And we confirm that this study was conducted in accordance with the Declaration of Helsinki.
Subjective Measures for Assessing Sleep
Pittsburgh Sleep Quality Index (PSQI): The PSQI is a 19-item assessment of sleep quality and sleep disorders over a one-month interval. Scores range from 0 to 21, with a score above 7 indicating poor sleep quality.
Insomnia Severity Index (ISI): ISI is a 7-item questionnaire that assesses nighttime symptoms and effects of insomnia during the previous month. All items were rated as 0, 1, 2, 3, 4 (0= no, 4= very severe) with total scores ranging from 0 to 28. Scores from 0–7 indicated no insomnia, 8–14 indicated subthreshold insomnia, 15–21 indicated moderate insomnia, and 22–28 indicated severe insomnia. The mean duration of insomnia in the chronic insomnia group was 13.2±4.7 months.
Detection of Biochemical and Other Indicators
Total cholesterol (TC), triglycerides (TG), low density lipoprotein cholesterol (LDL- C), blood uric acid, FBG, and Hcy levels were measured using an automatic biochemical analyzer. A mercury column sphygmomanometer was used to measure the BP of the research subjects.
Carotid Artery Ultrasound Examination
A CX50 color Doppler ultrasound detector (Philips) was used to measure CIMT in supine patients. The ultrasound probe was a 7.0–12.0 MHz linear array probe. The intima-media thickness of the common carotid artery was measured at the position of the common carotid artery. Longitudinal ultrasound imaging of the posterior wall of the common carotid artery at 1.5cm near the posterior wall of the fork shows relatively low echo separation and two parallel bright lines, which are called double line images. CIMT takes the inner line as the dividing line between the inner membrane and the lumen and the outer line as the distance between the middle and outer membrane dividing lines. Three consecutive cardiac cycles were measured and the average value was taken. Generally speaking, CIMT ≥ 0.09 cm at the carotid artery bifurcation is used as the standard for intima-media thickening, which is also the diagnostic standard for atherosclerosis. When the CIMT is locally thickened > 0.13 cm, it is defined as carotid atherosclerotic plaque formation.10 Thickness measurement is mainly carried out on the long axis image, combined with the short axis image. Unilateral or bilateral thickening ≥0.09cm and/or carotid atheromatous plaque formation, including the resulting complex lesions of ulcers, calcified aneurysms, and luminal stenosis, are all regarded as carotid atherosclerosis.
Pulse Wave Velocity Measurement
BaPWV measurement was performed by a trained professional using the Omron BP203RPEIII arteriosclerosis detector. Patients were fasted for 8 hours on the morning of the test and rested in a supine position for 20 minutes at a room temperature of 20°C to 25°C. After cleaning the skin locally with alcohol, the pressure cuff was placed on the brachial artery with the lower edge of the cuff is 2–3cm from the cubital fossa transverse stripes. Pressure cuffs were also placed at the position of the posterior tibial artery of both ankles 1–2cm from the lower edge of the cuff. Electrocardiogram electrode clamps were placed on the distal extremities. Measurements were made according to the operating procedures of the instrument, and data was recorded after the signal was clear and the baseline was stable. The baPWV blood pressure and electrocardiogram were recorded while the patient was supine. The sampling time was10s, automatic gain analysis and quality adjustment were performed during sampling, and all parameters were stored for analysis.
Statistical Methods
SPSS20 statistical software was used. Normally distributed measurement data are presented by (x ± s), non-normally distributed measurement data are presented by M (P25-P75), and count data are presented by [n (%)]. To compare between the groups, two independent sample t-tests were used when the variances of the measurement data were homogeneous and showed a normal distribution. The rank sum test was used when the variances were uneven or non-normally distributed, and the chi-square test was used for categorical data. The difference was statistically significant with P < 0.05.
Results
The results showed that there was no statistical significance in the age or gender compositions between the insomnia group and the control group (P > 0.05), there were no statistically significant differences in diastolic blood pressure, blood glucose, cholesterol, triglyceride, low density lipoprotein, homocysteine, BMI or smoking history between the two groups (P > 0.05), as shown in Table 1.
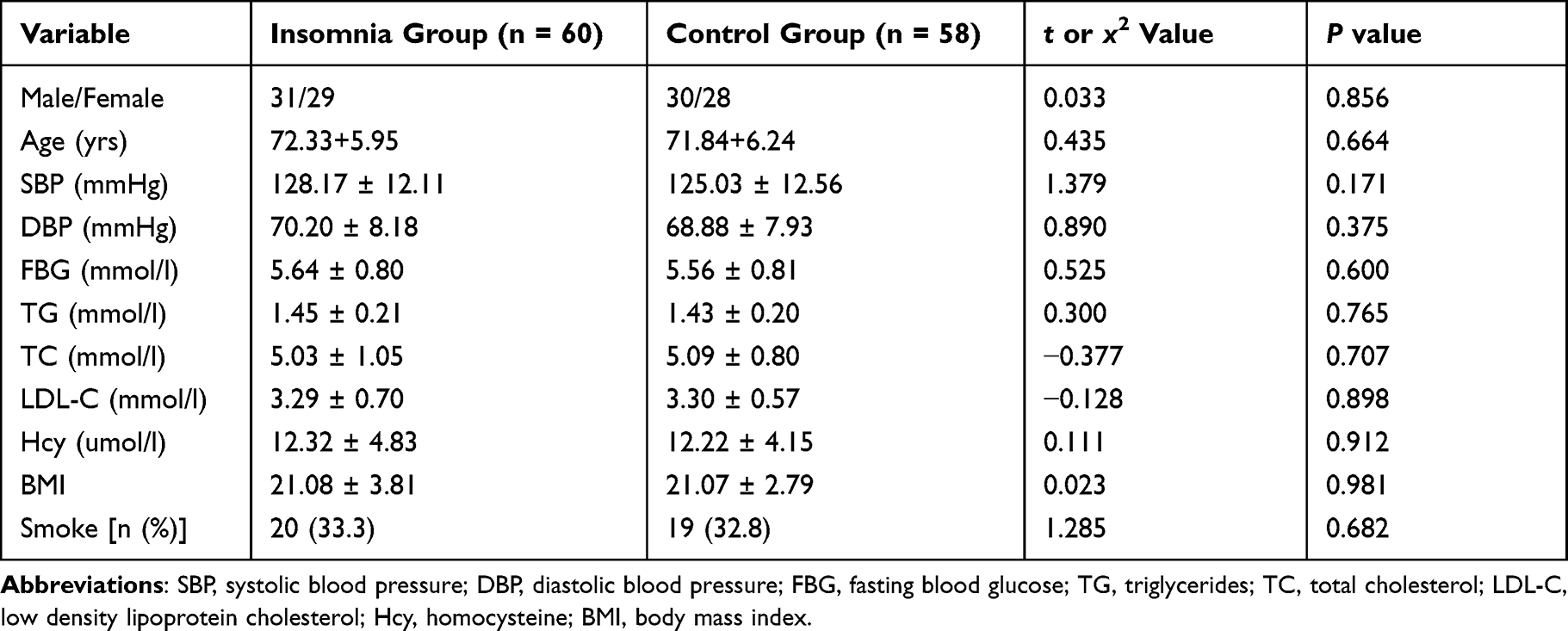 |
Table 1 Comparison of Gender, Age, Biochemical and Physiological Data |
The results showed that systolic blood pressure (SBP) in the insomnia group was slightly higher than that in the control group, but the difference was not statistically significant (P = 0.171).
The results showed that the baPWV was significantly higher in the insomnia group compared to the control group (1412.33 ± 141.80 cm/sec vs 1256.21 ± 140.00 cm/sec, t= 6.017, P < 0.001). In addition, greater intima-medial thickening was present in both the left (L) and right (R) carotid arteries in the insomnia group (L-CIMT 0.11 ± 0.03 mm vs 0.07 ± 0.02 mm, t = 6.996, P < 0.001; R-CIMT 0.12 ± 0.04 mm vs 0.07 ± 0.02 mm, t = 8.736, P < 0.001). Finally, the incidence of carotid plaque was also significantly greater in the insomnia group compared to the control group (31.7% vs 19.0% control, χ2 = 1.162, P = 0.023), as shown in Table 2.
 |
Table 2 Comparison of baPWV, CIMT, and Carotid Plaque Incidence: Insomnia versus Control |
Given the increase in atherosclerotic measures in the insomnia group, we were interested in whether the duration of insomnia played a role in the severity of atherosclerosis. We compared these parameters in the short-term and longer-term insomnia groups. The results showed that the baPWV, CIMT, and incidence of carotid plaque were all higher in the longer-term insomnia group than in the short-term insomnia group (Table 3). The baPWV was 1465.00 ± 142.58 cm/sec in the long-term group, compared to 1333.33 ± 98.94 cm/sec in the short-term group (t = 3.932, P < 0.001). The L-CIMT was 0.12 ± 0.03 mm in the long-term group, compared to 0.10 ± 0.03 mm in the short-term group (t = 2.473, P = 0.016). The R-CIMT was 0.13 ± 0.03 mm in the long-term group, compared to 0.11 ± 0.04 mm in the short-term group (t = 2.573, P = 0.013). Finally, the incidence of carotid plaque was 36.1% in the long-term group and 25.0% in the short- term group (χ2 = 1.101, P = 0.041).
 |
Table 3 Comparison of baPWV, CIMT and Carotid Plaque Incidence: Duration of Insomnia |
Multiple linear regression analysis was carried out to analyze the effects of insomnia, systolic blood pressure, blood glucose, triglyceride, cholesterol, BMI, age and low-density lipoprotein on atherosclerosis. The results showed that increased CIMT was significantly correlated with insomnia in atherosclerosis group (R2=0.27 on the left, R2=0.37 on the right, P < 0.001), as shown in Table 4.
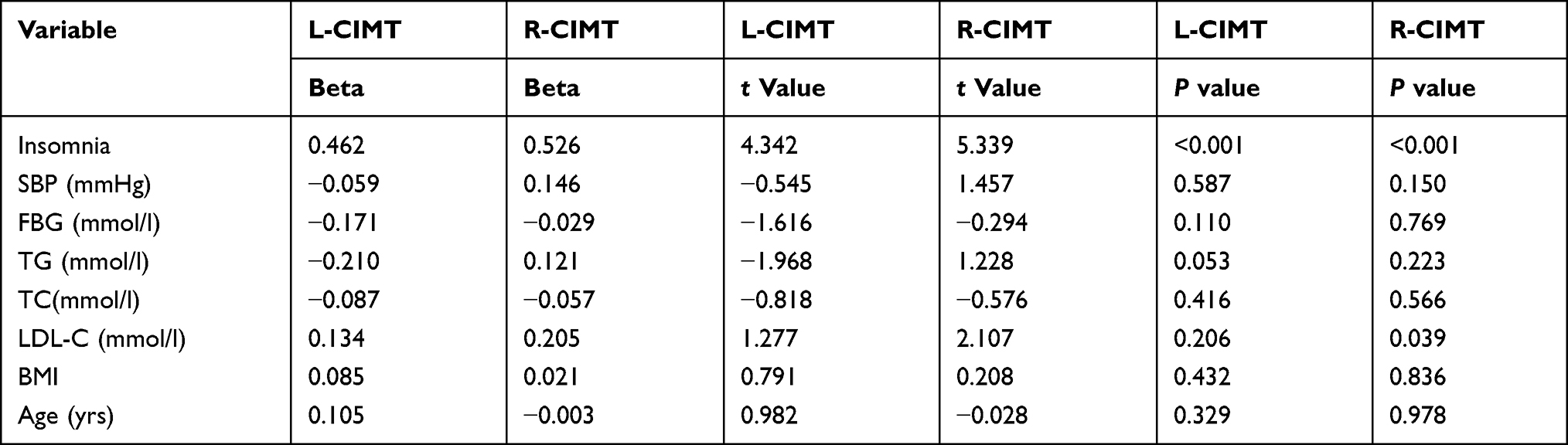 |
Table 4 Multiple Linear Regression Results of Influencing Factors of CIMT in Atherosclerosis Group |
Discussion
Atherosclerosis is a systemic diffuse disease that often affects large blood vessels, and the carotid artery is the most commonly involved site. As an evaluation method for early vascular disease, non-invasive detection techniques such as carotid ultrasound and PWV have been widely used. PWV can reflect the stiffness of large arteries and has been used clinically for many years as an index for evaluating arterial elasticity. It also has a good predictive value for cerebrovascular events, with a value of 1400cm/s as a cut-off point to discriminate patients with stroke or coronary heart disease. CIMT is recommended for use as a detection index for systemic atherosclerosis and can be used as a follow-up and predictive index for evidence of cardiovascular disease.11
Studies have shown that shorter sleep time increases the risk of diseases such as atherosclerosis.12 In a study of 86 elderly patients with atherosclerosis, those with a Pittsburgh Sleep Quality Index of short sleep time (<5hr) had a CIMT value that was significantly higher than that of the control group with a longer sleep time (>7hr).13 An additional study of 201 elderly patients showed that CIMT was higher in patients with subjective persistent insomnia than in patients without insomnia.14 Some large- scale studies have examined the relationship between subjective and objective sleep time and quality and CIMT and baPWV in healthy people. In a survey of 617 middle- aged, healthy subjects (37–52 yrs), Sands et al showed that shortening of sleep time is related to the increases in CIMT,8 and a recent study showed that short sleep time and fragmented sleep were independently associated with an increased risk of subclinical atherosclerosis.15 The results of our study were similar to the above-mentioned studies. In addition, analysis of the effect of the duration of insomnia on atherosclerosis shows that longer duration insomnia, the stronger the correlation.
Research on how sleep disorders lead to atherosclerosis includes several potential mechanisms. Short sleep time and low sleep quality may cause oxidative stress, subclinical systemic inflammation, and endothelial dysfunction.16 Short sleep time and low sleep quality may have a strong impact on aspects of endocrine, immune, and metabolic reactions, possibly interfering with the daily rhythm of the hypothalamus- pituitary-adrenal axis. Activation of this axis leads to increased cortisol levels, and high cortisol and insulin resistance are related to cardiovascular risk factors and coronary heart disease.17 Additionally, research shows that poor sleep quality caused by insomnia increases the risk of hypertension, diabetes, and dyslipidemia,18–21 which are key risk factors for the development of atherosclerosis and cardiovascular disease.
The results of a 2019 study showed that mice with long-term sleep fragmentation (sleep fragmentation, sleep interruption, or lack of sleep) have more severe atherosclerosis, which is related to the levels of hypocretin (Hcrt) produced in the hypothalamic region of the brain. Decreased Hcrt accelerated the production of immune cells, aggravated inflammation, and increased the development of atherosclerosis. When the hormone levels of these mice were restored, atherosclerosis was reduced.22 Studies have also shown that the levels of three key circulating micro RNAs (miRNAs) in the blood of patients with insufficient sleep (< 7hr), namely miRNA-125A, miRNA- 126, and miRNA-146a, were 40–60% lower than those in participants who slept for >7 or 8 hours. These three miRNAs are involved in maintaining vascular function by regulating gene expression, mainly to inhibit the expression of pro-inflammatory proteins. This study demonstrates the influence of good sleep on maintaining healthy arteries and good blood circulation.23
Conclusions
Our results show that insomnia correlated with increased arterial stiffness and carotid atherosclerosis, and as the course of insomnia prolongs, the stronger the correlation with increased arterial stiffness and atherosclerosis. Through the measurement of baPWV, CIMT, and carotid artery plaque incidence, atherosclerosis can be detected and diagnosed early, thereby providing early intervention for atherosclerosis in patients with insomnia, further avoiding the occurrence of cardiovascular and cerebrovascular diseases.
Acknowledgments
This study was funded by the Anhui Medical University Scientific Research Fund Project (No. 2020xkj219) and the Colleges and Universities of Anhui Provincial Department of Education (No. KJ2020A0189).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang T, Redline S. Cross-sectional and prospective associations of actigraphy- assessed sleep regularity with metabolic abnormalities: the multi-ethnic study of atherosclerosis. Diabetes Care. 2019;42(8):1422–1429. doi:10.2337/dc19-0596
2. Crunkhorn S. Sleep protects against atherosclerosis. Nat Rev Drug Discov. 2019;2:234–235.
3. Kadoya M, Koyama H. Sleep, autonomic nervous function and atherosclerosis. Int J Mol Sci. 2019;20(4):1–16. doi:10.3390/ijms20040794
4. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
5. Fulop T, Larbi A, Dupuis G, et al. Immunosenescence and inflamm-aging as two sides of the same coin: friends or foes? Front Immunol. 2018;8:1960. doi:10.3389/fimmu.2017.01960
6. Taylor DJ, Mallory LJ, Lichstein KL, et al. Comorbidity of chronic insomnia with medical problems. Sleep. 2007;30(2):13–18. doi:10.1093/sleep/30.2.213
7. Holth JK, Fritschi SK, Wang C, et al. The sleep-wake cycle regulates brain interstitial fluid tau in mice and CSF tau in humans. Science. 2019;363(6429):880–884. doi:10.1126/science.aav2546
8. Sands MR, Lauderdale DS, Liu K, et al. Short sleep duration is associated with carotid intima-media thickness among men in the Coronary Artery Risk Develop mentin Young Adults(CARDIA) Study. Stroke. 2012;43(12):2858–2864. doi:10.1161/STROKEAHA.112.660332
9. Munakata M. Brachial-ankle pulse wave velocity in the measurement of arterial stiffness: recent evidence and clinical applications. Curr Hypertens Rev. 2014;10(1):49–57. doi:10.2174/157340211001141111160957
10. Murray CSG, Nahar T, Kalashyan H, et al. Ultrasound assessment of carotid arteries: current concepts, methodologies, diagnostic criteria, and technological advancements. Echocardiography. 2018;35(12):2079–2091. doi:10.1111/echo.14197
11. Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2007;28(12):1462–1536. doi:10.1093/eurheartj/ehm236
12. Li-Ping C, Chung-Yi L. Work-related psychosocial hazards and arteriosclerosis a cross-sectional study among medical employees in a regional hospital in Taiwan. Int Heart J. 2015;56(6):644–650. doi:10.1536/ihj.15-143
13. Nakazaki C, Noda A, Koike Y, et al. Association of insomnia and short sleep duration with atherosclerosis risk in the elderly. Am J Hypertens. 2012;25(5):1149–1155. doi:10.1038/ajh.2012.107
14. Nagai M, Hoshide S, Nishikawa M, et al. Sleep duration and insomnia in the elderly: associations with blood pressure variability and carotid artery remodeling. Am J Hypertens. 2013;26(4):981–989. doi:10.1093/ajh/hpt070
15. Dominguez F, Fuster V, Fernandez-Alvira JM, et al. Association of sleep duration and quality with subclinical atherosclerosis. J Am Coll Cardiol. 2019;73(11):134–144. doi:10.1016/j.jacc.2018.10.060
16. Chen CY, Chen CL, Yu CC, et al. Association of inflammation and oxidative stress with obstructive sleep apnea in ischemic stroke patients. Sleep Med. 2015;16(2):113–118. doi:10.1016/j.sleep.2014.07.027
17. Lim GB. Sleep reduces haematopoiesis and atherosclerosis via a neuroimmune axis. Nat Rev Cardiol. 2019;16(4):199. doi:10.1038/s41569-019-0174-5
18. Vgontzas AN, Liao D, Bixler EO, et al. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep. 2009;32(8):491–497. doi:10.1093/sleep/32.4.491
19. Qian Y, Yi H, Zou J, et al. Independent association between sleep fragmentation and dyslipidemia in patients with obstructive sleep apnea. Sci Rep. 2016;6(5):84–89. doi:10.1038/srep26089
20. Barros D, Garcia-Rio F. Obstructive sleep apnea and dyslipidemia. From animal models to clinical evidence. Sleep. 2018;12(3):33–39.
21. Kent BD, Grote L, Ryan S, et al. Diabetes mellitus prevalence and control in sleep- disordered breathing: the European Sleep Apnea Cohort (ESADA) study. Chest. 2014;146(6):982–990. doi:10.1378/chest.13-2403
22. McAlpine CS, Kiss M, Rattik S, et al. Modulates hematopoiesis and protects against atherosclerosis. Nature. 2019;566(7744):383–387. doi:10.1038/s41586-019-0948-2
23. JG H, MA L, Garcia V, et al. Insufficient sleep is associated with pro- atherogenic circulating microRNA signature. Exp Physiol. 2019;12(6):82–91.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.